

Abstract
The multidisciplinary nature and long duration of birth cohort studies allow investigation of the relationship between general and oral health and indicate the most appropriate stages in life to intervene. To date, the worldwide distribution of oral health-related birth cohort studies (OHRBCSs) has not been mapped, and a synthesis of information on methodological characteristics and outcomes is not available. We mapped published literature on OHRBCSs, describing their oral health-related data and methodological aspects. A 3-step search strategy was adopted to identify published studies using PubMed, Embase, Web of Science, and OVID databases. Studies with baseline data collection during pregnancy or within the first year of life or linked future oral health data to exposures during either of these 2 life stages were included. Studies examining only mothers' oral health and specific populations were excluded. In total, 1,721 articles were suitable for initial screening of titles and abstracts, and 528 articles were included in the review, identifying 120 unique OHRBCSs from 34 countries in all continents. The review comprised literature from the mid-1940s to the 21st century. Fifty-four percent of the OHRBCSs started from 2000 onward, and 75% of the cohorts were from high-income and only 2 from low-income countries. The participation rate between the baseline and the last oral health follow-up varied between 7% and 93%. Ten cohorts that included interventions were mostly from 2000 and with fewer than 1,000 participants. Seven data-linkage cohorts focused mostly on upstream characteristics and biological aspects. The most frequent clinical assessment was dental caries, widely presented as decayed, missing, and filled teeth (DMFT/dmft). Periodontal conditions were primarily applied as isolated outcomes or as part of a classification system. Socioeconomic classification, ethnicity, and country- or language-specific assessment tools varied across countries. Harmonizing definitions will allow combining data from different studies, adding considerable strength to data analyses; this will be facilitated by forming a global consortium.
Keywords: longitudinal studies; life span; cohort analysis; oral health outcomes; follow-up, prospective studies
Introduction
Cohort studies are observational studies that provide the highest level of scientific evidence to understand the natural history and causality of diseases and disorders (Grimes and Schulz 2002; Cooper et al. 2012). Birth cohort studies allow the investigation of early life predictors and causes of diseases, disorders, and health. They provide unique opportunities to study life course epidemiology, in which biological, behavioral, and psychosocial processes that occur throughout the life of individuals are investigated as mechanisms linking health events and exposures occurring earlier in life (Lawlor et al. 2009).
Oral health is a highly relevant area to apply the life course approach as most oral diseases and conditions are chronic; hence, they need time to develop and are relatively prevalent (Crall and Forrest 2018). Prevention of oral diseases requires extensive knowledge of their causes such as socioeconomic inequalities (Peres, Peres, Thomson, et al. 2011), nutrition and dietary aspects (Peres et al. 2017), access to fluoride (Ha et al. 2019), and appropriate dental care (Camargo et al. 2012), all of which may start early in life. The multidisciplinary nature of birth cohort studies and their perspective of being longstanding studies allow the investigation of the relationship between general and oral health, as well as, for instance, the effect of detrimental health behaviors and conditions, including overweight and obesity, during the life cycle on the risk of periodontitis in adults (Nascimento et al. 2017).
Findings from the 15 largest and long-lasting oral health-related birth cohort studies (OHRBCSs) spread in all 5 continents were debated in a workshop held in Bangkok, Thailand, in 2019 (Peres et al. 2020). It was recognized that each existing cohort had collected comprehensive information on the participants from birth and provided critical evidence regarding dental diseases, as well as their etiology and prevention (Peres et al. 2020). In addition, it acknowledged the existence of several other OHRBCSs in different regions of the world, encompassing high/middle- and low-income countries (Araujo et al. 2020; Peres et al. 2020). However, to date, OHRBCSs worldwide are not mapped, and a synthesis of information with their methodological characteristics and outcomes has not been conducted. The comparison of data from different settings, the environmental exposures at various stages of the individuals' lives, the identification of the cross-validation of the available evidence, the dominant methods applied, and the nature of the existing gaps, along with pooled analysis of combined data sets, are among the gains to be achieved from mapping and articulating the existing OHRBCSs. Likewise, looking ahead, the documentation of OHRBCSs and their characteristics is a wise strategy in an epoch of limited research funding. Mapping potential collaborators will be the first phase of establishing an international consortium. This initiative may help optimize the use of existing resources and, consequently, enhance scientific evidence, as already achieved in other areas such as head and neck cancer (Di Credico et al. 2020) and maternal and child health (Richter et al. 2012).
This study aimed to identify and map the published literature on OHRBCSs and describe their oral health-related data and methodological aspects.
Methods
A scoping review was the preferred approach to map the discerning characteristics of OHRBCSs. Following established guidelines for scoping (Arksey and O’Malley 2005), the 5 steps included 1) identifying the review question, 2) identifying relevant studies, 3) selecting the studies, 4) charting the data, and 5) collating, summarizing, and reporting the results.
Review Questions
Where have OHRBCSs been undertaken worldwide?
What are the demographic and methodological characteristics of the identified OHRBCSs?
How have the researchers addressed oral and dental conditions in studies of this nature?
Search Strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was followed (Appendix File 1). A 3-step search strategy was adopted to identify published studies comprehensively. First, a tailored search strategy on the electronic PubMed database included search terms for identifying birth cohorts and population oral health outcomes. The second step included search on reference lists of selected studies. It aimed to identify relevant studies that might have been missed during the electronic database search. The third step comprised a systematic check of scoping or systematic reviews on general birth cohort studies as an interactive process between searching the literature and refining search strategy with revision of the included articles (Winn et al. 2015; Araujo et al. 2020). Finally, the same steps described above were extended to 3 other databases (Embase, Web of Science, and OVID) as part of the refining process. The search strategy was adapted for each database on November 3, 2020, and then updated on April 12, 2021 (Appendix File 2).
Study Selection
Inclusion criteria consisted of the following: 1) studies must have either started the baseline data collection during pregnancy or within the first year of life or linked future oral health data to exposures during either of these 2 life stages, and 2) studies based on clinical-epidemiological or self-reported oral health data obtained through at least 1 follow-up, or 3) OHRBCSs with nested interventional studies and contrariwise. Exclusion criteria comprised 1) studies published in a language other than English, 2) studies that did not collect child oral health data beyond the first wave (baseline), 3) studies that examined only mothers' oral health characteristics during pregnancy and birth outcomes, and 4) studies that specifically recruited premature/low birth weight/high birth weight children or population with other specific characteristics such as cohorts of adolescents. Cohorts generated through linked and registry data that fulfilled the above requirements on inclusion criteria were also considered in this review.
Articles identified in the electronic search were imported to a bibliographic software, Endnote X9. Titles and abstracts were first screened independently by at least 2 reviewers (coauthors). Full texts of relevant articles were then retrieved and examined for suitability. Any disagreements regarding the selection of studies were resolved through discussion with a third reviewer (the first author).
Charting the Data
The following descriptive epidemiological data were charted: cohort characteristics (name of the study, country, calendar year of the cohort baseline, eligibility criteria, sample sizes at general and oral health baseline assessments, age of participants in the last general and oral health follow-ups, number of oral health follow-ups, and follow-up rate), and oral health-related outcomes.
As 1 birth cohort study will often lead to many publications, birth cohort information was retrieved from the source study and the latest publication. Articles that reported significant departure from the original aims of the birth cohort studies were identified through the reference lists and relevant data charted. Searches in electronic pages of cohort studies and contact (via e-mail) with researchers/authors of these studies were performed when necessary.
Collating, Summarizing, and Reporting the Results
All identified OHRBCSs were geographically depicted on a world map and classified by income in line with the World Bank classification (Economic Department and Social Affairs 2020). A descriptive analysis was made of information from OHRBCSs in which oral health data were presented in 2 or more publications. OHRBCSs nested within interventional studies (and vice versa), OHRBCSs using exclusively data linkage, and cohorts with only 1 publication presenting oral health information were identified and presented separately as appendix material due to the relatively limited information on these cohorts.
Results
The flowchart describing the selection of the studies is presented in Figure 1. After removing 2,967 duplicates, 1,721 articles were suitable for the initial screening of titles and abstracts. Of these, 489 articles were deemed relevant for full-text reading. Finally, 528 articles met the eligibility criteria and were included in the qualitative synthesis, with an additional 7 articles obtained after contacting their authors. Lack of data from infancy and groups allocated by intervention at the baseline were the main exclusion reasons. Therefore, the final selected articles generated 120 unique OHRBCSs. Among them, we grouped prospective cohort studies with at least 2 oral health publications (n = 48), those with single oral health publications (n = 51), mixed cohort and interventional studies (n = 10), 7 cohort studies through data linkage with 2 or more publications, and 4 OHRBCSs whose age range of participants was broader than the inclusion criteria but included the target age.
Figure 1.
