

Abstract
Background
Mycoplasma pneumoniae respiratory infections are transmitted by aerosol and droplets in close contact.
Aim
We investigated global M. pneumoniae incidence after implementation of non-pharmaceutical interventions (NPIs) against COVID-19 in March 2020.
Methods
We surveyed M. pneumoniae detections from laboratories and surveillance systems (national or regional) across the world from 1 April 2020 to 31 March 2021 and compared them with cases from corresponding months between 2017 and 2020. Macrolide-resistant M. pneumoniae (MRMp) data were collected from 1 April 2017 to 31 March 2021.
Results
Thirty-seven sites from 21 countries in Europe, Asia, America and Oceania submitted valid datasets (631,104 tests). Among the 30,617 M. pneumoniae detections, 62.39% were based on direct test methods (predominantly PCR), 34.24% on a combination of PCR and serology (no distinction between methods) and 3.37% on serology alone (only IgM considered). In all countries, M. pneumoniae incidence by direct test methods declined significantly after implementation of NPIs with a mean of 1.69% (SD ± 3.30) compared with 8.61% (SD ± 10.62) in previous years (p < 0.01). Detection rates decreased with direct but not with indirect test methods (serology) (–93.51% vs + 18.08%; p < 0.01). Direct detections remained low worldwide throughout April 2020 to March 2021 despite widely differing lockdown or school closure periods. Seven sites (Europe, Asia and America) reported MRMp detections in one of 22 investigated cases in April 2020 to March 2021 and 176 of 762 (23.10%) in previous years (p = 0.04).
Conclusions
This comprehensive collection of M. pneumoniae detections worldwide shows correlation between COVID-19 NPIs and significantly reduced detection numbers.
Keywords: Face masks, nonpharmaceutical interventions (NPIs), personal protective equipment (PPE), pneumonia, Mycoplasma pneumoniae, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
Introduction
Non-pharmaceutical interventions (NPIs) were suggested to reduce the spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) during the worldwide coronavirus disease (COVID-19) pandemic [1]. Many countries introduced NPIs in March 2020, which included physical distancing measures, personal protective measures (e.g. the use of masks, improved hand hygiene, respiratory etiquette), stay-at-home orders, school and day-care closures, closing borders and travel restrictions. The NPIs have been temporally associated with a global unprecedented suppression of influenza epidemics and other viral respiratory infections, such as respiratory syncytial virus (RSV) [2-8]. COVID-19 vaccinations were available as measures in addition to NPIs since December 2020 [9].
Data from some countries during the first months in 2020 indicated that the introduction of NPIs also coincided with a reduction in Mycoplasma pneumoniae detections [2,6,10]. Mycoplasma pneumoniae is a major bacterial cause of respiratory tract infections in children and adults [11]. These infections occur both endemically in many different climates across the world and epidemically every few years. Previous epidemics in Europe were reported in 2010–2012, 2014–2015 and 2015–2017 [12-15]. Mycoplasma pneumoniae is transmitted by aerosol particles and respiratory droplets through close contacts within families, schools, military bases, institutions (residential care and nursing homes, homes for cognitively disabled people etc.) and among closed communities [15-17].
Diagnostic tests for M. pneumoniae include nucleic acid amplification tests (NAAT) such as PCR, antigen tests and culture from respiratory specimens (direct test methods) or serology (indirect test method) with varying sensitivities and specificities [11,18,19]. Real-time PCR applications are the most commonly used approach for detection of M. pneumoniae in clinical settings [20]. However, real-time PCR is not yet standardised across laboratories [20], and there are no internationally defined guidelines on the requirements for M. pneumoniae testing and surveillance [14]. Some countries collect laboratory reports on M. pneumoniae detections through national reference laboratories (e.g. England), but only few countries have a national surveillance (e.g. Denmark) [14]. To our knowledge, no analysis on the M. pneumoniae incidence from several United Nations (UN) regions has been published so far.
In this study, we used survey data on laboratory M. pneumoniae testing and detection before and during the COVID-19 pandemic across the world to assess the impact of NPIs on the global incidence of M. pneumoniae in the first year after the implementation of NPIs. Of particular interest was the impact of children returning to schools on M. pneumoniae incidence while maintaining other NPIs during the course of the pandemic, as children are believed to be the main drivers of M. pneumoniae transmission [16] and have greater difficulty adhering to physical distancing and personal protective measures. In this context, was also analysed the proportion of females in particular because of their assumed closer vicinity with children.
Methods
Study design
Survey development
A structured survey was developed by a group of members from the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Mycoplasma and Chlamydia Infections (ESGMAC), according to guidelines for survey research [21,22]. The survey consisted of six items, covering (i) details of the survey participant, (ii) information on laboratory and area, (iii) local information on stay-at-home orders and school closures during the first year of the pandemic, (iv) detailed information on the test method for M. pneumoniae detection (technique, product and company or reference), (v) M. pneumoniae test numbers (total tests, positive tests, positive tests by month, proportion of children/adolescents younger than 18 years and of females of any age) for the first 12-month period after the worldwide implementation of NPIs (1 April 2020 to 31 March 2021) and for the same period in the preceding 3 years (1 April 2017 to 31 March 2020), and (vi) macrolide-resistant M. pneumoniae (MRMp) testing and detection during the same periods. The survey was only administered in English and built in the SurveyMonkey online survey platform [23]. A pilot test was performed with 10 individuals (infectious diseases specialists and microbiologists) to ensure that the questions were understood and interpreted consistently and that collection of requested data was feasible within the survey time period. Details of the survey are shown in Supplementary Table S1.
Survey administration
Dissemination of the survey to invite participation was mixed-mode through societies (ESCMID, ESGMAC, International Organisation for Mycoplasmology (IOM) and national societies for infectious diseases and microbiology via newsletter or email distribution lists), social media (ESCMID, ESGMAC, IOM and personal accounts of authors), and through in-person contact to potential participants by one of the authors (P.M.M.S). Potential participants were defined as authors of publications about M. pneumoniae epidemiology (PubMed search terms: “Mycoplasma pneumoniae” [title] and “epidemiology” [all fields], 1 January 2000 to 30 March 2021; search results: 439), and more than 300 corresponding authors were approached via email. The email was accompanied by a one-page study description on behalf of the ESGMAC, the survey in PDF and Word format and the link to the online survey. Close attention was paid to ensure that all UN regions were represented during dissemination of the survey. Participation was voluntary and without compensation. There was no mechanism in place to acknowledge receipt of the survey if a laboratory did not provide information. Consent to publish the data and be listed as a participant was declared on the first page of the questionnaire. The survey was launched on 30 March 2021. Reminders were sent out after 4 and 6 weeks via social media and email. The survey was closed on 31 May 2021.
Data collection
Quality control
Entries were included if they met the following quality control criteria for valid datasets: (i) verification of the participant, laboratory and institution via provided link and/or references in PubMed, (ii) validation of the information and/or references about the test method, and (iii) data check for multiple entries from the same institutions (double reporting), invalid or incomplete data, and inconsistent entries. In case of inconsistency or multiple entries from the same institutions, participants were contacted by email to request clarification and/or adapt entries to exclude double reporting. Criteria for de-duplication and exclusion criteria are listed in Supplementary Table S2.
Case definition
Because of local variation in the definition of M. pneumoniae infection, absence of clinical data and the difficulty to differentiate between M. pneumoniae infection and carriage [24], this study collated information on M. pneumoniae detections and not infections. A case was defined as M. pneumoniae detection in an individual with currently available test methods. Detailed information about microbiological detection methods (technique, product and company or reference) is listed in Table 1. A positive IgM, IgG or IgA serology was defined as antibody level above the cut-off of the test, as indicated by the manufacturer (Table 1). Participants were asked whether a positive serology was confirmed by a fourfold increase in IgG levels measured in convalescent samples (as serological gold standard for M. pneumoniae infection [11]).
Table 1. Demographic characteristics and laboratory information of participating sites, by United Nations (UN) region, global survey of Mycoplasma pneumoniae detections, April 2017–March 2021.
