

Abstract
Role of clinical skill training in the formation of skills and professional competencies of midwifery students is important. Hence, the use of “training new methods are essential in clinical settings.” This study aimed at determining the effectiveness of simulation training in obstetric emergencies. In this meta-analysis study, international databases of Web of Science, Scopous, Proquest, and PubMed and Iranian databases such as Irandoc, Magiran, and SID were searched for studies published between 2000 and 2020 using related keywords. Based on the consortium checklist, the full text of the selected articles was reviewed and in case of a specific score, the article was analyzed. The results show that, out of 420 studies after applying the inclusion and exclusion criteria, only nine clinical trial articles were reviewed. Studies were conducted in Iran, the United States, France, China, and Chicago. The results of meta-analysis showed that the simulation training method can be effective in managing midwifery emergencies. Hence, the use of simulation training method can be effective in various areas of learning related to obstetric emergencies.
Keywords: Educational method, midwives, obstetrics emergency, simulation, student
Introduction
One of the fields of study related to medical sciences which tends to improve health and wellness in human society is midwifery.[1] Midwifery is one of the occupations that aims to ensure the health of mothers and infants and to maintain and promote community health.[2] In general, more than 80% of direct patient care in the maternity ward and gynecology ward is performed by midwives.[3] Midwives need to acquire clinical skills and professional standards during their studies so that they will be able to serve in the midwifery profession.[4] Clinical practice is what medical students and medical staff do in dealing with the patient at the office and patient's bed.[5] If midwives are competent in diagnosing pregnancy and natural childbirth, diagnosing activities and taking appropriate measures to diagnose high-risk cases and if necessary, timely referral to a specialist, the maternal mortality rate will be significantly reduced and thus arrangements also save government spending.[6] Considerable attention has been given to the health of women and children, especially mothers, by the WHO to ensure the health of the people all around the world.[5] Iran has achieved these MDG goals in 2015 and the maternal mortality rate was 25 deaths per 100,000 livebirths. However, it is still a long way from developed countries.[7] Many studies have shown that the quality of care and clinical skills of midwives is not appropriate. Farrokhi et al. (2009) reported that the quality of midwifery care provided by midwives is only 55% good.[8] Using a variety of training methods such as role playing, accuracy, and speed techniques, electronic and virtual education and simulation are learner-based educational methods. These methods can increase individuals’ awareness and knowledge and also improve their clinical performance.[9,10,11,12] One of the new educational methods is simulation. Simulation educational environments create a suitable educational environment, without harming the patient; moreover, they can promote clinical skills and cooperation among students. In the simulation method, the problem is presented and taught to the students like a comprehensible reality, therefore, the student learns the problem and offers new solutions.[13]
Materials and Methods
Study design and setting
A meta-analysis study was conducted by researcher to identify the effectiveness of simulation training in obstetric emergencies.
Data collection tool and technique
In order to access the study on the subject under study, a search was conducted between 2000 and 2020 in reputable Persian and English databases including Magiran, SID, Google Scholar, ProQuest, Web Of Sciences, PubMed, and Scopus. To access all articles in Persian and English including simulation, midwifery emergency and high-risk pregnancy were used. It should be noted that the search for these keywords in the title and abstract of the article is limited. In addition, various experimental and quasi-experimental studies were selected. In detail, the method was as follows: first, a list of titles and summaries of the articles were prepared. The main inclusion criteria for these studies in the present review study were published articles with clear objectives, methodology, and results. Exclusion criteria also included conference papers, letters to the editor, and insufficient data on the papers. First, based on the search strategy and the keywords, a list of all the articles in the databases was prepared. The titles of the articles searched by the authors were reviewed, and duplicated articles were excluded. Then, the titles and abstracts of the reviewed articles and unrelated articles were discarded. Then, the full text of the related articles was reviewed using consort checklist. Finally, the articles that had the highest score and were relevant to the purpose of the present study were selected and reviewed. In the next step, after choosing the selected articles, the researchers evaluated the articles in accordance with the 2010 CONSORT checklist. The 25-item CONSORT checklist consists of six general sections: 1 – title and abstract, 2 – introduction, 3 – methods, 4 – results, 5 – discussion, and 6 – other information. It is recommended that the results of each group are plotted and summarized in a flow chart. Articles that received a score of 15 or more from the CONSORT checklist were considered good quality and a score <15 was considered poor quality.[14] Out of 78 articles, nine articles received 15 scores or more. Two reviewers independently extracted data from the full text of the study. After extracting the data, the extracted data were reviewed again [Table 1]. In this study, the effect size was used to interpret and analyze the results. Cochran test and I2 index were used to determine the heterogeneity of the studies, and random-effects model was used in the case of statistical heterogeneity. To investigate the effect of simulation on midwifery emergencies, the difference between the mean numbers of samples to P value was used.
