

Abstract
Introduction
Coronavirus disease of 2019 (COVID-19) has resulted in millions of cases worldwide. As the pandemic has progressed, the understanding of this disease has evolved.
Objective
This narrative review provides emergency clinicians with a focused update of the resuscitation and airway management of COVID-19.
Discussion
Patients with COVID-19 and septic shock should be resuscitated with buffered/balanced crystalloids. If hypotension is present despite intravenous fluids, vasopressors including norepinephrine should be initiated. Stress dose steroids are recommended for patients with severe or refractory septic shock. Airway management is the mainstay of initial resuscitation in patients with COVID-19. Patients with COVID-19 and ARDS should be managed similarly to those ARDS patients without COVID-19. Clinicians should not delay intubation if indicated. In patients who are more clinically stable, physicians can consider a step-wise approach as patients' oxygenation needs escalate. High-flow nasal cannula (HFNC) and non-invasive positive pressure ventilation (NIPPV) are recommended over elective intubation. Prone positioning, even in awake patients, has been shown to lower intubation rates and improve oxygenation. Strategies consistent with ARDSnet can be implemented in this patient population, with a goal tidal volume of 4–8 mL/kg of predicted body weight and targeted plateau pressures <30 cm H2O. Limited data support the use of neuromuscular blocking agents (NBMA), recruitment maneuvers, inhaled pulmonary vasodilators, and extracorporeal membrane oxygenation (ECMO).
Conclusion
This review presents a concise update of the resuscitation strategies and airway management techniques in patients with COVID-19 for emergency medicine clinicians.
Keywords: Coronavirus-2019, COVID-19, Severe acute respiratory syndrome coronavirus 2, SARS-CoV-2
1. Introduction
Coronavirus disease of 2019 (COVID-19), caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), is a global pandemic, with the first outbreak in late 2019 in Wuhan, Hubei Province, China [1,2]. This paper is the final submission of a series that provides focused updates of COVID-19 for emergency clinicians [3,4]. This review will focus specifically on acute resuscitation and airway management in the patient with severe COVID-19 not involving cardiac arrest.
Although our understanding of COVID-19 has evolved, more treatments are available, and the virus itself has changed. Airway management remains a significant contributor to hospital resource utilization and patient outcomes. Early in the pandemic, a strategy of early intubation with mechanical ventilation was used for those with severe hypoxia. However, this strategy was not associated with improved patient outcomes including mortality. As the pandemic progressed, noninvasive techniques including high flow nasal cannula and noninvasive positive pressure ventilation (bilevel positive airway pressure [BPAP] and continuous positive airway pressure [CPAP]) have demonstrated efficacy and safety in improving patient respiratory status. The use of steroids for those with hypoxia has also become a central component of treatment.
Greater clinician experience and modifications in treatment strategy have resulted in improved patient outcomes during the pandemic. Data from the Centers for Disease Control and Prevention (CDC) and the National Hospital Care Survey (NHCS) submitted by 41 hospitals from March 2020 through September 2021 demonstrated an inpatient mortality rate for COVID-19 patients as high as 23.2% in April 2020, before falling to an all-time low of 2.8% in September 2021. During this same time frame, intubated patients with COVID-19 had a mortality rate ranging from 74.1% in March 2020 to a high of 81.8% in May 2021, before decreasing to under 50% in September 2021. Patients discharged alive following intubation or ventilator use had an average length of stay (LOS) of 30 days at the beginning of the pandemic. The most recent data from August 2021 shows the average length of stay (LOS) for this population is 21.3 days. For those patients requiring ventilation who died in-hospital, LOS was much shorter. In April 2020, average LOS was as short as 14.3 days, increasing to a high of 24.9 days in October 2021, with more recent data in August 2021 showing that the average LOS is approximately 2 weeks. It is important to note these data are not nationally representative of the United States (US) [5].
2. Methods
A literature review of PubMed and Google Scholar databases was performed for articles up to February 23, 2022, using the keywords ‘COVID’ OR ‘COVID-19’ OR ‘SARS-CoV-2’ OR ‘coronavirus’ AND ‘airway’ OR resuscitation’ for this narrative review. The authors included retrospective and prospective studies, systematic reviews and meta-analyses, clinical guidelines, and other narrative reviews. Commentaries and letters were also included. The literature search was restricted to studies published or translated into English. Authors reviewed all relevant articles and decided which studies to include for the review by consensus, with focus on emergency medicine-relevant articles, including guidelines. A total of 131 resources were selected for inclusion in this review.
3. Discussion
3.1. Initial resuscitation in patients with COVID-19 and septic shock
Patients presenting with COVID-19 and septic shock should be treated identically to other medical patients without COVID-19 who present with septic shock [6]. The definition of septic shock is unchanged in patients with COVID-19 (defined as an infectious source present with vasopressors necessary to maintain mean arterial pressure (MAP) > 65 mmHg, and lactate >2 mmol/L, without underlying hypovolemia) [6]. Resuscitation with buffered/balanced crystalloids instead of unbalanced crystalloids or colloids is recommended, and a conservative fluid resuscitation strategy is favored over a liberal approach [[6], [7], [8], [9], [10], [11]]. The World Health Organization (WHO) recommends administering an initial bolus of 250–500 mL of crystalloid (normal saline [NS], Ringer's lactate) rapidly over 15–30 min; additional fluid boluses of similar size should be tailored based on the patient's clinical response (fluid overload, MAP >65 mmHg, urine output (UOP) > 0.5 mL/kg/h, perfusion, capillary refill, hemodynamics, mental status, and lactate) [6]. To assess fluid responsiveness, skin temperature, capillary refill, and lactate measurements may be used in addition to dynamic measurements [[6], [7], [8]]. Limited evidence exists regarding this aspect of resuscitation and is based on historical treatment of patients with acute respiratory distress syndrome (ARDS). Albumin and colloids are not recommended for fluid resuscitation [8]. Hypoalbuminemia has been shown to be a risk factor for poor outcomes, but there is a lack of high-quality data supporting its use as a standard adjunct therapy [12].
3.2. Septic shock: Vasopressors and corticosteroids
If patients remain in shock during or after the initial fluid resuscitation, vasopressors should be initiated [6]. Among patients with COVID-19 treated in the intensive care unit (ICU), studies suggest that 28–94% require vasopressors [13,14]. Norepinephrine is the first-line vasopressor due to its ability to increase MAP with fewer adverse effects such as arrhythmias and lower all-cause mortality in septic shock compared to other pressors, including dopamine [[6], [7], [8],15]. Vasoactive agents should be titrated to a MAP of 60–65 mmHg, and an arterial catheter should be placed to monitor vascular pressure as soon as reasonably feasible [7,8]. Second line agents include vasopressin and epinephrine [7,8]. Vasopressin and epinephrine may be combined with norepinephrine to reach a MAP goal, while vasopressin can also be used as an adjunct to wean norepinephrine [7,8]. Dobutamine should be considered in patients who have signs of cardiac dysfunction and continuous organ hypoperfusion despite fluids and vasopressors [6,7]. A study of 31 ICU patients on norepinephrine found aerosolized milrinone did not have a positive impact on right ventricular (RV) function or afterload [16]. One retrospective study of 10 patients found adding angiotensin II reduced the norepinephrine equivalent dose by 30.4%; however, 50% of patients died after care was withdrawn and the other 50% of patients remained hospitalized [17]. In patients with severe or refractory septic shock, corticosteroids are recommended with consideration for dexamethasone or hydrocortisone as primary options (e.g., hydrocortisone 200 mg daily) [7]. For patients presenting with septic shock refractory to IV fluids and vasopressors who have previously received steroids for COVID-19, administering stress dose steroids (i.e., hydrocortisone 100 mg IV) should be considered. If they are currently receiving dexamethasone for treatment of COVID-19 but present with refractory septic shock, a steroid with mineralocorticoid effects (e.g., hydrocortisone) can be administered [7,18,19]. Additional discussion of the medical management for patients with COVID-19 has been addressed earlier in this series [4].
3.3. Airway updates and rescue maneuvers
Much of the morbidity and mortality associated with COVID-19 is due to pulmonary complications including hypoxemia and acute respiratory failure [[20], [21], [22]]. These typically occur the second week after the initial onset of symptoms [20,21]. As the disease progresses, patients may require increasing respiratory support, including low flow or high flow oxygen supplementation systems, noninvasive ventilation, and endotracheal intubation with mechanical ventilation. Patients with signs of severe respiratory failure or loss of airway control should be considered for early endotracheal intubation, especially if non-invasive options are unavailable.
3.3.1. Lung pathophysiology
The pathophysiology of lung injury in ventilated patients with COVID-19 and secondary ARDS may differ from those who are spontaneously breathing. Early evidence suggests that patient-self-inflicted lung injury (P-SILI) may be the corollary of ventilator-induced lung injury, which is caused by ventilation at high tidal volumes with increased pressures [23,24]. This can occur in early ARDS due to strong inspiratory effort causing elevated transpulmonary pressures and leakage of fluid. Initially, two subtypes of COVID-19 patients with ARDS (CARDS) were described: type L, which had low lung elastance and thus high compliance with a lower response to PEEP and type H, which were characterized by high lung elastance, low compliance and higher response to PEEP [24]. However, this has fallen out of favor, with more rigorous studies suggesting COVID-19 patients with ARDS should be managed similarly to ARDS patients without COVID-19 [8,25,26].
