

Abstract
Eating disorders (EDs) constitute a mental illness with the highest mortality. Today, mobile health apps provide promising means to ED patients for managing their condition. Apps enable users to monitor their eating habits, thoughts, and feelings, and offer analytic insights for behavior change. However, not only have scholars critiqued the clinical validity of these apps, their underlying design principles are not well understood. Through a review of 34 ED apps, we uncovered 11 different data types ED apps collect, and 9 strategies they employ to support collection and reflection. Drawing upon personal health informatics and visualization frameworks, we found that most apps did not adhere to best practices on what and how data should be collected from and reflected to users, or how data-driven insights should be communicated. Our review offers suggestions for improving the design of ED apps such that they can be useful and meaningful in ED recovery.
Keywords: eating disorder, self-tracking, apps, reflection
1. INTRODUCTION
Eating disorders (EDs) present an important public health problem in terms of cost, prevalence, and morbidity, and constitute a mental illness with the highest mortality [110]. Approximately 13% of young women and 6% of adults suffer from a diagnosable ED in their lifetime [110]. Although evidence-based clinical practice guidelines for effective therapy exist [70], only a small proportion of affected individuals seek and receive these treatments. Many challenges impair access to ED treatments, including insufficient numbers of clinicians adequately trained in evidence-based approaches [68], shame and stigma associated with EDs [61], fear of losing control [24], geographical constraints, and the economic costs of face-to-face treatment [37]. Consequently, for most ED patients, treatment is episodic, intermittent, taking place outside of a formal clinical setting, or remain self-managed for life [68].
In recent years, the increasingly pervasive use of mobile devices and smartphones has begun to redefine how mental illnesses, such as EDs, are managed [29]. Examples include how these devices empower individuals to take charge of their health challenges, how individuals find adjuvant pathways to care and help [67], and how they may serve as “non-dominant treatment models,” as argued by Kazdin et al. and others [22, 74, 76]. With 6% apps in Apple’s and Google’s app stores targeting mental health outcomes [53], scholars have further argued that mobile health (mHealth) applications (apps) may serve as a “digital lifeline” [27], “putting a portable therapist in every pocket” [34], and even serve as “a way [for] people getting access to treatment that’s flexible and fits in with their lifestyle and also deals with the issues around stigma – if people are not quite ready to maybe go and see their doctor” [27]. Essentially, such apps are argued to enable patients to approach treatment at an individualized pace, making treatment more accessible and reducing barriers and shame experienced in seeking in-person treatment [22, 74, 115].
Importantly, a key goal of these apps is to encourage users’ behavior change and enable reflection on personal health data (mood, exercise, physical activities, self-perceptions, etc.) [60, 82]. For EDs, in particular, these apps have been argued to be especially beneficial – because these disorders involve specific behaviors, like binge eating and purging, that must be regularly self-monitored in terms of frequency and intensity [115]. Consequently, a variety of mHealth apps are known to enable individuals to monitor their eating habits (e.g., meal portion size), as well as thoughts and feelings over time [115]. Some apps go further to obtain data-driven insights from the collected data and communicate such insights to users in the hopes of supporting reflection and behavior change [30].
Over the years, digital mental health scholars have sought to understand the usability of and users’ engagement with mental health apps; the extent to which these apps support delivering clinical interventions, such as cognitive behavioral therapy (CBT); whether these data and insights are valid, accurate, reliable; and if users feel satisfied [39, 53, 114]. However, current understanding of the design principles behind the functioning of these apps, from a user-centered perspective, is lacking. At the crux of the functionality of these apps is that they collect a variety of data from users, glean insights from these data using design and computational techniques [115], and then communicate these insights back to the users, to enable them to review those insights as a way of self-monitoring and self-tracking [62, 74]. Investigations of the design principles behind these functionalities are critical because patients with mental illness are often sensitive to personal health information collected and shown by apps [97]. Poor design also leads to poor adherence, with most end users stopping using an app two weeks after download [113]. For ED patients, in particular, placing attention on one’s eating or weight may trigger symptoms, relapses, and even denial of one’s condition [87]. Additionally, reviews of mental health apps reveal that a large amount of information provided by these apps was not only clinically unverified or grounded, but also can exacerbate an individual’s condition, instead of helping alleviate symptoms [102].
Beyond understanding their clinical efficacy, as has been the focus of existing research [39, 92], there is a burgeoning need to understand if ED apps collect, communicate, and support reflection on information effectively and safely. In particular: What information do existing ED apps collect from users? After collecting such information over a specific period, how do these ED apps convey data-driven insights to the users for self-reflection? What design principles do these apps use to collect, communicate, or support reflection on such information? What are the advantages and disadvantages of these design principles? Understanding the state-of-the-art approaches used in these apps to collect, communicate, and support reflection on data is invaluable for a number of reasons. First, it can ensure that these apps are useful to the individuals relying on them for managing their ED, whether in concert with their clinicians and caregivers or by themselves. And second, it can help align the apps with the preferences and goals of the intended users, in a way that fits into the fabric of a person’s life.
Using a theory-driven approach with frameworks grounded in the eating disorder, personal health informatics, and information visualization literatures, we review 34 ED-related apps (i) to identify and categorize different types of information they collect from or communicate back to users, and (ii) to extract different strategies these apps use for collecting, communicating, and supporting reflection on information. We find that despite the host of available apps to self-manage ED, the apps rarely adhere to the clinical complexities of the condition from the perspective of cognitive-behavioral treatments, and do not necessarily use the guidelines to make personal health data collection and reflection efficacious and meaningful to the end-user. With this review, we establish an understanding of the current landscape of ED apps, uncover which methods of data collection, reflection, and communication align with the best practices in ED treatment, and examine the extent to which the apps provide a suitable medium for communicating insights and facilitating user reflection. We conclude by suggesting areas of improvement that designers can take to improve the ED apps’ functioning and efficacy to ensure they serve as useful supports to managing their condition.
2. BACKGROUND AND RELATED WORK
2.1. Eating Disorders and the Role of Technology in Addressing EDs
Eating disorders are psychiatric disorders that demonstrate severe disturbances related to the behavior and perception of one’s eating habits, obsession, and overvaluation of body weight and shape [22]. Among the category of eating disorders, there are several primary diagnoses with different clinical features, as mentioned in the DSM-5. Anorexia Nervosa (AN) involves restricting energy intake and maintaining a significantly low body weight relative to what is normal, intense fear of gaining weight or becoming fat even when underweight, and distorted body image or denial of current low body weight [21]. Bulimia Nervosa (BN) is characterized by a cycle of binge eating and behaviors to prevent weight gain and compensate for binge eating, such as self-induced vomiting or misusing laxatives. Binge eating is defined as eating abnormal amounts of food in a short window (2 hours) and involves a lack of control regarding eating [21]. Binge Eating Disorder (BED) is similar to BN, as it also includes binging episodes and a lack of control over eating. However, the recurrent use of harmful compensatory behaviors such as vomiting is not necessarily present. Binge eating episodes are usually associated with eating until uncomfortably full, feeling disgusted or depressed after eating, or eating large amounts of food when not physically hungry [21]. Finally, OSFED (Other Specified Feeding or Eating Disorder) is a diagnosis that encompasses individuals who do not meet strict criteria for anorexia or bulimia but still have a significant eating disorder [21]. EDs present a critical public health problem because of their commonality and the strong effect in diminishing one’s quality of life. This condition affects one in eight women and 13% of adolescent females [110]. EDs are also intense, yet the process of seeking treatment is complicated, as the illness frequently goes undetected, and individuals suffering from an eating disorder delay treatment or remain unaware that they even suffer from it. ED sufferers may often feel shame or stigma from seeking treatment or find a lack of available and affordable resources hinder their ability to seek care [22].
Internet-based approaches to ED interventions are emerging because such technologies are widely available and accessible. Such methods can provide anonymous treatment, reach a broader audience, provide flexibility and personalization in treatment courses, and reduce the need for trained staff to administer help [88]. Bauer and Moessner note that technological interventions can aid in all stages of an ED, from early interventions to preventing relapses and maintaining support after treatment [30]. People with EDs may especially benefit from mobile app therapy because EDs feature frequent and specific symptoms (such as binge eating or purging) that need regular monitoring [115]. In the HCI field, in particular, recent literature has examined the role of social media and online communities in supporting individuals with ED, including enabling self-disclosure to fight stigma and shame [38, 51, 93], facilitating identity work [63, 118], providing social support [41], and augmenting recovery processes [42].
A large body of literature has worked to understand the effectiveness of online ED treatment approaches compared to traditional, face-to-face therapy. Student Bodies is an eight week structured online CBT program targeted towards college-aged women at risk for developing an ED. It was found to decrease the onset of clinical (symptoms were recognizable) and subclinical (symptoms were not identifiable) EDs [30]. Additionally, many apps are aimed to support ED emergence. Recovery Record is an ED app based on CBT and self-monitoring research. It allows users to self-monitor meals, emotions, behaviors, and thoughts, and also includes positive reinforcement, coping mechanisms, and social and clinical support to aid in treatment [115]. The app currently has over 100,000 users and reaches individuals who are not engaged in treatment, acting as a supplement to traditional therapy [115]. However, there is a concern that such apps are replacing or interfering with ED therapy altogether when that is not the intention [74].
As shown with the above examples, using technology for ED treatment has beneficial implications. However, a rigorous evaluation of such technology-enhanced interventions and an examination of the level of the guidance necessary that may be useful to users is needed. [30, 47]. As more ED apps emerge, their utility needs to be assessed from the users’ perspective to ensure they are providing legitimate information and that the users can gain value.
