

Abstract
Introduction
Nearly all (94%‐99%) pregnant persons in developed countries search for pregnancy‐related information online. The advent of the novel coronavirus disease 2019 (COVID‐19) and the associated restrictions in hospital policies may have pushed pregnant persons in the United States to consider giving birth at home to achieve their desired birth experience.
Methods
Google Trends is an open, rich source of real‐time, anonymized, relative data on disease patterns and population behavior that provides data in the form of search volume index (SVI): the search volume for a queried term relative to overall search volume for a given time frame and geographic location. The SVI is normalized to a scale of 0 to 100. After the World Health Organization declared COVID‐19 a pandemic on March 11, 2020, Google Trends was queried on February 21, 2021, for the search term home birth with location set to the United States and the time frame March 11, 2019 to February 21, 2021.
Results
The median SVI for home birth during nominally pre‐COVID‐19 baseline (weeks of March 17, 2019 to March 8, 2020) was relatively constant at 43 (range, 25‐56) and increased sharply to 77 during the week of March 15, to 86 during the week of March 22, and peaked at 100 during the week of March 29, 2020. The SVI declined substantially in the following weeks but remained significantly elevated compared with baseline levels. During the approximate 2‐year period of query, the states with the highest SVI values (≥80) were Arkansas, Washington, Montana, and Georgia.
Discussion
Interest in home birth spiked in the United States immediately after COVID‐19 was declared a pandemic and remained significantly elevated thereafter. These results have implications for caregivers and health systems to ensure safe pregnancies and childbirths through the resolution of the ongoing pandemic.
Keywords: SARS‐CoV‐2, novel coronavirus, COVID‐19, pandemic, home birth, pregnancy, childbirth
INTRODUCTION
Infection with novel coronavirus, named severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2), was first reported during December 2019 in Wuhan, China, and subsequently spread globally. 1 The World Health Organization declared coronavirus disease 2019 (COVID‐19) a pandemic on March 11, 2020. 2 To contain the person‐to‐person spread of the virus, physical distancing measures were put in place in many countries. Beginning in mid‐March 2020, governors across the United States issued stay‐at‐home or shelter‐in‐place orders with closure of nonessential businesses. 3 As of September 23, 2021, according to data from Johns Hopkins University, more than 230 million cases of COVID‐19 have been reported globally, with the largest number of cases (approximately 42.6 million [18%]) reported from the United States; among 4,721,803 deaths globally, 681,259 (14%) were from the United States. 4
The impact of COVID‐19 on pregnant and postpartum persons is not well characterized. Some systematic reviews of primarily case reports and case series appeared initially, mostly based on experience from early geographic locations of COVID‐19. 5 , 6 , 7 As of September 2021, pregnant women who were infected with COVID‐19 were considerably more likely to develop more serious symptoms, be admitted to an intensive care unit, receive extracorporeal membrane oxygenation or invasive ventilation, or die, compared with nonpregnant women. 8 , 9 Furthermore, pregnant women with COVID‐19 may face a greater risk of adverse pregnancy outcomes, including preterm birth. 10
QUICK POINTS
-
✦
Pregnant persons with coronavirus disease 2019 (COVID‐19) are at increased risk of adverse outcomes.
-
✦
Home birth can be one way to have a desired birthing experience and avoid potential exposure to COVID‐19 during the pandemic.
-
✦
Analysis of Google Trends data shows that the interest in home birth significantly increased in the United States immediately after COVID‐19 was declared a pandemic.
-
✦
Following the initial surge, the interest in home birth declined but continued to remain significantly higher than pre‐COVID‐19 levels.
-
✦
These findings have implications for caregivers and health systems in ensuring childbirth that is both safe and consistent with the desired experience of the pregnant person.
