

Abstract
Objectives
The study objectives were to examine: (1) adolescents’ media viewing habits, (2) associations with media viewing and self-reported exposure to unhealthy food and beverage advertising and (3) differences in trends among younger and older adolescents in six high and upper middle-income countries.
Design
Repeat cross-sectional online survey.
Setting
Australia, Canada, Chile, Mexico, the United Kingdom (UK) and the United States of America (USA).
Participants
Respondents to the International Food Policy Study who provided information on all variables of interest in November–December 2019 aged 10–17 years (n=9171).
Outcome measures
Self-reported exposure to screen-based media (screen time by media channel), use of social media platforms and self-reported location and frequency of exposure to unhealthy food and beverage advertising.
Results
The average amount of time spent in front of various screens ranged from 7.6 hours to 10.2 hours across countries per week day, which may include possible viewing of multiple media channels simultaneously. Overall, Instagram was the most popular social media platform (52%–68% by country), followed by Facebook (42%–79%) and Snapchat (28%–52%). The percentage of respondents who self-reported having seen unhealthy food advertisements in the past 30 days was highest on television (43%–69%), followed by digital media (27%–60%) and gaming applications (10%–17%). Self-reported daily exposure to advertising varied between countries for sugary drinks (10%–43%) and fast food (19%–44%) and was positively associated with self-reported screen time. Self-reported exposure to screen-based media and social media platforms differed by sociodemographic characteristics and was higher among older adolescents than younger adolescents.
Conclusions
The important amount of time spent on screen-based media reported by adolescents and large percentage of adolescents reporting social media usage, coupled with high rates of self-reported advertising exposure, support the need for policies to restrict marketing of unhealthy food and beverages appealing to adolescents on screen-based media.
Keywords: Food marketing, food policy, marketing to children, broadcast media, digital media, adolescents, food environment
Strengths and limitations of this study.
The study has a large sample size and employs the same measures across countries, allowing justifiable comparisons between countries.
Assessed self-reported exposure to a wide range of social media platforms and differentiated locations of self-reported exposure to screen-based advertisements.
Adolescents retrospectively self-reported the estimated screen time spent on each media channel rather than using a more objective approach.
Self-reported exposure to marketing may result in an underestimation of exposure to marketing, and this study provides a conservative estimate.
Time spent watching cable television versus on streaming applications (Netflix, Crave, Amazon Prime Video, etc) was not distinguished in this study.
Introduction
In recent decades, children and adolescents have become the targets of a variety of marketing techniques, many of which exploit their vulnerabilities. Children are most often not able to recognise the persuasive intent of marketing and may perceive it as entertainment, making them particularly susceptible to marketing content.1 Children and adolescents are a potentially important market segment, as effective marketing towards them can build early positive associations, create life-long consumers and brand relationships that extend into adulthood.2 3 As such, the World Health Organization (WHO) and others have called for restrictions on marketing to children and younger adolescents of specific products (such as tobacco or vaping products and unhealthy foods or beverages).4 Some jurisdictions, such as the province of Quebec (Canada), the UK, Chile and Mexico have implemented policies restricting unhealthy food marketing targeted at children and younger adolescents typically 13 years and under,5 as it is well established that food marketing influences children’s and adolescents’ dietary preferences for products, consumption patterns and shapes their purchasing behaviour as well as their purchase requests to parents.6–9
Effective food marketing depends on both exposure (defined as the number of people seeing the message and the frequency to which the person is exposed to the message) and power (defined as the ‘creative content, design and execution of the marketing message’), which both vary considerably between media channels or types.4 10 Various marketing techniques are used across media channels to optimise the effectiveness of marketing,8 11–14 and may differ both in their impact on children and adolescents as well as whether or not children and adolescents can recognise them as marketing.15 16 Screen-based media, which for the large part includes television, digital media (including social media) and gaming sites, all have different implications with regards to the exposure and power of marketing messages that reach their audience.
Companies are increasingly using digital platforms as a complement to traditional advertising on television in a mixed-media approach to maximise the reach, efficiency and effectiveness of marketing.17 18 Globally, time spent online on social media, gaming, streaming and browsing the web is significant and appears to be increasing in some countries,19 20 representing an important channel for advertising energy dense and nutrient-poor products.21–25 Given the shifting media consumption habits of children and adolescents, exploration of media consumption and associations with exposure to marketing of less healthy food products and their patterning by demographic and socioeconomic factors is warranted. Most studies to date that examine media consumption habits among children and adolescents have been limited to a single media type and do not examine exposure across multiple countries. This study aimed to explore adolescents’ media consumption habits (self-reported screen time and use of social media platforms) and associations with self-reported exposure to unhealthy food and beverage advertisements (location and frequency) across six high and upper middle-income countries (Australia, Canada, Chile, Mexico, UK and USA). As a secondary objective, the study aimed to examine differences in trends among younger adolescents (10–13 years) and older adolescents (14–17 years), the latter of which often fall outside the purview of policies restricting marketing of unhealthy food and beverages.
Subjects and methods
Data are from the 2019 International Food Policy Study (IFPS) Youth Survey, an annual repeat cross-sectional survey conducted in Australia, Canada, Chile, Mexico, the UK and the USA. Data were collected via self-completed, web-based surveys conducted in November–December 2019 with adolescents aged 10–17 years. According to the WHO, the period of adolescence is between 10 and 19 years of age;26 participants will henceforth be referred to as younger adolescents (ages 10–13) and older adolescents (ages 14–17). Respondents were recruited through parents/guardians enrolled in the Nielsen Consumer Insights Global Panel and their partners’ panels. Email invitations with unique survey links were sent to adult panellists within each country. Those who confirmed they had a child aged 10–17 living in their household were asked for permission for their child to complete the survey (only one child per household was invited). Adolescents aged 10–17 years were eligible to participate, with quotas for age and sex groups in the UK and USA. After eligibility screening, all potential respondents were provided with information about the study and asked to provide assent. Surveys were conducted in English in Australia and the UK; Spanish in Chile and Mexico; English or French in Canada and English or Spanish in the USA. Members of the research team who were native in each language reviewed the French and Spanish translations independently. The median survey time was 24 minutes (min).
The child’s parent/guardian received remuneration in accordance with their panel’s usual incentive structure (eg, points based or monetary rewards, chances to win prizes). A full description of the study methods is found in the IFPS: Technical Report—2019 Youth Survey at http://foodpolicystudy.com/methods/.27
Total screen time and screen time by media channel and activity
Self-reported daily screen time was measured using the question: On a normal weekday, how much time do you spend…? Participants were asked to answer this question for five different media channels and/or activities: YouTube, social media (including messaging, posting or liking posts); TV (shows, series or movies); playing games (on smartphones, computers or game consoles) and browsing (reading websites, Googling, etc). Responses for amount of screen time for each media channel were captured using a scale (none; up to 15 min; up to 30 min; up to 1 hour; up to 2 hours; up to 3 hours; up to 4 hours; more than 4 hours; do not know; refuse to answer). The same question was presented afterwards for a ‘normal weekend day’. Although the phrasing ‘up to’ means that participants could have watched less than the stated value, the ceiling value was used to calculate an estimated amount of time in minutes spent on each media channel and all channels combined. For example, up to 15 min was recoded as 15 min, and up to 1 hour was recoded as 60 min. Those who responded ‘more than 4 hours’ were recoded as 300 min (ie, 5 hours). As adolescents could have been viewing multiple media channels simultaneously, the sum of exposure (ie, total minutes across all media types) was used as an overall indicator of total amount of exposure to screen-based media. Winsorisation was used to limit the effect of extreme values on total screen time. The maximum amount of total screen time was set at the mean+2 SD, in this case, 1195 min for a weekday and 1268 min for a weekend day. Participants (n=572, weekday (6.2%) and n=432, weekend day (4.7%)) who exceeded this value had their total screen time decreased to the maximum. The winsorisation technique yielded a slightly higher cut-off (+73 min) for weekends, as might be expected. The maximum amount obtained using this method was compared with a hypothetical estimation based on an assumption that on a weekday, children and adolescents spend roughly 7 hours at school and 8 hours sleeping, which sums up to 15 hours. It is plausible that there may have been some screen time during school hours that would fall within the aforementioned categories (browsing or watching YouTube), and so it was assumed that this was approximately 1 hour. The total (14 hours) was subtracted from the length of a day (24 hours) to give a possible maximum of 10 hours of screen time, with a maximum of 20 hours if two screens were being used simultaneously. This estimation of 20 hours (1200 min) confirms the measure of total maximal screen time for weekdays (1195 min) and weekends (1268 min) has good face validity.