| UN region and country | City or region | National pandemic lockdown (days, period)a | School closure duration (days)b | Laboratory and/or systemc | Test method (technique; product) | Company or reference | Macrolide resistance determination |
|---|---|---|---|---|---|---|---|
| Europe | |||||||
| Western Europe | |||||||
| France | Bordeaux | 102 days (17 Mar–11 May 2020; 28 Oct–14 Dec 2020) |
43 | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; in-house) | [47] | Yes [48] |
| Switzerland | Geneva | 41 days (16 Mar–26 Apr 2020) |
31 | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, real-time; BioGX Sample-Ready BD MAX System) | BD Diagnostics | No |
| Lausanne | Hospital / clinical laboratory (secondary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel) | bioMérieux/BioFire Diagnostics | No | |||
| Bernd | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, real-time; Anyplex II RB5 Detection) | Seegene Inc. | No | |||
| Lucerned | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel) | bioMérieux/BioFire Diagnostics | No | |||
| Bellinzona | Surveillance system (regional; 0.4 million population) e | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel)f | bioMérieux/BioFire Diagnostics | No | |||
| Zurich (A) | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; in-house) | [49] | Yes [50] | |||
| Zurich (B)d | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; in-house)g | [49] | Yes [50] | |||
| St. Gallend | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, real-time; Allplex Respiratory Panel) | Seegene Inc. | No | |||
| Aarau | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel) | bioMérieux/BioFire Diagnostics | No | |||
| ELISAh (ImmunoWELL Mycoplasma IgM/IgG) | Thermo Fisher Scientific Remel Inc. | ||||||
| Basel (A) | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel) | bioMérieux/BioFire Diagnostics | No | |||
| Basel (B)d | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel)i | bioMérieux/BioFire Diagnostics | No | |||
| Germany | Homburg | 161 days (17 Mar–5 May 2020; 19 Dec 2020–end of survey period) |
92 | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, real-time; AID CAP Bac PCR Kit) | Autoimmun Diagnostika GmbH (AID) | No |
| CLIAh (Mycoplasma pneumoniae Virclia IgM/IgG Monotest) | Vircell, S.L. | ||||||
| Düsseldorf | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; in-house) | [51] | No | |||
| ELISAh (EIA Mycoplasma IgM/IgG/IgA) | DIAsource ImmunoAssays SA | ||||||
| Saxonyj | Surveillance system (regional; 4.1 million population) k | Combination of direct and indirect test methods (different techniques)k | [12] | No | |||
| Belgium | Antwerp, Leuven (national reference laboratory) | 52 days (18 Mar–9 May 2020) |
76 | Hospital / clinical laboratory (tertiary centre) and national reference laboratory l | NAAT (PCR, real-time; in-house) | [52] | Yes [48] |
| National surveillancej | Surveillance system (national; 60% of all Belgian microbiology laboratories) m | Direct test methods (different techniques)m | [53] | No | |||
| The Netherlands | Rotterdam | 99 days (16 Mar–6 Apr 2020; 15 Dec 2020–2 Mar 2021) |
74 | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; in-house) | [54] | No |
| Northern Europe | |||||||
| England | National reference laboratoryn | 72 days (14 Mar– 9 May 2020; 5 Nov–1 Dec 2020) |
102 | National reference laboratory | NAAT (multiplex PCR, real-time; in-house) | [20] | Yes [55] |
| Denmark | National surveillance | 99 days (12 Mar–13 Apr 2020; 25 Dec–1 Mar 2020) |
76 | Surveillance system (national; 5.8 million population) | NAAT (PCR, different techniques)o | [56] | No |
| Finland | Turku | 98 days (16 Mar–22 Jun 2020) |
42 | Hospital / clinical laboratory (tertiary centre) | Combination of direct and indirect test methods (different techniques)p | [57] | No |
| National surveillancej | Surveillance system (national; 5.5 million population) | Combination of direct and indirect test methods (different techniques)q | [6] | No | |||
| Norway | Trondheim | 81 days (12 Mar–1 Jun 2020) |
32 | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, real-time; in-house) | NA | No |
| Southern Europe | |||||||
| Portugal | Coimbrad | 103 days (19 Mar–2 May 2020; 15 Jan–15 Mar 2021) |
67 | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel) | bioMérieux/BioFire Diagnostics | No |
| Greece | Athens (A)d | 179 days (23 Mar–4 May 2020; 7 Nov 2020–22 Mar 2021) |
114 | Hospital / clinical laboratory (tertiary centre) | ELISA (DRG Mycoplasma pneumoniae ELISA IgM/IgG) | DRG International, Inc. | No |
| Athens (B)d | Hospital / clinical laboratory (tertiary centre) | ELISA (NovaLisa Mycoplasma pneumoniae IgM/IgG) | Novatec Immundiagnostica GmbH | No | |||
| Slovenia | Ljubljana | 46 days (19 Mar–4 May 2020) |
46 | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, real-time; Chla/Myco pneumo R-GENE) | bioMérieux/ARGENE | No |
| Asia | |||||||
| Western Asia | |||||||
| Israel | Jerusalem | 52 days (12 Mar–3 May 2020) |
139 | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; in-house) | [20] | No |
| Eastern Asia | |||||||
| Japan | Kurashiki City (Okayama)d | 0 days (no national lockdown) |
51 | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; in-house) | [58] | Yes [58] |
| Tokyo | Hospital / clinical laboratory (secondary centre) | Rapid antigen test (SAI; FUJI DRI-CHEM IMMUNO AG) | Fujifilm, Kanagawa, Japan | No | |||
| Taiwan | Taoyuand | 0 days (no national lockdown) |
0 (no official school closures) | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; in-house) | [59] | Yes [59] |
| South-eastern Asia | |||||||
| Singapore | Singapored | 55 days (7 Apr–1 Jun 2020) |
57 | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel) | bioMérieux/BioFire Diagnostics | No |
| South Asia | |||||||
| India | New Delhi | 74 days (25 Mar–7 Jun 2020) |
235 | Hospital / clinical laboratory (tertiary centre) | ELISA (NovaLisa Mycoplasma pneumoniae IgM) | Novatec Immundiagnostica GmbH | NO |
| America | |||||||
| Northern America | |||||||
| United States | Chicagod | 70 days (21 Mar–30 May 2020) |
192 | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel) | bioMérieux/BioFire Diagnostics | No |
| Caribbean | |||||||
| Cuba | National surveillance | 240 days (20 Mar–18 Jun 2020; 1 Nov 2020–end of survey period) |
121 | Surveillance system (national; 11.3 million population) | NAAT (PCR, real-time; in-house) | [60] | Yes [60] |
| Oceania | |||||||
| Australia | Darlinghurst (Sydney) | 53 days (23 Mar–15 May 2020) |
125 | Hospital / clinical laboratory (tertiary centre) | NAAT (PCR, real-time; EasyScreen Respiratory Pathogen Detection Kit) | Genetic Signatures | No |
| New Zealand | Auckland | 78 days (national: 23 Mar–13 May 2020; Auckland: 12–18 Aug 2020; 15–17 Feb 2021; 28 Feb–7 Mar 2021) |
40 | Hospital / clinical laboratory (tertiary centre) | NAAT (multiplex PCR, microarray; FilmArray Respiratory Panel)r | bioMérieux/BioFire Diagnostics | No |
CLIA: chemiluminescent immunoassay; ELISA: enzyme-linked immunosorbent assay; Ig, immunoglobulin; NA: not available; NAAT: nucleic acid amplification test; SAI: silver amplification immunochromatography; UN: United Nations.
a Stay-at-home orders for the general population (referred to as lockdown) according to an ECDC document [25] for Europe and to Wikipedia [26] for other UN regions, with adjustments made by the local participating author and considered until the end of the study period (31 March 2021).
b Full and partial school closure duration in days according to [27] until 2 March 2021 (last update before end of study period).
c More detailed information including reporting characteristics, de-duplication and exclusion criteria are provided in Supplementary Table S2.
d ≥ 90% of data are from children and adolescents < 18 years of age.
e Data from several hospitals in the region of Ticino.
f Additional use of a specific in-house PCR [52].
g From 12 October 2020 to the end of the survey period additional testing with the FilmArray Respiratory Panel (bioMérieux/BioFire Diagnostics).
h In addition to PCR also serological data separately reported.
i Multiplex PCR testing before 2020 using the Respifinder (Pathofinder), and single PCR testing over the total survey period with a specific in-house PCR, as described previously [61].
j Exclusively positive test numbers (and no total test numbers) available and/or reported.
k Data from the federal state of Saxony detected by the Landesuntersuchungsanstalt Sachsen based on combined direct and indirect test methods, but predominantly on serology (no information on isotypes) [12].
l National reference laboratory data from the two related hospitals (Antwerp, Leuven; 86–98%) and across the country (2–14%).
m Data collected through the Belgian Sentinel Network of Laboratories (SNL), a network of ca 95 microbiology laboratories (i.e. 60% of all Belgian microbiology laboratories) [53], based on direct test methods such as NAAT, antigen test, culture, microscopy, 'unknown' or 'other' (cases based on serology were excluded).
n Period of enhanced surveillance from 1 October 2019 to 30 March 2020.
o Different PCR assays, of which some are published [56] or commercial kits, but most are unpublished but validated in-house assays.
p Predominantly by serology (ca 75%; no information on isotypes), partly by multiplex PCR (Allplex Respiratory Panel, Seegene Inc.; ca 25%).
q Predominantly by PCR.
r Additional use of an in-house multiplex PCR (www.labplus.co.nz).
Entries in bold signify national and/or regional surveillances.
Stay-at-home order and school closure periods
Periods of stay-at-home orders for the general population (referred to as lockdowns) in Europe were obtained from the Response Measures Database (RMD) of the European Centre for Disease Prevention and Control (ECDC) [25] and those in other UN regions from a collection of pandemic lockdown dates in Wikipedia [26], with adjustments made by the participants. The total duration in days until the end of the study period was calculated for each site. School closure duration in days (full and partial closure in total) was determined according to the United Nations Children’s Fund (UNICEF) global school closures database until 2 March 2021 (last update before the end of the study period) [27].
Statistical analysis
Incidence was defined as the number of new cases over a specified period of time within a community [28]. Given the missing population denominators we were not able to report incidence rates. We compared M. pneumoniae detections between April 2020 and March 2021 with total numbers observed from April 2017 to March 2020. Fisher's exact test was used to compare proportions with corrections for multiple testing. Spearman rank correlation coefficient (R, rho) was used for analyses of correlation. All reported p values are two-tailed with statistical significance defined as p < 0.05. Data were analysed using R software (version 4.0.5) [29].
Results
Survey entries and detection methods
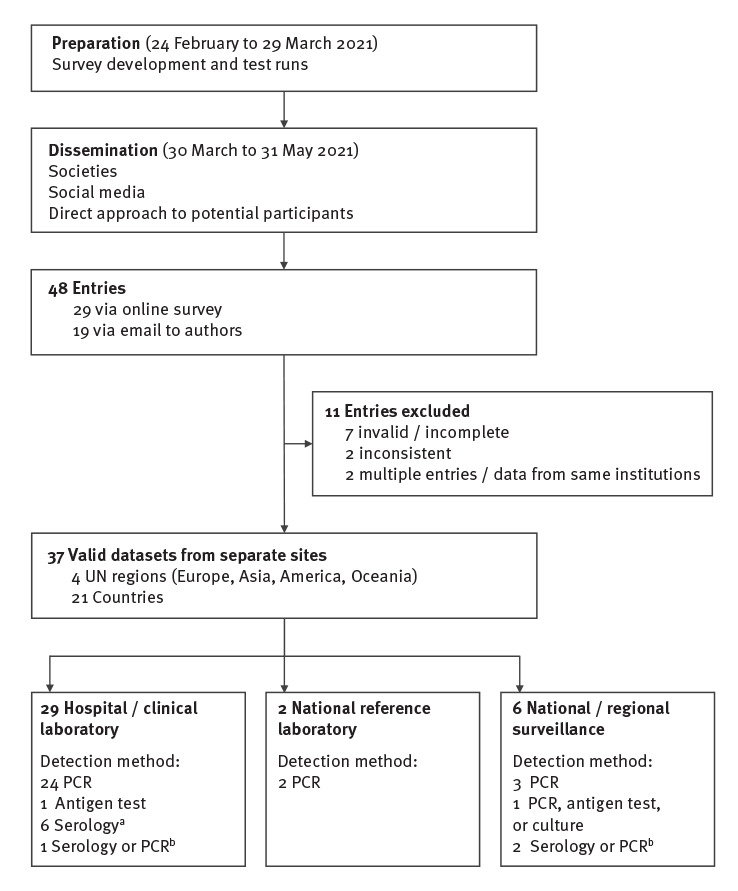
We received entries from 48 sites, of which 29 were entered via the online survey and 19 via email to authors. Of the 12 experts collating laboratory detections of M. pneumoniae in Europe and Israel for the ESGMAC in a previous study (January 2011–April 2016) [14], eight provided information for this survey. An overall response rate could not be calculated because the survey was widely disseminated through societies, social media and further dissemination among participants themselves. We excluded 11 entries because of invalid or incomplete data (n = 7), inconsistent data (n = 2; positive test numbers by month did not match with total numbers per year) or double reporting (n = 2; congruent data from same institutions). Thus, 37 valid datasets from separate sites in 21 countries from four UN regions were eligible for inclusion (Europe: n = 12; Asia: n = 5; America: n = 2; Oceania: n = 2), 29 from hospital laboratories, two from national reference laboratories and six from national and/or regional surveillance systems (Figure 1).
Figure 1.
Study profile, global survey of Mycoplasma pneumoniae detections, April 2017–March 2021
UN: United Nations.
a Three sites provided serological data in addition to PCR.
b No distinction possible between detection methods, but predominantly serological data included.