Early reports of a significant proportion of asymptomatic pregnant women in New York City hospitals who later tested positive for COVID‐19 11 led to hospitals limiting the exposure of hospital staff. For example, the number of individuals accompanying patients into labor and birth rooms was limited to no more than one, with additional restrictions that the individual could not leave and reenter or be replaced with another individual. 12 Although similar restrictions limiting accompanying family members were also in place in other departments of the hospital, for pregnant persons planning their birth experience as a culmination of their pregnancy, this was particularly disappointing. These initial restrictions were later relaxed to allow additional support persons and extend the duration of support. 13 During the spring of 2020, there was confusion about whether to keep newborns with their mothers with suspected or confirmed COVID‐19; early guidelines recommended separating newborns from such mothers for at least 14 days. 14 Since then, evidence has suggested that the risk of newborns acquiring COVID‐19 from mothers is low, regardless of whether the newborn stays in the same room as the mother or is separated, and the Centers for Disease Control and Prevention now recommends that mothers should discuss with their health care providers to decide whether to room‐in or separate their newborns. 15
Some pregnant persons may have reduced access to health care providers because of office closures for nonessential visits or fewer prenatal visits to limit physical contact. Access may also be reduced because of societal and economic factors such as reduced public transportation services or loss of job and health insurance. Pregnant women were reported to be apprehensive about entering the hospital building for their labor and birth, with a sense of isolation and uncertainty whether they would be able to fulfill their desired birthing experience. 16
Although not without risk, home birth can be one way to circumvent the hospital system for both prenatal care and birth, comply with stay‐at‐home recommendations, have a desired birthing experience, and avoid potential exposure to novel coronavirus during the pandemic. However, insurance coverage for home births is not uniform in the United States. Private insurance companies may not cover home births, and the coverage by Medicaid, which pays for approximately 40% of United States childbirths, varies by state. 17 , 18 As a result, individuals who decide to give birth at home may be required to bear the associated expenses on their own. 19 These factors could influence the risk‐benefit evaluation of home versus hospital birth.
Internet search data offer a unique and real‐world perspective on how the thinking of individuals and communities evolve as major health‐related events unfold. A home birth, which would limit the potential exposure to SARS‐CoV‐2 and allow participation of a pregnant person's full support network, could be more appealing to some than birth in a hospital setting, especially early in a public health event when the risks to a pregnant person and/or child are unknown. In the United States, only approximately 1% of women give birth at home. 20 Many factors influence the choice of birth location such as attitude toward medical interventions, the potential to manage labor pain with medications, the opportunity to give birth in a preferred position, and the potential risks and benefits of both settings. The primary aim of this study was to assess the level of interest in giving birth at home in the United States since COVID‐19 was declared a pandemic by analyzing Google Trends data. Considering the differences in the number of cases and deaths due to COVID‐19 among different states, a secondary aim of the study was to assess the interest in home birth in different geographies within the United States.
METHODS
This was a retrospective, observational Google Trends study. Google Trends is a publicly available online tool that provides real‐time (up to 36 hours before the search is conducted) and archived information on anonymous user queries since 2004. 21 It allows selecting geography, time frame, and category of search, and the results are reported as search volume index (SVI), defined as the search volume for a queried term relative to the overall search volume for a given time frame and geographic location. 22 , 23 The SVI is normalized to a scale of 0 to 100, where 100 corresponds to the peak popularity within the specified period and geography and all other values represent a proportion of comparative popularity; the numbers are not the absolute counts or volume. 24 The process excludes queries that are made over a short time frame from the same internet protocol address and queries that contain special characters. 22 Because Google Trends data are anonymized and available publicly, approval by an institutional review board was not considered necessary.
Google Trends was queried on February 21, 2021, for the search term home birth, with the geography set to United States, time frame March 11, 2019 to February 21, 2021 (weeks of March 17, 2019 to February 14, 2021), and no restrictions set for category (“All” was selected to be inclusive). The data within Google Trends are updated every Sunday, which includes all search data during the preceding 7 days. This means that the data for the weeks of March 17, 2019 to February 14, 2021, actually include data from March 11, 2019 to February 14, 2021. Our search time frame included 12 months before COVID‐19 was declared a pandemic to account for any seasonal variations. The query process followed the checklist for documentation of Google Trends data described previously, which incorporates search variables, search inputs, and rationales for search strategy. 25 The search term home birth was selected after performing a preliminary unrestricted Google Trends search for the terms home birth, home delivery, natural delivery, home birth kit, birthing center, birth center, natural birth, and natural childbirth based on the authors’ medical and lay perspectives for search terms. Home birth appeared to most closely represent the concept in question based on the “Related topics” and the “Related queries” that were generated by Google Trends. The search term birth center was also explored as a comparison to home birth.
Search results by Subregion, Metro, and City were also explored. Subregions of the United States returned results at the state level, which included the District of Columbia. Google Trends defines Metros as geographical areas that generally correspond to metropolitan areas. 26 City results are names of cities in the United States. The terms City and Metro are defined by Google; the parameters used to define these terms are not publicly disclosed.
Statistical Analyses
For statistical comparisons, the SVI data were separated into 3 periods: nominal pre‐COVID‐19 period or baseline (52 weeks from the weeks of March 17, 2019 to March 8, 2020), COVID‐19 onset period or phase 1 (12 weeks from the weeks of March 15 to May 31, 2020), and post‐COVID‐19 onset period or phase 2 (37 weeks from the weeks of June 7, 2020 to February 14, 2021). The pairwise comparisons were performed using the nonparametric Kruskal‐Wallis test. Trends over time within each period were analyzed using the nonparametric Mann‐Kendall trend test, where directionality was indicated by Kendall's tau (τ). 27 The data analysis was conducted using SAS/STAT software version 14.3 (Proc NPAR1WAY for the Kruskal‐Wallis test and Proc CORR for the Mann‐Kendall trend test) of the SAS system (Cary, North Carolina). Statistical significance was determined at the α = .05 level.