Table 1.
Summary of experimental studies conducted on the effect of simulation training method on midwifery emergencies in Iran and the world
| Author/year of reference | Country | Method | Samples | Obstetrics emergencies | Results |
|---|---|---|---|---|---|
| Gonzalves et al. (2018)[15] | France | Experimental two groups (simulation with video, power point) | 50 midwifery and medical students | Dystocia | The mean score of dystocia management in the simulation group increased compared to the control group after the intervention and there was a statistically significant difference after the intervention (P<0.001) |
| Lee et al. (2017)[16] | Chine | Experimental two groups (simulation, lecture) | 64 midwives | Dystocia | There was no statistically significant difference between the mean scores of distosis management in the simulation group compared to the control group after the intervention (P<0.05) |
| Kordi et al. (2017)[1] | Iran | Experimental two groups (simulation, lecture) | 51 midwives | Dystocia | The mean performance score of midwives in the simulation group increased compared to the lecture group after the intervention and there was a statistically significant difference after the intervention (P=0.040) |
| DiGiacomo (2017)[17] | State of pennsylvania | Experimental two groups (simulation, routine) | 81 nursing students | Postpartum hemorrhage | The mean performance score of midwives in the simulation group increased compared to the lecture group after the intervention and there was a statistically significant difference after the intervention (P=0.040) |
| Tabatabaeian et al. (2018)[18] | Iran | Experimental three groups (simulation, lecture, integrated) | 90 midwives | Preeclampsia and eclampsia | The mean cognitive skill score compared to the management of preeclampsia and eclampsia of midwives in the simulation group and the lecture and integrated group increased after the intervention and there was no statistically significant difference between the three groups after the intervention (P<0.05) but the mean cognitive skill score between The two groups of combination and lecture were significantly more than the simulation group (P<0.001) |
| Fakari et al. (2015)[19] | iran | Experimental three groups (simulation, lecture, web-based) | 105 midwifery students | Postpartum hemorrhage | The mean score of clinical competence compared to postnatal bleeding management in the web-based, simulation and traditional groups before the intervention increased compared to after the intervention, but there was a statistically significant difference between the three groups after the intervention (P=0.185) |
| Reynold et al. (2010)[20] | Portugal | Experimental two groups (simulation, lecture) | 50 midwifery students | Dystocia | The mean score of knowledge in the simulation group increased compared to the lecture group after the intervention and there was a statistically significant difference after the intervention (P=0.004) |
| Andrighetti et al. (2012)[21] | USA | Experimental two groups (simulation, class discussion and video) | 28 midwifery students | Dystocia and postpartum hemorrhage | The mean score of postpartum hemorrhage management skills and dystocia in the simulation group increased compared to the speech control group after the intervention and there was a statistically significant difference (P<0.001) |
| Fisher et al. (2010)[22] | Chicago | Experimental two groups (simulation, lecture) | 26 obstetricians and midwives | Eclampsia | There was no statistically significant difference between the mean scores of eclampsia in the simulation group compared to the lecture group after the intervention (P<0.05) |
| Goffman et al. (2008)[23] | America | Experimental two groups (simulation in both groups) | 66 residents of obstetrics and gynecology and obstetrics | Dystocia | The mean score of documentation in the simulation group increased compared to the control group after the intervention and there was a statistically significant difference after the intervention (P=0.004) |
Ethical consideration
Ethical aspects of this study were approved by research deputy in Isfahan University of Medical Sciences (IR.MUI.RESEARCH.REC.1399.690).
