

Abstract
Cultural differences have been reported between the taste sensitivity of persons of Asian and European ancestry, although findings have been mixed. This study sought to determine whether American and Chinese adults perform differently on a novel taste test that requires no water, can be self‐administered, and employs a representative of umami as one of its tastants. This 53‐trial test was administered to 113 Chinese and 214 Americans. The subjects orally sampled monomer cellulose pads containing one of four dried concentrations of sucrose, citric acid, NaCl, caffeine, and monosodium glutamate and indicated whether a sweet, sour, bitter, salty, brothy, or no taste sensation was perceived. Separate gender by culture analyses of covariance with age as the covariate were performed on the total score and the scores of each taste stimulus. For all taste qualities, women outperformed men and test scores declined with age. No difference between American and Chinese subjects was found for the total taste score (p = .129) or for the sucrose (p = .129) or NaCl (p = .368) scores. However, for monosodium glutamate, the scores were 28.40% higher for the Chinese than for the American subjects (p = .024), and for citric acid and caffeine, the scores were 24.12 and 21.79% higher for the American subjects (p's = .001 and .029). The basis for these differences is unclear, although both anatomical (e.g., differences in density or distribution of taste buds) and cultural factors may be involved. Future work is needed to determine the cause of these largely novel findings and whether they generalize to other Chinese and American samples.
Practical applicationsIn this study, a practical self‐administered quantitative taste test that requires no water was found to be sensitive to quality‐specific differences in test scores between Chinese and American subjects, as well as to age and gender. The Chinese subjects outperformed the American subjects in correctly identifying the quality of monosodium glutamate (umami), whereas the American subjects outperformed Chinese subjects in correctly identifying the bitter and sour qualities of caffeine and citric acid, respectively. Experiential factors related to culture‐specific cuisines may explain some of these differences. This research indicates that a relatively rapid taste test, which can be sent through the mail and which requires no test administrator or source of water, can be used in cross‐cultural studies to elucidate individual differences in taste perception.
1. INTRODUCTION
The sense of taste plays a significant role in everyday life, being a key arbiter for the oral acceptance or rejection of foods and beverages (Schier & Spector, 2019). Epidemiologic studies suggest that up to 20% of persons in Europe and the United States suffer from some degree of objectively measured taste dysfunction (Doty, 2019), despite most being unaware of their deficit (Soter et al., 2008). When extrapolated to the populations of China and the United States, this adds up to over 300 million people. These numbers are likely to increase given that taste dysfunction is present in a significant number of persons in not only such neurodegenerative diseases as Alzheimer's (Steinbach et al., 2010) and Parkinson's (Doty et al., 2015), but in many who have contracted SARS‐CoV‐2, the virus responsible for COVID‐19 (Singer‐Cornelius, Cornelius, Oberle, Metternich, & Brockmeier, 2021).
That being said, there are reports that performance on some taste tests differs between subjects from different cultures. For example, Shu‐Fen, Forde, Tey, and Henry (2018) found, in a study of 60 Chinese and 54 Indian subjects, that the Indian subjects were less sensitive, that is, had higher recognition thresholds, for sucrose, sodium chloride, citric acid, caffeine, and monosodium glutamate, the same tastants employed in the present study. Chinese and Japanese subjects have also been found to be more sensitive to the bitter taste of 6‐n‐propylthiouracil (PROP) than Caucasian subjects (Guo & Reed, 2001), conceivably reflecting a greater density of their fungiform papillae (Essick, Chopra, Guest, & McGlone, 2003). Even among European countries, cultural differences have been reported. For example, Ribeiro et al. (2016) found that Portuguese subjects underperformed German subjects on a 36‐trial taste strip test.
The present study compared the performance of a sizable sample of Chinese and American subjects on a recently developed and very reliable taste test that employs, in addition to representatives of the four classic basic taste qualities, umami, a tastant that is more common in Chinese than in American cuisine (Doty, Wylie, & Potter, 2021). This test uses taste stimuli embedded in disposable pads of cellulose and has been found to be sensitive to age, sex, phenylthiocarbamide taster status, and head trauma. It is more practical than other taste tests since it can be self‐administered and does not require a water source for rinsing or stimulus presentation.