RESULTS
A Google Trends search for the term home birth on February 21, 2021 showed that the weekly SVI was relatively constant during the nominal pre‐COVID‐19 baseline period (weeks of March 17, 2019 to March 8, 2020) (Figure 1). Following the World Health Organization declaration of the COVID‐19 pandemic on March 11, 2020, the SVI increased sharply in the next 3 weeks to reach the maximum (100) during the week of March 29, 2020, and then gradually declined during the rest of the COVID‐19 phase 1 (12 weeks from the weeks of March 15 to May 31, 2020). In the COVID‐19 phase 2 (37 weeks from the weeks of June 7, 2020 to February 14, 2021), the SVI remained relatively unaltered but at a level higher than during the baseline period. The median (range) SVI was 43.0 (25‐56) during the baseline period, increased to 70.5 (55‐100) during COVID‐19 phase 1, and then declined to 49.0 (38‐69) during COVID‐19 phase 2 (Figure 2). The mean SVI values were very close to the median values. Kruskal‐Wallis pairwise comparisons showed a significant increase from baseline to COVID‐19 phase 1, a significant decline from COVID‐19 phase 1 to phase 2, and significantly higher levels during COVID‐19 phase 2 compared with baseline (P < .001 for all comparisons). The Mann‐Kendall trends analysis showed that the interest in home birth was statistically unaltered during baseline (τ, −0.087; P = .37) and COVID‐19 phase 2 (τ, −0.053; P = .65); during COVID‐19 phase 1, the interest in home birth altered significantly, first increasingly rapidly over 3 weeks and then declining slowly over the next 9 weeks (τ for the 12‐week period, −0.576; P = .009).
Figure 1.
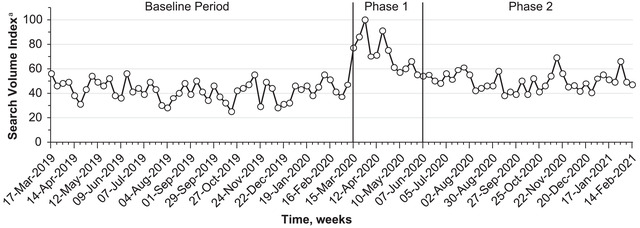
Search Volume Index for Home Birth in the United States During the Weeks of March 17, 2019, to February 14, 2021
Two vertical lines separate the baseline period (March 17, 2019 to March 8, 2020), COVID‐19 phase 1 (March 15 to May 31, 2020), and COVID‐19 phase 2 (June 7, 2020 to February 14, 2021).
aScoring is on a relative scale of 0 to 100 in which 100 represents the highest searched query as a fraction of total searches in that time and location and 50 represents the time and location where a query is searched half as often as the most popular query. A higher value represents a higher proportion among all queries, and not a higher absolute count of queries.
Data source: Google Trends (https://www.google.com/trends). Accessed February 21, 2021.
Figure 2.
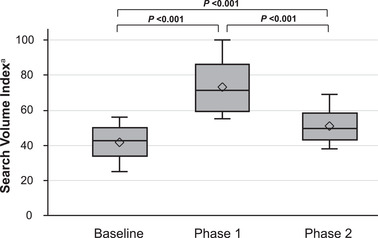
Search Volume Index for Home Birth in the United States in 3 Phases (Baseline, COVID‐19 Phase 1, COVID‐19 Phase 2)
Baseline period: March 17, 2019 to March 8, 2020; COVID‐19 phase 1: March 15 to May 31, 2020; and COVID‐19 phase 2: June 7, 2020 to February 14, 2021. The pairwise comparisons were performed using a Kruskal‐Wallis test. The horizontal line in each box represents median, diamond represents mean, lower and upper boundaries of each box represent 25% and 75% percentiles, and the error bars represent the full range of search volume indices.
aScoring is on a relative scale of 0 to 100 in which 100 represents the highest searched query as a fraction of total searches in that time and location and 50 represents the time and location in which a query is searched half as often as the most popular query. A higher value represents a higher proportion among all queries and not a higher absolute count of queries.
Data source: Google Trends (https://www.google.com/trends). Accessed February 21, 2021.
