

Abstract
The failure of hip prostheses is a problem that requires further investigation and analysis. Although total hip replacement is an extremely successful operation, the number of revision surgeries needed after this procedure is expected to continue to increase due to issues with both bone cement types and cementation techniques (depending on the producer). To conduct a comparative analysis, as a surgeon prepared the bone cement and introduced it in the body, this study’s team of researchers prepared three types of commercial bone cements with the samples mixed and placed them in specimens, following the timeline of the surgery. In order to evaluate the factors that influenced the chemical composition and structure of each bone cement sample under specific intraoperative conditions, analyses of the handling properties, mechanical properties, structure, and composition were carried out. The results show that poor handling can impede prosthesis–cement interface efficacy over time. Therefore, it is recommended that manual mixing be avoided as much as possible, as the manual preparation of the cement can sometimes lead to structural unevenness.
Keywords: bone cements, biomaterials, mechanical properties, orthopedic, handling
1. Introduction
Biomaterials are now used successfully not just in dentistry [1,2] and orthopedic surgery [3,4,5] but also in many medical specializations such as neurosurgery [6], ophthalmology [7], gynecology [8,9], cardiovascular surgery [10,11], general surgery [12,13,14,15] and maxillofacial surgery [16].
Bone cements are defined as mixtures of substances consisting of a powder phase and a liquid phase that, after mixing and homogenization, form a paste that can harden and self-stabilize once implanted in the body [17,18,19,20]. These materials have the ability to be modeled to ensure the fixation of the implant and act as an interface between bones and the implant material. Bone cements are widely used as materials for endoprosthesis replacement, vertebroplasty and cranioplasty. The two main types are calcium phosphate cements (CPCs) and polymethylmethacrylate bone cements (PMMAs) [21]. The selection of bone cements is carried out according to clinical needs.
For a cement to properly perform the clinical function for which it was created, it must simultaneously possess several characteristics: the ability to properly transmit static and dynamic loads, biocompatibility, properties similar to those of bone (e.g., elasticity), high fatigue resistance, crack resistance, resistance to abrasive processes, wear resistance, high coefficient of friction, relatively short link creation time, adequate polymerization temperature, high vibration damping factor, ease of handling, in vivo hardening in perfect time, nontoxicity, close to neutral pH during attachment, a contraction as small as possible during stabilization, good radiopacity and porosity. Although the requirements are known, the perfect cement has not been found so far; each of the materials used to date has its limitations. In current surgical interventions, the most frequently used cements can be classified as acrylic bone cements and calcium phosphate bone cements [22,23,24].
The mechanical resistance of the total hip prosthesis and particularly the adhesion quality between the implant and the bone primarily depend on the nature of the cement used and its mechanical and geometrical characteristics [25]. Acrylic bone cements are part of a group of materials that are created directly in their environment. They are obtained from PMMA, a simple liquid polymer/monomer system that hardens in the cold. The combination of the two components results in a viscous mass with a stabilization time of 7–10 min, until mechanical stability is reached. It is currently the most widely used biomaterial for fixing prostheses in arthroplasty and has a high performance due to its very good properties [26,27,28,29,30,31]. The properties and applications of acrylic bone cement are different, as shown in Figure 1 [32].
Figure 1.

Schematic data of the acrylic bone cements.
The general disadvantages of acrylic bone cement are the lack of osteoconductivity; aseptic weakening over time [33]; exothermic reaction during polymerization with possible local necrosis; reduced mechanical properties; lack of bioactivity [34]; hypersensitivity to the cement components [35]; possible cardiovascular reactions to acrylic bone cement [36]; possible leaching of the unreacted monomer into the surrounding tissues, leading to chemical necrosis [36]; and osteolysis due to the wear and tear of particles and debris from the bone cement.
Calcium phosphate cements (CPCs) are more similar to bone due to the presence of calcium phosphate [37,38].
Various papers describe the impact of cementation techniques on the clinical results of total hip or knee prosthesis, revealing that the cement mantle thickness influences the potential prosthesis migration and inflammatory reactions due to various wear particles [39,40,41,42]. Additionally, some failure analysis studies highlight the importance of intraoperative activities such as bone cement preparation [43,44,45,46].
The main function of bone cement is to adhere the prosthesis to the bone, resulting in the transference of body weight and mechanical loads from the prosthesis to the bone and the immediate immobilization of the prosthesis. This ensures the adequate fixation of the femoral component for from 10 to 15 years, but after this time failure is almost inevitable, even using the latest intraoperative methods for performing surgery and obtaining and handling cement. There are many reasons for endoprosthesis failure, such as the body’s excessive inflammatory response to infection, poor handling, soft tissue failure [47], aseptic loosening [48,49,50], improper mixing, failure to handle properly, poor stabilization, exothermic reaction [51] and the mechanical failure of the cement layer.
Since cementing is affected by various factors including lavage, hemostasis, bone density, the type of cement, mixing time, cement viscosity, timing, ambient temperature, cementing technique, component design and the surgeon’s experience, it is important to utilize reproducible cementing techniques [52,53]. There are different methods for handling the cement used to fix the femoral component, other methods for fixing the acetabular component and a completely different method for handling the cement used for BHR-type prostheses. As specified in the instructions for the use of the BIRMINGHAM HIP Resurfacing prosthesis (Surgical Technique), the low-viscosity cement is mixed and poured into the head implant. Alternatively, it can be drawn up into a bladder syringe and injected into the femoral component [54].
Although the stabilizing properties are primarily associated with the composition of the cement, it has been found that many other parameters affect the properties of bone cements, an important factor being the ambient temperature during handling. Higher temperatures decrease both the working time and the stabilization time, which can influence the handling of the cement [55]. The curing process is divided into four stages: (a) mixing, (b) waiting, (c) working and (d) hardening. The mixing can be carried out by hand or with the aid of centrifugation or vacuum technologies [18].
Previous results obtained by our group regarding the failure analysis of a hip-cemented prosthesis reveal that the improper preparation of the acrylic bone cements is one reason for prosthesis failure [56,57,58]. Figure 2 shows a hip resurfacing failure in which the defects due to the poor handling of the bone cement are highlighted.
Figure 2.

Schematic presentation of implant–cement and cement–bone interfaces.
