

Abstract
Aim
To test a model that examines the direct and indirect effects of work‐related stress on job‐related affective well‐being through compassion fatigue.
Background
Despite the danger of infection, nurses' dedication to their work appears to be an innate desire to provide care for patients with COVID‐19. Nonetheless, the universal effort to control the outbreak has led to extended work hours and workload, which has been defined as the primary contributor to work‐related stress among nurses and might impact their job‐related affective well‐being.
Method
We used a cross‐sectional exploratory design. Data were collected using an online survey from 161 nurses working in the Saudi health care system. The survey included obtaining information on demographics and work‐related stress using Professional Quality of Life Scale version 5 to measure compassion fatigue as well as a job‐related affective well‐being scale.
Results
Work‐related stress had significant negative direct effects on job‐related affective well‐being and positive effects on compassion fatigue. Compassion fatigue had significantly negative direct effects on job‐related affective well‐being. Work‐related stress exerted negative indirect effects on job‐related affective well‐being through compassion fatigue, which partially mediated the relationship.
Conclusion
The findings supported the model and added to our understanding regarding the impact of work‐related stress on nurses.
Implications for Nursing Management
Stress reduction is an important element in improving staff outcomes as well as job‐related affective well‐being.
Keywords: burnout, compassion fatigue, job‐related affective well‐being, secondary traumatic stress, work‐related stress
1. BACKGROUND
In March 2020, the World Health Organization announced the outbreak of the coronavirus disease (COVID‐19), which eventually turned into a pandemic (World Health Organization, 2020). The first cases were reported in Wuhan City, China, and shortly after, a steady increase in COVID‐19 cases occurred within and outside China. Globally, more than 445 million people have been infected, and more than six million have died (Worldometer, 2022). Just like in any pandemic outbreaks, health care systems work to contain the outbreak by preventing disease transmission and treating as well as alleviating the suffering of the infected patients (World Health Organization, 2014). Nurses are the largest number of health care providers and are at the frontline to face COVID‐19 outbreaks (Choi et al., 2020). Despite the danger of infection, nurses' dedication to their work appears to be an innate desire to provide care for patients with COVID‐19 (Natividad et al., 2021). Nonetheless, the universal effort to control the outbreak leads to higher work hours and workload, which has been defined as the primary contributor to work‐related stress among nurses (Alenezi et al., 2018; Duarte et al., 2020; Hoedl et al., 2021).
Work‐related stress has been defined in the literature as an arduous experience exacerbated by an employee's work and includes tension at the physical, mental and emotional levels (Alanazi et al., 2019; Alenezi et al., 2018). Work organization, work design, organizational cultural, time limits, patient demands, lack of social support and a sense of inadequate coping are components that contribute to the contemporary social hazard of work‐related stress (Pai Vernekar & Shah, 2018; Wang et al., 2020). Occasionally, job stress has a positive influence on people's motivation; however, it usually has adverse effects on their physical and psychological well‐being, which then undermine job satisfaction (Lee et al., 2019). Thus, during the COVID‐19 pandemic, several studies have aimed to identify sources of work‐related stress. Nurses' sociodemographic characteristics, such as age, sex, marital status, and nationality, as well as work‐related characteristics, such as position, average working hours per week, working area, inadequate staff, performing procedures that patients experience as painful, and lack of drugs and equipment required for nursing care (Alenezi et al., 2018; D'Emeh et al., 2021; Elkholy et al., 2021) have been found to be significant contributors to work‐related stress. During the COVID‐19 pandemic, the presence of a fear of being infected with COVID‐19, transmitting the infection to family members, and the absence of a cure for the disease were among the sources of work‐related stress (D'Emeh et al., 2021; Natividad et al., 2021). In the literature, high levels of work‐related stress have been associated with increased burnout, which is one of the components of compassion fatigue in the widely used Professional Quality of Life concept (Wang et al., 2020).
Compassion fatigue consists of two main concepts: burnout and secondary traumatic stress (Stamm, 2009). Burnout is a psychological condition caused by long‐term stress and can result in a lack of drive and interest in one's work (Alsulimani et al., 2021). Literature reports a difference between personal and work‐related burnout. Having health care conditions and providing care for infected patients was associated with an increase in both personal and work‐related burnout (Duarte et al., 2020). During the COVID‐19 pandemic, 75% of the sample of health care workers, which is composed of 46% of nurses, reported being burned out. Another study found that 53% of the participants experienced high levels of burnout and that burnout was influenced by age, gender, job category and site of practice (Jalili et al., 2021). Factors associated with burnout included extended working hours during the pandemic, the feeling of being forced to care for patients with COVID‐19, being tested for COVID‐19 many times, and age group (Alsulimani et al., 2021). Wang et al. (2020) found the mean burnout and traumatic stress to be 27.4 ± 5.3 and 26.9 ± 5.1, respectively. Martin et al. (2013) examined nurses' intention to work during the H1N1 pandemic. They found that nurses were less likely to work during pandemics if they had a fear of transmitting the disease to their family members. This fear might have been increased by vicarious trauma, which is defined as trauma resulting from empathizing with traumatized clients. It has been found that the public, volunteers and frontline nurses experienced vicarious trauma. Nonetheless, it has been claimed that during the COVID‐19 pandemic, frontline nurses, the ones coming in direct contact with patients having COVID‐19, have experienced significantly lower vicarious trauma compared with the public, volunteers and nurses who did not come in direct contact with patients having COVID‐19 (Li et al., 2020). Nonetheless, it can be argued that during outbreaks and pandemics, traumatic stress increases owing to work‐related events, which might affect the staff's job‐related affective well‐being.