The states with the highest SVI values (≥80) were Arkansas, Washington, Montana, and Georgia (Figure 3). The Metro areas with the highest SVI values (≥80) were Greenville‐New Bern‐Washington (North Carolina), Charleston‐Huntington (West Virginia), Ft. Wayne (Indiana), Spokane (Washington), Waco‐Temple‐Bryan (Texas), Lexington (Kentucky), Columbia (South Carolina), Colorado Springs‐Pueblo (Colorado), Greenville‐Spartanburg (South Carolina)‐Asheville (North Carolina)‐Anderson (South Carolina), Shreveport (Louisiana), and Des Moines‐Ames (Iowa) (Figure 4; Supporting Information: Appendix S1). The data at City level revealed interest in 4 cities: New York (SVI of 100), Los Angeles (100), Houston (98), and Chicago (86). The top 7 associated queries in Google Trends related to home birth were at home birth, birth control, home birth midwife, midwife, home water birth, home birth cost, and giving birth at home. These associated queries were not used in the analysis.
Figure 3.
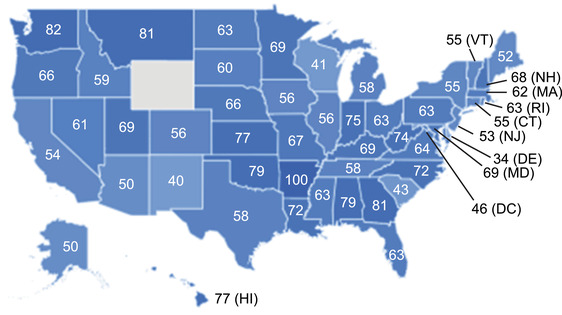
Search Volume Index by State for Home Birth in the United States During the Weeks of March 17, 2019 to February 14, 2021
Darker colors represent higher search volume index scores. The state with no color (Wyoming) denotes very low level of interest.
Data source: Google Trends (https://www.google.com/trends). Accessed February 21, 2021.
Figure 4.
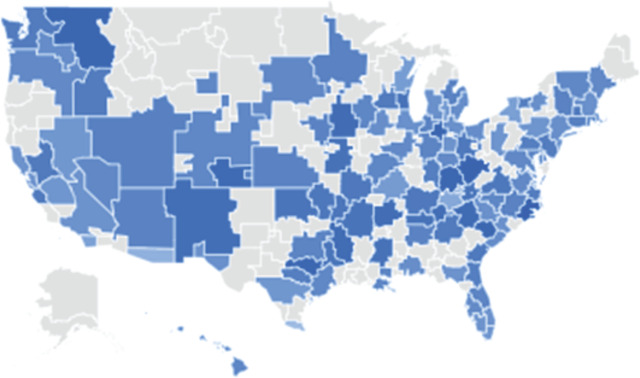
Search Volume Index by Metro Area for Home Birth in the United States During the Weeks of March 17, 2019 to February 14, 2021
Darker colors represent higher search volume index scores. The Metro areas with no color denote very low level of interest. Data source: Google Trends (https://www.google.com/trends). Accessed February 21, 2021.
To assess whether the SVI trends observed for home birth were specific to the COVID‐19 pandemic, we also ran a query for a related term birth center, keeping all other search parameters the same (Supporting Information: Appendix S2). The median SVI was 65 during baseline, 52.5 during COVID‐19 phase 1, and 57 during COVID‐19 phase 2. Within each period, the interest over time was consistent as determined by the Mann‐Kendall trend test (P = .45, .41, and .54 for the 3 periods). There was no significant difference (P = .49) in interest at baseline compared with COVID‐19 phase 2, significantly greater interest (P = .02) at baseline compared with COVID‐19 phase 1, and significantly less interest (P < .001) at COVID‐19 phase 1 compared with COVID‐19 phase 2.
DISCUSSION
Internet search has evolved into a rich source of real‐world and nearly real‐time health information, providing insights into patterns of disease and population behavior. Search engines are the most common method of obtaining information online, with 94%‐99% of women, primarily from the developed countries, searching for pregnancy‐related information at some time during pregnancy. 28 , 29 , 30 Google (Google Inc., Mountain View, California) is the leading search engine in the world, with 71% to 92% of the market share. 31 Google Trends, 32 the most popular tool employed for understanding trends in health issues using online data, was selected in this study to assess interest in home births. Google Trends has been used to study interest in a variety of health topics potentially affected by COVID‐19, such as suicide, plastic surgery, and gastrointestinal symptoms as predictors of COVID‐19. 33 , 34 , 35 To our knowledge, this is the first study assessing interest in home birth during the COVID‐19 pandemic using Google Trends.