2. METHODS
2.1. Subjects
A total of 327 healthy adult subjects 18 years of age or older with self‐rated normal taste abilities participated. These included 113 Chinese students or health care workers from the Second Affiliated Hospital of Xi'an Jiaotong University (52 men and 61 women; respective mean [SD] ages = 25.23 [6.93] and 24.61 [6.75] years; respective age ranges = 18–50 and 18–59) and 214 American volunteers recruited through multiple media sources (69 men and 145 women; respective mean [SD] ages = 41.19 [15.50] and 41.16 [16.15] years; respective age ranges = 18–76 and 18–79). The American sample was comprised of 185 White Americans (87%), 11 Asian Americans (5%), 9 African Americans (4%), and 9 Hispanic Americans (4%). The backgrounds of the Asian Americans were Chinese (n = 5), Indian (n = 5), and Vietnamese (n = 1). Exclusion criteria were a history of past or current nasal disease (allergic rhinitis or chronic rhinosinusitis), COVID‐19 disease, or smell or taste disorders. Informed written consent was obtained from all subjects. The study was approved by the ethics committee of the Second Affiliated Hospital of Xi'an Jiaotong University (No. 2021010), China, and the New England Independent Review Board (www.mbl.edu/osp/neirb; #1279756).
2.2. Waterless Empirical Taste Test
The Waterless Empirical Taste Test (WETT) (Sensonics International, Haddon Heights, NJ) consists of 53 plastic taste strips. Positioned on one side of each 1 × 6 cm strip is a 1 × 2.5 cm monomer cellulose pad containing a concentration of either dried sucrose (0.20, 0.10, 0.05, or 0.025 g/ml), citric acid (0.025, 0.05, 0.10, or 0.20 g/ml), sodium chloride (0.0313, 0.0625, 0.125, or 0.25 g/ml), caffeine (0.011, 0.022, 0.044, or 0.088 g/ml), monosodium glutamate (0.017, 0.034, 0.068, or 0.135 g/ml), or no stimulus. The version of the test which was used for the American element of the present study provides the taste strips in convenient packs where they can be removed for self‐administration in a numbered order by the subject. The answers are filled into the response forms as the subject goes through the test (Figure 1). The version of the test which was used for the Chinese element of the study houses the taste strips in compartments of a portable box (Figure 2). Each of the three drawers of the box is divided into nine compartments. These test strips are handed individually to each subject by a test administrator in an order denoted in each test drawer and the subject self‐administers the taste strips in the same manner as done in the American element of the study. In this case, the responses of the subjects are recorded by the examiner on the same test sheets pictured in Figure 1.
FIGURE 1.
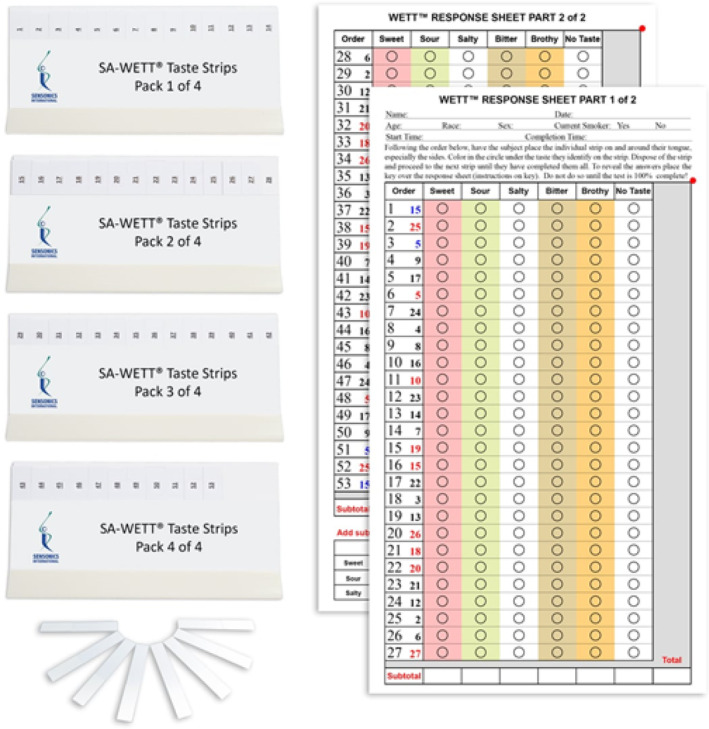
The stimulus holders and taste strips used in the Waterless Empirical Taste Test (WETT‐SA53) were employed in the American testing of this study. Each individual strip is pulled from the container by the subject in numbered order. The subject then moves its taste‐laden cellulose pad around the surfaces of the tongue and discards it into a waste container after use. The subject's responses are indicated by filling in the answer on a given line of the pictured response sheet. A key is then used to count the number of correct resonses in each column. Courtesy of Sensonics International, Haddon Heights, NJ. Copyright © 2015, 2019, Sensonics International
FIGURE 2.