3.3.2. Oxygen saturation targets
Diagnostic criteria for severe COVID-19 pulmonary infection includes patients with oxygen saturation < 94% on room air, respiratory rate > 30 breaths/min, more than 50% of lung infiltrates, or PaO2/FiO2 < 300 mmHg [7]. It is unclear what the ideal oxygen saturation is for those patients with hypoxemia and COVID-19, but the National Institutes of Health (NIH) suggests 92–96% [7]. The WHO recommends titrating oxygen saturation to ≥94% during the initial resuscitation; for those with stable hypoxia without signs of distress a level of ≥90% is reasonable. In pregnancy, the WHO recommends a goal oxygen saturation of 92–95% [6]. For patients with a peripheral oxygen saturation < 90–92%, the Society of Critical Care Medicine (SCCM) recommends initiating supplemental oxygen and titrating to an oxygen saturation no greater than 96% [7]. Supplemental oxygen should be administered by nasal cannula or high-flow nasal cannula (HFNC) for those with severe COVID-19 with pulmonary involvement or hypoxemia as an initial strategy [6,7] . Maintaining oxygenation saturations outside these ranges has been linked to worse clinical outcomes [7,27,28]. Higher oxygen saturation targets and hyperoxia should be avoided. In a multicenter, randomized trial, patients with ARDS assigned to a conservative‑oxygen strategy (goal PaO2 55–70 mmHg or pulse oximetry 88–92%) compared to a liberal oxygen strategy (goal PaO2 90–105 mmHg, pulse oximetry ≥96%) had higher 28-day (34.3% versus 26.5%) and 90-day mortality rates (44.4% versus 30.4%) [28]. Fig. 1 provides an algorithm for management of hypoxia in COVID-19.
Fig. 1.
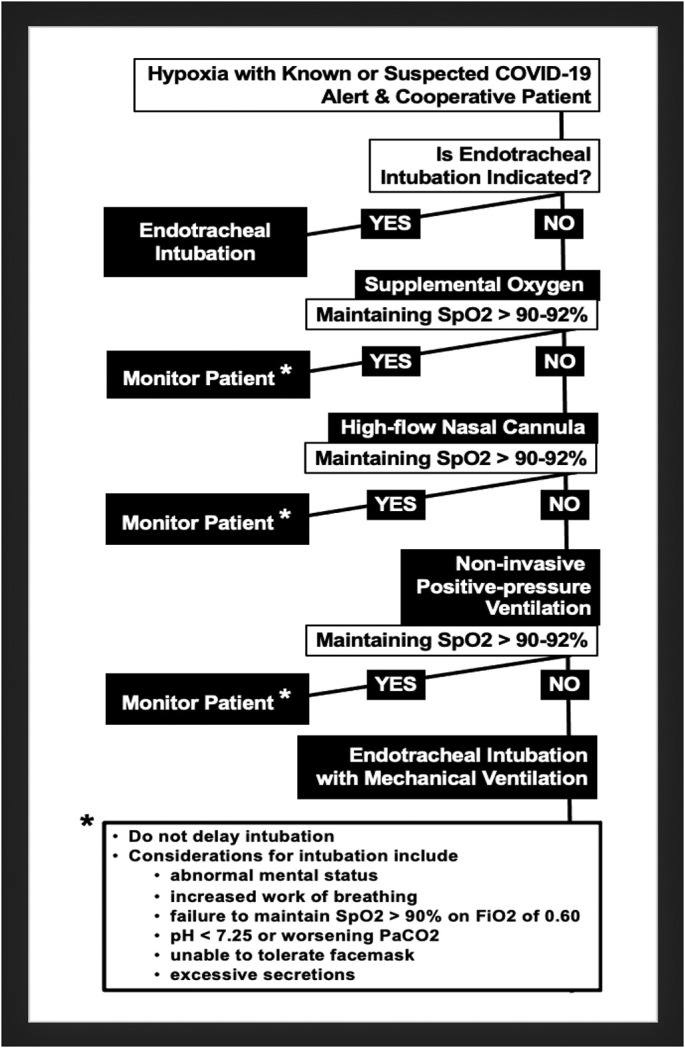
Algorithm for approaching the hypoxic COVID-19 patient. Physicians should initially assess the need for intubation. If the patient condition does not require immediate intubation, physicians should utilize a step-wise approach escalating oxygen therapy as needed. Patients should be closely monitored to evaluate for potential intubation and response to airway interventions.
3.3.3. Non-invasive oxygenation treatment modalities
Certain patients with severe COVID-19 require endotracheal intubation with mechanical ventilation early in their treatment course. However, many patients can be safely and appropriately managed with non-invasive means of oxygenation and ventilation (i.e., interventions other than endotracheal intubation). For patients with hypoxemia, supplemental oxygen via a low-flow system such as nasal cannula can be used initially [7,29]. If oxygen flow rates greater than 6 L/min via nasal cannula are needed to maintain an oxygen saturation ≥ 90–92%, supplementation via a facemask can be utilized for higher flow rates, or a Venturi mask can be utilized [[6], [7], [8],29]. For patients who remain hypoxic or demonstrate increased work of breathing despite these interventions, HFNC or NIPPV can be utilized [6,7,29]. With respect to terminology in this review, NIPPV refers to either CPAP or BPAP.
The NIH and SCCM recommend HFNC over NIPPV, though contraindications must be considered (Table 1, Table 2 ) [7,8]. Current data suggest HFNC reduces mortality, increases ventilator-free days, and decreases the risk of intubation [7,23]. HFNC is typically better tolerated compared to NIPPV due to patient comfort and improved ability to eat, drink, and speak. HFNC improves oxygenation by decreasing the anatomical dead space and provides a mechanism for increased PEEP [30,31]. Compared to other oxygen delivery systems, it can also humidify oxygen, allowing for washing out of CO2 while providing nearly 100% oxygen in certain instances [30,31]. One study of COVID-19 patients with hypoxemic respiratory failure found HFNC was associated with more ventilator-free days than conventional oxygen and NIPPV (24 days vs 22 days vs 19 days, respectively). Subgroup analysis of patients with a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen [PaO2/FiO2] ≤200 mmHg found that intubation rates were lower for HFNC versus conventional oxygen or NIPPV (hazard ratio 2.07 and 2.57, respectively) [32]. A later meta-analysis found HFNC reduced intubation rates compared to NIPPV (OR 0.48, 95% CI 0.31–0.73), as well as ICU mortality (OR 0.36, 95% 0.20–0.63) [33]. A randomized controlled trial (RCT) of patients with PaO2/FiO2 < 200 and COVID-19 found those receiving HFNC were less likely to be intubated (34.3% vs. 51%) and more likely to experience clinical recovery in 28 days (77.8% vs. 71%) compared to those receiving conventional oxygen [34].
Table 1.
HFNC and NIPPV Indications and Contraindications in COVID-19
| Indications for HFNC |
|
| Indications for NIPPV |
|
| Contraindications to HFNC and NIPPV |
|
Table 2.
Considerations in non-invasive oxygenation and ventilation for the known or suspected COVID-19 patient with acute hypoxic respiratory failure – the pros and cons of high-flow nasal cannula and non-invasive positive-pressure ventilation
| High-flow Nasal Cannula (HFNC) | Non-invasive Positive-pressure Ventilation (NIPPV) |
|---|---|
| Pros | Pros |
|
|
| Cons | Cons |
|
|
Early in the pandemic, a strategy of early intubation was frequently used, but more recent data and updated guidelines recommend the use of HFNC and NIPPV to avoid intubation, if clinically feasible (Table 1) [6,7,35]. If necessary, endotracheal intubation with mechanical ventilation should be pursued without delay. An RCT of 220 COVID-19 patients with ARDS comparing HFNC to conventional oxygen therapy found lower rates of intubation in the HFNC group (34.3% versus 51.0%, hazard ratio = 0.62, 95% CI 0.39–0.96) and more rapid time to recovery (HFNC: 11 days, IQR 9–14, conventional oxygen therapy: 14 days, IQR 11–19; hazard ratio = 1.39; 95% CI 1.00–1.92) [34]. When comparing HFNC and NIPPV, other studies have found no significant difference in intubation rate, mortality, or nosocomial infection of staff [36].
NIPPV can be utilized in patients who fail HFNC or in those with diseases which may benefit significantly from NIPPV, including chronic obstructive pulmonary disease (COPD) or left-sided heart failure with pulmonary edema. It may also be used in settings where there is no clear indication for endotracheal intubation, but HFNC is unavailable [7]. CPAP may be used initially to improve oxygenation in the setting of COVID-19 hypoxia and respiratory distress. If the patient has hypercarbia or obstructive lung disease, BPAP may be preferable [30,37]. Both BPAP and CPAP may be less effective in patients unable to tolerate the mask or with productive cough or secretions [30]. One study of 79 patients with respiratory failure due to COVID-19 found NIPPV was successful in 48.1% (n = 38) in providing appropriate oxygenation and thus avoided intubation, while NIPPV failed in 51.9% (n = 41) of patients. Of these patients failing NIPPV, 20 (25.3%) died, while 21 were intubated (26.6%) [38]. Another study of 286 patients found NIPPV was successfully used without the need for intubation in 63.6% (n = 182; 118 had moderate to severe ARDS) [39]. NIPPV failed in 82 patients (28.7%), and for patients in whom NIPPV failed and required mechanical ventilation, mortality was 78%. Failure of NIPPV was more common in those with higher disease severity, lower admission PaO2/FiO2 ratio, higher respiratory rates, and need for organ support [39].
