

Abstract
BACKGROUND:
Even in an era of automation and digitalization, Manual Material Handling (MMH) can be called the most common industrial task. The aim of this study was to evaluate the prevalence of musculoskeletal disorders (MSDs) induced by manual handling tasks on the workers of a printing factory in Tehran in 2017 and then to evaluate the effectiveness of a training intervention based on health promotion.
MATERIALS AND METHODS:
This study had quasi experimental design and was conducted on 40 men. First, demographic data were collected and the Nordic questionnaire was used to determine the prevalence of MSDs in workers. Then, MMH tasks were assessed using Manual Handling Assessment Chart (MAC). A short training course was designed to promote health. Finally, the same MMH tasks were re-evaluated 3 months after the training intervention.
RESULTS:
Among the various tasks, the highest prevalence of work-related MSDs (WMSDs) was observed in the lower back (77.5%) and shoulder (62.5%). Based on the final scores of the MAC method, the jobs that received the highest scores were cutting (individual lifting), with 22 scores and action level “immediately necessary,” cutting (individual load carrying), with 15 scores with action level “urgently needed.” Arranging the forms (individual lifting) received a similar score. After the training intervention, the estimated risk level reduced by 12, 9, and 6 points, respectively, reaching a safe action level, i.e., “necessary in the future.”
CONCLUSION:
The results demonstrated that educational interventions might be equally effective in low-technology work environments. More in general, the MAC method can be used to make informed planning of educational interventions against WMSDs risk in MSDs. This health promotion approach is critical for care of human recourse.
Keywords: Health education, low back pain, musculoskeletal disorders, Nordic questionnaire
Introduction
Printing industry is among the main industries in the country of Iran. Factories in Tehran, which is the capital of Iran, are significantly active in this industry. Workers in this industry are exposed to chemicals and solvents.[1] Furthermore, due to the type of process and their tasks, they are widely involved in inappropriate postures and manual material handling (MMH).[1] Manual handling is defined as any activity that requires a person to use force to push, pull, lift, lower, carries, or holds an object.[2] Occupational tasks in the printing industry that are considered ergonomically, include Manually carrying newspaper packages, repetitive movements of upper limb associated with paper cutting machines, cleaning and preparing the printing machine, embedding the papers and maintaining the machines, which usually puts a person in a difficult situation causing musculoskeletal damages.[1,3]
In general, musculoskeletal disorders (MSDs) have a multifactorial origin with physical, psychological, and social causes. The physical causes may include incorrect physical postures, repetitive movements, excessive force throughout the working day, as well as an unsuitable environment while MMH.[4] Studies have shown that mismatch between people and the workplace can lead to pain in the lower leg, foot sole, knee, neck, shoulders, and waist.[5] Work fatigue is defined as a difficulty in concentrating on continuous activities,[6] which is an effective factor in increasing the incidence of human error.[7] The possible consequences of fatigue are decreased ability in information processing, decreased level of safety, and level of physical and mental health and increased reaction time.[8] Work fatigue is recognized as a risk factor for MSDs. A work environment designed based on ergonomic principles can prevent MSDs among workers and also reduce fatigue among them.[9]
Work-related MSDs (WMSDS) can cause productivity reduction, decrease work quality,[10] and increase in absenteeism.[11] Evidence has shown that reducing and preventing musculoskeletal problems is an important global priority.[12] In assessing MSDs, self-report questionnaires[13] are used as a tool to collect data, with The Nordic Musculoskeletal Questionnaire (NMQ) as the most known.[14] In this questionnaire, a body map is provided which divides body into nine separate areas (neck, shoulders, elbows, wrists/hands, upper back, lower back, hips/thighs, and ankles/feet) and the presence or absence of pain and severity of pain in these areas has been monitored for the past 12 months.[15]
Khandan et al.,[16] showed that MSDs in the lower back with 35.1% had the highest prevalence among workers in the printing industry. Frequent and heavy weight MMH has been cited as a risk factor for occupational back pain.[17] Therefore, due to the importance of this ergonomic risk factor, the main purpose of ergonomic programs is to prevent MSDs related to lifting and repetitive tasks.[18] One of the preventive measures undertaken by various organizations is conducting methods for determining the permitted weight in manual handling tasks. These include Snook tables, manual handling assessment chart (MAC), National Institute for Occupational Safety and Health equations, and others. There are advantages and disadvantages to using any of the methods above.[17]
One method of assessing the risk of MSDs is the MAC. This method has been developed by the ergonomic laboratory of Health and Safety Executive (HSE) organization to facilitate the inspection of companies that perform MMH operations and it is superior compared to other methods of assessing physical condition in MMH in terms of ease of use and validity (accuracy). With this method, three types of activities can be evaluated, namely individual load lifting, individual load carrying, and team handling.[17] In the study by Hashemi Habibabadi et al.,[19] which were performed to assess MSDs in Bandar-Abbas charging berth workers using MAC method, the results showed high risk levels, namely risk levels 3 and 4 in all three activities of individual load lifting, individual load carrying, and team handling.