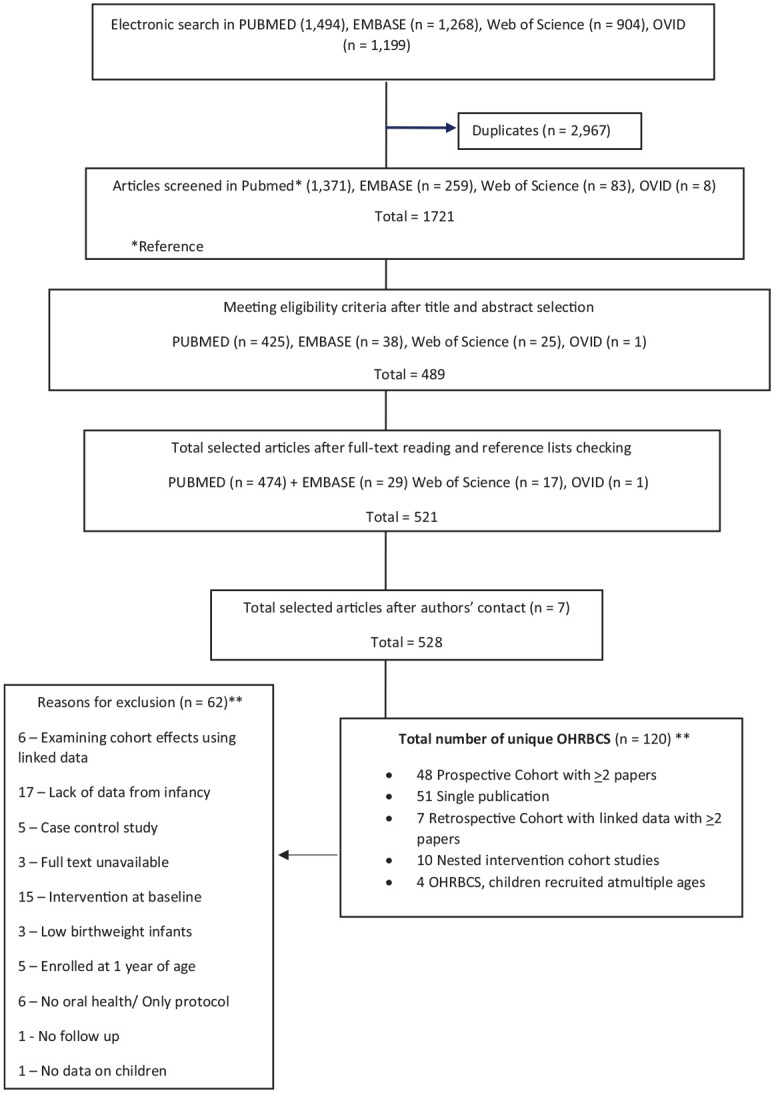
Flowchart for selection of studies. OHRBCS, oral health-related birth cohort studies.
**Boxes refer to the number of OHRBCS.
Figure 2 shows the geographic distribution of the OHRBCSs with their corresponding World Bank classification by income. Most of the cohorts (n = 88; 75%) were in high-income countries: 26 in upper-middle, only 1 in a low-middle, and 2 cohorts in low-income countries, whose representation ranged from a national to city level. The United States was the country with the highest number of OHRBCSs (n = 17), followed by Australia, Brazil (n = 15, each), and Sweden (n = 14).
Figure 2.

Geographical distribution and World Bank classification by income (World Bank 2020) of oral health-related birth cohort studies.
Over half of the OHRBCSs (54%) with 2 or more oral health publications started from 2000 onward, while nearly 15% were cohorts with a baseline before the 1980s (Table 1). The Iowa Facial Growth Study and The Newcastle Thousand Families cohort study are the oldest cohorts, with baseline data initiated in 1946 and 1947, respectively, followed by the Swedish Urban Community Study (1955–1958) (references in Appendix File 3). The recruitment process started with pregnant women in almost a third of studies. In approximately a quarter of the studies, the cohorts reached adulthood (Table 1). Studies with a single-publication OHRBCS had their baseline between 1981 and 2016, mostly from Brazil, Japan, and Sweden (Appendix Table 4).
Table 1.
General Characteristics of the Oral Health-Related Birth Cohort Studies with 2 or More Oral Health Publications.
| Cohort Name a | City or Cities, Country | Cohort Baseline | Eligibility Criteria | Last General Follow-up Age |
|---|---|---|---|---|
| 1. Australian ABC | Darwin, Australia | 1987 | Singleton born between January 1987 and March 1990 to an Aboriginal mother (Royal Darwin Hospital). | 25 y |
| 2. Australian Wide Twin Study | Australia | 2005 | Twins born in Australian states recruited through the Australian Twin Registry and the Australian Multiple Birth Association. | 14 y |
| 3. Avon Longitudinal Study of Parents and Children (ALSPAC) | Avon, England | 1991 | Pregnant women and their children. Children in Focus substudy: random 10% sample of children born in the last 6 mo (June to December 1992). | 25 y |
| 4. British Cohort Study (BCS) | England, Scotland, Wales | 1970 | All children currently living in England, Scotland, and Wales who were born in a single week of 1970. | 46 y |
| 5. Christchurch Child Development Study | Christchurch, New Zealand | 1977 | Children born in maternity units in urban regions (mid-1977). | 7 y |
| 6. Cleveland | Cleveland, USA | 2007–2010 | Healthy infants and mothers >18 y, living up to a 2-h driving distance from 2 neonatal hospitals. | 2 y |
| 7. Dundee Study | Dundee, Scotland | 1993–1994 | All children born during 1 calendar year (April 1993–March 1994). | 4 y |
| 8. Epsom General Hospital | Surrey, UK | 1995–1996 | Children born between April 1, 1995, and April 31, 1996, at Epsom General Hospital in the mid-Surrey area. | 1.5 y |
| 9. Flemish Preschool Children | Flanders, Belgium | 2003–2004 | All healthy children born in Tielt and Berlaar whose parents completed the questionnaires and intended to live in the region. Twins: 1 included. | 5 y |
| 10. Generation R | Rotterdam, Netherlands | 2002 | All pregnant mothers with an expected delivery date between April 2002 and January 2006. | 17 y |
| 11. GINIplus | Munich/Wesel, Germany | 1995–1998 | Healthy full-term newborns recruited from obstetric clinics. | 15 y |
| 12. Griffith University Environments for Healthy Living | South-East Queensland, Australia | 2006 | ≥24 wk of gestation, mothers >16 y of age who provided informed consent from Logan, Gold Coast, and Tweed public maternity hospitals. | 6–7 y |
| 13. Growth and Overweight Prevention Study | Halland, Sweden | 2007–2009 2010–2012 |
No specific inclusion criteria. | 5 y |
| 14. Growing Up in Ireland | Nationwide, Ireland | 2007–2008 | No specific inclusion criteria. | 3 y |
| 15. Gudaga Study | Sydney, Australia | 2005–2007 | Either biological parents identified as Aboriginal. | 9 y |
| 16. GUSTO | Singapore | 2009–2010 | Pregnant citizen or permanent resident ≥18 y willing to donate umbilical cord, placenta, and blood sample attending their first-trimester antenatal dating ultrasound scan. | 5 y |
| 17. Haitian Health Foundation | Jérémie, Haiti | 2005 | Children enrolled in the Haitian Health Foundation System with at least 2 recorded weights per year for at least 3 of the first 5 y of life. | 11–19 y |
| 18. Hong Kong Children of 1997 | Hong Kong, China | 1997 | Recruited only if their public water system had fluoride above 0.5 ppm. | 13 y |
| 19. Iowa Facial Growth Study | Iowa, USA | 1946 | Healthy full-term babies and likelihood of continuing residence in the community. | 26 y |
| 20. Iowa Fluoride Study (IFS) | Iowa, USA | 1992–1995 | Mothers of newborns were recruited from 8 Iowa hospitals postpartum. | 23 y |
| 21. João Pessoa | João Pessoa, Paraíba, Brazil | 2000 | Resident children born in a public hospital with gynecologic and obstetric care for poor families. | 3 y |
| 22. LISAplus | Munich, Germany | 1995–1999 | Newborns from parents with German nationality from Munich, Leipzig, Wesel, and Bad Honnef. | 15 y |
| 23. Longitudinal Study of Australian Children (LSAC) | Australia | 2003 | Children from urban and rural areas of all states and territories in Australia. | 11 y |
| 24. Mamma-Barn, Mother-Child (Mamba) | Umea, Sweden | 2007–2009 | Babies born in a small inland town or a coastal university city in Northern Sweden (September 7–January 9). | 3 y |
| 25. Mater Mother | South Brisbane, Australia | 2003 | Random preterm and full-term infants with normal birth weights (>2,500 g). | 2 y |
| 26. Mother-Child Binome Study | Aracatuba, Brazil | 2006 | All pregnant women enrolled in a government program for the monitoring of prenatal care. | 30 mo |
| 27. National Child Development Study (NCDS) | England, Scotland, Wales | 1958 | Intergenerational mobility and adult oral health in a British cohort. | 55 y |
| 28. Newcastle Thousand Families Cohort Study | Newcastle upon Tyne, UK | 1947 | Mothers resident in the city of Newcastle upon Tyne. | 51 y |
| 29. Northern Finland Birth Cohort (NFBC) | Oulu, Lapland, Finland | 1966 | Pregnant women and their children. | 46 y |
| 30. Northern Plains | Indiana, Iowa, and North Carolina, USA | 2010 | US Hispanic and White non-Hispanic children of similar ages. | 3 y |
| 31. OMIC Study | Umeå, Sweden | 2011 | Healthy infants born after a full-time pregnancy. | 5 y |
| 32. Osaka Maternal and Child Health Study | Neyagawa City, Osaka, Japan | 2001–2003 | Pregnant women who lived in the city and further 375 pregnant women recruited from outside Neyagawa. | 41–50 mo |
| 33. Pacific Islands Families Study | Auckland, New Zealand | 2000 | Pacific Islands ethnic infants and New Zealand permanent residents born in Middlemore Hospital. | 14 y |
