

Abstract
Objectives
This study aimed to evaluate the psychological and financial distress reported by citizens and permanent residents stranded abroad due to international travel restrictions introduced in response to the COVID-19 pandemic.
Design
An international cross-sectional study.
Setting
A primary analysis of data collected between July and September 2021 through an online survey targeting individuals stranded abroad and unable to return to their country of residence due to international travel restrictions.
Respondents
A total of 1054 individuals aged 18–84 years.
Data analysis
Multivariable logistic regression models were used to explore the relationship between higher levels of depression, anxiety and stress and participant variables.
Outcome measures
The survey answered questions regarding COVID-19 travel restriction-related impacts: personal stress, anxiety and depression (using the validated 21-item Depression, Anxiety and Stress Scale (DASS-21) tool), as well as impacts on housing and financial security and demographic data.
Results
A total of 75.4% of respondents reported wanting to return to the Oceania region (75.4%), with 45% stranded in Europe. 64.2% reported financial distress while stranded abroad. 64.4% (x̄=9.43, SD=5.81) reported moderate-to-extremely severe (based on the DASS-21 classification) levels of depression, 41.7% for anxiety (x̄=5.46, SD=4.74), and 58.1% for stress (x̄=10.64, SD=5.26). Multivariable analysis indicated that financial stress, an employment change, being <30 years, having a high perceived risk of contracting COVID-19 abroad and being stranded for >2 months were significantly related to scores of moderate-to-extremely severe depression, anxiety and stress.
Conclusion
The study is among the first to explore the psychological and financial distress-related impacts associated with being stranded abroad due to COVID-19 travel restrictions. It highlights a range of unintended consequences that arise from pandemic-related travel restrictions, identifies the health and social needs of a particularly vulnerable population, and provides clues as to the types of support that may be adopted to best support them.
Keywords: COVID-19, Public health, MENTAL HEALTH, INFECTIOUS DISEASES
Strengths and limitations of this study.
This study was open to participants worldwide to support a broad insight into the psychological and financial impact of COVID-19-related travel restrictions.
This study addressed the psychological impact of COVID-19-related travel restrictions using the validated 21-item Depression, Anxiety and Stress Scale, strengthening statistical analyses.
Multivariable analyses were conducted on respondents’ depression, anxiety, and stress scores to explore predictor and protective factors.
Psychological data were collected on self-reported scales, leading to responder bias.
Participant recruitment relied on convenience sampling and may not have captured impacted individuals from all relevant countries.
Background
In response to the COVID-19 pandemic, most countries worldwide have implemented some level of international travel restrictions or complete border closures.1–3 As of February 2020, many countries had commenced repatriation of their citizens stranded abroad. By the end of 2020, some countries like Japan and Spain claimed to have repatriated entirely every citizen who wanted to return. Reports continue to suggest stranded travellers were still trying to get to their country of residence (referred to as ‘home’) 20 months into the COVID-19 pandemic despite many countries reopening borders.4 5 In September 2021, every country has some level of travel restrictions (except those without data), with many countries still maintaining total border closures, while others had in place quarantine systems, screening measures and travel bans on high-risk regions.6
Factors impacting a person’s ability to return to their home have included countries placing limits on the number of passengers who can enter the country, caps on the hotel quarantine capacities, the cost of travel and hotel quarantine, and in some cases having restrictions on flights from certain high-risk countries. Our previous study suggested that the support available to those stranded abroad was limited and in some cases, challenging to access and comprehend.7 Support provided by countries has varied from repatriation flights, emergency accommodation, mental health and medical assistance, emergency call lines and financial assistance. However, of the countries that were reviewed, we were unable to identify any one country providing all the different support types listed.
Public commentary through news and social media has hinted at the level of psychosocial impact of these travel restrictions on citizens stranded abroad. These articles suggest that many of these travellers have felt abandoned by their governments, had little financial support, and for some, experienced depression and homelessness.8–10 While the findings from many COVID-19 studies have reported high levels of psychological distress in nearly all populations, the focus of these studies has been on domestic populations, like healthcare and frontline workers, students and those in lockdown and quarantine.10–19 With similar aims to the present study, one study found 63% of Saudi citizens living abroad as students during COVID-19 experienced ‘psychiatric’ distress symptoms.20
Even though travel restrictions have been in place since early 2020, there is currently a limited understanding of the level of psychological distress that has been experienced by those stranded abroad wanting to return. This study examined the impacts of travel restrictions on people stranded abroad who could not return to their country of citizenship/residence during the COVID-19 pandemic. We aimed to (1) measure the prevalence of psychological impact associated with being stranded overseas due to COVID-19-related travel restrictions, and (2) identify demographic and circumstantial factors associated with severe psychological impact.
Methods
Population and procedures
An online survey was created and administered anonymously using the Qualtrics21 survey platform, with respondents recruited through various social media channels. Respondents were those people who were either still stranded away from their country of residence/home or had been stranded at some point since the commencement of the COVID-19 pandemic. There were no limitations placed on the country of residence or the length of time the person had been stranded for. To meet the inclusion criteria, respondents had to self-identify as having attempted to return to their country of residence but have had their travel plans changed. The survey was open between 20 July 2021 and 24 September 2021. Respondents’ unique IP addresses prevented duplicate entries. This study did not receive any funding.
Patient and public involvement
No patient involved.