The portable Waterless Empirical Taste Test (WETT) kit with front door closed (left) and open (right). The three drawers containing the white plastic monomer cellulose pads embedded with tastants (in front of pictures) are shown. The taste strips are handed individually to each subject who self‐administers the taste strips (see text for details). Courtesy of Sensonics International, Haddon Heights, NJ. Copyright © 2015, 2019, Sensonics International
It should be noted that the WETT provides a general measure of the ability to identify various concentrations of taste stimuli with a minimum number of trials and without the calculation of thresholds, per se. Its presentation paradigm is operationally similar to that of a recognition threshold since ascending concentrations are presented in the first half of the test and descending concentrations in the second half of the test. However, the concentrations of a given tastant do not immediately follow one another, as normally occurs for a threshold test, but are interspersed among those of the other tastants. Such an approach maximizes efficiency, making it possible to test all five basic taste qualities in the same test session with short inter‐stimulus intervals not confounded by adaptation.
2.3. Testing procedure
On a given trial, each subject was instructed to move a strip's cellulose pad around the mouth, particularly along the tongue's dorsal edges, for 5–10 s, and to then identify the taste quality or to indicate that no taste can be perceived. The test strip was then discarded into a waste container after each trial. A standardized protocol was followed according to the administration manuals of the tests and subject responses were recorded on the test sheets, as noted in Figure 1. Within the test trial sequence, the four concentrations of each stimulus are presented twice. In the first half of the test (27 trials), which corresponds to the brief self‐administered WETT (SA‐WETT‐27), the stimulus concentrations proceed from weak to strong in an ascending sequence, with the different tastants being counterbalanced in presentation order. No tastant (e.g., sucrose) immediately follows itself. The blanks are presented after each of the four caffeine presentations, the 0.25 g/ml sodium chloride presentation, and the 0.025 and 0.10 g/ml citric acid presentations. In the second half of the test, the reverse presentation order is made, that is, going from strong to weak concentrations. The blank that follows the 0.25 g/ml sodium chloride stimulus, which is the last trial of the first series, is not repeated at the beginning of the second series, resulting in 26 rather than 27 trials for the second half of the test.
2.4. Statistical analyses
The total number of correct responses (sum of all correct responses) and the number of correct responses for each of the five taste stimuli were the dependent measures. Separate analyses of covariance were applied to each of these measures to compare the scores of the American and Chinese subjects and determine the influences of gender and age on such scores. The factors were gender and cultural group (Chinese, American); age was the covariate to examine age effects and to adjust for any age differences between the two groups. Pearson correlations were computed between the scores on the first and second halves of the test with p values Bonferroni corrected. Significance on all tests was set at the .05 alpha level. Statistical analyses were performed using SYSTAT 13.1 (Wilkinson, 1990).
3. RESULTS
The mean (SEM) age‐adjusted total WETT scores are presented in Table 1 for the male and female Chinese and American subjects. Included are the test scores summed across all trials, as well as test scores for each of the subcomponent stimuli.
TABLE 1.