Usage of social media platforms
Self-reported usage of various social media platforms was assessed using the measure: Do you use…? (select all that apply) (Response options: ‘Facebook’, ‘Instagram’, ‘TikTok’, ‘Twitter’, ‘Snapchat’, ‘none of the above’, ‘do not know’ or ‘refuse to answer’).
Self-reported location of exposure to unhealthy food and beverage advertisements
Self-reported location of exposure to advertisements was assessed using the question: Have you seen or heard advertisements for ‘unhealthy’ foods or drinks in any of these places in the last 30 days? Participants were instructed: Unhealthy food and drinks include processed foods high in sugar, salt, or saturated fat, such as soda/pop, fast food, chips, sugary cereals, cookies and chocolate bars. Participants could select all the responses that applied from a list of 13 potential media channels, and an ‘other’ option with an open-text box or ‘I haven’t seen any ads for unhealthy food in the last 30 days’, ‘do not know’ or ‘refuse to answer’. In this study, three channels were analysed that pertain to screen-based media (television shows, series or movies; website or social media and video or computer games). Open text data were reviewed, and responses were recoded to be included as one of the categorical options as applicable. ‘YouTube’ and ‘social media’ were recoded to be included in the category ‘website or social media’ and ‘TV’ was recoded in the category of television shows. When participants wrote ‘all’ in the open text, these responses were coded in each category of advertisement location.
Self-reported frequency of exposure to unhealthy food and beverage advertisements
Self-reported frequency of exposure to unhealthy food and beverage advertisements was assessed using the question: In the last 30 days, how often did you see or hear advertisements for these kinds of food or drinks? Participants responded for advertisements for six food categories, two of which were included in this analysis (sugary drinks; fast food from a restaurant). The frequency was assessed using a likert-type scale. (Response options: ‘never’, ‘less than once a week’, ‘once a week’, ‘a few times a week’, ‘everyday’, ‘more than once a day’, ‘don’t know’ and ‘refuse to answer’). Frequency of exposure was then recoded as a binary variable, where ‘everyday’ and ‘more than once a day’ were combined as ‘daily’, and the other options combined as ‘less than once a day’; responses of ‘do not know’ or ‘refuse to answer’ were considered as missing.
Sociodemographic measures
Sociodemographic data included age, ethnicity, sex, country, school grades and perceived income adequacy. Age was included as a binary variable (younger adolescents aged 10–13 years and older adolescents aged 14–17 years). Ethnicity was assessed using unique measures from each country and recoded to derive comparable measures across countries: majority or minority ethnicity. Participant’s sex was self-reported by asking Are you… with responses ‘male’ or ‘female’. School grades were measured using the question: What grades do you usually get in school? Response options varied across countries and were recoded to derive comparable measures across countries and three groups were created: ‘low’ (< grade of B in most countries), ‘mid’ (grade of B in most countries) or ‘high’ grades (grade of A in most countries). Perceived income adequacy was examined using the measure: Does your family have enough money to pay for things your family needs? (response options: ‘not enough money’, ‘barely enough money’, ‘enough money’, ‘more than enough money’, ‘do not know’ and ‘refuse to answer’). Perceived income adequacy was recoded as a binary variable (not enough money/barely enough money were combined as ‘inadequate’ and enough money/more than enough money were combined as ‘adequate’); responses of ‘do not know’ or ‘refuse’ were considered as missing and excluded from analyses. Participant’s body mass index (BMI) was calculated using self-reported height and weight. BMI was assessed using z-scores and classified according to the WHO recommendations.28 Severe thinness, thinness and normal weight were combined considering low levels of respondents for the severe thinness and thinness category (all countries=2.9%, Australia=3.3%, Canada=4.2%, Chile=0.9%, Mexico=1.7%, UK=2.8%, US=3.0%). Extreme values were recoded as missing (z-score < −5 or >5) according to the WHO growth reference guidelines.29 Extreme values as well as those participants whose height and/or weight were missing were coded as ‘not reported’ and included in the analytic sample to reduce bias as potentially important differences between those who do not report their height and weight in population-level surveys have been identified.30 A full list of measures in each country is available at http://foodpolicystudy.com/methods/ in the surveys section.31 The questionnaire has not been validated, but cognitive testing among a subsample of English-speaking adolescents for various questions including screen time and exposure to advertisements has been conducted to verify their understanding. When necessary, questions were adapted to improve comprehension (unpublished data).
Data analysis
A total of 11 491 adolescents completed the survey. Respondents were excluded for the following reasons: region was missing, ineligible or had an inadequate sample size (ie, Canadian territories); invalid response to a data quality question and/or survey completion time under 10 min (n=383). The analytic sample included 11 108 respondents (Australia: n=1435; Canada: n=3682; Chile: n=1252; Mexico: n=1616; UK: n=1520; USA: n=1603). A subsample (n=9171) was included in the current analysis after excluding respondents with missing data (including do not know and refuse to answer) for social media usage, screen time, location and frequency of exposure to unhealthy food and beverage advertisements, ethnicity, school grades and perceived income adequacy (online supplemental figure S1). Data were weighted with poststratification sample weights constructed using a raking algorithm with population estimates from the census in each country based on age group, sex, region and ethnicity (except in Canada). Reported estimates are weighted.
bmjopen-2021-058913supp001.pdf (613.5KB, pdf)
Descriptive statistics were tabulated including the self-reported mean number of hours viewing screen-based media across all channels and by channel on a weekday and weekend day, the self-reported usage of each social media platform and mean number of social media platforms (maximum of five platforms), the self-reported frequency of the three advertisement locations and the percentage of respondents reporting being exposed daily to advertisements for sugary drinks and fast food by country.
Regression models examined differences in the amount of self-reported exposure to screen-based media between countries and population subgroups. First, linear regressions were conducted with the amount of self-reported exposure to screen-based media (total screen time in minutes) as the dependent variable, including an indicator variable for country and age category (10–13 years, 14–17 years), adjusting for sex, ethnicity, perceived income adequacy, school grades and BMI. Next, separate logistic regression models were conducted for each social media type (1=yes, 0=no), including an indicator variable for country and age category and adjusting for the same variables listed above. Finally, separate logistic regression analyses were used to examine associations between the self-reported exposure to screen-based media and self-reported daily exposure to advertisements for each of the food categories (sugary drinks; fast food from a restaurant), with self-reported daily exposure to sugary drink or fast food marketing as the dependent variable, including indicator variables for the amount of exposure on a weekday (continuous) and country, adjusting for the same demographic correlates. Separate models were tested for self-reported exposure to screen-based media on weekends. For all regressions, survey-aware procedures were used to account for finite sampling methods, and 99% CIs are presented due to the use of multiple comparisons. Analyses were conducted using SAS Studio V.3.8.
Patient and public involvement
Patients and the public were not involved in the design, conduct, analysis or interpretation of the study. Study participants could have access to the study results on request.
Results
Weighted sample characteristics are presented in table 1. There were differences between countries in ethnicity group, school grades, perceived income adequacy and BMI. In general, a greater percentage of participants identified as a minority group in the USA, a smaller percentage had high school grades in Australia and the UK and a greater percentage perceived their family income as adequate in Canada.
Table 1.
Sample characteristics of adolescents in six countries (weighted) n=9171
| Characteristic | All countries (n=9171) | Australia (n=1127) | Canada (n=2869) | Chile (n=1124) | Mexico (n=1505) | UK (n=1140) |
USA (n=1406) |
| % (n) | |||||||
| Age (years) | |||||||
| 10–13 | 50 (4551) | 51 (574) | 50 (1438) | 47 (534) | 50 (750) | 49 (562) | 49 (693) |
| 14–17 | 50 (4620) | 49 (553) | 50 (1431) | 53 (590) | 50 (755) | 51 (578) | 51 (713) |
| Sex | |||||||
| Male | 51 (4664) | 52 (582) | 50 (1446) | 51 (572) | 51 (761) | 51 (581) | 51 (722) |
| Female | 49 (4507) | 48 (545) | 50 (1423) | 49 (552) | 49 (744) | 49 (559) | 49 (684) |
| Ethnicity | |||||||
| Majority group | 76 (6976) | 75 (850) | 73 (2098) | 85 (958) | 78 (1170) | 83 (941) | 68 (959) |
| Minority group | 24 (2195) | 25 (277) | 27 (771) | 15 (166) | 22 (335) | 17 (199) | 32 (447) |
| School grades | |||||||
| Low | 16 (1461) | 32 (365) | 13 (373) | 6 (65) | 7 (101) | 29 (334) | 16 (223) |
| Mid | 38 (3508) | 38 (430) | 34 (974) | 49 (555) | 36 (549) | 38 (430) | 41 (570) |
| High | 46 (4202) | 29 (332) | 53 (1522) | 45 (505) | 57 (855) | 33 (375) | 44 (613) |
| Perceived income adequacy | |||||||
| Inadequate | 24 (2222) | 25 (283) | 17 (488) | 31 (345) | 28 (418) | 26 (291) | 28 (397) |
| Adequate | 76 (6949) | 75 (844) | 83 (2381) | 69 (779) | 72 (1087) | 74 (849) | 72 (1009) |
| Self-reported BMI | |||||||
| Severe thinness/thinness/normal weight | 49 (4480) | 45 (509) | 57 (1630) | 43 (478) | 48 (717) | 41 (462) | 49 (683) |
| Overweight | 18 (1665) | 16 (176) | 16 (473) | 21 (231) | 22 (334) | 13 (147) | 22 (304) |
| Obesity | 10 (927) | 10 (113) | 9 (255) | 9 (97) | 10 (148) | 8 (92) | 16 (222) |
| Not reported | 23 (2100) | 29 (328) | 18 (511) | 28 (319) | 20 (306) | 39 (439) | 14 (197) |
BMI, body mass index.