Following these studies, the aim of this paper is to perform a comparative analysis of three different acrylic bone cements used in clinical practice for the same hip prosthesis fixation, Aminofix 1, Aminofix 3 and Simplex P, evaluating their surface and mechanical properties. Table 1 presents the stabilization parameters of some commercial acrylic bone cements.
Table 1.
| Bone Cement | Working Time (min) | Setting Time (min) | Peak Temperature (°C) |
|---|---|---|---|
| Fix 1 (Groupe Lepine) | 3 | 7 | 57 |
| Fix 2 (Groupe Lepine) | 4 | 9 | 57 |
| Aminofix 1 (Groupe Lepine) | 4 | 8 | 57 |
| Aminofix 3 (Groupe Lepine) | 5 | 10 | 58 |
| Simplex P(Stryker) | 7 | 14.3 | 90 |
| Palacos® + G(Heraeus) | 5 | 12.5 | 73 |
| CMW1(DePuy CMW) | 6.5 | 11 | 88 |
| Osteopal V (Heraeus) | 8 | 14 | 56 |
| KyphX HV-R | 8 | 20 | 56 |
2. Materials and Methods
2.1. Materials
Bone Cements Used
Bone cement samples were obtained directly in the operating room during surgery by mixing the liquid monomer with the powdered polymer. Cement was converted from a liquid to a solid state by an exothermic reaction.
Table 2 presents the chemical compositions of the commercial products used in this research: Aminofix 1 (Groupe Lépine, Genay, France) encoded as sample 1, Aminofix 3 (Groupe Lépine, France) encoded as sample 2 and Simplex P (Stryker, Kalamazoo, MI, USA) encoded as sample 3.
Table 2.
Chemical composition of the experimental samples of acrylic bone cements.
| Sample 1 | Sample 2 | Sample 3 | ||
|---|---|---|---|---|
| Liquid component | 14.4 g | 16.4 g | 18.79 g | |
| Methyl methacrylate | Monomer | 12.28 | 13.99 | 18.33 |
| Butyl methacrylate | Monomer | 1.90 | 2.16 | - |
| N, N-dimethyl-p-toluidine | Activator | 0.22 | 0.25 | 0.46 |
| Hydroquinone * | Inhibitor | 20 ppm | 20 ppm | 60 ppm |
| Powder component | 40 g | 40 g | 41 g | |
| Polymethyl methacrylate | Pre-polymerized polymer | 33.68 | 33.52 | 6.00 |
| Benzoyl peroxide | Initiator | 0.96 | 1.12 | 0.50 |
| Methyl methacrylate—styrene copolymer | Pre-polymerized copolymer | - | - | 30.00 |
| Barium sulphate | Radiopaque agent | 3.84 | 3.84 | 4 |
| Gentamicin sulfate | Antibiotic | 1.52 | 1.52 | - |
| Erythromycin | Antibiotic | - | - | 0.50 |
| Colistin Sulphomethate Sodium EP | Antibiotic | - | - | 3.00 million I.U. |
| Viscosity | standard | low | low |
* Hydroquinone was added in relation to the liquid component.
The investigated bone cements are used for different procedures in orthopedic surgery. The difference between preparing the cement in the laboratory and preparing it in the operatory is that some surgical procedures take longer than others, so the cement cannot settle too quickly or too slowly. Therefore, some manufacturers produce several different types of bone cement, each designed for particular circumstances.
Bone cement performance is directly linked to various parameters such as the mixing method, chemicals used, viscosity, porosity, antibiotics used in the cement composition, sterilization, working temperature, physical and mechanical properties and biocompatibility [61,62]. Additionally, different procedures for intraoperative handling of the bone cements are used in clinical practice. For classical hip arthroplasty, the bone cements are pressured inside the prepared bone and prosthesis components are inserted after into the cement (Figure 3), but in some specific cases such as hip resurfacing prostheses (e.g., Birmingham Hip Resurfacing Prosthesis), the bone cements are pressured inside the femoral head before the insertion of the prosthesis component into the prepared bone (Figure 4).
Figure 3.

Aspects regarding the handling of bone cements for classical hip prosthesis fixation: (a) Bone cement application. (b) Postoperative radiography. (c) Failed hip prosthesis.
Figure 4.

Aspects regarding the handling of bone cements for resurfacing hip prosthesis (e.g., BHR) fixation: (a) bone preparation; (b) cement pressure into the prosthetic components; (c) postoperative radiography; (d) failed BHR hip prostheses [63].
2.2. Methods
2.2.1. Scanning Electron Microscopy Coupled with Energy Dispersive Spectroscopy
The morphology of the experimental samples and the elementary chemical composition were evaluated using a QUANTA INSPECT F scanning electron microscope (FEI Company, Eindhoven, The Netherlands) equipped with an energy-dispersive X-ray spectrometer detector (EDAX) (FEI Company, Eindhoven, The Netherlands) with a 132 eV resolution at MnK.
2.2.2. Contact Angle Measurements
The samples’ wettability was assessed by contact angle measurements performed using the KRÜSS DSA30 Drop Shape Analysis System.
The contact angle measurements were performed using the sessile drop method, with each measurement being repeated five times. The samples were fixed on a support to ensure flatness, and, using the automatic dosing system, drops of distilled water with variable volumes were deposited (5–15 µL) depending on the available flat surface. Once the drop of distilled water was deposited, an image was captured using the built-in measuring system camera. The obtained images were processed with the help of the ImageJ software, with which the contact angle was determined.
2.2.3. Compressive Strength Measurements
The mechanical properties of the experimental samples were also evaluated, following their compression strength. The contact area of the acrylic cement with the bone is intensely mechanically stressed, so the determination of the compressive strength is very important [64,65].
This study was designed to determine the properties of the bone cements, mainly their structural characteristics, based on the viscosity information reported by the producer and their mechanical properties using a compression test. For the compression tests, the experiment was randomized. The sample size was influenced by the volume of available materials.
The compression tests were performed conforming to the ASTM D695 Standard Test Method for Compressive Properties of Rigid Plastics specifications using cylindrical specimens with a length double the diameter (ø20 mm × 40 mm). These were subjected to a mechanical compression test using a Walter + Bai LFV 300 device. Figure 5 schematically shows the system used for the compression test and the behavior of the cement during this test.
Figure 5.

Schematic depicting the experimental set-up used for compression testing and sample behavior during the test (image not to scale).