Demographic characteristics and laboratory information of participating sites are shown in Table 1. The detection method varied between sites: 29 (78.38%) sites reported exclusively PCR (n = 17 multiplex); three sites used exclusively serology (enzyme-linked immunosorbent assay (ELISA)), three sites reported combined PCR and serology (no distinction possible between detection methods, but predominantly serology), one site used a combination of direct test methods (i.e. PCR, antigen test or culture) and one site used exclusively rapid antigen testing. Three sites reported only the number of positive tests over the entire study period (Saxony (Germany) and national surveillance systems of Belgium and Finland), and another three sites provided serological data in addition to PCR.
Detections before and after the introduction of non-pharmaceutical interventions
A total of 631,104 tests were performed during the study period from April 2017–March 2021 (three sites did not have data about total test numbers available). Overall, 30,617 M. pneumoniae detections were confirmed from participating sites. Among those with available information on age/sex, 54.92% (n = 11,029/20,081) were reported in children/adolescents younger than 18 years of age and 52.90% (n = 12,794/24,184) in females. The greatest number of positive tests were obtained with direct test methods (n = 19,102; 62.39%; predominantly PCR) followed by a combination of PCR and serology (n = 10,483; 34.24%; no information on isotypes) or serology alone (n = 1,032; 3.37%; only IgM was considered if all isotypes were reported). Information about convalescent samples for serological testing was not available. No routine testing for a fourfold increase in IgG levels was reported. De-duplication data were determined at site level (Supplementary Table S2 lists the reporting characteristics per site).
There was a significant reduction of M. pneumoniae detections after the introduction of NPIs (Figure 2). Among total detections, 1,714 (5.60%) derived from April 2020 to March 2021 compared with 28,903 (94.40%) from April 2017 to March 2020 (Table 2). Mycoplasma pneumoniae testing and detection in children/adolescents and females per year is shown in Table 3. The annual proportion of children/adolescents and females with detections before and during the COVID-19 pandemic was 55.16% vs 49.77% (p < 0.01) and 53.01% vs 50.86% (p = 0.15), respectively. Detailed graphs for each site and country are shown in Supplementary Figures S1–S6. The difference in detections before and during the COVID-19 pandemic was more obvious for direct test methods (Figure 2A) than indirect test methods (Figure 2B). This is supported by a direct comparison of detections with PCR and single-sample serology (IgM, IgG and IgA) from the three sites that reported data separately for each method, which did not show any correlation between those two test methods (Figure 3).
Figure 2.
Global detection of Mycoplasma pneumoniae, April 2017–March 2021 (n = 30,617)
Ig: immunoglobulin.
Data from combined serology and PCR tests are shown under indirect test methods (no distinction possible between detection methods, but predominantly serology; Table 1). For serology, only total test numbers of IgM considered. The grey backgrounds indicate the presence of non-pharmaceutical interventions during the COVID-19 pandemic. Detailed graphs separately for each site and country with corresponding local lockdown periods are shown in Supplementary Figures S1–S6.

Table 2. Mycoplasma pneumoniae testing and detection rates per year, April 2017–March 2021 (n = 631,104).
| UN region and country | City or region | Test method | April 2017–March 2018 | April 2018–March 2019 | April 2019–March 2020 | April 2020–March 2021 (COVID-19 pandemic) |
Difference in detection rate (%) pre-pandemic vs COVID-19 pandemica |
Pb | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total tests (N) |
Positive tests (n) |
Detection rate (%) |
Total tests (N) |
Positive tests (n) |
Detection rate (%) |
Total tests (N) |
Positive tests (n) |
Detection rate (%) |
Total tests (N) |
Positive test (n) |
Detection rate (%) |
|||||
| Europe | ||||||||||||||||
| Western Europe | ||||||||||||||||
| France | Bordeaux | PCR | 619 | 16 | 2.58 | 625 | 22 | 3.52 | 530 | 41 | 7.74 | 466 | 4 | 0.86 | –80.72 | <0.01 |
| Switzerland | Geneva | PCR | 1,347 | 30 | 2.23 | 1,622 | 76 | 4.69 | 2,119 | 76 | 3.59 | 1,193 | 7 | 0.59 | –83.60 | <0.01 |
| Lausanne | PCR | 388 | 6 | 1.55 | 406 | 4 | 0.99 | 592 | 20 | 3.38 | 246 | 0 | 0.00 | –100.00 | 0.02 | |
| Bernc | PCR | 134 | 17 | 12.69 | 175 | 43 | 24.57 | 191 | 29 | 15.18 | 41 | 0 | 0.00 | –100.00 | <0.01 | |
| Lucernec | PCR | NA | 7 | NA | 229 | 10 | 4.37 | 215 | 21 | 9.77 | 129 | 1 | 0.78 | –88.90 | <0.01 | |
| Bellinzona | PCR | 701 | 10 | 1.43 | 1,104 | 76 | 6.88 | 1,540 | 43 | 2.79 | 804 | 0 | 0.00 | –100.00 | <0.01 | |
| Zurich (A) | PCR | 1,067 | 17 | 1.59 | 1,361 | 41 | 3.01 | 1,620 | 50 | 3.09 | 1,823 | 11 | 0.60 | –77.38 | <0.01 | |
| Zurich (B)c | PCR | 104 | 21 | 20.19 | 123 | 22 | 17.89 | 201 | 54 | 26.87 | 1,659 | 6 | 0.36 | –98.40 | <0.01 | |
| St. Gallenc | PCR | 20 | 7 | 35.00 | 18 | 5 | 27.78 | 19 | 6 | 31.58 | 8 | 1 | 12.50 | –60.42 | 0.42 | |
| Aarau | PCR | 1,431 | 36 | 2.52 | 1,586 | 55 | 3.47 | 1,955 | 77 | 3.94 | 1,601 | 10 | 0.62 | –81.51 | <0.01 | |
| IgM ELISA | 220 | 14 | 6.36 | 229 | 19 | 8.30 | 191 | 23 | 12.04 | 183 | 13 | 7.10 | –18.81 | 0.55 | ||
| IgG ELISA | 220 | 43 | 19.55 | 229 | 50 | 21.83 | 191 | 48 | 25.13 | 183 | 46 | 25.14 | + 14.10 | 0.37 | ||
| Basel (A) | PCR | 1,535 | 9 | 0.59 | 2,212 | 12 | 0.54 | 5,028 | 53 | 1.05 | 3,061 | 2 | 0.07 | –92.25 | <0.01 | |
| Basel (B)c | PCR | 870 | 10 | 1.15 | 845 | 6 | 0.71 | 1,050 | 19 | 1.81 | 634 | 6 | 0.95 | –25.24 | 0.69 | |
| Germany | Homburg | PCR | 2,321 | 10 | 0.43 | 2,395 | 19 | 0.79 | 2,773 | 17 | 0.61 | 2,570 | 1 | 0.04 | –93.67 | <0.01 |
| IgM ELISA | 486 | 67 | 13.79 | 492 | 70 | 14.23 | 544 | 71 | 13.05 | 588 | 70 | 11.90 | –12.89 | 0.31 | ||
| IgG ELISA | 486 | 277 | 57.00 | 492 | 291 | 59.15 | 544 | 341 | 62.68 | 588 | 331 | 56.29 | –5.75 | 0.15 | ||
| Düsseldorf | PCR | 1,515 | 27 | 1.78 | 1,530 | 18 | 1.18 | 1,283 | 16 | 1.25 | 1,011 | 12 | 1.19 | –15.79 | 0.65 | |
| IgM ELISA | 398 | 18 | 4.52 | 446 | 78 | 17.49 | 585 | 148 | 25.30 | 538 | 134 | 24.91 | + 45.87 | <0.01 | ||
| IgG ELISA | 530 | 298 | 56.23 | 491 | 288 | 58.66 | 561 | 307 | 54.72 | 522 | 315 | 60.34 | + 6.90 | 0.13 | ||
| IgA ELISAd | NA | NA | NA | 241 | 95 | 39.42 | 560 | 195 | 34.82 | 521 | 142 | 27.26 | –24.72 | <0.01 | ||
| Saxony | PCR or serologye | NA | 2,013 | NA | NA | 1,044 | NA | NA | 927 | NA | NA | 303 | NA | NA | NA | |
| Belgium | Antwerp, Leuven (national reference laboratory) | PCR | 2,698 | 30 | 1.11 | 1,150 | 15 | 1.30 | 1220 | 32 | 2.62 | 864 | 3 | 0.35 | –77.15 | <0.01 |
| National surveillance | Direct test methods (different techniques) | NA | 1,151 | NA | NA | 548 | NA | NA | 833 | NA | NA | 230 | NA | NA | NA | |
| The Netherlands | Rotterdam | PCR | NA | NA | NA | 240 | 36 | 15.00 | 407 | 56 | 13.76 | 444 | 36 | 8.11 | –42.98 | <0.01 |
| Northern Europe | ||||||||||||||||
| England | National reference laboratoryf | PCR | 138 | 19 | 13.77 | 110 | 11 | 10.00 | 263 | 118 | 44.87 | 155 | 10 | 6.45 | –77.72 | <0.01 |
| Denmark | National surveillance | PCR | 100,257 | 5,303 | 5.29 | 80,965 | 1,371 | 1.69 | 100,879 | 4,383 | 4.34 | 58,716 | 177 | 0.30 | –92.31 | < 0.01 |
| Finland | Turku | PCR or serologye | NA | NA | NA | NA | NA | NA | 5,413 | 211 | 3.90 | 3,462 | 70 | 2.02 | –48.13 | <0.01 |
| National surveillance | PCR or serologye | NA | 2,420 | NA | NA | 1,728 | NA | NA | 1,312 | NA | NA | 455 | NA | NA | NA | |
| Norway | Trondheim | PCR | 3,306 | 230 | 6.96 | 2,330 | 56 | 2.40 | 2,014 | 48 | 2.38 | 1,263 | 0 | 0.00 | –100.00 | <0.01 |
| Southern Europe | ||||||||||||||||
| Portugal | Coimbrac | PCR | 803 | 5 | 0.62 | 924 | 90 | 9.74 | 1,084 | 19 | 1.75 | 161 | 0 | 0.00 | –100.00 | <0.01 |