Although the business literature examined the association between work‐related events and job‐related affective well‐being (Ohly & Schmitt, 2015), this association was not explored in the nursing profession. The studied work‐related events ranged from positive to negative, and in some cases, traumatizing encounters, which resulted in job‐related affective well‐being that ranged from positive affective feelings, such as happiness and pride, to negative affective feelings, such as anger and sadness (Jaworek et al., 2019; Ohly & Schmitt, 2015). However, there is no clear relationship clarifying which event will result in positive or negative affective feelings. A taxonomy of work‐related events was established by Ohly and Schmitt (2015) in which four positive and seven negative clusters were created. The positive cultures are goal attainment, problem solving, and task‐related success; praise, appreciation, and positive feedback; perceived competence in or through social interactions; and passively experienced, externally determined positive experience clusters. On the other hand, the negative clusters are hindrances in goal attainment, obstacles in completing work tasks, and overload; conflicts and communication problems; technical difficulties and problems with work tools and equipment; managerial and internal problems and organizational climate; ambiguity, insecurity, and loss of control; and problems in interactions with clients or patients.
During pandemics, health care workers, including nurses, experience loss of control and events that are included in Ohly and Schmitt's (2015) negative events clusters, which might contribute to the development of negative job‐related affective feelings. For instance, during COVID‐19, nurses have higher anxiety levels compared with physicians (Huang, Han, et al., 2020). Researchers also found considerable levels of anxiety, fear, sadness and anger among nurses during the COVID‐19 outbreak (Huang, Xu, & Liu, 2020). Additionally, in the nursing literature, trauma was associated with other variables such as burnout and stress (Jaworek et al., 2019), and due to the connection between work‐related events that can be amplified during the pandemic and job‐related affective well‐being, it is very important to gain an in‐depth understanding of this issue. Thus, this study aimed to examine the direct and indirect effect of work‐related stress on job‐related affective well‐being and compassion fatigue among nurses during the COVID‐19 pandemic. We set out to test the model examining the direct and indirect effect of work‐related stress on job‐related affective well‐being through compassion fatigue.
2. METHOD
2.1. Design
We used a cross‐sectional exploratory design to achieve the aim of this study.
2.2. Study setting and sample
The study was conducted using an online survey between December 2020 and May 2021. Nurses were recruited from a teaching hospital located in the capital city of Saudi Arabia during the COVID‐19 pandemic. This selected hospital has 800 to 1200 beds, and it is responsible to provide care to COVID‐19 patients. After receiving the IRB approval, the hospital's nursing administration was approached by the researchers to describe the study and ask to recruit nurses who met the inclusion criteria. Nurses who were full‐time and worked for more than 6 months were eligible to take part in the study. The administration nursing office sent the invitation link address to the eligible nurses through their professional emails. In the created link address, the nurses can access the description of the study as well as the informed consent with the contact information of the researchers. Nurses who agreed to take part in the study, they can provide their consent by clicking ‘Agree’, and then they can start filling up the questionnaires. After completing the questionnaire, they can submit the questionnaire automatically to the researchers. A reminder email was sent through the nursing office after 4 weeks from the first email. In total, 161 nurses participated in the study. The required sample size was calculated using G*power. When the α level was set as .05, effect size as 0.1 and power as 0.95, the required sample size was estimated to be 158 participants.
2.3. Measurement
The survey was composed of four parts: demographic information (age, nationality, gender, education and experience), work‐related stress, Professional Quality of Life Scale version 5 to measure compassion fatigue and job‐related affective well‐being scale (JAWS). All questionnaires were presented in two languages, Arabic and English. Before the beginning of the study, the scales were adapted to Saudi context and translated to Arabic using an integrated method (Sidani et al., 2010). First, the conceptual equivalence of the selected measures was assessed by collaborating with five health professionals, who are bicultural and bilingual individuals. These health professionals have knowledge about the study concepts and Saudi health care system. The health professionals were asked to individually rate each scales' item in terms of the comprehension and relevance to the context (10‐point numeric rating scale indicating extremes of ‘not at all’ and ‘very much’). Mostly the experts rated the items as easy to understand (i.e., comprehension > 5) and relevant (i.e., relevance > 5). Thus, content validity index (CVI) ranged from 0.8 to 1. Then, forward translation into Arabic was conducted by professional translators. Yet back translation was not conducted as it was optional in the followed method. The final draft of the adapted and translated scales was pilot tested with 30 nurses. The result showed good evidence of reliability as Cronbach's alpha ranged .78 to .92.
2.4. Demographic information
We measured the nurses' age, nationality, gender, education and experience. Furthermore, we included three questions about COVID‐19, which are as follows: Are/were there COVID‐19 cases in your health care organization? Do/did you administer direct care to patients with COVID‐19? Have you been diagnosed with COVID‐19?