Results
In the initial search, 420 articles were found, and after reviewing the titles and abstracts of the articles and removing duplicate and irrelevant items, 220 possible related articles were examined. From these 220 articles, 90 ones were excluded from the study due to noncompliance with the inclusion criteria, lack of access to the original article and insufficient information in the abstract, failure to report mean and standard deviation, and finally nine clinical trials were reviewed. The studies were experimental (clinical trial), and the characteristics of these studies are shown in Table 1.
The data were extracted from all studies and recorded in the computer using Excel software. After reviewing the eligible studies and extracting the desired information, the data were analyzed using R statistical software. Random- and fixed-effect statistical models were applied to analyze and integrate the results. The fixed-effects model assumes that all studies considered in the share treatment so that the met effects can be considered as a part of the same distribution. In the model with the default random effect, the effect of the treatment is not the same in different studies; therefore, the effect of the treatment varies from one study to the next and the main purpose of the meta-analysis is to estimate the mean. Finally, the evaluation of nine articles included in the meta-analysis was examined, which showed high heterogeneity with I2 = 89%, df = 8, and Tau2 = 0.794. By observing the high heterogeneity, finally, all nine articles were included in the meta-analysis. The results of the meta-analysis showed that there was no statistically significant difference between the intervention and control groups (P = 0.182) [Figures 1 and 2].
Figure 1.

Estimated effect of means and 95% confidence interval for the studied studies. Simulation training method on performance improvement related to midwifery emergencies
Figure 2.
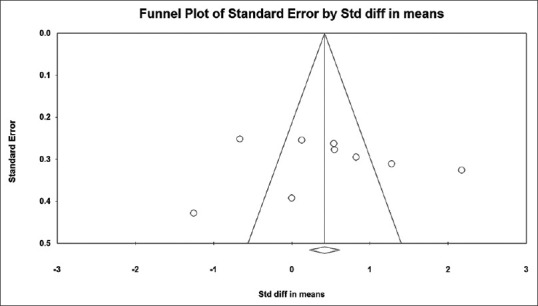
Funnel diagram of standard error based on analyzed studies
Discussion
The results of the study showed that simulation training method can be effective on the performance of students, midwives, and residents of gynecology and midwifery. In the review of articles and according to Table 1, only the articles that have been included in the meta-analysis on the management of hard labor (dystocia), postpartum hemorrhage, eclampsia, and preeclampsia; in addition, the effect of simulation training method on these midwifery emergencies was analyzed. In all the reviewed articles, only the articles that had mean and standard deviation before and after the intervention were analyzed. The results of Gonzalves et al. in France showed the mean and standard deviation of performance score of midwifery and medical students before the intervention in the simulation group were 7 (1.7) and in the control group (PowerPoint) were 7.2 (1.6), respectively, whereas the mean and standard deviation of performance score after the intervention in the simulation group were 9.3 (1.4) and in the control group (PowerPoint) were 7 (2.61), respectively.[15] The results of this study suggest that the use of simulation can be a useful method for managing difficult labor. In this study, the use of PowerPoint reduced the interaction of students in managing difficult labor and like other conventional methods of lecturing, it has become a passive method. Therefore, it is expected that this method will be much less effective in comparison with the simulation method. In addition, the results of the study by Andrighetti et al. (2012) also showed that the mean and standard deviation of the skill score of midwifery students before the intervention in the simulation group were 29.4 (2.8) and in the control group (lecture) were 29.8, respectively (5.4). However, the mean and standard deviation of performance score after the intervention in the simulation group were 35.3 (2) and in the control group (lecture) were 30.6 (4.4), respectively. However, both training methods (i.e., simulation and lecture) can improve the students’ skills.[21] The management of eclampsia and preeclampsia has also included in this review using the simulation training method. The results of Fisher et al.'s study showed that the mean score of eclampsia before the intervention in the simulation group was 15 (3.5) and in the lecture group was 16 (1.5). Moreover, the mean score after the intervention was 19 (3) in the simulation group and 19 (2) in the lecture group. Although the scores of eclampsia management skills increased significantly in both groups and the mean scores in both educational groups changed significantly, no statistically significant relationship was found between the two groups after the intervention.[22,23]
Limitation and recommendation
This suggests that both simulation and lecture methods can be effective on managing eclampsia as an obstetric emergency. However, the meta-analysis has shown that the simulation method is effective in the four emergencies studied including the management of difficult labor, eclampsia and preeclampsia, and postpartum hemorrhage.
