

On June 10, 2021, the UK and USA released a joint statement about the visit of US President Joe Biden to the G20 Summit at the invitation of UK Prime Minister Boris Johnson. Within this statement (point 18) is the following: “We will convene the first US–UK Bilateral Cancer Summit and bring together researchers, patients, and other stakeholders to share ideas and identify opportunities for collaboration to accelerate advances in lifesaving approaches to cancer, which remains a leading cause of death worldwide.”1 On Nov 10, 2021, the UK Research and Innovation announced that this Summit would take place on Nov 13–14, 2021, “…to identify transformative research grand challenges and ways to resolve barriers to progress in cancer research.”2 Information arising from this meeting is scarce, but we know that several different domains from prevention and early detection to exploring social, economic, and environmental factors that contribute to health inequalities were on the agenda.
The UK and USA have nearly a two-decade history of formal cooperation originally built on the Good Friday Agreement on cancer research from 1999.3 Since 1980, the UK and USA have seen substantial growth in their respective cancer research outputs as assessed by publication volume (figure 1A). In the past decade (2011–20), the UK’s cancer research output (peer-reviewed publications) of 63 722 papers represented 9·4% of the total UK biomedical research output, and 5·7% of the world’s total. Cancer research coauthored by researchers in the USA and UK has been increasing at a much faster rate than that of the individual countries, with an annual average percentage growth of 9·3% compared with the UK at 4·3% and the USA at 4·1%. The UK has been responsible for most of this collaborative increase, with nearly 26% of its total output in 2020 coauthored with collaborators in the USA compared with only 6% of US cancer research output coauthored with collaborators in the UK (figure 1B). This rate has increased substantially for the UK, particularly since 1990, but only slowly for the USA, reflecting a general pattern of increasing international collaboration by European countries.4
Figure 1: Trends in individual and collaborative outputs from the USA and UK.
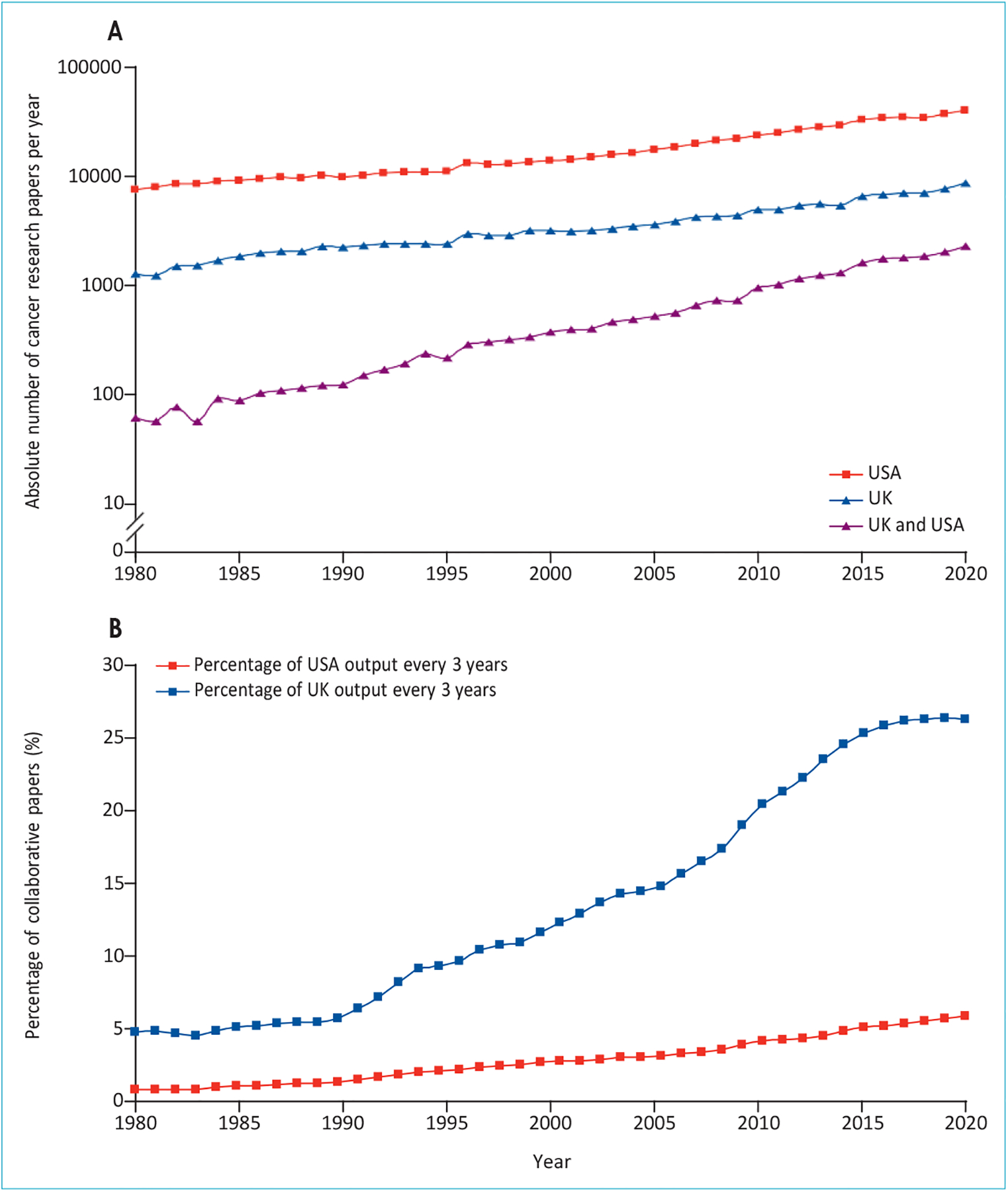
(A) Absolute numbers of cancer research papers from the UK, USA, and UK–USA coauthored publications from 1980 to 2020. (B) UK–USA collaborative papers in cancer research as a percentage of each country’s output from 1980 to 2020.
