

ABSTRACT
Osteochondroma usually arises from the metaphyseal region of growing bones. The occurrence of extraskeletal osteochondroma is rare with very few case reports. Para-articular osteochondroma is a type of extraskeletal osteochondroma. It frequently occurs around the knee, usually at infrapatellar Hoffa's fat pad. It is usually intracapsular but extrasynovial and arises from the capsule and connective tissues due to osteocartilaginous metaplasia. We present a case of 19-years male with anterior knee pain for 3 years, swelling, and deformity of the knee with flexion limitation for one year. Radiography revealed ovoid, corticated lesion free from adjoining bones. Mass interpreted as benign, so planned for excision. Well circumscribed nodule excised from the medial parapatellar approach. Histology revealed cartilaginous tissues surrounded by fibrous tissues with scattered enchondral ossification. Postoperatively and subsequent follow-up resulted in pain-free joint, complete recovery of range of motion with no clinicoradiological evidence of recurrence.
Keywords: adipose tissue, knee joint, osteochondroma
INTRODUCTION
Osteochondroma is the most common benign bone tumor. It usually arises in the metaphyseal region of growing bones. Extraskeletal osteochondroma is very rare, manifestation is common in the knee particularly in the infrapatellar fat pad of Hoffa. It originates from the capsule or adjoining connective tissue as a result of osteocartilaginous metaplasia. It may be the sequel of Hoffa's disease which is the consequence of various traumatic events or repetitive microtrauma of the infrapatellar fat.1-5 We present a case of para-articular extrasynovial osteochondroma of the knee in a young adult and discuss the clinico-radiological features, histopathological features, pathogenesis, treatment, and outcome.
CASE REPORT
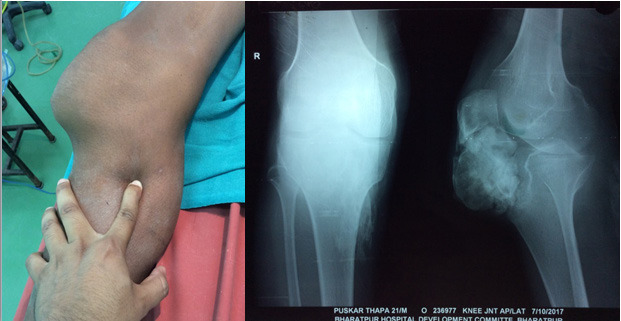
A 19 years old male presented with gradually increasing swelling at the anterior aspect of the right knee with deformity, anterior knee pain for 3 years, and difficulty in flexing the knee for 1 year. The pain was primarily activity-related. No history of relevant trauma. There was no any mass in other parts of the body. On examination there was a non-tender, irregular, bony hard swelling prominent over the medial aspect of the patella tendon, flexion restricted beyond 90 degrees.
Blood parameters were normal. Radiographs revealed a well-circumscribed, ovoid, corticated mass at the infrapatellar fat pad region. It was free from adjoining bones (Figure 1). Further radiological investigations not done due to financial constrain.
Figure 1. Preoperative clinical picture and radiograph.
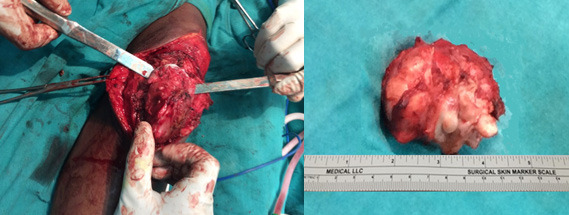
Clinico-radiologically, it was interpreted as benign and marginal excision was planned. Well circumscribed, intracapsular, and extrasynovial mass measuring about (6x4x3) cm excised through the medial parapatellar approach (Figure 2).
Figure 2. Intraoperative picture of marginal resection and excised mass.