2.2. Understanding the Role of Apps in Mental Health and ED
Many technological approaches exist today to manage mental illnesses. Mobile phones are a promising medium for providing access to support and care for ED patients due to the increased access to mobile devices and the use of such technology interwoven in our lives [103]. Mental health is a popular application for smartphones, as mobile mHealth has been argued to be able to reach a broader audience to provide diagnosis, self-monitoring, and treatment to individuals who lack the means for face-to-face therapy [103]. In particular, in the last five years, many apps designed for ED patients have emerged, addressing coping strategies, managing harmful symptoms, general information, and more [103]. However, with the proliferation of these apps, it is critical to evaluate if they provide consistent, sound advice or care to their intended audience [36, 89].
Given the proliferation of such apps for mental health in general and EDs in particular, researchers have been interested in identifying and characterizing the factors relating to adoption, persistent use, and abandonment, and evaluate their clinical utility, efficacy in delivering interventions, and the extent to which they can support CBT based treatment [40, 53, 69, 90]. In an early pioneering work, Chan et al. provided a framework to evaluate mental health apps [39]. They developed a 3-dimensional framework (usefulness, usability, and usage), each with several subcategories and questions for patients and providers to ask about apps. They also provided seven categories (education, reference, historical data, physical data, diagnosis, treatment/intervention, and patient-provider communication) that cover potential applications and use cases of such technology. Guided by this framework, this paper argued that a lack of standardized evaluation and rating tools has prevented clinicians and patients in identifying high-quality and safe mobile apps. Along similar lines, Powell et al. compiled 22 metrics of evaluating apps for depression and smoking and found low interrater reliability for effectiveness and ease of use, citing that some evaluation benchmarks are more ambiguous than others [96]. Currently, the One Mind PsyberGuide [92] serves as a widely adopted benchmark to assess the quality of digital mental health products to empower users in making informed choices about these resources; also see Bakker et al. [29] who provide evidence-based recommendations and Torous et al. [112] who develop standards for evaluating mental health apps. Other work has focused on categorizing existing mental health apps and understanding their purpose. A study by Shen et al. characterized mobile phone depression apps on major app stores and found a ratio of 3:1 for nonspecific depression apps to specific depression apps [103]. A majority of apps failed to mention their organizational affiliations and sources [103]. Many apps were meant for treatment and education, so such statistics raise questions about the apps’ credibility. Further, a lack of standardized categorization makes it difficult to find reliable apps [103].
Some researchers have also sought to understand the attitudes of individuals towards smartphone-delivered therapies versus traditional face-to-face therapy [22, 30, 62, 74, 104]. Users and clinicians alike remain concerned about most apps’ privacy and security features [95], their (lack of) transparency [23], and ethics [52]. A prominent takeaway from this research has been that most mental health including ED apps are not clinically grounded, verified, or vetted; therefore not only are their therapeutic effects a suspect, but they can also exacerbate an individual’s condition, instead of helping alleviate significant symptoms [102]. Eating disorders make up a subset of mental disorders, and the number of apps targeting people with ED and ED professionals is also rising, including the appropriation of more general-purpose health apps for ED needs [56, 58]. Fairburn and Rothwell conducted a review of ED apps and found that most were for providing advice, but the information ranged from sound to harmful [62]. These authors, therefore, recommended that such apps need more investigation regarding their clinical utility. Clinicians should be aware of such apps and ask their patients about them, and leading eating disorder organizations should publish a standard list of the best ED apps [62]. Along similar lines, Eikey examined provider perspectives on ED apps [55] and how users negotiate their social connectivity needs with privacy concerns [54].
The growing numbers of apps create a need for standardized evaluation criteria to help patients and clinicians identify the best apps that can meet their needs and provide sound advice and care. Although previous reviews have been conducted, our study is unique in categorizing and evaluating the effectiveness of information being collected from and presented back to individuals with ED. Assessing such criteria from a design perspective can shine a light on the practices apps employ to inform users to then identify opportunities to increase their effectiveness.
3. RELEVANT THEORETICAL FRAMEWORKS
To examine the theoretical basis of ED apps, we draw from two different domains – personal health informatics, including conceptualizations of the process of reflection, and information visualization, outlining several best practices surrounding communicating data to end-users.
First, prior frameworks of usage and behavior change in personal informatics exist to formalize user motivations, behavior changes, and any challenges of using personal informatics apps. We extend this knowledge to understand the behavior and journey of individuals with ED when using such apps, what needs they see these apps fulfilling, and the challenges of usage that arise. Additionally, such insight can help uncover what causes people to decline usage and how personal informatics app creators can mitigate those effects and create valuable ways to display personal data.
Several frameworks formalize the journey users undergo when using personal informatics technologies. Epstein et al. [60] introduce a model that captures the motivations to decide and begin tracking, integrating data (tracking and acting), and reasons for lapsing tracking. For our research here involving a review of ED apps, we focus on three stages present in the tracking and acting phase: collection, integration, and reflection, to categorize the information found in ED apps and understand how individuals use them to find insights. Collection and reflection are fundamental processes for interacting with personal informatics apps, but unlike collection, reflection is a concept defined in various ways [64]. Understanding what is meant by the term reflection is important for categorizing and understanding how the reviewed ED apps incorporate reflection in designs. A large body of literature from various domains has worked to define reflection as a topic and how to best design technologies to support reflection [31, 60, 64, 101, 105]. We discuss some of these approaches below.
Epstein et al. mention reflection as a process that occurs alongside a collection to check on the information users have entered [60]. Along similar lines, Baumer notes three fundamental concepts in the process of reflection in personal informatics that illuminate how designs can support reflection: 1) breakdown (of expectations), 2) inquiry 3) transformation (inspiring some change) [31]. Fleck and Fitzpatrick posit reflection as a multi-level process: Description (revisiting), Reflective Description (revisiting with explanation), Dialogic Reflection (exploring relationships), Transformative Reflection (fundamental change), Critical Reflection (wider implications) [64]. Each level continues from the previous one, and each layer provides a progressively deeper understanding of data [64]. Drawing on “reflective practicum” from Schön [101], Slovák et al. emphasize the importance of scaffolding the reflective process, i.e., helping people learn how to reflect [105]. Although many frameworks exist for reflection as a process, many similarities are present. The examples mentioned above show reflection as a process that gives meaningful interactions with data to provide change. In our review of ED apps, we draw on these frameworks of reflection.
Next, a core focus of this review paper is to understand how ED apps communicate information to their end-users, as a way to support the reflective process. An appropriate visual representation of data can make it easier to aggregate large amounts of data and pinpoint specific values of interest [48]. Visualizing collected data aids in the process of reflection by enabling users to review their activities in both high-level and granular ways [48]. Because ED personal informatics apps involve synthesizing a large amount of data collection and providing tailored feedback, we draw upon the information visualization (infovis) literature to obtain guidelines and strategies for evaluating the effectiveness of the data communication methods shown by the ED apps.
In particular, we engage with prior research on topics such as ranking and determining the effectiveness of different types of visualizations [83, 100, 107], providing design implications and pairings for data types and visualizations [80, 98], and capturing the relationship between people’s activities and information goals when viewing a visualization [26, 80, 100]. Other work in information visualization has focused on categorizing visualizations’ capabilities and providing guidelines to designers to understand their effectiveness. Amar et al. introduce a framework of 10 analysis tasks (retrieve value, filter, compute derived value, sort, etc.) that explain the standard methods for how people understand data with visualizations. These tasks explain the current advantages and limitations of visualizations and introduce a common language that can describe visualization capabilities [26]. Kim and Heer similarly tested a framework with two broad task categories: value tasks (reading and comparing individual values) and summary task (finding the maximum value, comparing averages) [80]. Sarikaya and Gleicher propose a different 12-task framework for scatterplots, specifically, from object-centric browsing, to aggregate tasks [100].
There has also been research that seeks to recommend the appropriate types of visualizations for specific analysis tasks. Mackinlay introduced an automatic recommendation system for visualizations with two criteria: effectiveness and expressiveness, and critiqued visualizations’ design decisions. A visualization is potentially expressive if it can display all its assigned information over time. It is potentially effective if it can express information in a way that does not exploit a human’s visual system [83]. Kim and Heer explore the effect of visualization tasks and design attributes (color, size, and orientation) to find suitable pairings between tasks and visualization design [80]. Their study involved a controlled experiment that validated Mackinlay’s ranking scheme, and it proposed design recommendations considering color, size, and orientation for different visualization types [80]. Additionally, Saket et al. studied users’ performance and preferences when dealing with visualization methods for a selected number of tasks [98]. Spence and Lewandowsky focus on the effectiveness of bar charts, pie charts, and tables [107]. Both studies found that certain types of visualization methods outperform the others depending on the task [98, 107]. Additionally, Sarikaya and Gleicher dive into the design options and analysis tasks of scatterplots through a literature review to understand how these designs influence a scatterplot’s effectiveness and provide example best practices for design [100]. Pousman et al. explore visualizations that are pushed to the periphery of traditional infovis. They look at systems beyond productivity and focus to understand the usefulness and satisfaction that nontraditional visualization systems can offer [94].
This variety of visualization literature can provide formalized criteria to help us understand the types of analyses users of ED apps can perform with the information the apps communicate back to them. Additionally, it can provide us design considerations and rankings to evaluate the effectiveness of visualization strategies used by existing ED apps and identify the most appropriate visualization methods for communicating ED-specific information.