Self-reported exposure to screen-based media
Figure 1 shows the mean amount of total self-reported screen time for a weekday among participants across countries, which ranged from 7.6 hours (Canada and Australia) to 10.2 hours (Chile). Similar findings were observed across countries for a weekend day, but with higher total amounts (online supplemental figure S2). Time spent on various media channels is shown in online supplemental figure S3. Digital media, comprised of YouTube, social media and browsing, reading websites and Googling, was the largest contributor overall. Across all countries, participants in Chile spent the highest amount of time on YouTube, social media, playing games and browsing, while participants in the USA spent the most time watching television on a weekday.
Figure 1.

Mean hours of total self-reported screen time (including YouTube, social media, television, playing games and browsing) on a weekday among adolescents in six countries after winsorisation (n=9171). AUS, Australia; CAN, Canada; MEX, Mexico; UK, United Kingdom; USA, United States of America.
Estimates from a linear regression model examining the total amount of self-reported exposure to screen-based media on a weekday across countries are shown in table 2. Total screen time differed by country, and across all demographic correlates. Participants in Canada and Australia reported less screen time than those in Chile, Mexico and USA; and Chilean participants reported more screen time than those in all other countries except Mexico. Older adolescents spent more time on screens than younger adolescents. The same pattern of results was observed for a weekend day (online supplemental table S1).
Table 2.
Estimates from a linear regression model examining the amount of self-reported exposure to screen-based media (in minutes) on a weekday among adolescents in six countries (n=9171)
| Parameter | Weekday screen time | |
| Wald χ2 | B (CI) | |
| Country | 64.2* | |
| AUS vs CAN | −18.1 (−47.2 to 11.0) | |
| AUS vs CHILE | −170.2 (−205.8 to −134.5) | |
| AUS vs MEX | −144.3 (−179.3 to −109.3) | |
| AUS vs UK | −26.8 (−60.7 to 7.2) | |
| AUS vs USA | −107.8 (−142.6, to −72.9) | |
| CAN vs CHILE | −152.1 (−181.9 to −122.3) | |
| CAN vs MEX | −126.2 (−154.9 to −97.5) | |
| CAN vs UK | −8.7 (−37.7 to 20.3) | |
| CAN vs USA | −89.7 (−118.2 to −61.1) | |
| CHILE vs MEX | 25.8 (−9.1 to 60.8) | |
| CHILE vs UK | 143.4 (107.9 to178.9) | |
| CHILE vs USA | 62.4 (26.7 to 98.0) | |
| MEX vs UK | 117.6 (82.7 to 152.4) | |
| MEX vs USA | 36.5 (1.9 to 71.2) | |
| UK vs USA | −81.0 (−116.1 to −45.9) | |
| Sex | 25.3* | |
| Female vs male | −34.7 (−52.4 to −16.9) | |
| Age | 209.4* | |
| 10–13 years vs 14–17 years | −99.7 (−117.4 to −81.9) | |
| Ethnicity | 18.5* | |
| Majority vs minority | −38.9 (−62.2 to −15.6) | |
| Perceived income adequacy | 16.0* | |
| Adequate vs inadequate | −33.0 (−54.3 to −11.8) | |
| School grades | 19.9* | |
| High vs low | −64.0 (−90.7 to −37.2) | |
| High vs mid | −26.6 (−46.2 to −7.0) | |
| Low vs mid | 37.4 (10.6 to 64.1) | |
| BMI | 16.9* | |
| Not reported vs obesity | −67.5 (−102.2 to −32.8) | |
| Not reported vs overweight | −28.8 (−57.2 to −0.3) | |
| Not reported vs severe thinness/thinness/normal weight | 12.4 (−10.3 to 35.1) | |
| Obesity vs overweight | 38.7 (2.5 to 74.9) | |
| Obesity vs severe thinness/thinness/normal weight | 79.9 (47.8 to 112.0) | |
| Overweight vs severe thinness/thinness/normal weight | 41.2 (16.4 to 65.9) | |
The variable listed second is the reference variable.
*Indicates significant Wald χ2 test (p<0.01).
AUS, Australia; B, Beta; BMI, body mass index; CAN, Canada; CI, 99% confidence interval; MEX, Mexico; UK, United Kingdom; USA, United States of America.
Self-reported social media exposure
The percentage of participants self-reporting using different social media platforms across countries is shown in figure 2. Overall, 77%–87% of adolescents were using at least one of the social media platforms, which varied by country. On average, the most commonly used platform was Instagram (range: from 52% in Australia and the USA to 68% in Chile), followed by Facebook (range: from 42% in Canada to 79% in Mexico) and Snapchat (range: from 28% in Chile to 52% in the UK). Participants who reported no social media application use ranged from 13% (Mexico) to 23% (Australia). After stratifying self-reported social media usage by age category (online supplemental figure S4), usage was still common among younger adolescents (10–13 years), and TikTok usage was more frequent among 10–13 than 14–17-year-old adolescents in all countries. The mean number of social media platforms used per respondent across countries is shown in online supplemental figure S5 and ranged from 1.9 platforms (Australia and Chile) to 2.2 platforms (Mexico).
Figure 2.

Percentage of adolescents in six countries self-reporting using platforms of social media (Facebook; Instagram; TikTok; Twitter; Snapchat; None) (n=9171). AUS, Australia; CAN, Canada; MEX, Mexico; UK, United Kingdom; USA, United States of America.
Estimates from separate logistic regression models examining self-reported exposure to social media platforms across countries are shown in table 3 and differed by country and age group for all platforms. Specifically, participants in Canada were less likely to use Facebook than those in all other countries, whereas participants in Mexico were more likely to use Facebook than those in all other countries. Those in Chile were more likely to use Instagram than those in all other countries. Participants from Canada were more likely to use TikTok than participants in Australia, Chile, Mexico and the UK. Participants in Mexico were more likely to use Twitter than participants in all other countries and those in the UK were more likely to use Snapchat than those in all other countries except the USA. Participants in Australia were more likely to not use a social media platform compared with all other countries except the USA. Older adolescents (ages 14–17) were more likely to use all social media platforms except TikTok compared with younger adolescents (ages 10–13).
Table 3.
