

Successful implementation required a large amount of logistic planning, flexibility, and improvisation. Close and timely postdelivery support by the manufacturer is crucial to the authors' ongoing success.
SUMMARY:
Low-field, portable MR imaging may expedite patient management in the setting of critical illness. We successfully implemented low-field MR imaging at the Queen Elizabeth Central Hospital in Malawi; a low-resource setting. We present our experience of low-field, portable MR imaging start-up and use in Malawi; the first of its kind in Sub-Saharan Africa, together with complementary troubleshooting mechanisms that may be used especially in similar resource-constrained contexts.
Low-field, portable MR imaging scanners may aid in the care of critically ill patients, especially those in whom transport to fixed magnets is challenging. These include unconscious comatose patients undergoing evaluation in emergency departments or bed-bound in-patients who have developed sudden-onset neurologic deficits. Portability of this family of MR imaging scanners enables this imaging technique to be used as a point-of-care tool, potentially leading to a faster diagnosis and expedited treatment, which may be life-saving. Other favorable characteristics that separate this type of low-field scanner from a high-field scanner include reduced overall scanner purchase price and running costs (reduced energy consumption), reduced costs relating to infrastructure requirements to house and operate it compared with a high-field scanner, reduced or often nullified electromagnetic interference, and increased patient comfort (reduced noise during scan acquisition and reduced patient-perceived claustrophobia). Conversely, low-field portable scanners have lower resolution and contrast of acquired images, constraints with regard to coil types limiting the body parts accessible to imaging, and limited sequence acquisitions (as in for example the current inability to acquire postcontrast T1-weighted images).1,2
Although most experience with this imaging technique has taken place in high-income countries, medical care facilities in low-resource settings may also benefit from this technology. In many low- and middle-income countries, there is a high burden of both communicable and noncommunicable diseases with a predilection for the neuroaxis. MR imaging diagnostics may be pivotal in establishing diagnoses and optimizing patient management. In environments where conventional CT and MR imaging are often unavailable, access to a low-field, portable MR imaging scanner may transform a wide variety of patients’ diagnostic journeys, treatment plans, and outcomes.
We recently implemented a low-field (0.0625T), portable MR imaging scanner at the Queen Elizabeth Central Hospital in Blantyre, Malawi. In the past year, our facility has acquired 260 brain scans using this technology. Indications for imaging are divided into the routine clinical care arm (for which infections, pediatric developmental delay, and, to a smaller extent, posttrauma prognostication are the most common indications) (Fig 1), and the clinical research arm (Fig 2).
FIG 1.

Hyperfine Swoop MR images of a 12-year-old child who was admitted to the pediatric ward at our institution with focal neurology, reduced consciousness, and septicemia when CT imaging was not available at our institution. The child’s MR imaging demonstrated a right-sided subdural empyema, which was confirmed at surgery. MR imaging findings were of a well-defined, septated T2-weighted hyperintense subdural fluid collection associated with mass effect (A), with a corresponding T1-weighted hyperintense subdural fluid collection (B).
FIG 2.

Hyperfine Swoop MR images of a 6-year-old child who was admitted to our institution under the research study arm with a decreased level of consciousness and malaria parasitemia. The child’s MR imaging demonstrates typical findings associated with malarial encephalopathy of diffuse right-sided parietotemporal T2-weighted hyperintensity in the gray and subcortical white matter with an associated localized mass effect in the form of sulcal effacement on the coronal T2-weighted sequence (A), with corresponding restriction of diffusion on the DWI b=900 image and ADC images (B and C).
Here, we describe the challenges that our group encountered during this process of low-field MR imaging scanner implementation in a resource-constrained environment and the solutions we implemented to overcome these problems. Our experiences may be applicable to implementation of such technology in other low-resource environments (Table).