| 34. Pelotas Birth Cohort Study (1982) | Pelotas, Brazil | 1982 | Children born in maternity units in the urban region during the year. | 31 y |
| 35. Pelotas Birth Cohort Study (1993) | Pelotas, Brazil | 1993 | Children born in maternity units in the urban region during the year. | 22 y |
| 36. Pelotas Birth Cohort Study (2004) | Pelotas, Brazil | 2004 | Children born in maternity units in the urban region during the year. | 13 y |
| 37. Ribeirão Preto | Ribeirão Preto, Brazil | 1994 | Residents born at 10 hospitals in the city over a period of 4 mo. | School age |
| 38. São Luís | Sao Luís, Brazil | 1997 | Births between March 1997 and February 1998 in 10 private and public hospitals. | 18–19 y |
| 39. Study of Mothers’ and Infants’ Life Events (SMILE) | Adelaide, Australia | 2014 | English-speaking mothers from the 3 major hospitals, with intention to live in the city. | 3 y |
| 40. Swedish Urban Community | Sweden | 1955–1958 | Children from a Swedish urban community. | 18 y |
| 41. Thai PCTC | 4 districts and Bangkok, Thailand | 2000 | Pregnant women who resided or intended to bring their children in the Kanchanaburi, Nan (a), Khon Kaen (b), Bangkok, and Songkhla (c) districts. | a: 3 y b: 6–7 y c: 18 mo |
| 42. The Dunedin Multidisciplinary Health and Development Study | Dunedin, New Zealand | 1972 | Babies born at the only maternity unit at the time (April 1, 1972, to March 31, 1973), living in the greater Dunedin area in the next 3 y after birth. | 45 y |
| 43. The Epigenetic Twins Study | Melbourne, Australia | 2007 | Pregnant women from 3 Melbourne hospitals in their second trimester (18–22 wk of gestation). | 6 y |
| 44. The Finnish Family Competence Study | Turku, Finland | 1986 | Nulliparous pregnant women from the Province of Turku and Pori, visiting a public health nurse. | 10 y |
| 45. TUMME Study | Umeå, Sweden | 2009–2012 | 0- to 2-mo-old babies, birth weight 2,500–4,500 g, full term, and exclusively breastfed or formula fed. | 4 mo |
| 46. VicGeneration (VicGen) | Victoria State, Australia | 2008 | Mothers and their babies born in Maternal and Child Health Centres (metropolitan, regional, and rural areas) who intended to live there in the next year. | 6 y |
| 47. Women, Infants, and Children (WIC) Cohort–Southeast Iowa | Iowa, USA | 2003–2004 | Children ranging in age from 6 to 24 mo who were enrolled in the IOWA WIC program. | Baseline + 18 mo |
| 48. Xinhua Town | Guangzhou, China | 2008 | Parents of children physically healthy at birth and who had lived in the district for ≥2 y. | 2 y |
Reference list: Appendix File 3.
The number of general waves varied across OHRBCSs with 2 or more publications. Older studies had higher numbers, such as the Dunedin study. However, some younger cohorts since 2000 have relatively large numbers of overall follow-ups, such as the Generation R study and GUSTO study (references in Appendix File 3). Oral health follow-ups, which included oral health clinical data in all waves, were found in over 70% of the cohorts. The participation rate between the baseline and the last oral health follow-up varied between 7% and 93%. While some studies highlighted their ethnic diversity (Table 2 and Appendix Table 4), most of them had similar representation by sex.
Table 2.
Design Characteristics of the Oral Health-Related Birth Cohort Studies with ≥2 Oral Health Publications.
| Cohort Name a | Baseline Sample | W1 | W2 | W3 (Starting Age) | Number (%) of Participants in the Last Oral Health Follow-up (% Followed in Relation to the Oral Health Baseline)/Ethnicity | Last Oral Health Follow-up |
|---|---|---|---|---|---|---|
| 1. Australian ABC | 686 | 4 | 1 | 1 (16–20 y) | 442 (69%) | 18 y |
| 2. Australian Wide Twin Study | 913 | 3 | 3 | 3 (6 y) | 208 (32%) | 14 y |
| 3. Avon Longitudinal Study of Parents and Children (ALSPAC) | 14,541 | 25 | 3 | 3 (2 y) | “Children in Focus” substudy, 1,429 (baseline data not provided)/96% (White), 4% (non-White) | 5 y |
| 4. British Cohort Study (BCS) | 16,569 | 9 | 2 | 2 (26 y) | 8,581 (52%)/95% (White), 5% (non-White) | 46 y |
| 5. Christchurch Child Development Study | 1,265 | 9 | 1 | 1 (7 y) | 1,127 (85%)/93% (White), 7% (non-White) | 7 y |
| 6. Cleveland | 468 | 2 | 2 | 2 (8 mo) | 378 (80%)/68% (Black), 32% (non-Black) | 18–20 mo |
| 7. Dundee Study | 1,703 | 4 | 4 | 4 (1–4 y) | 765 (70%) | 4 y |
| 8. Epsom General Hospital | 2,300 | 3 | 2 | 2 (1 y) | 163 (7%) | 1.5 y |
| 9. Flemish Preschool Children | 972 | 3 | 3 | 2 (3 y) | 703 (72%) | 5 y |
| 10. Generation R | 9,749 | 11 | 2 | 2 (6 y) | 7,393 (76%)/68% (Dutch, other-European), 32% (other) | 10 y |
| 11. GINIplus | 2,949 | 15 | 2 | 2 (10 y) | 652 (22%) | 15 y |
| 12. Griffith University Environments for Healthy Living | 2,904 | — | 1 | 1 (6 y) | 174 (unclear) | 6 y |
| 13. Growth and Overweight Prevention Study | 551 | 3 | 3 | 2 (3 y) | 292 (53%) | 5 y |
| 14. Growing Up in Ireland | 11,134 | — | 1 | 1 (3 y) | 9,793 (88%)/84% (Irish), 16% (other) | 3 y |
| 15. Gudaga Study | 149 | — | 2 | 2 (7 y) | 98 (65%) | 9 y |
| 16. GUSTO | 1,176 | 14 | 2 | 2 (2 y) | 721 (61%)/57% (Chinese), 27% (Malay), 16% (Indian) | 3 y |
| 17. Haitian Health Foundation | 1,183 | 1 | 1 | 1 (11–19 y) | 1,058 (89%) | 11–19 y |
| 18. Hong Kong Children of 1997 | 668 | 23 | 3 | 3 (12 y) | 485 (73%) | 12 y |
| 19. Iowa Facial Growth Study | 183 | 4 | 4 | Unavailable | Unclear | 26 y |
| 20. Iowa Fluoride Study (IFS) | 1,387 | 8 | 5 | 5 (5 y) | 342 (25%)/96% (White), 4% (other) | 23 y |
| 21. João Pessoa | 246 | 6 | 5 | 5 (1 y) | 224 (93%) | 3 y |
| 22. LISAplus | 1,467 | 8 | 2 | 2 (10 y) | 400 (27%) | 15 y |
| 23. Longitudinal Study of Australian Children (LSAC) | 10,090 | 8 | 6 | 6 (0–1 y) | 7,301 (72%)/3% (Indigenous), 97% (other) | 11 y |
| 24. Mamma-Barn, Mother-Child (Mamba) | 207 | 1 | 1 | 1 (3 y) | 155 (65%) | 3 y |
| 25. Mater Mother | 312 | 1 | 6 | 6 (3 mo) | 111 (36%)/80% (White), 20% (other) | 2 y |
| 26. Mother-Child Binome Study | 120 | 3 | 3 | 3 (12 mo) | 80 (67%) | 30 mo |
| 27. National Child Development Study (NCDS) | 17,416 | 8 | 4 | 4 (33 y) | 11,468 (70%)/95% (White), 5% (non-White) | 33 y |
| 28. Newcastle Thousand Families Cohort Study | 1,142 | 7 | 1 | 1 (49–51 y) | 337 (30%) | 49–51 y |
| 29. Northern Finland Birth Cohort (NFBC) | 12,058 | 3 | 1 | 1 (31 y) | 1,945 (60%) | 46 y |
| 30. Northern Plains | 239 | 7 | 7 | 7 (4 mo) | 232 (97%) | 3 y |
| 31. OMIC Study | 206 | 5 | 5 | 5 (2 d) | 116 (56%) | 5 y |
| 32. Osaka Maternal and Child Health Study | 1,002 | 6 | 1 | 1 (41–50 mo) | 315 (32%) | 41–50 mo |
| 33. Pacific Islands Families Study | 1,376 | 5 | 1 | 1(4 y) | 1,048 (76%)/45% (Samoan), 21% (Tongan), 18% (Cook Island Māori), 8% (other Pacific), 7% (non-Pacific) | 14 y |
| 34. Pelotas Birth Cohort Study (1982) | 5,914 | 11 | 3 | 3 (15 y) | 539 (60%)/78% (White), 22% (non-White) | 31 y |
| 35. Pelotas Birth Cohort Study (1993) | 5,249 | 10 | 3 | 3 (6 y) | 1,203 (sample was inflated in the last follow-up) | 18 y |
| 36. Pelotas Birth Cohort Study (2004) | 4,231 | 8 | 2 | 2 (5 y) | 992 (88%) | 12 y |
| 37. Ribeirão Preto | 2,911 | 1 | 1 | 1 (school age) | 790 (69%)/57% (White), 43% (non-White) | School age |