Ergonomic training is useful as a low-cost intervention to reduce the risk factors in WMSDs.[20] Medical evidence suggests that effective ergonomic interventions have reduced the number and severity of related injuries.[21] Ergonomic interventions include engineering controls and management controls. Engineering intervention strategies include job design and designing proper tools for the job. Management control strategies include employee training and job rotation. The training methods along with engineering strategies are one of the most important intervention approaches to reduce injuries to individuals. Training is more affordable and accessible than other types of interventions, but it is more difficult to achieve effective results compared to technical interventions.[21,22] In a study by Morken et al.,[23] showed that a training program for workers to acquire the knowledge on the prevention of MSDs in the workplace would prevent health disabilities, including MSDs. Education is one of the most important factors affecting safety and health and thus health promotion, which has been widely studied by other researchers.[24] The health education approach actually starts from the ground up and advises people to change their behaviour and move in a specific direction that is beneficial to their health.[25] Health education for workers is in the field of work fatigue, proportion of work environment components with workers, ergonomic risk factors and the correct way of MMH with the aim of preventing MSDs and safe load carrying, which ultimately leads to improved health among workers. The study by Feuerstein et al.,[26] showed that ergonomic training along with evaluation and correction of workstations significantly reduced pain and work-related symptoms in upper limbs.
In the printing factory examined in the current study, magazines were classified in large numbers and the worker carried the magazines in several batches. In this case, the worker was faced with a significant load weight and due to the low number of workers in the factory each person had to carry that load rapidly. Furthermore, due to the repetitive nature of the work, the workers of this factory were exposed to risk factors for MSDs. Accordingly, the importance of training on MSDs and the correct principles of MMH, also to increase productivity and eliminate economic losses caused by MSDs, evaluation of MMH tasks, training intervention and in fact health education based on health promotion seemed necessary.
Therefore, this study was conducted with the following objectives on the workers of a printing factory in Tehran:
Evaluation of the prevalence of MSDs using the Nordic questionnaire
Evaluation of MMH using MAC method
Training intervention and health education based on health promotion
Re-evaluation of MMH using MAC method after training intervention.
Materials and Methods
Study design and setting
This study had quasi experimental design. The production line of the factory was visited and it was coordinated with the management of the printing factory. The various tasks of the printing production line were examined, and the workers with MMH tasks were selected. The MMH tasks were analysed and a description of each task was prepared. Then, each task classified into three categories of, individual load lifting, individual load carrying, and team handling.
The production process of the factory was as follows: In the rolling section, the rolls were opened and placed inside the machine. Then these rolls were moved by two workers and were placed inside the printing machine using a jack. In the printing section, two workers lifted the ink barrel and placed it on top of the other barrel, and the ink barrel was carried to the printing machine by a jack. In the cutting section, the worker lifted the papers from the pallet and placed them on the machine. After cutting the paper with a Hindu machine, the worker carried the paper out of the machine and placed it on a pallet. In the folding section, the worker lifted the covers of the magazine off the table and placed it on the conveyor, then lifted the sorted magazines off the machine and placed them on the pallet. In the forms arranging section, the worker carried the forms from the surface of the pallets and placed them on the conveyor. After passing the forms through the printing machine, the worker lifted the forms from the conveyor, put them on top of each other, then placed them on a table surface and strapped around them. Two people carried the forms from the table surface and put them on pallets. In the waste collection section, the worker collected the waste paper from the ground and placed them in a paper pressure chamber to be used for other purposes. In the waste disposal section, a worker picked up the wastes and transported it to a pickup truck.
Study participants and sampling
The study population consisted of 45 men, 5 of whom were excluded due to a history of MSDs. In the study by Panjali et al.,[27] was performed on 44 workers in one of the metal casting industries with MMH tasks. In the study by Dehnavi et al.,[28] the subject number was calculated using the following formula: N= ([2 σ2][z1-α/2 + z1-β]2)/d2. According to the previous studies, the standard deviation and absolute error are 30. The reliability of this test is 95% and the test power is considered equal to 0.80. By substituting the values in the above formula, a minimum subject size of at least 17 was obtained per group. Finally, 40 men who were eligible for the study were evaluated before the intervention and re-evaluated after the training intervention. The inclusion criteria were no history of severe MSDs or accidents affecting the musculoskeletal system.
Data collection tool and technique
The demographic data got collected including age, sex, height, weight, level of education, marital status, smoking, work experience, and average working hours per day. Then, the NMQ was used by self-report method. For this questionnaire, reliability tests were performed using a test–retest method which the results showed that 0%–23% of the answers was non-identical. Furthermore, the validity of the NMQ against clinical history showed a range of 0%–20% disagreement. In this questionnaire, the body is divided into nine areas.[15] The first question for each area of the body was whether the worker had experienced any musculoskeletal discomfort in that area in the last 12 months. If the worker did not have any symptoms, he should have selected the “no symptoms” option. If he did report symptoms, an additional question was asked about the severity of the symptoms: (mild, moderate, or severe)[29] .