A retrospective study of 318 patients with COVID-19 found that 41% of patients with acute respiratory failure failed HFNC and were managed with NIPPV [40]. This study found that those with PaO2/FiO2 ratios <200 were more likely to fail HFNC, and of those who failed and required NIPPV, their PaO2/FiO2 ratio improved significantly 1–2 h after starting NIPPV [40]. An RCT published in January 2022 including 1273 patients with COVID-19 respiratory failure found CPAP reduced the need for intubation and mortality within 30 days compared to conventional oxygen (33.3% vs. 44.4%) [41]. Other studies have found intubation may be avoided in 37–80% of patients with COVID-19 undergoing NIPPV [[42], [43], [44], [45]]. A retrospective analysis of 88 patients receiving CPAP in the United Kingdom found a 56% survival rate, and a prospective observational study demonstrated 55% of cases successfully avoided intubation using helmet CPAP and were transferred to the general ward [46,47]. The SCCM and NIH guidelines do not include recommendations concerning the use of helmet NIPPV.
Clinically, patients who do not require immediate intubation are often trialed through several oxygenation/ventilation strategies prior to endotracheal intubation, with escalation if one modality fails [6]. One such general strategy is depicted in Fig. 1. In a trial of COVID-19 patients with acute hypoxic respiratory failure, 65 patients in the HFNC group had escalation to CPAP, with only 15% ultimately requiring intubation, while a second group of 48 patients utilizing an initial combined therapy of both HFNC and CPAP failed non-invasive methods with 42% requiring intubation [48]. Another study examined a non-invasive trial (delivered in this study using facemask and ventilator with positive pressure support and defined as NIV by the study authors) as rescue therapy if CPAP failed to avoid intubation, finding slightly lower mortality rates in patients who used a stepwise approach of CPAP, BPAP, and then endotracheal intubation (20%) versus CPAP followed by endotracheal intubation (22%) (Kaplan Meier overall survival probability P < 0.01) [49]. A suggested ladder to approaching oxygen therapy may include: 1) NC up to 6 L/min 2) Venturi mask up to 50% or NRB 3) NC + NRB 4) HFNC +/− NRB 5) NIPPV 6) endotracheal intubation (Table 2) [29,30,40,[50], [51], [52], [53], [54], [55]].
3.3.4. Aerosolization and clinician infection risk for HFNC and NIPPV
Both HFNC and NIPPV are aerosol-generating procedures. Higher flows with HFNC may increase the risk of aerosolization, with one study finding a flow of 10 L/min had a dispersion distance of 6.5 cm and a flow of 60 L/min had a dispersion of 17.2 cm, though this is less than a facemask at 10 L/min (9.5 cm) and non-rebreather at 10 L/min (24.6 cm) [56,57]. Cough droplets may spread to 2.91 m with HFNC at 60 L/min [58]. However, there is currently a lack of evidence regarding the risk of aerosolization and risk of infection for COVID-19 specifically, and HFNC has not demonstrated increased aerosolization compared to conventional oxygen [[59], [60], [61]]. In fact, some authors suggest HFNC has a similar risk as conventional oxygen therapy [62]. Limited data suggest an increase in aerosolization of virus particles near the patient but no definitive relationship with nosocomial infection of hospital staff, and the risk is low if appropriate PPE is used [63]. If possible, an airborne infection isolation room (negative pressure room) should be utilized, but if unavailable, a room with a closed door can be used. Both HFNC and NIPPV should be utilized at the lowest effective flow rate/pressure to improve patient oxygenation and work of breathing while reducing unnecessary aerosolization of infectious particles [23]. A surgical mask can be placed over the HFNC device on the patient's face [62,64]. If NIPPV is utilized, a full face mask or oronasal mask should be used with a good seal and not an anti-asphyxiation valve or port. A dual limb circuit with an expiratory limb viral filter may reduce dispersion [23]. A viral filter should otherwise be applied directly to the NIPPV mask to reduce dispersion of viral particles [23].
3.3.5. Predictors of endotracheal intubation
In all patients receiving oxygen supplementation (conventional oxygen, HFNC, and NIPPV), close monitoring of the patient's respiratory status is necessary, including respiratory rate, work of breathing, oxygen saturation (absolute and relative to the fraction of inspired oxygen), and mental status (Table 3 ). Of note, the ROX index which integrates the oxygen saturation, FiO2, and respiratory rate, can be utilized to predict failure of HFNC and need for endotracheal intubation [[65], [66], [67], [68]]. Prior to the COVID-19 pandemic, evidence suggested a ROX index ≥4.88 at 2, 6, and 12 h after initiation of HFNC is associated with lower risk of intubation, but the risk of failure is high with levels <3.85 [65,68]. Among COVID-19 patients, a ROX index >3 at 2, 6, and 12 h is associated with HFNC success (85.3% sensitivity), though a separate study found the most sensitive value was 5.37 at 4 h [66,67]. The most important consideration regarding the ROX index is to incorporate patient appearance with the trend of the ROX index, rather than using ROX as an isolated value [69]. Patients who improve with HFNC or NIPPV after 3 h may be continued on the therapy or weaned. If the patient does not improve but is stable, awake repositioning/proning can be attempted.
Table 3.
Indicators of HFNC/NIPPV failure
|
3.3.6. Rescue strategies: Awake proning
Prone positioning can be used for those on conventional oxygen, HFNC, NIPPV, and mechanical ventilation [[6], [7], [8]]. Several studies conducted in patients with COVID-19 requiring oxygen supplementation found that prone positioning improved oxygenation and lowered intubation rates [[70], [71], [72], [73], [74]]. Guidelines recommend that for patients with an increasing oxygen requirement, but no other indication for intubation, awake prone positioning can be used [7]. While the prone position is the most common position utilized, patients may also lie on their sides [[75], [76], [77]]. Another variation has been described in which the patient sits on a chair and rests in a semi-prone position with their chest on an elevated/flat surface [78].
A multinational randomized controlled open-label study of 1126 patients on HFNC receiving either awake prone positioning or standard care concluded the number needed to treat (NNT) to avoid treatment failure (intubation or death) within 28 days of enrollment was 15 (95% CI 8–156) [73]. The relative risk of treatment failure at day 28 was 0.86 (95% CI 0.75–0.98) [73]. Although there was no significant difference in 28-day mortality (RR 0.87, 95% CI 0.71–1.07), patients in the awake prone positioning study group had higher odds of weaning from HFNC compared to the usual care group (HR 1.19, 95% CI 1.01–1.39) [73]. Importantly, the rate of adverse effects associated with position changes (e.g., line dislodgement, skin breakdown, cardiac arrest) was similar between the awake proning group and standard care [73]. In the PROFLO multicenter RCT, 75 patients were randomized to the prone group or control to determine its impact on rates of intubation [79]. The authors found no significant difference between the two groups, and the study was terminated prematurely due to futility [79]. One study of 27 patients with COVID-19 requiring oxygen supplementation randomized to self-proning versus control found no statistically significant decrease in oxygen requirements, though authors found self-proning was easy to implement and that it was well tolerated [80]. A prospective study of non-intubated patients with hypoxemic respiratory failure with COVID-19 found those tolerating prone positioning experienced improvement with prone positioning [71]. A prospective cohort including 56 non-intubated patients found oxygenation improved the PaO2/FiO2 ratio from 181 mmHg (supine) to 286 mmHg (prone). This improvement was maintained in 23% of patients [81]. For awake patients, the WHO recommends a total proning duration of 8–12 h each day, divided into shorter periods [6].
Pregnant patients with COVID-19 are an especially vulnerable population, and limited data exist evaluating optimal practices, with most peer-reviewed literature in the form of case reports or case series [[82], [83], [84], [85], [86]]. Appropriate care of the critically ill pregnant COVID-19 patient requires early collaboration between multiple care teams including obstetrics, intensivists, pulmonologists, infectious diseases, and neonatology to ensure the best outcomes for mother and child [82,[87], [88], [89]]. According to the Society for Maternal-Fetal Medicine and guidance published by the American Journal of Obstetrics and Gynecology Maternal Fetal Medicine, prone positioning can be considered in pregnant patients, especially if complicated by ARDS, in either the left lateral decubitus position, fully prone, or a modified prone position combined with left lateral tilt and has been done successfully in women with gestational age as late as 24 weeks [7,[87], [88], [89], [90], [91], [92], [93]]. In order to successfully support patients with optimal prone or lateral decubitus positioning, clinicians should be cognizant of the potential need for additional resources including padding, mechanical rotating beds, fetal observation, invasive hemodynamic monitoring, and definitive airway management. Prone positioning may be especially challenging once the patient reaches 34 weeks of pregnancy due to physical constraints; delivery as an alternative to proning should be critically examined [87,88].
Awake prone positioning is not recommended as a rescue therapy in patients who clinically should be intubated, are in respiratory distress, or hemodynamically unstable [7]. Patients who have undergone recent abdominal surgery, with facial and/or pelvic fractures or open/unstable chest, or have an unstable spine are not candidates for awake prone positioning either [7].
