

Abstract
Osteo-lipoma is a very rare benign tumor with a good prognosis. It is composed mainly of mature fatty tissue with a bony component. The diagnosis is based on the histological study, given the clinical and radiological characters that can simulate other benign or malignant pathologies. Osteosarcoma is the main differential diagnosis. The distinction between these two neoplasms is essential as the basis of the treatment is different. We report the case of a patient with a giant ossifying lipoma independent of bone tissue located in the thigh.
INTRODUCTION
Lipoma is a benign mesenchymal neoplasm composed of mature white adipocytes. Occasionally, it can contain other mesenchymal elements and form many variants. Osteolipoma is a very rare histological variant which is composed of mature lamellar bone within the lobules of mature adipocytes. It could be as parosteal or periosteal or more rarely independent of bone tissue. We present a rare case of a giant ossifying lipoma independent of bone tissue located in the thigh in a 48-year-old female patient.
CASE REPORT
We report the case of 48-year-old woman without notable pathological history, who consulted for a thigh mass that appeared 5 months ago. Clinical examination found a mass on the anterior surface of the root of the right thigh. It was mobile, firm and measured ~10 × 4 cm. The hip examination was unremarkable.
Radiographic examination by panoramic radiography showed thickening of the soft tissue of the right hip with calcifications (Fig. 1). Magnetic resonance imaging (MRI) revealed a well-circumscribed mass of the upper part of the anterior compartment of the thigh, non-attached to bone structures, measuring 11 × 4 cm. It has a high signal intensity on Tl and low signal intensity on T2, without enhancement after injection of gadolinium (Fig. 2) A diagnosis of lipoma was rendered.
Figure 1.

Standard X-ray of the hip profile (A) and face (B) with thickening of the soft tissue of the right hip with dispersed calcifications.
Figure 2.
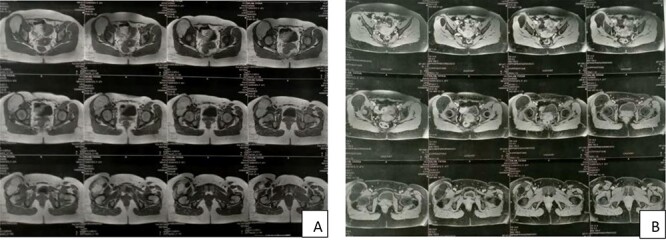
MRI showing a well-circumscribed mass in high signal intensity on Tl (A) and low signal intensity on T2 (B).
Faced with these radiological results, surgical excision of the mass was decided. We received the resected specimen weighing 222 g and measuring 10.5 × 4 × 3 cm. It was well limited and encapsulated. On the cut surface, this mass had a homogeneous fatty appearance with ossified areas (Fig. 3).
Figure 3.

Cut section of the resected specimen showing the fatty appearance with ossified areas.
Histopathologic examination showed lipomatous proliferation circumscribed by a thin fibrous capsule. It consisted of areas of mature and regular adipocytes without nuclear atypias or mitotic figures. Within this proliferation, we observed trabecular mature bone structures surrounded by regular osteoblastic cells. These elements were, by place, surrounded by a cartilaginous cap (Fig. 4).
Figure 4.