Manual handling assessment chart before training intervention
In order to evaluate the MMH and the working and environmental conditions, the worker was filmed during the work cycle (each task is usually <15 min, which is repeated regularly and makes the cycle). Filming was done on the days and hours when the worker had the most inappropriate posture (the day and time of which were determined after starting the study and observing the workers in all hours of the week). Then, the weight of the load carried by subjects was measured using SG100 industrial scale. The MAC evaluation chart was used to review and score manual handling tasks. The validity and reliability of this method has been approved by the HSE and has been mentioned in many existing studies.[27,30] Three MAC evaluation charts were used to examine the three tasks of individual load lifting, individual load carrying and team handling. Each chart contains parameters assigning a colour code per task and a numerical score that these codes and scores were extracted from the relevant tables and graphs.[31] Risk levels are categorized as follows:
G: Green-low risk level
The vulnerability of individuals should be considered in expiry cases.
A: Amber-medium risk level
Works closely examined.
R: Red-high risk level
Immediate measures are needed. This risk can put a large number of workers in danger.
P: Purple-very high risk level
Such an operation expresses a serious risk of injury and should be carefully monitored, especially when the total weight load is on a person.
Finally, to determine the total score of the MAC, the scores dedicated to each variable were summed up, and for each task a total score was obtained. The control action is based on the total MAC score:
Level 1: If 4 ≤ MAC ≤ 0 action is not required
Level 2: If 12 ≤ MAC ≤ 5 action is needed in the near future
Level 3: If 20 ≤ MAC ≤ 13, the action is urgently needed
Level 4: If 31 ≤ MAC ≤ 21 the action is immediately necessary.
Tasks with control action other than “action is not necessary” should be corrected.[30]
Training intervention
Having obtained permission from the factory management, the workers gathered in a conference room on the office site and were taught the principles of MMH by lecturing by 2 experts with a master's degree in occupational health and safety at work and presenting a training PowerPoint. Workers were trained in five sessions, each lasting 45 min. Training session was included information on ergonomic risk factors and MMH, MSDs, the importance of preventing MSDs, warm-up exercises at the beginning and during work to reduce excessive work-related stress, correcting workstation settings, the correct way of using equipment as well as the correct way of performing MMH during each task, charging fire extinguisher capsules at proper periods, considering sufficient space to carry the load, proper lighting, proper hygiene, adequate first aid facilities, proper disposal of waste and sewage, minimizing the risk of fire and electrocution, improving the safety of the building according to the latest standards.[5,32] Furthermore, posters in the form of messages and images related to MMH were installed at the workstations. Finally, based on the results of the MAC evaluation and according to the type of control action, tasks were prioritized and suggestions were made to improve the tasks, work environment, and reduce the level of risk, including:
Train the worker to put the arm and forearm vertically when lifting the load, lifting the load above the knee height or under the height of the elbow while body is straight. Load symmetrically and hold the load and hands in front of the body. The lower back should be without rotation or bending, or the bending and rotation should be low
Cut the number of journals and formats half that each time they carry, which will reduce the weight of the load
Increase co-operation while team handling the load, carrying it in coordination and at the same time
Lay the pallets closer to the outlet of the machine to reduce the carrying distance of the load
Keep the ground surface permanently dry and clean and keep it in good condition, and the waste papers should be collected quickly from the floor of the factory to prevent them from getting stuck in worker's hands and feet during loading.
Manual handling assessment chart evaluation after training intervention
Eventually, 3 months later,[28] the tasks were re-evaluated and scored by MAC method to evaluate the effect of training intervention and ensure safe MMH by workers.
Ethical consideration
In order to observe the research ethics, all participants were informed of the working method and objectives of the study, and the information was kept confidential and written consent was obtained from the individuals. The present study was conducted with the full approval of the ethics committee of the Shahid Beheshti University of Medical Science (Approval ID: IR. SBMU. PHNS. REC.1396.28)
Statistical analysis
Statistical analysis of the obtained data was performed using the SPSS software (SPSS V.22 Inc., Chicago, IL, USA). Kolmogorov–Smirnov test was used to check the normal distribution of the data. Descriptive statistical indices, including mean, standard deviation, and frequency, were used in accordance with quantitative and qualitative data. Mann–Whitney U nonparametric test was used to investigate the relationship between demographic variables and MSDs. Furthermore, a significant difference in MAC score before and after the training intervention was determined using the nonparametric Wilcoxon signed-rank test. Significance level in the tests was considered 0.05.