The UK and USA have major differences in their historical patterns for collaborative research with other countries (appendix pp 1–2). Overall, the USA collaborates less than the UK internationally. Between 2011 and 2020, only 36% of all USA cancer research papers were internationally coauthored, compared with 55% of total UK outputs. Although the USA is the largest collaborator with the UK by total volume of papers, there have been eight other countries with which the UK has major research collaborations (each with more than 10% of its total research output) in the past decade, including six countries in Europe (the Netherlands, Sweden, Spain, France, Italy, and Germany), Canada, and Australia. For the USA, the top collaborating countries were China (25·7%), followed by the UK (13·5%), Canada (13·3%), Germany (12·8%) and Italy (11·8%). The USA collaborates far less with Europe (excluding the UK), and relatively little with lower-middle-income countries.
UK and USA collaborative cancer research is focused on haematology–oncology and breast cancer (figure 2). The USA is relatively stronger in research on brain and pancreatic cancers, whereas the UK is stronger in colorectal and oesophageal cancer research (figure 3). A similar comparative analysis of research domains (figure 4) reveals that the UK and USA are remarkably aligned with their focus on fundamental and discovery cancer research, pharmaceutical (eg, biomarker and systemic therapies research), and epidemiological research (figure 5). However, there is little bilateral collaboration in domains such as palliative care, surgery, radiotherapy, health services research, and screening.