3.3.7. Endotracheal intubation
The decision to intubate can be challenging but should be individualized based on the patient. HFNC and NIPPV should be trialed with frequent evaluations. If these measures fail or if contraindications to HFNC and NIPPV are present, endotracheal intubation is recommended [[6], [7], [8]]. Early intubation compared to delayed or no intubation has not been associated with improved ICU mortality (21% versus 33%) or fewer ventilator-free days (3 days versus 2 days) [94]. A meta-analysis of 8944 patients with COVID-19 found no difference in mortality in patients receiving HFNC or NIPPV prior to intubation compared to those intubated without HFNC or NIPPV [95].
Patients who demonstrate rapid progression of respiratory compromise, persistent need for high flows of FiO2, worsening hypercapnia, increasing work of breathing, worsening mental status, decreasing tidal volume, worsening desaturations, and hemodynamic instability will likely require endotracheal intubation [96]. Other patients requiring endotracheal intubation include those with poorly controlled secretions, mask intolerance, and multiorgan dysfunction [[96], [97], [98]].
3.3.8. Aerosolization and clinician infection risk for endotracheal intubation
Intubation can be a high-risk procedure for infection if clinicians are not wearing appropriate personal protective equipment [3]. In the beginning of the COVID-19 pandemic, the rate of infection for clinicians performing the intubation was 3.6% at 7 days, 6.1% at 14 days, and 8.5% at 21 days, but more current data suggest far lower numbers [[99], [100], [101], [102]]. A study of 72 intubations found that although PPE was used in 97% of cases, the clinician performing the intubation did not report being sick or require time off work at 5, 10, or 14 days [103].
If intubation is required, full contact and airborne personal protective equipment (PPE) should be utilized including a powered air-purifying respirator or fit-tested disposable N95 respiratory mask with eye protection [6,8]. If possible, intubation should be performed in an airborne infection isolation room, but if this is not available, a room with a closed door should be utilized [6]. The most experienced clinician should perform the intubation [6]. The patient should be preoxygenated prior to the event, ideally with a tight-fitting bag-valve-mask (BVM) with a high-efficiency hydrophobic viral filter to minimize aerosolization [3,96,104,105]. Video laryngoscopy is recommended for the intubation attempt [7,8]. BVM ventilation should be minimally used before and after intubation if possible, with the viral filter placed between the breathing circuit or resuscitation bag and the facemask [1,3]. If the patient does require BVM, a two-person technique with two-hand mask seal is recommended [1,3]. The ventilator, including the circuit, should be prepared to immediately connect to the endotracheal tube (ETT) as soon as placement is confirmed without using BVM to reduce exposure. In-line suction devices and adapters should also be attached in advance [106]. A high-efficiency particulate air (HEPA) filter should be present on the ventilator expiratory limb to reduce the risk of contamination [106]. Point-of-care ultrasound can be used to rapidly confirm correct endotracheal tube position after placement [[107], [108], [109]].
3.3.9. Ventilation strategies in COVID-19 complicated by ARDS
In patients with ARDS who are mechanically ventilated, the COVID-19 Treatment Guidelines Panel recommends using a tidal volume of 4–8 mL/kg of predicted body weight and targeting plateau pressures <30 cm H2O in conjunction with a conservative fluid strategy [[6], [7], [8]]. A tidal volume of 6 mL/kg predicted body weight (PBW) is the recommended starting point by WHO; escalation up to 8 mL/kg PBW can be considered based on the patient scenario such as acidosis or dyssynchrony. Additionally, permissive hypercapnia is allowed and is thought to minimize ventilator-induced lung injury (VILI) [6,24]. Oxygen should be titrated to an oxygen saturation of 88–96%. These recommendations persist given that there is no evidence that significantly differentiates ARDS associated with COVID-19 from ARDS due to other causes [7]. As such, patients with COVID-19 who are mechanically ventilated should be treated similarly to patients with ARDS according to ARDSnet protocols [7]. Higher positive end-expiratory pressure (PEEP) is preferred over lower PEEP [[6], [7], [8]]. An early study of 7 intubated patients undergoing decremental PEEP trials, with optimal PEEP calculated to give maximum values of PaO2/FiO2 of 17.9 (SD +/− 3.6) millibars, concluded higher PEEP is preferred to lower PEEP [110]. A study of mechanically ventilated patients with COVID-19 found low tidal volumes, high PEEP, and low driving pressures were widely used [111]. If the PEEP is >10 mmHg, clinicians should closely monitor for effects of potential barotrauma [8]. The patient's response to ventilation should be assessed frequently. For those with an FiO2 less than 0.6 and a PaO2/FiO2 > 150 mmHg, this ventilator strategy may be continued.
3.3.10. Rescue strategies in intubated patients with COVID-19 and ARDS
In patients who are mechanically ventilated with refractory hypoxemia despite maximized ventilation strategies, proning should be implemented for 12–16 h per day [7]. Patients should be monitored for barotrauma and other complications related to higher PEEP protocols [7]. As proning of the intubated patient requires significant coordination and monitoring, this should be performed at the times of greatest staff availability to ensure safety. Low quality evidence suggests patients with COVID-19 and ARDS respond well to proning with one small study suggesting a reduction in mortality (NNT = 8) [[112], [113], [114]]. It is unclear the ideal duration of proning, although some authors suggest a minimum of 12 h [115]. Current guidelines recommend proning ventilated patients with either moderate or severe ARDS for 12–16 h [7,8]. A retrospective study of 38 patients compared standard proning duration (more than 75% of proning cycles were approximately 16 h) versus prolonged proning duration (more than 75% of the proning cycles were approximately 40 h) and found no difference in ICU LOS or mortality, but there was a non-significant increase in bed sores in the prolonged prone group (67% versus 44%, P = 0.167) [116].
In intubated, mechanically ventilated patients with moderate-to-severe ARDS, either intermittent boluses of neuromuscular blocking agents (NMBA) or continuous infusions may be used to improve ventilation [7]. A continuous NMBA infusion can be used for up to 48 h, assuming the patient's anxiety and pain can be monitored and treated. NMBA infusions may also be used in instances of persistent high plateau pressures, patient-ventilator dyssynchrony, ongoing deep sedation, or prone ventilation [[6], [7], [8]]. In a multicenter observational trial of 407 patients with COVID-19 and severe ARDS, researchers found no significant difference in unassisted respiratory support or time to extubation by 28 days between patients who received NMBA for shorter (<2 days) or longer (>2 days) duration [117]. However, additional studies of NMBAs in COVID-19 are necessary.
Recruitment maneuvers to improve oxygenation in severe COVID-19 are recommended, apart from staircase or incremental PEEP method [[6], [7], [8]]. A small study of 20 patients found after a recruitability assessment with a PEEP of 15 cm H2O, PaO2 slightly improved (68.0 ± 10.3 vs. 69.7 ± 7.9 mmHg, p = 0.31) but PaCO2(72.5 ± 7.1 vs. 75.1 ± 9.0 mmHg; p < 0.01) and static respiratory system compliance (17.5 ± 3.5 vs. 16.6 ± 3.9 mL/cm H2O; p = 0.05) worsened [118]. Other studies of PEEP recruitment maneuvers found ventilation strategies utilizing ARDSnet low PEEP-FIO2 table (PEEP 11 ± 6 cm H2O) and best‑oxygenation (highest PaO2/FiO2) (PEEP 11 ± 3 cm H2O) led to higher PEEP, compared to the best-compliance strategy (6 ± 2 cm H2O, p = 0.001) [119]. This elevation in PEEP with use of the ARDSnet low PEEP-FiO2 table and best‑oxygenation strategy led to higher plateau and driving pressures and mechanical power, potentially increasing the risk of ventilator-induced lung injury, compared to the best-compliance strategy. However, gas exchange was not significantly affected regardless of PEEP strategy [119].
Inhaled pulmonary vasodilators can be used as rescue therapy, but if no significant improvement is seen quickly, then they should be weaned and discontinued [7,8,120]. A study of 38 patients receiving either inhaled epoprostenol or nitric oxide with COVID-19 found no significant difference in outcomes (PaO2, SpO2, and less than 10% increase in PaO2/FiO2) between non-responders and responders (>10% increase PaO2/FiO2) [120]. Clinicians should be cautioned about the development of hemodynamic instability and methemoglobinemia [120]. The Society of Critical Care Medicine (SCCM) recommends against the routine use of nitric oxide [8].