2.5. Work‐related stress
Work‐related stress was measured using work‐related strain inventory (Revicki et al., 1991). The scale has 18 items measuring stress and strain in the work environment on a 4‐point Likert scale (ranging from does not apply to me at all to completely applies to me). The scores can range from 18 to 72 with higher scores indicating high work strain. The items focus on work‐related expectations and stress, interactions between work and family, interpersonal communication in work settings and so on. The scale was administered to different health professions, including nurses, and showed evidence of validity and reliability (Revicki et al., 1991). It was administered to nurses in Turkey (Oncel et al., 2007) and Saudi Arabia and showed internal consistency and reliability ranging from 0.85 to 0.90 (Miligi et al., 2019). In the current study, the scale's reliability was 0.72.
2.6. Compassion fatigue
Compassion fatigue was measured using Professional Quality of Life Scale version 5 (PROQOL5) (Stamm, 2009). PROQOL5 is a 30‐item scale that has three subscales with 10 items in each subscale. It is the most commonly used measure of the negative and positive effects of helping others who experience suffering and trauma. The positive aspect is compassion satisfaction (gratification from helping others), and the negative aspect is compassion fatigue. Compassion fatigue has two dimensions: burnout (exhaustion, frustration and anger) and secondary traumatic stress (negative feelings attributable to a combination of both primary and secondary work‐related trauma) (Stamm, 2009). The score range for each of the subscales is from 10 to 50, and a sum of ≤22 indicates low scores, 23–41 indicates moderate scores and ≥42 indicates high scores. PROQOL5 has evidence of good reliability and validity as Cronbach's alpha coefficients for internal consistency ranged from .72 to .90 (Duarte et al., 2016). In this study, the scale's Cronbach's alpha for burnout and secondary traumatic stress were .73 and .87, respectively, and compassion fatigue was treated as a latent variable with two indicators: burnout and secondary traumatic stress.
2.7. Job‐related affective well‐being
JAWS (Warr, 1990) was used to measure work‐related affective feelings. JAWS consist of 12 items (feelings such as tense, calm and worried) in two subscales: job‐related anxiety–contentment and job‐related depression–enthusiasm. The items answered the following question: ‘Thinking of the past few weeks, how much of the time has your job made you feel each of the following:’ The items are scored on a 6‐point Likert type scale, from 1 (never) to 6 (all the time), and higher scores indicate positive well‐being. Psychometrics testing was performed in three independent studies in which the scale showed adequate validity and reliability. Cronbach's alpha for the subscales ranged from .76 to .80 (Warr, 1990). The subscale's Cronbach's alpha for the current study was job‐related anxiety–contentment = .820 and job‐related depression–enthusiasm = .575. In our current study, job‐related affective well‐being was treated as latent variable with two indicators, which are job‐related anxiety–contentment and job‐related depression–enthusiasm.
2.8. Data analysis
Data were analysed using Statistical Package for the Social Sciences Version 25 and MPLUS version 8. Missing data were analysed, and 15 out of 70 items had missing data. The range of the missing data in the 15 variables was 5% to 0.6%. Little's MCAR test was significant (χ 2 = 2117.942, p < .001). Thus, multiple imputation was used to replace the missing value. Reliability testing was conducted to examine the scales' reliability. Univariate descriptive analyses (frequency, mean, standard deviation and distribution analysis) were conducted to describe the participants' demographic characteristics and the study variables. Bivariate analyses, including Pearson's correlation, Spearman correlation and point biserial correlation, were conducted to assess the association between study observed variables and participants' background characteristics.
Structural equation modelling (SEM), which estimates the causal pathway between the observed and latent variables, was conducted (Kline, 2011). In the analysis, both compassion fatigue and work‐related affective feelings were latent variables, whereas job‐related stress was treated as an observed variable. Fitting indices, such as root‐mean‐squared error of approximation (RMSEA), standardized root‐mean‐squared residual (SRMR), comparative fit index (CFI), Tucker–Lewis Index (TLI) and chi‐square test, were used to determine if the model fit the data. Furthermore, both standardized (β) and unstandardized path (B) coefficients were reported.
2.9. Ethical considerations
Institutional review board approval was obtained from King Saud University (# E‐20‐5463). Online informed consent was collected before initiating the survey. Personal information, for example, name and ID number, was not collected to maintain anonymity. Additionally, the collected data were stored in a password‐protected hard drive and will only be disseminated in the aggregated format.
3. RESULT
Participant's demographics are reported in Table 1. The participants' mean age was 33.94 years (SD = 5.78 years), and their mean experience was 11.21 years (SD = 5.96 years). Most of the participants were female (88.8), and 61.5% of them reported their nationality as Saudi. More than half of the participants held bachelor's degrees. More than half of nurses (66.5%) provided direct care to patients with COVID‐19. Among the participants, 16.1% were previously diagnosed with COVID‐19.
TABLE 1.