Figure 2:
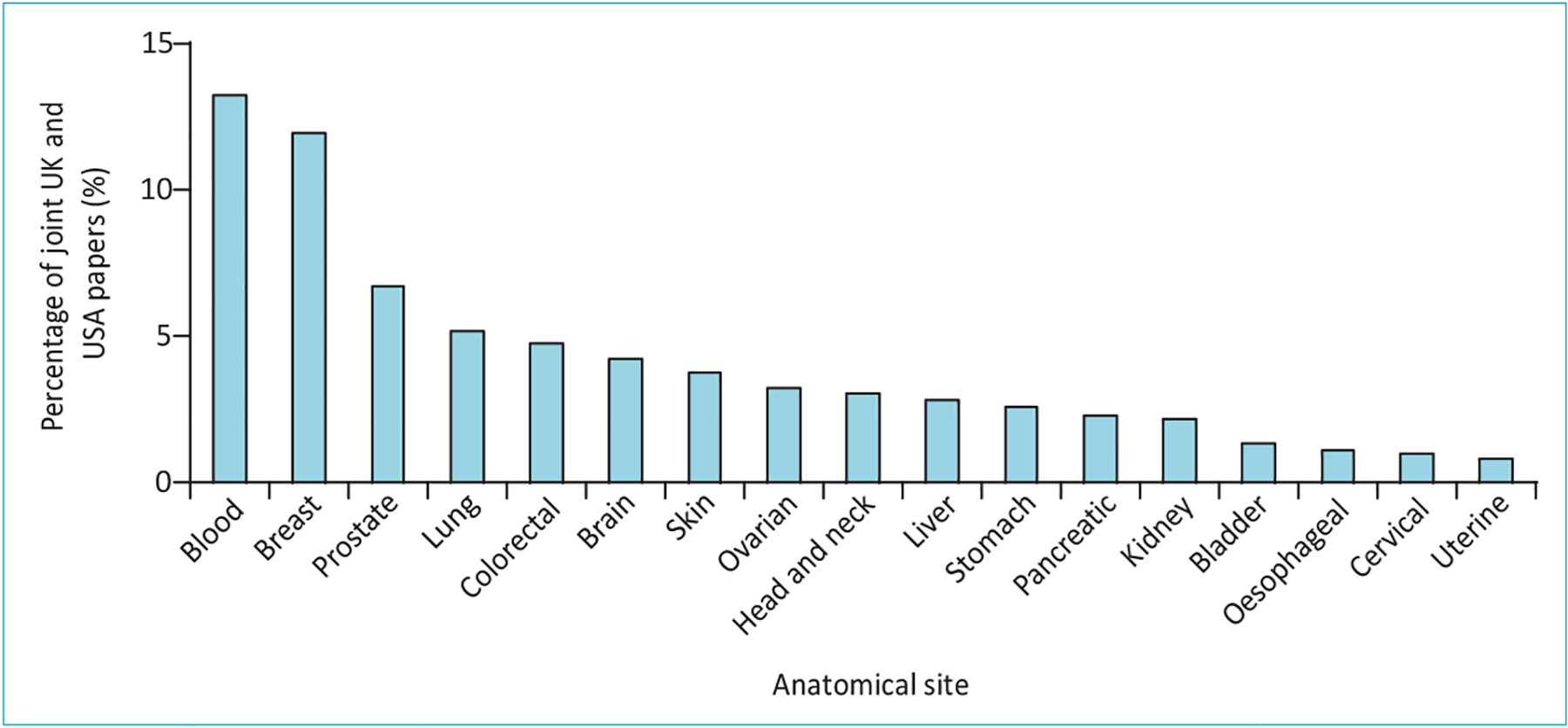
Percentage presence of site-specific cancers in joint UK–USA cancer research papers from 2011 to 2020
Figure 3: Percentage of USA cancer research on 17 anatomical sites plotted against the percentage of UK cancer research outputs for the same sites (2011–20).
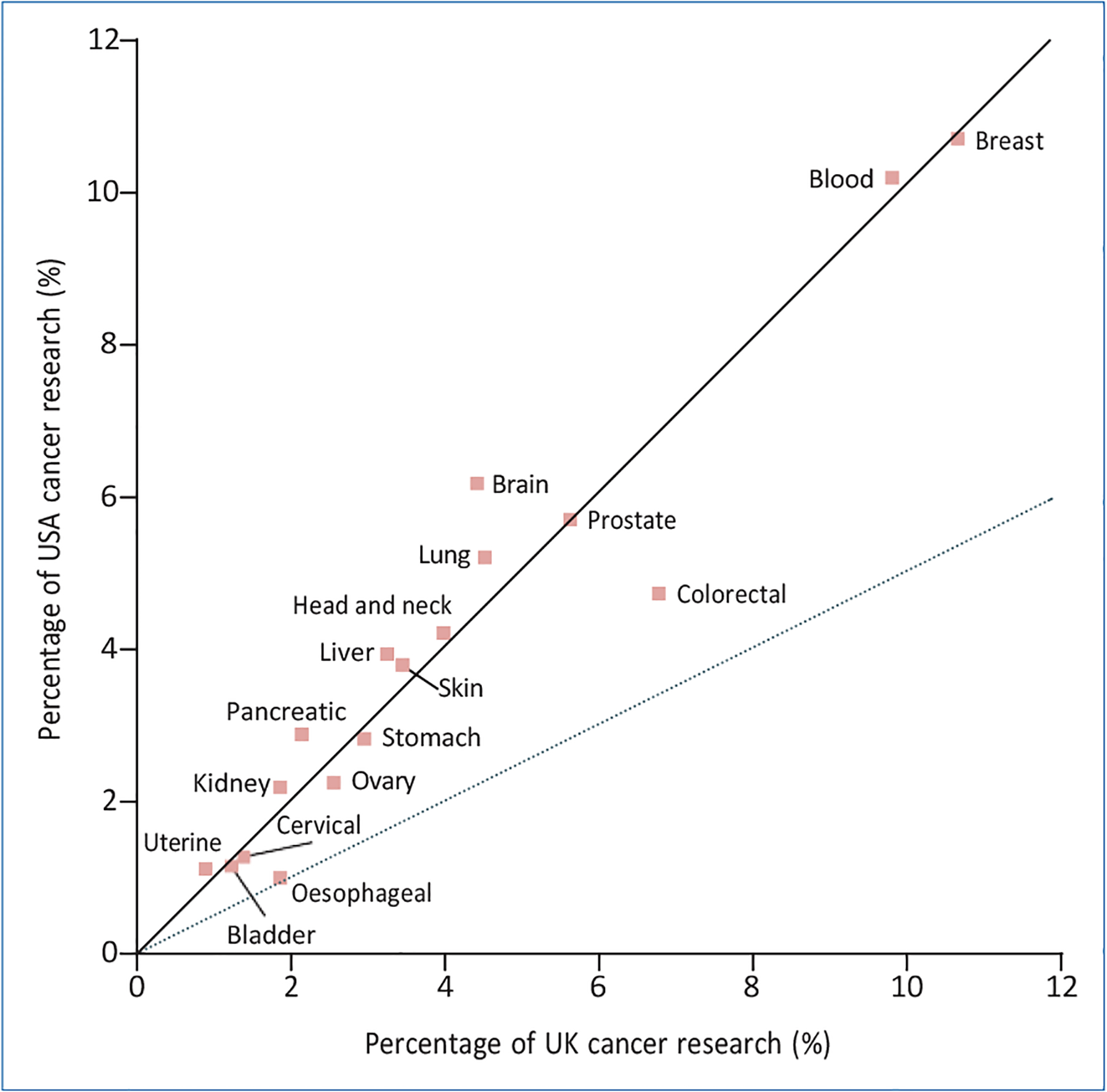
Dashed line represents UK percentage cancer research outputs twice that of the USA.
Figure 4:
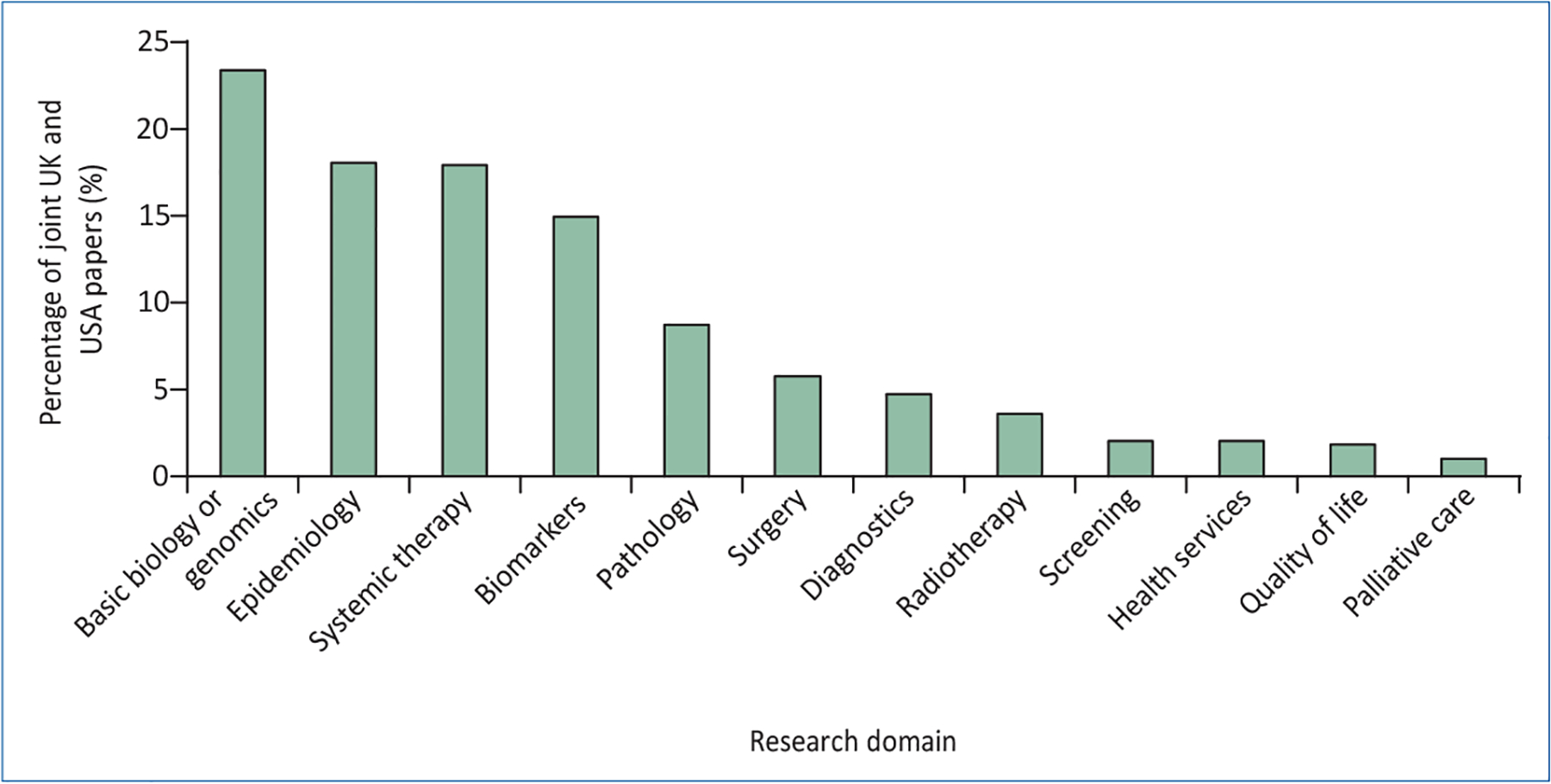
Percentage presence of research domains in joint UK–USA cancer research papers from 2011 to 2020
Figure 5: Percentage of USA cancer research in 12 domains plotted against the percentage of UK cancer research (2011–20).
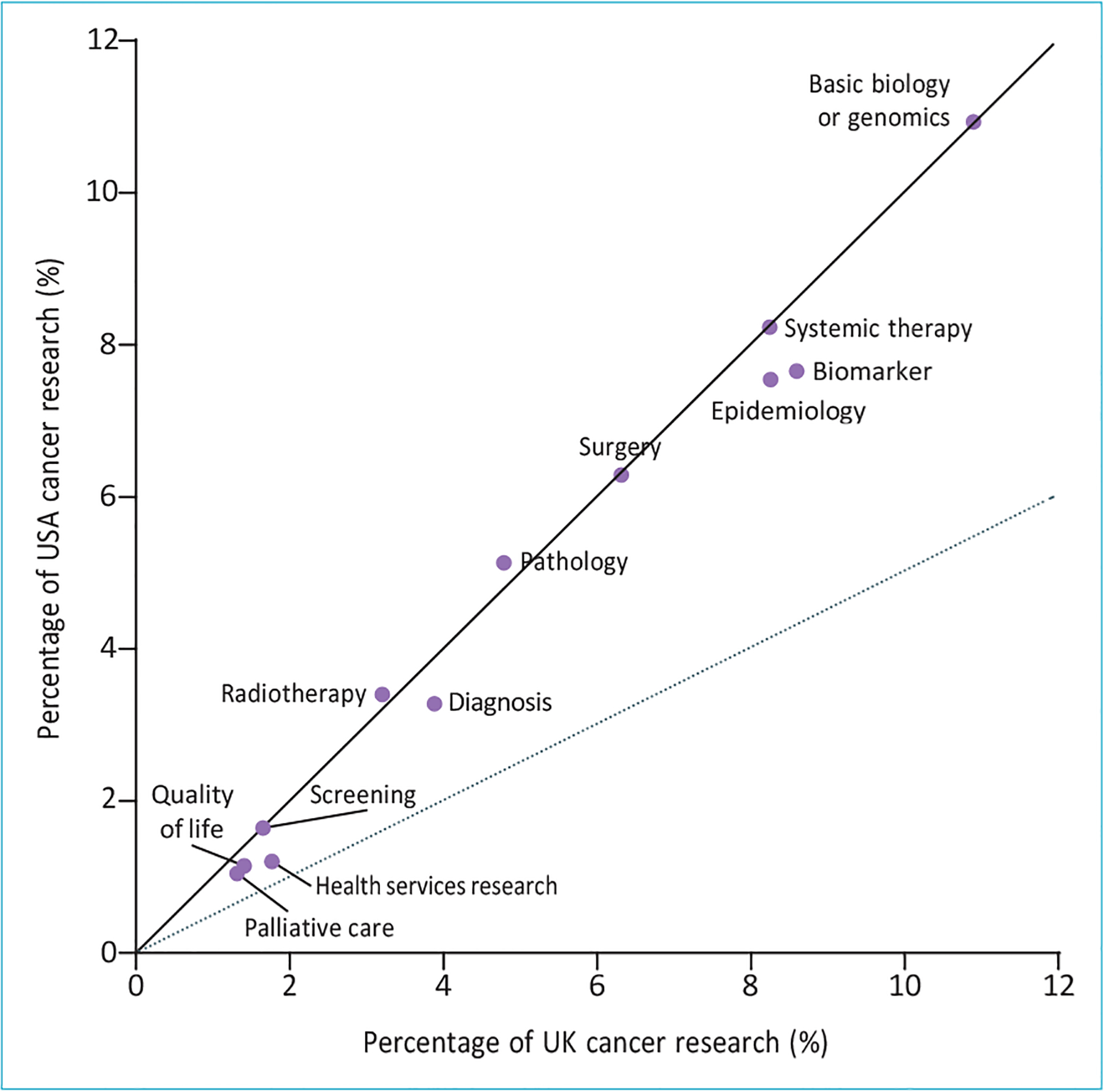
Dashed line represents UK percentage cancer research outputs twice that of the USA.
The research funding organisation landscape across the UK and USA shows notable differences. In the UK, 33% of cancer research publications acknowledge funding from four government agencies compared with 88% in the USA (particularly the US National Cancer Institute and National Institutes of Health; appendix pp 3–5). Charities and foundations account for 33% of cancer research