Survey instruments and measures
Demographics: including gender, age, level of education, ethnicity, employment status, history of chronic illness and living status. Ethnicity was classified based on the nine broad groups according to the Australian Standard Classification of Cultural and Ethnic Groups.22
Travel experiences: respondents were asked where they were stranded abroad and where they intended to return to, and these data were recoded into geographical groups based on the WHO regions.23 Questions focused on their current situation (whether they had returned, were still stranded abroad awaiting return or still abroad but had decided to stay), flight cancellations/delays, length of time waiting to return and their experiences with travel.
Mental well-being: the 21-item Depression, Anxiety and Stress Scale (DASS-21) was used in this study.24 The DASS-21 is a validated self-report tool, previously used in COVID-19 research studies,14 25 containing 21 items assessing scores of depression, anxiety and stress symptoms (seven items each). Respondents were asked to reflect on when they were stranded abroad (for respondents who had already returned reflecting on the last 2 weeks and rate each statement on a 4-point Likert scale from 0 (unsure/do not recall; did not apply to me at all) to 3 (applied to me very much, or most of the time)). Scores in subsection are then multiplied by 2 to give a final score categorising the depression, anxiety and stress into normal (depression: 0–9; anxiety: 0–7; stress: 0–14), mild (depression: 10–13; anxiety: 8–9; stress: 15–18), moderate (depression: 14–20; anxiety: 10–14; stress: 19–25), severe (depression: 21–27; anxiety: 15–19; stress: 26–33) or extremely severe (depression: 28+; anxiety: 20+; stress: 34+). Higher scores reflect increased emotional and psychological distress.
As we suspected some potential respondents had returned home already and could be potentially reflecting further than 2 weeks, we included an additional option of ‘unsure/do not recall’, with any respondent who selects this option to be removed from DASS-21 analysis, which would allow for removal of recall bias during the analyses phase. Respondents were asked whether they had access to crisis support or mental health services while abroad and if ‘yes’, whether they had used this service or support. Finally, respondents reported their perceived risk of contracting COVID-19 both in the country where they are/were stranded and the country where they had or were waiting to return to (scale of 1–10; 1 being no risk and 10 being high risk).
Financial well-being: respondents were initially asked whether they felt financial stress while stranded abroad (yes/no), then if ‘yes’ were asked how they addressed the financial stress (receiving financial support from family, government loans, bank credit or social services). Questions on employment situation and changes while abroad were asked along with a question on whether the participant experienced homelessness while abroad. Homelessness was defined as a period where respondents did not have somewhere to stay/live.
Statistical analyses
We aimed to collect responses from a minimum of 1200 people to allow analysis with a margin of error of approximately 3.2%. Descriptive analysis involved the calculation of means, SD, CI and SEs. Χ2 test of independence was first used to compare categorical variables. Independent variables that showed a significant association with DASS severity scores at a p<0.2 level were included in the model as predictor variables. The DASS scores were dichotomised to reflect either no/mild symptom severity or moderate-to-extremely severe. Multivariable logistic regression was then performed to analyse the effect of age, perceived risk of contracting COVID-19 while stranded, financial stress, time stranded, employment change and homelessness on predicting moderate-to-extremely severe DASS. No multicollinearity among variables was identified. P values of <0.05 were considered statistically significant. All data analyses were conducted using SPSS.26
Results
Respondent characteristics
A total of 1054 respondents completed the full survey, while a further 296 completed over 50% of the questions and were included in the descriptive analysis but excluded from regression analysis (see figure 1 for a full breakdown on inclusions). Demographic information is provided in table 1. The mean age was 41.09±13.08 years, with 69.5% (733 of 1054) being female, 43.8% (462 of 1054) of North-West European ethnicity, while most had tertiary education (90.7%, 956 of 1054) and were stranded in the European Region (45.3%, 608 of 1341) and were trying to return to the Western Pacific Region (WPR) (75.4%, 1011 of 1341).
Figure 1.
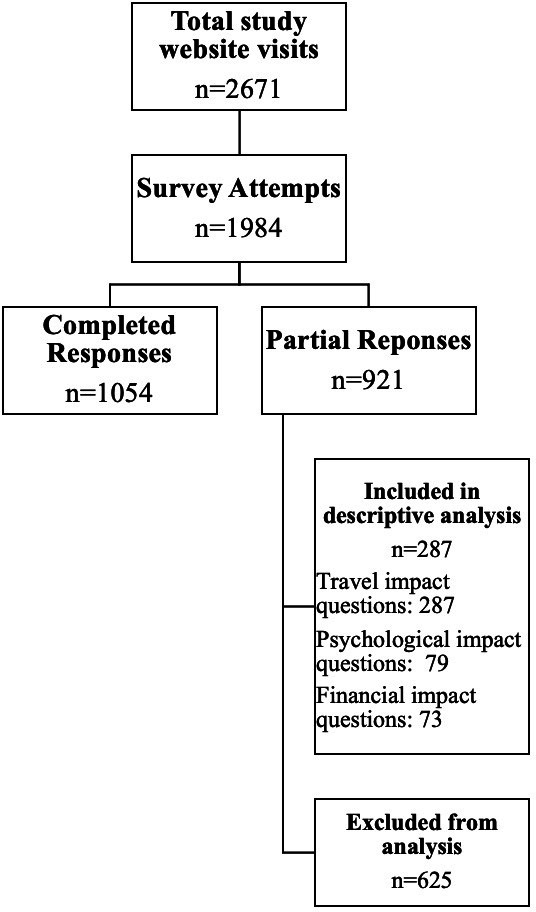
Flow chart of participant inclusion.
