

Dystonia is a syndrome consisting of sustained or intermittent contraction of muscle that leads to abnormal movements or postures. The etiology of dystonia remains largely unknown, whereas genetic etiologies have aroused sustainable attention. With the development of sequencing methods and bioinformatic algorithms, vacuolar protein sorting 16 homolog gene (VPS16) and VPS41 are 2 novel causative genes for early‐onset dystonia. 1
In our study, we systematically screened VPS16 and VPS41 in a cohort of 219 Chinese patients with isolated dystonia and 19 patients with combined dystonia with whole‐exome sequencing who have been excluded for known genetic causes (Table S1). Rare variants with minor allele frequency <0.1% in VPS16 and VPS41 were analyzed. Sanger sequencing was performed to validate the variants.
No truncating variant in VPS16 was identified. However, we identified 1 patient with a rare missense variant (c.692A>G, p. Tyr231Cys) in VPS16. The patient was a 9‐year‐old girl who developed difficulty in writing and abnormal movements in both upper arms at the age of 8. Neurological examination revealed that the patient had mild dystonia with upper limb myoclonus, but without psychiatric problems and intellectual disability (Table S2). The symptom was aggravated by the moods of anger and excitement, was relieved at rest, and disappeared during sleep. The dystonic symptoms gradually expanded to the trunk and the right lower limbs. The patient underwent brain magnetic resonance imaging examination in the local hospital, which revealed no structural abnormality in the brain. Before she came to our clinic, the patient had been treated with Traditional Chinese Medicine, and she claimed relief in these symptoms. At our clinic, she was treated with antiepileptic treatment for 1 month, including levetiracetam (UCB Pharma S.A.) and Topamax (Xian Janssen Pharmaceutical Ltd,China), but responded poorly. The variant in VPS16 had a very low frequency in the public database (moderate evidenve for pathogenicity 2) and was predicted to be damaging by several in silico tools (Supporting evidence of pathogenicity 3). Moreover, the variant was absent in the patient's parents and was considered de novo (Fig. 1) (Strong evidence of pathogenicity 2). Therefore, the variant (c.692A>G, p. Tyr231Cys) can be classified as a likely pathogenic variant 2 (Table S3). No homozygous variant or compound heterozygous variant was identified in VPS41 among our cohort.
FIG. 1.
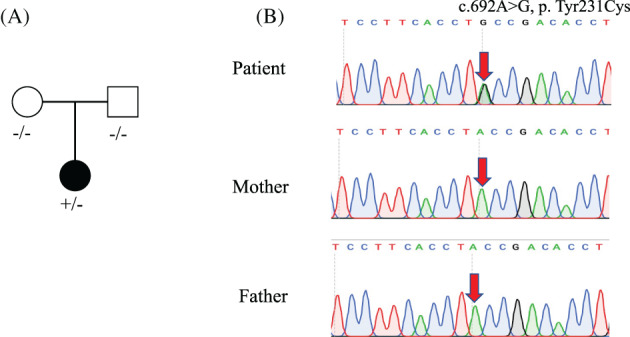
(A) Pedigree charts of the proband family. Filled and empty symbols indicate individuals affected with dystonia and without dystonia, respectively. ‐, reference allele; +, mutated allele. (B) Sanger sequencing of the pedigree. Segregation analysis showed that the variant was de novo.
The study by Steel et al identified loss‐of‐function variants and microdeletions in VPS16 to be autosomal dominant inherited and VPS41 to be autosomal recessive inherited for early‐onset dystonia. 1 Further microscopy study of patient‐derived lymphocytes and fibroblasts observed endosomal–lysosomal dysfunction, which might contribute to the pathogenesis of dystonia. 1 Since then, a few studies reported several other loss‐of‐function variants and microdeletions of VPS16 in patients with generalized dystonia and multifocal dystonia from different ethnicities, where myoclonus was rarely described 3 , 4 , 5 , 6 , 7 (Table S4). A missense variant of uncertain significance in a Chinese patient with segmental dystonia (cranial–cervical dystonia) was also reported. 3 In the current study, we identified 1 likely pathogenic de novo rare missense variant in a Chinese patient with childhood‐onset generalized dystonia with myoclonus, which has been rarely reported previously.