funding in the UK, but only 8% in the USA. UK cancer researchers also acknowledge more than 8% of their funding from EU sources. For UK and USA collaborative papers only, the National Cancer Institute and other National Institutes of Health organisations dominated, along with the American Cancer Society, whereas the UK funding for such collaborations was split between Cancer Research UK, the National Institute of Health Research (the funding group of the UK Government’s Department of Health and Social Care), the Medical Research Council (UK Research and Innovation for the UK Government), and the independent charity Wellcome Trust, along with substantial acknowledgment of EU funding (appendix p 6). Our data show that there is already substantial collaboration in cancer research between the USA and UK, but most of this collaborative research focuses narrowly on the pharmaceutical and precision medicine agenda. Delivery of high-quality and affordable cancer care requires a balanced research portfolio across the cancer care continuum, which neither the USA nor the UK currently have.5 Improving cancer collaboration between the USA and the UK should not focus on expanding the existing domains, but rather broadening the focus on cancer research of both countries, in site-specific domains, research areas, and geographical regions. Although much has been said about the need to build cancer care capacity in low-income and middle-income countries, there has been little concerted effort to integrate or lead global cancer by either the UK or USA.6 Our analysis reveals a gap in the respective countries’ research agendas in important areas, such as value and affordability, and cancer systems research that are crucial to global leadership. This speaks to the importance of a much broader research agenda in cancer domains, such as palliative care, quality of life, survivorship, and reintegration into society, but also taking a much wider disciplinary vision to embrace the rich methodological diversity of the social and economic sciences.7
The COVID-19 pandemic has had, and will continue to have, substantial and negative effects on cancer research.8 In the global fight against cancer, the USA and UK have a responsibility to assist cancer research systems strengthening, and progress towards the key global targets, especially within the non-communicable disease global action plan. Joint UK and USA leadership in global cancer would also attract other investors to meeting 2030 commitments for cancer prevention and control, and would be an opportunity to develop global cancer control through research capacity and capability (panel).
Panel: Key cancer research trends in the USA and UK.