The compression test parameters were set according to the ASTM D695 specifications: The test was controlled by displacement using a speed of 1.3 ± 0.3 mm/min until the yield point was reached; then, the speed was increased to 5 mm/min. The repeatability, reproducibility and accuracy of the test results were verified against previous data [2,66,67]. The calibration and accuracy check of the testing machine were performed by the producer, and interlaboratory tests were performed regularly. Following the compression test, the software automatically generated the stress–strain diagram for all tested samples.
3. Results and Discussion
3.1. Scanning Electron Microscopy Coupled with Energy-Dispersive Spectroscopy Determinations
SEM analysis was carried out to evaluate the structure of the experimental samples and reveal the presence of potential agglomerations that could affect its homogeneity. The elemental composition of the samples was determined using EDS analysis.
Figure 6 shows the SEM images and corresponding EDS spectra for all the investigated samples. The SEM images highlight typical microstructures for PMMA-based cements: beads from the polymer powder; the matrix of the polymerized monomer; and the radiopacifying element—in this case, barium sulphate (BaSO4) and pores.
Figure 6.

Representative SEM images and corresponding EDS spectra of the investigated samples: (a) sample 1; (b) sample 2; (c) sample 3.
The most homogeneous structure was observed for sample 3. For sample 1, SEM images display a slight tendency of barium sulphate to form agglomerates, and some pores could be observed. For sample 2, in contrast, the SEM images highlight agglomerations of the radiopacifying element due to an improper mixing of the cement’s components. As a first conclusion, we recommend centrifugal mixing for this type of cement and avoiding the manual mixing of the cement.
The EDS analysis confirmed the composition of the commercial bone cement and highlighted the presence of the C and O from the two polymer phases (majority elements) and the Ba and S from the radiopacifying element composition.
Regarding the clinical significance of the results shown in this section, we should mention that the mixing is a very important step in bone cement preparation. If the bone cement is not well mixed, agglomerations can appear in the structure with a strong influence on the mechanical properties.
3.2. Contact Angle Determination
The values of the contact angles and the corresponding images for each investigated sample are presented in Table 3 and Figure 7.
Table 3.
Contact angle values for the experimental samples.
| Sample/Bone Cement | Liquid | Contact Angle (°) |
|---|---|---|
| Sample 1 | water | 59.33 ± 2.68 |
| Sample 2 | water | 60.67 ± 4.59 |
| Sample 3 | water | 55.10 ± 3.57 |
Figure 7.
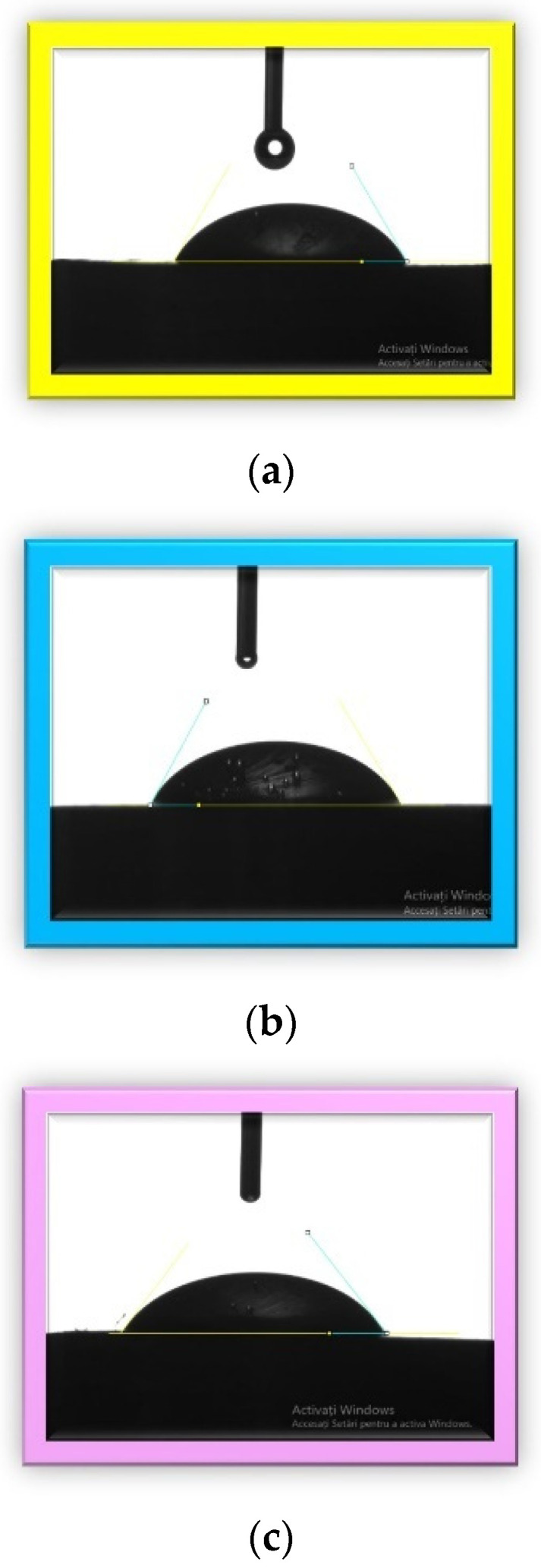
Images of liquid droplets on the surface of materials: (a) sample 1, (b) sample 2, (c) sample 3.
The hydrophilic versus hydrophobic state of a material gives information about its biocompatibility because the surface properties strongly influence the interfaces between biomaterials and tissues [68]. In the literature, polymethylmethacrylate has an intrinsic contact angle of less than 90. The contact angles for the investigated samples in this study were very close to each other and to the PMMA angle, which was around 69° [69,70]. The obtained results indicated that the sample surfaces were hydrophilic. A hydrophilic surface reflects a good wettability and adhesiveness and thus a better osteointegration. Osteointegration is very important from the clinical point of view. An optimal contact angle for cell adhesion is around 55° [71,72], and we obtained the closest angle in this research with sample 3 (55.1°), followed by sample 1 and sample 2.
3.3. Compression Strength Determination
The aspects of the samples before and after performing the compression test are presented in Figure 8. For each investigated bone cement, we used three specimens (except for sample 1, for which 4 specimens were used), each of which had a cylindrical shape.
Figure 8.

Images of the specimens before and after the compressive strength test (before compression—left; after compression—right.