| 38. São Luís | 2,541 | 2 | 1 | 1 | 2,515 (sample was inflated in the last follow-up) | 18–19 y |
| 39. Study of Mothers’ and Infants’ Life Events (SMILE) | 2,181 | 5 | 1 | 1 (2–3 y) | 1,040 (48%) | 3 y |
| 40. Swedish Urban Community | 212 | 23 | 23 | 23 (1 y) | 201 (95%) | 18 y |
| 41. Thai PCTC | Mueng Nan,n = 783; Khon Kaen, n = 860; Thepa/Songkhla, n = 795 | 10 | Mueng Nan, n = 6; Khon Kaen, n = 7; Thepa/Songkhla, n = 3 | Nan, n = 2 (2 y); Khon Kaen, n = 3 (2 y); Songkhla, n = 3 (9 mo) | Mueng Nan, n = 597 (76%); Khon Kaen, n = 290 (68%); Thepa/Songkhla, n = 495 (62%) | Mueng Nan: 3 y; Khon Kaen: 6–7 y; Thepa/Songkhla: 18 mo |
| 42. The Dunedin Multidisciplinary Health and Development Study | 1,037 | 14 | 12 | 8 (5 y) | 896 (89%) | 45 y |
| 43. The Epigenetic Twins Study | 250 twin pairs | 3 | 1 | 1 (6 y) | 344 participants from 172 twin pairs (69%) | 6 y |
| 44. The Finnish Family Competence Study | 1,443 | 7 | 4 | 4(3 y) | 1,074 (74%) | 10 y |
| 45. TUMME Study | 240 | 4 | 2 | 2 | 133 (55%) | 4 mo |
| 46. VicGeneration (VicGen) | 466 | 7 | 7 | 7 (1 mo) | 270 (58%) | 5 y |
| 47. Women, Infants, and Children (WIC) Cohort–Southeast Iowa | 212 | — | Not reported | 1 (6 to 24 mo) | 128 (60%)/75% (White), 18% (Hispanic), 3% (Black), 4% (mixed race) | 18 mo after baseline |
| 48. Xinhua Town | 225 | 5 | 5 | 5 (8 mo) | 155 (69%) | 2 y |
W1, total number of general waves; W2, total number of oral health waves; W3, number of waves including oral health clinical epidemiological data and starting age.
Reference list: Appendix File 3
Table 3 displays oral health outcomes from the OHRBCSs with 2 or more publications. The most frequently investigated oral condition through clinical examination was dental caries, widely presented as decayed, missing, and filled teeth (DMFT/dmft). The International Caries Detection and Assessment System (ICDAS) index was given in nearly one-third of studies with a baseline from 2000 onward, although ongoing studies starting in the 1960s (GINIplus study) and the 1990s (LISAplus study) also used this index. Oral microbiota (n = 18), the level of dental plaque (n = 13), teeth emergence (n = 12), and enamel defects (n = 11) were the next most published dental outcomes. Periodontal conditions were depicted through a wide range of indices as isolated outcomes or as part of a classification system. Self-reported outcomes were, among others, dental caries, periodontal conditions, xerostomia, temporomandibular disorders, and halitosis, as well as a self-perception of the overall oral health status. However, most of the self-reported conditions were assessed with nonvalidated instruments (Appendix File 3).
Table 3.
Oral Health-Related Characteristics of the Oral Health-Related Birth Cohort Studies with ≥2 Oral Health Publications.
| Dental/Oral-Related Measurements | Level of Investigation | Study |
|---|---|---|
| Dental caries | Self-reported | Longitudinal Study of Australian Children; NFBC; Osaka Maternal and Child Health Study; Pacific Islands Families study; Pelotas (1982) |
| Decayed, missing, and filled teeth (DMFT/dmft) | ABC; ALSPAC; Born in Bradford cohort; Christchurch Child Development Study; Cleveland; Dunedin; Epsom General Hospital; Flemish Preschool Children; Generation R; GINIplus; Grow and Overweight Prevention study; LISAplus; NFBC; Osaka Maternal and Child Health Study; PCTC; Pelotas (1982); Pelotas (1993); The Finnish Competence Study | |
| Decayed, missing and filled surfaces in permanent (DMFS) and primary (dmfs) dentitions; decayed and filled surfaces attack rate (DFSAR)1 | Dundee Study; Dunedin1; GINIplus; IFS1; João Pessoa; LISAplus; Mamba; Northern Plains; Pelotas (1982); Pelotas (2004); SMILE; VicGen; Xinhua Town | |
| International Caries Detection and Assessment System (ICDAS) Caries lesions (white spots or cavitation)2 |
Australian Wide Twin Research; Cleveland; Detroit; GINIplus; Griffith University Environments for Healthy Living; GUSTO; LISAplus; Mother–Child Binome Study2; NFBC; São Luís2; SMILE; The Epigenetic Twins Study; VicGen | |
| U, D1, D2, D3 | Dundee Study; PCTC; Women, Infants, and Children (WIC)–Iowa | |
| Early Childhood Oral Health Program (ECOH) | Gudaga | |
| Gingival conditions | Plaque; Silness-Löe Plaque Index3; Simplified Oral Hygiene Index4; Visible Plaque Index5 | ABC; Australian Wide Twin Research; Cleveland; Epsom General Hospital5; Flemish Preschool Children5; GINIplus; GUSTO3; LISAplus; NFBC; Pelotas (1982); Pelotas (1993); Pelotas (2004)4; São Luís5 |
| Gingivitis, calculus; Gingival Bleeding Index6 | ABC; Australian Wide Twin Research; Cleveland; GINIplus; GUSTO; LISAplus; NFBC; Pelotas (1982); Pelotas (1993), São Luís6 | |
| Self-reported | NCDS; NFBC | |
| Periodontal diseases | American Academy of Periodontology definition7; clinical attachment level, probing depth, gingival recession8; self-reported9; probing pocket depth, bleeding on probing, clinical attachment level10; probing pocket depth, bleeding on probing, alveolar bone level, presence of plaque11 | ABC7; Dunedin8,9; NFBC11; Pelotas (1982)7,10; Pelotas (1993)10; São Luís10 |
| Dental fluorosis | Fluorosis Risk Index (FRI)12; Tooth Surface Index of Fluorosis13; fluorosis (diffuse opacities)14; presence of fluorosis in the upper central incisors15; presence of fluorosis in the primary dentition16 | ABC15; GINIplus14; IFS12,13,16; LISAplus14 |
| Xerostomia | Self-reported | Dunedin; NFBC |
| Enamel defects | Molar incisor hypoplasia17; hypomineralized second primary molars18; amelogenesis and dentinogenesis imperfecta19; Developmental Defects of Enamel Index (DDE)20 | Australian Wide Twin Research17; Cleveland17; Generation R17; GINIplus17,19; Hong Kong17,20; João Pessoa20; LISAplus17,19; PCTC17; São Luís20; The Epigenetic Twins Study18; Xinhua Town17,20 |
| Occlusal status/malocclusion crowding7 | The Index of Orthodontic Treatment Need (IOTN)21; intercanine and intermolar widths22; overjet/overbite/posterior crossbite—primary dentition23; Peer Assessment Rating24; World Health Organization index25; Dental Aesthetic Index (DAI)25; self-reported26 | Generation R21; Iowa Facial Growth Study22; Mother–Child Binome Study23; NFBC24; Pelotas (1982)25; Pelotas (1993)23; Pelotas (2004)23,24,25; Dunedin26 |
| Temporomandibular disorders | Diagnostic Criteria for Temporomandibular Disorders (DCTD) | Dunedin; NFBC |
| Self-reported | Dunedin | |
| Oral microbiota | Mutans streptococci | Cleveland; Epsom General Hospital; Jefferson County; Mamba; Mater Mother; Newcastle; Northern Plains; Australian Wide Twin Research; Umea; WIC–Iowa; Xinhua Town |
| Mutans streptococci and lactobacilli | Australian Wide Twin Research; Griffith University Environments for Healthy Living | |
| Streptococcus mutans, Streptococcus sobrinus, lactobacilli, and yeasts | Dundee | |
| Total lactobacilli, S. mutans, and S. sobrinus | Mamba | |
| S. mutans and S. sobrinus | Northern Plains | |
| Firmicutes, Proteobacteria, Actinobacteria, Bacteroidetes, Fusobacteria, Abiotrophia, Actinomyces, Capnocytophaga, Corynebacterium, Fusobacterium, Kingella, Leptotrichia, Neisseria, and Porphyromonas | OMIC | |