Age‐corrected mean (SEM) WETT scores for the Chinese and American Men and Women
| Gender | Chinese | American | % Difference |
|---|---|---|---|
| Total taste test score (score of 53 possible) | |||
| Men | 32.24 (1.36) | 31.83 (1.15) | −1.27 |
| Women | 33.85 (1.27) | 38.19 (0.81) | +12.82 |
| % Diff | +4.99 | +19.98 | |
| Sucrose (sweet) taste score (score of 8 possible) | |||
| Men | 5.25 (0.31) | 4.73 (0.26) | −9.90 |
| Women | 5.12 (0.29) | 5.76 (0.18) | +12.50 |
| % Diff | −2.48 | +21.78 | |
| Citric acid (sour) taste test score (score of 8 possible) | |||
| Men | 4.31 (0.34) | 4.96 (0.29) | +15.08 |
| Women | 4.65 (0.32) | 6.16 (0.20) | +32.5 |
| % Diff | +7.89 | +24.19 | |
| Sodium chloride (salty) taste test score (score of 8 possible) | |||
| Men | 5.04 (0.31) | 5.14 (0.26) | +0.02 |
| Women | 5.49 (0.29) | 5.92 (0.18) | +7.83 |
| % Diff | +8.93 | +15.18 | |
| Caffeine (bitter) taste test score (score of 8 possible) | |||
| Men | 4.34 (0.34) | 4.55 (0.31) | +4.84 |
| Women | 4.37 (0.34) | 5.67 (0.22) | +29.75 |
| % Diff | +0.01 | +24.62 | — |
| Monosodium glutamate (brothy) taste test score (score of 8 possible) | |||
| Men | 2.60 (0.32) | 2.15 (0.27) | −17.31 |
| Women | 3.63 (0.30) | 2.71 (0.19) | −25.34 |
| % Diff | +39.62 | +26.05 | |
3.1. Total test scores
The total test scores of the American and Chinese groups did not differsigniicantly (respective means [SEMs] = 35.01 [0.72] and 33.05 [0.98]; Group F [1,322] = 2.32, p = .129). The test scores of women were 15.07% higher than those of men (respective means [SEMs] = 36.01 [0.72] and 32.04 [0.87]; F [1,322] = 12.63, p < .0001; η 2 = 0.04) and performance declined as a function of age (F [1,322] = 14.89, p < .0001; η 2 = 0.04). As can be seen in Table 1, American women outperformed all other groups (group by gender interaction F [1,322] = 4.48, p = .035; η 2 = 0.04; Tukey's honestly significant difference (HSD) p values for differences: American men, p < .0001; Chinese men, p = .002; Chinese women, p = .029). The Pearson r between the total scores of the first and second halves of the test was 0.90 (p < .0001).
3.2. Sucrose (sweet) test scores
The means of the Chinese and American sweet test scores were essentially equivalent (respective means [SEMs] = 5.19 [0.22] and 5.25 [0.16]; F [1,322] = 0.04, p = .833). Although gender did not reach the 0.05 level of statistical significance (F [1,322] = 3.22, p = .074), a significant gender by group interaction (F [1,322] = 5.33, p = .022; η 2 = 0.02) revealed a greater sex difference in the test scores between the male and female American subjects than between those of their Chinese counterparts (21.78% vs. −2.48%; Tukey's HSD test p = .004; all other Tukey p's > 0.25). An overall age‐related decline was present (F [1,322] = 24.33, p < .0001; η 2 = 0.07). The Pearson r between the sucrose scores of the first and second halves of the test was 0.63 (p < .0001).
3.3. Citric acid (sour) test scores
The average sour scores of the American subjects were 24.12% higher than those of the Chinese subjects (respective means [SEMs] = 5.56 [0.18] and 4.48 [0.24]; F [1,322] = 11.47, p = .001, η 2 = 0.03). The scores decreased with age (F [1,322] = 13.50, p < .0001; η 2 = 0.04) and were 16.63% higher in women than in men (respective means [SEMs] = 5.40 [0.18] and 4.63 [0.22]; F [1,322] = 7.57, p = .006, η 2 = 0.02). While there was a tendency for American women to outperform the other subjects, the group by gender interaction was not statistically significant (F [1,322] = 2.38, p = .124; η 2 = 0.01). The Pearson r between the citric acid scores of the first and second halves of the test was 0.69 (p < .0001).
3.4. Sodium chloride (salty) test scores
No significant difference was evident between the salty scores of the American and Chinese subjects (respective means [SEMs] = 5.53 [0.16] and 5.27 [0.22]; F [1,322] = 0.81, p = .368, η 2 = 0.00). The mean score was 13.53% higher in women than in men (respective means [SEMs] = 5.79 [0.15] and 5.10 [0.19]; F [1,322] = 5.93, p = .015, η 2 = 0.02). Although the gender differences appear to be larger in the American than in the Chinese women (15.8% vs. 8.93%), the group by gender interaction was not statistically significant (F [1,322] = 0.45, p = .50; η 2 = 0.00). Unlike the other taste qualities, age did not achieve the 0.05 level of statistical significance (F [1,322] = 1.50, p = .22; η 2 = 0.00). The Pearson r between the sodium chloride scores of the first and second halves of the test was 0.48 (p < .0001).