Table 1.
Characteristics of respondents stranded during COVID-19
| Variables | n | % |
| Sex recorded at birth | (1054) | |
| Female | 733 | 69.5 |
| Male | 308 | 29.2 |
| Another term | 2 | 0.2 |
| Prefer not to say | 11 | 0.8 |
| Gender | (1054) | |
| Female | 732 | 69.4 |
| Male | 304 | 28.8 |
| Another term | 5 | 0.5 |
| Prefer not to say | 13 | 1.2 |
| Age | (1054) | |
| 18–29 | 226 | 21.4 |
| 30–49 | 545 | 51.7 |
| 50–69 | 262 | 24.9 |
| 70+ | 21 | 1.1 |
| Main language spoken at home | (1054) | |
| English | 940 | 89.2 |
| Other | 83 | 7.9 |
| Spanish | 11 | 1.0 |
| Urdu | 7 | 0.7 |
| French | 7 | 0.7 |
| Chinese | 6 | 0.6 |
| Highest level of education | (1054) | |
| Tertiary education | 956 | 90.7 |
| Secondary education | 91 | 8.6 |
| Primary education | 5 | 0.5 |
| No formal education | 2 | 0.2 |
| Current employment situation | (1250) | |
| Working now for pay | 620 | 56.0 |
| Unemployed | 240 | 21.7 |
| Other | 95 | 8.6 |
| Student | 88 | 7.9 |
| Live with parents/guardians | 86 | 8.0 |
| Stay-at-home parent/caregiver | 84 | 7.6 |
| Retired | 82 | 7.4 |
| Volunteer | 23 | 2.1 |
| Unable to work due to disability or illness | 18 | 1.6 |
| Ethnicity | (1054) | |
| North-West European | 462 | 43.8 |
| Oceanian | 242 | 23 |
| Unsure | 134 | 12.7 |
| South-East Asian | 70 | 6.6 |
| Southern and Eastern European | 68 | 6.5 |
| Southern and Central Asian | 27 | 2.6 |
| People of the Americas | 26 | 2.5 |
| North-East Asian | 11 | 1.0 |
| North African and Middle Eastern | 10 | 0.9 |
| Sub-Saharan African | 4 | 0.4 |
| Usual country of residence | (1341) | |
| WPR | 1011 | 75.4 |
| EUR | 176 | 13.1 |
| AMR | 93 | 6.9 |
| SEAR | 29 | 2.2 |
| EMR | 25 | 1.9 |
| AFR | 7 | 0.5 |
| Country where stranded | (1341) | |
| EUR | 608 | 45.3 |
| WPR | 311 | 23.2 |
| AMR | 238 | 17.7 |
| EMR | 79 | 5.9 |
| SEAR | 78 | 5.8 |
| AFR | 27 | 2.0 |
| Initial reason for leaving country of residence | (1245) | |
| Long-term employment | 550 | 44.2 |
| Other | 272 | 21.8 |
| Visiting family or friends | 260 | 20.9 |
| Travel to study overseas | 72 | 5.8 |
| Travel for business | 54 | 4.3 |
| Tourism | 37 | 3.0 |
AFR, African Region; AMR, Region of the Americas; EMR, Eastern Mediterranean Region; EUR, European Region; SEAR, South-East Asian Region; WPR, Western Pacific Region.
Approximately 25% (303 of 1214) reported a historical or current COVID-19 infection, and of those the majority rated a ‘mild’ symptom severity (85.1%, 258 of 303). Respondents’ mean overall level of perceived risk of contracting COVID-19 while abroad (on a scale of 1–10, where 1=no risk and 10=high risk) was 6.64 (n=1182, SD=2.85), with 24.7% (300 of 1214) rating the perceived risk while abroad at high risk.10 Comparatively, the overall mean level of perceived risk of contracting COVID-19 in the country where respondents had returned to was 4.11 (n=673, SD=2.81), with only 8.02% (54 of 673) rating the perceived risk at ‘home’ as high risk.
Travel experiences
Initially, 44% (550 of 1245) of respondents had left their country of residence to take up long-term employment, with over 60% stranded abroad for more than 5 months (63.7%, 854 of 1341), with 28.7% (357 of 1245) either having had booked a flight or awaiting flight availability (refer to table 2 for a full breakdown of respondents’ experiences and current situation while stranded abroad).
Table 2.