This study revealed a sharp increase from baseline in the interest in home births in the United States in the weeks after COVID‐19 was declared a pandemic on March 11, 2020, which was followed by a sustained elevated interest in the subsequent months. For comparison, we looked at some popular terms available in Google Trends. For example, the SVI for the term royal baby in 2019 showed baseline levels near 0, peaking at 100 during the week of May 5, which coincided with birth of Prince Harry and Meghan Markle's baby Archie on May 6, followed by a rapid decline to baseline level of interest near 0. 36 , 37 Similarly, compared with the SVI for a related term birth center, the SVI for home birth was consistently lower before the declaration of the pandemic, became higher during the COVID‐19 phase 1, and then declined to be similar during the phase 2. Overall, these comparisons suggested that the term home birth reliably captured how the interest in this concept evolved in relation to the COVID‐19 pandemic. The results of this study, showing significantly increased interest in home birth following the declaration of the COVID‐19 pandemic, are consistent with an online survey conducted in April 2020 that showed a much higher preference among American women for home and birth center births (5.4%) compared with the pre‐COVID‐19 national average (1.6%). 38
The states with the highest SVI (Arkansas, Washington, Montana, and Georgia) were mostly rural. This is generally consistent with the location of perinatal care deserts, which exist primarily in rural counties; among women living in these areas, only 1 in 5 lives in a large metropolitan area or urban setting. 39 Notably, none of the states with the highest SVI were the ones with high numbers of COVID‐19 cases or deaths during COVID‐19 onset period (phase 1). Interestingly, 2 of these states (Arkansas and Georgia) had proportions of actual home births below the national average (0.99%) before COVID‐19. 20 Together, these observations suggest that the increased interest in home birth was not limited to regions primarily affected by the pandemic or those that had a higher incidence of home births before COVID‐19.
Childbirth at home has been transpiring since the beginning of humanity. Hospital birth has only become standard in the United States in the past approximately 100 years. 40 Almost all (>99%) childbirths in the United States occur in hospitals; an estimated approximately 0.9% (35,000) of childbirths occur at home every year, of which approximately one‐fourth are unplanned or unattended. 41 There are benefits and risks to births in both settings. Outcomes of home birth have been difficult to study in a randomized controlled trial setting, and many observational trials are limited by methodologic issues. Meta‐analyses demonstrate that, in low‐risk pregnancies, the risk of perinatal or neonatal mortality or morbidity does not differ between intended home or hospital births. 42 , 43 Planned hospital birth offers a safe and controlled setting with ready access to antibiotics, labor anesthesia, and rapid conversion to cesarean birth, if needed. Compared with planned hospital births, planned birth center and home births resulted in significantly fewer interventions such as labor induction or augmentation and cesarean or operative vaginal birth. 44 Planned home births are also associated with fewer perineal, vaginal, and severe lacerations and lower maternal infectious morbidity. 41
According to the American College of Obstetricians and Gynecologists (ACOG), these findings reflect that pregnant persons planning home births, many of whom are parous (ie, having given birth to one or more viable children), may have fewer obstetric risk factors compared with those planning hospital births. 41 With midwifery support and timely access to obstetric consultation and transfer to a nearby hospital, planned home birth may be a reasonable choice for pregnant persons with low obstetric risk, especially during the COVID‐19 pandemic. 45 However, some conditions such as prior cesarean birth, multiple gestation, and fetal malpresentation (eg, breech), all easily identifiable before labor, are deemed by the ACOG Committee on Obstetric Practice and American College of Nurse‐Midwives (ACNM) as absolute contraindications to planned home birth. 41 , 45
In conjunction with ACNM, the American Academy of Family Physicians, and the Society for Maternal Fetal Medicine, ACOG recently released a statement reiterating that during the COVID‐19 pandemic, “Hospitals and birth centers that are both licensed and accredited remain safe places to give birth in the United States.” 46 Increased interest in home birth in the United States during the COVID‐19 pandemic suggests a need for prenatal care providers to proactively bring up the topic of home births in the context of the pandemic. An open and collaborative dialogue between patients and health care providers about benefits and risks of both home and hospital births, including insurance coverage, is needed during a public health crisis. Policymakers should consider coverage of home birth with midwifery support, especially in perinatal care deserts. It remains to be seen whether increased interest in home birth will lead to increased rates of home births in the United States.
The strengths of this study include rapid, real‐time assessment of what people are interested in, ability to compare geographic regions, and data anonymity. Higher SVI in specific states can allow early interventions in those areas. Individuals may feel less hesitant to search topics of their interest on the internet rather than or before speaking with a health care professional. Faced with the lack of clear maternal clinical guidance, expectant parents may actively seek information on the internet to guide their decisions. The study limitations include inability to fully identify the demography of those interested in home birth, specific factors leading to increase in relative interest (eg, access to care, loss of job and health insurance, and fear and anxiety), potential bias in the studied population, and the presentation of geographical results across the entire time frame of the study. Nonavailability of information on race, ethnicity, age, or any comorbidity (because of the fact that Google Trends data is anonymous) limited the ability to fully understand which specific interventions or educational support could add value. Search term misidentification is another potential limitation. We addressed this by first conducting a preliminary unrestricted Google Trends query on several related terms. A review of the related queries strongly suggested that the term home birth used in this study reflected interest in giving birth to a newborn at home. By using Google Trends, an internet‐based tool, we may have excluded people who do not have easy internet access, potentially introducing bias into our study population. A final limitation is that the results by geography were conducted across the entire time frame of the study, rather than broken down by phases, which could have masked changes within geographical areas. Despite these limitations, the results of this study reveal that home births are of elevated interest during these unprecedented times.