3.5. Caffeine (bitter) test scores
The bitter scores were 21.79% higher in the American than in the Chinese subjects (respective means [SEMs] = 5.11 [0.19] and 4.36 [0.26]; Group F [1,322] = 4.84, p = .029, η 2 = 0.01) and 13.00% higher in women than in men (respective means [SEMs] = 5.02 [0.19] and 4.45 [0.23]; F [1,322] = 3.73, p = .054, η 2 = 0.01). Test scores declined with age (F [1,322] = 9.56, p = .002, η 2 = 0.03). The Pearson r between the caffeine scores of the first and second halves of the test was 0.67 (p < .0001).
3.6. Monosodium glutamate (umami/brothy) test scores
The brothy test scores were 28.40% higher in the Chinese than the American subjects (respective means [SEMs] = 3.12 [0.23] and 2.43 [0.17]; F [1,322] = 5.15, p = .024, η 2 = 0.01). Women outperformed men independent of cultural background (respective means [SEMs] = 3.17 [0.17] and 2.38 [0.20]; F [1,322] = 9.13, p = .003, η 2 = 0.03). A decline in test scores with age was evident (F [1,322] = 7.98, p = .005, η 2 = 0.02). The Pearson r between the monosodium glutamate scores of the first and second halves of the test was 0.42 (p < .0001).
4. DISCUSSION
The present study assessed performance differences between American and Chinese adult subjects on a recently developed waterless taste test that assessed umami in addition to the classic four basic tastes. Although no difference between the American and Chinese subjects was present for the total WETT scores or for sucrose and NaCl, the scores for monosodium glutamate (MSG), a representative of the umami taste quality, were 28.40% higher for the Chinese than for the American subjects. The opposite occurred for caffeine and citric acid, where the American scores were 24.12 and 21.79% higher than the Chinese scores. For the total WETT, American women significantly outperformed Chinese women and both the Chinese and American men.
The basis for the cultural differences in performance on the WETT is unknown, although both environmental and genetic factors may be involved. However, cultural factors seem preopotent. Thus, the sole tastant for which the Chinese subjects outperformed the American subjects was monosodium glutamate, a food additive that is much more common in Chinese and other Asian cuisines than in American ones. In fact, China is the largest producer and consumer of MSG in the world (Rosenthal, 2000). Our findings are congruent with those of Kobayashi and Kennedy (2002), who found lower MSG thresholds in Japanese than in American or European subjects, and that Japanese subjects could better identify MSG in foods. In this same study, exposure of the non‐Japanese subjects to shrimp crackers containing MSG for 11 to 12 days resulted in their ability to identify MSG at lower concentrations than non‐exposed controls, stressing the role of experience in altering MSG sensitivity.
The better performances of the Americans on caffeine and citric acid are somewhat more difficult to explain on the basis of putative cultural factors, although in the case of caffeine, experience may well be a factor. Coffee, which is the most common bitter‐tasting drink in North America, is much less popular in China. Indeed, according to the International Coffee Organization (http://www.ico.org), the average Chinese person drinks only five cups of coffee per year, which is 1.3% of the amount consumed by the average American. Although Chinese and Japanese subjects are reported to be more sensitive than Caucasian subjects to the bitter taste of PROP, one of a number of well‐studied bitter substances (Guo & Reed, 2001), perceived caffeine bitterness is related to daily caffeine intake (Lipchock et al., 2017). Although sour‐tasting citric acid is widely found in citrus fruits and is present in American food products, including soda, fruit‐flavored beverages, candy, and flavored syrups and lemonade, grapefruit juice, and orange juice, it is not clear whether it is a more common staple in America than in China.
Our observation of no difference between the Chinese and American subjects for the taste of sucrose is in accord with the findings of some, but not all, prior studies. Ketel, de Wijk, de Graff, and Steiger (2020) found no differences in sucrose thresholds between Chinese subjects and Dutch subjects. However, another study found Chinese students rated suprathreshold concentrations of sucrose as stronger and sweeter than U.S. students of European ancestry (Bertino & Chan, 1986). In that study, relative to the U.S. students, the Chinese students also rated low concentrations of salt as tasting saltier and high concentrations of salt as tasting less salty, in contrast to our finding of no differences in salty perception between the two cultural groups.