Estimates from separate logistic regression models examining self-reported exposure to social media platforms among adolescents in six countries (n=9171)
| Parameter | Exposure to Facebook | Exposure to Instagram | Exposure to TikTok | Exposure to Twitter | Exposure to Snapchat | No exposure to social media | ||||||
| Wald χ2 | Odds ratio (CI) | Wald χ2 | Odds ratio (CI) | Wald χ2 | Odds ratio (CI) | Wald χ2 | Odds ratio (CI) | Wald χ2 | Odds ratio (CI) | Wald χ2 | Odds ratio (CI) | |
| Country | 81.7* | 17.6* | 15.2* | 28.4* | 43.3* | 10.0* | ||||||
| AUS vs CAN | 1.28 (1.04 to 1.56) | 0.90 (0.73 to 1.11) | 0.80 (0.64 to 1.00) | 0.92 (0.70 to 1.20) | 0.77 (0.63 to 0.95) | 1.29 (1.01 to 1.66) | ||||||
| AUS vs CHILE | 0.81 (0.63 to 1.04) | 0.48 (0.37 to 0.62) | 1.41 (1.07 to 1.86) | 0.72 (0.52 to 0.99) | 1.96 (1.50 to 2.56) | 1.72 (1.25 to 2.36) | ||||||
| AUS vs MEX | 0.23 (0.18 to 0.30) | 0.95 (0.74 to 1.21) | 1.54 (1.15 to 2.04) | 0.37 (0.28 to 0.50) | 1.57 (1.22 to 2.03) | 2.18 (1.57 to 3.03) | ||||||
| AUS vs UK | 0.89 (0.70 to 1.14) | 0.82 (0.64 to 1.05) | 1.05 (0.80 to 1.36) | 0.54 (0.40 to 0.73) | 0.62 (0.48 to 0.79) | 1.59 (1.16 to 2.18) | ||||||
| AUS vs USA | 0.84 (0.66 to 1.06) | 1.06 (0.83 to 1.35) | 0.85 (0.66 to 1.09) | 0.60 (0.44 to 0.81) | 0.73 (0.57 to 0.92) | 1.19 (0.89 to 1.60) | ||||||
| CAN vs CHILE | 0.64 (0.51 to 0.79) | 0.53 (0.43 to 0.66) | 1.76 (1.40 to 2.22) | 0.78 (0.61 to 1.01) | 2.53 (2.02 to 3.18) | 1.33 (1.01 to 1.75) | ||||||
| CAN vs MEX | 0.18 (0.14 to 0.22) | 1.05 (0.86 to 1.28) | 1.92 (1.51 to 2.44) | 0.41 (0.33 to 0.51) | 2.03 (1.64 to 2.50) | 1.69 (1.27 to 2.25) | ||||||
| CAN vs UK | 0.70 (0.56 to 0.87) | 0.91 (0.73 to 1.12) | 1.31 (1.04 to 1.64) | 0.59 (0.46 to 0.76) | 0.80 (0.65 to 0.98) | 1.23 (0.93 to 1.63) | ||||||
| CAN vs USA | 0.66 (0.54 to 0.80) | 1.17 (0.96 to 1.42) | 1.06 (0.87 to 1.30) | 0.65 (0.52 to 0.82) | 0.94 (0.78 to 1.13) | 0.92 (0.72 to 1.18) | ||||||
| CHILE vs MEX | 0.28 (0.22 to 0.37) | 1.96 (1.54 to 2.51) | 1.09 (0.82 to 1.46) | 0.52 (0.40 to 0.68) | 0.80 (0.61 to 1.05) | 1.27 (0.91 to 1.78) | ||||||
| CHILE vs UK | 1.10 (0.85 to 1.42) | 1.70 (1.32 to 2.19) | 0.74 (0.56 to 0.98) | 0.75 (0.56 to 1.01) | 0.31 (0.24 to 0.41) | 0.92 (0.66 to 1.30) | ||||||
| CHILE vs USA | 1.04 (0.81 to 1.32) | 2.19 (1.71 to 2.80) | 0.60 (0.46 to 0.79) | 0.83 (0.63 to 1.10) | 0.37 (0.29 to 0.48) | 0.69 (0.51 to 0.95) | ||||||
| MEX vs UK | 3.91 (2.99 to 5.10) | 0.86 (0.67 to 1.11) | 0.68 (0.51 to 0.91) | 1.46 (1.11 to 1.90) | 0.39 (0.30 to 0.51) | 0.73 (0.51 to 1.03) | ||||||
| MEX vs USA | 3.68 (2.86 to 4.73) | 1.11 (0.88 to 1.42) | 0.55 (0.42 to 0.73) | 1.61 (1.25 to 2.07) | 0.46 (0.36 to 0.59) | 0.55 (0.40 to 0.75) | ||||||
| UK vs USA | 0.94 (0.74 to 1.20) | 1.29 (1.01 to 1.66) | 0.81 (0.63 to 1.05) | 1.11 (0.83 to 1.46) | 1.18 (0.93 to 1.50) | 0.75 (0.54 to 1.04) | ||||||
| Sex | 0.6 | 69.7* | 250.4* | 1.9 | 163.6* | 85.3* | ||||||
| Female vs male | 1.04 (0.92 to 1.18) | 1.50 (1.33 to 1.71) | 2.31 (2.02 to 2.65) | 0.92 (0.80 to 1.07) | 1.87 (1.65 to 2.12) | 0.55 (0.47 to 0.65) | ||||||
| Age | 601.2* | 705.2* | 30.1* | 380.7* | 406.4* | 588.0* | ||||||
| 10–13 years vs 14–17 years | 0.30 (0.26 to 0.34) | 0.27 (0.24 to 0.30) | 1.34 (1.17 to 1.54) | 0.31 (0.27 to 0.36) | 0.37 (0.32 to 0.42) | 6.24 (5.14 to 7.58) | ||||||
| Ethnicity | 0.4 | 1.5 | 0.0 | 2.3 | 0.2 | 1.1 | ||||||
| Majority vs minority | 0.96 (0.82 to 1.13) | 0.93 (0.79 to 1.09) | 1.01 (0.85 to 1.20) | 0.90 (0.74 to 1.08) | 0.97 (0.83 to 1.14) | 1.09 (0.88 to 1.34) | ||||||
| Perceived income adequacy | 6.1 | 2.6 | 1.3 | 7.6* | 0.4 | 0.1 | ||||||
| Adequate vs inadequate | 0.87 (0.75 to 1.01) | 1.10 (0.95 to 1.27) | 0.93 (0.80 to 1.09) | 1.20 (1.01 to 1.43) | 0.96 (0.83 to 1.12) | 1.02 (0.84 to 1.23) | ||||||
| School grades | 11.1* | 2.3 | 10.2* | 2.1 | 7.3* | 12.3* | ||||||
| High vs low | 0.80 (0.66 to 0.97) | 0.98 (0.81 to 1.18) | 0.73 (0.60 to 0.89) | 1.20 (0.95 to 1.51) | 0.83 (0.69 to 1.00) | 1.42 (1.11 to 1.82) | ||||||
| High vs mid | 0.78 (0.68 to 0.90) | 0.89 (0.78 to 1.03) | 0.82 (0.71 to 0.96) | 1.03 (0.88 to 1.21) | 0.82 (0.72 to 0.95) | 1.35 (1.13 to 1.61) | ||||||
| Low vs mid | 0.98 (0.81 to 1.18) | 0.92 (0.76 to 1.11) | 1.13 (0.93 to 1.38) | 0.86 (0.68 to 1.08) | 0.99 (0.82 to 1.19) | 0.95 (0.74 to 1.22) | ||||||
| BMI | 12.1* | 7.8* | 3.0 | 4.1* | 10.8* | 12.8* | ||||||
| Not reported vs obesity | 0.64 (0.50 to 0.81) | 0.74 (0.58 to 0.94) | 0.78 (0.61 to 1.00) | 0.77 (0.58 to 1.02) | 0.71 (0.56 to 0.90) | 1.86 (1.38 to 2.52) | ||||||
| Not reported vs overweight | 0.72 (0.59 to 0.89) | 0.74 (0.61 to 0.90) | 0.85 (0.69 to 1.05) | 0.78 (0.61 to 0.98) | 0.69 (0.56 to 0.84) | 1.59 (1.24 to 2.04) | ||||||
| Not reported vs severe thinness/thinness/normal weight | 0.93 (0.79 to 1.10) | 0.76 (0.65 to 0.90) | 0.95 (0.80 to 1.13) | 0.94 (0.77 to 1.15) | 0.72 (0.61 to 0.85) | 1.32 (1.09 to 1.62) | ||||||
| Obesity vs overweight | 1.13 (0.88 to 1.45) | 1.00 (0.78 to 1.28) | 1.09 (0.84 to 1.41) | 1.02 (0.77 to 1.35) | 0.97 (0.76 to 1.24) | 0.85 (0.62 to 1.18) | ||||||
| Obesity vs severe thinness/thinness/normal weight | 1.46 (1.17 to 1.82) | 1.03 (0.83 to 1.29) | 1.22 (0.97 to 1.53) | 1.23 (0.96 to 1.59) | 1.02 (0.82 to 1.26) | 0.71 (0.53 to 0.95) | ||||||
| Overweight vs severe thinness/thinness/normal weight | 1.28 (1.08 to 1.53) | 1.03 (0.87 to 1.23) | 1.12 (0.93 to 1.34) | 1.21 (1.00 to 1.48) | 1.05 (0.88 to 1.24) | 0.83 (0.66 to 1.05) | ||||||
The variable listed second is the reference variable.
*Indicates significant Wald χ2 test (p<0.01).