Following the compression test, the software automatically generates the stress–strain diagram for all tested samples as well as a comparative diagram with the values obtained from all samples (Figure 9). From this figure, we can observe, after the compression test, ductile behavior in all the investigated samples. The numerical values after the compression test performed on the investigated samples are presented in Table 4.
Figure 9.

Diagram with the results for compression testing for all experimental samples (sample 1—code 1.1, 1.2, 1.3, 1.4; Sample 2—code 2.1, 2.2, 2.3; and Sample 3 code 3.1, 3.2, 3.3).
Table 4.
The compression test results for the bone cement samples.
| Sample Code | Modulus of Elasticity (MPa) | Yield Strength (MPa) | Maximum Stress (MPa) |
|---|---|---|---|
| 1.1 | 2070.74 | 78.46 | 85.21 |
| 1.2 | 2456.87 | 77.44 | 87.88 |
| 1.3 | 2507.49 | 79.17 | 87.16 |
| 1.4 | 2699.90 | 76.98 | 84.30 |
| Sample 1 average | 2433.75 | 78.01 | 86.14 |
| 2.1 | 1610.59 | 65.59 | 71.60 |
| 2.2 | 2459.59 | 78.73 | 84.02 |
| 2.3 | 2726.22 | 88.33 | 96.55 |
| Sample 2 average | 2265.47 | 77.55 | 84.06 |
| 3.1 | 2272.86 | 94.59 | 107.84 |
| 3.2 | 2335.92 | 90.01 | 101.04 |
| 3.3 | 2315.32 | 94.22 | 100.41 |
| Sample 3 average | 2308.03 | 92.94 | 103.10 |
From the values obtained for yield strength, we observed that all the investigated bone cements fulfilled the minimum value established by the ASTM F451 standard (70 MPa). The best value was recorded for sample 3, an average of 92.94 MPa, followed by sample 1 (78.01 MPa) and sample 2 (77.55 MPa). Regarding the modulus of elasticity of the investigated samples, the values were close. The average modulus of elasticity of the Aminofix 1 sample (sample 1) was 2433.75 ± 263.68 MPa. The Aminofix 3 (sample 2) had an average modulus of elasticity of 2265.47 ± 582.60 MPa, and for the Simplex P (sample 3), the average was 2308.03 ± 32.15. Maximum stress represents the highest stress recorded during the test, and the two types of cement manufactured by the same manufacturer had similar values (~85 MPa).
In Figure 10, we compare the modulus of elasticity, the yield strength and the maximum stress variations, which were later tested using an ANOVA.
Figure 10.

Comparison of the elastic modulus (a), the yield strength (b) and the maximum stress (c) using an ANOVA test.
In a three-level ANOVA (for sample 1, we only used the first three values) of the modulus of elasticity and of the yield strength of the bone cement, the null hypothesis was accepted at α = 0.05; the expectation was that there would be no variation, as observed in the results shown in Table 5 and Table 6.
Table 5.
The ANOVA results for the elastic modulus.
| Source for Variation | Sum of Squares | Degrees of Freedom | Mean Squares | F0 | Fcrit |
|---|---|---|---|---|---|
| Treatments | 6868.58 | 2 | 3434.29 | 0.0249 | 5.1439 |
| Error | 829,084 | 6 | 138,181 | ||
| Total | 835,952 | 8 |
Table 6.
The ANOVA results for the yield strength.
| Source for Variation | Sum of Squares | Degrees of Freedom | Mean Squares | F0 | Fcrit |
|---|---|---|---|---|---|
| Treatments | 450.18 | 2 | 225.09 | 4.909 | 5.143 |
| Error | 275.10 | 6 | 45.85 | ||
| Total | 725.28 | 8 |
Regarding the maximum stress, the results presented in Table 7 show that there was variation within the results; thus, the alternative hypothesis was accepted.
Table 7.
The ANOVA results for the maximum stress.
| Source for Variation | Sum of Squares | Degrees of Freedom | Mean Squares | F0 | Fcrit |
|---|---|---|---|---|---|
| Treatments | 636.99 | 2 | 318.49 | 5.48 | 5.14 |
| Error | 349.02 | 6 | 58.17 | ||
| Total | 986.01 | 8 |
4. Conclusions
In the early stage of arthroplasty, it was difficult for orthopedic surgeons to identify the importance of the cementing technique and the bone cement selected, facts that led to numerous implant failures [73,74,75,76,77,78]. It is imperative for the clinical personnel who intraoperatively prepare the bone cements to precisely know all the required steps, mixing techniques, polymerization characteristics and handling procedures of the bone cements used in order to obtain a durable and high-quality fixation of the prosthesis components [55].
The investigated samples showed a structure that is typical for acrylic bone cements, with a tendency to form agglomerates due to improper mixing, specifically in the case of sample 2, which clearly demonstrated that manual product preparation can sometimes lead to structural unevenness. The wettability measured by determining the contact angle indicated the hydrophilicity of the investigated samples. In terms of mechanical properties, all investigated samples showed optimal values in accordance with the ASTM F451 standard; sample 3 achieved the best yield strength.
From the obtained results, we can conclude that the cement handling process (mixing stage, sticky/waiting stage, working stage) has an important role to play in the structural integrity and mechanical properties of bone cements and that manual mixing is to be avoided in the specific case of low-viscosity bone cements.
Although this study presents some limitations related to the small number of samples used and the reproducibility of the in vivo working conditions, we consider that the important information obtained will be of use to specialists in bone cement production as well as the clinicians who use bone cements.
In this paper, we found that there is no universal bone cement that can be used for all hip prostheses and that the selection and use of bone cements for hip prosthesis fixation must be correlated with hip prosthesis design, the fixation technique and devices used and the material properties.