In conclusion, our observation of 1 likely pathogenic de novo missense variant in VPS16 in a Chinese patient with childhood‐onset generalized dystonia with myoclonus expanded both the genotype and phenotype spectrum of VPS16‐related dystonia, suggesting that a missense variant in VPS16 should also be valued. However, no patient with autosomal recessive inherited VPS41 was identified in the current study. more studies in different genetic background are needed.
Author Roles
(1) Research Project: A. Conception, B. Organization, C. Execution; (2) Statistical Analysis: A. Design, B. Execution, C. Review and Critique; (3) Manuscript Preparation: A. Writing of the First Draft, B. Review and Critique.
X.J.G.: 1A, 1B, 1C, 2A, 2B, 3A
J.Y.L.: 1C, 2B
Y.B.H.: 1C, 2B
L.Y.Z.: 1C, 2B
H.F.S.: 1A, 1B, 2C, 3C
Disclosures
Ethical Compliance Statement
The study was approved by the ethics committee of West China Hospital, Sichuan University. Written informed consent was obtained from all participants. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding Sources and Conflict of Interest
This work was supported by the 1.3.5 Project for Disciplines of Excellence, West China Hospital, Sichuan University (ZYJC18038 and ZY2016203). All authors declare no conflicts of interest.
Financial Disclosures for the Previous 12 Months
Nothing to report.
Supporting information
Table S1. Demographic features of the studied participants.
Table S2. Description of the psychiatric and cognitive assessments of the patient.
Table S3. Description of the variant in VPS16 identified in the patient.
Table S4. Summary for the published studies about VPS16S in dystonia.
Relevant disclosures and conflicts of interest are listed at the end of this article.
Data Availability
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- 1. Steel D, Zech M, Zhao C, et al. Loss‐of‐function variants in HOPS complex genes VPS16 and VPS41 cause early onset dystonia associated with lysosomal abnormalities. Ann Neurol 2020;88:867–877. 10.1002/ana.25879. [DOI] [PubMed] [Google Scholar]
- 2. Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med 2015;17:405–423. 10.1038/gim.2015.30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Li LX, Jiang LT, Liu Y, et al. Mutation screening of VPS16 gene in patients with isolated dystonia. Parkinsonism Relat Disord 2021;83:63–65. 10.1016/j.parkreldis.2020.12.014. [DOI] [PubMed] [Google Scholar]
- 4. Li X, Wang L, Guo Y, Wan XH. Mutations in the VPS16 gene in 56 early‐onset dystonia patients. Mov Disord 2021;36:780–781. 10.1002/mds.28540. [DOI] [PubMed] [Google Scholar]
- 5. Ostrozovicova M, Jech R, Steel D, et al. A recurrent VPS16 p.Arg187* nonsense variant in early‐onset generalized dystonia. Mov Disord 2021;16:16–18. 10.1002/mds.28647. [DOI] [PubMed] [Google Scholar]
- 6. Zech M, Boesch S, Škorvánek M, et al. Clinically relevant copy‐number variants in exome sequencing data of patients with dystonia. Parkinsonism Relat Disord 2021;84:129–134. 10.1016/j.parkreldis.2021.02.013. [DOI] [PubMed] [Google Scholar]
- 7. Pott H, Brüggemann N, Reese R, et al. Truncating VPS16 mutations are rare in early onset dystonia. Ann Neurol 2021;89:625–626. 10.1002/ana.25990. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Demographic features of the studied participants.
Table S2. Description of the psychiatric and cognitive assessments of the patient.
Table S3. Description of the variant in VPS16 identified in the patient.
Table S4. Summary for the published studies about VPS16S in dystonia.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.