| Greece | Athens (A)c | IgM ELISA | 212 | 19 | 8.96 | 236 | 51 | 21.61 | 250 | 65 | 26.00 | 167 | 35 | 20.96 | + 8.36 | 0.66 |
| IgG ELISA | 212 | 44 | 20.75 | 236 | 29 | 12.29 | 250 | 37 | 14.80 | 167 | 41 | 24.55 | + 55.79 | <0.01 | ||
| Athens (B)c | IgM ELISA | 185 | 9 | 4.86 | 181 | 15 | 8.29 | 231 | 27 | 11.69 | 172 | 14 | 8.14 | –4.72 | 1.00 | |
| IgG ELISA | 185 | 59 | 31.89 | 181 | 88 | 48.62 | 231 | 92 | 39.83 | 172 | 44 | 25.58 | –36.10 | <0.01 | ||
| Slovenia | Ljubljana | PCR | 1,604 | 22 | 1.37 | 1,887 | 153 | 8.11 | 2,639 | 495 | 18.76 | 1,241 | 20 | 1.61 | –85.26 | <0.01 |
| Asia | ||||||||||||||||
| Western Asia | ||||||||||||||||
| Israel | Jerusalem | PCR | 1,364 | 45 | 3.30 | 1,299 | 62 | 4.77 | 1,637 | 53 | 3.24 | 666 | 0 | 0.00 | –100.00 | <0.01 |
| Eastern Asia | ||||||||||||||||
| Japan | Kurashiki City (Okayama)c | PCR | 30 | 4 | 13.33 | 64 | 14 | 21.88 | 34 | 3 | 8.82 | 5 | 0 | 0.00 | –100.00 | 1.00 |
| Tokyof | Rapid antigen test | 346 | 56 | 16.18 | 140 | 36 | 25.71 | 600 | 36 | 6.00 | 120 | 4 | 3.33 | –71.72 | <0.01 | |
| Taiwan | Taoyuanc | PCR | 116 | 20 | 17.24 | 159 | 63 | 39.62 | 204 | 131 | 64.22 | 44 | 5 | 11.36 | –74.56 | <0.01 |
| South-eastern Asia | ||||||||||||||||
| Singapore | Singaporec | PCR | 4,212 | 387 | 9.19 | 8,765 | 307 | 3.50 | 15,860 | 613 | 3.87 | 8,835 | 33 | 0.37 | –91.76 | <0.01 |
| South Asia | ||||||||||||||||
| India | New Delhi | IgM ELISA | 245 | 19 | 7.76 | 320 | 18 | 5.63 | 205 | 19 | 9.27 | 153 | 16 | 10.46 | + 43.79 | 0.19 |
| America | ||||||||||||||||
| Northern America | ||||||||||||||||
| United States | Chicagoc | PCR | 4,221 | 10 | 0.24 | 4,199 | 25 | 0.60 | 4,990 | 42 | 0.84 | 1,695 | 2 | 0.12 | –79.45 | 0.01 |
| Caribbean | ||||||||||||||||
| Cuba | National surveillance | PCR | 902 | 18 | 2.00 | 62 | 4 | 6.45 | 844 | 20 | 2.37 | 4 | 0 | 0.00 | –100.00 | 1.00 |
| Oceania | ||||||||||||||||
| Australia | Darlinghurst (Sydney) | PCR | 15,751 | 60 | 0.38 | 12,187 | 55 | 0.45 | 21,086 | 168 | 0.80 | 70,807 | 19 | 0.03 | –95.35 | <0.01 |
| New Zealand | Auckland | PCR | 543 | 21 | 3.87 | 993 | 26 | 2.62 | 858 | 41 | 4.78 | 2,723 | 4 | 0.15 | –96.00 | <0.01 |
| Total (global, participating countries)g | Direct test methods (PCR or rapid antigen test considered only) | 148,343 | 6,453 | 4.35 | 129,705 | 2,733 | 2.11 | 173,735 | 6,780 | 3.90 | 162,989 | 374 | 0.23 | –93.51 | <0.01 | |
| Indirect test methods (IgM considered only) | 1,746 | 146 | 8.36 | 1,904 | 251 | 13.18 | 2,006 | 353 | 17.60 | 1,801 | 282 | 15.66 | + 18.08 | 0.01 | ||
COVID-19: coronavirus disease; ELISA: enzyme-linked immunosorbent assay; Ig: immunoglobulin; NA: not available; UN: United Nations.
a Difference in detection rate between April 2017 and March 2020 (mean positive/total tests across the 3 years) and between April 2020 and March 2021 (absolute number positive/total tests). Percentages showing a reduction in detection rate are indicated in bold.
b Proportions of positive/total tests from April 2020 to March 2021 were compared with total numbers from April 2017 to March 2020 by Fisher's exact test. p values < 0.05 are indicated in bold.
c ≥ 90% of data are from children and adolescents < 18 years of age.
d IgA ELISA introduced in November 2018.
e Data from combined serology and PCR tests (no distinction possible between detection methods; Table 1).
f Period of enhanced surveillance from 1 October 2019 to 30 March 2020.
g These numbers include only data from PCR or rapid antigen test (for direct test methods) and IgM serology (for indirect test methods).
Entries in italics signify serological data (± PCR).
Table 3. Mycloplasma pneumoniae testing and detection in children/adolescents and females per year, April 2017–March 2021 (n = 154,241 children/adolescents and 285,238 females).
| UN region and country | City or region | Test method | April 2017–March 2018 | April 2018–March 2019 | April 2019–March 2020 | April 2020–March 2021 (COVID-19 pandemic) |
||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Children/ adolescents |
Females | Children/ adolescents |
Females | Children/ adolescents |
Females | Children/ adolescents |
Females | |||||||||||||||||||
| N | n | % | N | n | % | N | n | % | N | n | % | N | n | % | N | n | % | N | n | % | N | n | % | |||
| Europe | ||||||||||||||||||||||||||
| Western Europe | ||||||||||||||||||||||||||
| France | Bordeaux | PCR | 335 | 9 | 2.69 | 236 | 11 | 4.66 | 282 | 15 | 5.32 | 280 | 11 | 3.93 | 272 | 28 | 10.29 | 248 | 17 | 6.85 | 220 | 2 | 0.91 | 193 | 0 | 0.00 |
| Switzerland | Geneva | PCR | 201 | 8 | 3.98 | 579 | 17 | 2.94 | 301 | 43 | 14.29 | 704 | 39 | 5.54 | 354 | 45 | 12.71 | 392 | 34 | 8.67 | 161 | 2 | 1.24 | 449 | 3 | 0.67 |
| Lausanne | PCR | 42 | 1 | 2.38 | 226 | 5 | 2.21 | 18 | 1 | 5.56 | 200 | 1 | 0.50 | 36 | 4 | 11.11 | 325 | 9 | 2.77 | 2 | 0 | 0.00 | 123 | 0 | 0.00 | |
| Berna | PCR | 134 | 17 | 12.69 | 65 | 8 | 12.31 | 175 | 43 | 24.57 | 74 | 18 | 24.32 | 191 | 29 | 15.18 | 78 | 14 | 17.95 | 41 | 0 | 0.00 | 16 | 0 | 0.00 | |
| Lucernea | PCR | NA | 7 | NA | NA | 3 | NA | 229 | 10 | 4.37 | NA | 3 | NA | 215 | 21 | 9.77 | NA | 5 | NA | 129 | 1 | 0.78 | NA | 1 | NA | |
| Bellinzona | PCR | 155 | 6 | 3.87 | 315 | 2 | 0.63 | 471 | 66 | 14.01 | 500 | 41 | 8.20 | 354 | 22 | 6.21 | 661 | 19 | 2.87 | 118 | 0 | 0.00 | 328 | 0 | 0.00 | |
| Zurich (A) | PCR | 29 | 2 | 6.90 | NA | 43 | 6 | 13.95 | NA | 44 | 8 | 18.18 | NA | 35 | 1 | 2.86 | NA | |||||||||
| Zurich (B)a | PCR | 104 | 21 | 20.19 | NA | 123 | 22 | 17.89 | NA | 201 | 54 | 26.87 | NA | 1,659 | 6 | 0.36 | NA | |||||||||
| St. Gallena | PCR | 20 | 7 | 35.00 | 14 | 4 | 28.57 | 18 | 5 | 27.78 | 12 | 5 | 41.67 | 19 | 6 | 31.58 | 7 | 3 | 42.86 | 8 | 1 | 12.50 | 4 | 1 | 25.00 | |
| Aarau | PCR | 441 | 13 | 2.95 | 603 | 14 | 2.32 | 392 | 22 | 5.61 | 723 | 24 | 3.32 | 484 | 26 | 5.37 | 891 | 38 | 4.26 | 287 | 4 | 1.39 | 658 | 6 | 0.91 | |
| IgM ELISA | 25 | 4 | 16.00 | 91 | 10 | 10.99 | 20 | 8 | 40.00 | 99 | 7 | 7.07 | 33 | 8 | 24.24 | 77 | 10 | 12.99 | 16 | 3 | 18.75 | 69 | 9 | 13.04 | ||
| IgG ELISA | 25 | 3 | 12.00 | 91 | 15 | 16.48 | 20 | 6 | 30.00 | 99 | 19 | 19.19 | 33 | 9 | 27.27 | 77 | 15 | 19.48 | 16 | 1 b | 6.25 | 69 | 18 | 26.09 | ||
| Basel (A) | PCR | 4 | 0 | 0.00 | 644 | 6 | 0.93 | 5 | 0 | 0.00 | 937 | 7 | 0.75 | 9 | 0 | 0.00 | 2,201 | 25 | 1.14 | 1 | 0 | 0.00 | 1,251 | 2 | 0.16 | |
| Basel (B)a | PCR | 863 | 10 | 1.16 | 404 | 5 | 1.24 | 845 | 6 | 0.71 | NA | 1 | NA | 1,050 | 19 | 1.81 | NA | NA | NA | 634 | 6 | 0.95 | NA | NA | NA | |
| Germany | Homburg | PCR | 53 | 2 | 3.77 | NA | 4 | NA | 75 | 3 | 4.00 | NA | 8 | NA | 111 | 4 | 3.60 | NA | 7 | NA | 88 | 0 | 0.00 | NA | 1 | NA |
| IgM ELISA | NA | NA | NA | NA | NA | NA | NA | NA | ||||||||||||||||||
| IgG ELISA | NA | NA | NA | NA | NA | NA | NA | NA | ||||||||||||||||||
| Düsseldorf | PCR | 1,003 | 21 | 2.09 | 618 | 10 | 1.62 | 1,026 | 16 | 1.56 | 649 | 5 | 0.77 | 882 | 15 | 1.70 | 523 | 6 | 1.15 | 621 | 10 | 1.61 | 471 | 4 | 0.85 | |
| IgM ELISA | 264 | 12 | 4.55 | 179 | 9 | 5.03 | 246 | 36 | 14.63 | 173 | 24 | 13.87 | 246 | 52 | 21.14 | 182 | 37 | 20.33 | 253 | 47 | 18.58 | 161 | 29 | 18.01 | ||
| IgG ELISA | 307 | 168 | 54.72 | 237 | 142 | 59.92 | 255 | 141 | 55.29 | 187 | 118 | 63.10 | 226 | 98 | 43.36 | 174 | 96 | 55.17 | 238 | 132 | 55.46 | 157 | 103b | 65.61 | ||
| IgA ELISA | NA | NA | 120 | 36 | 30.00 | 80 | 26 | 32.50 | 226 | 37 | 16.37 | 174 | 46 | 26.44 | 237 | 17b | 7.17 | 156 | 24 | 15.38 | ||||||
| Saxony | PCR or serology | NA | NA | NA | NA | NA | NA | NA | NA | |||||||||||||||||
| Belgium | Antwerp, Leuven (national reference laboratory) | PCR | 748 | 16 | 2.14 | 1,132 | 17 | 1.50 | 208 | 4 | 1.92 | 486 | 9 | 1.85 | 240 | 15 | 6.25 | 510 | 17 | 3.33 | 100 | 2 | 2.00 | 356 | 0 | 0.00 |
| National surveillance | Direct test methods (different techniques) | NA | 740 | NA | NA | 639 | NA | NA | 362 | NA | NA | 285 | NA | NA | 493 | NA | NA | 433 | NA | NA | 86b | NA | NA | 140b | NA | |