| Streptococcus, Actinobacteria, Bacteroidetes, Firmicutes, Fusobacteria, GNO2, Proteobacteria, SR1, Synergistes, Tenericutes, TM7, and Lactobacillus | TUMME | |
| Streptococcus mitis group, Gemella haemolysans, Streptococcus salivarius group, Rothia mucilaginosa, Staphylococcus caprae, Haemophilus parainfluenzae, and Campylobacter concisus | VicGen | |
| Oral mucosal lesions | Presence of selected mucosal lesions27; presence of acute necrotizing ulcerative gingivitis, white lesion, candidiasis, leukoplatia, carcinoma, other28 | ABC27; Pelotas (1982)28; Pelotas (1993)28; Pelotas (2004)28 |
| Dental trauma | History of trauma in enamel or dentine (anterior teeth) | ABC |
| Teeth emergence | Tooth retention29; primary dentition30; permanent dentition31 | ABC29; Australian Wide Twin Research30; ALSPAC30; Cleveland30; Generation R30,31; GUSTO30; Hong Kong31; NFBC30; Northern Plains30; Pelotas (1993)30,31; Swedish Urban Community31; The Epigenetic Twins Study30 |
| Saliva analysis | Salivary buffer capacity32; salivary flow rate33; salivary levels of total IgA, IgG, and IgM34 | Griffith University Environments for Healthy Living32; NFBC33; Mater Mother34 |
| Dental health problem | Self-reported (“Has <child> been to visit the dentist because of a problem with his/her teeth?”) | Growing Up in Ireland |
| Arch width, micrognathis | Maxillary anterior/posterior arch width, mandibular anterior/posterior arch width | Iowa Facial Growth Study |
| Tooth wear | Attrition35; primary dentition36; Basic Erosive Wear Examination Index (BEWE)37 | ABC35; IFS36; NFBC37 |
| Self-reported oral health | “Would you say that your dental health (mouth, teeth, denture) is excellent, very good, good, fair or poor?”38; “In your opinion, do you have a healthy mouth without a need of any dental treatment?”39; “Compared to people of your age, how do you consider the condition of your teeth, lips, jaws, or mouth?”40 | NCDS38; NFBC39; Pelotas (1993)40 |
| Number of lost teeth | Clinical examination41; self-reported42 | Dunedin41; NFBC42; Newcastle Thousand Families Cohort Study41; Osaka Maternal and Child Health Study42; Pacific Islands Families study42; Pelotas (1982)41 |
| Dental anxiety/fear | Modified Dental Anxiety Scale (MDAS) | NFBC; Dunedin |
| Self-reported | ABC; Pelotas (1982); Pelotas (2004) | |
| Orofacial pain | Self-reported | NFBC |
| Restorative material | Type of material, tooth, and cavity, long life43; quality of restorations44 (Modified United States Public Health Service) | Pelotas (1982)43; Pelotas (2004)44 |
| Prosthesis needs | World Health Organization criteria | Pelotas (1982) |
| Bruxism parafunction | Self-reported | Dunedin; Pelotas (1982); Ribeirão Preto |
| Halitosis | Self-reported | Pelotas (1982) |
| Dental pain | Self-reported | ABC; Pelotas (1993); Pelotas (2004) |
Reference numbers in the second column refer to studies listed in the third column.
ABC, The Australian ABC study; ALSPAC, Avon Longitudinal Study of Parents and Children; Dunedin, The Dunedin Multidisciplinary Health and Development Study; IFS, Iowa Fluoride Study; NCDS, National Child Development Study; NFBC, Northern Finland Birth Cohort; SMILE, Study of Mothers’ and Infants’ Life Events.
Table 4 (references in Appendix File 5) shows the OHRBCSs that included nested intervention studies or were follow-ups in studies initially designed to test interventions. Eight of the 10 birth cohorts of this kind dated from 2000 and had sample sizes of fewer than 1,000 participants at baseline. Interventions were related to oral health promotion, in particular, breastfeeding counseling (60%) and methods focusing on dental caries prevention.
Table 4.
Oral Health-Related Birth Cohort Studies That Included Interventions.
| Cohort Name a | City or Cities, Country | Cohort Baseline | Recruited (Birth) | Eligibility Criteria | Intervention b | Last Follow-up Age | Main Outcome |
|---|---|---|---|---|---|---|---|
| 1. Oral Health Promotion Program (OHPP) | Vorarlberg, Austria | 1998 | 600 | Children aged 5 y attending dental examinations at kindergartens | Counselling breastfeeding, diet, pacifier use | 5 y | Caries |
| 2. German Birth Cohort | Jena, Germany | 2009–2010 | 1,162 | All newborns in the region | Maternal counseling, fluoride varnish and toothpaste | 8 y | Caries, DDE, occlusion |
| 3. Toddler Overweight and Tooth Decay Prevention Study (TOTS) | Portland, USA | 2006 c | 272/100% (American Indian) | Births in 4 geographically separated tribal groups under WIC/MCH/dental clinic structures | Counseling breastfeeding, sugar-sweetened beverages, type of water (community and family levels) | 18–30 mo (target 24 mo) | Caries |
| 4. MAYA trial | California, USA | 2003–2007 | 361/97% (Hispanic), 3% (other) | Maternal age of 18–33 y, singleton fetus, and stable local residency, intended to give birth in Mexico | Oral health counseling, chlorhexidine, fluoride varnish | 3 y | Caries, microorganisms |
| 5. New Zealand | Aotearoa, New Zealand | 2011–2012 | 200/100% (Māori) | Māori mothers residing within the Waikato-Tainui tribal area | Dental care (pregnancy), fluoride varnish, motivational interviewing, guidance in advance | 3 y | Caries |
| 6. São Leopoldo Birth Cohort Study | São Leopoldo, Brazil | 2001–2002 | 500 | Full-term, normal-weight babies | Nutritional advice (breastfeeding), healthy weaning (home visits) | 4 y | Caries |
| 7. Early Life Nutrition and Health Birth Cohort Study | Porto Alegre, Brazil | 2008 | 715/55% (White), 45% (Black) | Mother–child (<1 y) pairs from municipal health centers (>100 annual appointments) | Guidance on the introduction of high-sugar foods and drinks, duration and frequency of breastfeeding | 6 y | Caries, dental trauma |
| 8. Promotion of Breastfeeding Intervention Trial (PROBIT) | Belarus | 1997 | 17,046 | Mother–infant pairs from 31 maternity hospitals and polyclinics | Counseling breastfeeding | 11 y | Caries |
| 9. The Queensland Birth Cohort Study | Logan-Beaudesert, QLD, Australia | 2007–2008 | 714 | Healthy pregnant women from the community birthing clinics in the district | Casein phospho-peptide–amorphous calcium phosphate paste, chlorhexidine gel, oral health promotion | 12 y | Caries/cost |
| 10. PROMISE-EBF study | Uganda | 2006 | 765 | Pregnant women from 24 clusters | Peer counseling exclusive breastfeeding | 5 y | Caries |
DDE, Developmental Defects of Enamel Index; MCH, Maternal Child Health; WIC, Women, Infants, and Children.
Reference list: Appendix File 5.
Interventions varied across follow-up.
Follow-up after 18 to 30 mo from the baseline.
Data linkage of OHRBCSs with 2 or more publications (n = 7) was primarily undertaken in Scandinavian countries (n = 5) (Appendix Table 6). Primary exposures were concentrated on upstream characteristics such as socioeconomic status, family characteristics, and biological as well as congenital aspects and birth outcomes. Finally, Appendix Table 7 gives details of the 4 OHRBCSs that recruited participants at a range of ages, with 3 conducted in the United States and 1 in Australia.