AUS, Australia; BMI, body mass index; CAN, Canada; CI, 99% confidence interval; MEX, Mexico; UK, United Kingdom; USA, United States of America.
Location of self-reported screen-based exposure to advertisements for unhealthy foods or drinks
The percentage of adolescents who reported that they were exposed to advertisements for unhealthy foods or drinks in three locations in the previous 30 days is shown in figure 3. Overall, TV shows, series or movies accounted for the largest number of participants self-reporting exposure to advertisements (range: from 43% in the UK to 69% in Mexico and Chile), followed by websites or social media (range: from 27% in the UK to 60% in Chile) and video or computer games (range: from 10% in Australia and the UK to 17% in Chile).
Figure 3.

Percentage of adolescents in six countries self-reporting exposure to advertisements for unhealthy foods or drinks in three locations (TV shows, series or movies; website or social media; video or computer games; none) in the last 30 days (n=9171). AUS, Australia; CAN, Canada; MEX, Mexico; UK, United Kingdom; USA, United States of America.
Self-reported daily exposure to sugary beverage and fast food advertisements
The percentage of respondents who reported that they were exposed daily to advertisements for both food categories in the last 30 days is shown in figure 4. Self-reported daily exposure to sugary drinks advertisements ranged from 10% (UK) to 43% (Mexico). Self-reported daily exposure to fast food advertisements was relatively more consistent across countries, with the exception of the UK (range: from 19% in the UK to 44% in the USA).
Figure 4.
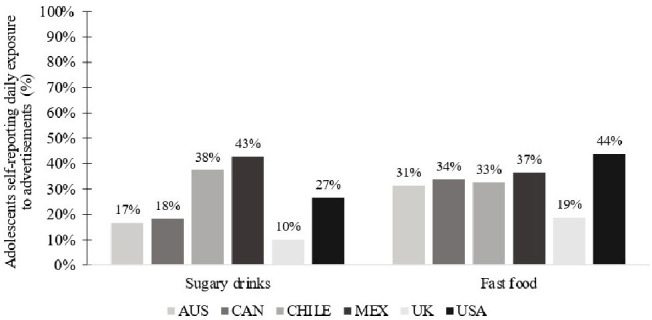
Percentage of adolescents in six countries self-reporting daily exposure to advertisements for sugary drinks and fast food in the last 30 days (n=9171). AUS, Australia; CAN, Canada; MEX, Mexico; UK, United Kingdom, USA, United States of America.
Estimates from separate logistic regression models examining self-reported daily exposure to sugary beverage and fast food advertisements across countries are shown in table 4. Participants who self-reported more time spent on screen-based media were more likely to report daily exposure to advertisements for both food categories. Self-reported daily exposure to advertisements for sugary drinks and fast food differed by country and amount of self-reported exposure to screen-based media (total screen time in minutes), and patterns were mostly similar across both food categories; there was no significant difference in self-reported exposure between age groups. Overall, participants in Mexico and Chile were much more likely to report daily exposure to sugary beverage advertisements than participants in all other countries, with fewer differences for fast food advertisements. Participants in the UK were less likely to report daily exposure to advertisements of sugary drinks and fast food compared with all other countries and those in the USA were more likely to report daily exposure to fast food advertisements than those in all other countries. The same pattern of results was observed for exposure to screen-based media on a weekend day (online supplemental table S2).
Table 4.
Estimates from separate logistic regression models examining daily self-reported exposure to sugary beverage and fast food advertisements among adolescents in six countries on a weekday (n=9171)
| Parameter | Daily exposure to sugary drinks ads | Daily exposure to fast food ads | ||
| Wald χ2 | Odds ratio (CI) | Wald χ2 | Odds ratio (CI) | |
| Country | 70.4* | 24.3* | ||
| AUS vs CAN | 0.89 (0.69 to 1.15) | 0.89 (0.72 to 1.10) | ||
| AUS vs CHILE | 0.37 (0.28 to 0.49) | 1.11 (0.86 to 1.43) | ||
| AUS vs MEX | 0.29 (0.22 to 0.38) | 0.90 (0.70 to 1.15) | ||
| AUS vs UK | 1.77 (1.26 to 2.50) | 2.00 (1.52 to 2.62) | ||
| AUS vs USA | 0.62 (0.47 to 0.81) | 0.67 (0.52 to 0.84) | ||
| CAN vs CHILE | 0.41 (0.33 to 0.52) | 1.24 (1.00 to 1.54) | ||
| CAN vs MEX | 0.33 (0.27 to 0.41) | 1.00 (0.82 to 1.23) | ||
| CAN vs UK | 1.99 (1.47 to 2.70) | 2.24 (1.76 to 2.84) | ||
| CAN vs USA | 0.69 (0.56 to 0.86) | 0.75 (0.62 to 0.90) | ||
| CHILE vs MEX | 0.79 (0.62 to 1.00) | 0.81 (0.63 to 1.03) | ||
| CHILE vs UK | 4.80 (3.46 to 6.67) | 1.80 (1.36 to 2.39) | ||
| CHILE vs USA | 1.67 (1.30 to 2.14) | 0.60 (0.47 to 0.76) | ||
| MEX vs UK | 6.07 (4.39 to 8.39) | 2.23 (1.69 to 2.94) | ||
| MEX vs USA | 2.11 (1.66 to 2.68) | 0.74 (0.59 to 0.94) | ||
| UK vs USA | 0.35 (0.25 to 0.48) | 0.33 (0.26 to 0.43) | ||
| Sex | 1.5 | 0.4 | ||
| Female vs male | 1.07 (0.93 to 1.23) | 1.03 (0.91 to 1.17) | ||
| Age | 0.0 | 1.2 | ||
| 10–13 years vs 14–17 years | 1.00 (0.86 to 1.16) | 0.95 (0.83 to 1.08) | ||
| Ethnicity | 0.1 | 0.0 | ||
| Majority vs minority | 1.02 (0.85 to 1.23) | 1.00 (0.85 to 1.18) | ||
| Perceived income adequacy | 1.0 | 4.5 | ||
| Adequate vs inadequate | 0.94 (0.80 to 1.11) | 0.88 (0.76 to 1.03) | ||
| School grades | 0.4 | 3.2 | ||
| High vs low | 0.93 (0.75 to 1.17) | 0.95 (0.79 to 1.15) | ||
| High vs mid | 0.96 (0.82 to 1.13) | 0.87 (0.76 to 1.00) | ||
| Low vs mid | 1.03 (0.83 to 1.29) | 0.92 (0.76 to 1.11) | ||
| BMI | 6.3* | 6.4* | ||
| Not reported vs obesity | 0.73 (0.56 to 0.95) | 0.75 (0.59 to 0.94) | ||
| Not reported vs overweight | 0.70 (0.56 to 0.88) | 0.75 (0.61 to 0.92) | ||
| Not reported vs severe thinness/thinness/normal weight | 0.79 (0.66 to 0.96) | 0.78 (0.66 to 0.93) | ||
| Obesity vs overweight | 0.96 (0.74 to 1.25) | 1.01 (0.79 to 1.28) | ||
| Obesity vs severe thinness/thinness/normal weight | 1.09 (0.86 to 1.38) | 1.05 (0.85 to 1.30) | ||
| Overweight vs severe thinness/thinness/normal weight | 1.14 (0.94 to 1.38) | 1.04 (0.88 to 1.24) | ||
| Exposure to screen based media (weekday) | 88.2* | 1.05 (1.04 to 1.07) | 121.4* | 1.05 (1.04 to 1.07) |
The variable listed second is the reference variable. Exposure to screen-based media is expressed in minutes.
*Indicates significant Wald χ2 test (p<0.01).
AUS, Australia; BMI, body mass index; CAN, Canada; MEX, Mexico; UK, United Kingdom; USA, United States of America.
Discussion
Summary of main findings
This study found that adolescents across Australia, Canada, Chile, Mexico, UK and USA are self-reporting considerable amounts of time viewing screen-based media, although these self-reported estimates include simultaneous viewing of multiple media. Digital media accounted for the most time on screens and social media use varied by platforms. Across all countries, self-reported exposure to advertisements in the past 30 days was most frequent on television, followed by digital media and gaming platforms. Between-country differences were identified: participants in the UK reported less daily exposure to fast food and sugary drink advertisements, whereas participants in the USA reported greater daily exposure to fast food advertisements. Most importantly, our results show that in all countries, self-reported exposure to advertisements increased with greater screen time. Analyses suggested important differences in self-reported exposure to screen-based media and social media platforms between age groups, with older adolescents generally reporting a greater exposure.