Travel experiences of respondents stranded abroad during COVID-19
| Variables | n | % |
| Time stranded abroad | (1341) | |
| <1 month | 89 | 6.6 |
| 1–2 months | 91 | 6.8 |
| 2–3 months | 128 | 9.5 |
| 3–5 months | 98 | 7.3 |
| >5 months | 853 | 63.6 |
| No wait | 82 | 6.1 |
| Number of flight cancellations/changes | (1245) | |
| Not applicable | 319 | 25.6 |
| 0 changes | 152 | 12.2 |
| 1 cancellation or delay | 245 | 19.7 |
| 2 cancellations or delay | 196 | 15.7 |
| 3 cancellations or delay | 147 | 11.8 |
| 4 cancellations or delay | 65 | 5.2 |
| 5 cancellations or delay | 31 | 2.5 |
| >5 cancellations or delays | 90 | 7.2 |
| Experiences while trying to return | (1245) | |
| Limit on the number of people who could enter the country | 740 | 59.4 |
| Inability to book a flight | 671 | 53.9 |
| Flight cancellation | 660 | 15.3 |
| COVID-19 testing requirements prior to flying | 281 | 22.6 |
| Other | 229 | 18.4 |
| Separation from family/companion | 172 | 13.8 |
| Visa issues | 147 | 11.8 |
| Delays during transit | 44 | 3.5 |
| Current situation | (1245) | |
| Booked a flight/waiting for flight availability | 357 | 26.6 |
| Unable to return but have decided to stay | 352 | 26.2 |
| Returned to country of residence after delays | 323 | 24.1 |
| Other | 295 | 22 |
| Returned to country of residence after being stuck in transit | 14 | 1 |
Mental well-being
Figure 2 presents the respondents’ (n=1133) self-reported depression, anxiety and stress symptom severity score categories based on the DASS-21 tool. Of the respondents, 64.4% scored moderate-to-extremely severe depression symptoms (x̄=18.87, SD=11.62), 41.7% scoring moderate-to-extremely severe anxiety symptoms (x̄=10.91, SD=9.47), and 58.1% scoring between moderate and extremely severe stress symptoms (x̄=21.48, SD=10.52).
Figure 2.

Depression, anxiety and stress categories of citizens stranded abroad during COVID-19 (% of sample).
Many reported no access to crisis support or mental health services while abroad (63.5%, 719 of 1133), and of those who did have access, only 37.9% (157 of 414) used the services. A total of 12% (133 of 1112) experienced a period of homelessness while stranded abroad. Of those who were willing to share their experiences (n=94 of 133), commonly noted situations included living in temporary accommodation (32%, 30 of 94), sleeping on the couch or in a spare bedroom at a friend/family member’s place (32%, 30 of 94) and staying in emergency accommodation (including homeless shelters) (17%, 16 of 94). Less common experiences were those who lived on the street, trains, at the airport, in cars and in tents (<20%, 18 of 94). Two respondents disclosed having experienced a sexual assault while staying at a homeless shelter.
Financial well-being
Financial distress was reported in 64.2% (723 of 1127), and 38.4% (433 of 1127) reported a change in employment. A breakdown of ways in which respondents sought to address financial distress along with employment changes and current employment situation is reported in table 3.
Table 3.
Financial and employment characteristics of respondents stranded abroad during COVID-19
| Variables | n | % |
| Addressing financial stress | (n/836 responses) | % of respondents (n=1127) |
| Received financial support from family or friends | 354 | 31.4 |
| Other | 201 | 17.8 |
| Borrowed money from a bank | 58 | 5.1 |
| Personal savings | 47 | 4.2 |
| Accessed emergency financial support from the organisation or services in the country you were stuck | 43 | 3.8 |
| Received financial support from employer | 39 | 3.5 |
| Applied but did not receive a government loan | 39 | 3.5 |
| Early withdrawal of superannuation | 27 | 2.4 |
| Received a government loan to cover living costs | 14 | 1.2 |
| Received a government loan to cover the cost of a flight home | 8 | 0.7 |
| Received financial support from an insurance company | 6 | 0.5 |
| Current employment situation | (1250) | |
| Working now for pay | 620 | 56.0 |
| Unemployed | 240 | 21.7 |
| Retired | 82 | 7.4 |
| Student | 88 | 7.9 |
| Unable to work due to disability or illness | 18 | 1.6 |
| Volunteer | 23 | 2.1 |
| Stay-at-home parent/caregiver | 84 | 7.6 |
| Other | 95 | 8.6 |
| Employment change while abroad | (n/717 responses) | % of respondents (n=1127) |
| Worked remotely | 123 | 10.9 |
| Lost job | 119 | 10.6 |
| Other | 113 | 10.0 |
| Resigned | 77 | 6.8 |
| Contract not renewed | 69 | 6.1 |
| Reduction of hours | 63 | 5.6 |
| Stood down, not working for pay, but not fired | 45 | 4.0 |
| Pay cut | 32 | 2.8 |
| Back in paid work | 31 | 2.8 |
| Not working but receiving government assistance | 27 | 2.4 |
| Increase in hours | 18 | 1.6 |
Factors associated with and predictors of depression, anxiety and stress
Χ2 analyses revealed significant associations between respondents’ DASS categories and their age, time stranded abroad, financial stress, homelessness, employment change and their perceived risk of contracting COVID-19 (on a scale from 1 to 10, with 1–3 being considered low risk, 4–6 moderate risk and 7–10 high risk). No associations were found between DASS severity categories and having access to crisis support or mental health services (see online supplemental file 1). For depression, logistic regression identified financial stress, employment change and a high perceived risk of contracting COVID-19 as predictors of moderate-to-extremely severe depression. Overall, the model correctly discriminated 67.7% of cases and Nagelkerke R2 indicated a 14% variation of depression explained by the model. For anxiety, logistic regression identified financial stress, employment change and a high perceived risk of contracting COVID-19, as predictors of moderate-to-extremely severe anxiety. Overall, the model correctly discriminated 64.5% of cases and Nagelkerke R2 indicated a 13% variation of anxiety explained by the model. Finally for stress, logistic regression identified financial stress, employment change and a high perceived risk of contracting COVID-19, as predictors of moderate-to-extremely severe stress. Overall, the model showed goodness of fit to the data (χ2 (14)=95.772, p<0.001), correctly discriminated 63.6% of cases and Nagelkerke R2 indicated a 13% variation of stress explained by the model. Table 4 presents results of the multivariable logistic regression. Being 30 years or older and stranded for 2 months or less were associated with decreased odds of moderate-to-extremely severe depression, anxiety and stress.