Background characteristics of the study participants (n = 161)
| Characteristics | Frequency | % |
|---|---|---|
| Gender | ||
| Male | 18 | 11.2 |
| Female | 143 | 88.8 |
| Nationality | ||
| Saudi | 99 | 61.5 |
| Non‐Saudi | 62 | 38.5 |
| Education | ||
| Diploma | 36 | 22.4 |
| Bachelor | 94 | 58.4 |
| Master | 30 | 18.6 |
| PhD | 1 | 0.6 |
| Area of practice | ||
| Direct patient care | 146 | 90.7 |
| Management | 15 | 9.3 |
| Providing care to COVID‐19 cases | ||
| Yes | 107 | 66.5 |
| No | 54 | 33.5 |
| COVID‐19 diagnoses | ||
| Yes | 26 | 16.1 |
| No | 135 | 83.9 |
| Characteristics | M | SD | Range |
|---|---|---|---|
| Age | 33.94 | 5.78 | 23–57 |
| Years of experience | 11.21 | 5.96 | 1–32 |
The descriptive statistics of the study variables are reported in Table 2. The participants' mean work‐related stress scores were 43.12 (SD = 7.40); the minimum score was 23, and the maximum was 63. In terms of job‐related affective well‐being, the participants' mean job‐related anxiety–contentment was 3.17 (SD = 0.97) and mean job‐related depression–enthusiasm was 3.76 (SD = 0.82). The mean scores of the participants' compassion fatigue components were 27.26 (SD = 5.88) for burnout and 25.90 (SD = 7.98) for secondary traumatic stress. Among the participants, around 22% (n = 35) reported low burnout and around 39% (n = 63) reported low secondary traumatic stress. Additionally, around 76% (n = 122) of the participants reported moderate burnout, and around 57% (n = 92) reported moderate secondary traumatic stress. Finally, 2.5% (n = 4) of the participants reported high burnout, and around 4% (n = 6) reported high secondary traumatic stress.
TABLE 2.
Descriptive statistics for study observed variables (n = 161)
| Characteristics | M | SD | Range | Sk | Ku |
|---|---|---|---|---|---|
| Overall work‐related stress | 43.12 | 7.40 | 23–63 | .33 | .30 |
| Job‐related affective well‐being | |||||
| Job‐related anxiety–contentment | 3.17 | .97 | 1–6 | −.45 | .03 |
| Job‐related depression–enthusiasm | 3.76 | .82 | 1–5.17 | −.81 | .33 |
| Compassion fatigue | |||||
| Burnout | 27.26 | 5.88 | 13–48 | .36 | 1.15 |
| Secondary traumatic stress | 25.90 | 7.98 | 12–46 | .55 | −.45 |
Correlation analysis results are presented in Table 3. The analysis indicated that only a significant negative weak association between age and burnout (r = −.217, p = .006) was found, whereas age was not significantly associated with other observed variables. As well, the analysis showed that all study observed variables were not associated with nurses' gender, educational levels, years of experience, nationality (Saudi/non‐Saudi), providing direct care to COVID‐19 patients and being diagnosed with COVID‐19. Thus, none of background characteristics was considered as a controlling variable in the current study.
TABLE 3.
The association between the participants' background and study observed variables (n = 161)
| Work‐related stress | Job‐related anxiety–contentment | Job‐related depression–enthusiasm | Burnout | Secondary traumatic stress | |
|---|---|---|---|---|---|
| Age | −.118 | .068 | .134 | −.224** | −.095 |
| Gender | −.002 | .056 | .053 | −.065 | −.056 |
| Education | .027 | −.055 | −.027 | .011 | −.022 |
| Experience | .056 | .007 | .007 | −.109 | −.087 |
| Nationality | −.044 | −.119 | −.077 | .052 | −.005 |
| Providing care to COVID‐19 cases | −.092 | .113 | .145 | −.122 | −.127 |
| COVID‐19 diagnoses | .119 | −.010 | −.051 | .048 | −.014 |
p < .05.
p < .01.
p < .001 (two‐tailed).
A statistically significant negative association was found between job‐related anxiety–contentment and work‐related stress (r = −.605, p < .001), burnout (r = −.612, p < .001) and secondary traumatic stress (r = −.379, p < .001). Additionally, job‐related depression–enthusiasm was found to be statistically significantly negatively associated with work‐related stress (r = −.650, p < .001), burnout (r = −.598, p < .001) and secondary traumatic stress (r = −.329, p < .001). Moreover, a statistically significant positive association was found between job‐related anxiety–contentment and job‐related depression–enthusiasm (r = .816, p < .001). Work‐related stress was significantly positively associated with burnout (r = .649, p < .001) and secondary traumatic stress (r = .467, p < .001). Finally, a statistically significant positive association was found between burnout and secondary traumatic stress (r = .549, p < .001).
Factor loadings for the latent measures (compassion fatigue and job‐related affective well‐being) were statistically significant with magnitude ranging from 0.602 to 0.915 (Figure 1). From SEM, the model had significant fit with the data, χ 2 (10) = 429.84, p < CFI = 0.992; TLI = 0.972; RMSEA = 0.086 (90% CI: 0.000–0.177); SRMR = 0.020. Work‐related stress had significant direct negative effects on job‐related effective well‐being (β = −.367, p = .00) and positive effect on compassion fatigue (β = .718, p = .00) (Table 4). Compassion fatigue had significant negative direct effects on job‐related effective well‐being (β = −.262, p = .00). Work‐related stress exerted indirect negative effect on job‐related effective well‐being (β = −.329, p = .001) through compassion fatigue which partially mediated the relationship.
FIGURE 1.
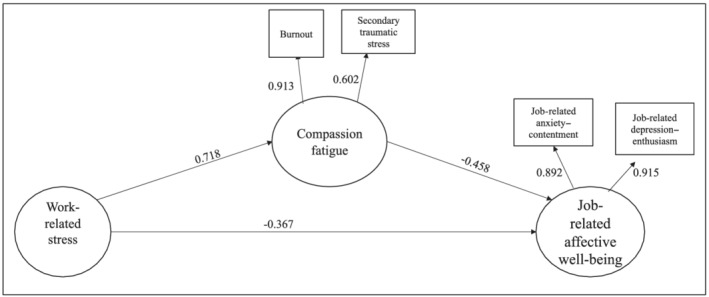
Direct and indirect effect of SEM
TABLE 4.