Relationships with existing knowledge
The estimates from this study are similar to other international estimates of self-reported screen time. In the USA, screen time among children 8–12 years in 2019 was estimated to be 4 hours 44 min, and 7 hours and 22 min among 13–18 year olds,32 compared with over 9 hours in the current study among the older age group. A large national Canadian study from 2013 to 2014 suggests that youth ages 13–18 spent on average between 7.6 hours and 8 hours in front of screens daily (depending on province and sex),33 very similar to the current findings of approximately 8.5 hours among older adolescents. However, the current estimates appear to be higher than several European estimates from various countries,34 which may be due to differences in the types of questions asked and the study context that may affect recall and self-report. Even with limitations on the precision of screentime estimates due to self-report, most participants in the current study exceeded screen time guidelines across countries, which recommend entertainment screen time be limited to less than 2 hours daily for school-aged children and adolescents.35–37 Screen time has previously been associated with youth obesity,38 39 poorer diet quality40 and consumption of less healthy foods and beverages.41 42 The general level of exposure reported among the sample, while an approximation, is cause for concern.
The large proportion of adolescents reporting using social media platforms has important implications for food and beverage marketing. Companies are increasingly developing strategies to engage with their audience through these media platforms, which have a high likelihood of reaching children and adolescents even when they are not the primary target audience. Research from Canada has estimated that children ages 7–11 years were exposed to food and beverage marketing (of which the great majority is ‘less healthy’) on social media apps 30 times per week while adolescents ages 12–16 years were exposed on average 189 times per week.23 In our study, adolescents reported using two social media platforms on average, therefore exposing them to various types and amounts of marketing strategies across platforms. For instance, Instagram—the most commonly reported social media platform among participants—is known to promote poor nutritional quality foods and are commonly promoted through popular brand accounts using a range of marketing strategies that appeal to a young audience, such as competitions and the use of characters.43 Unhealthy food brands on Facebook are known to use techniques such as competitions based on user-generated content, interactive games and apps.44
In this study, a greater proportion of adolescents reported exposure to advertisements for unhealthy foods or drinks on television compared with websites, social media applications or gaming sites. Greater reporting may be in part due to the different types of advertising between these channels. In order for children and adolescents to be aware of advertisements, they need not only to be able to identify the difference between an advertisement and other content but also to understand the persuasive intent behind the message.15 Self-reported exposure to advertisements on television may have been higher as it is more easily identifiable compared with digital marketing, which often uses subtle marketing techniques (eg, celebrity endorsements by influencers and native advertising designed to imitate editorial content) and is frequently disguised as entertainment.15 16 On digital media, adolescents may simply be less able to discriminate advertisements from other content, making marketing on these channels particularly alarming. Digital marketing via advertisements is typically targeted, using cookies and other means, which record personal preferences, online activity and location and these data are then used to personalise and target the content of marketing to individual users, therefore increasing the persuasive power of marketing.10 11 The subtle advertising techniques used on digital media, such as influencer endorsements or advergames, may be more likely to bypass children’s and younger adolescents’ cognitive awareness. Our data align with marketing expenditure data, an objective indicator of marketing efforts by companies: fast food advertisement expenditures are the highest for television, although digital marketing expenditures increased by 74% between 2012 and 2019.45 However, digital marketing expenditures are likely underestimated as not all industry spending can be captured and spending is not necessarily associated with the reach of the message on digital media.46 Therefore, both self-reported exposure data and the general digital marketing expenditure data likely underestimate the amount of digital marketing to which adolescents are currently exposed.
Self-reported daily exposure to advertisements was common for both fast food and sugary drinks, with 34% and 25% of the sample reporting daily exposure, respectively, in all countries. Perhaps unsurprisingly, those reporting more screen time were more likely to report daily exposure to sugary drinks and fast food advertisements. Differences across countries may in part relate to differences in restrictions on marketing directed at children. In the UK, where participants were less likely to self-report daily exposure to advertisements for fast food and sugary drinks than those in all other countries, a total ban of advertisements for unhealthy foods and beverages has been in place since 2007 during and adjacent to television programmes appealing to children and adolescents under the age of 16.47 The lower likelihood of self-reported exposure to advertisements aligns with what would be expected with the UK’s current policy in place, although evidence on the impact of the UK policy is mixed. Findings suggest that despite some changes in children’s exposure, advertisements typically shifted to other media channels, implying important loopholes in regulations.48 49 In the USA, where participants were more likely to report daily exposure to fast food advertisements than those in all other countries, voluntary self-regulatory approaches to restrict marketing by the industry are the only form of marketing restrictions, which target children under 12 years of age on media where the audience is mostly children50 and have largely proven ineffective at decreasing children’s exposure to marketing for unhealthy products.45 51 52 It is important to note that the present study cannot capture the effectiveness of restrictive marketing policies by its cross-sectional design, but studying trends in self-reported screen time, social media use and exposure to advertisements annually over time using the IFPS should help evaluate the impact of impending policies, such as the recently announced policy in the UK, which will ban online advertising by the end of 2022 and ban advertising of foods high in fat, sugar and salt between 5:30 am and 9:00 pm.53–55
Age group was an important predictor for reported screen-based media and social media exposure, with older adolescents reporting spending more time on screens and using social media platforms more than younger adolescents. Older adolescents may be an age group of particular interest to marketers because of their greater spending power compared with younger adolescents, which also increases with age, therefore having the potential to create life-long brand relationships and product consumers.56 57 Marketers target adolescents through digital media by using ‘ubiquitous connectivity, personalisation, peer-to-peer networking, engagement, immersion and content creation’, which are features especially appealing to this age group.57 In our study, there were no differences in self-reported daily exposure to sugary drink and fast food advertisements between age groups. Despite adolescents having an improved ability to recognise advertisement content and the persuasive intent of marketing compared with children, adolescents may be even more vulnerable to digital food marketing, because of their increased use of these platforms as well as desire to conform with social norms in their peer group.58 59 Greater exposure to digital and social media platforms may also increase the number of subtle marketing strategies, for example, viral marketing (peer-to-peer), contests, quizzes and marketing by influencers, which may not be captured in self-report measures if the participant is unable to identify these as marketing strategies.
Strengths and limitations
This study has a large sample size, and the same measures were used across countries, allowing justifiable comparisons between countries. Many studies use gross rating points or expenditure data as a proxy for exposure to advertising. While the latter provide objective data, they are unlikely to be accurate for digital advertising46 and do not indicate who is exposed at the individual level, including individual-level correlates. More intensive approaches—such as devices that directly monitor websites or device usage—provide precise measures of exposure to marketing but are typically less feasible at a population level. One of the major strengths of this study is the wide range of social media platforms and the differentiated locations of exposure to screen-based advertising assessed. Self-reported exposure to food marketing is a method used by researchers in large population samples58 60 61 as a subjective indicator of actual exposure, although actual exposure is likely to be higher because of the frequent and implicit nature of marketing, resulting in a probable underestimation of exposure to marketing. Our measures may further underestimate exposure as such a measure may be less reliable in a sample of adolescents due to risk of recall errors, and inability to recognise all forms of marketing (particularly in digital media).15
This study is subject to limitations common to survey research. Respondents were recruited using non-probability-based sampling; therefore, although the data were weighted by age group, sex, region and ethnicity (except in Canada), the findings do not provide nationally representative estimates. In addition, there were notably higher levels of missing data for BMI in the UK. The measures used also have some limitations. For example, time spent watching cable television versus on streaming applications (Netflix, Crave, Amazon Prime Video, etc) was not distinguished in this study. The amount of marketing exposure on cable television and free streaming websites compared with subscription platforms (that are typically ad-free) is likely very different, and this may play an important role in understanding the amount of exposure. Additionally, adolescents retrospectively self-reported the estimated screen time spent on each media channel rather than using a more objective approach, and this may have been influenced by whether or not a parent was present when completing the survey. This approach has not yet been validated in the literature but nevertheless seems comparable to self-report estimates from other surveys. Responses may not be precisely accurate and likely overestimate the absolute amount of screen time reported by youth as overall exposure was calculated by summing self-reported exposure to individual media channels and, thus, may include simultaneous use of multiple screens. Indicators of simultaneous viewing of screens were not directly measured in the survey. Nevertheless, this tool allows for comparisons of the relative amount of exposure across countries, as it is likely that the challenge of estimations, and associated error, would be similar across countries. Finally, the measures did not distinguish between recreational screen time and screen time that was spent for school purposes (eg, on websites).