Table 4.
Predictors of moderate-to-extremely severe depression, anxiety and stress in respondents stranded abroad during COVID-19 (n=956)
| Variables | Depression | Anxiety | Stress | ||||||
| OR | 95% CI | P value | OR | 95% CI | P value | OR | 95% CI | P value | |
| Age (years) | 0.005 | 0.030 | 0.007 | ||||||
| 18–29* | |||||||||
| 30–49 | 0.535 | 0.366 to 0.780 | 0.646 | 0.461 to 0.906 | 0.644 | 0.452 to 0.917 | |||
| 50–69 | 0.542 | 0.350 to 0.839 | 0.563 | 0.375 to 0.845 | 0.579 | 0.383 to 0.873 | |||
| >69 | 0.303 | 0.097 to 0.945 | 0.767 | 0.238 to 2.407 | 0.174 | 0.046 to 0.660 | |||
| Perceived risk of COVID-19 | 0.026 | 0.003 | 0.003 | ||||||
| Not applicable | 1.595 | 0.384 to 6.627 | 1.608 | 0.433 to 5.840 | 2.317 | 0.573 to 9.368 | |||
| Low risk* | |||||||||
| Moderate risk | 1.099 | 0.723 to 1.672 | 0.700 | 0.456 to 1.076 | 1.042 | 0.691 to 1.571 | |||
| High risk | 1.617 | 1.147 to 2.279 | 1.364 | 0.973 to 1.912 | 1.708 | 1.223 to 2.387 | |||
| Time stranded | <0.001 | <0.001 | 0.003 | ||||||
| No wait | 0.893 | 0.399 to 1.997 | 0.697 | 0.308 to 1.579 | 0.936 | 0.421 to 2.082 | |||
| <1 month | 0.357 | 0.174 to 0.735 | 0.332 | 0.149 to 0.738 | 0.459 | 0.224 to 0.940 | |||
| 1–2 months | 0.396 | 0.201 to 0.781 | 0.420 | 0.208 to 0.849 | 0.475 | 0.242 to 0.932 | |||
| 2–3 months | 0.587 | 0.313 to 1.101 | 0.571 | 0.303 to 1.078 | 0.702 | 0.377 to 1.308 | |||
| 3–5 months* | |||||||||
| >5 months | 1.281 | 0.770 to 2.129 | 0.984 | 0.601 to 1.610 | 1.062 | 0.647 to 1.743 | |||
| Homelessness, ref no | 1.522 | 0.947 to 2.444 | 0.082 | 1.392 | 0.920 to 2.105 | 0.118 | 1.186 | 0.767 to 1.834 | 0.444 |
| Employment change, ref no | 1.405 | 1.040 to 1.900 | 0.027 | 1.569 | 1.177 to 2.092 | 0.002 | 1.564 | 1.171 to 2.090 | 0.002 |
| Financial stress, ref no | 1.501 | 1.103 to 2.041 | 0.010 | 1.728 | 1.268 to 2.345 | <0.001 | 1.682 | 1.246 to 2.269 | <0.001 |
OR, log OR controlling for other variables in the model; EXP (B), adjusted OR; p, probability value (statistically significant <0.05).
*Reference variable.
bmjopen-2021-059922supp001.pdf (142.1KB, pdf)
Discussion
This study evaluated the psychological and financial distress of individuals stranded abroad during the COVID-19 pandemic and highlights the importance of providing additional support to this vulnerable group in future public health events. Among our respondents, we found that over half had been stranded for longer than 5 months, with the majority having more than one flight cancellation or change. Our results confirm sentiments shared on social media by people stranded abroad that reflect experiences of having no financial support, depression, homelessness and a general feeling of abandonment by their governments.8–10
Given the continued flight changes and delays (incurring additional costs) in the population of individuals stranded abroad, along with changes to employment, it is perhaps not surprising that we documented a high level of financial distress (64.2%), employment changes (38.4%) and experiences of homelessness (12%). Our findings align with results from non-travel-related COVID-19 studies which have indicated an increase in financial distress,17 increases in experiences of homelessness27 and growing employment changes28 during the pandemic. Comparatively, we reported much higher findings compared with a survey of the general population conducted within the first 6 months of the pandemic, a finding that 30% of Australians were financially stressed because of the pandemic.29 This difference could be explained by those stranded abroad having different elements of uncertainty (additional flight costs, additional rent, expenses due to the length of time stranded and uncertain employment) compared with the general population.