Challenges encountered and proposed solutions for low-field MR imaging implementation in a resource-limited setting
| Challenge | Proposed Solution/Troubleshooting Option |
|---|---|
| Equipment delivery and receipt logistics | Needs assessment of the most reliable and safe equipment transportation routeUse of a reputable carrier with tracking facilitiesInsurance coverageUncrating and setup training before equipment receiptAcquisition of tools needed for uncrating and setup before equipment receiptOn receipt, close inspection of external container gauges for warnings |
| Equipment roadmap | Needs assessment of the expected routes of equipment portability within the health care facilityConstruction of low-incline, smooth ramps to mitigate steep and irregular terrain |
| Equipment storage | Needs assessment of storage and operating conditions inclusive of temperature and humidity |
| Equipment operation | Training of end user operators |
| Equipment utilities | Needs assessment of hospital infrastructure including electricity supply and Internet speedAcquisition of a manufacturer-recommended compatible electrical surge protector |
| Non-resource-constrained specific items | Patient and equipment safetyPatient privacy and confidentiality |
Challenge I: Logistics of Delivery and Receipt of Equipment
Currently, the only available portable low-field MR imaging scanner is Hyperfine Swoop (Hyperfine Research). The first challenge in implementing this technology for our group in Malawi was transporting the scanner to southeastern Africa. Safe and efficient equipment transportation from the manufacturer to the receiving hospital is often a daunting and multistep process. There are few shippers with experience in the transportation of large, heavy, delicate imaging equipment. When the equipment reaches its final destination, it is often received only by those working in the hospital and not by manufacturer’s representatives (Fig 3). Because uncrating and setup is a complex process, it is important that at least 1 person with prior training on the container-unpacking process be present during equipment receipt. The process of uncrating and setup requires supplementary tools at the receiving site and knowledge of the indicators on the external shell of the container to ensure proper care of the equipment during transportation. At the time of receipt, the container must be examined for gauges indicating possible equipment malalignment or temperature breaches during transit. Once the Hyperfine Swoop is unpacked, it can be set up so that the scanner is ready for use immediately. In our facility, the time interval between opening the crate and scanning our first patient was 4 hours.
FIG 3.

The Hyperfine Swoop, still crated, at the time of receipt at our institution.
Solutions.
Once a suitable shipper is identified, flexibility and back-up plans (in case the route of travel is interrupted) are needed. Accuracy and clear communication with shipping agents relating to the dimensions of the holding crate are vital to avoid unnecessary in-transit equipment-delivery delays.
In our case, a member of our team traveled to the manufacturer’s headquarters in Connecticut to receive training on how to uncrate and inspect the equipment on receipt at its final destination.
Challenge II: Building a Roadmap for Equipment Movement
The Hyperfine Swoop MR imaging scanner weighs 630 kg and is moved by a motor at its base. Movement of the equipment up ordown inclines of >5° is not recommended by the manufacturer because the motor may not be powerful enough to safely navigate these inclines or declines. Therefore, the terrain over which the MR imaging scanner is to be transported must be closely examined before equipment receipt. Off-loading from long-distance transport, often by forklift, may not be able to deliver the machine close to its final location. Challenges in low-resource hospital settings include steep or rough terrain inclinations, narrow passageways (the Hyperfine Swoop is 158 cm wide), or unroofed building routes.
Solutions.
We suggest a thorough predelivery review of the roadmap on which the scanner will be maneuvered to allow mitigation of terrain challenges before equipment receipt. In our case, terrain challenges required a re-evaluation of the setting in which the scanner would be housed. Additional troubleshooting mechanisms include the construction of strong, shallow-incline, smooth ramps at crucial locations.
Challenge III: Equipment Storage
As with all imaging equipment, low-field, portable MR imaging scanners must be stored and operated within a range of temperature and humidity conditions. These variables are especially important in low-resource peri-equatorial locations where a stable and uniform health care facility environment may not be present.
Solutions.
Our group suggests a thorough needs assessment focusing on optimal environment preparation through the installation of air conditioning and dehumidifier units at sites where equipment is intended to be stored before equipment receipt. The manufacturer recommends that the Hyperfine Swoop be operated and stored at temperatures of 15–30 °C with an operating humidity of 15%–85%, noncondensing.