Results
The study population was 40 male participants ranging in age from 26 to 45 years. The mean and standard deviation of age is 36.4 ± 5.7. The minimum work experience among the workers was 5 years and the maximum was 13 years, the mean and standard deviation of work experience was 8.45 ± 2.49 years. The height of the workers was in the range of 170–188 cm with the average height and standard deviation of 179.1 ± 4.5 cm. The weight range was 71–89 kg with the mean and standard deviation of 79 ± 4.5 kg. Workers’ body mass index (BMI) was in the range of 22.6–26.4 kg/m2, BMI mean and standard deviation was 24.6 ± 0.8 kg. Furthermore, 27 (67.5%) of subjects were in the healthy weight range and 13 (32.5%) were in the overweight range (obesity limit).
The level of education of all participants was below high-school diploma. Thirty-one participants (75.5%) were married with 9 single (22.5%) participants. Furthermore, 13 participants (32.5%) were smokers and 27 participants (67.5%) were non-smokers. The distribution of tasks with MMH among workers is as follows: 26 participants (65%) had the task of arranging the forms, 4 participants (10%) had the task of rolling, 2 participants (5%) had the task of cutting, 2 participants (5%) had the task of waste disposing, 2 participants (5%) had the task of printing, 2 participants (5%) had the task of folding, and 2 participants (5%) had the task of waste collecting.
Findings from the Nordic questionnaire showed that 90% of workers had WMSDs. The highest prevalence of 72.5% was related to the lower back and prevalence in other areas were 62.5% (shoulders), 55% (knees), 52.5% (elbows), 35% (neck), 17.5% (wrists/hands), 15% (upper back), 10% (ankles/feet), and 5% (hips/thighs), respectively [Figure 1].
Figure 1.
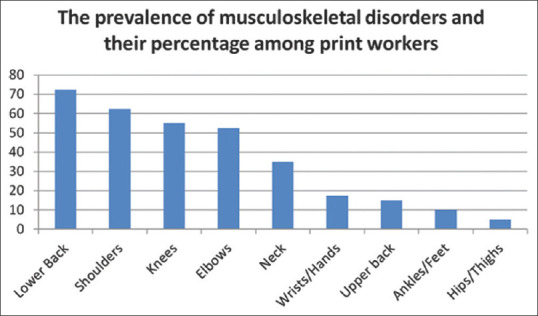
The prevalence of musculoskeletal disorders and their percentage among print workers
Based on the Kolmogorov–Smirnov test, the data were not normally distributed. According to nonparametric Mann–Whitney U test, it was found that there was no significant difference between demographic variables including Work experience, height, weight, BMI, age, type of task, smoking, and marital status with MSDs (P > 0.05) [Table 1]. The evaluation of four MMH tasks with the highest MAC score is shown in Tables 2 and 3.
Table 1.
Results of studying a significant difference of demographic variables between two groups
| Variable | Musculoskeletal Disorders | Sig* | |
|---|---|---|---|
|
| |||
| Has it Mean | Does not have Mean | ||
| Work experience (Year) | 19.35 | 30.88 | 0.06 |
| Height (cm) | 20.25 | 22.75 | 0.71 |
| Weight (kg) | 19.92 | 25.75 | 0.37 |
| BMI (kg/m2) | 20.33 | 0.811 | 22 |
| Age (Year) | 20.47 | 0.983 | 20.75 |
*Difference between two groups
Table 2.
Results of MAC method for individual load lifting situation in tasks 1 & 2
| Task 1 : Cutting | Task 2 : Arranging the forms | ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Risk Factors | Before Intervention | After Intervention | Risk Factors | Before Intervention | After Intervention | ||||
|
|
|
|
|
||||||
| Color Code (P, R, A, G) | Numeric Score | Color Code (P, R, A, G) | Numeric Score | Color Code (P, R, A, G) | Numeric Score | Color Code (P, R, A, G) | Numeric Score | ||
| Weight/Frequency of load | A | 4 | G | 0 | Weight/Frequency of load | G | 0 | G | 0 |
| Distance of load to body | R | 6 | A | 3 | Distance of load to body | A | 3 | G | 0 |
| the height of the load lifting place | R | 3 | R | 3 | the height of the load lifting place | R | 3 | G | 0 |
| Checking the Lumbar situation (rotation and bending sideways) | R | 2 | G | 0 | Checking the Lumbar situation (rotation and bending sideways) | R | 2 | G | 0 |
| Body movement constraints | R | 3 | R | 3 | Body movement constraints | R | 3 | R | 3 |
| load gripping | A | 1 | A | 1 | load gripping | A | 1 | A | 1 |
| ground condition | A | 1 | A | 1 | ground condition | A | 1 | A | 1 |
| Other environmental factors | R | 2 | A | 1 | Other environmental factors | R | 2 | A | 1 |
| Final Score | 5R3A | 22 | 2G4A2R | 12 | Final Score | 4G1R3A | 15 | 4R3A1G | 6 |
Table 3.