CONCLUSION
Interest in home birth spiked in the United States immediately after COVID‐19 was declared a pandemic and remained significantly elevated. These results have implications for caregivers, health systems, and policymakers to ensure safe pregnancies and desirable childbirth experience until the full resolution of the ongoing pandemic. Caregivers should encourage an open dialogue with patients about benefits and risks of home and hospital births.
CONFLICT OF INTEREST
R.J.C. and S.N. are employees of Johnson & Johnson and may own company stocks and/or stock options. A.C.F. is a former employee of and former consultant for Johnson & Johnson and owns company stocks.
Supporting information
Table S1. Search volume index for home birth by metro area in the United States between the weeks of March 17, 2019 and February 14, 2021.
Figure S1. Search volume index over time for the search terms home birth (empty circles) and birth center (filled circles) in the United States during the weeks of March 17, 2019 to February 14, 2021
ACKNOWLEDGMENTS
This work was supported by Johnson & Johnson. The authors thank Mariana Coelho for her early contribution to the study. Writing assistance was provided by Narender Dhingra, MBBS, PhD, CMPP, and Allison Marin, PhD, both of System One, and funded by Janssen Global Services, LLC. This study was presented at the American Academy of Family Physicians Family Medicine Experience Meeting; September 28‐October 2, 2021; Anaheim, California.
Ru‐fong J. Cheng: https://orcid.org/0000‐0003‐2564‐0947
Alan C. Fisher: https://orcid.org/0000‐0003‐3663‐7508
Susan Nicholson: https://orcid.org/0000‐0003‐4989‐1986
REFERENCES
- 1. Outbreak of pneumonia of unknown etiology (PUE) in Wuhan, China. Centers for Disease Control and Prevention. Accessed March 29, 2021. https://emergency.cdc.gov/han/HAN00424.asp
- 2. Cucinotta D, Vanelli M. WHO declares COVID‐19 a pandemic. Acta Biomed. 2020;91(1):157‐160. 10.23750/abm.v91i1.9397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mervosh S, Lu D, Swales V. See which states and cities have told residents to stay at home. The New York Times. Accessed March 29, 2020. https://www.nytimes.com/interactive/2020/us/coronavirus‐stay‐at‐home‐order.html
- 4.COVID‐19 dashboard by the Center for Systems Science and Engineering. Johns Hopkins University Coronavirus Resource Center . Accessed September 23, 2021. https://coronavirus.jhu.edu/map.html
- 5. Juan J, Gil MM, Rong Z, Zhang Y, Yang H, Poon LC. Effect of coronavirus disease 2019 (COVID‐19) on maternal, perinatal and neonatal outcome: systematic review. Ultrasound Obstet Gynecol. 2020;56(1):15‐27. 10.1002/uog.22088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Yang Ziyi, Wang Min, Zhu Ziyu, Liu Yi. Coronavirus disease 2019 (COVID‐19) and pregnancy: a systematic review. The Journal of Maternal‐Fetal & Neonatal Medicine. 2020; 10.1080/14767058.2020.1759541 [DOI] [PubMed] [Google Scholar]
- 7. Galang RR, Chang K, Strid P, et al. Severe coronavirus infections in pregnancy: a systematic review. Obstet Gynecol. 2020;136(2):262‐272. 10.1097/AOG.0000000000004011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Ellington S, Strid P, Tong VT, et al. Characteristics of women of reproductive age with laboratory‐confirmed SARS‐CoV‐2 infection by pregnancy status—United States, January 22–June 7, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(25):769–775. 10.15585/mmwr.mm6925a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Zambrano LD, Ellington S, Strid P, et al. Update: characteristics of symptomatic women of reproductive age with laboratory‐confirmed SARS‐CoV‐2 infection by pregnancy status ‐ United States, January 22‐October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(44):1641‐1647. 10.15585/mmwr.mm6944e3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Investigating the impact of COVID‐19 during pregnancy. Centers for Disease Control and Prevention. Accessed March 29, 2021. https://www.cdc.gov/coronavirus/2019‐ncov/cases‐updates/special‐populations/pregnancy‐data‐on‐covid‐19/what‐cdc‐is‐doing.html