Author Contributions
A.A. and I.A. conceived and designed the experiments, A.R., R.C., M.B.C. and I.D.C. performed the experiments, H.D. and N.F. analyzed the data, A.A. and I.A. conceived the methodology, A.R., R.C., A.A., I.A., A.D.R., H.D., N.F. and I.D.C. validated the obtained results; A.R. and A.A. wrote the original draft; I.A. performed review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by a grant of the Romanian Ministry of Education and Research, CNCS-UEFISCDI, Project number PN-III-P4-ID-PCE-2020-2591, within PNCDI III. In addition, financial support from the Competitiveness Operational Program 2014-2020, Action 1.1.3: Creating synergies with RDI actions of the EU’s HORIZON 2020 framework program and other international RDI programs, MySMIS Code 108792, Acronym project “UPB4H”, financed by contract: 250/11.05.2020 is gratefully acknowledged.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Footnotes
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Corobea M.S., Albu M.G., Ion R., Cimpean A., Miculescu F., Antoniac I.V., Raditoiu V., Sirbu I., Stoenescu M., Voicu S.I., et al. Modification of Titanium Surface with Collagen and Doxycycline as a New Approach in Dental Implants. J. Adhes. Sci. Technol. 2015;29:2537–2550. doi: 10.1080/01694243.2015.1073661. [DOI] [Google Scholar]
- 2.Pantea M., Antoniac I., Trante O., Ciocoiu R., Fischer C.A., Traistaru T. Correlations between Connector Geometry and Strength of Zirconia-Based Fixed Partial Dentures. Mater. Chem. Phys. 2019;222:96–109. doi: 10.1016/j.matchemphys.2018.09.063. [DOI] [Google Scholar]
- 3.Marinescu R., Antoniac I., Laptoiu D., Antoniac A., Grecu D. Complications Related to Biocomposite Screw Fixation in ACL Reconstruction Based on Clinical Experience and Retrieval Analysis. Mater. Plast. 2015;52:340–344. [Google Scholar]
- 4.Botez P., Sirbu P., Simion L., Munteanu F.L., Antoniac I. Application of a Biphasic Macroporous Synthetic Bone Substitutes Ceraform®: Clinical and Histological Results. Eur. J. Orthop. Surg. Traumatol. 2009;19:387–395. doi: 10.1007/s00590-009-0445-7. [DOI] [Google Scholar]
- 5.Gheorghe D., Pop D.M., Ciocoiu R., Trante O., Milea C., Mohan A.G., Benea H., Saceleanu V. Microstructure Development in Titanium and Its Alloys Used for Medical Applications. UPB Sci. Bull. Ser. B Chem. Mater. Sci. 2019;81:244–258. [Google Scholar]
- 6.Cavalu S., Antoniac I.V., Fritea L., Mates I.M., Milea C., Laslo V., Vicas S., Mohan A. Surface Modifications of the Titanium Mesh for Cranioplasty Using Selenium Nanoparticles Coating. J. Adhes. Sci. Technol. 2018;32:2509–2522. doi: 10.1080/01694243.2018.1490067. [DOI] [Google Scholar]
- 7.Antoniac I.V., Ionescu R.D., Burcea M., Balta F. IOL’s Opacification: A Complex Analysis Based on the Clinical Aspects, Biomaterials Used and Surface Characterization of Explanted IOL’s. Mater. Plast. 2015;52:109–112. [Google Scholar]
- 8.Cirstoiu M., Cirstoiu C., Antoniac I., Munteanu O. Levonorgestrel-Releasing Intrauterine Systems: Device Design, Biomaterials, Mechanism of Action and Surgical Technique. Mater. Plast. 2015;52:258–262. [Google Scholar]
- 9.Brătilă E., Comandasu D., Milea C., Berceanu C., Vasile E., Antoniac I., Mehedintu C. Effect of the Surface Modification of the Synthetic Meshes Used in the Surgical Treatment of Pelvic Organ Prolapse on the Tissue Adhesion and Clinical Functionality. J. Adhes. Sci. Technol. 2017;31:2028–2043. doi: 10.1080/01694243.2017.1294358. [DOI] [Google Scholar]
- 10.Moldovan H., Gheorghita D., Antoniac I., Gheorghe D., Fiori F., Mohan A., Raftu G., Ionel C., Costache V. Bioadhesives Used in Cardiovascular Surgery. Rev. De Chim. 2018;69:2799–2803. doi: 10.37358/RC.18.10.6627. [DOI] [Google Scholar]
- 11.Costache V.S., Meekel J.P., Costache A., Melnic T., Solomon C., Chitic A.M., Bucurenciu C., Moldovan H., Antoniac I., Candea G., et al. Geometric Analysis of Type B Aortic Dissections Shows Aortic Remodeling After Intervention Using Multilayer Stents. Materials. 2020;13:2274. doi: 10.3390/ma13102274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mavrodin C.I., Pariza G., Ion D., Antoniac V.I. Abdominal Compartment Syndrome—a Major Complication of Large Incisional Hernia Surgery. Chirurgia. 2013;108:414–417. [PubMed] [Google Scholar]
- 13.Pariza G., Mavrodin C.I., Antoniac I. Dependency Between the Porosity and Polymeric Structure of Biomaterials Used in Hernia Surgery and Chronic Mesh—Infection. Mater. Plast. 2015;52:484–486. [Google Scholar]
- 14.Manescu V., Paltanea G., Antoniac I., Vasilescu M. Magnetic Nanoparticles Used in Oncology. Materials. 2021;14:5948. doi: 10.3390/ma14205948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chitea C., Tomoaia G., Toader O.D., Milea C., Trante O., Earar K., Saceleanu V. Evaluation of the Biocompatibility and Graft Integration Following Ligamentoplasty or Augmentation. Experimental Study on Rabbits. Rev. Chim. 2019;70:1460–1465. doi: 10.37358/RC.19.4.7149. [DOI] [Google Scholar]
- 16.Cavalu S., Antoniac I.V., Mohan A., Bodog F., Doicin C., Mates I., Ulmeanu M., Murzac R., Semenescu A. Nanoparticles and Nanostructured Surface Fabrication for Innovative Cranial and Maxillofacial Surgery. Materials. 2020;13:5391. doi: 10.3390/ma13235391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Robu A., Antoniac A., Grosu E., Vasile E., Raiciu A.D., Iordache F., Antoniac V.I., Rau J.V., Yankova V.G., Ditu L.M., et al. Additives Imparting Antimicrobial Properties to Acrylic Bone Cements. Materials. 2021;14:7031. doi: 10.3390/ma14227031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Vaishya R., Chauhan M., Vaish A. Bone Cement. J. Clin. Orthop. Trauma. 2013;4:157–163. doi: 10.1016/j.jcot.2013.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Deb S. Orthopedic Bone Cement. In: Metin A., editor. Wiley Encyclopedia of Biomedical Engineering. John Wiley & Sons; Hoboken, NJ, USA: 2006. [Google Scholar]