Results of MAC method for individual load carrying and team handling situation in tasks 3 & 4
| Task 3 : Cutting (individual load carrying) | Task 4 : Arranging the forms (team handling) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Risk Factors | Before Intervention | After Intervention | Risk Factors | Before Intervention | After Intervention | ||||
|
|
|
|
|
||||||
| Numeric Score | Color Code (P, R, A, G) | Numeric Score | Color Code (P, R, A, G) | Numeric Score | Color Code (P, R, A, G) | Numeric Score | Color Code (P, R, A, G) | ||
| Weight/Frequency of load | A | 4 | G | 0 | Weight/Frequency of load | R | 6 | G | 0 |
| Distance of load to body | A | 3 | A | 3 | Distance of load to body | A | 3 | G | 0 |
| Body/load asymmetry | G | 0 | G | 0 | the height of the load lifting place | G | 0 | G | 0 |
| limits of the body movements | A | 1 | A | 1 | Checking the Lumbar situation (rotation and bending sideways) | G | 0 | G | 0 |
| load gripping | A | 1 | A | 1 | Body movement constraints | G | 0 | G | 0 |
| ground condition | A | 1 | A | 1 | load gripping | A | 1 | A | 1 |
| Other environmental factors | R | 2 | A | 1 | ground condition | A | 1 | A | 1 |
| The distance that load carry | A | 1 | G | 0 | Other environmental factors | R | 2 | R | 2 |
| obstacles on the load carrying route | A | 2 | A | 2 | Collaboration between individuals | A | 1 | G | 0 |
| Final Score | 1R7A1G | 15 | 3G6A | 9 | Final Score | 2R4A3G | 14 | 2A1R | 4 |
Task 1 was cutting, whose job description was that the worker lifted the papers from the pallet and placed them on the work surface of the machine. Then, the papers were cut by the machine. For this task, the individual load lifting worksheet of MAC evaluation chart was used. The MAC score was 22 (5R3A) before the training intervention and decreased to 12 (2G4A2R) after the training intervention [Table 2].
Task 2 was arranging the forms, whose job description was that the worker lifted the forms from the pallet surface and placed them on the conveyor. For this task, the individual load lifting worksheet of MAC evaluation chart was used. The MAC score was 15 (4R3A1G) before the training intervention and decreased to 6 (4G1R3A) after the training intervention [Table 2].
Task 3 was cutting, whose job description was that the worker picked up the papers that have been cut from the output of the machine and after handling the load for a while, placed them on the pallet. For this task, the individual load carrying worksheet of MAC evaluation chart was used. The MAC score was 15 (1R7A1G) before the training intervention and decreased to 9 (3G6A) after the training intervention [Table 3].
Task 4 was also arranging the forms, whose job description was that the worker lifted the categorized magazines from the conveyor and put them on top of each other, then placed them on a table surface and strapped around them. Two people carried the forms from the table surface and put them on pallets. For this task, the team handling worksheet of MAC evaluation chart was used. The MAC score was 14 (2R4A3G) before the training intervention and decreased to 4 (2A1R) after the training intervention [Table 3].
The results of the MAC evaluation before the training intervention showed that 65% (26 cases) of the tasks are at risk level 3, which is “urgently needed.” 15% (6 cases) of tasks are at risk level 4 which is “immediately necessary.” 15% (6 cases) of tasks are at risk level 2 which is “needed in the near future” and 5% (2 cases) of tasks are at risk level 1 which is “not required.”
After the training intervention, 60% (24 cases) of the tasks were at risk level 2 which is “needed in the near future” and 40% (16 cases) of the tasks were at risk level 1 which is “not required”. Furthermore, according to the analysis of Wilcoxon signed-rank test, there was a significant difference between MAC score before and after the training intervention (P = 0.0001). In order to reduce the risks of MSDs associated to the four MMH tasks with highest MAC score, the following technical measures were proposed:
Using mechanical lifting equipment to transfer stacks of magazines and forms from the conveyor to the pallet and vice versa, which in the type of glossy paper has more than 70 kg
Using a trolley that has a higher surface than the pallet; in this way, the distance between the load to the body and the height of the load lifting position decreases
Improving the layouts of workstations, by slightly moving the workbench and the machine, so that the person does not take limited posture due to the limited space
Installing additional lamps and opening windows to use natural light for improving brightness in the workstations; opening doors to use the outside air flow to make the indoor temperature and ventilation suitable.
Discussion
The mean of the participants’ age showed that the participants were young to middle-aged. The mean of the participants’ body mass also confirms the fact that the subjects were neither obese nor very thin. The small standard deviation of the variables indicates that the participants are close to each other in terms of the desired variables and the exact matching of the participants is observed to some extent. The points above indicate that the participants selected for the study were within the defined framework of the study.