Discussion
Main Findings
We mapped 120 OHRBCSs distributed in 34 countries across all continents. These included literature from the mid-1940s to the 21st century and revealed how initiating birth cohorts expanded over time worldwide. Studies from high-income countries were predominant until the early 1980s, when a population-based birth cohort study, the Pelotas Birth Cohort Study (1982 PBCS) in Brazil (Peres, Peres, Demarco, et al. 2011), was launched in 1982, followed by The Birth to Ten Study in Johannesburg/Soweto, South Africa, in 1990 (MacKeown et al. 2000). Interestingly, OHRBCSs in non-high-income countries account for approximately 50% of cohorts since 2000, although many of these had only 1 publication—for example, 5 cohorts from Brazil (Massoni et al. 2009; Guedes et al. 2015; Campos et al. 2018; Pinho et al. 2019), 2 from China (Sun 2020; Wu et al. 2020), and 1 study each from Iran (Poureslami et al. 2013), Egypt (Khalifa et al. 2014), Thailand (Pattanaporn et al. 2013), Mexico (Wu et al. 2019), Turkey (Sahin et al. 2008), and Haiti (Reyes-Perez et al. 2014). Identifying these studies in such diverse countries creates new opportunities in oral health epidemiology. Collaborative work between these cohorts would allow investigations into the role of different environmental exposures related to oral diseases of children and adults and test the hypothesis of the interaction between genetic and environmental factors that contribute to the development of chronic noncommunicable diseases (Barker and Thornburg 2013). Early life exposures may act in different directions in high-income and emerging countries. For instance, while breastfeeding tends to be associated with high socioeconomic status in wealthy populations, the reverse is often the case in low- and middle-income countries, complicating important public health messages of the effects of breastfeeding on child oral health (Victora and Barros 2006).
Long-term cohorts reaching adulthood and presenting oral health data are scarce and found mostly in wealthy countries (Bishara et al. 1997; Pearce et al. 2005; Thomson et al. 2019; Wilson et al. 2019; Delgado-Angulo et al. 2020). The 1982 PBCS is considered an exception and was identified as the largest and longest birth cohort in a non-high-income country (Harpham et al. 2003). Limited research funds often cannot support more than 1 or 2 rounds of study. Moreover, as members of the cohort reach adulthood, the possibility of movement in search of employment increases, making it difficult to plan and conduct follow-up studies.
We found that caries at the cavitation level was the most common oral condition among these cohort studies. However, recognizing the epidemiological transition of the disease and the development of new tools have encouraged the adoption of new strategies for including the earliest stages of dental caries (Bell et al. 2019; Laajala et al. 2019). The positive side is that the standardized nature of these new instruments encourages comparability across different cohorts. Although OHRBCSs with periodontal data from adults are few, some explored social factors related to the periodontal diseases and demonstrated that proximal factors, such as dental plaque, use of dental services, and toothbrushing, were not sufficient to overcome the burden imposed by social factors experienced in early life (Peres et al. 2018; Schuch et al. 2019). On a similar note, studies exploring the relationship between periodontitis and systemic diseases suggest that instead of being causally related, these conditions are more likely to happen synchronously by sharing common risk factors. This finding calls into question the infectious role of periodontal diseases (Shearer et al. 2018; Leite et al. 2020). However, as periodontal diseases appear later in life, few cohorts were able to assess periodontal disease longitudinally (such as the Dunedin study), and most of the current evidence originates from cross-sectional assessments nested within birth cohorts.
Intervention Studies
Intervention studies, such as randomized controlled trials (RCTs) nested in OHRBCSs and RCTs followed up as a cohort study, were identified and described separately in this review. They are overrepresented within high-income countries (Kramer et al. 2009; Seow et al. 2009; Maupome et al. 2010; Broughton et al. 2013; Wagner and Heinrich-Weltzien 2017; Wagner et al. 2020); however, Brazil (Feldens et al. 2010; Chaffee, Vitolo, et al. 2014) and Uganda (Birungi et al. 2016) contributed toward expanding such studies to other parts of the world. These 2 forms of substudies can add value to the original research and encourage future longitudinal studies. When developing an RCT within an OHRBCS, there is a likelihood of significant cost savings in participants' enrollment and during follow-ups. Tracking the developmental of enamel defects and mutans streptococci colonization as risk factors for primary dental caries and evaluating the efficacy of different strategies for reducing the disease early in a child's life, for instance, were gains obtained when RCTs were nested in prospective cohort studies (Seow et al. 2009). Conversely, prospective observational studies were nested within RCTs in Brazil, taking advantage of many socioeconomic, environmental, and nutritional factors assessed throughout the trials (Feldens et al. 2010; Chaffee, Feldens, et al. 2014). Funding opportunities may increase as specific research questions are introduced during birth cohort studies, and the preexistence of structured research may increase new funders' confidence. The retention rate of participants can also be improved with such approaches, as positive RCT results can benefit everyone in the community. On the other hand, interventions may modify the cohort's external validity.
Data Linkage Studies
It was decided to exclude studies from the main analyses where birth cohorts were generated using national or district data registries. The decision was finely balanced, and it is worth considering reasons for this decision as data on health and health-related information are increasingly held electronically, and greater computing power is facilitating linkage between registries. In their favor are the following: 1) a large number of potential subjects are available (often the scope is national), 2) high proportions of the population may have been included in the registers, and 3) the data acquisition is inexpensive compared with face-to-face interviews. Disadvantages include 1) information relevant to the study may not have been collected or was excluded during anonymization, and 2) there are legal and ethical considerations about consent. Data linkage in OHRBCSs is prevalent in Japan and Scandinavia. For example, in Japan, Tanaka et al. (2015) related pregnancy and early life exposure to tobacco smoke to caries experience at 3 y in 76,920 children, controlling for maternal and child factors. In Sweden, Julihn et al. (2018) related pregnancy and early life experience to caries experience at ages 3 y and 7y in 65,259 children. In both examples, all data were retrieved from electronic registries. The legal and ethical constraints on linking regional or national data registries are being considered in many countries, for example, with the establishment of the Secure Anonymised Information Linkage Databank in the United Kingdom (Mourby et al. 2019) and the Swedish Data Inspection Board, which considers applications for data linkage research (Julihn et al. 2018).
Achievements
The achievements, challenges, and potential of OHRBCSs have been summarized (Peres et al. 2020). In addition, in this review, we identified remarkable achievements over the long history of OHRBCSs. First, more sophisticated data collection methods were incorporated over time: for instance, the understanding of early life predictors and causes was reinforced with the inclusion of more advanced methods, for example, analysis of genetic material and microbiome. In addition, these are likely to minimize misclassification of outcomes, therefore increasing confidence in resulting interventions. Extracting DNA from saliva samples and storing it in biobanks will allow for future genome-wide and full-genome analysis as well as epigenetic studies of some cohorts or the combination of them. We believe that the oldest cohorts' experiences helped improve data collection and change current paradigms of understanding oral diseases. Second, there was an increase in retention rate. While, on the one hand, physical access to cohort members has become more complex, on the other hand, new technologies such as social media and mobile phones make it easier to find and contact them.
Despite the fact that we did not restrict the outcomes to any life stage, it was noticeable that childhood outcomes were more predominant because many cohorts are not yet mature enough to address longer-term outcomes. However, some very longstanding birth cohorts are now following offspring well into adulthood and the later years of life.
Limitations
We may not have captured all relevant articles due to the search strategy and date of the last search. Our inclusion criteria did not distinguish between pregnancy cohorts and birth cohorts, although there may be differences in uptake and information recall between them. We also did not restrict the oral health outcomes to any life stage, widening the information recorded in studies, so that it was suitable for a scoping approach rather than a systematic review. As some identified cohorts had ongoing follow-ups when writing this article, some information might have been missed. Cohorts of pregnant women that investigated mothers' oral health and perinatal outcomes, rather than the oral health of their offspring, were excluded but are relatively numerous. The strategy to incorporate oral health assessments in a birth cohort study starting during pregnancy and linking these to their descendants' data is not new in high-income countries. Most recently, young birth cohorts found worldwide have the potential to contribute to intergenerational analyses on aspects of oral health. Indeed, OHRBCSs face different challenges and barriers when moving across generations; however, this topic deserves a specific review. Finally, our review included only studies published in English, and this might have led to publication bias—the diverse geographical locations of the studies obliged us to restrict the study language.
Final Considerations
Birth cohort studies vary in size and scope, but each can contribute much to knowledge. Large cohorts can target rare and chronic diseases, but they need high levels of research funding. Alternatively, well-designed small cohorts investigating novel hypotheses may contribute to new discoveries. The OHRBCSs included in this review revealed significant heterogeneity regarding the investigated exposures. As expected, basic socioeconomic classification, ethnicity, questionnaire definitions, and country- or language-specific assessment tools varied across countries. Also, there was a variation in the level of representativeness of the cohorts. Although challenging, the difficulties these differences create can be overcome by combining, where possible, and harmonizing different cohorts’ data to establish future joint projects, adding considerable strength by combined data analyses.
Ultimately, birth cohort studies want to identify early life predictors and causes to inform early interventions to prevent the incidence of poor health and the most appropriate stages in life to intervene. Identifying relevant quality data registries, such as from hospital and health services, and using data linkage is an important strategy for the future. In addition, when designing a new OHRBCS, the insertion of oral health into existing general birth cohorts may be an economic and sensible choice since a diversity of social, biological, behavioral, and general clinical data is likely to be available.