3.3.11. Extracorporeal membrane oxygenation
Extracorporeal membrane oxygenation (ECMO) is an invasive treatment modality that may be required if mechanical ventilation is ineffective despite other rescue therapies [7,8]. WHO recommends considering ECMO for patients with refractory hypoxemia Pa:FiO2 < 50 mmHg for 3 h or Pa:FiO2 < 80 mmHg for 6 h in spite of lung protective strategies [6]. Pre-pandemic data from the Extracorporeal Life Support Organization (ELSO) registry found venous-venous (V-V) ECMO mortality to be approximately 40% with a mean duration of 12 days; of those patients with COVID-19 on ECMO therapy, more than 90% used V-V ECMO with a mean duration of 18 days [121]. According to the ELSO COVID-19 Dashboard, in-hospital mortality is 47% [122]. This is slightly higher than a systematic review and meta-analysis of 4044 COVID-19 patients receiving ECMO, which found in-hospital mortality was 39% [123]. Early in the pandemic, it appeared that the duration of ECMO was longer for patients with COVID-19 and mortality rates were similar, but this trend appears to be changing as studies continue to be published [121]. Centers that initiated ECMO in COVID-19 patients after May 1, 2020, had a higher adjusted relative risk of in-hospital mortality 90 days after ECMO initiation compared to centers who initiated ECMO in COVID-19 patients prior to that date (1.42, 95% CI 1.17–1.73) [124]. Over time, emerging evidence demonstrates varying mortality rates among patients with COVID-19 receiving ECMO compared to non-COVID-19 ECMO patients [121]. Much of this variation may be due to patient selection and timing in their clinical course rather than ECMO itself [121,125]. An early single-site study of 27 COVID-19 patients on V-V ECMO found the survival rate to be 96.3% [126]. As the pandemic has progressed, other studies have not been as promising, with a multi-institutional analysis of 100 ECMO patients to have a survival rate from 25% (V-A ECMO) to 51% (V-V ECMO) [127]. A meta-analysis of 22 studies of 1896 COVID-19 patients on ECMO (98.6% V-V ECMO) found the pooled in-hospital mortality to be 37.1% (95% CI 32.3%–42.0%) [128]. This mortality rate is comparable to two RCTs (Extracorporeal Membrane Oxygenation for Severe ARDS [EOLIA] and Conventional Ventilatory Support Versus Extracorporeal Membrane Oxygenation for Severe Adult Respiratory Failure [CESAR]) and a meta-analysis studying mortality rates of ARDS patients without COVID-19 receiving ECMO [[128], [129], [130], [131]]. In the EOLIA trial, the mortality rate was 35% in the ECMO group compared to 57% in the control group, (RR = 0.76, 95% CI 0.55–1.04) [131]. In the CESAR trial, 63% of those designated for ECMO survived to 6 months without disability compared to 47% in the conventional management group (95% CI 0.05–0.97) [130]. In the meta-analysis of these two studies, the 90-day mortality in the ECMO group was 36% compared to 48% in the control group (RR = 0.75, 95% CI 0.6–0.94) [129]. Additional data are necessary for further decisions regarding the use of ECMO in patients with COVID-19.
4. Conclusions
COVID-19 can result in respiratory failure, septic shock, and multi-organ failure. Hypotension should be managed with balanced crystalloids, and if they demonstrate refractory hypotension, vasopressors should be initiated. Stress dose steroids such as hydrocortisone are recommended for patients with severe or refractory septic shock. Airway management is a key component of initial resuscitation. Patients with COVID-19 and ARDS should be managed similarly to ARDS patients without COVID-19. Clinicians should not delay intubation if needed. For patients with hypoxia, a step-wise approach can be utilized as oxygenation needs escalate. HFNC and NIPPV are recommended over elective intubation. Prone positioning is associated with lower intubation rates and improved oxygenation. Ventilation strategies based on ARDSnet can be implemented in this patient population, using a tidal volume of 4–8 mL/kg of predicted body weight and targeted plateau pressures <30 cm H2O. Other treatments include NBMA, recruitment maneuvers, inhaled pulmonary vasodilators, and ECMO.
CRediT authorship contribution statement
Summer Chavez: Writing – review & editing, Writing – original draft, Conceptualization. William J. Brady: Conceptualization, Writing – original draft, Writing – review & editing. Michael Gottlieb: Writing – review & editing, Conceptualization. Brandon M. Carius: Writing – review & editing, Conceptualization. Stephen Y. Liang: Conceptualization, Writing – review & editing. Alex Koyfman: Conceptualization, Writing – review & editing. Brit Long: Writing – review & editing, Writing – original draft, Conceptualization.
Declaration of Competing Interest
None.
Acknowledgements
All authors conceived the idea for this manuscript and contributed substantially to the writing and editing of the review. This manuscript did not utilize any grants, and it has not been presented in abstract form. This clinical review has not been published, it is not under consideration for publication elsewhere, its publication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if accepted, it will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder. This review does not reflect the views or opinions of the U.S. government, Department of Defense, U.S. Army, U.S. Air Force, or SAUSHEC EM Residency Program.
References
- 1.Chavez S., Long B., Koyfman A., Liang S.Y. Coronavirus disease (COVID-19): a primer for emergency physicians. Am J Emerg Med. 2021;44:220–229. doi: 10.1016/j.ajem.2020.03.036. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Centers for Disease Control and Prevention . Basics of COVID-19. 2020. COVID-19 and your health.https://www.cdc.gov/coronavirus/2019-ncov/your-health/about-covid-19/basics-covid-19.html Feb. 11. (accessed Mar. 02, 2022) [PubMed] [Google Scholar]
- 3.Long B., et al. Clinical update on COVID-19 for the emergency clinician: presentation and evaluation. Am J Emerg Med. 2022;54:46–57. doi: 10.1016/j.ajem.2022.01.028. Apr. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Long B., et al. Clinical update on COVID-19 for the emergency and critical care clinician: medical management. Am J Emerg Med. 2022;56:158–170. doi: 10.1016/j.ajem.2022.03.036. Mar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention . COVID-19 Hospital Data. 2022. In-hospital mortality among confirmed COVID-19 encounters by week.https://www.cdc.gov/nchs/covid19/nhcs/hospital-mortality-by-week.htm Jan. 12. (accessed Mar. 02, 2022) [Google Scholar]
- 6.World Health Organization . COVID-19 Clinical management; 2021. COVID-19 Clinical management: Living guidance, 23 November 2021.https://files.magicapp.org/guideline/0a6099d8-72d5-4d1d-9438-ecfb7417a16b/published_guideline_5852-3_0.pdf Nov. 23. (accessed Mar. 02, 2022) [Google Scholar]
- 7.COVID-19 Treatment Guidelines Panel . National Institutes of Health; 2022. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines.https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.pdf [PubMed] [Google Scholar]
- 8.Alhazzani W., et al. 2020. Surviving Sepsis campaign: Guidelines on the Management of Critically ill Adults with coronavirus disease 2019 (COVID-19) p. 101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Poston J.T., Patel B.K., Davis A.M. Management of critically ill adults with COVID-19. JAMA. 2020;323(18):1839–1841. doi: 10.1001/jama.2020.4914. May. [DOI] [PubMed] [Google Scholar]
- 10.Kazory A., Ronco C., McCullough P.A. SARS-CoV-2 (COVID-19) and intravascular volume management strategies in the critically ill. Proc (Bayl Univ Med Cent) 2020;0(0):1–6. doi: 10.1080/08998280.2020.1754700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hajjar L.A., et al. Intensive care management of patients with COVID-19: a practical approach. Ann Intensive Care. 2021;11(1):36. doi: 10.1186/s13613-021-00820-w. Feb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Huang J., et al. Hypoalbuminemia predicts the outcome of COVID-19 independent of age and co-morbidity. J Med Virol. 2020;92(10):2152–2158. doi: 10.1002/jmv.26003. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Michard F., Vieillard-Baron A. Critically ill patients with COVID-19: are they hemodynamically unstable and do we know why? Intensive Care Med. 2021;47(2):254–255. doi: 10.1007/s00134-020-06238-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Serafim R.B., Póvoa P., Souza-Dantas V., Kalil A.C., Salluh J.I.F. Clinical course and outcomes of critically ill patients with COVID-19 infection: a systematic review. Clin Microbiol Infect. 2021;27(1):47–54. doi: 10.1016/j.cmi.2020.10.017. Jan. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Avni T., Lador A., Lev S., Leibovici L., Paul M., Grossman A. Vasopressors for the treatment of septic shock: systematic review and meta-analysis. PLoS One. 2015;10(8) doi: 10.1371/journal.pone.0129305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Norden N., et al. Cardiac involvement in critically ill and mechanically ventilated patients with COVID-19 - a prospective, observational echocardiographic study. Am J Cardiovasc Dis. 2021;11(2):253–261. [PMC free article] [PubMed] [Google Scholar]