4. METHODS: CODING AND CATEGORIZATION
Our three-prong methodology first found popular health websites (e.g., healthline.com, verywellmind.com) that suggested ED apps. Second, we compiled the following serial search terms “‘eating disorders,” “anorexia, ” “bulimia, ” “binge eating, ” and “binge eating disorder” from prior ED app reviews [62] to find apps on dominant mobile platform app stores (App Store for iOS, and Google Play for Android). Third, we gathered apps from prior work [62] that were not noted in the first two sources. We included free apps and paid apps with an English-language interface and 100+ downloads, based on similar filtering considerations used in prior research on evaluating mobile mental health apps [62, 74]. In total, we found 55 unique mental health apps that addressed EDs. Of these 55 apps, we could not find 11 of the apps listed in prior work [62, 74]. Ten more apps were excluded because of various technical issues, such as the app failing to start. Therefore, we discuss a final set of 34 apps in subsequent sections of this paper. Two coders, who are also coauthors of this paper, reviewed the apps independently. First, since the coders were not ED patients themselves, they achieved a common ground and understanding of the topic iteratively by consulting the related prior literature and periodic team discussions involving a clinical psychologist who treats ED patients. After a desired level of familiarity was achieved, the coders installed each app on the Google Play and App Store and acted like a typical user of the app (an individual with an ED). They followed each app’s onboarding process and inputted information the app prompted them to enter. The coders used each app for a week so the app would have a sufficient amount of their personal data. For the 55 apps, the coders assessed each one’s primary objective (ED advice, treatment, etc.). Additionally, they took note of different information types these apps presented to them, such as a summary of meal portions, physical activity, and user’s feelings and emotions over time. They also recorded how each app reports information to end-users (e.g., using a visual like chart, text, etc.)
Following the exploratory use phase, the coders used an open-coding based thematic analysis [35] to describe the design strategies the apps use for data collection and reflection. The coders compiled the different ways each app collected data and they categorized the data types each app communicates, including any media it uses. Then, concepts (from personal informatics, info vis, and from ED treatment research; ref. Section 3) were applied to organize those themes through the lens of existing understandings. The coders found that these apps collect large amounts of information across a variety of data attributes. However, overall there was no systematic approach the apps took to display information back to users. Although most apps were designed for ED patients, we also included apps targeted at comorbid psychological challenges such as depression and anxiety [110]. The coders did a recheck of the final 34 apps to ensure we disregard apps that could exacerbate EDs [102]. We excluded food journaling apps that were not primarily designed for individuals with an ED, as food logging apps have been noted to exacerbate ED behaviors [25, 55]. Additionally, we also excluded any weight tracking apps that showed up in our search results, as persistent weight tracking through the use of fitness apps may trigger negative behaviors [57].
Accordingly, from the coding process, we identified two categories, “Collection” and “Reflection,” drawing on the different stages defined in Epstein et al.’s [60] model. Compared to other models, Epstein et al.’s framework is particularly relevant to our work as it captures diverse user goals and is aware of processes that occur outside of app usage that impact the tracking process. Since we focus on the design of existing ED apps, we sought to categorize the apps based on the activities their functionality intended to support. For our ensuing discussion, collection refers to the gathering of personal information (e.g., meals, feelings) from users. Reflection on the other hand, is designed to support users in introspection about their ED condition to facilitate taking action to address their ED. An app was only coded as Reflection if it provided functionality that enabled new information or insights, or gave information in a novel format instead of only listing a user’s data. Of the 34 apps, 4 apps included only Collection, 13 included only Reflection, and 17 included both Collection and Reflection (see Table 1 for a list of the apps in each category).
Table 1:
List of 34 apps classified into 3 categories
| Collection Only (4) | |
|---|---|
| Kick the eating disorder out | 12 Steps Overeaters Anonymous |
| Gratitude Journal (Happiness Journal) | Booster Buddy |
| Reflection Only (13) | |
| Recovery Record Clinician | GG Body Image |
| Anorexia Help Calendar | Food Addiction Calendar |
| Eating Disorder Guide | Anorexia Nervosa Abnormal ED |
| Anorexia | Anorexia Recovery Guide |
| How To Stop Binge Eating | Stop Binge Eating With Hypnosis |
| How to Stop Binge Eating - Complete Guide | Overeaters Anonymous Speaker Tapes |
| Eating Disorders - Compulsive Overeating | |
| Both Collection and Reflection (17) | |
| Recovery Record | Rise Up + Recover |
| CBT Diary | Jourvie |
| deVicer | What’s Up? |
| Mindshift CBT | Nourishly |
| Woebot | 7 Cups of Tea |
| Eating Disorder Test | Blue Buddy |
| RealifeChange | Eating Time - meal reminder |
| New Gratitude Journal | Anorexia and Bulimia therapy - ED Help |
| DBT Diary Card and Skills Coach | |
5. RESULTS
5.1. Defining the Categories of ED Apps
Collection Only:
These apps mainly collect data related to users’ thoughts, emotions, meals, and ED symptoms. Users have a central space to enter information related to their disorder freely. For example, with apps like Gratitude Journal [12], 12 Steps Overeaters Anonymous [1], and Kick the eating disorder out [10], users create a journal and record things they are grateful for, the food they ate, and any new things that they have learned to battle eating disorders respectively. Many of the collection-only apps collect this data to increase the user’s accountability for positive actions by enabling them to check in their emotions and any harmful behaviors they experienced in the moment [60]. For instance, Booster Buddy [6] allows users to check-in by selecting their mood from four preset options (Good, Not Great, Struggling, and Crisis). Along with this, it also asks users whether or not they have had alcohol in the last 24 hours, at the same time allowing users to maintain a log by typing in their favorite quotes to improve their mental health (see Figure 1-(a)). Even though the act of collecting data can prompt reflection without any feedback [43, 44], we labeled apps that excluded functionality specifically intended to support reflection as Collection-Only.
Figure 1:
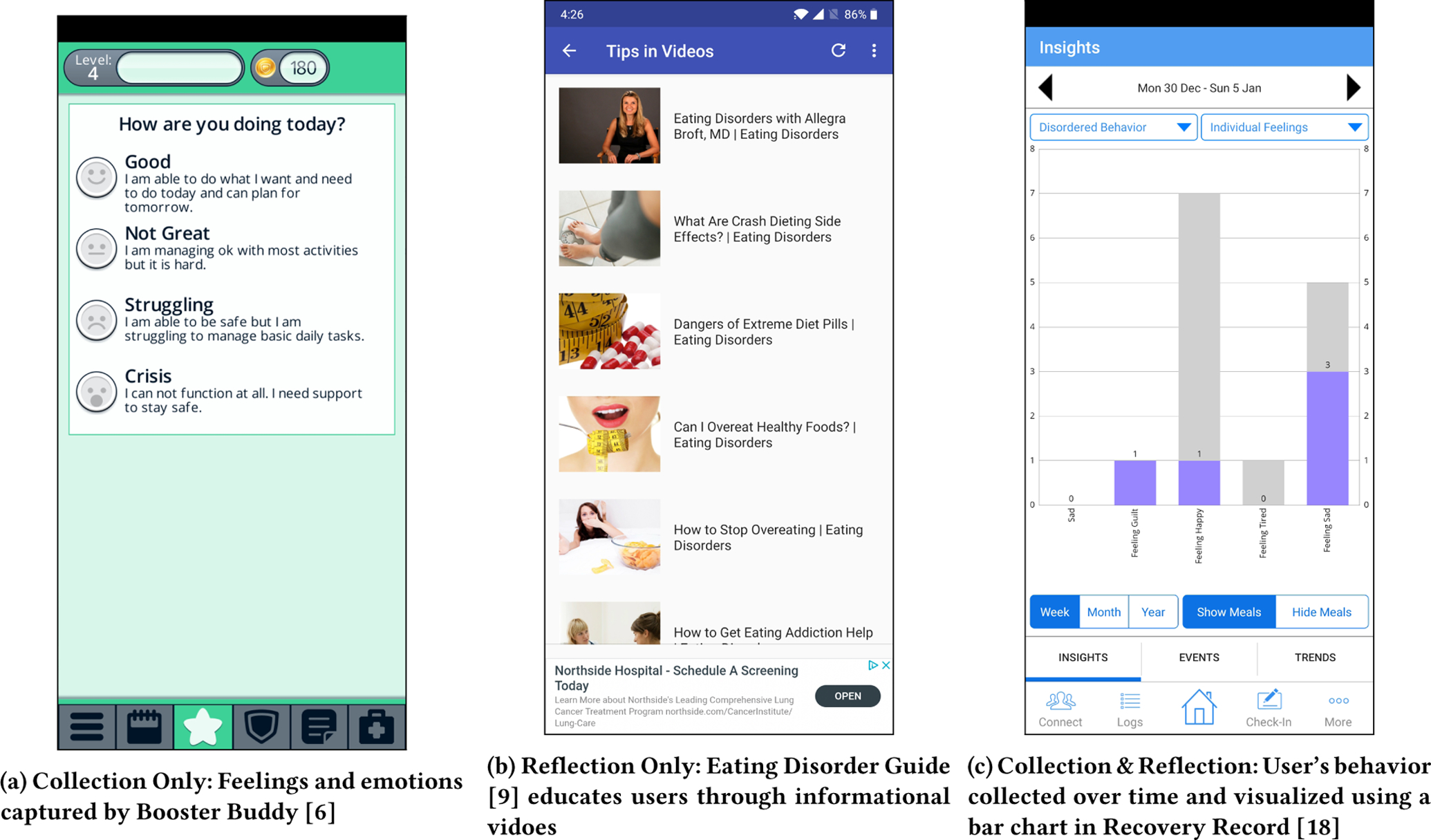
Screenshots of Collection only, Reflection only, and Collection & Reflection apps.