The findings of the study showed that the prevalence of MSDs in 3 areas of the lower back (72.5%), shoulders (62.5%), and knees (55%) was higher than other parts of the body. The main causes of these disorders can be as carrying large and heavy batches of paper and magazines, improper load lifting and unsuitable environmental and work conditions, which puts a lot of pressure on the mentioned areas. Khandan et al.,[16] concluded that the highest prevalence of MSDs among printing industry workers is in the lower back, shoulders, and ankles. The results of this study are consistent with the present study. One of the main reasons for the increase in MAC score was the weight of the load, which can cause damages to the lower back and other parts of the body. The high percentage (90%) of the prevalence of MSDs among the subjects and the allocation of the highest percentage of prevalence to the lower back (72.5%) indicated the need to evaluate the manual handling tasks and proper training of MMH to workers. After the training intervention, the weight of the load was reduced and the posture of the workers during the load handling as well as the working environment conditions improved. Hashemi Habibabadi et al.[19] also considered excess load weight as an important risk factor and one of the reasons for the increase in MAC score.
The results showed that there was no significant relationship between demographic variables such as work experience, age, height, weight, BMI, type of task, smoking, and marital status with MSDs. The study of Hashemi Habibabadi et al.[19] is consistent with this finding.
The MAC risk level for task 1 (cutting/individual load lifting) was level 4, which was reduced to risk level 2 after the training intervention. In this task, the heavy weight of the load, the large distance between the load and the body, the height of the load lifting place, the improper position of the lower back increased the MAC score and created an unsuitable condition for lifting the load. After the training intervention, the score of the mentioned parameters decreased and therefore task 1 changed to a safe and appropriate task [Table 2].
The MAC risk level for task 2 (arranging the forms/individual load lifting) was level 3, which was reduced to risk level 2 after the training intervention. The reason for improving the load lifting situation was that, after the training intervention, the worker raised the height of the pallet surface, so the score of “the height of the load lifting place” decreased. The worker corrected his posture and moved the load close to the body without rotating or bending the lower back to the sides. Furthermore, the temperature of the factory was adjusted as the ventilation condition improved. Therefore, task 3 was changed to a safe and appropriate task [Table 2].
The MAC risk level for task 3 (cutting/individual load carrying) was level 3, which was reduced to risk level 2 after the training intervention. The reason for the improvement in the load carrying situation was that, after the training intervention, the amount of papers the worker carried was cut to half, thus the weight of the load was reduced, a number of lamps were installed in the factory and the factory temperature was adjusted by improving the ventilation condition. In results the “other environmental factors” parameter score was reduced, and by moving the pallets closer to the machine output, the distance at which the load was carried was reduced to a minimum, so task 2 was changed to a safe and convenient task [Table 3].
The MAC risk level for task 4 (arranging the forms/team handling) was level 3, which was reduced to risk level 1 after the training intervention. The reason for improving the load lifting situation was that, after the training intervention, the weight of the load was reduced. The workers corrected their posture and lifted the load close to the body, the cooperation between people while lifting the load increased and the body's limits of movement while lifting the load was deleted. Therefore, task 4 was changed to a safe and appropriate task [Table 3]. In the study by Dormohammadi et al.,[30] the risk level for the task of team handling was in level 3 in moulding unit, which is consistent with MAC action level before intervention for tasks 2, 3, and 4 in the current study.
The results of MAC evaluation before and after the training intervention showed that the risk level of all tasks was reduced to levels 1 and 2 (acceptable risk level), which this reduction was significant (P = 0.0001) according to the analysis of Wilcoxon signed-rank test between MAC Score, before and after the intervention. Both results confirm the effect of the training intervention on the correct load handling and reduction of the MAC score.
Dehnavi et al.[28] results are consistent with the current study stating that the positive effect of training-engineering interventions can reduce the severity of pain in the different parts of the body and reduce the risk factors for cumulative injuries in the workplace of printing industry workers. In a review study, Faisting and de Oliveira Sato[33] stated that ergonomic training alone or in combination with other types of interventions is effective in reducing WMSDs. In addition, other studies[20] are consistent with the present study. Proportion between workers and work environment components was one of the important factors that were considered during the training intervention and health education. In the long run, disproportion causes fatigue among workers. In addition, high workload, shift work, stress, and lack of workforce can be the causes of work fatigue. Due to the role of fatigue in reducing the quality of work and human error and the subsequent occurrence of MSDs, effective training in this field can eventually improve the health of workers.[5,24]
Limitations and recommendations
The current paper had limitations, including time and space constraints in accurate filming of the worker's physical condition due to high work load, small workstation, and lack of sufficient space, with the possibility of damages to experts in such a small space. Therefore, to conduct similar research in future, it is suggested that factories with a large number of workers (larger sample size) and a larger work environment be selected to remove the restrictions and ensure safety in the workplace. The results of the study can also be used to properly design the workstations.