- 17.Ofosu-Barko K., et al. Angiotensin II administration in patients with COVID-19 shock. Crit Pathw Cardiol. 2021;20(2):100–102. doi: 10.1097/HPC.0000000000000246. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Heming N., Sivanandamoorthy S., Meng P., Bounab R., Annane D. Immune effects of corticosteroids in Sepsis. Front Immunol. 2018;9:1736. doi: 10.3389/fimmu.2018.01736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gibbison B., et al. Corticosteroids in septic shock: a systematic review and network meta-analysis. Crit Care. 2017;21(1):78. doi: 10.1186/s13054-017-1659-4. Mar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zayet S., Gendrin V., Klopfenstein T. Natural history of COVID-19: back to basics. New Microb New Infect. 2020;38 doi: 10.1016/j.nmni.2020.100815. Nov. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chen S., et al. Patterns of deterioration in moderate patients With COVID-19 from jan 2020 to mar 2020: A multi-center, retrospective cohort study in China. Front Med (Lausanne) 2020;7:567296. doi: 10.3389/fmed.2020.567296. Dec. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ferrando C., et al. Patient characteristics, clinical course and factors associated to ICU mortality in critically ill patients infected with SARS-CoV-2 in Spain: a prospective, cohort, multicentre study. Rev Esp Anestesiol Reanim (Engl Ed) 2020;67(8):425–437. doi: 10.1016/j.redar.2020.07.003. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sullivan Z.P., Zazzeron L., Berra L., Hess D.R., Bittner E.A., Chang M.G. Noninvasive respiratory support for COVID-19 patients: when, for whom, and how? J Intensive Care. 2022;10(1):3. doi: 10.1186/s40560-021-00593-1. Jan. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Marini J.J., Gattinoni L. Management of COVID-19 respiratory distress. JAMA. 2020;323(22):2329–2330. doi: 10.1001/jama.2020.6825. Jun. [DOI] [PubMed] [Google Scholar]
- 25.Ziehr D.R., et al. Respiratory pathophysiology of mechanically ventilated patients with COVID-19: a cohort study. Am J Respir Crit Care Med. 2020;201(12):1560–1564. doi: 10.1164/rccm.202004-1163LE. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Pearce A.K., McGuire W.C., Malhotra A. Lung and chest wall mechanics in COVID-19 acute respiratory distress syndrome. J Thorac Dis. 2021;13(11) doi: 10.21037/jtd-21-1567. Nov. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shenoy N., Luchtel R., Gulani P. Considerations for target oxygen saturation in COVID-19 patients: are we under-shooting? BMC Med. 2020;18(1):260. doi: 10.1186/s12916-020-01735-2. Aug. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Barrot L., et al. Liberal or conservative oxygen therapy for acute respiratory distress syndrome. N Engl J Med. 2020;382(11):999–1008. doi: 10.1056/NEJMoa1916431. Mar. [DOI] [PubMed] [Google Scholar]
- 29.Long B., Liang S.Y., Hicks C., Gottlieb M. Just the facts: what are the roles of oxygen escalation and noninvasive ventilation in COVID-19? CJEM. 2020;22(5):587–590. doi: 10.1017/cem.2020.396. Sep. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Carter C., Aedy H., Notter J. COVID-19 disease: non-invasive ventilation and high frequency nasal oxygenation. Clin Integrat Care. 2020;1 doi: 10.1016/j.intcar.2020.100006. Jul. [DOI] [Google Scholar]
- 31.Ashraf-Kashani N., Kumar R. High-flow nasal oxygen therapy. BJA Education. 2017;17(2):63–67. doi: 10.1093/bjaed/mkw041. Feb. [DOI] [Google Scholar]
- 32.Frat J.-P., et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185–2196. doi: 10.1056/NEJMoa1503326. Jun. [DOI] [PubMed] [Google Scholar]
- 33.Ni Y.-N., Luo J., Yu H., Liu D., Liang B.-M., Liang Z.-A. The effect of high-flow nasal cannula in reducing the mortality and the rate of endotracheal intubation when used before mechanical ventilation compared with conventional oxygen therapy and noninvasive positive pressure ventilation. A systematic review and meta-analysis. Am J Emerg Med. 2018;36(2):226–233. doi: 10.1016/j.ajem.2017.07.083. Feb. [DOI] [PubMed] [Google Scholar]
- 34.Ospina-Tascón G.A., et al. Effect of high-flow oxygen therapy vs conventional oxygen therapy on invasive mechanical ventilation and clinical recovery in patients with severe COVID-19: a randomized clinical trial. JAMA. 2021:2161–2171. doi: 10.1001/jama.2021.20714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Villarreal-Fernandez E., Patel R., Golamari R., Khalid M., DeWaters A., Haouzi P. A plea for avoiding systematic intubation in severely hypoxemic patients with COVID-19-associated respiratory failure. Crit Care. 2020;24(1):337. doi: 10.1186/s13054-020-03063-6. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Duan J., et al. Use of high-flow nasal cannula and noninvasive ventilation in patients with COVID-19: a multicenter observational study. Am J Emerg Med. 2021;46:276–281. doi: 10.1016/j.ajem.2020.07.071. Aug. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Carpagnano G.E., et al. Bilevel and continuous positive airway pressure and factors linked to all-cause mortality in COVID-19 patients in an intermediate respiratory intensive care unit in Italy. Expert Rev Respir Med. 2022:1–5. doi: 10.1080/17476348.2021.1866546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Menzella F., et al. Effectiveness of noninvasive ventilation in COVID-19 related-acute respiratory distress syndrome. Clin Respir J. 2021;15(7):779–787. doi: 10.1111/crj.13361. Jul. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Chacko B., et al. Noninvasive ventilation in the management of respiratory failure due to COVID-19 infection: experience from a resource-limited setting. Mayo Clin Proc. 2022;97(1):31–45. doi: 10.1016/j.mayocp.2021.10.002. Jan. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Wang K., Zhao W., Li J., Shu W., Duan J. The experience of high-flow nasal cannula in hospitalized patients with 2019 novel coronavirus-infected pneumonia in two hospitals of Chongqing, China. Ann Intensive Care. 2020;10(1):37. doi: 10.1186/s13613-020-00653-z. Mar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Perkins G.D., et al. Effect of noninvasive respiratory strategies on intubation or mortality among patients with acute hypoxemic respiratory failure and COVID-19: the RECOVERY-RS randomized clinical trial. JAMA. 2022;327(6):546–558. doi: 10.1001/jama.2022.0028. Feb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Alviset S., et al. Continuous positive airway pressure (CPAP) face-mask ventilation is an easy and cheap option to manage a massive influx of patients presenting acute respiratory failure during the SARS-CoV-2 outbreak: a retrospective cohort study. PLoS One. 2020;15(10) doi: 10.1371/journal.pone.0240645. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Noeman-Ahmed Y., Gokaraju S., Powrie D.J., Amran D.A., Sayed I.E., Roshdy A., et al. medRxiv. 2020 doi: 10.1101/2020.06.14.20130880. p. 2020.06.14.20130880, Jun. 16. [DOI] [PubMed] [Google Scholar]
- 44.Cammarota G., et al. Noninvasive respiratory support outside the intensive care unit for acute respiratory failure related to coronavirus-19 disease: a systematic review and meta-analysis. Crit Care. 2021;25(1):268. doi: 10.1186/s13054-021-03697-0. Jul. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Brusasco C., et al. Continuous positive airway pressure in COVID-19 patients with moderate-to-severe respiratory failure. Eur Respir J. Feb. 2021;57(2) doi: 10.1183/13993003.02524-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Aliberti S., et al. Helmet CPAP treatment in patients with COVID-19 pneumonia: a multicentre cohort study. Eur Respir J. 2020;56(4):2001935. doi: 10.1183/13993003.01935-2020. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Nightingale R., et al. CPAP delivered outside critical care during the second wave of COVID-19: outcomes from a UK respiratory surge unit. BMJ Open Respir Res. 2021;8(1) doi: 10.1136/bmjresp-2021-000907. Sep. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Colaianni-Alfonso N., et al. Combined noninvasive respiratory support therapies to treat COVID-19. Respir Care. 2021;66(12):1831–1839. doi: 10.4187/respcare.09162. Dec. [DOI] [PubMed] [Google Scholar]
- 49.Coppola S., et al. Feasibility and clinical outcomes of a step up noninvasive respiratory support strategy in patients with severe COVID-19 pneumonia. J Clin Med. Jan. 2021;10(22) doi: 10.3390/jcm10225444. Art no 22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Giron F., Rao S., Tapaskar N. A multicomponent oxygen delivery strategy for COVID-19 patients in a step-down intensive care unit: a case series. Respir Med Case Rep. 2020;31 doi: 10.1016/j.rmcr.2020.101209. Aug. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Acevedo R.A., Fascia W., Pedley J., Kaul V. The use of non-rebreather masks on top of high-flow nasal cannula at maximal settings. Respir Care. 2021;66(Suppl. 10) https://rc.rcjournal.com/content/66/Suppl_10/3605381 Oct. Accessed: May 05, 2022. [Online]. Available: [Google Scholar]
- 52.Zodda D., Hanson A., Berns A. Optimizing non-invasive oxygenation for COVID-19 patients presenting to the emergency department with acute respiratory distress: a case report. Clin Pract Cases Emerg Med. 2020;4(3):327–331. doi: 10.5811/cpcem.2020.6.48456. Aug. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Wang Z., et al. The use of non-invasive ventilation in COVID-19: a systematic review. Int J Infect Dis. 2021;106:254–261. doi: 10.1016/j.ijid.2021.03.078. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Schünemann H.J., et al. Ventilation techniques and risk for transmission of coronavirus disease, including COVID-19: a living systematic review of multiple streams of evidence. Ann Intern Med. 2020;173(3):204–216. doi: 10.7326/M20-2306. Aug. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Bonnesen B., et al. Management of COVID-19-associated acute respiratory failure with alternatives to invasive mechanical ventilation: high-flow oxygen, continuous positive airway pressure, and noninvasive ventilation. Diagnostics (Basel) 2021;11(12):2259. doi: 10.3390/diagnostics11122259. Dec. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Hui D.S., et al. Exhaled air dispersion during high-flow nasal cannula therapy versus CPAP via different masks. Eur Respir J. 2019;53(4):1802339. doi: 10.1183/13993003.02339-2018. Apr. [DOI] [PubMed] [Google Scholar]