Reflection Only:
This category of apps is designed to support users in introspection about their ED condition. Such apps can provide generic inspirational quotes and positive images to help users practice mindfulness and healthy wellbeing. They also provide informational resources related to ED, such as tips for combating negative behavior/symptoms, which may help users apply that knowledge to their personal needs. Overall these apps may act as a supplement to ED treatment. For example, apps like Eating Disorder Guide [9] provide helpful techniques that people can use to develop mindful eating habits (Figure 1-(b)). Similarly, apps such as Anorexia Nervosa Abnormal ED [4] and Anorexia Recovery Guide [3] provide helpful information such as causes, signs and symptoms, and treatment of AN. Some apps also deliver this in multiple modes - such as text and videos. However, this category of apps lacks personal (health-related) data collection, causing the materials that were intended to support reflection to be less tailored than apps with health data collection.
Both Collection and Reflection:
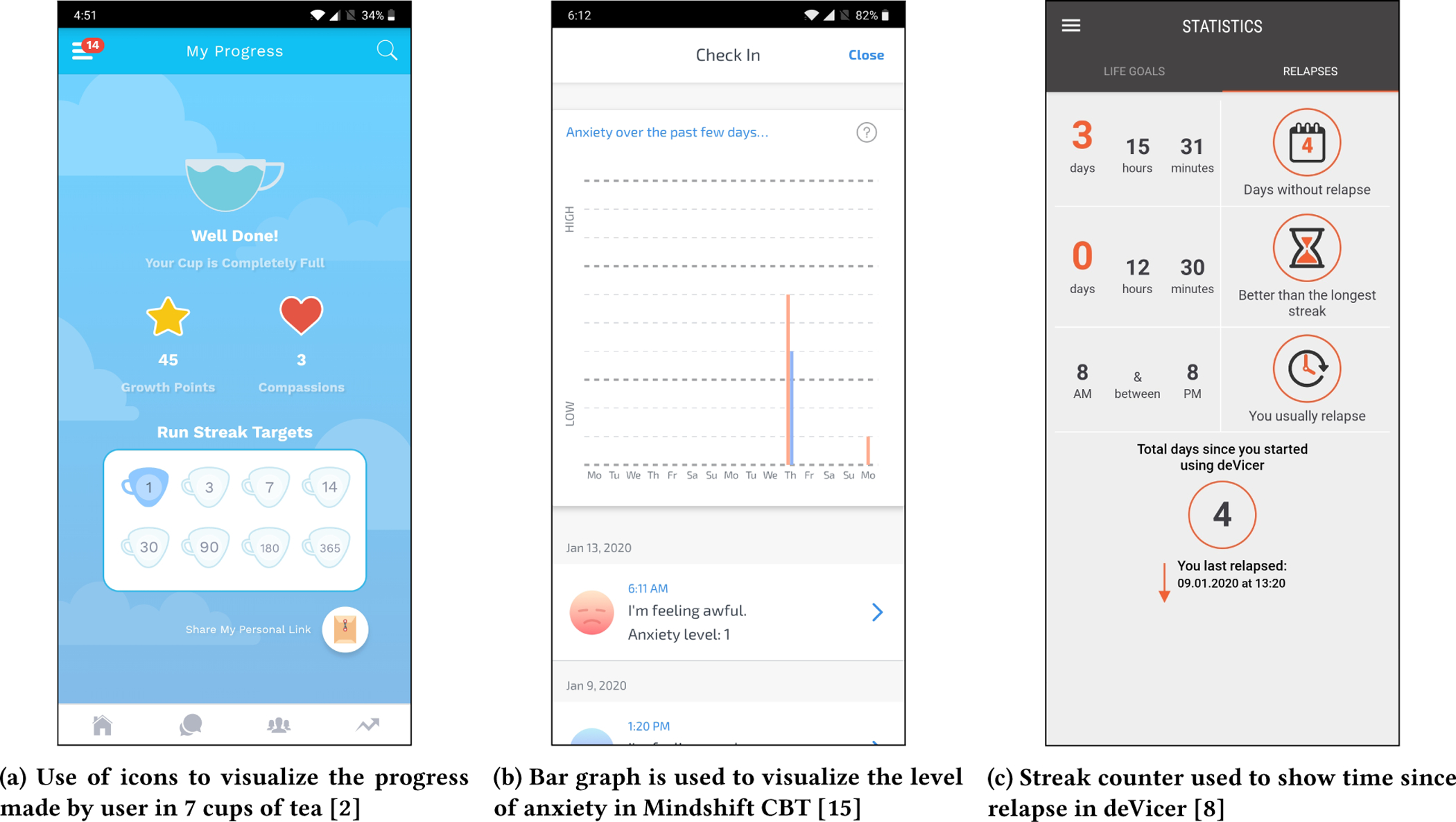
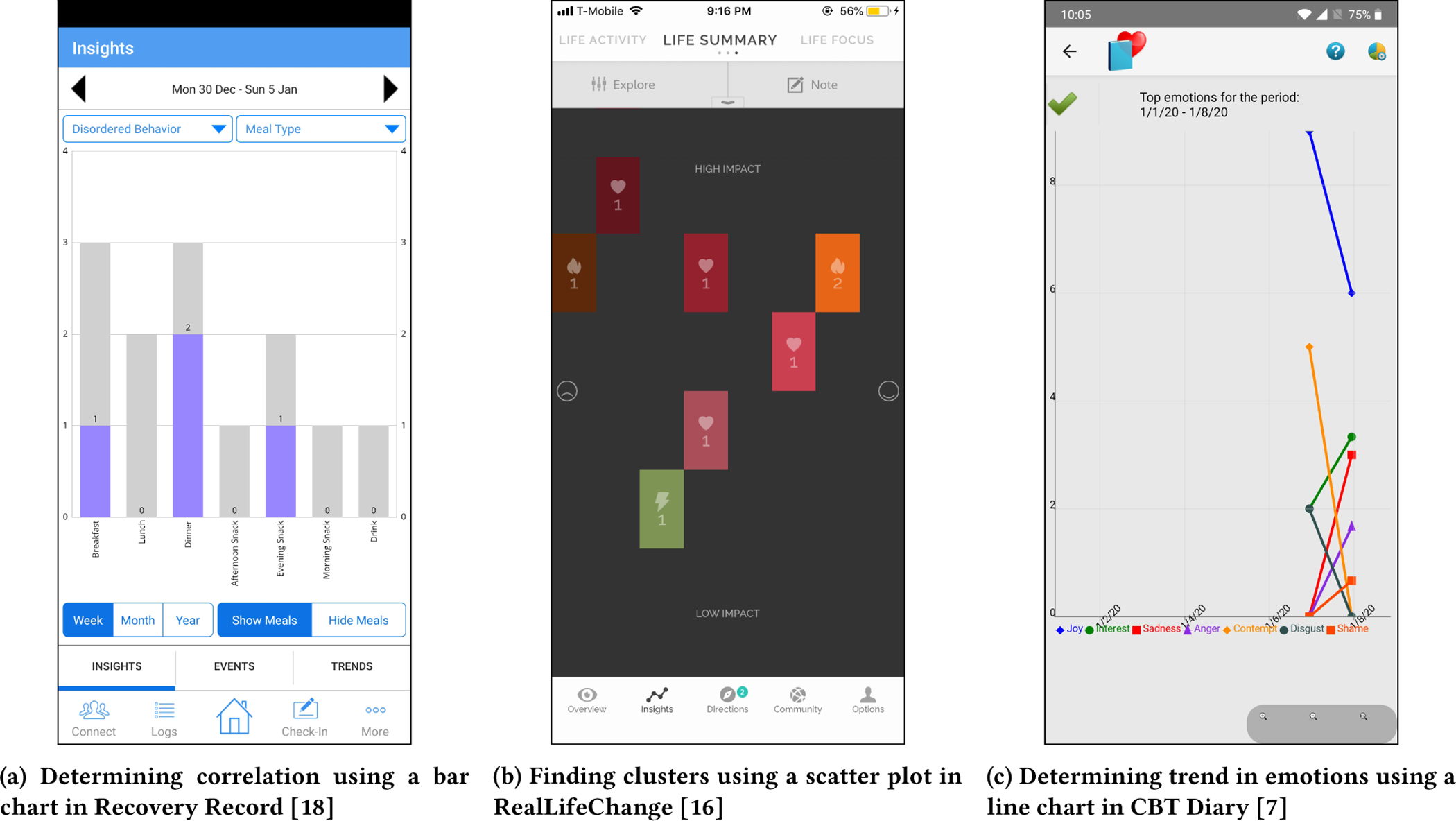
Apps that fall under this category allow users to monitor eating disorder attributes over time while providing functionality that supports users’ ability to reflect on their ED. While the design of some apps in this category (e.g., Recovery Record [18]) may include educational content, simply examining one’s own data is neither sufficient nor necessary for reflection [105] [31]. People that use these apps may develop a habit of collecting data related to behavior, meals, thoughts, etc., over time on these apps. Based on this information, these apps provide them with visual feedback in the forms of text, icons, and graphs, enabling users to reflect on their recorded data. For instance, apps like Recovery Record [18], Rise Up + Recover [17], and Jourvie [14] require users to record each meal individually along with accompanying thoughts and emotions. The apps also aim to establish healthy eating behavior patterns by gathering information about other related factors, such as whether the users restricted or binged while eating, with whom they had the meal, where they had the meal, and how long it took to finish eating. This data gets saved as logs in the form of text and icons. With collected information, these apps provide feedback. Through bar graphs, users of Recovery Record [18] can view for which meals they had different types of disordered behavior along with other information such as meal type, meal companions, location, etc. (Figure 1-(c)). Apps like Rise Up + Recover [17] and Jourvie [14] also allows users to export logged meals as a pdf file and share it. Jourvie [14] alternatively visualizes information such as meal type, location, and companions with simpler visuals like pie charts.