- 20.Rivis M., Pricop M., Talpos S., Ciocoiu R., Antoniac I., Gheorghita D., Trante O., Moldovan H., Grigorescu G., Seceleanu V., et al. Influence of the Bone Cements Processing on the Mechanical Properties in Cranioplasty. Rev. Chim. 2018;69:990–993. doi: 10.37358/RC.18.4.6243. [DOI] [Google Scholar]
- 21.Vasilyev A.V., Kuznetsova V.S., Bukharova T.B., Grigoriev T.E., Zagoskin Y.D., Korolenkova M.V., Zorina O.A., Chvalun S.N., Goldshtein D.V., Kulakov A.A. Development Prospects of Curable Osteoplastic Materials in Dentistry and Maxillofacial Surgery. Heliyon. 2020;6:e04686. doi: 10.1016/j.heliyon.2020.e04686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Al-Maawi S., Ambrosio L., Best S.M., Brown O., Chambers P., Chamorro N.P., Chatzistavrou X., Cifuentes Cuellar S., de Santis R., Delgado López J., et al. List of Contributors. In: Pawelec K.M., Planell J.A., editors. Bone Repair Biomaterials. Elsevier; Amsterdam, The Netherlands: 2019. pp. 233–271. [Google Scholar]
- 23.Cojocaru F.D., Balan V., Popa M.I., Lobiuc A., Antoniac A., Antoniac I.V., Verestiuc L. Biopolymers—Calcium Phosphates Composites with Inclusions of Magnetic Nanoparticles for Bone Tissue Engineering. Int. J. Biol. Macromol. 2019;125:612–620. doi: 10.1016/j.ijbiomac.2018.12.083. [DOI] [PubMed] [Google Scholar]
- 24.Ishikawa K., Takagi S., Chow L., Ishikawa Y. Properties and mechanisms of fast-setting calcium phosphate cements. J. Mater. Sci. Mater. Med. 1995;6:528–533. doi: 10.1007/BF00151034. [DOI] [Google Scholar]
- 25.Ouinas D., Bouiadjra B.B., Serier B., Benderdouche N., Ouinas A. Numerical Analysis of Brazilian Bioceramic Discs under Diametrical Compression Loading. Comput. Mater. Sci. 2009;45:443–448. doi: 10.1016/j.commatsci.2008.11.004. [DOI] [Google Scholar]
- 26.Eliaz N., Metoki N. Calcium Phosphate Bioceramics: A Review of Their History, Structure, Properties, Coating Technologies and Biomedical Applications. Materials. 2017;10:334. doi: 10.3390/ma10040334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lodoso-Torrecilla I., van den Beucken J.J.J.P., Jansen J.A. Calcium Phosphate Cements: Optimization toward Biodegradability. Acta Biomater. 2021;119:1–12. doi: 10.1016/j.actbio.2020.10.013. [DOI] [PubMed] [Google Scholar]
- 28.Pivec R., Johnson A.J., Mears S.C., Mont M.A. Hip Arthroplasty. Lancet. 2012;380:1768–1777. doi: 10.1016/S0140-6736(12)60607-2. [DOI] [PubMed] [Google Scholar]
- 29.Kurtz S., Ong K., Lau E., Mowat F., Halpern M. Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. 2007;89:780–785. doi: 10.2106/00004623-200704000-00012. [DOI] [PubMed] [Google Scholar]
- 30.Singh J.A. Epidemiology of Knee and Hip Arthroplasty: A Systematic Review. Open Orthop. J. 2011;5:80–85. doi: 10.2174/1874325001105010080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Liu X.-W., Zi Y., Xiang L.-B., Wang Y. Total Hip Arthroplasty: Areview of Advances, Advantages and Limitations. Int. J. Clin. Exp. Med. 2015;8:27–36. [PMC free article] [PubMed] [Google Scholar]
- 32.Ginebra M.-P., Montufar E.B. Bone Repair Biomaterials. Elsevier; Amsterdam, The Netherlands: 2019. Cements as Bone Repair Materials; pp. 233–271. [Google Scholar]
- 33.Orban H., Cirstoiu C., Zaharia C., Cincu C. Acrylic Cement Advantages or Disadvantages in Orthopaedic Surgery. Rev. Chim. 2008;59:688. doi: 10.37358/RC.08.6.1856. [DOI] [Google Scholar]
- 34.Bentia D.R., Iacob G., Ciurea A.V. Biomateriale În Vertebroplastia Percutană. Rom. J. Med. Pract. 2017;12:212–219. doi: 10.37897/RJMP.2017.4.7. [DOI] [Google Scholar]
- 35.Haddad F.S., Levell N.J., Dowd P.M., Cobb A.G., Bentley G. Cement Hypersensitivity: A Cause of Aseptic Loosening? J. Bone Jt. Surg. Br. 1995;77:329–330. doi: 10.1302/0301-620X.77B2.7706360. [DOI] [PubMed] [Google Scholar]
- 36.Aronson J.K., editor. Meyler’s Side Effects of Drugs. Elsevier; Amsterdam, The Netherlands: 2016. Acrylic Bone Cement; pp. 63–64. [Google Scholar]
- 37.Nasrollahi N., Nourian Dehkordi A., Jamshidizad A., Chehelgerdi M. Preparation of Brushite Cements with Improved Properties by Adding Graphene Oxide. Int. J. Nanomed. 2019;14:3785–3797. doi: 10.2147/IJN.S196666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Engstrand J., Persson C., Engqvist H. The Effect of Composition on Mechanical Properties of Brushite Cements. J. Mech. Behav. Biomed. Mater. 2014;29:81–90. doi: 10.1016/j.jmbbm.2013.08.024. [DOI] [PubMed] [Google Scholar]
- 39.Nelissen R.G.H.H., Garling E.H., Valstar E.R. Influence of Cement Viscosity and Cement Mantle Thickness on Migration of the Exeter Total Hip Prosthesis. J. Arthroplast. 2005;20:521–528. doi: 10.1016/j.arth.2004.09.036. [DOI] [PubMed] [Google Scholar]
- 40.Mulroy R., Harris W. The Effect of Improved Cementing Techniques on Component Loosening in Total Hip Replacement. An 11-Year Radiographic Review. J. Bone Jt. Surg. 1990;72:757–760. doi: 10.1302/0301-620X.72B5.2211749. [DOI] [PubMed] [Google Scholar]
- 41.Randall D.J., Anderson M.B., Gililland J.M., Peters C.L., Pelt C.E. A Potential Need for Surgeon Consensus: Cementation Techniques for Total Knee Arthroplasty in Orthopedic Implant Manufacturer’s Guidelines Lack Consistency. J. Orthop. Surg. 2019;27:1–16. doi: 10.1177/2309499019878258. [DOI] [PubMed] [Google Scholar]
- 42.Niculescu M., Solomon B.L., Viscopoleanu G., Antoniac I. Evolution of Cementation Techniques and Bone Cements in Hip Arthroplasty. In: Antoniac I.V., editor. Handbook of Bioceramics and Biocomposites. Springer International Publishing; Cham, Switzerland: 2014. pp. 1–41. [Google Scholar]