- 57.Ip M., et al. Airflow and droplet spreading around oxygen masks: a simulation model for infection control research. Am J Infect Control. 2007;35(10):684–689. doi: 10.1016/j.ajic.2007.05.007. Dec. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Loh N.-H.W., et al. The impact of high-flow nasal cannula (HFNC) on coughing distance: implications on its use during the novel coronavirus disease outbreak. Can J Anaesth. 2020;67(7):893–894. doi: 10.1007/s12630-020-01634-3. Jul. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Bem R.A., et al. Risk of aerosol formation during high-flow nasal cannula treatment in critically ill subjects. Respir Care. 2021;66(6):891–896. doi: 10.4187/respcare.08756. Jun. [DOI] [PubMed] [Google Scholar]
- 60.Lyons C., Callaghan M. The use of high-flow nasal oxygen in COVID-19. Anaesthesia. 2020;75(7):843–847. doi: 10.1111/anae.15073. Jul. [DOI] [PubMed] [Google Scholar]
- 61.Leung C.C.H., et al. Comparison of high-flow nasal cannula versus oxygen face mask for environmental bacterial contamination in critically ill pneumonia patients: a randomized controlled crossover trial. J Hosp Infect. 2019;101(1):84–87. doi: 10.1016/j.jhin.2018.10.007. Jan. [DOI] [PubMed] [Google Scholar]
- 62.Li J., Fink J.B., Ehrmann S. High-flow nasal cannula for COVID-19 patients: low risk of bio-aerosol dispersion. Eur Respir J. 2020;55(5):2000892. doi: 10.1183/13993003.00892-2020. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Haymet A., Bassi G.L., Fraser J.F. Airborne spread of SARS-CoV-2 while using high-flow nasal cannula oxygen therapy: myth or reality? Intensive Care Med. 2020;46(12):2248–2251. doi: 10.1007/s00134-020-06314-w. Dec. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Hui D.S., et al. Exhaled air dispersion during coughing with and without wearing a surgical or N95 mask. PLoS One. 2012;7(12) doi: 10.1371/journal.pone.0050845. Dec. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Roca O., et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: the utility of the ROX index. J Crit Care. 2016;35:200–205. doi: 10.1016/j.jcrc.2016.05.022. Oct. [DOI] [PubMed] [Google Scholar]
- 66.Chandel A., et al. High-flow nasal cannula therapy in COVID-19: using the ROX index to predict success. Respir Care. 2021;66(6):909–919. doi: 10.4187/respcare.08631. Jun. [DOI] [PubMed] [Google Scholar]
- 67.Zucman N., Mullaert J., Roux D., Roca O., Ricard J.-D., Contributors Prediction of outcome of nasal high flow use during COVID-19-related acute hypoxemic respiratory failure. Intensive Care Med. Oct. 2020;46(10):1924–1926. doi: 10.1007/s00134-020-06177-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Roca O., et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am J Respir Crit Care Med. 2019;199(11):1368–1376. doi: 10.1164/rccm.201803-0589OC. Jun. [DOI] [PubMed] [Google Scholar]
- 69.Xia J., et al. High-flow nasal oxygen in coronavirus disease 2019 patients with acute hypoxemic respiratory failure: a multicenter, retrospective cohort study. Crit Care Med. 2020;48(11):e1079–e1086. doi: 10.1097/CCM.0000000000004558. Nov. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Sun Q., Qiu H., Huang M., Yang Y. Lower mortality of COVID-19 by early recognition and intervention: experience from Jiangsu Province. Ann Intensive Care. 2020;10(1):33. doi: 10.1186/s13613-020-00650-2. Mar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Elharrar X., et al. Use of prone positioning in nonintubated patients with COVID-19 and hypoxemic acute respiratory failure. JAMA. 2020;323(22):2336–2338. doi: 10.1001/jama.2020.8255. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Sartini C., et al. Respiratory parameters in patients with COVID-19 after using noninvasive ventilation in the prone position outside the intensive care unit. JAMA. 2020;323(22):2338–2340. doi: 10.1001/jama.2020.7861. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Ehrmann S., et al. Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: a randomised, controlled, multinational, open-label meta-trial. Lancet Respir Med. 2021;9(12):1387–1395. doi: 10.1016/S2213-2600(21)00356-8. Dec. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Caputo N.D., Strayer R.J., Levitan R. Early self-proning in awake, non-intubated patients in the emergency department: a single ED’s experience during the COVID-19 pandemic. Acad Emerg Med. 2020;27(5):375–378. doi: 10.1111/acem.13994. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Schifino G., de Grauw A.J., Daniele F., Comellini V., Fasano L., Pisani L. Effects of prone and lateral position in non-intubated patients with 2019 novel coronavirus (COVID-19) pneumonia. Pulmonology. 2021;27(2):167–171. doi: 10.1016/j.pulmoe.2020.10.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Mlček M., et al. Targeted lateral positioning decreases lung collapse and overdistension in COVID-19-associated ARDS. BMC Pulm Med. 2021;21(1):133. doi: 10.1186/s12890-021-01501-x. Apr. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Ni Z., et al. Efficacy of early prone or lateral positioning in patients with severe COVID-19: a single-center prospective cohort. Precision Clin Med. 2020;3(4):260–271. doi: 10.1093/pcmedi/pbaa034. Dec. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Coppo A., et al. Rodin’s thinker: an alternative position in awake patients with COVID-19. Am J Respir Crit Care Med. 2021;204(6):728–730. doi: 10.1164/rccm.202104-0915LE. Sep. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Rosén J., et al. Awake prone positioning in patients with hypoxemic respiratory failure due to COVID-19: the PROFLO multicenter randomized clinical trial. Crit Care. 2021;25(1):209. doi: 10.1186/s13054-021-03602-9. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Kharat A., et al. Self-proning in COVID-19 patients on low-flow oxygen therapy: a cluster randomised controlled trial. ERJ Open Res. 2021;7(1):00692–02020. doi: 10.1183/23120541.00692-2020. Jan. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Coppo A., et al. Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID-19 (PRON-COVID): a prospective cohort study. Lancet Respir Med. 2020;8(8):765–774. doi: 10.1016/S2213-2600(20)30268-X. Aug. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Society for Maternal-Fetal Medicine COVID-19 Task Force, Halscott T., Vaught J. Management considerations for pregnant patients With COVID-19. Soc Maternal-Fetal Med. 2021 https://s3.amazonaws.com/cdn.smfm.org/media/2734/SMFM_COVID_Management_of_COVID_pos_preg_patients_2-2-21_(final).pdf Feb. 02. (accessed May 05, 2022) [Google Scholar]
- 83.Boelig R.C., et al. Labor and delivery guidance for COVID-19. Am J Obstet Gynecol MFM. 2020;2(2) doi: 10.1016/j.ajogmf.2020.100110. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Juan J., Gil M.M., Rong Z., Zhang Y., Yang H., Poon L.C. Effect of coronavirus disease 2019 (COVID-19) on maternal, perinatal and neonatal outcome: systematic review. Ultrasound Obstet Gynecol. 2020;56(1):15–27. doi: 10.1002/uog.22088. Jul. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Di Mascio D., et al. Outcome of coronavirus spectrum infections (SARS, MERS, COVID-19) during pregnancy: a systematic review and meta-analysis. Am J Obstet Gynecol MFM. 2020;2(2) doi: 10.1016/j.ajogmf.2020.100107. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Zaigham M., Andersson O. Maternal and perinatal outcomes with COVID-19: a systematic review of 108 pregnancies. Acta Obstet Gynecol Scand. 2020;99(7):823–829. doi: 10.1111/aogs.13867. Jul. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Tolcher M.C., et al. Prone positioning for pregnant women with hypoxemia due to coronavirus disease 2019 (COVID-19) Obstet Gynecol. 2020;136(2):259–261. doi: 10.1097/AOG.0000000000004012. Aug. [DOI] [PubMed] [Google Scholar]
- 88.Schnettler W.T., Al Ahwel Y., Suhag A. Severe acute respiratory distress syndrome in coronavirus disease 2019-infected pregnancy: obstetric and intensive care considerations. Am J Obstet Gynecol MFM. Aug. 2020;2(3):100120. doi: 10.1016/j.ajogmf.2020.100120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Palmrich P., et al. Multiprofessional perinatal care in a pregnant patient with acute respiratory distress syndrome due to COVID-19. BMC Pregnancy Childbirth. 2021;21(1):587. doi: 10.1186/s12884-021-04059-y. Aug. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Pourdowlat G., Mikaeilvand A., Eftekhariyazdi M., Nematshahi M., Ebrahimi M., Kazemzadeh A. Prone-position ventilation in a pregnant woman with severe COVID-19 infection associated with acute respiratory distress syndrome. Tanaffos. 2020;19(2):152–155. Nov. [PMC free article] [PubMed] [Google Scholar]
- 91.Testani E., Twiehaus S., Waters T., Pombar X. Conscious prone positioning in a pregnant patient with COVID-19 respiratory distress: a case report and review. Case Rep Womens Health. 2021;31 doi: 10.1016/j.crwh.2021.e00339. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Blauvelt C.A., et al. Acute respiratory distress syndrome in a preterm pregnant patient with coronavirus disease 2019 (COVID-19) Obstet Gynecol. 2020;136(1):46–51. doi: 10.1097/AOG.0000000000003949. Jul. [DOI] [PubMed] [Google Scholar]