Based on our findings, we recommend policymakers prioritise increasing the availability of financial assistance in the form of government grants or loans for living and flight costs incurred due to being stranded abroad, or alternatively providing the option to access social support while abroad if an individual would have been eligible had they not been abroad. Furthermore, considering the proportion of people who reported experiencing homelessness, the cases of sexual assault within homeless shelters and previous research indicating a lack of emergency accommodation options for citizens abroad during COVID-19,7 it is recommended that policymakers provide a solution to these issues. Whether it be through financial assistance or an emergency accommodation programme similar to those that the French and Spanish governments introduced, where citizens residing permanently abroad have the option of offering accommodation or a room to citizens who are stranded, governments have to prioritise a solution and effectively communicate this support package.7
At this stage in the pandemic, it is almost indisputable that COVID-19 has had a psychological impact on populations around the world, whether it be healthcare workers, people in lockdown or quarantine, or specific countries or communities, the stressors were all encompassing.11–14 19 30 Our findings reflect much higher incidence of moderate-to-extremely severe depression (64.4%), anxiety (41.7%) and stress (58.1%), compared with domestic populations around the world.25 Previous research shows lower DASS severity scores,25 especially when comparing our results with studies exploring psychological impacts of COVID-19 on healthcare workers31 32 and domestic students.33 34 One study observing the psychological correlates of COVID-19 on the general population in Austria reported drastically lower scores of depression (21.6%), anxiety (28.6%) and stress (28%), and found that ‘frequent contact with family or friends’ was shown to be a protective factor.25
However, research on international students during COVID-19 has reflected high DASS severity, aligned with our study findings.20 35 Possible reasons for these differences could be the parallels between international student experiences and those stranded, both living abroad and arguably away from their immediate social support network (family). A range of factors contributed to the psychological well-being of individuals in this study. Having financial stress, an employment change and having a high perceived risk of contracting COVID-19 were all associated with predicting moderate-to-extremely severe depression, anxiety and stress. Additionally, the length of time stranded was also associated with higher severity of DASS, with >5 months for depression and stress, and 3–5 months for anxiety. These results are not surprising considering the literature shows that many stressors, like financial distress, fear of COVID-19 infection, loneliness, inadequate information and employment issues, have all presented as predictors of poor mental health and in the case of financial distress, can go further than predicting depression to suicidal thoughts and behaviours.19 36 Unique to this study, however, is the finding that the longer an individual is stranded abroad, the more likely they are to present with moderate-to-severe DASS symptoms.
Interestingly, of the age categories in this investigation, respondents >69 years had lower scores of depression, anxiety and stress, inconsistent with research conducted in Spain and Canada suggesting increased DASS scores in elders.37 38 This, as was noted by the authors of the Sightlines Project,39 may be due to older people being more financially secured than other age groups. It may also reflect that older people were less likely to have insecurity associated with employment or have younger dependent family members to provide direct care to. This may have provided more opportunities for flexibility in their travel plans. These results, reflecting high severity of DASS in those stranded abroad, provide both current and future direction for policymakers. We recommend policymakers provide adequate mental health interventions to those stranded abroad, either online or face-to-face where possible through a local consulate.
It is hard to deny that people have been deprived of the ability to return to their country of citizenship or permanent residence, as shown by the 63.3% of our respondents being stranded abroad for longer than 5 months. Addressing public health threats from a health security perspective has already increased fears that it legitimises government actions, potentially undermining personal sovereignty and impeding human rights.40 A commonly cited human rights treaty in response to imposed restrictions is Article 1241 of the International Covenant on Civil and Political Rights (ICCPR), a treaty with 74 signatories and 173 parities which states that ‘No one shall be arbitrarily deprived of the right to enter his own country’.41
The most frequently mentioned human rights breach was the Australian government imposing not only a complete ban on incoming flights from India, but potential criminal penalties to Australian citizens or permanent residents of up to 5 years of imprisonment, and/or fines up to $A66 000, for attempting to enter Australia from India through a third country.42 Mostly in reference to breaching Article 1241 of the ICCPR, this ban, implemented under the Biosecurity Act 2015,43 between April and May 2021, has been labelled a ‘racist rights breach’,44 with the Australian Human Rights Commission approaching the federal government directly with their concerns.42 Due to impacts of ongoing border closures and individuals struggling to return home, as further highlighted in this study where the majority of respondents were trying to return to, Australian citizens stranded abroad submitted a human rights complaint to the United Nations (UN) Human Rights Committee under the ICCPR, with the UN Human Rights Committee already successfully requesting to the Australian Government the prompt repatriation of two Australians in April 2021.45
Due to the results of our study, alongside the probable human rights breaches, we recommend policymakers seriously reconsider current and future restriction of movement of citizens and permanent residents returning home who are at risk of financial distress and severe DASS the longer that they are stranded for. With international borders reopening around the world, some being restricted for nearly 20 months, it is critical to not only look at the impact of travel restrictions from the perspective of reducing infectious disease importations, but also from the perspective of those stranded abroad, who were arguably one of the most impacted by them. In doing so, policymakers can determine where further support is needed in future emergency situations resulting in people stranded abroad.
Limitations
This work is not without limitations. First, like other cross-sectional survey studies, it lacks a longitudinal follow-up on respondents. Second, the self-report questionnaire for psychological symptoms raises possible selection bias and subjectivity; however, our sample size being large, and the addition of an optional ‘do not recall’ response, should mitigate certain bias. Third, we were unable to capture the specific immigration status of those returning, that is, whether they were citizens, permanent residents or short-term visa holders. Finally, we did not examine pre-existing mental health conditions which could prove to be a confounding factor, and there was an over-representation of women, those returning to the WPR and respondents with an academic background, possibly due to convenience sampling issues and survey distribution originating in Australia, which may not fully represent the population of people who were stranded abroad. The study did not collect information on treatment of anxiety, stress or depression, nor did we collect data on suicidal ideation. Notwithstanding the previously mentioned limitations, findings from this study provide insights not previously reported into the psychological and financial impacts and support needed for individuals stranded abroad due to COVID-19 travel restrictions. These insights will be valuable for policymakers as they design and deliver support programmes in response and preparation for future events.