Direct and indirect effect of SEM
| Structural path | Unstandardized coefficients | Standardized coefficients | SE | p value | |
|---|---|---|---|---|---|
| Direct effect | |||||
| Work‐related stress | Job‐related affective well‐being | −.043 | −.367 | 0.109 | .001 |
| Work‐related stress | Compassion fatigue | .521 | .718 | 0.056 | .00 |
| Compassion fatigue | Job‐related affective well‐being | −.074 | −.458 | 0.120 | .00 |
| Indirect effect | |||||
| Work‐related stress | Job‐related affective well‐being | −.039 | −.329 | 0.096 | .00 |
4. DISCUSSION
Our findings support the hypothesized model in which work‐related stress was directly and indirectly associated with increased negative job‐related affective well‐being through the mediation effect of compassion fatigue. To the best of our knowledge, our study is the first to explore this model among nurses during the COVID‐19 pandemic to increase our understanding regarding the impact of work‐related stress on job‐related affective well‐being. The importance of the current study is due to the evidence that supports the crucial role of affective well‐being on staffs' attitude and behaviour (Laguna et al., 2019). Thus, employees who possess positive work‐related affect are likely to have higher job satisfaction, job commitment and job performance (Courbalay et al., 2022). Nonetheless, employees related affective well‐being is generally inadequately investigated (Qian & Fan, 2019). Therefore, the current study makes a unique contribution and adds to our knowledge about the impact of work‐related stress and compassion fatigue on affective well‐being among nurses during the pandemic. A significant contribution of this study is that work‐related stress directly and indirectly through compassion fatigue increase negative affective well‐being, which might result in increased negative employee attitude and behaviour such as deviant workplace activities and turnover. This understanding highlights the importance of providing nurses with psychological support and educating them in terms of stress reduction techniques as well as providing special attention to the experience of compassion fatigue (burnout and secondary traumatic stress).
Among the studied sample, work‐related stress was above average and higher than the score found by both Pekince and Aslan (2020) who reported a mean WRS of 41.18 ± 2.68 and Erdoğan et al. (2020) who reported a mean of 38.85 ± 5.76. These studies were conducted in Turkey before the COVID‐19 pandemic. Thus, the current higher score might be attributable to the impact of the COVID‐19 pandemic according to a post‐COVID‐19 study by D'Emeh et al. (2021) who found above average nurses' stress overload among a sample of nurses in Saudi Arabia. On the other hand, our current sample's job‐related affective well‐being was almost average, particularly in terms of job‐related anxiety–contentment, and it could be considered as a positive feeling in the depression–enthusiasm axis. The current study followed the scoring instruction for JAWS reported in a study by Warr (1990). However, in the literature, studies such as those by Toderi and Balducci (2018) have grouped the positive feelings in one subscale and the negative feelings in another, and it has been found that the mean score of the negative feelings was lower than that of the positive feelings. Both of these findings might indicate that even in the time of crisis and work overload, nurses tend to maintain a positive outlook towards their job. Among the general population, Warr (1990) found that in a sample of male and female workers, the job‐related anxiety–contentment mean was 4.17 and job‐related depression–enthusiasm mean was 4.55. A more recent study among the general population by Wood et al. (2020) found that the studied sample had a job‐related anxiety–contentment mean of 3.74 and job‐related depression–enthusiasm mean of 4.16. The current study findings show slightly lower values in terms of both job‐related anxiety–contentment and job‐related depression–enthusiasm, indicating that our sample might have experienced negative job‐related affective well‐being.
The majority of the study participants had reported moderate levels of both burnout and secondary traumatic stress. Additionally, a limited number of the participants had scored high in both burnout and secondary traumatic stress. This finding is comparable with the findings of Wang et al. (2020) who reported moderate levels of burnout and secondary traumatic stress in a sample of Chinese nurses before the COVID‐19 pandemic and the findings of Adolfo (2021) who reported moderate levels of burnout and secondary traumatic stress in a sample of Filipino nurses during the COVID‐19 pandemic. Similar to these findings in 2018, Keshavarz et al. (2019) have reported moderate secondary traumatic stress; however, they reported low burnout in a sample of nurses in Iran. These findings indicate that compassion fatigue might not have been impacted by the pandemic and is similar among nurses across cultures.
Our study showed that work‐related stress directly and indirectly influences job‐related affective well‐being and compassion fatigue partially mediated the relationship. Although, to the best of our knowledge, this is the first study examining such a relationship, this current finding is consistent with the findings of existing studies. For example, in the non‐nursing population, stress decreases job‐related affective well‐being among teachers (Li & Zhang, 2019). The Vitamin Model found that nurses' job characteristics, including job demands, autonomy and support, are associated with affective well‐being, which includes job‐related anxiety, satisfaction and burnout (De Jonge & Schaufeli, 1998). Moreover, nurses' experience of conflicts, constraints, workload and toxic leadership explains the variability of job‐related affective well‐being (Hadadian & Sayadpour, 2018). Our finding extended the existing literature by showing the psychological impact of work‐related stress on nurses' positive affective well‐being as well as their experience of compassion fatigue. Our study highlights the negative effect of stress on nurses' mental health, including their motivation and contentment at the workplace. Satisfied and motivated employees can make effective efforts in achieving organization goals and overcome challenges (Warr, 1990). Stress due to the workload, for example, might increase nurses' feeling of depression and anxiety.