Conclusion
Assessing the prevalence of MSDs using the Nordic questionnaire provided an overview of the state of the industry before assessing MMH. The high prevalence of MSDs in the lower back indicated the presence of pressure on this area due to excessive load weight and improper load handling. Assessing MMH using MAC method also identified the risk factors for MSDs. Therefore, it provided proper planning for the implementation of the training program. Eventually, this training intervention improved the workers posture during MMH and the effectiveness of which was determined by MAC evaluation after the intervention. Implementing health education is important in the sense that people can improve their health by changing their practical and work style. Moreover, the goal is for the specialist to develop the knowledge and skills for individuals to make an informed choice about their health that ultimately leads to improved health.[25]
Financial support and sponsorship
This article is a part of the research project, which was supported by Shahid Beheshti University of Medical Sciences (Grant Number 11551).
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank subjects for their generous participation and sharing to make this project possible.
References
- 1.Ashrafi E. Introduce a Health and Safety Organization in Print Industry. J Print Industry Monthly. 2014:387. [Google Scholar]
- 2.Salehi Sahl Abadi A, Mazloumi A, Nasl Saraji G, Zeraati H, Hadian MR, Jafari AH. Determining changes in electromyography indices when measuring maximum acceptable weight of lift in Iranian male students. J Biomed Phys Eng. 2018;8:73–86. [PMC free article] [PubMed] [Google Scholar]
- 3.Bernard B, Sauter S, Fine L, Petersen M, Hales T. Job task and psychosocial risk factors for work-related musculoskeletal disorders among newspaper employees. Scand J Work Environ Health. 1994;20:417–26. doi: 10.5271/sjweh.1379. [DOI] [PubMed] [Google Scholar]
- 4.Coenen P, Gouttebarge V, van der Burght AS, van Dieën JH, Frings-Dresen MH, van der Beek AJ, et al. The effect of lifting during work on low back pain: A health impact assessment based on a meta-analysis. Occup Environ Med. 2014;71:871–7. doi: 10.1136/oemed-2014-102346. [DOI] [PubMed] [Google Scholar]
- 5.Arefi MF, Pouya AB, Poursadeqiyan M. Investigating the match between anthropometric measures and the classroom furniture dimensions in Iranian students with health approach: A systematic review. J Educ Health Promot. 2021;10:38. doi: 10.4103/jehp.jehp_516_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Grimes P, Legg S. Musculoskeletal disorders (MSD) in school students as a risk factor for adult MSD: A review of the multiple factors affecting posture, comfort and health in classroom environments. J Hum Environ Syst. 2004;7:1–9. [Google Scholar]
- 7.Dianat I, Karimi MA, Asl Hashemi A, Bahrampour S. Classroom furniture and anthropometric characteristics of Iranian high school students: Proposed dimensions based on anthropometric data. Appl Ergon. 2013;44:101–8. doi: 10.1016/j.apergo.2012.05.004. [DOI] [PubMed] [Google Scholar]
- 8.Lahad A, Malter AD, Berg AO, Deyo RA. The effectiveness of four interventions for the prevention of low back pain. JAMA. 1994;272:1286–91. [PubMed] [Google Scholar]
- 9.Heidarimoghadam R, Motamedzade M, Roshanaei G, Ahmadi R. Investigating the match between male primary students’ anthropometric dimensions and existing furniture dimensions in Hamadan schools in 2013. J Ergon. 2014;2:9–18. [Google Scholar]
- 10.Shankar S, Naveen Kumar R, Mohankumar P, Jayaraman S. Prevalence of work-related musculoskeletal injuries among South Indian hand screen-printing workers. Work. 2017;58:163–72. doi: 10.3233/WOR-172612. [DOI] [PubMed] [Google Scholar]
- 11.Salehi Sahl Abadi A, Nasl Saraji G, Mazloumi A, Zeraati H, Hadian MR, Jafari AH. Changes in back compressive force when measuring maximum acceptable weight of lift in Iranian male students. Iran J Public Health. 2016;45:1199–207. [PMC free article] [PubMed] [Google Scholar]
- 12.Buckle PW, Devereux JJ. The nature of work-related neck and upper limb musculoskeletal disorders. Appl Ergon. 2002;33:207–17. doi: 10.1016/s0003-6870(02)00014-5. [DOI] [PubMed] [Google Scholar]
- 13.David GC. Ergonomic methods for assessing exposure to risk factors for work-related musculoskeletal disorders. Occup Med (Lond) 2005;55:190–9. doi: 10.1093/occmed/kqi082. [DOI] [PubMed] [Google Scholar]