Conclusion
This research suggests that being stranded abroad during the COVID-19 pandemic may lead to not only an increase in financial stress, but also quite severe depression, anxiety and stress. Our findings show that being young, stranded abroad for a longer time, having a high perception of infection risk, experiencing employment changes and financial stress are all associated with increased severity of depression, anxiety and stress. Respondents reported lack of mental and social health support while stranded. This indicates that there are gaps in services available for this vulnerable population or lack of communication as to how to access them; both issues need to be resolved.
Supplementary Material
Footnotes
Twitter: @merusheel, @hollyseale
Contributors: PM conducted data collection, data analysis, manuscript writing and contributed to study design. AC, MS and HS conceived the study design, interpreted the data, were involved in manuscript writing and had final oversight. KB supported the statistical analysis of the data and ST supported the interpretation and write-up of the findings. All authors read and approved the final manuscript and HS is the guarantor.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available upon reasonable request. The data used in this study are available upon request from the authors.
Ethics statements
Patient consent for publication
Not required.
Ethics approval
Ethical approval for this study was granted by the UNSW Human Research Ethics Committee (#210418). All respondents indicated their consent to participate.
References
- 1.Chinazzi M, Davis JT, Ajelli M, et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020;368:395–400. 10.1126/science.aba9757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Seyfi S, Hall CM, Shabani B. COVID-19 and international travel restrictions: the geopolitics of health and tourism. Tourism Geographies 2020:1–17. [Google Scholar]
- 3.von Tigerstrom BJ, Halabi SF, Wilson KR. The International health regulations (2005) and the re-establishment of international travel amidst the COVID-19 pandemic. J Travel Med 2020;27. 10.1093/jtm/taaa127. [Epub ahead of print: 23 12 2020]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ministry of foreign Affairs to complete repatriation of Spaniards on close to 50 flights: Ministerio de Asuntos Exteriores, 2020. Available: http://www.exteriores.gob.es/Portal/en/SalaDePrensa/NotasdePrensa/Paginas/2020_NOTAS_P/20200430_NOTA065.aspx
- 5.Keynote Speech by Foreign Minister MOTEGI at the 2ND TOKYO GLOBAL DIALOGUE “Japan’s Foreign Policy towards the post-COVID-19 world”: Ministry of Foreign Affairs of Japan, 2021. Available: https://www.mofa.go.jp/fp/pp/page3e_001109.html
- 6.Hale T, Angrist N, Goldszmidt R, et al. A global panel database of pandemic policies (Oxford COVID-19 government response Tracker). Nat Hum Behav 2021;5:529–38. 10.1038/s41562-021-01079-8 [DOI] [PubMed] [Google Scholar]
- 7.McDermid P, Craig A, Sheel M, et al. How have governments supported citizens stranded abroad due to COVID-19 travel restrictions? A comparative analysis of the financial and health support in eleven countries. BMC Infect Dis 2022;22:161. 10.1186/s12879-022-07155-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Devlin M. "It was the worst possible situation": Canadians stuck abroad months into pandemic. DH News, 2020. [Google Scholar]
- 9.Fuller K. Australians stranded overseas 'betrayed', says a man telling of months of injury, illness and homelessness. ABC Illawarra, 2020. [Google Scholar]
- 10.Capper S. Abandoned overseas: The mental health toll of Australia’s closed borders on its citizens. SBS News, 2021. [Google Scholar]
- 11.Burke T, Berry A, Taylor LK, et al. Increased psychological distress during COVID-19 and quarantine in Ireland: a national survey. J Clin Med 2020;9:3481. 10.3390/jcm9113481 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dawel A, Shou Y, Smithson M, et al. The effect of COVID-19 on mental health and wellbeing in a representative sample of Australian adults. Front Psychiatry 2020;11. 10.3389/fpsyt.2020.579985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kalok A, Sharip S, Abdul Hafizz AM, et al. The psychological impact of movement restriction during the COVID-19 outbreak on clinical undergraduates: a cross-sectional study. Int J Environ Res Public Health 2020;17. 10.3390/ijerph17228522. [Epub ahead of print: 17 11 2020]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Newby JM, O'Moore K, Tang S, et al. Acute mental health responses during the COVID-19 pandemic in Australia. PLoS One 2020;15:e0236562. 10.1371/journal.pone.0236562 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.O’Sullivan D, Rahamathulla M, Pawar M. The impact and implications of COVID-19: an Australian perspective. The International Journal of Community and Social Development 2020;2:134–51. 10.1177/2516602620937922 [DOI] [Google Scholar]
- 16.Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr 2020;52:102066. 10.1016/j.ajp.2020.102066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Robillard R, Saad M, Edwards J, et al. Social, financial and psychological stress during an emerging pandemic: observations from a population survey in the acute phase of COVID-19. BMJ Open 2020;10:e043805. 10.1136/bmjopen-2020-043805 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sher L. The impact of the COVID-19 pandemic on suicide rates. QJM 2020;113:707–12. 10.1093/qjmed/hcaa202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Stevenson C, Wakefield JRH. Financial distress and suicidal behaviour during COVID-19: family identification attenuates the negative relationship between COVID-related financial distress and mental ill-health. J Health Psychol 2021;26:2665–75. 10.1177/13591053211014597 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Behisi MA, Altaweel HM, Gassas RF, et al. COVID-19 pandemic and mental health status of Saudi citizens living abroad. Int J Environ Res Public Health 2021;18. 10.3390/ijerph18157857. [Epub ahead of print: 25 Jul 2021]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Qualtrics . Qualtrics. Provo, Utah, USA, 2005. [Google Scholar]
- 22.Australian standard classification of cultural and ethnic groups (ASCCEG) 2016.