Challenge IV: Operating the Equipment
The lower magnetic field strength of portable MR imaging systems results in fewer restrictions on the site of equipment storage or operation. Metal objects are allowed in the scanning room in proximity to the scanner. This adds to the cost-effectiveness of this type of imaging because acquiring MR imaging–compatible equipment (eg, patient monitors and transportation trolleys) is unnecessary. No previous radiography technology training is required to operate a portable, low-field MR imaging scanner; the equipment was designed for use by clinicians at the point of care—a quality that makes it very attractive for use in resource-constrained settings where trained radiographers are uncommon. Nonetheless, operators require training from the manufacturer. Optimally, they should be identified and trained before scanner receipt.
Solutions.
While the Queen Elizabeth Central Hospital is fortunate to have an MR imaging–trained radiographer on staff, other nonradiography team members have successfully operated the equipment. A manufacturer-led remote training session on equipment operation and a user-friendly iPad (Apple) control panel interface led to successful scan acquisition by non-radiography-trained operators. Excellent support from the manufacturer, including trouble shooting and periodic software upgrades, is crucial to the smooth operation of the equipment.
Challenge V: Adapting to Different Patient Populations
The Hyperfine Swoop is FDA-approved for use in children. However, currently available portable, low-field MR imaging scanners only accommodate adult-sized head coils. Head positioning of young children within the coil is challenging. If a child’s head is not placed far in enough into the coil, it produces an artifact in the occipital region of the images, impacting the completeness of interpretation.
Solutions.
The percentage of the patient’s head that is located within the scanner is indicated on the Hyperfine app when imaging begins. Our group recommends that after acquiring the first localizer sequence, special attention be paid to a flashing red alert icon in the top right of the iPad controller screen. If this icon is clicked and the error message indicates that the “percentage of section detected” is <75%, the patient needs to be repositioned with the head placed further into the coil. Our preferred technique to overcome this challenge is to swaddle and cross the child’s arms over the thorax in a cloth, allowing the patient to be placed further within the coil. Padding under the patient’s upper back also aids in moving the head further into the coil (Fig 4). We suggest noting this alert immediately after obtaining localizer sequences to correct the patient’s position and avoid artifacts on subsequently acquired images.
FIG 4.
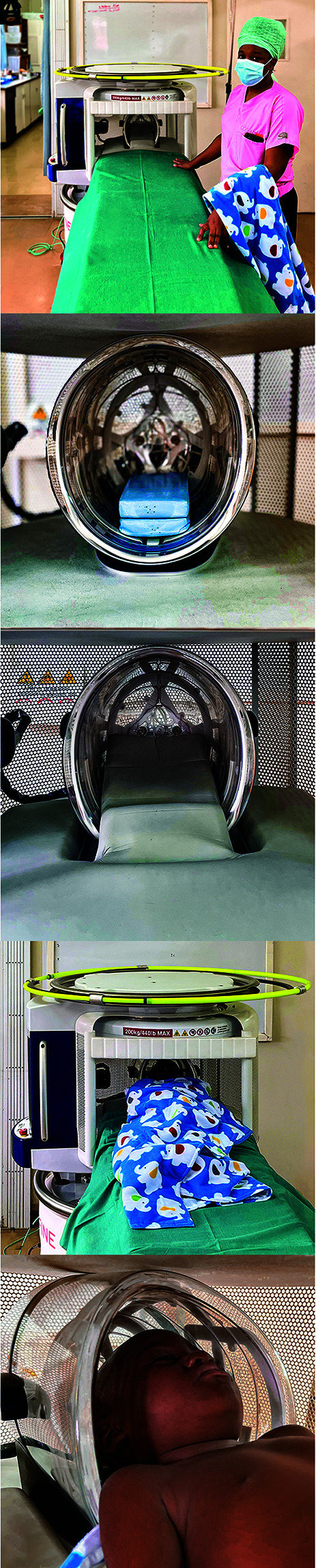
The Hyperfine Swoop at our institution is set up in an appropriately optimized temperature- and humidity-controlled dedicated scanning room (A) with a patient scanning couch of an appropriate height adjacent to it. B and C, The blue padding block was sourced by our group and is applied within the head coil of the scanner with the gray manufacturer-provided padding applied over it, extending onto the patient’s scanning couch. The role of the blue padding block is to elevate the patient’s head a little further, thereby optimizing the patient’s head position further in the scanner head coil for more optimal head coverage during scanning. A patient model within the scanner (D) demonstrating the swaddling technique and a detailed view of the patient’s head position within the head coil (E).