| The Netherlands | Rotterdam | PCR | NA | NA | 47 | 11 | 23.40 | 119 | 22 | 18.49 | 89 | 26 | 29.21 | 163 | 23 | 14.11 | 54 | 12 | 22.22 | 176 | 19 | 10.80 | ||||
| Northern Europe | ||||||||||||||||||||||||||
| England | National reference laboratory | PCR | 39 | 8 | 20.51 | 63 | 7 | 11.11 | 34 | 2 | 5.88 | 45 | 9 | 20.00 | 84 | 51 | 60.71 | 102 | 50 | 49.02 | 58 | 7 | 12.07 | 49 | 5 | 10.20 |
| Denmark | National surveillance | PCR | 15,879 | 2,374 | 14.95 | 55,874 | 2,843 | 5.09 | 9,121 | 515 | 5.65 | 44,132 | 768 | 1.74 | 14,307 | 1,854 | 12.96 | 55,356 | 2,374 | 4.29 | 2,650 | 68 | 2.57 | 27,693 | 83 | 0.30 |
| Finland | Turku | PCR or serology | NA | NA | NA | NA | 1,488 | 138 | 9.27 | NA | 804 | 51 | 6.34 | NA | ||||||||||||
| National surveillance | PCR or serology | NA | NA | 1,344 | NA | NA | NA | 997 | NA | NA | NA | 699 | NA | NA | NA | 265 | NA | |||||||||
| Norway | Trondheim | PCR | 3,306 | 230 | 6.96 | 1,556 | 113 | 7.26 | 2,330 | 56 | 2.40 | 1,041 | 26 | 2.50 | 2,014 | 48 | 2.38 | 920 | 22 | 2.39 | 1,263 | 0 | 0.00 | 486 | 0 | 0.00 |
| Southern Europe | ||||||||||||||||||||||||||
| Portugal | Coimbraa | PCR | 803 | 5 | 0.62 | 374 | 4 | 1.07 | 924 | 90 | 9.74 | 460 | 38 | 8.26 | 1,084 | 19 | 1.75 | 469 | 8 | 1.71 | 161 | 0 | 0.00 | 69 | 0 | 0.00 |
| Greece | Athens (A)a | IgM ELISA | 212 | 19 | 8.96 | 92 | 9 | 9.78 | 236 | 51 | 21.61 | 125 | 32 | 25.60 | 250 | 65 | 26.00 | 118 | 28 | 23.73 | 167 | 35 | 20.96 | 73 | 15 | 20.55 |
| IgG ELISA | 212 | 44 | 20.75 | 92 | 19 | 20.65 | 236 | 29 | 12.29 | 125 | 13 | 10.40 | 250 | 37 | 14.80 | 118 | 16 | 13.56 | 167 | 41 | 24.55 | 73 | 19 | 26.03 | ||
| Athens (B)a | IgM ELISA | 185 | 9 | 4.86 | 90 | 3 | 3.33 | 181 | 15 | 8.29 | 87 | 6 | 6.90 | 231 | 27 | 11.69 | 106 | 14 | 13.21 | 172 | 14 | 8.14 | 90 | 8 | 8.89 | |
| IgG ELISA | 185 | 59 | 31.89 | 90 | 25 | 27.78 | 181 | 88 | 48.62 | 87 | 46 | 52.87 | 231 | 92 | 39.83 | 106 | 46 | 43.40 | 172 | 44 | 25.58 | 90 | 20 | 22.22 | ||
| Slovenia | Ljubljana | PCR | 530 | 19 | 3.58 | 708 | 7 | 0.99 | 745 | 119 | 15.97 | 857 | 75 | 8.75 | 1,326 | 402 | 30.32 | 1,382 | 218 | 15.77 | 320 | 14 | 4.38 | 528 | 8 | 1.52 |
| Asia | ||||||||||||||||||||||||||
| Western Asia | ||||||||||||||||||||||||||
| Israel | Jerusalem | PCR | 256 | 17 | 6.64 | 573 | 19 | 3.32 | 337 | 39 | 11.57 | 610 | 33 | 5.41 | 364 | 29 | 7.97 | 760 | 25 | 3.29 | 216 | 0 | 0.00 | 275 | 0 | 0.00 |
| Eastern Asia | ||||||||||||||||||||||||||
| Japan | Kurashiki City (Okayama)a | PCR | 30 | 4 | 13.33 | 16 | 2 | 12.50 | 64 | 14 | 21.88 | 26 | 5 | 19.23 | 34 | 3 | 8.82 | 15 | 1 | 6.67 | 5 | 0 | 0.00 | 5 | 0 | 0.00 |
| Tokyo | Rapid antigen test | 25 | NA | NA | 52 | 33 | 63.46 | 80 | 25 | 31.25 | 60 | 9 | 15.00 | 420 | 22 | 5.24 | 180 | 14 | 7.78 | 60 | 3 | 5.00 | 60 | 1 | 1.67 | |
| Taiwan | Taoyuana | PCR | 116 | 20 | 17.24 | 56 | 11 | 19.64 | 159 | 63 | 39.62 | 77 | 31 | 40.26 | 204 | 131 | 64.22 | 113 | 71 | 62.83 | 44 | 5 | 11.36 | 16 | 0b | 0.00 |
| South-eastern Asia | ||||||||||||||||||||||||||
| Singapore | Singaporea | PCR | 4,212 | 387 | 9.19 | NA | 8,765 | 307 | 3.50 | NA | 15,860 | 613 | 3.87 | NA | 8,835 | 33 | 0.37 | NA | ||||||||
| South Asia | ||||||||||||||||||||||||||
| India | New Delhi | IgM ELISA | 159 | 12 | 7.55 | 30 | 7 | 23.33 | 207 | 7 | 3.38 | 105 | 8 | 7.62 | 113 | 14 | 12.39 | 67 | 7 | 10.45 | 84 | 13 | 15.48 | 49 | 5 | 10.20 |
| America | ||||||||||||||||||||||||||
| Northern America | ||||||||||||||||||||||||||
| United States | Chicagoa | PCR | 3,818 | 10 | 0.26 | 1,892 | 3 | 0.16 | 3,873 | 21 | 0.54 | 1,814 | 15 | 0.83 | 4,653 | 39 | 0.84 | 2,258 | 21 | 0.93 | 1,589 | 2 | 0.13 | 735 | 0 | 0.00 |
| Caribbean | ||||||||||||||||||||||||||
| Cuba | National surveillance | PCR | 535 | 12 | 2.24 | 398 | 6 | 1.51 | 38 | 1 | 2.63 | 25 | 0 | 0.00 | 497 | 15 | 3.02 | 385 | 6 | 1.56 | 0 | NA | NA | 0 | NA | NA |
| Oceania | ||||||||||||||||||||||||||
| Australia | Darlinghurst (Sydney) |
PCR | 3,975 | 35 | 0.88 | 8,303 | 36 | 0.43 | 3,050 | 30 | 0.98 | 6,241 | 22 | 0.35 | 4,784 | 111 | 2.32 | 11,242 | 82 | 0.73 | 9,487 | 10 | 0.11 | 36,408 | 10 | 0.03 |
| New Zealand | Auckland | PCR | 154 | 11 | 7.14 | 252 | 10 | 3.97 | 167 | 8 | 4.79 | 475 | 13 | 2.74 | 226 | 22 | 9.73 | 401 | 21 | 5.24 | 561 | 3 | 0.53 | 1,219 | 3 | 0.25 |
COVID-19: coronavirus disease; ELISA: enzyme-linked immunosorbent assay; Ig: immunoglobulin; NA: not available; UN: United Nations.
a ≥ 90% of data are from children and adolescents < 18 years of age.
b Statistically significant difference in proportions of children/adolescents or females with positive tests between April 2020 and March 2021 and between April 2017 and March 2020 (Fisher's exact test, p < 0.05).
For serology only total test numbers of IgM considered. Entries in italics signify serological data (± PCR).
Figure 3.
Detection of Mycoplasma pneumoniae at sites that provided single-sample serological data in addition to PCR, April 2017–March 2021 (n = 14,702a)
a For serology only total test numbers of IgM considered.
Grey backgrounds indicate local stay-at-home order (lockdown) periods. Another site from Germany (Homburg) did also provide PCR and serological data separately but numbers by month were not available.

Following the introduction of NPIs, the M. pneumoniae incidence by direct test methods decreased significantly from 8.61% ± 10.62 (mean of incidences from each site ± standard deviation) during April 2017 to March 2020 to 1.69% ± 3.30 in April 2020 to March 2021 (p < 0.01). The detection rates decreased with direct but not with indirect test methods (−93.51% vs +18.08%; p < 0.01) (Table 2). Although 27 sites reported also a reduction in total number of tests (–44.52% ± 24.61) in April 2020 to March 2021, seven sites showed an increase in total test numbers during the COVID-19 pandemic (because SARS-CoV-2 PCR was included in a multiplex panel that also contained M. pneumoniae PCR) (Table 2). In the year before the introduction of NPIs (April 2019 to March 2020), direct M. pneumoniae detections were significantly increased in several countries across UN regions compared with the period April 2018 to March 2019, which was indicative of an M. pneumoniae epidemic (Figure 2A).
Total duration of lockdown (82.80 days ± 55.73; range: 0–240) and school closure periods (84.05 days ± 56.33; range: 0–235) varied widely across countries. There was no correlation of the duration of lockdown or school closure periods with direct M. pneumoniae detection rates from April 2020 to March 2021. Several sites reported a longer duration of lockdown than school closure periods, which suggested that children returned to schools while lockdown continued for some time (Table 1). The re-opening of schools had no observable impact on the incidence of M. pneumoniae as direct detections remained remarkably low throughout the period April 2020 to March 2021. Detections were very low or absent even in countries where no school closures or official lockdowns were enforced (e.g. Japan, Taiwan; see Supplementary Figure S3 for M. pneumoniae detections in Asia).
Macrolide resistance
As a consequence of the significant decrease in M. pneumoniae detections after the introduction of NPIs, only few cases were investigated for macrolide resistance. In total, seven sites from Europe, Asia and America reported MRMp rates from April 2017 to March 2021 (Table 4). Macrolide resistance determination was reported as part of national surveillance of positive samples (Japan, Cuba) or only on positive samples identified at the reference laboratory and/or upon physician request. The MRMp detections among investigated cases are shown as absolute numbers in Figure 4A and as percentages in Figure 4B. The highest MRMp rate was found in Taiwan from April 2018 to March 2019 with 42 of 53 isolates. The national surveillance from Japan contributed the greatest number of strains investigated for macrolide resistance. Overall, MRMp was detected in one of 22 investigated cases from April 2020 to March 2021 and in 176 of 762 (23.10%) from April 2017 to March 2020 (p = 0.04).