5.2. What Information is Collected and Reflected? And How?
Enriching the app categorization based on their data collection and reflection abilities, the two coders who reviewed the 34 apps also noted each different type of information the apps aimed to collect from and communicate information about to users. After recording this for each app, the coders looked for patterns or similarities in the data each app collects or shows to users, and began grouping them into categories that each represent a different data type (e.g., meal, thoughts, emotions, etc.). The coders also categorized different methods these apps use to collect data (e.g., text, icon, etc.) or show insights (e.g., charts, tables, etc.) through a thematic analysis. Across the 34 apps, they found 11 different data types for collection and reflection, 4 types of strategies for collecting the data, and 5 types of strategies for reflecting the data. See Figure 2 that visualizes the distribution of these apps across different data types and strategies for collecting and reflecting data.
Figure 2:
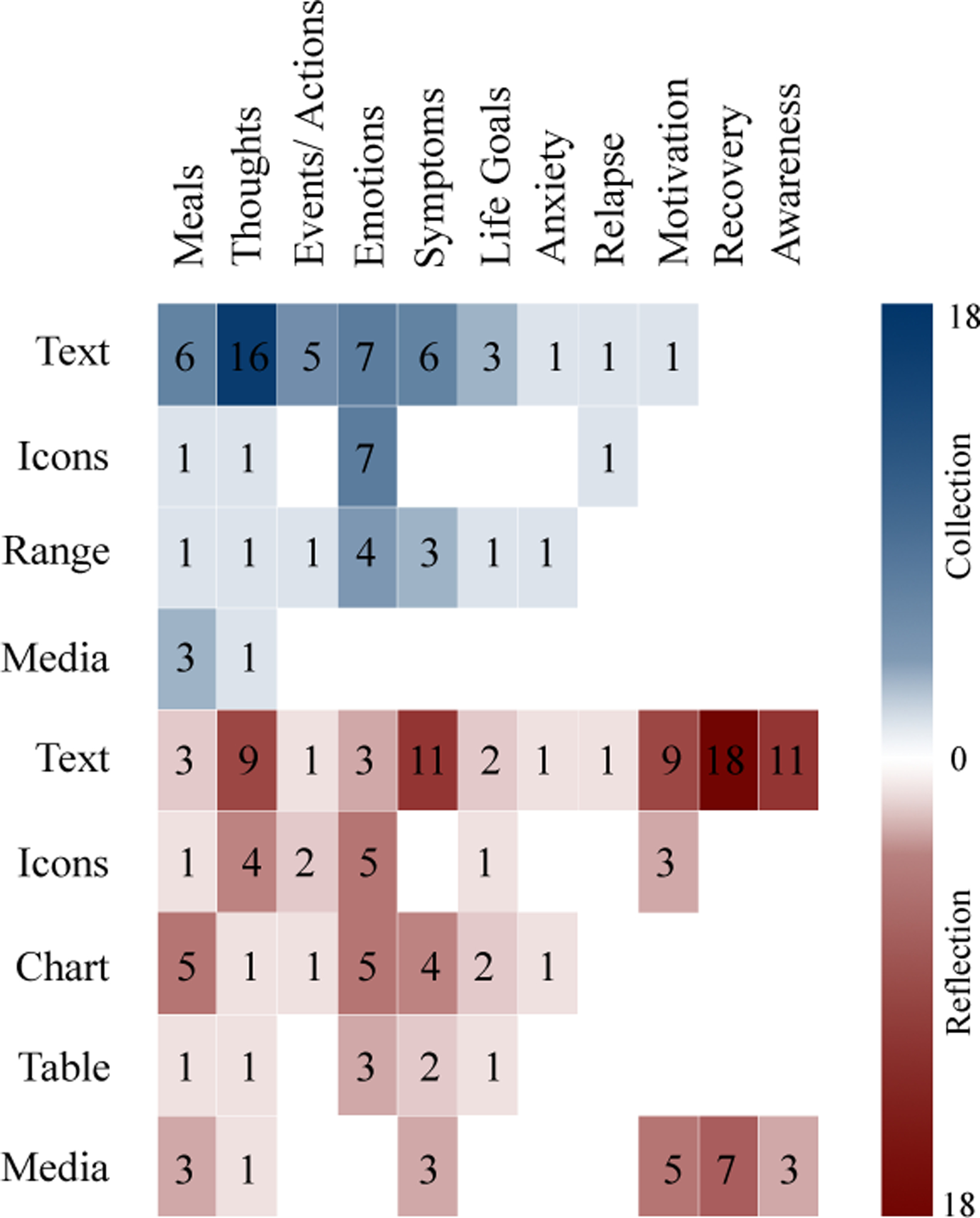
Distribution of eating disorder apps based on type of data and the visualization strategies used for collection and reflection.
Meals:
Meal logging is vital in ED treatment, as regular eating is foundational in order for other strategies and improvements to be made [115]. In ED therapy based on the CBT framework [91], clinicians provide meal logs that help patients self-monitor their eating patterns. By collecting real-time meal information, apps can help individuals develop a heightened awareness of their consumption habits and associated experiences. This information can elicit patterns that can help the individual break out of detrimental behaviors [115]. 7 of 34 apps that we reviewed ask users about their meals and accompanying details, such as the type of meal, the time they consumed the meal, where they ate the meal, etc. The primary method of collecting this information is through text. Collecting meal information is useful for people with BED or BN to enter meals along with a timestamp to help them understand how often they eat and enter contextual factors that influenced their eating. For AN patients, collecting meal information is essential to maintain a regular eating schedule and eating more, as patients with AN engage in skipping meals or other forms of restricting food. Additionally, for BED or BN, apps like Jourvie [14] also collect who was present during the meal. This information is useful, as BED patients tend to experience shame or disgust with their binging and avoid eating with others [21]. Most apps that collect meal information do not include caloric intake and focus on patients considering how they feel in the moment. However, as part of a food diary, Blue Buddy [5] shows users their BMI chart. Kay et al. found that a consumers’ perception of weight is often disconnected from scales’ capabilities and clinical relevance [75]. Although this app does not show weight directly, in the context of EDs, including metrics that may potentially cause a fixation on weight is a significant trigger that contributes to disordered weight-control behaviors. This fixation is why ED patients are only allowed to weigh themselves in the presence of a clinician weekly [91]. It is essential to omit caloric intake and limit similar physiological metrics in these apps so users can avoid a fixation on numbers that could lead to unhealthy behavior [71].
Events and Actions:
Episodes of disordered eating behaviors (such as restriction in the context of AN, or binge eating or purging for BN or BED) can be triggered by external events (e.g., exposures to stimuli associated with the behavior) [74]. Additionally, certain life events could have played a critical role in the development of the ED [91]. By collecting event and action data from users, apps can increase their awareness of potential triggers. By visualizing this information, apps can further help users identify positive events or actions to use as distractions or provide proactive problem-solving techniques to reduce the likelihood of negative eating behaviors [91]. 5 of 34 apps collect data related to the events a user experiences or the actions they take. Users enter this data with text. For example, Realifechange [16] asks users to type in various life events and select the impact of these life events and if the event was more positive or negative. CBTDiary [7] asks users to enter events that happened in their day and type additional thoughts to identify sources of stress. Apps that display event data provide this information with text and icons to aid in reflection. Reallifechange [16] is unique in showing event/action information and the associated emotional impact. The x-axis position indicates how happy/sad the user felt, and the action’s opacity demonstrates its impact (See Figure 3-(b)).
Figure 3:
Screenshots of apps showing Meals, Events/Actions, and Emotions data.
Thoughts:
Many people with an ED suffer from a preoccupation with thoughts about their shape and weight [91]. Apps can collect thought information to help individuals reduce their preoccupation with thoughts about eating and determine if any associations exist between their thoughts and self-reported meals/emotions/other data collected [91]. Most importantly, they can help users separate their thoughts with actual truths about their body and take steps to break their overvaluation of their shape [91]. 16 of 34 apps in our dataset collect thought information, primarily through textual input. Some apps treat thought data as standalone entries that users can supply at their convenience and will, while other apps actively prompt users to type their thoughts when logging activities or meals. Logging thoughts alongside meals (e.g., in the app Rise Up and Recover [16]) may help those with AN identify causes for skipped meals by exploring how they felt in the moment. Additionally, logging thoughts alongside events (as in CBTDiary [7]) can help those with BN identify the reasoning behind triggers for binging and purging. 7 apps display thought data as descriptive diary entries. The app Rise Up and Recover [17] additionally compiles these entries into an exportable table. On the other hand, GG Body Image [11] gamifies thought data by making users distinguish between positive and negative examples.