Challenge VI: Equipment Utility Challenges
Images obtained by the scanner are stored in the Internet cloud. Both a stable electrical supply and adequate Internet speed and stability are required for the scan acquisition and uploading of images for interpretation. Achieving appropriate Internet bandwidth speed and stability can be challenging in resource-constrained environments. A slow or unstable Internet connection results in loss of communication between the iPad console and the scanner, necessitating a complete restart of the scan. Slow uploading of images to the cloud results in delays in both image interpretation and patient management. In Malawi, an Internet bandwidth speed of ≥2.1 MB per second allows smooth image acquisition and uploading.
Solutions.
Before the receipt and setup of the equipment in Malawi, our group acquired a permanently connected voltage-compatible, manufacturer-recommended electrical surge protector. The scanner is otherwise operated through a standard AC wall power outlet.
In the relatively infrequent instances in which image upload to the cloud platform was delayed due to temporary Internet unavailability, our group resorted to 1 of 2 troubleshooting mechanisms. If a radiologist was on site during acquisition, the images may be directly visualized on the iPad controller. If a radiologist was not physically present, screenshots of the iPad controller could be emailed to remotely placed radiologists for preliminary interpretation. Once Internet connectivity was restored, radiologists provided full interpretation using conventional methods using the full PACS functionality. These 2 troubleshooting mechanisms enabled a short turnaround time to provide a preliminary report, ensuring little-to-no adverse clinical care impact related to delayed MR imaging interpretation.
Challenge VII: Site Nonspecific Challenges
Other implementation challenges are not context- or equipment-specific. These include gentle patient maneuvering into the scanner to avoid patient or equipment harm and ensuring equipment cleanliness. As with high-field scanners, patient noncooperation leading to motion artifacts may reduce the ability to acquire high-quality images. We use “feed and wrap” techniques for neonates, swaddling and imaging during periods of natural sleep whenever possible, in a sleep-conducive MR imaging scanner environment. Sensitivity to patient privacy and confidentiality is a further priority.
Solutions.
We have a predefined equipment-cleaning program followed by designated, preselected personnel. We ensure patient privacy and confidentiality through restriction of image access on the cloud platform to preselected authorized personnel.
Our successful implementation of this technology at the Queen Elizabeth Central Hospital, the largest public health care facility in Malawi, has facilitated patient care. Successful implementation required a large amount of logistical planning, flexibility, and improvisation. Close and timely postdelivery support by the manufacturer is crucial to our ongoing success. With careful planning, imaging modalities such as this low-field, portable MR imaging scanner now in place in our hospital can be implemented in other resource-constrained environments.
Footnotes
This work was supported by the National Institutes of Health, grant No: 5U01AI126610.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- 1.Lee CS, Davis SM, McGroder C, et al. Analysis of low-field MRI scanners for evaluation of shoulder pathology based on arthroscopy. Orthop J Sports Med 2014;2:2325967114540407 10.1177/2325967114540407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Deoni SC, Bruchhage MM, Beauchemin J, et al. Accessible pediatric neuroimaging using a low field strength MRI scanner. Neuroimage 2021;238:118273 10.1016/j.neuroimage.2021.118273 [DOI] [PubMed] [Google Scholar]