- 93.Roddy J.T., Collier W.S., Kurman J.S. Prone positioning for severe ARDS in a postpartum COVID-19 patient following caesarean section. BMJ Case Rep. 2021;14(3) doi: 10.1136/bcr-2020-240385. Mar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Siempos I.I., et al. Effect of early vs. delayed or no intubation on clinical outcomes of patients with COVID-19: an observational study. Front Med (Lausanne) 2020;7 doi: 10.3389/fmed.2020.614152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Papoutsi E., Giannakoulis V.G., Xourgia E., Routsi C., Kotanidou A., Siempos I.I. Effect of timing of intubation on clinical outcomes of critically ill patients with COVID-19: a systematic review and meta-analysis of non-randomized cohort studies. Crit Care. 2021;25(1):121. doi: 10.1186/s13054-021-03540-6. Mar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Montrief T., Ramzy M., Long B., Gottlieb M., Hercz D. COVID-19 respiratory support in the emergency department setting. Am J Emerg Med. 2020;38(10):2160–2168. doi: 10.1016/j.ajem.2020.08.001. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Luo M., et al. Precautions for intubating patients with COVID-19. Anesthesiology. 2020;132(6):1616–1618. doi: 10.1097/ALN.0000000000003288. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.de Roquetaillade C., et al. Timing and causes of death in severe COVID-19 patients. Crit Care. 2021;25(1):224. doi: 10.1186/s13054-021-03639-w. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.El-Boghdadly K., et al. Risks to healthcare workers following tracheal intubation of patients with COVID-19: a prospective international multicentre cohort study. Anaesthesia. 2020;75(11):1437–1447. doi: 10.1111/anae.15170. Nov. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Weissman D.N., de Perio M.A., Radonovich L.J. COVID-19 and risks posed to personnel during endotracheal intubation. JAMA. 2020;323(20):2027–2028. doi: 10.1001/jama.2020.6627. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Parotto M., Cavallin F., Bryson G.L., Chin K.J., intubateCOVID Canadian collaborators. intubateCOVID Canadian collaborators and the intubateCOVID International Coordinating Centre Risks to healthcare workers following tracheal intubation of patients with known or suspected COVID-19 in Canada: data from the intubateCOVID registry. Can J Anaesth. 2021;68(3):425–427. doi: 10.1007/s12630-020-01890-3. Mar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Shrestha G.S., et al. Emergency intubation in Covid-19. N Engl J Med. 2021;384(7) doi: 10.1056/NEJMvcm2007198. Feb. [DOI] [PubMed] [Google Scholar]
- 103.Mullington C.J., Shetty P., Dalton J. Intubation of COVID patients: always a risky business? Anaesthesia. 2021;76(S3):3–4. doi: 10.1111/anae.15196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Meng L., et al. Intubation and ventilation amid the COVID-19 outbreak: Wuhan’s experience. Anesthesiology. 2020;132(6):1317–1332. doi: 10.1097/ALN.0000000000003296. Jun. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Kovacs G., Sowers N., Campbell S., French J., Atkinson P. Just the Facts: Airway management during the coronavirus disease 2019 (COVID-19) pandemic. CJEM. 2022:1–5. doi: 10.1017/cem.2020.353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Lucchini A., Giani M., Winterton D., Foti G., Rona R. Procedures to minimize viral diffusion in the intensive care unit during the COVID-19 pandemic. Intensive Crit Care Nurs. 2020;60 doi: 10.1016/j.iccn.2020.102894. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Gottlieb M., Alerhand S., Long B. Point-of-care ultrasound for intubation confirmation of COVID-19 patients. West J Emerg Med. 2020;21(5):1042–1045. doi: 10.5811/westjem.2020.7.48657. Sep. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Gottlieb M., Holladay D., Peksa G.D. Ultrasonography for the confirmation of endotracheal tube intubation: a systematic review and meta-analysis. Ann Emerg Med. 2018;72(6):627–636. doi: 10.1016/j.annemergmed.2018.06.024. Dec. [DOI] [PubMed] [Google Scholar]
- 109.Gottlieb M., Holladay D., Burns K.M., Nakitende D., Bailitz J. Ultrasound for airway management: an evidence-based review for the emergency clinician. Am J Emerg Med. 2020;38(5):1007–1013. doi: 10.1016/j.ajem.2019.12.019. May. [DOI] [PubMed] [Google Scholar]
- 110.Mittermaier M., et al. Evaluation of PEEP and prone positioning in early COVID-19 ARDS. EClinicalMedicine. 2020;28 doi: 10.1016/j.eclinm.2020.100579. Nov. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Botta M., et al. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): a national, multicentre, observational cohort study. Lancet Respir Med. 2021;9(2):139–148. doi: 10.1016/S2213-2600(20)30459-8. Feb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Weiss T.T., et al. Prone positioning for patients intubated for severe acute respiratory distress syndrome (ARDS) secondary to COVID-19: a retrospective observational cohort study. Br J Anaesth. 2021;126(1):48–55. doi: 10.1016/j.bja.2020.09.042. Jan. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Pan C., et al. Lung Recruitability in COVID-19-associated acute respiratory distress syndrome: a single-center observational study. Am J Respir Crit Care Med. 2020;201(10):1294–1297. doi: 10.1164/rccm.202003-0527LE. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Shelhamer M.C., et al. Prone positioning in moderate to severe acute respiratory distress syndrome due to COVID-19: a cohort study and analysis of physiology. J Intensive Care Med. 2021;36(2):241–252. doi: 10.1177/0885066620980399. Feb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Ghelichkhani P., Esmaeili M. Prone position in management of COVID-19 patients; a commentary. Arch Acad Emerg Med. 2020;8(1) p. e48, Apr. [PMC free article] [PubMed] [Google Scholar]
- 116.Rezoagli E., Mariani I., Rona R., Foti G., Bellani G. Difference between prolonged versus standard duration of prone position in COVID-19 patients: a retrospective study. Minerva Anestesiol. 2021;87(12):1383–1385. doi: 10.23736/S0375-9393.21.15864-X. 10.23736/S0375-9393.21.15864-X Dec. [DOI] [PubMed] [Google Scholar]
- 117.Courcelle R., Gaudry S., Serck N., Blonz G., Lascarrou J.-B., Grimaldi D. Neuromuscular blocking agents (NMBA) for COVID-19 acute respiratory distress syndrome: a multicenter observational study. Crit Care. 2020;24:446. doi: 10.1186/s13054-020-03164-2. Jul. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Sang L., et al. Lung recruitment, individualized PEEP, and prone position ventilation for COVID-19-associated severe ARDS: a single center observational study. Front Med (Lausanne) 2020;7 doi: 10.3389/fmed.2020.603943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Pan C., et al. Evaluation of positive end-expiratory pressure strategies in patients with coronavirus disease 2019–induced acute respiratory distress syndrome. Front Med. 2021;8:984. doi: 10.3389/fmed.2021.637747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.DeGrado J.R., et al. Evaluation of the efficacy and safety of inhaled epoprostenol and inhaled nitric oxide for refractory hypoxemia in patients with coronavirus disease 2019. Crit Care Explor. 2020;2(10) doi: 10.1097/CCE.0000000000000259. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Badulak J., et al. Extracorporeal membrane oxygenation for COVID-19: updated 2021 guidelines from the extracorporeal life support organization. ASAIO J. 2021;67(5):485–495. doi: 10.1097/MAT.0000000000001422. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Extracorporeal Life Support Organization COVID-19 registry dashboard. ECLS. 2022 https://www.elso.org/Registry/FullCOVID-19RegistryDashboard.aspx (accessed Mar. 02, 2022) [Google Scholar]
- 123.Bertini P., et al. ECMO in COVID-19 patients: A systematic review and meta-analysis. J Cardiothorac Vasc Anesth. Nov. 2021 doi: 10.1053/j.jvca.2021.11.006. pp. S1053–0770(21)00971-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Barbaro R.P., et al. Extracorporeal membrane oxygenation for COVID-19: evolving outcomes from the international extracorporeal life support organization registry. Lancet. 2021;398(10307):1230–1238. doi: 10.1016/S0140-6736(21)01960-7. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Vuylsteke A. ECMO in COVID-19: do not blame the tool. Lancet. 2021;398(10307):1197–1199. doi: 10.1016/S0140-6736(21)02137-1. Oct. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Kon Z.N., et al. Extracorporeal membrane oxygenation support in severe COVID-19. Ann Thorac Surg. 2021;111(2):537–543. doi: 10.1016/j.athoracsur.2020.07.002. Feb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Jacobs J.P., et al. Multi-institutional analysis of 100 consecutive patients with COVID-19 and severe pulmonary compromise treated with extracorporeal membrane oxygenation: outcomes and trends over time. ASAIO J. 2021;67(5):496–502. doi: 10.1097/MAT.0000000000001434. May. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Ramanathan Kollengode, et al. Extracorporeal membrane oxygenation for COVID-19: a systematic review and meta-analysis. Crit Care. 2021;25 doi: 10.1186/s13054-021-03634-1. Dec. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Combes A., et al. ECMO for severe ARDS: systematic review and individual patient data meta-analysis. Intensive Care Med. 2020;46(11):2048–2057. doi: 10.1007/s00134-020-06248-3. Nov. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Peek G.J., et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374(9698):1351–1363. doi: 10.1016/S0140-6736(09)61069-2. Oct. [DOI] [PubMed] [Google Scholar]
- 131.Combes A., et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018;378(21):1965–1975. doi: 10.1056/NEJMoa1800385. May. [DOI] [PubMed] [Google Scholar]