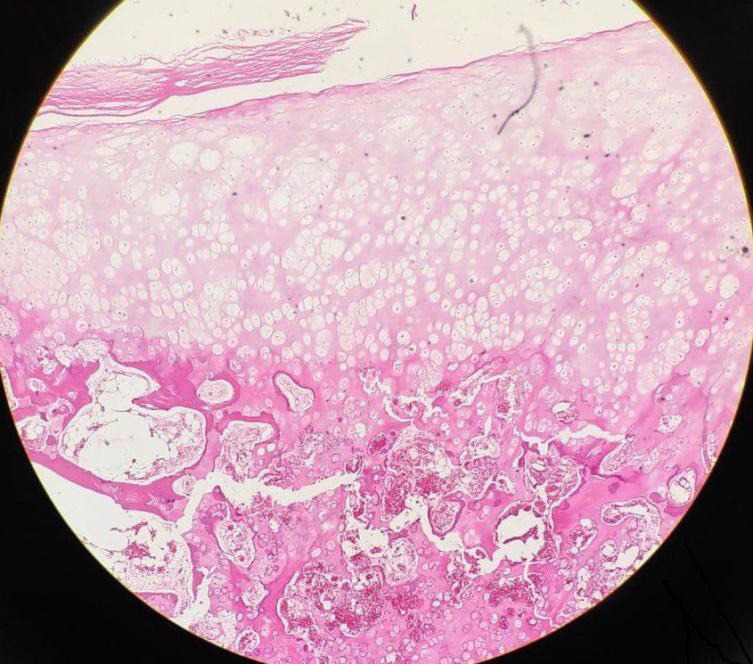
Histology revealed cartilaginous tissue with scattered enchondral ossification within, surrounded by capsular fibrous tissue. There was no evidence of malignant features (Figure 3). The pathological features were diagnostic of extraskeletal para-articular osteochondroma.
Figure 3. Histopathological picture showing cartilaginous tissue with scattered enchondral ossification and fibrous capsular tissue.
Postoperatively knee mobilization and weight-bearing allowed as tolerated. Knee was pain-free, with complete recovery of range of motion on subsequent follow-up. There was no clinico-radiological evidence of recurrence at 1 year follow-up (Figure 4).
Figure 4. Immediate and 1 year follow-up radiographs.

DISCUSSION
Extraskeletal osteochondroma is very rare. There are 3 different types of extraskeletal osteochondroma: a) synovial chondromatosis, b) soft tissue chondroma and c) para-articular osteochondroma. In synovial chondromatosis, multiple intrasynovial osteocartilaginous nodules are seen as loose bodies. Soft tissue chondromas are usually seen at hands and feet. According to Reith et al, a lesion is called paraarticular osteochondroma if: (a) the lesion presents as a single, dominant mass, both radiographically and grossly; (b) the mass consists histopathologically both bone and cartilage, organized in a manner similar to conventional osteochondromas; and (c) the lesion is not intra-articular, that is, it does not arise within the synovial lining of a joint.1-3
Para-articular osteochondroma usually manifests in joints with a potential capsular space, such as the patellofemoral joint or infrapatellar Hoff's fat pad, although they may occur in other regions too.1,4,5 It may occur at any age, but most of them are reported at 3060 years.1,6,7 This is case of 19 years gentleman, with a solitary mass in the infrapatellar region lined by joint capsule externally and synovial membrane internally with no evidence of underlying bone continuity. Radiographs usually reveal a single, marginated bony mass with internal trabeculae. Histopathologically, mass is characterized by enchondral ossification surrounded by hyaline cartilage, fibrous and adipose tissue. So, the most appropriate term to define this lesion is "para-articular, extrasynovial osteochondroma". Similar clinico-radiological and histopathological findings are seen in other case reports on extraskeletal osteochondroma.1-4,8-10
The exact pathogenesis is still unknown, but it is supposed to be due to osteocartilaginous metaplasia of the articular or para-articular connective tissue, or metaplasia of Hoffa's fat pad due to trauma, or sequel of end-stage of Hoffa's disease (chronic impingement of Hoffa's fat pad). So, in this case, the pathogenesis is not relatable to a mechanical post-traumatic event or chronic impingement of Hoffa's fat pad but to primary osteocartilaginous metaplasia of infrapatellar fat pad.1,2,4,5
CT scan and MRI were not done due to financial constrain, which is the limitation of this case report. Clinically and radiographically, the tumor was interpreted as benign, so we planned marginal resection and sent for histopathological examination which confirmed our diagnosis. Marginal resection is the treatment of choice, especially for para-articular osteochondroma.2,3,6 There is no known recurrence of the lesions after complete resection.1,3,11
Para-articular extrasynovial osteochondroma is an unusual lesion that commonly arises around the knee joint, particularly the infrapatellar Hoffa's fat pad due to the osteocartilaginous metaplasia of capsule and adjoining connective tissues. Clinico-radiological examinations are often diagnostic but integrated radio-pathological examination helps to distinguish it from other differentials. Marginal resection is the treatment of choice and these lesions are not known to recur.