This study has several limitations. First, the study was conducted in a single teaching hospital in Saudi Arabia, which might impact generalization. We recommend that future research be conducted in multiple hospitals to examine the variation in stress, compassion fatigue and affective well‐being. Second, the data were collected using a self‐administered questionnaire, which might have introduced a self‐serving bias. In an attempt to mitigate this bias, information that might identify the participants was not collected in this study. Finally, this study used the cross‐sectional method for data collection, which might have affected the study's validity. Studies with a longitudinal study design should be performed in the future to overcome this limitation.
5. CONCLUSION
To the best of our knowledge, this is the first study that examines a model to investigate the direct and indirect impact of work‐related stress on job‐related affective well‐being through compassion fatigue. The finding supported the model and added to our understanding regarding the impact of work‐related stress on nurses. Our findings suggest that reducing work‐related stress among nurses will result in higher positive job‐related affective feelings, thus improving nurses' job‐related affective well‐being. The findings provide evidence to support nurse managers' and health care organizations' effort to control stressors among nurses.
6. IMPLICATION FOR NURSING MANAGEMENT
Frontline nurse managers and leaders should include stress prevention among staff nurses as one of their management plan objectives. This objective may be achieved by implementing evidence‐based management in the nurses' day‐to‐day decision‐making and problem‐solving activities. Moreover, it could be achieved by adapting an open‐door policy, improving effective communication and acknowledging nurses' effort as active participants in the health care team. Nonetheless, it should be recognized that nursing is one of the highly stressful professions; thus, stress might not be completely avoidable. Therefore, stress reduction is an important element in improving staff outcomes, including improving job‐related affective well‐being. Staff nurses with positive attitudes towards their job might be more committed, tend to stay in their organization and improve their job performance. Thus, nurse managers should capitalize on building a work culture that supports nurses and reduces stressors through the establishment of support groups and by providing psychological counselling. Moreover, nurses should be trained in terms of methods and techniques to reduce work‐related stress, such as time management and prioritization. Additionally, unit rotation should be provided for nurses who work in highly stressful units, such as intensive care units. Finally, during times of crisis and work overload, nurse managers must ensure that they acknowledge the staff's effort and approach them properly.
ACKNOWLEGEMENT
This research project was supported by a grant from the ‘Research Centre of the Female Scientific and Medical Colleges’, Deanship of Scientific Research, King Saud University.
CONFLICT OF INTEREST
Authors declare that they have no conflict of interest to declare.
ETHICS STATEMENT
IRB approval was obtained from the King Saud University, College of Medicine IRB committee (# E‐20‐5463).
Falatah, R. , & Alhalal, E. (2022). A structural equation model analysis of the association between work‐related stress, burnout and job‐related affective well‐being among nurses in Saudi Arabia during the COVID‐19 pandemic. Journal of Nursing Management, 30(4), 892–900. 10.1111/jonm.13587
Funding information Research Centre of the Female Scientific and Medical Colleges
DATA AVAILABILITY STATEMENT
Authors do not wish to share the data.
REFERENCES
- Adolfo, C. S. (2021). Predictors of professional quality of life among nurses: A cross‐sectional study. International Journal of Advanced and Applied Sciences, 8(2), 44–53. 10.21833/ijaas.2021.02.006 [DOI] [Google Scholar]
- Alanazi, A. , Mohamed, A. , Hammad, S. , & Alanazi, A. (2019). Job‐related stress among nurses in primary healthcare centers in Arar city, Saudi Arabia. Electronic Physician, 11(3), 7594–7601. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5633215/ [Google Scholar]
- Alenezi, A. M. , Aboshaiqah, A. , & Baker, O. (2018). Work‐related stress among nursing staff working in government hospitals and primary health care centres. International Journal of Nursing Practice, 24(5), 1–8. 10.1111/ijn.12676 [DOI] [PubMed] [Google Scholar]