Policy implications
These results reinforce the need to implement restrictive policies on marketing of unhealthy food and beverages appealing to a young audience, not only on television but also on digital media considering the widespread self-reported usage of social media platforms among adolescents across countries and the persuasiveness of marketing that is often targeted. Future research examining children’s and adolescents’ exposure to digital marketing, as well as research modelling of the impact of potential policy measures, are likely to be important in making the case for restricting less healthy food and beverage content via these channels.62 This study also demonstrated the variety of media channels that are being used by adolescents, even though their content may not be ‘child-targeted’63 (ie, social media, websites, etc) but are indeed ‘child appealing’.62 64 Almost all social media platforms (such as Instagram, Facebook and Snapchat) have a minimum age of 13 to register,65–67 but previous research has suggested that nearly a quarter of children aged 8–11 years have an account,68 demonstrating that self-imposed age restrictions are not effective. Our results were similar, with the younger adolescents (10–13 years) self-reporting widespread usage of social media platforms. The high rates of social media usage and self-reported exposure to advertisements via this medium further demonstrates the need for restrictions to limit exposure to this vulnerable age group.
The results of this study will be useful for future research as a baseline for comparison with exposure to less healthy food marketing after the implementation of marketing policies and also in comparing adolescents’ exposure to screen-based media and marketing after important worldwide events leading to possible changes in media consumption habits, such as changes in exposure as a result of the COVID-19 pandemic.69
Supplementary Material
Footnotes
Twitter: @LanaVanderlee
Contributors: LV, CMW and DH designed research; CMW and DH conducted research; ED-P analysed data and wrote the paper; LV had primary responsibility for final content and is the guarantor for this work; MW, MPK, DH, CN, CMW, XZ and LV reviewed and edited the manuscript. All authors read and approved the final manuscript.
Funding: This work was supported by the Public Health Agency of Canada (PHAC, no grant number available), with additional support from a Canadian Institutes of Health Research (CIHR) Project Grant (PJT-162167).
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available upon reasonable request. Data are available directly from the International Food Policy Study team on reasonable request (see www.foodpolicystudy.com).
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
The study was reviewed by and received ethics clearance through a University of Waterloo Research Ethics Committee (ORE number 41477) and Laval University Ethics Committee (number 2021-318). All participants provided informed consent to take part. Participants gave informed consent to participate in the study before taking part.
References
- 1.John DR. Consumer socialization of children: a retrospective look at Twenty‐Five years of research. J Consum Res 1999;26:183–213. 10.1086/209559 [DOI] [Google Scholar]
- 2.Guest L. Brand Loyalty revisited: a twenty-year report. Am J Appl Psychol. 1964;48:93–7. 10.1037/h0046667 [DOI] [Google Scholar]
- 3.Haryanto JO, Moutinho L, Coelho A. Is brand loyalty really present in the children’s market? A comparative study from Indonesia, Portugal, and Brazil. J Bus Res 2016;69:4020–32. 10.1016/j.jbusres.2016.06.013 [DOI] [Google Scholar]
- 4.World Health Organization . A framework for implementing the set of recommendations on the marketing of foods and non-alcoholic beverages to children 2012.
- 5.Taillie LS, Busey E, Stoltze FM, et al. Governmental policies to reduce unhealthy food marketing to children. Nutr Rev 2019;77:787–816. 10.1093/nutrit/nuz021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hastings G, McDermott L, Angus K. The Extent, Nature and Effects of Food Promotion to Children : A Review of the Evidence - Technical Paper Prepared for the World Health Organization, 2006. [Google Scholar]
- 7.Sadeghirad B, Duhaney T, Motaghipisheh S, et al. Influence of unhealthy food and beverage marketing on children's dietary intake and preference: a systematic review and meta-analysis of randomized trials. Obes Rev 2016;17:945–59. 10.1111/obr.12445 [DOI] [PubMed] [Google Scholar]
- 8.Smith R, Kelly B, Yeatman H, et al. Food Marketing Influences Children’s Attitudes, Preferences and Consumption: A Systematic Critical Review. Nutrients 2019;11:875. 10.3390/nu11040875 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wellard L, Chapman K, Wolfenden L, et al. Who is responsible for selecting children’s fast food meals, and what impact does this have on energy content of the selected meals? Nutrition & Dietetics 2014;71:172–7. 10.1111/1747-0080.12106 [DOI] [Google Scholar]
- 10.World Health Organization . Tackling food marketing to children in a digital world : trans-disciplinary perspectives, 2016. [Google Scholar]
- 11.Tan L, Ng SH, Omar A, et al. What's on YouTube? A case study on food and beverage advertising in Videos targeted at children on social media. Child Obes 2018;14:280–90. 10.1089/chi.2018.0037 [DOI] [PubMed] [Google Scholar]
- 12.Coates AE, Hardman CA, Halford JCG, et al. Social media Influencer marketing and children's food intake: a randomized trial. Pediatrics 2019;143. 10.1542/peds.2018-2554. [Epub ahead of print: 04 03 2019]. [DOI] [PubMed] [Google Scholar]
- 13.Smit CR, Buijs L, van Woudenberg TJ, et al. The impact of social media Influencers on children's dietary behaviors. Front Psychol 2019;10:2975. 10.3389/fpsyg.2019.02975 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Smith R, Kelly B, Yeatman H, et al. Advertising placement in digital game design influences children's choices of Advertised snacks: a randomized trial. J Acad Nutr Diet 2020;120:404–13. 10.1016/j.jand.2019.07.017 [DOI] [PubMed] [Google Scholar]
- 15.Blades M, Oates C, Li S. Children's recognition of advertisements on television and on web Pages. Appetite 2013;62:190–3. 10.1016/j.appet.2012.04.002 [DOI] [PubMed] [Google Scholar]
- 16.Owen L, Lewis C, Auty S, et al. Is Children’s Understanding of Nontraditional Advertising Comparable to Their Understanding of Television Advertising? J Public Policy Mark. 2013;32:195–206. 10.1509/jppm.09.003 [DOI] [Google Scholar]
- 17.Goerg GM, Best C, Shobowale S, et al. When to combine television with online campaigns. cost savings versus extended reach. J Advert Res 2017;57:283–304. 10.2501/jar-2017-037 [DOI] [Google Scholar]
- 18.Facebook for Business . Internet:. Available: https://www.facebook.com/business/news/Ad-Week-UK [Accessed October 3 2021].
- 19.Ofcom . Children and parents: media use and attitudes report, 2015
- 20.Ofcom . Children and parents : Media Use and Attitudes Report, 2021
- 21.Bragg MA, Pageot YK, Amico A, et al. Fast food, beverage, and snack brands on social media in the United States: an examination of marketing techniques utilized in 2000 brand posts. Pediatr Obes 2020;15:e12606. 10.1111/ijpo.12606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rummo PE, Cassidy O, Wells I, et al. Examining the relationship between Youth-Targeted food marketing expenditures and the demographics of social media followers. Int J Environ Res Public Health 2020;17. 10.3390/ijerph17051631. [Epub ahead of print: 03 03 2020]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Potvin Kent M, Pauzé E, Roy E-A, et al. Children and adolescents' exposure to food and beverage marketing in social media apps. Pediatr Obes 2019;14:e12508. 10.1111/ijpo.12508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kelly B, Bosward R, Freeman B. Australian children's exposure to, and engagement with, web-based marketing of food and drink brands: cross-sectional observational study. J Med Internet Res 2021;23:e28144. 10.2196/28144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nieto C, Valero I, Buenrostro N, et al. Children and adolescents’ exposure to digital food and beverage marketing in Mexico during COVID-19 times. Curr Dev Nutr 2021;5:562. 10.1093/cdn/nzab043_014 [DOI] [Google Scholar]
- 26.World Health Organization . Internet. Available: https://apps.who.int/adolescent/second-decade/section2/page1/recognizing-adolescence.html
- 27.Hammond D, White CM, Rynard VL, et al. International Food Policy Study: Technical Report - 2019 Youth Survey. University of Waterloo, 2021. [Google Scholar]
- 28.World Health Organization . BMI-for-age (5-19 years), 2021
- 29.World Health Organization . WHO AnthroPlus for Personal Computers Manual : Software for assessing growth of the world’s children and adolescents, 2009. [Google Scholar]
- 30.Read SH, Lewis SC, Halbesma N, et al. Measuring the association between body mass index and all-cause mortality in the presence of missing data: analyses from the Scottish national diabetes register. Am J Epidemiol 2017;185:641–9. 10.1093/aje/kww162 [DOI] [PubMed] [Google Scholar]
- 31.Hammond D. International Food Policy Study : 2019 Youth Survey - Canada. University of Waterloo, 2021. [Google Scholar]
- 32.Rideout V, Robb MB. The common sense census: Media use by tweens and teens, 2019. In: Media CS, ed, 2019.