- 23.Alderslade R, Bellman M, Rawson N. The national childhood encephalopathy study: a report on 1000 cases of serious neurologic disorders in infants and young children from the NCES research team. In: Whooping cough: reports from the Committee on the Safety of Medicines and the Joint Committee on Vaccination and Immunisation. Department of Health & Social Security, HMSO; 1981, 1981: 1–184. [Google Scholar]
- 24.Lovibond PF, Lovibond SH. Manual for the depression anxiety stress scales. 2nd. Ed. Sydney: Psychology Foundation, 1995. [Google Scholar]
- 25.Traunmüller C, Stefitz R, Gaisbachgrabner K, et al. Psychological correlates of COVID-19 pandemic in the Austrian population. BMC Public Health 2020;20:1395. 10.1186/s12889-020-09489-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.IBM SPSS statistics for MAC. 28 ED. Armonk, NY: IBM Corp 2021.
- 27.Kunz. RSaM . COVID-19 impacts us all: ensuring the safety and well-being of people on temporary visas during COVID-19, 2020. [Google Scholar]
- 28.Tušl M, Brauchli R, Kerksieck P, et al. Impact of the COVID-19 crisis on work and private life, mental well-being and self-rated health in German and Swiss employees: a cross-sectional online survey. BMC Public Health 2021;21:741. 10.1186/s12889-021-10788-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Taking the pulse of the nation: Melbourne Institute’s Survey of the Impact of COVID-19 in Australia. The University of Melbourne 2020.
- 30.Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord 2020;277:55–64. 10.1016/j.jad.2020.08.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hammond NE, Crowe L, Abbenbroek B, et al. Impact of the coronavirus disease 2019 pandemic on critical care healthcare workers' depression, anxiety, and stress levels. Aust Crit Care 2021;34:146–54. 10.1016/j.aucc.2020.12.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lenzo V, Quattropani MC, Sardella A, et al. Depression, anxiety, and stress among healthcare workers during the COVID-19 outbreak and relationships with expressive flexibility and context sensitivity. Front Psychol 2021;12:623033. 10.3389/fpsyg.2021.623033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Juchnowicz D, Baj J, Forma A, et al. The outbreak of SARS-CoV-2 pandemic and the well-being of Polish students: the risk factors of the emotional distress during COVID-19 Lockdown. J Clin Med 2021;10:944. 10.3390/jcm10050944 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Vala N, Vachhani M, Sorani A. Study of anxiety, stress, and depression level among medical students during COVID-19 pandemic phase in Jamnagar City. Natl J Physiol Pharm Pharmacol 2020;10:1–5. 10.5455/njppp.2020.10.07205202031072020 [DOI] [Google Scholar]
- 35.Alam MD, Lu J, Ni L, et al. Psychological outcomes and associated factors among the International students living in China during the COVID-19 pandemic. Front Psychiatry 2021;12:707342. 10.3389/fpsyt.2021.707342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Serafini G, Parmigiani B, Amerio A, et al. The psychological impact of COVID-19 on the mental health in the general population. QJM 2020;113:531–7. 10.1093/qjmed/hcaa201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ozamiz-Etxebarria N, Dosil-Santamaria M, Picaza-Gorrochategui M, et al. Stress, anxiety, and depression levels in the initial stage of the COVID-19 outbreak in a population sample in the Northern Spain. Cad Saude Publica 2020;36:e00054020. 10.1590/0102-311X00054020 [DOI] [PubMed] [Google Scholar]
- 38.Nwachukwu I, Nkire N, Shalaby R, et al. COVID-19 pandemic: age-related differences in measures of stress, anxiety and depression in Canada. Int J Environ Res Public Health 2020;17. 10.3390/ijerph17176366. [Epub ahead of print: 01 09 2020]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.The Sightlines Project: seeing our way to living long & living well in 21st century America: Stanford Center on Longevity, 2016. Available: https://www.soa.org/globalassets/assets/files/research/projects/research-2016-sightlines-report.pdf
- 40.Indicators HJ. Indicators, security and sovereignty during COVID-19 in the global South. International Journal of Law in Context 2021;17:249–60. [Google Scholar]
- 41.International covenant on civil and political rights (16 December 1966).
- 42.Statement on travel ban and sanctions on Australians travelling from India . Australian human rights Commission, 2021. [Google Scholar]
- 43.Biosecurity act Sect. 477 (2015).
- 44.Australia’s India ban criticised as 'racist' rights breach. BBC News 2021.
- 45.Hicks E. A Right to Come Home? Repatriation Rights & Policy in Australia. Melbourne: The Univeristy of Melbourne, 2021. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2021-059922supp001.pdf (142.1KB, pdf)
Data Availability Statement
Data are available upon reasonable request. The data used in this study are available upon request from the authors.