Feelings/Emotions:
Many individuals with an ED tend to mislabel negative emotional states as “feeling fat”, prolonging their distorted body image thoughts and triggering adverse ED symptoms [91]. In traditional CBT therapy, clinicians help identify underlying negative moods or feelings that may be maintaining the patient’s eating disorder. Apps that allow individuals to self-report their emotions and feelings can help them address the underlying sources of their emotions and gain control over their mood through mindfulness [91]. 13 of the 34 apps collect data on users’ feelings and emotions, primarily using text and icons. We found that apps in our dataset reflect emotion data with icons that can be associated with other data attributes, such as the user’s meal (Recovery Record [18]), thoughts (What’s Up? [19]), or anxiety (Mindshift CBT [15]), or can be standalone data (Woebot [20]). The ability to see emotions associated with a meal could help identify when a negative behavior would occur (e.g., a person with BN reports feeling guilty after a meal and engages in purging). Additionally, for individuals who suffer from a comorbid disorder, the ability to see emotions alongside thoughts can help them identify negative thinking patterns that contribute to depression/anxiety and their distorted body image thoughts. 3 apps display emotional data as text-heavy log entries or with a table, while 5 apps generate charts for emotion data, choosing to show emotion data by itself or associated with other data attributes. For example, CBTDiary [7] shows users their emotions over a week (Figure 3-(c)).
Goals and Habits:
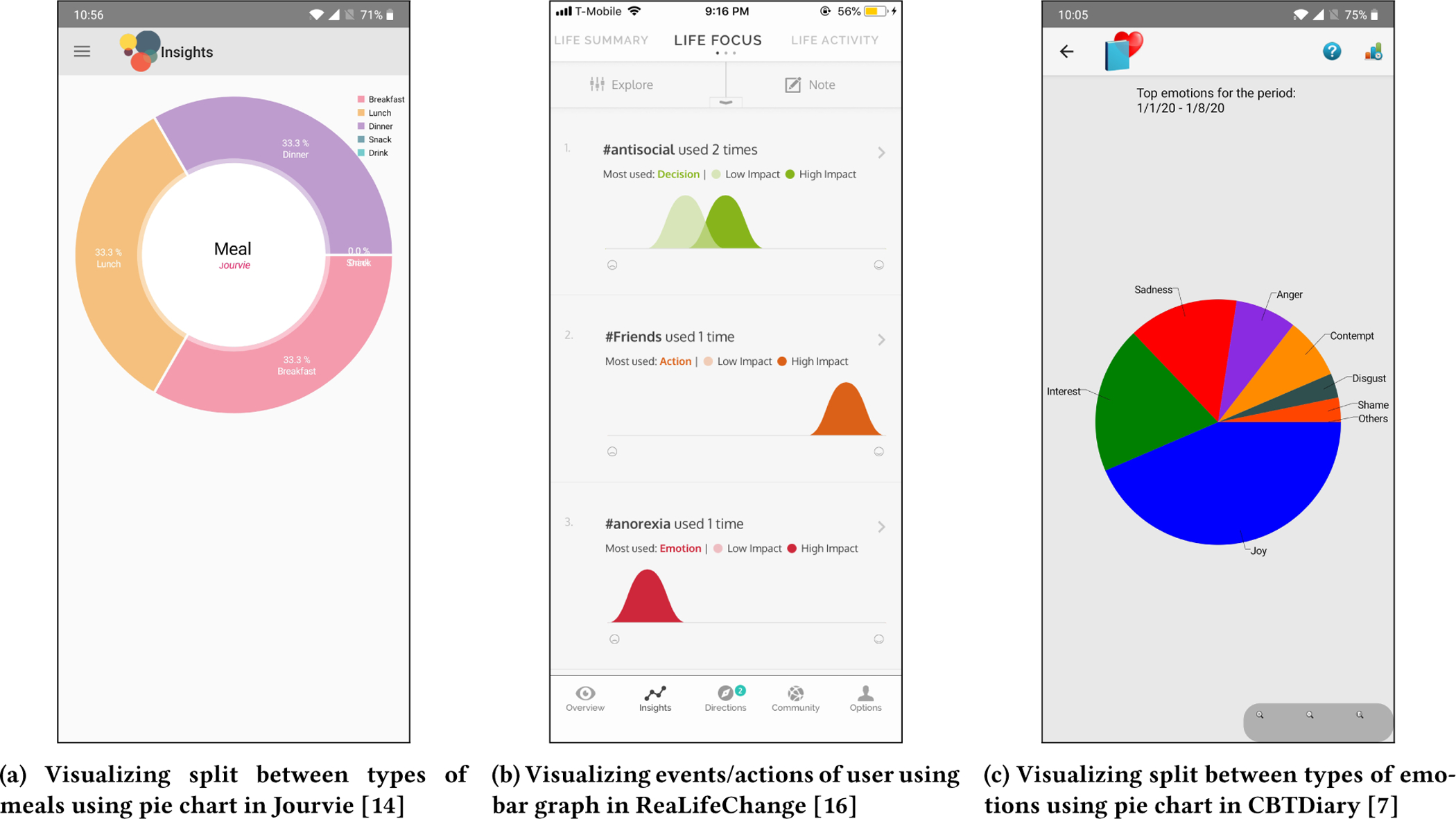
ED patients tend to have multiple, rigid, and extreme goals, and in traditional ED CBT therapy, their clinician can help assess whether these goals impair their actual progress [91]. Additionally, clinicians work with patients to set goals or achievements, either related to overcoming their ED or generally about their life, and help them make steady progress towards their goals [91]. By collecting information about life goals and what people want to achieve, apps can ground users in remembering what accomplishments they will work towards. 4 of 34 apps collect life goal and habit information. Users can type a list of positive habits they want to maintain and negative patterns they want to end. These apps reflect this information to show users their progress towards the user’s set goals or how often they log. For instance, 7 Cups of Tea [2] uses icons to show the progress made by the user. As the user makes progress, the cup fills up (See Figure 4-(a)). On the other hand, deVicer [8] shows progress towards personal life goals with line graphs. Recovery Record[18] also allows users to set calendar reminders to complete specific goals. The ability to set specific goals is useful to address the various dietary rules that people with different EDs engage in; for example, individuals who binge-eat commonly perform food avoidance (avoidance of specific foods) and could use goal-setting to gradually reintroduce avoided food into their diet [91].
Figure 4:
Screenshots of apps showing Life Goals, Anxiety, and Relapse data.
Motivational Rewards:
Paper-based therapy homework does not provide immediate feedback or encouragement upon completion [115]; however, clinicians frequently meet (weekly or twice a week) with patients to monitor their progress and encourage them along with their treatment [91]. Many individuals with EDs, especially those with AN, express ambivalence to change [74]. By collecting motivational information from the user, apps can frequently display this content to build a positive association with self-monitoring activities [115]. Only 1 of the 34 apps allows users to note down their favorite quotes to keep them motivated. To motivate continuous logging, 9 of 34 apps provide rewards to their users. These rewards are text (inspirational quotes or positive affirmations from other ED users), images that convey a positive message, and music to listen to calm users. Recovery Record [18] additionally uses gamification by providing jigsaw puzzle pieces that users can collect and complete to unlock further rewards.
ED Symptoms:
Depending on their ED’s severity, individuals may engage in harmful behaviors like vomiting and starvation to control eating, shape, and weight [91]. This behavior encourages a cycle of restrictive diet and destructive coping mechanisms that ultimately prolongs the core eating disorder, and body concerns [91]. Therefore, clinicians collaborate with patients to establish a regular eating practice and find strategies that can help them reduce the need to partake in such behaviors [91]. 6 out of 34 apps collect data related to ED symptoms, and users can enter this data through text or select it on a range indicator. These apps typically show this information alongside meals, thoughts, actions, and other collected data. Apps that collect real-time information about specific ED symptoms can help users self-monitor their consumption habits and associated activities. For example, an individual with AN can select from a predetermined list of harmful behaviors (e.g., skipping meals, overexercising) to log its occurrence along with other data, such as an event trigger or a meal entry, and they can view entries where harmful coping mechanisms occurred. In reflecting this information, apps can help users elicit patterns and behaviors to target to help break out of their adverse eating habits and gain context about their harmful symptoms [115].
Anxiety:
Many individuals with AN or BN also have features of anxiety or depression [91]. Even if not formally diagnosed, individuals with ED may express behaviors such as irritability, impaired concentration, loss of libido, and obsessive thoughts [91]. By collecting anxiety symptoms, apps can help users better understand potential triggers to minimize anxiety. Only 1 app (Mindshift CBT [15]) collects anxiety symptoms (such as racing thoughts, trouble concentrating) from users alongside thoughts and emotions. Users rate their anxiety on a scale of 1 to 10 and select from a list of common anxiety symptoms. Mindshift CBT [15] shows this data back to users along with their emotions (sad or happy) for a given week (See Figure 4-(b)).
Relapse:
Maintaining treatment progress after therapy has finished can be challenging for patients, as the relapsing rate is considerable without support [74]. Previously, Bauer and Moessner [30] showed even a low-intensity intervention was enough to maintain treatment progress, demonstrating that patients benefit from aftercare. Only 1 app (deVicer [8]) allows users to record relapse information with the press of a button, i.e., record the timestamp at which a relapse has occurred. Its reflection method is limited, as it only generates a streak counter showing how many days have passed since a relapse (See Figure 4-(c)). By collecting relapse information with timestamps, apps can provide users proactive support and help them understand their relapse patterns to identify potential triggers and setbacks as early as possible [91].
Awareness:
Providing awareness about body image and eating is important as many individuals with an ED have misconceptions that maintain their ED [91]. 11 of 34 apps educate users about different eating disorders and their causes, using text or videos to convey this information. Some apps (ex: How to Stop Binge Eating [13]) provide information about a specific ED, while other apps speak more generally about EDs (ex: Eating Disorder Guide [9]). Most apps include information about the harmful effects of dieting and adverse behaviors such as purging or restricting. The information provided by these apps is typically not tailored to specific informational goals (no functionality to customize the presented information was apparent) and instead provides overall education.