The present study found that the ability to detect each of the five basic taste qualities declined with age, although the effect was muted for NaCl. We also found that such ability was greater in women than in men, regardless of their cultural background. These phenomena were also evidence in the clinical participants of the validation study of the WETT, where age and gender were significant factors for not only the WETT, but also for two chemically based taste tests (Doty et al., 2021). Again, however, the age‐related affect was attenuated for NaCl on all three tests. Such findings are generally congruent with a large taste perception literature, although marked variation among studies is present (Barragán et al., 2018; Bartoshuk, Rifkin, Marks, & Bars, 1986; Doty et al., 2016; Fikentscher, Roseburg, Spinar, & Bruchmuller, 1977; Fischer et al., 2013; Mennella, Reed, Roberts, Mathew, & Mansfield, 2014; Sergi, Bano, Pizzato, Veronese, & Manzato, 2017; Stinton, Atif, Barkat, & Doty, 2010; Yoshinaka et al., 2016). This variation potentially reflects differences in psychophysical test procedures, stimulus concentrations, and sample sizes. For example, in a study of 81 men and women between 23 and 88 years of age, Weiffenbach, Baum, and Burghauser (1982) found detection thresholds for sodium chloride and quinine sulfate to be weakly impacted by age. However, sucrose and citric acid thresholds were not, and gender effects were found only for citric acid. Mojet, Christ‐Hazelhof, and Heidema (2001) noted elevated thresholds in 21 older (65–75 years) subjects relative to 21 younger (19–33 years) ones for NaCl, sucrose, aspartame, acetic acid, citric acid, caffeine, quinine, MSG, and inosine 5′‐monophosphate, in accord with our findings. However, sex effects were not generally evident. Barragán et al. (2018) examined taste intensity ratings for five concentrations of sucrose, NaCl, citric acid, PROP, l‐glutamic acid, and monopotassium salt monohydrate (MPG) in a sample of 1,020 Spanish subjects between the ages of 18 and 80 years. Age‐related decrements in taste perception were observed for all stimuli. Greater female performance was also found, although the effect was not statistically significant for MPG, the umami representative.
The overall split‐half correlation of the WETT observed in this study was strong (r = 0.90), with the subcomponents being less so (respective sweet, sour, bitter salty, and umami r's = 0.63, 0.69, 0.67, 0.48, and 0.42). When limitations on time are critical and a measure of overall function is needed, the first half of the test, that is, 27 items, can provide an accurate assessment of overall taste function. The sweet, sour, bitter, and salty coefficients were lower than those in the original validation study, which were 0.80, 0.77, 0.73, and 0.84, respectively. No value for MSG was presented in that study since its goal was to compare coefficients with other tests that did not employ MSG. The lower correlations of the present study likely reflect more attenuation of the range of the present test scores, since unlike the validation study, the subjects were non‐clinical subjects with normal taste function and a narrower range of test scores. It is well established that correlation coefficients are extremely sensitive to restricted ranges of data (Bland & Altman, 2011).
The present study has both strengths and weaknesses. Its strengths are the use of a well‐validated taste test and relatively large Chinese and American sample sizes. Its use of monosodium glutamate in addition to stimuli associated with the four classic taste qualities is also a strength, along with the fact that the test can be employed in settings where purified water is not available for rinsing. While the lower age of the Chinese sample would appear to be a limitation, the use of age as a covariate mitigated this problem. This study shares with most other taste studies the lack of random sampling of the population that was tested. Moreover, the present study did not assess regional taste differences despite the fact that these strips could be used for this purpose. While whole‐mouth testing is the best reflection of overall taste perception, future studies are needed to evaluate whether and to what degree regional differences are found in cross‐cultural studies.
CONFLICT OF INTEREST
R.L.D. is a consultant to Eisai Co, Merck Pharmaceuticals, the Michael J. Fox Foundation for Parkinson's Research, Septodont, Inc, and Johnson & Johnson. He receives royalties from Cambridge University Press, Johns Hopkins University Press, and John Wiley & Sons, and is president of, and a major shareholder in, Sensonics International, a manufacturer and distributor of smell and taste tests, including the test used in this study. The remaining authors have no disclosures.