- 33.Katapally TR, Laxer RE, Qian W, et al. Do school physical activity policies and programs have a role in decreasing multiple screen time behaviours among youth? Prev Med 2018;110:106–13. 10.1016/j.ypmed.2017.11.026 [DOI] [PubMed] [Google Scholar]
- 34.European Commission . Directorate-General for Health and Food Safety. Study on the exposure of children to linear, non-linear and online marketing of foods high in fat, salt or sugar : final report 2021.
- 35.Council on Communications and Media . Children, adolescents, and the media. Pediatrics 2013;132:958–61. 10.1542/peds.2013-2656 [DOI] [PubMed] [Google Scholar]
- 36.Canadian 24-Hour Movement Guidelines for Children and Youth . An integration of physical activity, sedentary behaviour, and sleep, 2021. [DOI] [PubMed] [Google Scholar]
- 37.Sociedad Chilena de Pediatria . Ninos Y dispositivos electronicos: lo bueno Y lo malo de Una exposicion inevitable, 2015. [Google Scholar]
- 38.Lissak G. Adverse physiological and psychological effects of screen time on children and adolescents: literature review and case study. Environ Res 2018;164:149–57. 10.1016/j.envres.2018.01.015 [DOI] [PubMed] [Google Scholar]
- 39.Cox R, Skouteris H, Rutherford L, et al. Television viewing, television content, food intake, physical activity and body mass index: a cross-sectional study of preschool children aged 2-6 years. Health Promot J Austr 2012;23:58–62. 10.1071/HE12058 [DOI] [PubMed] [Google Scholar]
- 40.Paisi M, Witton R, Plessas A. Is there an association between children's screen use and cariogenic diet? Evid Based Dent 2019;20:115–6. 10.1038/s41432-019-0064-z [DOI] [PubMed] [Google Scholar]
- 41.Avery A, Anderson C, McCullough F. Associations between children's diet quality and watching television during meal or snack consumption: a systematic review. Matern Child Nutr 2017;13. 10.1111/mcn.12428. [Epub ahead of print: 17 02 2017]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Andreyeva T, Kelly IR, Harris JL. Exposure to food advertising on television: associations with children's fast food and soft drink consumption and obesity. Econ Hum Biol 2011;9:221–33. 10.1016/j.ehb.2011.02.004 [DOI] [PubMed] [Google Scholar]
- 43.Vassallo AJ, Kelly B, Zhang L, et al. Junk food marketing on Instagram: content analysis. JMIR Public Health Surveill 2018;4:e54. 10.2196/publichealth.9594 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Freeman B, Kelly B, Baur L, et al. Digital junk: food and beverage marketing on Facebook. Am J Public Health 2014;104:e56–64. 10.2105/AJPH.2014.302167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Harris JL, Fleming-Milici F, Phaneuf L, et al. Fast food advertising : Billions in spending, continued high exposure by youth. Rudd Center for Food Policy and Obesity 2021.
- 46.Tatlow-Golden M, Parker D. The devil is in the detail: challenging the UK department of health's 2019 impact assessment of the extent of online marketing of unhealthy foods to children. Int J Environ Res Public Health 2020;17. 10.3390/ijerph17197231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.House of Commons Library . Advertising to children, 2021. [Google Scholar]
- 48.Boyland EJ, Harrold JA, Kirkham TC, et al. The extent of food advertising to children on UK television in 2008. Int J Pediatr Obes 2011;6:455–61. 10.3109/17477166.2011.608801 [DOI] [PubMed] [Google Scholar]
- 49.Adams J, Tyrrell R, Adamson AJ, et al. Effect of restrictions on television food advertising to children on exposure to advertisements for 'less healthy' foods: repeat cross-sectional study. PLoS One 2012;7:e31578. 10.1371/journal.pone.0031578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Council of Better Business Bureaus . The Children’s Food and Beverage Advertising Initiative in Action : A Report on Compliance and Progress During 2016, 2017. [Google Scholar]
- 51.Harris JL, Kalnova SS. Food and beverage TV advertising to young children: measuring exposure and potential impact. Appetite 2018;123:49–55. 10.1016/j.appet.2017.11.110 [DOI] [PubMed] [Google Scholar]
- 52.Fleming-Milici F, Harris JL. Food marketing to children in the United States: can industry voluntarily do the right thing for children's health? Physiol Behav 2020;227:113139. 10.1016/j.physbeh.2020.113139 [DOI] [PubMed] [Google Scholar]
- 53.Department of Health and Social Care and Department for Digital C, . Introducing a total online advertising restriction for products high in fat, sugar and salt (HFSS, 2021. [Google Scholar]
- 54.Mytton OT, Boyland E, Adams J, et al. The potential health impact of restricting less-healthy food and beverage advertising on UK television between 05.30 and 21.00 hours: A modelling study. PLoS Med 2020;17:e1003212. 10.1371/journal.pmed.1003212 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Adams J, Tyrrell R, Adamson AJ, et al. Socio-Economic differences in exposure to television food advertisements in the UK: a cross-sectional study of advertisements broadcast in one television region. Public Health Nutr 2012;15:487–94. 10.1017/S1368980011001686 [DOI] [PubMed] [Google Scholar]
- 56.Brownell KD, Schwartz MB, Puhl RM, et al. The need for BOLD action to prevent adolescent obesity. J Adolesc Health 2009;45:S8–17. 10.1016/j.jadohealth.2009.03.004 [DOI] [PubMed] [Google Scholar]
- 57.Montgomery KC, Chester J. Interactive food and beverage marketing: targeting adolescents in the digital age. J Adolesc Health 2009;45:S18–29. 10.1016/j.jadohealth.2009.04.006 [DOI] [PubMed] [Google Scholar]
- 58.Harris JL, Brownell KD, Bargh JA. The food marketing defense model: integrating psychological research to protect youth and inform public policy. Soc Issues Policy Rev 2009;3:211–71. 10.1111/j.1751-2409.2009.01015.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Harris JL, Yokum S, Fleming-Milici F. Hooked on Junk: Emerging Evidence on How Food Marketing Affects Adolescents’ Diets and Long-Term Health. Curr Addict Rep 2021;8:19–27. 10.1007/s40429-020-00346-4 [DOI] [Google Scholar]
- 60.Forde H, White M, Levy L, et al. The relationship between self-reported exposure to sugar-sweetened beverage promotions and intake: cross-sectional analysis of the 2017 international food policy study. Nutrients 2019;11. 10.3390/nu11123047. [Epub ahead of print: 13 Dec 2019]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Vanderlee L, Czoli CD, Pauzé E, et al. A comparison of self-reported exposure to fast food and sugary drinks marketing among parents of children across five countries. Prev Med 2021;147:106521. 10.1016/j.ypmed.2021.106521 [DOI] [PubMed] [Google Scholar]
- 62.Tatlow‐Golden M, Jewell J, Zhiteneva O, et al. Rising to the challenge: introducing protocols to monitor food marketing to children from the world Health organization regional office for Europe. Obesity Reviews 2021;22. 10.1111/obr.13212 [DOI] [PubMed] [Google Scholar]
- 63.Tatlow-Golden M, Garde A. Digital food marketing to children: exploitation, surveillance and rights violations. Global Food Security 2020;27:100423. 10.1016/j.gfs.2020.100423 [DOI] [Google Scholar]
- 64.World Cancer Research Fund International . How digital media markets unhealthy foods to children, 2017. [Google Scholar]
- 65.Snap Inc . Internet:. Available: https://www.snap.com/en-US/terms [Accessed 3 October 2021].
- 66.Instagram . Internet. Available: https://help.instagram.com/581066165581870# [Accessed 3 October 2021].
- 67.Facebook . Internet. Available: https://www.facebook.com/help/157793540954833/ [Accessed October 3 2021].
- 68.Ofcom . Children and parents: media use and attitudes report, 2017. [Google Scholar]
- 69.Gerritsen S, Sing F, Lin K, et al. The timing, nature and extent of social media marketing by unhealthy food and drinks brands during the COVID-19 pandemic in New Zealand. Front Nutr 2021;8:645349. 10.3389/fnut.2021.645349 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2021-058913supp001.pdf (613.5KB, pdf)
Data Availability Statement
Data are available upon reasonable request. Data are available directly from the International Food Policy Study team on reasonable request (see www.foodpolicystudy.com).