- 11. Sutton D, Fuchs K, D'Alton M, Goffman D. Universal screening for SARS‐CoV‐2 in women admitted for delivery. N Engl J Med. 2020;382(22):2163‐2164. 10.1056/NEJMc2009316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. New York State Department of Health Pregnancy and COVID‐19 resources for health care providers. March 21, 2020. Accessed March 29, 2021. https://coronavirus.health.ny.gov/system/files/documents/2020/03/covid‐19pregnancyguidanceforproviders3.21.20.pdf
- 13. Secretary to the Governor Melissa DeRosa issues report to Governor Cuomo outlining the COVID‐19 Maternity Task Force's initial recommendations. 2020. New York State website. Accessed March 29, 2021. https://www.governor.ny.gov/news/secretary‐governor‐melissa‐derosa‐issues‐report‐governor‐cuomo‐outlining‐covid‐19‐maternity
- 14. Martin N. What coronavirus means for pregnancy, and other things new and expecting mothers should know. ProPublica. March 19, 2020. Accessed March 29, 2021. https://www.propublica.org/article/coronavirus‐and‐pregnancy‐expecting‐mothers‐q‐and‐a
- 15. Evaluation and management considerations for neonates at risk for COVID‐19. Updated December 8, 2020. Centers for Disease Control and Prevention . 2020. Accessed March 9, 2021. https://www.cdc.gov/coronavirus/2019‐ncov/hcp/caring‐for‐newborns.html
- 16. de Freytas‐Tamura K Pregnant and scared of 'Covid Hospitals,' they're giving birth at home. The New York Times. April 24, 2020. Accessed March 29, 2021. https://www.nytimes.com/2020/04/21/nyregion/coronavirus‐home‐births.html
- 17. Martin JA, Hamilton BE, Osterman MJK, Driscoll AK. Births: final data for 2018. Natl Vital Stat Rep. 2019;68(13):1‐47. [PubMed] [Google Scholar]
- 18. Gifford K, Walls J, Ranji U, Salganicoff A, Gomez I. Medicaid Coverage of April 2017 Pregnancy and Perinatal Benefits: Results from a State Survey . Henry J. Kaiser Family Foundation; 2017. Accessed September 19, 2021. https://files.kff.org/attachment/Report‐Medicaid‐Coverage‐of‐Pregnancy‐and‐Perinatal‐Benefits
- 19. Thayer Z. U.S. coronavirus advice is failing pregnant women. Sapiens. May 21, 2020. Accessed March 29, 2021. https://www.sapiens.org/biology/covid‐19‐and‐childbirth/
- 20. MacDorman MF, Declercq E. Trends and state variations in out‐of‐hospital births in the United States, 2004‐2017. Birth. 2019;46(2):279‐288. 10.1111/birt.12411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Mavragani A, Ochoa G. Google Trends in infodemiology and infoveillance: methodology framework. JMIR Public Health Surveill. 2019;5(2):e13439. 10.2196/13439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. FAQ about Google Trends data. Accessed March 29, 2021. https://support.google.com/trends/answer/4365533?hl=en
- 23. Dreher PC, Tong C, Ghiraldi E, Friedlander JI. Use of Google Trends to track online behavior and interest in kidney stone surgery. Urology. 2018;121:74‐78. 10.1016/j.urology.2018.05.040 [DOI] [PubMed] [Google Scholar]
- 24. How to use Google Trends for SEO. FATJOE. Accessed March 29, 2021. https://fatjoe.com/google‐trends/
- 25. Nuti SV, Wayda B, Ranasinghe I, et al. The use of Google Trends in health care research: a systematic review. PLoS One. 2014;9(10):e109583. 10.1371/journal.pone.0109583 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Google Trends help. Accessed March 29, 2021. https://support.google.com/trends/answer/4355212?hl=en#:~:text=Metros%20are%20geographical%20areas%20that,provides%20metros%20for%20some%20countries.&text=Open%20Google%20Trends.,term%2C%20like%20%E2%80%9Candroid.%E2%80%9D
- 27. Lehman EL. Nonparametrics: Statistical Methods Based on Ranks. San Francisco, CA: Holden‐Day, Inc.; 1975. [Google Scholar]
- 28. Declercq ER, Sakala C, Corry MP, Applebaum S, Herrlich A. Listening to MothersSM III: Pregnancy and Birth. Report of the Third National U.S. Survey of Women's Childbearing Experiences. Childbirth Connection; 2013. Accessed March 29, 2021. https://www.nationalpartnership.org/our‐work/resources/health‐care/maternity/listening‐to‐mothers‐iii‐pregnancy‐and‐birth‐2013.pdf [Google Scholar]
- 29. Huberty J, Dinkel D, Beets MW, Coleman J. Describing the use of the internet for health, physical activity, and nutrition information in pregnant women. Matern Child Health J. 2013;17(8):1363‐1372. 10.1007/s10995-012-1160-2 [DOI] [PubMed] [Google Scholar]