ACKNOWLEDGMENTS
This work was supported by the Fundamental Research Funds for the Central Universities (JC, Grant No. xzy012020046) and the Basic Research Program of Natural Science Foundation of Shaanxi Province (JC, Grant No. 2021JQ‐418).
Chen, J. , Ren, X. , Yan, H. , Zhao, B. , Chen, J. , Zhu, K. , Lyu, H. , Li, Z. , & Doty, R. L. (2022). Comparison of Chinese and American subjects on the self‐administered Waterless Empirical Taste Test. Journal of Sensory Studies, e12745. 10.1111/joss.12745
Funding information Basic Research Program of Natural Science Foundation of Shaanxi Province, Grant/Award Number: 2021JQ‐418; Fundamental Research Funds for the Central Universities, Grant/Award Number: xzy012020046
DATA AVAILABILITY STATEMENT
Research data are not shared.
REFERENCES
- Barragán, R. , Coltell, O. , Portolés, O. , Asensio, E. M. , Sorlí, J. V. , Ortega‐Azorín, C. , … Corella, D. (2018). Bitter, sweet, salty, sour and umami taste perception decreases with age: Sex‐specific analysis, modulation by genetic variants and taste‐preference associations in 18 to 80 year‐old subjects. Nutrients, 10, 1539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bartoshuk, L. M. , Rifkin, B. , Marks, L. E. , & Bars, P. (1986). Taste and aging. Journal of Gerontology, 41, 51–57. [DOI] [PubMed] [Google Scholar]
- Bertino, M. , & Chan, M. M. (1986). Taste perception and diet in individuals with Chinese and European ethnic backgrounds. Chemical Senses, 11, 229–241. [Google Scholar]
- Bland, J. M. , & Altman, D. G. (2011). Correlation in restricted ranges of data. BMJ, 342, d556. [DOI] [PubMed] [Google Scholar]
- Doty, R. L. (2019). Epidemiology of smell and taste dysfunction. Handbook of Clinical Neurology, 164, 3–13. [DOI] [PubMed] [Google Scholar]
- Doty, R. L. , Heidt, J. M. , MacGillivray, M. R. , Dsouza, M. , Tracey, E. H. , Mirza, N. , & Bigelow, D. (2016). Influences of age, tongue region, and chorda tympani nerve sectioning on signal detection measures of lingual taste sensitivity. Physiology & Behavior, 155, 202–207. [DOI] [PubMed] [Google Scholar]
- Doty, R. L. , Nsoesie, M. T. , Chung, I. , Osman, A. , Pawasarat, I. , Caulfield, J. , … Leon‐Sarmiento, F. E. (2015). Taste function in early stage treated and untreated Parkinson's disease. Journal of Neurology, 262, 547–557. [DOI] [PubMed] [Google Scholar]
- Doty, R. L. , Wylie, C. , & Potter, M. (2021). Validation of the Waterless Empirical Taste Test (WETT®). Behavior Research Methods, 53, 864–873. [DOI] [PubMed] [Google Scholar]
- Essick, G. K. , Chopra, A. , Guest, S. , & McGlone, F. (2003). Lingual tactile acuity, taste perception, and the density and diameter of fungiform papillae in female subjects. Physiology & Behavior, 80, 289–302. [DOI] [PubMed] [Google Scholar]
- Fikentscher, R. , Roseburg, B. , Spinar, H. , & Bruchmuller, W. (1977). Loss of taste in the elderly: Sex differences. Clinical Otolaryngology and Allied Sciences, 2, 183–189. [DOI] [PubMed] [Google Scholar]
- Fischer, M. E. , Cruickshanks, K. J. , Schubert, C. R. , Pinto, A. , Klein, B. E. , Klein, R. , … Snyder, D. J. (2013). Taste intensity in the beaver dam offspring study. Laryngoscope, 123, 1399–1404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo, S. W. , & Reed, D. R. (2001). The genetics of phenylthiocarbamide perception. Annals of Human Biology, 28, 111–142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ketel, E. C. , de Wijk, R. A. , de Graff, C. , & Steiger, M. (2020). Effect of cross‐cultural differences on thickness, firmness and sweetness sensitivity. Food Research International, 152, 109890. 10.1016/j.foodres.2020.109890 [DOI] [PubMed] [Google Scholar]