Table 4. Macrolide-resistant Mycoplasma pneumoniae testing and detection rates per year, April 2017–March 2021 (n = 784).
| UN region and country | City or region | Macrolide resistance determination (reference) | April 2017–March 2018 | April 2018–March 2019 | April 2019–March 2020 | April 2020–March 2021 (COVID-19 pandemic) |
Difference in detection rate (%) pre-pandemic vs COVID-19 pandemica |
P b | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total tests (N) | Positive tests (n) | Detection rate (%) | Total tests (N) | Positive tests (n) | Detection rate (%) | Total tests (N) | Positive tests (n) | Detection rate (%) | Total tests (N) | Positive tests (n) | Detection rate (%) | |||||
| Europe | ||||||||||||||||
| Western Europe | ||||||||||||||||
| France | Bordeaux | [48] | 10 | 0 | 0.00 | 15 | 2 | 13.33 | 30 | 3 | 10.00 | 3 | 0 | 0.00 | –100.00 | 1.00 |
| Switzerland | Zurich (A + Bc)d | [50] | 0 | NA | NA | 2 | 2 | 100.00 | 10 | 7 | 70.00 | 3 | 1 | 33.33 | –55.56 | 0.24 |
| Belgium | Antwerp, Leuven (national reference laboratory) | [48] | 26 | 1 | 3.85 | 15 | 0 | 0.00 | 30 | 0 | 0.00 | 2 | 0 | 0.00 | –100.00 | 1.00 |
| England | National reference laboratorye | [55] | 19 | 3 | 15.79 | 11 | 0 | 0.00 | 104 | 1 | 0.96 | 6 | 0 | 0.00 | –100.00 | 1.00 |
| Asia | ||||||||||||||||
| Eastern Asia | ||||||||||||||||
| Japan | National surveillance | [58] | 103 | 20 | 19.42 | 97 | 5 | 5.15 | 124 | 18 | 14.52 | 8 | 0 | 0.00 | –100.00 | 0.60 |
| Taiwan | Taoyuan c | [59] | 10 | 6 | 60.00 | 53 | 42 | 79.25 | 80 | 62 | 77.50 | 0 | NA | NA | NA | NA |
| America | ||||||||||||||||
| Caribbean | ||||||||||||||||
| Cuba | National surveillance | [60] | 14 | 2 | 14.29 | 0 | NA | NA | 9 | 2 | 22.22 | 0 | NA | NA | NA | NA |
COVID-19: coronavirus disease; SD: standard deviation; MRMp: macrolide-resistant Mycoplasma pneumoniae; NA: not applicable; UN: United Nations.
a Difference in detection rate between April 2017 and March 2020 (mean positive/total tests across the 3 years) and April 2020 and March 2021 (absolute number positive/total tests). Percentages showing a reduction in detection rate are indicated in bold.
b Proportions of positive/total tests from April 2020 to March 2021 were compared with total numbers from April 2017 to March 2020 by Fisher's exact test.
c ≥ 90% of data are from children and adolescents < 18 years of age.
d Macrolide resistance determination only upon physician's request in case of clinically suspected MRMp infection. Data reported for both sites from Zurich (A + B).
e Period of enhanced surveillance from 1 October 2019 to 30 March 2020.
Entries in italics signify macrolide resistance determination only upon physician’s request in case of clinically suspected MRMp infection.
Figure 4.
Macrolide-resistant Mycoplasma pneumoniae testing and detection in different countries across the world, April 2017–March 2021 (n = 784)
MRMp: Macrolide-resistant Mycoplasma pneumoniae.
The coloured parts of the bar graph with numbers represent absolute numbers or proportions of MRMp detection (the colours correspond with colours for sites in Figure 2). Data derived from the COVID-19 pandemic (April 2020–March 2021) are indicated by a grey background. Japan and Cuba reported national MRMp surveillance data (Table 4). Macrolide resistance determination in Switzerland was performed only upon request from a physician (in case of clinically suspected MRMp infection).

Discussion
This global survey showed that all countries experienced a decrease in M. pneumoniae incidence by direct test methods in April 2020–March 2021, relative to the previous three years. This decline corresponded with the timing of the implementation of NPIs against COVID-19 in March 2020 in each country. We also observed a decrease in MRMp rates in April 2020 to March 2021. The MRMp rates before the COVID-19 pandemic were lower in Europe than in America or Asia, consistent with previous reports [11].
A reduction in M. pneumoniae detections after the introduction of NPIs was observed with direct test methods such as PCR but not with serology. This effect could be explained by the long-lasting nature of antibodies against M. pneumoniae. Mycoplasma pneumoniae-specific antibodies (IgM and IgG) persist for months to years after infection, and significantly longer than M. pneumoniae DNA in the upper respiratory tract [30,31]. Based on these kinetics, we would expect a decline in positive IgM serology in the second year of the COVID-19 pandemic, but not necessarily in IgG serology as M. pneumoniae-specific IgG antibodies can persist lifelong [30]. There is also the possibility of false-positive results caused by limited assay performance [32] as serological detections are reported from single-sample serology, which was in most cases not confirmed by the detection of a significant antibody level change in convalescent sera. In addition, PCR and serology (IgM and IgG) can be positive in asymptomatic carriers [11]. The detection of specific antibody-secreting cells by enzyme-linked immunospot (ELISpot) assay may allow for differentiation between infection and carriage [24], and a combination of clinical features and biomarkers can help identify patients at high risk for M. pneumoniae community-acquired pneumonia [15]. However, no clinical features were reported in this study and cases were defined by local practice.
Our findings are in line with several reports about a worldwide reduction in infections with respiratory and gastrointestinal pathogens after the introduction of NPIs [2,3,5-7,33-37]. The incidence of invasive bacterial diseases caused by Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis that are transmitted via the respiratory route were also considerably reduced during the early months of the COVID-19 pandemic [38]. The interruption of direct person-to-person transmission was suspected to be the most plausible explanation for the reduction in respiratory infections. These remained low even after the re-opening of schools, except for rhinovirus [6,39-41].
Direct detections of M. pneumoniae between April 2020 and March 2021 were significantly below levels of non-epidemic periods of M. pneumoniae across countries despite widely differing lockdown or school closure periods, and even in countries where no official lockdowns or school closures were enforced. This suggests that the observed low M. pneumoniae incidence may be explained by the continuation of NPIs such as personal protective and physical distancing measures. Other factors that may be involved in restricting M. pneumoniae transmission are behavioural responses to the pandemic (e.g. limited mobility related to COVID-19) and change in healthcare utilisation (e.g. telemedicine visits). After the re-opening of schools, direct M. pneumoniae detections remained low. This was also observed at sites where lockdown and restrictions for the adult population continued while children returned to schools. Children have greater difficulty adhering to physical distancing and personal protective measures so that M. pneumoniae transmission may be less effectively prevented in schools than in the adult population. Unfortunately, we did not have information on the age distribution in children to look at the pre-school and school age groups separately. The low incidence despite the re-opening of schools might suggest that adults play a more important role in transmission of M. pneumoniae than previously thought. This is supported by the observed decrease in the proportion of children and adolescents with M. pneumoniae detection during the COVID-19 pandemic. Notably, there was no change in the proportion of females with M. pneumoniae infection before and during the COVID-19 pandemic. Reduced transmission by shielding of adults (regardless of school closures) was also discussed as possible reason for the decrease in invasive pneumococcal disease [38]. Interestingly, nasopharyngeal pneumococcal carriage in children was only slightly reduced during the first year of the COVID-19 pandemic and the reduction in invasive pneumococcal disease was therefore attributed to the suppression of specific respiratory viruses such as RSV and influenza, which are often implicated as co-pathogens with S. pneumoniae [42]. Mycoplasma pneumoniae is also frequently detected with other viruses in the upper respiratory tract [15,43-45], but the role of co-detections in M. pneumoniae respiratory disease remains unclear [44]. A direct biological effect of SARS-CoV-2 on M. pneumoniae by interference or interaction could be another explanation. To our knowledge, data supporting this hypothesis do not exist so far. Further, transient herd immunity from the recent epidemic period in April 2019–March 2020 in several countries in Europe and Asia could have led to a decreased M. pneumoniae incidence during the COVID-19 pandemic [12]. However, the incidence was also reduced in countries that had not experienced a recent epidemic (e.g. Norway).
The study has a number of limitations. Firstly, because of the variable reporting methods and testing criteria at each site, conclusions based on the analysis across countries must be considered with caution. Data obtained from a single hospital laboratory from a specific region may not be fully representative of the country as a whole. No information about catchment area and numbers of laboratories within regions were available. The study also lacks representation from Africa and South America (no survey response and/or no testing for M. pneumoniae reported). Secondly, defining study-wide case definitions and de-duplication criteria was not feasible given the heterogeneous nature of data collection between sites. De-duplication methodologies were therefore set at site level. Thirdly, as mentioned previously, serological detections were not confirmed by antibody changes in paired sera in most cases. Fourthly, analysis of the local clinical testing pathway for M. pneumoniae was not possible within this study. Decision-making to test or not to test with specific methodologies during the COVID-19 pandemic may have impacted which individuals and sites offered testing at which time. The number of tests increased in one fifth of the sites during the period April 2020 to March 2021 and also the incidence was significantly lower compared with the pre-pandemic period; hence, we do not believe that the overall reduction in M. pneumoniae detections can solely be accounted for by reduced testing. Nor was there an indication that M. pneumoniae testing was reduced because of shifting laboratory resources towards SARS-CoV-2 testing during the whole first year after the introduction of NPIs covered by this study. Finally, an overall survey response rate could not be calculated because of the widespread dissemination of the survey. Incomplete response to a survey can introduce a bias related to differences in incidence between the responders and the non-responders [21,46]. However, this risk seems minimal as our survey dealt with microbiological laboratory data and generated a large and varied sample [46].
This study is another example of how pandemic-focused public health measures may have prevented infections caused by other respiratory pathogens. The COVID-19 pandemic resulted in restrictive NPIs such as lockdowns and school closures, which are unsustainable in the longer term. The results of this study suggest that even less restrictive NPIs such as personal protective and physical distancing measures might have prevented transmission of M. pneumoniae in the community.
The study also highlights the importance of establishing international working groups to investigate pathogen epidemiology where surveillance systems are lacking. It underlines the need for an international case definition for infection with M. pneumoniae (detection method and clinical criteria). The influence of the detection method for epidemiological surveillance of M. pneumoniae is shown in the discrepancy between PCR and single-sample serology in this study. Serological surveillance of M. pneumoniae may be only accurate by using paired sera in order to detect a fourfold increase in IgG levels [11]. However, such procedures are time-consuming and are not useful for acute patient care. A more rapid response to public health measures may be obtained by surveillance of M. pneumoniae using PCR.