Successful examples of small and large consortia of principal investigators in diverse areas (Richter et al. 2012; Di Credico et al. 2020) can inspire the researchers involved in OHRBCSs, both presently and in the future. Since oral conditions are relatively prevalent, the need for large numbers when studying moderate to weak associations with potential risk and protective factors or common genetic variants studies could be overcome by adopting the strategy of a consortium that would involve some standardization of methods and joint analysis of pooled data. Additional effort to create a standardized reporting database for the OHRBCS registry, following the example of RCTs, would facilitate access to these studies.
This study identified potential members for the formation of an OHRBCS consortium. Efforts will be made to build an OHRBCS consortium as an inclusive process, ensuring a flexible commitment to occasional participation. Small funds to kickstart establishing the initial infrastructure and a data management center have been already obtained. The hub of the global dissemination will be a joint initiative between the National Dental Research Institute Singapore and SingHealth Duke–NUS Global Health Institute Singapore. Bearing in mind the high costs and long-term follow-up periods of cohort studies, this consortium and pooled data will especially benefit middle/low-income countries. This initiative may further support relevant activities through direct and indirect funding. The OHRBCS consortium will be launched in 2022 to bring together the experiences of more longstanding studies with newly established cohorts to consider a joint research agenda. An executive committee has been created to stimulate potential members to discuss guidelines that include ethical considerations and authorship in combined data analysis and subsequent joint publications. This initiative should provide a rich source of valuable oral health data to be efficiently explored.
Author Contributions
K.G. Peres, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; G.G. Nascimento, contributed to design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; A. Gupta, L. Schertel Cassiano, contributed to design, data acquisition, and analysis, drafted and critically revised the manuscript; A. Singh, contributed to conception and acquisition, drafted and critically revised the manuscript; A.J. Rugg-Gunn, contributed to conception, design, data analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
Supplemental material, sj-docx-1-jdr-10.1177_00220345211062475 for Scoping Review of Oral Health-Related Birth Cohort Studies: Toward a Global Consortium by K.G. Peres, G.G. Nascimento, A. Gupta, A. Singh, L. Schertel Cassiano and A.J. Rugg-Gunn in Journal of Dental Research
Acknowledgments
We thank Dr. Dandara Haag for the artistic creation of the map with the cohort countries.
Footnotes
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by the Borrow Foundation (K.G. Peres).
ORCID iDs: K.G. Peres  https://orcid.org/0000-0002-1730-2123
https://orcid.org/0000-0002-1730-2123
A. Singh
https://orcid.org/0000-0003-1336-6493
A.J. Rugg-Gunn
https://orcid.org/0000-0001-7495-1894
References
- Araujo WRM, Santos IS, Menezes Filho NA, Souza M, Cunha A, Matijasevich A. 2020. Brazilian cohorts with potential for life-course studies: a scoping review. Rev Saude Publica. 54:48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arksey H, O’Malley L. 2005. Scoping studies: towards a methodological framework. Int J Soc Res Methodol Theory Pract. 8(1):19–32. [Google Scholar]
- Barker DJ, Thornburg KL. 2013. Placental programming of chronic diseases, cancer and lifespan: a review. Placenta. 34(10):841–845. [DOI] [PubMed] [Google Scholar]
- Bell LK, Schammer C, Devenish G, Ha D, Thomson WM, Spencer JA, Do LG, Scott JA, Golley RK. 2019. Dietary patterns and risk of obesity and early childhood caries in Australian toddlers: findings from an Australian cohort study. Nutrients. 11(11):2828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birungi N, Fadnes LT, Nankabirwa V, Tumwine JK, Astrom AN. 2016. Caretaker’s caries experience and its association with early childhood caries and children’s oral health-related quality of life: a prospective two-gen eration study. Acta Odontol Scand. 74(8):605–612. [DOI] [PubMed] [Google Scholar]
- Bishara SE, Jakobsen JR, Treder J, Nowak A. 1997. Arch width changes from 6 weeks to 45 years of age. Am J Orthod Dentofacial Orthop. 111(4):401–409. [DOI] [PubMed] [Google Scholar]
- Broughton JR, Maipi JT, Person M, Thomson WM, Morgaine KC, Tiakiwai SJ, Kilgour J, Berryman K, Lawrence HP, Jamieson LM. 2013. Reducing disease burden and health inequalities arising from chronic disease among indigenous children: an early childhood caries intervention in Aotearoa/New Zealand. BMC Public Health. 13:1177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Camargo MB, Barros AJ, Frazao P, Matijasevich A, Santos IS, Peres MA, Peres KG. 2012. Predictors of dental visits for routine check-ups and for the resolution of problems among preschool children. Rev Saude Publica. 46(1):87–97. [DOI] [PubMed] [Google Scholar]
- Campos M, Valenca PAM, Silva GMD, Lima MC, Jamelli SR, Goes PSA. 2018. Influence of head and linear growth on the development of malocclusion at six years of age: a cohort study. Braz Oral Res. 32:e98. [DOI] [PubMed] [Google Scholar]
- Chaffee BW, Feldens CA, Vitolo MR. 2014. Association of long-duration breastfeeding and dental caries estimated with marginal structural models. Ann Epidemiol. 24(6):448–454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chaffee BW, Vitolo MR, Feldens CA. 2014. The Porto Alegre early life nutrition and health study. Rev Bras Epidemiol. 17(4):1015–1018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper C, Frank J, Leyland A, Hardy R, Lawlor DA, Wareham NJ, Dezateux C, Inskip H. 2012. Using cohort studies in lifecourse epidemiology. Public Health. 126(3):190–192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crall JJ, Forrest CB. 2018. A life course health development perspective on oral health. In: Halfon N, Forrest CB, Lerner RM, Faustman EM, editors. Handbook of life course health development. Cham (Switzerland): Springer. p. 299–320. [PubMed] [Google Scholar]
- Delgado-Angulo EK, Alshehri R, Scambler S, Bernabe E. 2020. Is grandparents’ social class associated with adult grandchildren’s oral health? Analysis of two British cohorts. Community Dent Oral Epidemiol. 48(5):402–408. [DOI] [PubMed] [Google Scholar]
- Di Credico G, Polesel J, Dal Maso L, Pauli F, Torelli N, Luce D, Radoi L, Matsuo K, Serraino D, Brennan P, et al. 2020. Alcohol drinking and head and neck cancer risk: the joint effect of intensity and duration. Br J Cancer. 123(9):1456–1463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Economic Department and Social Affairs. 2020. Country classifications. World Economic Situation and Prospects 2020. United Nations [accessed 2021 Aug 11]. https://www.un.org/development/desa/dpad/wp-content/uploads/sites/45/WESP2020_Annex.pdf.