- Kobayashi, C. , & Kennedy, L. M. (2002). Experience‐induced changes in taste identification of monosodium glutamate. Physiology & Behavior, 75, 57–63. [DOI] [PubMed] [Google Scholar]
- Lipchock, S. V. , Spielman, A. I. , Mennella, J. A. , Mansfield, C. J. , Hwang, L. D. , Douglas, J. E. , & Reed, D. R. (2017). Caffeine bitterness is related to daily caffeine intake and bitter receptor mRNA abundance in human taste tissue. Perception, 46, 245–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mennella, J. A. , Reed, D. R. , Roberts, K. M. , Mathew, P. S. , & Mansfield, C. J. (2014). Age‐related differences in bitter taste and efficacy of bitter blockers. PLoS One, 9, e103107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mojet, J. , Christ‐Hazelhof, E. , & Heidema, J. (2001). Taste perception with age: Generic or specific losses in threshold sensitivity to the five basic tastes? Chemical Senses, 26, 845–860. [DOI] [PubMed] [Google Scholar]
- Ribeiro, J. C. , Chaves, M. , Chaves, C. , Lemos, L. , Silva, E. D. , Paiva, A. , & Hummel, T. (2016). Cross‐cultural validation of a taste test with paper strips. European Archives of Oto‐Rhino‐Laryngology, 273, 3407–3411. [DOI] [PubMed] [Google Scholar]
- Rosenthal, E. (2000, December 14). In China, MSG is no headache, it's a new treat. New York Times, Section A, 3.
- Schier, L. A. , & Spector, A. C. (2019). The functional and neurobiological properties of bad taste. Physiological Reviews, 99, 605–663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sergi, G. , Bano, G. , Pizzato, S. , Veronese, N. , & Manzato, E. (2017). Taste loss in the elderly: Possible implications for dietary habits. Critical Reviews in Food Science and Nutrition, 57, 3684–3689. [DOI] [PubMed] [Google Scholar]
- Shu‐Fen, C. L. , Forde, C. G. , Tey, S. L. , & Henry, C. J. (2018). Taste sensitivities and diet of Chinese and Indians in Singapore. Asia Pacific Journal of Clinical Nutrition, 27, 681–685. [DOI] [PubMed] [Google Scholar]
- Singer‐Cornelius, T. , Cornelius, J. , Oberle, M. , Metternich, F. U. , & Brockmeier, S. J. (2021). Objective gustatory and olfactory dysfunction in COVID‐19 patients: A prospective cross‐sectional study. European Archives of Oto‐Rhino‐Laryngology, 278, 3325–3332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soter, A. , Kim, J. , Jackman, A. , Tourbier, I. , Kaul, A. , & Doty, R. L. (2008). Accuracy of self‐report in detecting taste dysfunction. Laryngoscope, 118, 611–617. [DOI] [PubMed] [Google Scholar]
- Steinbach, S. , Hundt, W. , Vaitl, A. , Heinrich, P. , Forster, S. , Burger, K. , & Zahnert, T. (2010). Taste in mild cognitive impairment and Alzheimer's disease. Journal of Neurology, 257(2), 238–246. [DOI] [PubMed] [Google Scholar]
- Stinton, N. , Atif, M. A. , Barkat, N. , & Doty, R. L. (2010). Influence of smell loss on taste function. Behavioral Neuroscience, 124, 256–264. [DOI] [PubMed] [Google Scholar]
- Weiffenbach, J. M. , Baum, B. J. , & Burghauser, R. (1982). Taste thresholds: Quality specific variation with human aging. Journal of Gerontology, 37, 372–377. [DOI] [PubMed] [Google Scholar]
- Wilkinson, L. (1990). SYSTAT: The system for statistics. Evanston, IL: SYSTAT, Inc. [Google Scholar]
- Yoshinaka, M. , Ikebe, K. , Uota, M. , Ogawa, T. , Okada, T. , Inomata, C. , … Maeda, Y. (2016). Age and sex differences in the taste sensitivity of young adult, young‐old and old‐old Japanese. Geriatrics & Gerontology International, 16, 1281–1288. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Research data are not shared.