Conclusion
The use of simulation training method can be effective in various areas of learning related to midwifery emergencies. Furthermore, the results of the study showed that simulation training method can be effective on the performance of students, midwives, and residents of gynecology and midwifery.
Financial support and sponsorship
This research was supported (Ethic code: IR.MUI.RESEARCH.REC.1399.690) from Isfahan University of Medical Science, Isfahan, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We greatly appreciate the support and collaboration of Isfahan University of Medical Sciences.
References
- 1.Kordi M, Erfanian F, Fakari FR, Dastfan F, Nejad KS. The comparison the effect of training by means of simulation and oral method on midwives’ skill in management of shoulder dystocia. J Educ Health Promot. 2017;6:50. doi: 10.4103/jehp.jehp_115_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tafazoli M, Hosseini S, Sharbaf HA, Makarem A, Zadeh SE. A study of relationship between emotional intelligence and clinical performance in training field in midwifery students of Nursing and Midwifery School. Future Med Educ J. 2012;2:13–8. [Google Scholar]
- 3.Talasaz ZH, Saadoldin SN, Shakeri MT. The relationship between job satisfaction and job performance among midwives working in healthcare centers of Mashhad, Iran. J Midwifery Reprod Health. 2014;2:157–64. [Google Scholar]
- 4.Dadgari A, Kasaeian A, Atash SG, Naseri FL, Dadvar L, Kalateh JM. Efficacy of Midwifery Clinical Curriculum in Achieving Core Learning Goals: Tutors and students' point of view. 2009;4(3):28–33. [Google Scholar]
- 5.Kevin JW, Kendall SF. The student nurses view of the future of nursing. Australian Electronic Journal of Nursing Education (AEJNE) 2000 Jun;6(1):47–55. [Google Scholar]
- 6.Mirzakhani K, Jahani Shorab N, Golmakani N, Tafazoli M, Ebrahimzadeh S. Evaluation of clinical skills in midwives graduated from Mashhad nursing and midwifery faculty and employed in Mashhad health care centers. Nurs Midwifery J. 2012;9(6):1–9. [Google Scholar]
- 7.Tafazoli M, Ezzati R, Mazlom SR, Asgharipour N. The effect of empathy skills training on the Empathetic behaviours of Midwifery students. J Midwifery Reprod Health. 2018;6:1236–43. [Google Scholar]
- 8.Farrokhi F, Khdyvzadh T. Quality of midwives practice in Midwifery care during pregnancy in the health centers affiliated to Mashhad University of Medical Sciences. Payesh Health Monit. 2009;7(3) [Google Scholar]
- 9.Ghafari S, Yazdannik A, Mohamadirizi S. Education promotion based on “mobile technology” in the critical care nursing department: Four-phase intervention. J Educ Health Promot. 2020;9:325. doi: 10.4103/jehp.jehp_34_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mohamadirizi S, Bahadoran P, Mohamadirizi S. An active teaching approach for fetal and maternal assessment in delivery room: A randomized clinical trial. Iran J Neonatol. 2017;8:23–6. [Google Scholar]