Recovery:
Along with collecting logged data, apps provide information on standard recovery techniques and coping mechanisms to help users manage disordered behaviors. Smartphone apps are well suited to deliver in-the-moment interventions to help when someone with an ED is exposed to a trigger and feels an urge to partake in harmful behavior [74]. 8 apps provide ED-specific coping strategies, 4 apps offer mental health resources, and 3 apps give both. All typically provide text-based information (in the form of articles), but some provide videos for users to watch at their convenience. Some apps use audio such as meditation sounds to relax and calm their users. Overall, this information is not tailored to an individual’s unique behavior or the needs they may have surrounding triggers that may precipitate disordered eating behaviors. Only 1 app (Recovery Record [18]) allows users to customize their coping skills and indicate when they want to receive a coping skill (e.g., someone with BN reports they have the urge to binge, so Recovery Record [18] shows them a coping strategy they have preselected). This ability is useful to provide proactive problem-solving techniques to combat problematic behavior [74].
ED apps have the potential to aid in therapy as they provide a means for individuals to regularly self-monitor the specific behaviors that EDs involve. The apps we reviewed collect various data types that are important for an individual to understand their ED. The apps were more consistent in how they gathered information, allowing users to type in data or select from text options. Additionally, meals, emotions, and thought data were the data categories that most apps collected. Some apps were more comprehensive than others in terms of the amount of data they collect and the level of detail and flexibility they provide to users to understand their information. However, the reviewed apps were less consistent in their choice to display information back to users, with most apps using simple visuals and some apps merely showing the data again as logs of text. Because of this lack of uniformity, we turn to visualization literature to determine the effectiveness of the apps’ different methods to aid in reflection.
5.3. How is Data Visualized for Communication?
Finally, by visualizing the collected data, ED apps can allow users to process information through visual perception and develop an understanding of underlying data, as has been argued for other application areas in visual analytics [98]. Charts and tables are prominent strategies for visualizing collected data. We notice that these two strategies for communicating insights relate to the data types identified in our app review process (Section 5.2). However, a large body of research in the data visualization community critically discusses the effectiveness of visualization techniques [80, 98, 100], as noted in Section 3. This research demonstrates that visualized information’s efficacy depends on several factors, including the analysis task at hand and data attributes shown. For example, while one chart might be suitable for answering a specific question (e.g., is there a correlation between two data attributes?), it might not be appropriate for other task types (e.g., finding a data point with the lowest value). We borrow from Amar et al.’s task taxonomy [26] to organize the visualizations’ capabilities and to analyze the goals that they allow users to perform. Additionally, we briefly discuss the approaches the ED apps took to visualize such information. The remainder of this subsection discusses how this relationship – between the type of visualization used in ED apps and the goals each visualization is meant to support – aligns with or deviates from guidelines provided in the infovis literature.
Determining Correlation:
Among all the reviewed, 5 ED apps enabled users to determine if a correlation exists between a set of two or more data attributes (e.g., meal type and disordered behavior, meals and emotions, etc.). For example, a user of Recovery Record [18] with BN could evaluate the correlation between meals for which they experienced an urge to binge and the type of meal they consumed for a given week (See Figure 5-(a)). This is an important observation, as they can pinpoint a relationship that may suggest the cause of a trigger and use that knowledge to manage their condition accordingly. Three apps displayed correlations with a line chart, and two apps (Recovery Record [18] and Woebot [20]) used bar charts and line charts interchangeably for communicating correlations among multiple data attributes.
Figure 5:
Screenshots of Visualization Methods used by both Collection & Reflection apps.
Concerning the guidelines established by the infovis research [80, 98, 100, 107], line charts are significantly more accurate and efficient than bar charts when determining a correlation between two attributes [98]. Saket et al. also showed that user preferences in using line charts and bar charts are significantly higher than other visualizations types for finding correlations between two attributes. This is because, although scatterplots can be useful for finding correlations [100], as the number of elements increases in a dataset, scatterplots can become overly cluttered [80]. Additionally, Spence and Lewandowsky found that a pie chart had a higher accuracy and lower error rates when it came to aggregating and comparing two groups of elements against each other [107]. However, none of the apps used pie charts or scatterplots for this task, signaling a gap in utilizing these relevant visualization types over bar charts when determining the relationships between 3 or more data attributes.
Finding Clusters and Filtering:
Some ED apps also use data visualizations to enable users to find clusters of groups with similar data attributes and filter attributes of interest. For example, Real-LifeChange [16] uses a scatterplot to visualize clusters of logged events and actions based on their severity of impact and feelings associated with it (See Figure 5-(b)). The ability to find a cluster of events and actions associated with sadness may help discover opportunities for helpful interventions or coping strategies to be delivered to reduce the likelihood of purging. Additionally, Recovery Record [18] displays clusters of similar meals with a bar chart; for example, a user with AN could see how many of their meals were associated with satisfaction, motivating them to eat regularly.
Saket et al. found bar charts are the recommended form of visualization for finding clusters and filtering, as they are significantly more accurate and faster than any other type of visualization for these tasks [98]. Kim and Heer also found that colored scatterplots served summary tasks well but reduced the effectiveness of value tasks [80]. Alternatively, Spence et al. found that between a table, pie chart, and bar chart, bar charts have the highest accuracy for comparing two elements, but when more elements are added, a pie chart was the best for summing the value of two groups and comparing them [107]. Also, Sarikaya and Gleicher noted that using point encodings (such as changing the symbol or color of individual points), grouping, and rearranging similar points together support finding known patterns such as a cluster [100]. However, other than scatterplots and bar charts, we did not find evidence of any other forms of visualization to present groupings of data in the ED apps or to filter on attributes of interest. The apps, therefore, largely align with the recommended visualization techniques for performing both these tasks.
Characterizing Distribution:
Some apps, such as Recovery Record [18] and Jourvie [14], allow users to see distributions of collected data. Users can obtain information about such attributes at a high level, such as seeing what percentage of meals eaten were alone or what percentage of negative emotions they reported. However, apps should display this information carefully as it could be misappropriated; for example, showing a high percentage of binge eating episodes could potentially cause someone with BN to become distressed and fixate on their meal consumption, potentially leading them to partake in negative behaviors such as purging [106].
Bar charts and pie charts are the most accurate and time-saving forms of visualization methods for this type of task. Contrastively, scatterplots are a time-consuming form of visualization for representing distributions [98]. Spence and Lewandowsky found that pie charts outperformed bar charts when participants were asked to compare combinations of proportions [107]. However, the data points in scatterplots can be encoded and positioned in a way that allows for a range of values to become apparent, allowing distributions to be presented adequately [100]. If points overlap or other visualization elements (e.g., labels) occlude the actual values, it becomes difficult to perceive points’ positions [83]. Although a few apps employed the recommended visualizations, the considerations from the literature could be more apparent in how the apps used visualizations to characterize distributions of data attributes.
Determining Trends:
Determining trends in the information logged over time can help users gain awareness of their current status and encourage positive behavior towards goals [60]. This information is advantageous for EDs. As traditional ED therapy requires patients to self-monitor ED symptoms [104], observing trends of their symptoms, meals, and other attributes with visual representations would help ED patients gain a clearer understanding of their eating problem and any progress they made [62].
Several of the apps reviewed use different visualization techniques to communicate trends to end-users. For example, while CBT Diary [7] uses line charts to visualize the changes in the value of each emotion logged over time (See Figure 5-(c)), Mindshift CBT [15] uses bar charts to present a weekly trend of emotions and their severity. Additionally, Jourvie [14] uses a pie chart to display ED symptoms for a given time interval. Saraiya et al. found that using trend lines help aggregates data, find anomalies, and explore patterns of data [99]. Additionally, users in Saket et al.’s study found line charts useful for representing trends and that finding trends is more commonly associated with line charts compared to bar charts [98]. Overall, the design decisions in the apps mostly align with recommendations in the information visualization literature.
Viewing and Retrieving Aggregated Summary Data:
A small number of ED apps use data visualizations to enable users to compute an aggregated value from a set of data values. For example, CBT Diary [7] generates a table for the self-reported emotion data, allowing users to find the minimum, average, and maximum counts of each emotion over time, which is useful for understanding behavior over time and identify progress [91]. Bar charts, pie charts, and tables are equally effective in communicating aggregated value to end-users [98]. However, Spence and Lewandowsky found that bar charts and pie charts outperformed tables for aggregating two groups of data and comparing it against each other [107]. CBT Diary [7] did not consider this aspect in their design decision.
Additionally, many ED apps enabled users to retrieve a given attribute’s value, but they employed different visualization strategies. For example, using the Rise Up + Recover [17] app, users can view a detailed description of their daily logged meals. Similarly, users can view a thought entry for a particular date and time using the CBT Diary [7] app. This ability is useful not only for ED patients to get a detailed account of their condition, but for them to also share with support networks (such as a clinician) to give them insight into their behavior [115]. Both apps use tables for this purpose. Some apps like Blue Buddy [5] or deVicer [8] use other techniques such as bar charts and scatterplots to communicate individual data points. Bar charts and tables are significantly more accurate and faster than other charts for retrieving a value [98]. Alternatively, if using a scatterplot, the individual points need to be encoded and grouped in a way that allows users to explore the dataset and find points of interest [100]. However, Mackinlay notes that a scatterplot is suitable when the retrieved data is a quantitative or ordinal value [83]. Essentially, while many apps did use the recommended visualizations for this type of data communication, the subtleties of when some of them might be better suited than others were not apparent in our review.