- 30. Lagan BM, Sinclair M, Kernohan WG. Internet use in pregnancy informs women's decision making: a web‐based survey. Birth. 2010;37(2):106‐115. 10.1111/j.1523-536X.2010.00390.x [DOI] [PubMed] [Google Scholar]
- 31. Chris A. Top 10 search engines in the world. Accessed March 29, 2021. https://www.reliablesoft.net/top‐10‐search‐engines‐in‐the‐world/
- 32. Explore what the world is searching. Google Trends . Accessed March 29, 2021. https://trends.google.com/trends/?geo=US
- 33. Ahmad I, Flanagan R, Staller K. Increased internet search interest for GI symptoms may predict COVID‐19 cases in US hotspots. Clin Gastroenterol Hepatol. 2020;18(12):2833‐2834 e3. 10.1016/j.cgh.2020.06.058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Ayers JW, Poliak A, Johnson DC, et al. Suicide‐related internet searches during the early stages of the COVID‐19 pandemic in the US. JAMA Netw Open. 2021;4(1):e2034261. 10.1001/jamanetworkopen.2020.34261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Duggan RP, Tran JP, Phillips LG. Interest in plastic surgery during COVID‐19 pandemic: a Google Trends analysis. Plast Reconstr Surg Glob Open. 2020;8(10):e3268. 10.1097/GOX.0000000000003268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. BBC News . Royal baby: All you need to know about the birth of Harry and Meghan's child. Accessed March 29, 2021. https://www.bbc.com/news/uk‐47934729#:~:text=When%20was%20the%20baby%20born,7lbs%203oz%20(3.2kg)
- 37. Google Trends Explore. Search term: royal baby. Accessed March 29, 2021. https://trends.google.com/trends/explore?date=2019‐01‐01%202019‐12‐31&q=Royal%20baby&geo=US
- 38. Gildner TE, Thayer ZM. Birth plan alterations among American women in response to COVID‐19. Health Expect. 2020;23(4):969‐971. 10.1111/hex.13077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. March of Dimes . Nowhere to Go: Maternity Care Deserts Across the U.S. 2018. Accessed March 29, 2021. https://www.marchofdimes.org/materials/Nowhere_to_Go_Final.pdf [Google Scholar]
- 40. McCool WF, Simeone SA. Birth in the United States: an overview of trends past and present. Nurs Clin North Am. 2002;37(4):735‐746. 10.1016/s0029-6465(02)00020-8 [DOI] [PubMed] [Google Scholar]
- 41.Committee on Obstetric Practice. Committee opinion No. 697: planned home birth. Obstet Gynecol. 2017;129(4):e117‐e122. 10.1097/aog.0000000000002024 [DOI] [PubMed] [Google Scholar]
- 42. Hutton EK, Reitsma A, Simioni J, Brunton G, Kaufman K. Perinatal or neonatal mortality among women who intend at the onset of labour to give birth at home compared to women of low obstetrical risk who intend to give birth in hospital: a systematic review and meta‐analyses. EClinicalMedicine. 2019;14:59‐70. 10.1016/j.eclinm.2019.07.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Rossi AC, Prefumo F. Planned home versus planned hospital births in women at low‐risk pregnancy: a systematic review with meta‐analysis. Eur J Obstet Gynecol Reprod Biol. 2018;222:102‐108. 10.1016/j.ejogrb.2018.01.016 [DOI] [PubMed] [Google Scholar]
- 44. Snowden JM, Tilden EL, Snyder J, Quigley B, Caughey AB, Cheng YW. Planned out‐of‐hospital birth and birth outcomes. N Engl J Med. 2015;373(27):2642‐2653. 10.1056/NEJMsa1501738 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.American College of Nurse‐Midwives. Midwifery provision of home birth services. J Midwifery Womens Health. 2016;61(1):127‐133. 10.1111/jmwh.12431 [DOI] [PubMed] [Google Scholar]
- 46. Patient‐centered care for pregnant patients during the COVID‐19 pandemic. The American College of Obstetricians and Gynecologists. Accessed March 29, 2021. https://www.acog.org/news/news‐releases/2020/03/patient‐centered‐care‐for‐pregnant‐patients‐during‐the‐covid‐19‐pandemic
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Search volume index for home birth by metro area in the United States between the weeks of March 17, 2019 and February 14, 2021.
Figure S1. Search volume index over time for the search terms home birth (empty circles) and birth center (filled circles) in the United States during the weeks of March 17, 2019 to February 14, 2021