- 11.Nasr-Esfahani M, Yazdannik A, Mohamadiriz S. Development of nursing students’ performance in advanced cardiopulmonary resuscitation through role-playing learning model. J Educ Health Promot. 2019;8:151. doi: 10.4103/jehp.jehp_125_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mohamadirizi S, Noroozi M, Mohamadirizi S. The effect of speed and precaution technique on postpartum bleeding among midwifery students in the clinical field. J Educ Health Promot. 2019;8:72. doi: 10.4103/jehp.jehp_328_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Beilondi RR, Rahmani M. The effect of simulation training on midwifery students’ clinical competence in vaginal breech delivery. Educ Strategy Med Sci. 2016;9:351–6. [Google Scholar]
- 14.Schulz KF, Altman DG, Moher D Consort Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Trials. 2010;11:32. [Google Scholar]
- 15.Gonzalves A, Verhaeghe C, Bouet PE, Gillard P, Descamps P, Legendre G. Effect of the use of a video tutorial in addition to simulation in learning the maneuvers for shoulder dystocia. J Gynecol Obstet Hum Reprod. 2018;47:151–5. doi: 10.1016/j.jogoh.2018.01.004. [DOI] [PubMed] [Google Scholar]
- 16.Lee MM, Chan CN, Lau BY, Ma TW. Randomised controlled study to assess skill retention at 6 vs.12 months after simulation training in shoulder dystocia. BMJ Simul Technol Enhanc Learn. 2017;3:142–8. doi: 10.1136/bmjstel-2017-000195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.DiGiacomo P. Evaluating the Use of a Postpartum Hemorrhage Simulation as a Teaching Strategy in an Undergraduate Nursing Program. [PhD thesis in USA]: Temple University. 2017. available at: https://www.proquest.com/openview/99b5ffa59170e90b8907f85590d3fb48/1?cbl=18750&parentSessionId=oIjrDfj5UwoEWD20yBIL06M00eNq%2FRQh54cZ5l%2BnExA%3D&pqorigsite=gscholar&accountid=41305 .
- 18.Tabatabaeian M, Kordi M, Dadgar S, Esmaeily H, Khadivzadeh T. Comparing the effects of simulation-based training, blended, and lecture on the simulated performance of midwives in preeclampsia and eclampsia. J Educ Health Promot. 2018;7:110. doi: 10.4103/jehp.jehp_116_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fakari FR, Kordi M, Mazloom SR, Khadivzadeh T, Tara M, Akhlaghi F. Comparing the effect of traditional, web based and simulation training on midwifery students’ clinical competence in postpartum hemorrhage management. J Mazandaran Univ Med Sci. 2015;25:65–77. [Google Scholar]
- 20.Reynolds A, Ayres-de-Campos D, Pereira-Cavaleiro A, Ferreira-Bastos L. Simulation for teaching normal delivery and shoulder dystocia to midwives in training. Educ Health (Abingdon) 2010;23:405. [PubMed] [Google Scholar]
- 21.Andrighetti TP, Knestrick JM, Marowitz A, Martin C, Engstrom JL. Shoulder dystocia and postpartum hemorrhage simulations: Student confidence in managing these complications. J Midwifery Womens Health. 2012;57:55–60. doi: 10.1111/j.1542-2011.2011.00085.x. [DOI] [PubMed] [Google Scholar]
- 22.Fisher N, Bernstein PS, Satin A, Pardanani S, Heo H, Merkatz IR, et al. Resident training for eclampsia and magnesium toxicity management: Simulation or traditional lecture? Am J Obstet Gynecol. 2010;203:5.e1–5. doi: 10.1016/j.ajog.2010.06.010. [DOI] [PubMed] [Google Scholar]
- 23.Goffman D, Heo H, Chazotte C, Merkatz IR, Bernstein PS. Using simulation training to improve shoulder dystocia documentation. Obstet Gynecol. 2008;112:1284–7. doi: 10.1097/AOG.0b013e31818c177b. [DOI] [PubMed] [Google Scholar]