Finally, epidemiological surveillance should also include antimicrobial resistance testing of M. pneumoniae. This study represents the most comprehensive estimate of global resistance documented to date and is important for clinicians and infectious disease surveillance considering that macrolides remain the main global treatment option for children with M. pneumoniae infection.
Conclusion
The results of this study from diverse geographical locations and healthcare settings suggest that the implementation of NPIs against COVID-19 probably restricted transmission of M. pneumoniae, leading to a significant reduction in M. pneumoniae infections in many countries across the world from April 2020 to March 2021. The retention of some NPIs after the COVID-19 pandemic e.g. improved hand hygiene, respiratory etiquette or physical distancing in the community, or the use of masks in health care institutions may help reduce the burden of M. pneumoniae infections. The large collaborative network established for this study allows to assess the resurgence of M. pneumoniae infections at a later time.
Funding statement
PMMS was supported by a Walter und Gertrud Siegenthaler Fellowship and the career development program “Filling the Gap” of the University of Zurich, outside of this study. The ESGMAC covered costs for the survey development and administration.
Ethical statement
This study collected aggregated and anonymized data. The need for ethics approval for this study varied by country, and was administered by participants if required (Supplementary Table S2).
Acknowledgements
We are very grateful to all those who helped with the study: Laure F. Pittet (Department of Pediatrics, Division of General Pediatrics, Children’s Hospital, Faculty of Medicine, University of Geneva Hospitals, Geneva, Switzerland); Petra Zimmermann (Faculty of Science and Medicine, University of Fribourg, Fribourg, Switzerland); Jan Fehr (Epidemiology, Biostatistics and Prevention Institute, University of Zurich, Zurich, Switzerland); Lucas M. Bachmann (Medignition Inc. Research Consultants, Zurich, Switzerland); Semjon Sidorov (Division of Infectious Diseases and Hospital Epidemiology, University Children’s Hospital Zurich, Zurich, Switzerland); Wendy W.J. Unger (Division of Infectious Diseases and Immunology, Department of Pediatrics, Erasmus MC University Medical Center–Sophia Children's Hospital, Rotterdam, The Netherlands); Samuel Rhedin (Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden); Todd A. Florin (Feinberg School of Medicine, Northwestern University, Chicago, IL, USA); Lilliam Ambroggio (Sections of Emergency Medicine and Hospital Medicine, Department of Pediatrics, Children’s Hospital Colorado, University of Colorado, Denver, CO, USA); Asha C. Bowen (Department of Infectious Diseases, Perth Children's Hospital, Perth, Western Australia, Australia); ESCMID: William Caddy (executive office), Patrick Kudyba (science coordinator); Swiss Society for Infectious Diseases (SSI): Pierre-Yves Bochud (president); Pediatric Infectious Disease Group of Switzerland (PIGS): Andrea Duppenthaler (secretary); Swiss Society for Microbiology (SSM): Nathalie Mermoud (general secretary).
Supplementary Data
Conflict of interest: None declared.
Authors’ contributions: Study conceptualisation and lead: PMMS. Study design: PMMS, MLB, RNP, RD. Acquisition of data: all authors including all ESGMAC–MyCOVID Study Team members. Analysis and interpretation of data: PMMS, MLB, SAU, NB, MV, KL, SP, CB, DK, JD, BA, VJC, GG, RNP, RD. Writing of the original manuscript draft: PMMS. Formal analysis: PMMS, MLB, RNP, RD. All authors, including all ESGMAC–MyCOVID Study Team members, contributed to the work, reviewed and approved the manuscript.
References
- 1. Cowling BJ, Ali ST, Ng TWY, Tsang TK, Li JCM, Fong MW, et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: an observational study. Lancet Public Health. 2020;5(5):e279-88. 10.1016/S2468-2667(20)30090-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Oster Y, Michael-Gayego A, Rivkin M, Levinson L, Wolf DG, Nir-Paz R. Decreased prevalence rate of respiratory pathogens in hospitalized patients during the COVID-19 pandemic: possible role for public health containment measures? Clin Microbiol Infect. 2021;27(5):811-2. 10.1016/j.cmi.2020.12.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Huang QS, Wood T, Jelley L, Jennings T, Jefferies S, Daniells K, et al. ; Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat Commun. 2021;12(1):1001. 10.1038/s41467-021-21157-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Baker RE, Park SW, Yang W, Vecchi GA, Metcalf CJE, Grenfell BT. The impact of COVID-19 nonpharmaceutical interventions on the future dynamics of endemic infections. Proc Natl Acad Sci USA. 2020;117(48):30547-53. 10.1073/pnas.2013182117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Emborg HD, Carnahan A, Bragstad K, Trebbien R, Brytting M, Hungnes O, et al. Abrupt termination of the 2019/20 influenza season following preventive measures against COVID-19 in Denmark, Norway and Sweden. Euro Surveill. 2021;26(22):2001160. 10.2807/1560-7917.ES.2021.26.22.2001160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Haapanen M, Renko M, Artama M, Kuitunen I. The impact of the lockdown and the re-opening of schools and day cares on the epidemiology of SARS-CoV-2 and other respiratory infections in children - A nationwide register study in Finland. EClinicalMedicine. 2021;34:100807. 10.1016/j.eclinm.2021.100807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Wan WY, Thoon KC, Loo LH, Chan KS, Oon LLE, Ramasamy A, et al. Trends in respiratory virus infections during the COVID-19 pandemic in Singapore, 2020. JAMA Netw Open. 2021;4(6):e2115973. 10.1001/jamanetworkopen.2021.15973 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. von Hammerstein AL, Aebi C, Barbey F, Berger C, Buettcher M, Casaulta C, et al. Interseasonal RSV infections in Switzerland - rapid establishment of a clinician-led national reporting system (RSV EpiCH). Swiss Med Wkly. 2021;151(35-36):w30057. 10.4414/SMW.2021.w30057 [DOI] [PubMed] [Google Scholar]
- 9. Zhang Y, Quigley A, Wang Q, MacIntyre CR. Non-pharmaceutical interventions during the roll out of covid-19 vaccines. BMJ. 2021;375(2314):n2314. 10.1136/bmj.n2314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Zhang Y, Huang Y, Ai T, Luo J, Liu H. Effect of COVID-19 on childhood Mycoplasma pneumoniae infection in Chengdu, China. BMC Pediatr. 2021;21(1):202. 10.1186/s12887-021-02679-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Waites KB, Xiao L, Liu Y, Balish MF, Atkinson TP. Mycoplasma pneumoniae from the respiratory tract and beyond. Clin Microbiol Rev. 2017;30(3):747-809. 10.1128/CMR.00114-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Jacobs E, Ehrhardt I, Dumke R. New insights in the outbreak pattern of Mycoplasma pneumoniae. Int J Med Microbiol. 2015;305(7):705-8. 10.1016/j.ijmm.2015.08.021 [DOI] [PubMed] [Google Scholar]
- 13. Uldum SA, Bangsborg JM, Gahrn-Hansen B, Ljung R, Mølvadgaard M, Føns Petersen R, et al. Epidemic of Mycoplasma pneumoniae infection in Denmark, 2010 and 2011. Euro Surveill. 2012;17(5):20073. 10.2807/ese.17.05.20073-en [DOI] [PubMed] [Google Scholar]
- 14. Beeton ML, Zhang XS, Uldum SA, Bébéar C, Dumke R, Gullsby K, et al. Mycoplasma pneumoniae infections, 11 countries in Europe and Israel, 2011 to 2016. Euro Surveill. 2020;25(2):1900112. 10.2807/1560-7917.ES.2020.25.2.1900112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Meyer Sauteur PM, Krautter S, Ambroggio L, Seiler M, Paioni P, Relly C, et al. Improved diagnostics help to identify clinical features and biomarkers that predict Mycoplasma pneumoniae community-acquired pneumonia in children. Clin Infect Dis. 2020;71(7):1645-54. 10.1093/cid/ciz1059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Dorigo-Zetsma JW, Wilbrink B, van der Nat H, Bartelds AI, Heijnen ML, Dankert J. Results of molecular detection of Mycoplasma pneumoniae among patients with acute respiratory infection and in their household contacts reveals children as human reservoirs. J Infect Dis. 2001;183(4):675-8. 10.1086/318529 [DOI] [PubMed] [Google Scholar]
- 17. Waites KB, Talkington DF. Mycoplasma pneumoniae and its role as a human pathogen. Clin Microbiol Rev. 2004;17(4):697-728. 10.1128/CMR.17.4.697-728.2004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Loens K, Ieven M. Mycoplasma pneumoniae: current knowledge on nucleic acid amplification techniques and serological diagnostics. Front Microbiol. 2016;7:448. 10.3389/fmicb.2016.00448 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Meyer Sauteur PM, Unger WWJ, Nadal D, Berger C, Vink C, van Rossum AMC. Infection with and carriage of Mycoplasma pneumoniae in children. Front Microbiol. 2016;7:329. 10.3389/fmicb.2016.00329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Dumke R, Benitez AJ, Chalker V, Gullsby K, Henrich B, Hidalgo-Grass C, et al. Multi-center evaluation of one commercial and 12 in-house real-time PCR assays for detection of Mycoplasma pneumoniae. Diagn Microbiol Infect Dis. 2017;88(2):111-4. 10.1016/j.diagmicrobio.2017.03.004 [DOI] [PubMed] [Google Scholar]
- 21. Pulcini C, Leibovici L, CMI Editorial Office . CMI guidance for authors of surveys. Clin Microbiol Infect. 2016;22(11):901-2. 10.1016/j.cmi.2016.08.015 [DOI] [PubMed] [Google Scholar]
- 22. Bennett C, Khangura S, Brehaut JC, Graham ID, Moher D, Potter BK, et al. Reporting guidelines for survey research: an analysis of published guidance and reporting practices. PLoS Med. 2010;8(8):e1001069. 10.1371/journal.pmed.1001069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.SurveyMonkey. How SurveyMonkey gets its data. [Accessed: 30 April 2021]. Available from: www.surveymonkey.com/mp/survey-methodology
- 24. Meyer Sauteur PM, Seiler M, Trück J, Unger WWJ, Paioni P, Relly C, et al. Diagnosis of Mycoplasma pneumoniae pneumonia with measurement of specific antibody-secreting cells. Am J Respir Crit Care Med. 2019;200(8):1066-9. 10.1164/rccm.201904-0860LE [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.European Centre for Disease Prevention and Control (ECDC). Data on country response measures to COVID-19. Stockholm: ECDC. [Accessed: 30 April 2021]. Available from: https://www.ecdc.europa.eu/en/publications-data/download-data-response-measures-covid-19