There has been growing collaboration in cancer research between the USA and UK over the past 40 years, driven mainly by the UK; however, both countries have substantial collaborations with other high-income countries
Neither the UK nor the USA have notable cancer research collaborations with low-income or middle-income countries, apart from the USA with China
Haematology–oncology and breast cancer are the major site-specific areas for collaborative research between the USA and UK
The UK and USA collaborative and individual cancer research ecosystems are narrowly focused on basic discovery science and biopharmaceutical research; many important domains (eg, palliative care and surgery) are relatively neglected
A wide range of government and philanthropic cancer research funders exist in the UK and USA; although the UK has substantial philanthropic funding, the USA is dominated by government funding, particularly from the US National Cancer Institute and National Institutes of Health
Finally, in seeking to build international leadership through better collaboration between the UK and USA, not reinventing the wheel is crucial. A substantial amount of work already exists in the public domain analysing the research landscape from the Lancet Oncology Commissions on delivering affordable cancer care in high-income countries5 and future cancer research priorities in the USA9 to critical examinations of global cancer research by the USA’s American Society of Clinical Oncology10 and the UK’s Global Cancer Research Network.11 Pursuing a broader cooperative cancer research agenda that is aligned to the challenges that specific countries and regions face, especially in low-income and middle-income countries and globally deprived populations, provides an unrivalled opportunity for the UK and USA to show real global leadership.
Supplementary Material
Footnotes
ML has received honoraria from Pfizer, EMG Serono, Roche, Novartis, and Bayer for presentations unrelated to this work. JG has participated on data safety monitoring boards or advisory boards for Roche– Genentech, AstraZeneca, Radius, and Immunomedics (with no payment received) and is the Chief Medical Officer for the American Society of Clinical Oncology. All other authors declare no competing interests
See Online for appendix
References
- 1.The White House. Joint statement on the visit to the United Kingdom of the Honorable Biden Joseph R. Jr., President of the United States of America at the invitation of the Rt. Hon. Boris Johnson, M.P., the Prime Minister of the United Kingdom of Great Britain and Northern Ireland. June 10, 2021. https://www.whitehouse.gov/briefing-room/statements-releases/2021/06/10/joint-statement-on-the-visit-to-the-united-kingdom-of-the-honorable-joseph-r-biden-jr-president-of-the-united-states-of-america-at-the-invitation-of-the-rt-hon-boris-johnson-m-p-the-prime-min/ (accessed Feb 10, 2022).
- 2.UK Research and Innovation. https://www.ukri.org/news/uk-usa-scientific-summit-to-bolster-cancer-research-collaboration/.
- 3.Lewison G, Gavin A, McCallion K, McDermott R, Sullivan R, Lawler M. The ‘Good Friday Agreement’ and cancer research on the island of Ireland: evidence for the impact of a tripartite cancer research partnership. Eur J Cancer 2020; 129: 15–22. [DOI] [PubMed] [Google Scholar]
- 4.Begum M, Lewison G, Lawler M, Sullivan R. Mapping the European cancer research landscape: an evidence base for national and Pan-European research and funding. Eur J Cancer 2018; 100: 75–84. [DOI] [PubMed] [Google Scholar]
- 5.Sullivan R, Peppercorn J, Sikora K, et al. Delivering affordable cancer care in high-income countries. Lancet Oncol 2011; 12: 933–80. [DOI] [PubMed] [Google Scholar]
- 6.Mukherji D, Murillo RH, Van Hemelrijck M, et al. Global cancer research in the post-pandemic world. Lancet Oncol 2021; 22: 1652–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rodin G, Ntizimira C, Sullivan R. Biomedicine and the soul of medicine: optimising the balance. Lancet Oncol 2021; 22: 907–09. [DOI] [PubMed] [Google Scholar]
- 8.Van Hemelrijck M, Lewison G, Fox L, et al. Global cancer research in the era of COVID-19: a bibliometric analysis. Ecancermedicalscience 2021; 15: 1264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jaffee EM, Dang CV, Agus DB, et al. Future cancer research priorities in the USA: a Lancet Oncology Commission. Lancet Oncol 2017; 18: e653–706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gralow JR, Asirwa FC, Bhatt AS, et al. Recommendations from the ASCO Academic Global Oncology Task Force. JCO Glob Oncol 2020; 6: 1666–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stanway S, Lodge M, Sullivan R, et al. The UK’s contribution to cancer control in low-income and middle-income countries. Lancet Oncol 2021; 22: e410–18. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.