- Alsulimani, L. K. , Farhat, A. M. , Borah, R. A. , AlKhalifah, J. A. , Alyaseen, S. M. , Alghamdi, S. M. , & Bajnaid, M. J. (2021). Health care worker burnout during the COVID‐19 pandemic: A cross‐sectional survey study in Saudi Arabia. Saudi Medical Journal, 42(3), 306–314. 10.15537/SMJ.2021.42.3.20200812 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choi, K. R. , Skrine Jeffers, K. , & Cynthia Logsdon, M. (2020). Nursing and the novel coronavirus: Risks and responsibilities in a global outbreak. Journal of Advanced Nursing, 76(7), 1486–1487. 10.1111/jan.14369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Courbalay, A. , Brandet, Q. , Girard, D. , & Gillet, N. (2022). Benefits of a brief physical activity programme on employees' affective well‐being and momentary affective states: A quasi‐experimental study. Journal of Happiness Studies, 0123456789. 10.1007/s10902-021-00489-9 [DOI] [Google Scholar]
- De Jonge, J. , & Schaufeli, W. B. (1998). Job characteristics and employee well‐being: A test of Warr's vitamin model in health care workers using structural equation modelling. Journal of Organizational Behavior: The International Journal of Industrial, Occupational and Organizational Psychology and Behavior, 19(4), 387–407. [DOI] [Google Scholar]
- D'Emeh, W. M. , Yacoub, M. I. , & Shahwan, B. S. (2021). Work‐related stress and anxiety among frontline nurses during the COVID‐19 pandemic: A cross‐sectional study. Journal of Psychosocial Nursing and Mental Health Services, 59(8), 31–42. 10.3928/02793695-20210322-02 [DOI] [PubMed] [Google Scholar]
- Duarte, I. , Teixeira, A. , Castro, L. , Marina, S. , Ribeiro, C. , Jácome, C. , Martins, V. , Ribeiro‐Vaz, I. , Pinheiro, H. C. , Silva, A. R. , Ricou, M. , Sousa, B. , Alves, C. , Oliveira, A. , Silva, P. , Nunes, R. , & Serrão, C. (2020). Burnout among Portuguese healthcare workers during the COVID‐19 pandemic. BMC Public Health, 20(1), 1–11. 10.1186/s12889-020-09980-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duarte, J. , Pinto‐Gouveia, J. , & Cruz, B. (2016). Relationships between nurses’ empathy, self‐compassion and dimensions of professional quality of life: A cross‐sectional study. International Journal of Nursing Studies, 60, 1–11. 10.1016/j.ijnurstu.2016.02.015 [DOI] [PubMed] [Google Scholar]
- Elkholy, H. , Tawfik, F. , Ibrahim, I. , Salah El‐din, W. , Sabry, M. , Mohammed, S. , Hamza, M. , Alaa, M. , Fawzy, A. Z. , Ashmawy, R. , Sayed, M. , & Omar, A. N. (2021). Mental health of frontline healthcare workers exposed to COVID‐19 in Egypt: A call for action. International Journal of Social Psychiatry, 67(5), 522–531. 10.1177/0020764020960192 [DOI] [PubMed] [Google Scholar]
- Erdoğan, C. , Doğan, S. , Çakmak, R. , Kizilaslan, D. , Hizarci, B. , Karaaslan, P. , & Öz, H. (2020). Assessment of job satisfaction, work‐related strain, and perceived stress in nurses working in different departments in the same hospital: A survey study. Ain‐Shams Journal of Anesthesiology, 12(1). 10.1186/s42077-020-00084-9 [DOI] [Google Scholar]
- Hadadian, Z. , & Sayadpour, Z. (2018). Relationship between toxic leadership and job related affective well‐being: The mediating role of job stress. European Online Journal of Natural and Social Sciences: Proceedings, 7(1 (s)), 137. [Google Scholar]
- Hoedl, M. , Bauer, S. , & Eglseer, D. (2021). Influence of nursing staff working hours on stress levels during the COVID‐19 pandemic. HeilberufeSCIENCE. 10.1007/s16024-021-00354-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang, J. Z. , Han, M. F. , Luo, T. D. , Ren, A. K. , & Zhou, X. P. (2020). Mental health survey of 230 medical staff in a tertiary infectious disease hospital for COVID‐19. Chinese Journal of Industrial Hygiene and Occupational Diseases, 38(E001). [DOI] [PubMed] [Google Scholar]
- Huang, L. , Xu, F. M. , & Liu, H. R. (2020). Emotional responses and coping strategies of nurses and nursing college students during COVID‐19 outbreak. MedRxiv, 2020.03.05.20031898. 10.1101/2020.03.05.20031898 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jalili, M. , Niroomand, M. , Hadavand, F. , Zeinali, K. , & Fotouhi, A. (2021). Burnout among healthcare professionals during COVID‐19 pandemic: A cross‐sectional study. International Archives of Occupational and Environmental Health, 94(6), 1345–1352. 10.1007/s00420-021-01695-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jaworek, M. A. , Marek, T. , & Karwowski, W. (2019). The scale of work‐related affective feelings (WORAF). 10.1016/j.apergo.2019.102945 [DOI] [PubMed] [Google Scholar]
- Keshavarz, Z. , Gorji, M. , Houshyar, Z. , Tamajani, Z. T. , & Martin, J. (2019). The professional quality of life among health‐care providers and its related factors. Social Health and Behavior.. 10.4103/SHB.SHB [DOI] [Google Scholar]
- Kline, R. B. (2011). Convergence of structural equation modeling and multilevel modeling. 10.4135/9781446268261.n31 [DOI] [Google Scholar]
- Laguna, M. , Mielniczuk, E. , & Razmus, W. (2019). Test of the bifactor model of job‐related affective well‐being. Europe's Journal of Psychology, 15(2), 342–357. 10.5964/ejop.v15i2.1632 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, J. H. , Hwang, J. , & Lee, K. S. (2019). Job satisfaction and job‐related stress among nurses: The moderating effect of mindfulness. Work, 62(1), 87–95. 10.3233/WOR-182843 [DOI] [PubMed] [Google Scholar]