- 26.Wikipedia. COVID-19 lockdowns. [Accessed: 30 April 2021]. Available from: https://en.wikipedia.org/wiki/COVID-19_lockdowns
- 27.United Nations Children's Fund (UNICEF). COVID-19 and school closures. New York: UNICEF; 2021. Available from: https://data.unicef.org/resources/one-year-of-covid-19-and-school-closures
- 28.Center for Disease Control and Prevention (CDC). Principles of epidemiology in public health practice. 3rd Edition. Lesson 3: Measures of risk. Atlanta: CDC; 2012 Available from: https://www.cdc.gov/csels/dsepd/ss1978/lesson3/section2.html
- 29.R Core Team. R: A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2021. Available from: http://www.R-project.org
- 30. Meyer Sauteur PM, Trück J, van Rossum AMC, Berger C. Circulating antibody-secreting cell response during Mycoplasma pneumoniae childhood pneumonia. J Infect Dis. 2020;222(1):136-47. 10.1093/infdis/jiaa062 [DOI] [PubMed] [Google Scholar]
- 31. Nir-Paz R, Michael-Gayego A, Ron M, Block C. Evaluation of eight commercial tests for Mycoplasma pneumoniae antibodies in the absence of acute infection. Clin Microbiol Infect. 2006;12(7):685-8. 10.1111/j.1469-0691.2006.01469.x [DOI] [PubMed] [Google Scholar]
- 32. Beersma MF, Dirven K, van Dam AP, Templeton KE, Claas EC, Goossens H. Evaluation of 12 commercial tests and the complement fixation test for Mycoplasma pneumoniae-specific immunoglobulin G (IgG) and IgM antibodies, with PCR used as the "gold standard". J Clin Microbiol. 2005;43(5):2277-85. 10.1128/JCM.43.5.2277-2285.2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Angoulvant F, Ouldali N, Yang DD, Filser M, Gajdos V, Rybak A, et al. Coronavirus disease 2019 pandemic: impact caused by school closure and national lockdown on pediatric visits and admissions for viral and nonviral infections - a time series analysis. Clin Infect Dis. 2021;72(2):319-22. 10.1093/cid/ciaa710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Rhedin SA, Ryd Rinder M, Hildenwall H, Herlenius E, Hertting O, Luthander J, et al. Reduction in paediatric emergency visits during the COVID-19 pandemic in a region with open preschools and schools. Acta Paediatr. 2021;110(10):2802-4. 10.1111/apa.15978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Yeoh DK, Foley DA, Minney-Smith CA, Martin AC, Mace AO, Sikazwe CT, et al. Impact of coronavirus disease 2019 public health measures on detections of influenza and respiratory syncytial virus in children during the 2020 australian winter. Clin Infect Dis. 2021;72(12):2199-202. 10.1093/cid/ciaa1475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Leuzinger K, Roloff T, Gosert R, Sogaard K, Naegele K, Rentsch K, et al. Epidemiology of severe acute respiratory syndrome coronavirus 2 emergence amidst community-acquired respiratory viruses. J Infect Dis. 2020;222(8):1270-9. 10.1093/infdis/jiaa464 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Ullrich A, Schranz M, Rexroth U, Hamouda O, Schaade L, Diercke M, et al. Impact of the COVID-19 pandemic and associated non-pharmaceutical interventions on other notifiable infectious diseases in Germany: An analysis of national surveillance data during week 1-2016 - week 32-2020. Lancet Reg Health Eur. 2021;6:100103. 10.1016/j.lanepe.2021.100103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Brueggemann AB, Jansen van Rensburg MJ, Shaw D, McCarthy ND, Jolley KA, Maiden MCJ, et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: a prospective analysis of surveillance data. Lancet Digit Health. 2021;3(6):e360-70. 10.1016/S2589-7500(21)00077-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Kohns Vasconcelos M, Meyer Sauteur PM, Keitel K, Santoro R, Heininger U, van den Anker J, et al. Strikingly decreased community-acquired pneumonia admissions in children despite open schools and day-care facilities in Switzerland. Pediatr Infect Dis J. 2021;40(4):e171-2. 10.1097/INF.0000000000003026 [DOI] [PubMed] [Google Scholar]
- 40. Poole S, Brendish NJ, Tanner AR, Clark TW. Physical distancing in schools for SARS-CoV-2 and the resurgence of rhinovirus. Lancet Respir Med. 2020;8(12):e92-3. 10.1016/S2213-2600(20)30502-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Oh DY, Buda S, Biere B, Reiche J, Schlosser F, Duwe S, et al. Trends in respiratory virus circulation following COVID-19-targeted nonpharmaceutical interventions in Germany, January - September 2020: Analysis of national surveillance data. Lancet Reg Health Eur. 2021;6:100112. 10.1016/j.lanepe.2021.100112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Danino D, Ben-Shimol S, Van Der Beek BA, Givon-Lavi N, Avni YS, Greenberg D, et al. Decline in pneumococcal disease in young children during the COVID-19 pandemic in Israel associated with suppression of seasonal respiratory viruses, despite persistent pneumococcal carriage: A prospective cohort study. Clin Infect Dis. 2021;ciab1014. 10.1093/cid/ciab1014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Jain S, Williams DJ, Arnold SR, Ampofo K, Bramley AM, Reed C, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015;372(9):835-45. 10.1056/NEJMoa1405870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Diaz MH, Cross KE, Benitez AJ, Hicks LA, Kutty P, Bramley AM, et al. Identification of bacterial and viral codetections with Mycoplasma pneumoniae using the TaqMan Array Card in patients hospitalized with community-acquired pneumonia. Open Forum Infect Dis. 2016;3(2):ofw071. 10.1093/ofid/ofw071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Zheng X, Lee S, Selvarangan R, Qin X, Tang YW, Stiles J, et al. Macrolide-resistant Mycoplasma pneumoniae, United States. Emerg Infect Dis. 2015;21(8):1470-2. 10.3201/eid2108.150273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Bates SM, Rogstad KE. Postal research: too many problems? Sex Transm Infect. 2000;76(5):332-4. 10.1136/sti.76.5.332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Touati A, Benard A, Hassen AB, Bébéar CM, Pereyre S. Evaluation of five commercial real-time PCR assays for detection of Mycoplasma pneumoniae in respiratory tract specimens. J Clin Microbiol. 2009;47(7):2269-71. 10.1128/JCM.00326-09 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Peuchant O, Ménard A, Renaudin H, Morozumi M, Ubukata K, Bébéar CM, et al. Increased macrolide resistance of Mycoplasma pneumoniae in France directly detected in clinical specimens by real-time PCR and melting curve analysis. J Antimicrob Chemother. 2009;64(1):52-8. 10.1093/jac/dkp160 [DOI] [PubMed] [Google Scholar]
- 49. Meyer Sauteur PM, Bleisch B, Voit A, Maurer FP, Relly C, Berger C, et al. Survey of macrolide-resistant Mycoplasma pneumoniae in children with community-acquired pneumonia in Switzerland. Swiss Med Wkly. 2014;144:w14041. [DOI] [PubMed] [Google Scholar]
- 50. Wagner K, Imkamp F, Pires VP, Keller PM. Evaluation of Lightmix Mycoplasma macrolide assay for detection of macrolide-resistant Mycoplasma pneumoniae in pneumonia patients. Clin Microbiol Infect. 2019;25(3):383.e5-7. 10.1016/j.cmi.2018.10.006 [DOI] [PubMed] [Google Scholar]
- 51. Hardegger D, Nadal D, Bossart W, Altwegg M, Dutly F. Rapid detection of Mycoplasma pneumoniae in clinical samples by real-time PCR. J Microbiol Methods. 2000;41(1):45-51. 10.1016/S0167-7012(00)00135-4 [DOI] [PubMed] [Google Scholar]
- 52. Ursi D, Dirven K, Loens K, Ieven M, Goossens H. Detection of Mycoplasma pneumoniae in respiratory samples by real-time PCR using an inhibition control. J Microbiol Methods. 2003;55(1):149-53. 10.1016/S0167-7012(03)00131-3 [DOI] [PubMed] [Google Scholar]
- 53. Berger N, Muyldermans G, Dupont Y, Quoilin S. Assessing the sensitivity and representativeness of the Belgian Sentinel Network of Laboratories using test reimbursement data. Arch Public Health. 2016;74(1):29. 10.1186/s13690-016-0145-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Spuesens EB, Hoogenboezem T, Sluijter M, Hartwig NG, van Rossum AM, Vink C. Macrolide resistance determination and molecular typing of Mycoplasma pneumoniae by pyrosequencing. J Microbiol Methods. 2010;82(3):214-22. 10.1016/j.mimet.2010.06.004 [DOI] [PubMed] [Google Scholar]
- 55. Brown RJ, Macfarlane-Smith L, Phillips S, Chalker VJ. Detection of macrolide resistant Mycoplasma pneumoniae in England, September 2014 to September 2015. Euro Surveill. 2015;20(48):30078. 10.2807/1560-7917.ES.2015.20.48.30078 [DOI] [PubMed] [Google Scholar]
- 56. Rasmussen JN, Voldstedlund M, Andersen RL, Ellermann-Eriksen S, Jensen TG, Johansen HK, et al. Increased incidence of Mycoplasma pneumoniae infections detected by laboratory-based surveillance in Denmark in 2010. Euro Surveill. 2010;15(45):19708. 10.2807/ese.15.45.19708-en [DOI] [PubMed] [Google Scholar]
- 57. Hohenthal U, Vainionpää R, Meurman O, Vahtera A, Katiskalahti T, Nikoskelainen J, et al. Aetiological diagnosis of community acquired pneumonia: utility of rapid microbiological methods with respect to disease severity. Scand J Infect Dis. 2008;40(2):131-8. 10.1080/00365540701534525 [DOI] [PubMed] [Google Scholar]
- 58. Kawai Y, Miyashita N, Kubo M, Akaike H, Kato A, Nishizawa Y, et al. Therapeutic efficacy of macrolides, minocycline, and tosufloxacin against macrolide-resistant Mycoplasma pneumoniae pneumonia in pediatric patients. Antimicrob Agents Chemother. 2013;57(5):2252-8. 10.1128/AAC.00048-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Hung HM, Chuang CH, Chen YY, Liao WC, Li SW, Chang IY, et al. Clonal spread of macrolide-resistant Mycoplasma pneumoniae sequence type-3 and type-17 with recombination on non-P1 adhesin among children in Taiwan. Clin Microbiol Infect. 2021;27(8):1169.e1-6. 10.1016/j.cmi.2020.09.035 [DOI] [PubMed] [Google Scholar]
- 60. Rodriguez N, Mondeja B, Sardiñas R, Vega D, Dumke R. First detection and characterization of macrolide-resistant Mycoplasma pneumoniae strains in Cuba. Int J Infect Dis. 2019;80:115-7. 10.1016/j.ijid.2018.12.018 [DOI] [PubMed] [Google Scholar]
- 61. Dierig A, Hirsch HH, Decker ML, Bielicki JA, Heininger U, Ritz N. Mycoplasma pneumoniae detection in children with respiratory tract infections and influence on management - a retrospective cohort study in Switzerland. Acta Paediatr. 2020;109(2):375-80. 10.1111/apa.14891 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.