- 43.Donaldson A.J., Thomson H.E., Harper N.J., Kenny N.W. Bone Cement Implantation Syndrome. Br. J. Anaesth. 2009;102:12–22. doi: 10.1093/bja/aen328. [DOI] [PubMed] [Google Scholar]
- 44.van de Groes S.A.W., de Waal Malefijt M.C., Verdonschot N. Influence of Preparation Techniques to the Strength of the Bone–Cement Interface behind the Flange in Total Knee Arthroplasty. Knee. 2013;20:186–190. doi: 10.1016/j.knee.2012.08.002. [DOI] [PubMed] [Google Scholar]
- 45.Grecu D.C., Antoniac I.V., Trante O., Niculescu M., Lupescu O. Failure Analysis of Retrieved Polyethylene Insert in Total Knee Replacement. Mater. Plast. 2016;53:776–780. [Google Scholar]
- 46.Antoniac I., Negrusoiu M., Laptoiu D., Miculescu M. Biomaterials Researches to Improve the Biofunctionality of an Mixed Fixing System for Long Bone Fractures; Proceedings of the Transactions of the 7th World Biomaterials Congress; Sydney, Australia. 17–21 May 2004. [Google Scholar]
- 47.Pala E., Trovarelli G., Calabrò T., Angelini A., Abati C.N., Ruggieri P. Survival of Modern Knee Tumor Megaprostheses: Failures, Functional Results, and a Comparative Statistical Analysis. Clin. Orthop. Relat. Res. 2015;473:891–899. doi: 10.1007/s11999-014-3699-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Henderson E.R., Groundland J.S., Pala E., Dennis J.A., Wooten R., Cheong D., Windhager R., Kotz R.I., Mercuri M., Funovics P.T., et al. Failure Mode Classification for Tumor Endoprostheses: Retrospective Review of Five Institutions and a Literature Review. J. Bone Jt. Surg. 2011;93:418–429. doi: 10.2106/JBJS.J.00834. [DOI] [PubMed] [Google Scholar]
- 49.Shehadeh A., Noveau J., Malawer M., Henshaw R. Late Complications and Survival of Endoprosthetic Reconstruction after Resection of Bone Tumors. Clin. Orthop. Relat. Res. 2010;468:2885–2895. doi: 10.1007/s11999-010-1454-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Bergin P.F., Noveau J.B., Jelinek J.S., Henshaw R.M. Aseptic Loosening Rates in Distal Femoral Endoprostheses: Does Stem Size Matter? Clin. Orthop. Relat. Res. 2012;470:743–750. doi: 10.1007/s11999-011-2081-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Jorge R.M.N., Piloto P.A.G., Belinha J., Oliveira V.C.C., Fonseca E.M.M., Rua C.C. Bone Metastatic Tumour Minimisation Due to Thermal Cementoplasty Effect, Clinical and Computational Methodologies. Int. J. Med. Eng. Inform. 2020;13:35–43. doi: 10.1504/IJMEI.2020.10031214. [DOI] [Google Scholar]
- 52.Bitsch R.G., Jäger S., Lürssen M., Loidolt T., Schmalzried T.P., Weiss S. The Influence of Cementing Technique in Hip Resurfacing Arthroplasty on the Initial Stability of the Femoral Component. Int. Orthop. 2011;35:1759–1765. doi: 10.1007/s00264-011-1212-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Ko D.O., Lee S., Kim K.T., Lee J.I., Kim J.W., Yi S.M. Cement Mantle Thickness at the Bone Cement Interface in Total Knee Arthroplasty: Comparison of PS150 RP and LPS-Flex Knee Implants. Knee Surg. Relat. Res. 2017;29:115–121. doi: 10.5792/ksrr.16.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Surgical Technique for BIRMINGHAM HIP Resurfacing Prosthesis. [(accessed on 4 February 2022)]. Available online: https://www.smith-nephew.com/global/surgicaltechniques/recon/04727%20v2%2045670103%20revc%20us%20bhr%20surgical%20technique%2001.18hr.pdf/
- 55.Niculescu M., Viscopoleanu G., Sirbu A., Antoniac I. Tehnica Cimentarii in Artroplastia Totala de Sold. Universitatea Carol Davila; Bucuresti, Romania: 2017. [Google Scholar]
- 56.Ionescu R., Cristescu I., Dinu M., Saban R., Antoniac I., Vilcioiu D. Clinical, Biomechanical and Biomaterials Approach in the Case of Fracture Repair Using Different Systems Type Plate-Screw. Key Eng. Mater. 2013;583:150–154. doi: 10.4028/www.scientific.net/KEM.583.150. [DOI] [Google Scholar]
- 57.Carbonell-Blasco P., Martín-Martínez J.M., Antoniac I.V. Synthesis and Characterization of Polyurethane Sealants Containing Rosin Intended for Sealing Defect in Annulus for Disc Regeneration. Int. J. Adhes. Adhes. 2013;42:11–20. doi: 10.1016/j.ijadhadh.2012.11.011. [DOI] [Google Scholar]
- 58.Antoniac I., Antoniac A., Gheorghita D., Gradinaru S. In Vitro Study on Biodegradation of Absorbable Suture Materials Used for Surgical Applications. Mater. Plast. 2021;58:130–139. doi: 10.37358/MP.21.2.5484. [DOI] [Google Scholar]
- 59.He Z., Zhai Q., Hu M., Cao C., Wang J., Yang H., Li B. Bone Cements for Percutaneous Vertebroplasty and Balloon Kyphoplasty: Current Status and Future Developments. J. Orthop. Transl. 2015;3:1–11. doi: 10.1016/j.jot.2014.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Anselmetti G.C., Manca A., Kanika K., Murphy K., Eminefendic H., Masala S., Regge D. Temperature Measurement During Polymerization of Bone Cement in Percutaneous Vertebroplasty: An In Vivo Study in Humans. Cardiovasc. Interv. Radiol. 2009;32:491–498. doi: 10.1007/s00270-009-9509-7. [DOI] [PubMed] [Google Scholar]
- 61.Bacali C., Badea M., Moldovan M., Sarosi C., Nastase V., Baldea I., Chiorean R.S., Constantiniuc M. The Influence of Graphene in Improvement of Physico-Mechanical Properties in PMMA Denture Base Resins. Materials. 2019;12:2335. doi: 10.3390/ma12142335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Bacali C., Buduru S., Nastase V., Craciun A., Prodan D., Constantiniuc M., Badea M., Moldovan M., Sarosi C. Solubility, Ductility and Resilience of a PMMA Denture Resin with Graphene and Silver Nanoparticles Addition. Studia Univ. Babeș-Bolyai Chem. 2019;64:471–481. doi: 10.24193/subbchem.2019.2.40. [DOI] [Google Scholar]
- 63.How Do We Choose a Hip Prosthesis for the Patient? [(accessed on 7 February 2022)]. Available online: https://vladpredescu.ro.