- Li, Q. , Guan, X. , Wu, P. , Wang, X. , Zhou, L. , Tong, Y. , Ren, R. , Leung, K. S. M. , Lau, E. H. Y. , Wong, J. Y. , Xing, X. , Xiang, N. , Wu, Y. , Li, C. , Chen, Q. , Li, D. , Liu, T. , Zhao, J. , Liu, M. , … Feng, Z. (2020). Early transmission dynamics in Wuhan, China, of novel coronavirus‐infected pneumonia. New England Journal of Medicine, 1199–1207. 10.1056/nejmoa2001316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, Y. , & Zhang, R. C. (2019). Kindergarten teachers' work stress and work‐related well‐being: A moderated mediation model. Social Behavior and Personality: An International Journal, 47(11), 1–11. 10.2224/sbp.8409 [DOI] [Google Scholar]
- Martin, D. , Brown, L. , & Reid, M. (2013). Predictors of Nurses' intentions to work during the 2009 influenza A (H1N1) pandemic. AJN, American Journal of Nursing., 113(12), 24–31. 10.1097/01.NAJ.0000438865.22036.15 [DOI] [PubMed] [Google Scholar]
- Miligi, E. , Alshutwi, S. , & Alqahtani, M. (2019). The impact of work stress on turnover intentions among palliative care nurses in Saudi Arabia. 6(2), 84–88. 10.15640/ijn.v6n2a8 [DOI] [Google Scholar]
- Natividad, M. J. B. , Aljohani, K. A. , & Gamboa, H. M. (2021). Feelings, stress, and coping of nurses amidst COVID‐19 outbreak in Saudi Arabia. Sudan Journal of Medical Sciences, 16(2), 285–300. 10.18502/sjms.v16i2.9295 [DOI] [Google Scholar]
- Ohly, S. , & Schmitt, A. (2015). What makes us enthusiastic, angry, feeling at rest or worried? Development and validation of an affective work events taxonomy using concept mapping methodology. Journal of Business and Psychology, 30(1), 15–35. 10.1007/s10869-013-9328-3 [DOI] [Google Scholar]
- Oncel, S. , Ozer, Z. C. , & Efe, E. (2007). Work‐related stress, burnout and job satisfaction in Turkish midwives. Social Behavior and Personality, 35(3), 317–328. 10.2224/sbp.2007.35.3.317 [DOI] [Google Scholar]
- Pai Vernekar, S. , & Shah, H. (2018). A study of work‐related stress among nurses in a tertiary care hospital in Goa. International Journal of Community Medicine and Public Health, 5(2), 657. 10.18203/2394-6040.ijcmph20180246 [DOI] [Google Scholar]
- Pekince, H. , & Aslan, H. (2020). Determining the work‐related strain levels of nurses and influencing factors. International Journal of Caring Sciences, 13(1), 1–135. Retrieved from https://www.internationaljournalofcaringsciences.org [Google Scholar]
- Qian, Y. , & Fan, W. (2019). Men and women at work: Occupational gender composition and affective well‐being in the United States. Journal of Happiness Studies, 20(7), 2077–2099. 10.1007/s10902-018-0039-3 [DOI] [Google Scholar]
- Revicki, D. A. , May, H. J. , & Whitley, T. W. (1991). Reliability and validity of the work‐related strain inventory among health professionals. Behavioral Medicine, 17(3), 111–120. 10.1080/08964289.1991.9937554 [DOI] [PubMed] [Google Scholar]
- Sidani, S. , Guruge, S. , Miranda, J. , Ford‐Gilboe, M. , & Varcoe, C. (2010). Cultural adaptation and translation of measures: An integrated method. Research in Nursing & Health, 33(2), 133–143. 10.1002/nur.20364 [DOI] [PubMed] [Google Scholar]
- Stamm, B. H. (2009). The ProQOL manual. Sidran Press. [Google Scholar]
- Toderi, S. , & Balducci, C. (2018). Stress‐preventive management competencies, psychosocialwork environments, and affective well‐being: A multilevel, multisource investigation. International Journal of Environmental Research and Public Health, 15(3), 1–17. 10.3390/ijerph15030397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, J. , Okoli, C. T. , He, H. , Feng, F. , Li, J. , Zhuang, L. , & Lin, M. (2020). Factors associated with compassion satisfaction, burnout, and secondary traumatic stress among Chinese nurses in tertiary hospitals: A cross‐sectional study. International Journal of Nursing Studies, 102, 103472. 10.1016/j.ijnurstu.2019.103472 [DOI] [PubMed] [Google Scholar]
- Warr, P. (1990). The measurement of well‐being and other aspects of mental health. Journal of Occupational Psychology, 63(3), 193–210. 10.1111/j.2044-8325.1990.tb00521.x [DOI] [Google Scholar]
- Wood, S. , Daniels, K. , & Ogbonnaya, C. (2020). Use of work–nonwork supports and employee well‐being: The mediating roles of job demands, job control, supportive management and work–nonwork conflict. The International Journal of Human Resource Management, 31(14), 1793–1824. 10.1080/09585192.2017.1423102 [DOI] [Google Scholar]
- World Health Organisation . (2014). Hospital preparedness for epidemics. Retrieved from http://apps.who.int/iris/bitstream/10665/151281/1/9789241548939_eng.pdf [Google Scholar]
- World Health Organization . (2020). Coronavirus disease (COVID‐19) outbreak. Retrieved from https://www.who.int/westernpacific/emergencies/covid-19 [Google Scholar]
- Worldmater COVID‐19 pandmic . (2022). Retrived from https://www.worldometers.info/coronavirus/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Authors do not wish to share the data.