- 14.Balogh I, Ørbaek P, Winkel J, Nordander C, Ohlsson K, Ektor-Andersen J, et al. Questionnaire-based mechanical exposure indices for large population studies – Reliability, internal consistency and predictive validity. Scand J Work Environ Health. 2001;27:41–8. doi: 10.5271/sjweh.585. [DOI] [PubMed] [Google Scholar]
- 15.Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233–7. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 16.Koohpaei A, Khandan M, Vosoughi S, Khammar A, Mobinizade V, Farrokhi M, Poursadeghiyan M. Industrial workers' postures analysis by a new method named" loading on the upper body assessment" in Iran. Annals of Tropical Medicine and Public Health. 2017;1(10(4)) [Google Scholar]
- 17.Beigee H, Oliayee M, Syedi MD. Manual handling assessment in a brickyard and provide control proposals. The First International Conference on Ergonomics Iran Tehran. 2008 [Google Scholar]
- 18.Helander M. A Guide to Human Factors and Ergonomics. CRC Press; 2005. [Google Scholar]
- 19.Hashemi Habibabadi R, Mohammadi M, Zare Mehrani E, Ansari Moghaddam A. Risk assessment of musculoskeletal disorders in bandar-abbas charging berth workers Using MAC method in 2011. J Rafsanjan Univ Med Sci. 2016;15:527–36. [Google Scholar]
- 20.Bulduk S, Bulduk EÖ, Süren T. Reduction of work-related musculoskeletal risk factors following ergonomics education of sewing machine operators. Int J Occup Saf Ergon. 2017;23:347–52. doi: 10.1080/10803548.2016.1262321. [DOI] [PubMed] [Google Scholar]
- 21.Marras WS, Fine LJ, Ferguson SA, Waters TR. The effectiveness of commonly used lifting assessment methods to identify industrial jobs associated with elevated risk of low-back disorders. Ergonomics. 1999;42:229–45. doi: 10.1080/001401399185919. [DOI] [PubMed] [Google Scholar]
- 22.Poosanthanasarn N, Lohachit C, Fungladda W, Sriboorapa S, Pulkate C. An ergonomics intervention program to prevent worker injuries in a metal autoparts factory. Southeast Asian J Trop Med Public Health. 2005;36:512–22. [PubMed] [Google Scholar]
- 23.Morken T, Moen B, Riise T, Hauge SH, Holien S, Langedrag A, et al. Effects of a training program to improve musculoskeletal health among industrial workers – Effects of supervisors role in the intervention. Int J Ind Ergon. 2002;30:115–27. [Google Scholar]
- 24.Hemati K, Darbandi Z, Kabir-Mokamelkhah E, Poursadeghiyan M, Ghasemi MS, et al. Ergonomic intervention to reduce musculoskeletal disorders among flour factory workers. Work. 2020;67(3):611–618. doi: 10.3233/WOR-203275. [DOI] [PubMed] [Google Scholar]
- 25.Koelen MA, Van den Ban AW. Health education and health promotion: Wageningen Academic Publishers. 2004 [Google Scholar]
- 26.Feuerstein M, Nicholas RA, Huang GD, Dimberg L, Ali D, Rogers H. Job stress management and ergonomic intervention for work-related upper extremity symptoms. Appl Ergon. 2004;35:565–74. doi: 10.1016/j.apergo.2004.05.003. [DOI] [PubMed] [Google Scholar]
- 27.Panjali Z, Zakerian S, Abedinlo R, Rezaee E. Assessment of manual material handling using Iranian MMH regulations and comparison with NIOSH equation and MAC method in one of the metal casting industries in Tehran. 2011;2013:27–34. [Google Scholar]
- 28.Dehnavi S, Vahedi A, Moghimbeigi A. The effects of ergonomic interventions in manual activities to reduce musculoskeletal disorders in manual activities by ManTRA. Iran J Ergon. 2017;4:57–67. [Google Scholar]
- 29.Wong K, Grundfast KM, Levi JR. Assessing work-related musculoskeletal symptoms among otolaryngology residents. Am J Otolaryngol. 2017;38:213–7. doi: 10.1016/j.amjoto.2017.01.013. [DOI] [PubMed] [Google Scholar]
- 30.Dormohammadi A, Motamedzade M, Zarei E, Asghari M, Musavi S. Comparative assessment of manual material handling using the two methods of NIOSH lifting equation in a tile manufacturing company MAC and revised. Iran Occup Health. 2013;10:71–81. [Google Scholar]
- 31.Choobineh A. Posture Assessment Methods in Occupational Ergonomics. Hamedan: Fanavaran Publication; 2004. pp. 80–9. [Google Scholar]
- 32.Hoe VC, Urquhart DM, Kelsall HL, Sim MR. Ergonomic design and training for preventing work-related musculoskeletal disorders of the upper limb and neck in adults. Cochrane Database Syst Rev. 2012;2012:CD008570. doi: 10.1002/14651858.CD008570.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Faisting AL, de Oliveira Sato T. Effectiveness of ergonomic training to reduce physical demands and musculoskeletal symptoms – An overview of systematic reviews. Int J Ind Ergon. 2019;74:102845. [Google Scholar]