- 64.Chua C.K., Wong C.H., Yeong W.Y. Standards, Quality Control, and Measurement Sciences in 3D Printing and Additive Manufacturing. 1st ed. Academic Press; Cambridge, MA, USA: 2017. [Google Scholar]
- 65.Kuehn K.-D., Ege W., Gopp U. Acrylic Bone Cements: Mechanical and Physical Properties. Orthop. Clin. N. Am. 2005;36:29–39. doi: 10.1016/j.ocl.2004.06.011. [DOI] [PubMed] [Google Scholar]
- 66.Dascalu C.-A., Miculescu F., Mocanu A.-C., Constantinescu A.E., Butte T.M., Pandele A.M., Ciocoiu R.-C., Voicu S.I., Ciocan L.T. Novel Synthesis of Core-Shell Biomaterials from Polymeric Filaments with a Bioceramic Coating for Biomedical Applications. Coatings. 2020;10:283. doi: 10.3390/coatings10030283. [DOI] [Google Scholar]
- 67.Maidaniuc A., Miculescu F., Ciocoiu R.C., Butte T.M., Pasuk I., Stan G.E., Voicu S.I., Ciocan L.T. Effect of the Processing Parameters on Surface, Physico-Chemical and Mechanical Features of Bioceramics Synthesized from Abundant Carp Fish Bones. Ceram. Int. 2020;46:10159–10171. doi: 10.1016/j.ceramint.2020.01.007. [DOI] [Google Scholar]
- 68.Antoniac I., Stoia D., Ghiban B., Tecu C., Miculescu F., Vigaru C., Saceleanu V. Failure Analysis of a Humeral Shaft Locking Compression Plate—Surface Investigation and Simulation by Finite Element Method. Materials. 2019;12:1128. doi: 10.3390/ma12071128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Ma Y., Cao X., Feng X., Ma Y., Zou H. Fabrication of Super-Hydrophobic Film from PMMA with Intrinsic Water Contact Angle below 90°. Polymer. 2007;48:7455–7460. doi: 10.1016/j.polymer.2007.10.038. [DOI] [Google Scholar]
- 70.Brugnara M., Volpe C.D., Siboni S., Zeni D. Contact Angle Analysis on Polymethylmethacrylate and Commercial Wax by Using an Environmental Scanning Electron Microscope. Scanning. 2007;28:267–273. doi: 10.1002/sca.4950280504. [DOI] [PubMed] [Google Scholar]
- 71.Chen S., Guo Y., Liu R., Wu S., Fang J., Huang B., Li Z., Chen Z., Chen Z. Tuning Surface Properties of Bone Biomaterials to Manipulate Osteoblastic Cell Adhesion and the Signaling Pathways for the Enhancement of Early Osseointegration. Colloids Surf. B Biointerfaces. 2018;164:58–69. doi: 10.1016/j.colsurfb.2018.01.022. [DOI] [PubMed] [Google Scholar]
- 72.Xu C., Yang F., Wang S., Ramakrishna S. In Vitro Study of Human Vascular Endothelial Cell Function on Materials with Various Surface Roughness. J. Biomed. Mater. Res. 2004;71:154–161. doi: 10.1002/jbm.a.30143. [DOI] [PubMed] [Google Scholar]
- 73.Tecu C., Antoniac I., Goller G., Yavas B., Gheorghe D., Antoniac A., Ciuca I., Semenescu A., Raiciu A.D., Cristescu I. The Sintering Behaviour and Mechanical Properties of Hydroxyapatite—Based Composites for Bone Tissue Regeneration. Mater. Plast. 2019;56:644–648. doi: 10.37358/MP.19.3.5246. [DOI] [Google Scholar]
- 74.Nica M., Cretu B., Ene D., Antoniac I., Gheorghita D., Ene R. Failure Analysis of Retrieved Osteosynthesis Implants. Materials. 2020;13:1201. doi: 10.3390/ma13051201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Chirca O., Biclesanu C., Florescu A., Stoia D.I., Pangica A.M., Burcea A., Vasilescu M., Antoniac I.V. Adhesive-Ceramic Interface Behavior in Dental Restorations. FEM Study and SEM Investigation. Materials. 2021;14:5048. doi: 10.3390/ma14175048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Marinescu R., Antoniac V.I., Stoia D.I., Lăptoiu D.C. Clavicle Anatomical Osteosynthesis Plate Breakage—Failure Analysis Report Based on Patient Morphological Parameters. Rom. J. Morphol. Embryol. 2017;58:593–598. [PubMed] [Google Scholar]
- 77.Antoniac I., Negrusoiu M., Mardare M., Socoliuc C., Zazgyva A., Niculescu M. Adverse Local Tissue Reaction after 2 Revision Hip Replacements for Ceramic Liner Fracture. Medicine. 2017;96:e6687. doi: 10.1097/MD.0000000000006687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Bane M., Miculescu F., Blajan A.I., Dinu M., Antoniac I. Failure Analysis of Some Retrieved Orthopedic Implants Based on Materials Characterization. Solid State Phenom. 2012;188:114–117. doi: 10.4028/www.scientific.net/SSP.188.114. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.