- Feldens CA, Giugliani ER, Duncan BB, de Lourdes Drachler M, Vitolo MR. 2010. Long-term effectiveness of a nutritional program in reducing early childhood caries: a randomized trial. Community Dent Oral Epidemiol. 38(4):324–332. [DOI] [PubMed] [Google Scholar]
- Grimes DA, Schulz KF. 2002. Cohort studies: marching towards outcomes. Lancet. 359(9303):341–345. [DOI] [PubMed] [Google Scholar]
- Guedes KM, Guimaraes AM, de Souza Bastos A, Salviano KG, Sales NJ, Almeida ML, Gurgel RQ. 2015. Stomatognathic evaluation at five years of age in children born premature and at term. BMC Pediatr. 15:27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ha DH, Spencer AJ, Peres KG, Rugg-Gunn AJ, Scott JA, Do LG. 2019. Fluoridated water modifies the effect of breastfeeding on dental caries.J Dent Res. 98(7):755–762. [DOI] [PubMed] [Google Scholar]
- Harpham T, Huttly S, Wilson I, De Wet T. 2003. Linking public issues with private troubles: panel studies in developing countries. J Int Dev. 15(3):353–363. [Google Scholar]
- Julihn A, Soares FC, Hjern A, Dahllof G. 2018. Socioeconomic determinants, maternal health, and caries in young children. JDR Clin Trans Res. 3(4):395–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khalifa AM, El Gendy RA, El-Mohsen MMA, Hammour AA, Aly RSAEL. 2014. Relationship between gestational age, birth weight and deciduous tooth eruption. Egypt Pediatr Assoc Gaz. 62(2):41–45. [Google Scholar]
- Kramer MS, Matush L, Bogdanovich N, Aboud F, Mazer B, Fombonne E, Collet JP, Hodnett E, Mironova E, Igumnov S, et al. 2009. Health and development outcomes in 6.5-y-old children breastfed exclusively for 3 or 6 mo. Am J Clin Nutr. 90(4):1070–1074. [DOI] [PubMed] [Google Scholar]
- Laajala A, Pesonen P, Anttonen V, Laitala ML. 2019. Association of enamel caries lesions with oral hygiene and DMFT among adults. Caries Res. 53(4):475–481. [DOI] [PubMed] [Google Scholar]
- Lawlor DA, Andersen AM, Batty GD. 2009. Birth cohort studies: past, present and future. Int J Epidemiol. 38(4):897–902. [DOI] [PubMed] [Google Scholar]
- Leite FRM, Nascimento GG, Peres KG, Demarco FF, Horta BL, Peres MA. 2020. Collider bias in the association of periodontitis and carotid intima-media thickness. Community Dent Oral Epidemiol. 48(4):264–270. [DOI] [PubMed] [Google Scholar]
- MacKeown JM, Cleaton-Jones PE, Edwards AW. 2000. Energy and macronutrient intake in relation to dental caries incidence in urban black South African preschool children in 1991 and 1995: the birth-to-ten study. Public Health Nutr. 3(3):313–319. [DOI] [PubMed] [Google Scholar]
- Massoni AC, Chaves AM, Rosenblatt A, Sampaio FC, Oliveira AF. 2009. Prevalence of enamel defects related to pre-, peri- and postnatal factors in a Brazilian population. Community Dent Health. 26(3):143–149. [PubMed] [Google Scholar]
- Maupome G, Karanja N, Ritenbaugh C, Lutz T, Aickin M, Becker T. 2010. Dental caries in American Indian toddlers after a community-based beverage intervention. Ethn Dis. 20(4):444–450. [PMC free article] [PubMed] [Google Scholar]
- Mourby M, Gowans H, Aidinlis S, Smith H, Kaye J. 2019. Governance of academic research data under the GDPR—lessons from the UK. Int Data Priv Law. 9(3):192–206. [Google Scholar]
- Nascimento GG, Peres MA, Mittinty MN, Peres KG, Do LG, Horta BL, Gigante DP, Correa MB, Demarco FF. 2017. Diet-induced overweight and obesity and periodontitis risk: an application of the parametric G-formula in the 1982 Pelotas Birth Cohort. Am J Epidemiol. 185(6):442–451. [DOI] [PubMed] [Google Scholar]
- Pattanaporn K, Saraithong P, Khongkhunthian S, Aleksejuniene J, Laohapensang P, Chhun N, Chen Z, Li Y. 2013. Mode of delivery, mutans streptococci colonization, and early childhood caries in three- to five-year-old Thai children. Community Dent Oral Epidemiol. 41(3):212–223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearce MS, Steele JG, Campbell DI, Thomas JE. 2005. Tooth loss and Helicobacter pylori seropositivity: the Newcastle Thousand Families Cohort Study at age 49–51 years. Helicobacter. 10(1):90–94. [DOI] [PubMed] [Google Scholar]
- Peres KG, Nascimento GG, Peres MA, Mittinty MN, Demarco FF, Santos IS, Matijasevich A, Barros AJD. 2017. Impact of prolonged breastfeeding on dental caries: a population-based birth cohort study. Pediatrics. 140(1):e20162943. [DOI] [PubMed] [Google Scholar]
- Peres KG, Peres MA, Demarco FF, Tarquinio SB, Horta BL, Gigante DP. 2011. Oral health studies in the 1982 Pelotas (Brazil) birth cohort: methodology and principal results at 15 and 24 years of age. Cad Saude Publica. 27(8):1569–1580. [DOI] [PubMed] [Google Scholar]
- Peres KG, Thomson WM, Chaffee BW, Peres MA, Birungi N, Do LG, Feldens CA, Fontana M, Marshall TA, Pitiphat W, et al. 2020. Oral health birth cohort studies: achievements, challenges, and potential. J Dent Res. 99(12):1321–1331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peres MA, Nascimento GG, Peres KG, Demarco FF, Menezes AB. 2018. Oral health-related behaviours do not mediate the effect of maternal education on adolescents’ gingival bleeding: a birth cohort study. Community Dent Oral Epidemiol. 46(2):169–177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peres MA, Peres KG, Thomson WM, Broadbent JM, Gigante DP, Horta BL. 2011. The influence of family income trajectories from birth to adulthood on adult oral health: findings from the 1982 Pelotas Birth Cohort. Am J Public Health. 101(4):730–736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinho JRO, Thomaz E, Ribeiro CCC, Alves CMC, Silva A. 2019. Factors associated with the development of dental defects acquired in the extrauterine environment. Braz Oral Res. 33:e094. [DOI] [PubMed] [Google Scholar]
- Poureslami H, Bafti LS, Hashemi Z, Salari Z. 2013. Comparison of occurrence of early childhood caries in two groups of children delivered by cesarean section and normal birth: a longitudinal study. J Compr Pediatr. 4(1):76–81. [Google Scholar]
- Reyes-Perez E, Borrell LN, Katz RV, Gebrian BJ, Prophete S, Psoter WJ. 2014. Effect of early childhood protein-energy malnutrition on permanent dentition dental caries. J Public Health Dent. 74(3):181–187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richter LM, Victora CG, Hallal PC, Adair LS, Bhargava SK, Fall CH, Lee N, Martorell R, Norris SA, Sachdev HS, et al. 2012. Cohort profile: the consortium of health-orientated research in transitioning societies. Int J Epidemiol. 41(3):621–626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sahin F, Camurdan AD, Camurdan MO, Olmez A, Oznurhan F, Beyazova U. 2008. Factors affecting the timing of teething in healthy Turkish infants: a prospective cohort study. Int J Paediatr Dent. 18(4):262–266. [DOI] [PubMed] [Google Scholar]
- Schuch HS, Nascimento GG, Peres KG, Mittinty MN, Demarco FF, Correa MB, Gigante DP, Horta BL, Peres MA, Do LG. 2019. The controlled direct effect of early-life socioeconomic position on periodontitis in a birth cohort. Am J Epidemiol. 188(6):1101–1108. [DOI] [PubMed] [Google Scholar]
- Seow WK, Lam JH, Tsang AK, Holcombe T, Bird PS. 2009. Oral streptococcus species in pre-term and full-term children—a longitudinal study. Int J Paediatr Dent. 19(6):406–411. [DOI] [PubMed] [Google Scholar]
- Shearer DM, Thomson WM, Cameron CM, Ramrakha S, Wilson G, Wong TY, Williams MJA, McLean R, Theodore R, Poulton R. 2018. Periodontitis and multiple markers of cardiometabolic risk in the fourth decade: a cohort study. Community Dent Oral Epidemiol. 46(6):615–623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun L. 2020. The association between postpartum depression and early childhood caries. Acta Odontol Scand. 78(5):352–357. [DOI] [PubMed] [Google Scholar]
- Tanaka S, Shinzawa M, Tokumasu H, Seto K, Tanaka S, Kawakami K. 2015. Secondhand smoke and incidence of dental caries in deciduous teeth among children in Japan: population based retrospective cohort study. BMJ. 351:h5397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomson WM, Broadbent JM, Caspi A, Poulton R, Moffitt TE. 2019. Childhood IQ predicts age-38 oral disease experience and service-use. Community Dent Oral Epidemiol. 47(3):252–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Victora CG, Barros FC. 2006. Cohort profile: the 1982 Pelotas (Brazil) Birth Cohort Study. Int J Epidemiol. 35(2):237–242. [DOI] [PubMed] [Google Scholar]
- Wagner Y, Heinrich-Weltzien R. 2017. Evaluation of a regional German interdisciplinary oral health programme for children from birth to 5 years of age. Clin Oral Investig. 21(1):225–235. [DOI] [PubMed] [Google Scholar]
- Wagner Y, Knaup I, Knaup TJ, Jacobs C, Wolf M. 2020. Influence of a programme for prevention of early childhood caries on early orthodontic treatment needs. Clin Oral Investig. 24(12):4313–4324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson R, Kuh D, Stafford M. 2019. Variations of health check attendance in later life: results from a British birth cohort study. BMC Public Health. 19(1):1518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winn DM, Lee YC, Hashibe M, Boffetta P; INHANCE consortium. 2015. The INHANCE consortium: toward a better understanding of the causes and mechanisms of head and neck cancer. Oral Dis. 21(6):685–693. [DOI] [PubMed] [Google Scholar]
- World Bank. New World Bank country classifications by income level: 2020-2021. [accessed 2021 Aug 11]. https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2020-2021.
- Wu H, Xu B, Guan Y, Chen T, Huang R, Zhang T, Sun R, Xie K, Chen M. 2020. A metabolomic study on the association of exposure to heavy metals in the first trimester with primary tooth eruption. Sci Total Environ. 723:138107. [DOI] [PubMed] [Google Scholar]
- Wu Y, Jansen EC, Peterson KE, Foxman B, Goodrich JM, Hu H, Solano-Gonzalez M, Cantoral A, Tellez-Rojo MM, Martinez-Mier EA. 2019. The associations between lead exposure at multiple sensitive life periods and dental caries risks in permanent teeth. Sci Total Environ. 654:1048–1055. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-1-jdr-10.1177_00220345211062475 for Scoping Review of Oral Health-Related Birth Cohort Studies: Toward a Global Consortium by K.G. Peres, G.G. Nascimento, A. Gupta, A. Singh, L. Schertel Cassiano and A.J. Rugg-Gunn in Journal of Dental Research