Consent:
JNMA Case Report Consent Form was signed by the patient and the original article is attached with the patient's chart.
Conflict of Interest
None.
REFERENCES
- 1.Sen D, Satija L, Kumar KS, Rastogi V, Sunita BS. Giant intra-articular extrasynovial osteochondroma of the Hoffa's fat pad. Med J Armed Forces India. 2015;71:S8–11. doi: 10.1016/j.mjafi.2012.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rizzello G, Franceschi F, Meloni MC, Cristi E, Barnaba SA, Rabitti C, et al. Para-articular Osteochondroma of the Knee. Arthroscopy. 2007;23(8):910e1–4. doi: 10.1016/j.arthro.2006.05.030. [DOI] [PubMed] [Google Scholar]
- 3.Oliva F, Marconi A, Fratoni S, Maffulli N. Extra-osseous osteochondroma-like soft tissue mass of the patello-femoral space. BMC Musculoskelet Disord. 2006;7:1–6. doi: 10.1186/1471-2474-7-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ingabire MI, Deprez FC, Bodart A, Puttemans T. Soft tissue chondroma of Hoffa's fat pad. Jbr-Btr. 2012;95(1):15–7. doi: 10.5334/jbr-btr.72. [DOI] [PubMed] [Google Scholar]
- 5.De Maio F, Bisicchia S, Potenza V, Caterini R, Farsetti P. Giant intra-articular extrasynovial osteochondroma of the knee: a report of two cases. Open Orthop J. 2011;5(1):368–71. doi: 10.2174/1874325001105010368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hung JY, Huang GS, Peng YJ, Wu SS, Chao KH. Fat-pad osteochondroma of the knee. Journal of Medical Sciences. 2005;25(6):315–7. [Google Scholar]
- 7.Turhan E, Doral MN, Atay AÖ, Demirel M. A giant extrasynovial osteochondroma in the infrapatellar fat pad: End stage Hoffa's disease. Arch Orthop Trauma Surg. 2008;128(5):515–9. doi: 10.1007/s00402-007-0397-5. [DOI] [PubMed] [Google Scholar]
- 8.Sivrioglu AK, Ozyurek S, Incedayi M, Mutlu H. A rarely diagnosed cause of anterior knee pain: Hoffa's disease. BMJ Case Rep. 2013:1–2. doi: 10.1136/bcr-2013-008795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mulcahy H, Hoch B. An extraskeletal para-articular osteochondroma of Hoffa's fat pad. Radiol Case Reports. 2010;5(4):420. doi: 10.2484/rcr.v5i4.420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Demir MK, Unlu E, Usta U. A curious mass of the anterior compartment in the knee. Br J Radiol. 2009;82(977):435–7. doi: 10.1259/bjr/26981441. [DOI] [PubMed] [Google Scholar]
- 11.Mozella A de P, da Silveira Moller JV, de Araujo Barros Cobra HA. Tumor formation in Hoffa's infrapatellar fat: Case report [Internet]. Rev Bras Ortop. 2015;50(1):117–21. doi: 10.1016/j.rboe.2015.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Evaniew N, Bayegan D, Popovic S, Parasu N, Ghert M. Infrapatellar fat pad osteochondroma: three cases and a systematic review. J Knee Surg. 2015;28(3):229–38. doi: 10.1055/s-0034-1378192. [DOI] [PubMed] [Google Scholar]