Microscopic image showing a fatty proliferation made of mature adipocytes dissociated by bony trabeculae (HE ×200, ×100).
The post-operative course was uneventful. No recurrence was observed after 14 months of clinical and radiological follow ups.
DISCUSSION
Lipoma is the most common mesenchymal benign neoplasm accounting for ~50% of all soft tissue neoplasms [1]. It occurs, most frequently, among adults between age 40 and 60 years of age and it is more common among men [2]. Lipoma can arise in subcutaneous tissue or deep soft tissues or on the surface of the bone (parosteal lipoma) [3]. Histologically, a conventional lipoma is composed of mature adipocytes. Other mesenchymal elements may be present and form many histological variants such as chondrolipomas (with cartilaginous areas), angiolipomas (with vascular elements) and fibrolipomas (with fibrous elements) [3].
Osteolipoma is a rare histologic variant of lipoma which contains areas of bone formation. The first case was reported by Plaut et al. in 1959 [4].
Various theories concerning the pathogenesis of osteolipoma have been advanced. Some authors have reported that ossification is secondary to repeated trauma or possibly ischemia that lead to metaplasia of the fibrous elements pre-existing within the tumor. Other authors support the theory that blood-borne monocytes or osteogenic factors convert fibroblasts into osteoblasts in a metaplastic response. A third theory suggests these tumors may originate directly from pluripotent stem cells which differentiate into lipoblasts, or osteoblasts and fibroblasts, characterizing a mesenchymoma [5].
Chromosomal abnormalities, such as translocations in 11q13, are found in osteolipomas [6].
In the different reviews of the literature, osteolipomas have been reported in variant locations, including head and neck, thigh, hand, oral cavity, paravetetebral and the suprasellar and hypothalamic regions [7]. This tumor arises more frequently inside or adjacent to bone and forms intraosseous, parosteal or periosteal forms. Only a few cases of osteolipomas independent of bone structures are reported in the literature [8].
Clinically, osteolipomas are generally painless and show slow progression [9].
Radiologically, different imaging techniques may be used, including panoramic radiography and MRI. However, lipoma variants do not present specific features and may suggest other diagnoses, including well-differentiated liposarcomas [10].
The definitive diagnosis is retained after the anatomopathological results. The pathological examination shows a trabecula of bone within the mature adipose cells without cellular atypia.
The differential diagnoses for osteolipomas depend on the locations. Generally, It includes osteochrondromas, myositis ossificans, teratoma and well-differentiated liposarcomas [11].
Complete surgical excision is the optimal treatment of osteolipoma [12].
It rarely recurs, and no cases of malignant transformation have been reported [13].
CONCLUSION
Osteolipoma is a very rare histological variant of lipoma with a good prognosis. The definitive diagnosis is based on pathological examination. The main challenge for the pathologist is to differentiate these benign lesions from other malignant differential diagnoses, mainly well-differentiated liposarcomas.
Contributor Information
Ihssan Elouarith, Pathology Department, Faculty of Medicine and Pharmacy, Oncology National Institute, Mohammed V University, Rabat 10100, Morocco.
Salma Elmajoudi, Pathology Department, Faculty of Medicine and Pharmacy, Oncology National Institute, Mohammed V University, Rabat 10100, Morocco.
Kadiri Habiba, Pathology Department, Faculty of Medicine and Pharmacy, Oncology National Institute, Mohammed V University, Rabat 10100, Morocco.
Soumaya Ech-charif, Pathology Department, Faculty of Medicine and Pharmacy, Oncology National Institute, Mohammed V University, Rabat 10100, Morocco.
Youssef Mahdi, Pathology Department, Faculty of Medicine and Pharmacy, Oncology National Institute, Mohammed V University, Rabat 10100, Morocco.
Mouna Khmou, Pathology Department, Faculty of Medicine and Pharmacy, Oncology National Institute, Mohammed V University, Rabat 10100, Morocco.
Basma El khannoussi, Pathology Department, Faculty of Medicine and Pharmacy, Oncology National Institute, Mohammed V University, Rabat 10100, Morocco.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
This study was not funded.
CONSENT FOR PUBLICATION
Written consent has been obtained from the patient and the patient’s family for the publication of this case report.
GUARANTOR
Ihssan Elouarith.
References
- 1. Nie P, Guo J, Xu Y, He Z, Han M, Dai B, et al. Parosteal ossifying lipoma of the clavicle: a case report. Mol Clin Oncol 2017;6:419–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Castilho RM, Squarize CH, Nunes FD, Pinto Júnior DS. Osteolipoma: a rare lesion in the oral cavity. Br J Oral Maxillofac Surg 2004;42:363–4. [DOI] [PubMed] [Google Scholar]
- 3. WHO Classification of Tumours Editorial Board . Soft tissue and bone tumours. Lyon (France): International Agency for Research on Cancer, 2020. [Google Scholar]
- 4. Plaut GS, Salm R, Truscott DE. Three cases of ossifying lipoma. J Pathol Bacteriol 1959;78:292. [PubMed] [Google Scholar]
- 5. Bohm KC, Birman MV, Silva SR, Lesperance MM, Marentette LJ, Beyer GR, et al. Ossifying lipoma of c1-c2 in an adolescent. J Pediatr Orthop 2011;31:e53–6. [DOI] [PubMed] [Google Scholar]
- 6. Firth NA, Allsobrook OFL, Patel M. Osteolipoma of the buccal mucosa: a case report. Aust Dent J 2017;62:378–81. [DOI] [PubMed] [Google Scholar]
- 7. Brones A, Mengshol S, Wilkinson CC. Ossifying lipoma of the cervical spine. J Neurosurg Pediatr 2010;5:283–4 Retrieved Jan 5, 2022. [DOI] [PubMed] [Google Scholar]
- 8. Demiralp B, Alderete JF, Kose O, Ozcan A, Cicek I, Basbozkurt M. Osteolipoma independent of bone tissue: a case report. Cases J 2009;2:8711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Cakir Karabas H, Ozcan I, Soluk Tekkesin M, Isler SC. Osteolipoma: a review of the literature and a rare case report. Oral Radiol 2021;37:560–5. [DOI] [PubMed] [Google Scholar]
- 10. Gaskin CM, Helms CA. Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): results of MRI evaluations of 126 consecutive fatty masses. AJR Am J Roentgenol 2004;182:733–9. [DOI] [PubMed] [Google Scholar]
- 11. Minutoli F, Mazziotti S, Gaeta M, et al. Ossifying lipoma of the parapharyngeal space: CT and MRI findings. Eur Radiol 2001;11:1818–21. [DOI] [PubMed] [Google Scholar]
- 12. Adebiyi KE, Ugboko VI, Maaji SM, Ndubuizu GTU. Osteolipoma of the palate: report of a case and review of the literature. Niger J Clin Pract 2011;14:242–4. [DOI] [PubMed] [Google Scholar]
- 13. Fukushima Y, Kitamura T, Hayashi N, Enoki Y, Sato T, Yoda T. A huge osteolipoma involving the coronoid process: a case report. J Oral Sci 2016;58:141–4. [DOI] [PubMed] [Google Scholar]