Finally, some apps use non-conventional visualizations to convey summary patterns in data. Woebot [20] shows emotions via emojis, and 7 Cups [2] uses teacup icons to communicate progress data in a tabular format. The more filled cups, the more goals a user has achieved. These examples indicate the apps’ tendency to be more artistic and creative with how data is communicated. Pousman et al., however, recommend using participatory design and ethnographic research methods to design such visualizations. Having an understanding of a user’s goals and activities can result in more relevant visualization techniques to support such needs [94]. Therefore, we conclude here that such artistic infovis techniques adopted by Woebot [20] and 7 Cups [2] may only be useful for less task-driven information [94].
To summarize, while many of the ED apps use various visualization techniques, the selection of a specific technique rarely took into account the effectiveness of that visualization technique for communicating the given insight to end-users. A few apps did use a well-suited visualization technique, such as CBT Diary’s [7] use of line charts, to represent trends over time. In most cases, though, the visualization technique was either non-optimal or potentially contrary to the goal the visualization was meant to support.
6. DISCUSSION
Based on our review, in this section, we present several opportunities and guidelines for eating disorder apps to be better suited to the needs of individuals with an eating disorder.
6.1. Opportunities to Improve Data Collection in ED Apps
As mentioned earlier, personal data collected about various health indicators is valuable in helping gain self-awareness and facilitate self-management of one’s data [59, 79]. For the apps reviewed, guided by this principle, we found that eating disorder data can be incredibly detailed, and more than 60% of the apps required users to log information daily. However, is this extent and type of data collection likely to support improved outcomes in ED?
First, while the process of journaling is essential for tracking progress, app users may face several challenges when recording information. A survey conducted by Cordeiro et al. found that users who journaled meal information multiple times a day described the process as “too much effort,” “time-consuming,” or “tedious” [46]. A majority of the reviewed apps that collect data make users type out this information. If users find this process difficult, they may track in a way that diminishes their data accuracy. People skip tracking when the data is complicated and becomes time-consuming to log (such as meal information) [46, 60]. Missing an entry reduces future results’ accuracy, which unmotivates users and leads them to abandon journaling altogether [46, 60]. Besides this, if users have limited choices for logging their data, they may find it challenging to determine which option represents their experience, which in turn leads to entering data that may not express their true feelings [46]. Additionally noteworthy is that individuals with an ED perceive stigma for engaging in treatment [30]. However, the long commitment towards data collection in the reviewed apps may result in this process not being discreet. Some individuals may feel discouraged or embarrassed using these apps around others as it highlights their disorder, resulting in them stopping tracking.
Moreover, recently, concerns have been raised about the implications of using self-tracking tools and their potential to trigger, maintain, or exacerbate eating disorders [58]. These technologies require close monitoring of caloric consumption or meals and quantify behaviors to assess health. However, in the case of ED patients, scholars have noted that they can become a way to quantify self-worth (e.g., based on caloric intake or output [84]). Rigid and perfectionist thinking surrounding weight and corresponding numbers is relatively common among individuals with ED [50, 73]. Like many of the apps we reviewed in this paper, regular use of these tools that emphasize documenting various numbers can potentially induce inflexible thinking regarding caloric intake, eating habits, or body weight. Further, for individuals with perfectionist tendencies, deviation from allotted calories or physical activity goals might engender feelings of anxiety and guilt; negative affect is a well-known predictor of ED pathology [109]. Summarily, the data collection strategies employed in the ED apps we reviewed need to be revisited and rethought for alternatives.
Design Guidelines:
In addition to text boxes – a common feature in the reviewed ED apps to log data, future iterations of these apps can provide different modalities of collecting information, such as voice inputs or taking photos of meals that do not emphasize details of the food. However, depending on the user’s context (such as being in public), journaling information with these modalities may not be discreet. For meal information, tracking detailed data that reminds users of their weight and shape may cause them to become overwhelmed [87] or overly preoccupied with their eating habits and lifestyle [57]. Therefore alternative methods that capture relevant information passively or do not rely on users to input such information may be more appropriate. These methods will have to consider the user’s current health and clinical state so that apps do not become a new means of inordinate interest in eating and related phenomena or potentially delay seeking help. Most of the reviewed apps allowed the recording of users’ own volition and not in the context of treatment or recovery. Another opportunity for design is to consider the user’s goals in a given time and alter the type of information collected. For example, enhanced CBT for ED therapy features four stages with different goals and outcomes, with the first stage focused on weekly weighing and regular eating [91]. Apps can emphasize timely reminders to eat and aid users to log meals at regular intervals, which could be adjuvant to logging and collecting meal data. In general, apps can consider a user’s context and progress in treatment and collect information that can be displayed in an ecologically sensitive way to aid in future progress. Such an ecologically sensitive approach to data collection may, in turn, facilitate self-monitoring as in CBT [91], and thereby support improved health outcomes.
6.2. Opportunities to Improve Data Reflection in ED Apps
Self-reflection has been recognized to help understand one’s health concerns better and gain self-awareness. Broadly, the self-reflective process, often based on past behaviors and past data, can result in behavioral change, improved problem solving, and personal and professional awareness as well as improved patient care [33, 64, 81, 85]. Consequently, supporting reflection has been at the crux of the personal informatics literature [48, 60, 82]. Facilitating reflection through an ED app may assist in the continuous process of recovery and early relapse detection by monitoring ED behavior and a patient’s cognition [22]. Due to high relapse rates of AN and BED, ED apps may be particularly useful in addressing this issue [22]. Additionally, by supporting self-reflection, ED apps can mimic existing CBT treatments; they can ensure that the app users have a greater understanding of their eating behaviors, what influences them, and can even provide interventions that prevent relapse episodes [62].
As we saw in our review, most ED apps tend to collect various types of data from users to facilitate reflection via understanding daily habitual patterns and finding opportunities for change. However, we also found that making sense of large amounts of collected data and providing value for users – as is the goal of the self-reflection process – is a challenge for personal informatics apps, and ED apps are no exception. There is an overall lack of customization available in the reviewed apps; only Recovery Record [18] allowed users to set goals and receive reminders as well as select coping strategies. The apps we reviewed obtain personal ED data and translate them into information that seeks to aid in reflection in various ways. However, for EDs, reflection without proper context poses complex challenges [49, 108]. For example, a person suffering from an ED may believe that since they feel “fine,” they are healthy, even though their body weight could be 60% below the clinically healthy range and their eating habits may be disordered [87, 102]. As a result, the individual may pursue returning to a low-weight state, often while denying the pathology of their condition [117]. Furthermore, conscious attention to the ED can exacerbate the condition [25]. For this reason, although clinicians often weigh patients receiving treatment for ED, the patient’s weight is not revealed to them to prevent their fixation upon it [87, 102]. Friends and family also play a crucial role in effective treatment, although well-meaning members of a support network can inadvertently trigger adverse effects simply by asking how well a patient is eating [28, 86, 111]. Given these complexities, the wide variety of tracking of diverse data in the reviewed ED apps may, in fact, be clinically detrimental to a user from the perspective of self-reflection. Furthermore, users may not be keen to inspect large amounts of data, as they may want to discover insights with minimal effort. Presenting summaries of data after long periods of collection has previously led to users reminiscing about past habits, but it did not necessarily help enable future directions for change – a core purpose of reflection [59]. Overall, the ED apps we reviewed do not include appropriate methods and selecting the right amount of collected data that make the data interpretable yet allow for detailed exploration that would not hinder or worsen clinical and functional outcomes.
Design Guidelines:
As mentioned in prior work [31], reflection needs to enable internal examination and exploration of concerning issues, triggered by an experience. For mental health conditions like ED, it must create and clarify meaning of self and lead to changed conceptual perspectives about one’s wellbeing [72]. Individuals should feel supported by self-reflection that helps them challenge how they holistically think and feel about their illness [78], a process referred to as transformative reflection [31, 105]. While the reviewed apps provided many different data types for users to understand and reflect on their ED, supporting these nuanced higher-order meta-cognitive processes relating to the condition needs incorporating alternative design elements. New approaches grounded in user-centered design are necessary to ensure the apps follow systematic guidance to determine the right kinds of information to show a particular user to aid with reflection. Overall, we found that the reviewed apps offered some functionality to discover insights, especially in filtering data and retrieving values. However, apps can integrate more functionality to involve user feedback in determining valuable cuts; users can indicate what cuts they find helpful, and apps can generate similar subsets of data or even predict what may be valuable [59]. In the context of EDs, users could potentially bookmark effective coping strategies or skills or save specific data cuts (e.g., seeing the correlation between meals consumed, meals eaten alone, and disordered behavior) that they find the most insightful [74]. This design decision could reduce their effort needed to interact with the app and get more personalized insight. Importantly, ED treatment requires collaboration and a shared value of treatment goals between a therapist and the patient to be effective [91]. App users may find it hard to make sense of their data by themselves and may benefit with clinician input. However, most apps we reviewed did not have features to share their data with a trusted source. ED apps can include features that promote sharing to facilitate observational learning when integrated with therapy, leading to more motivation towards treatment [45]. Finally, to aid in behavior change, apps can determine a user’s context and present recommendations at opportune moments. Epstein et al. mention that providing real-time recommendations could be inferred from previous days’ behavior [59], and only 1 app (deVicer [8]) demonstrated functionality to predict relapses based on previously entered relapses. This may provide more targeted insights relevant to a user’s goals, but apps need to ensure that this information is clinically valid and accurate to prevent misleading information. Additionally, aggregating data to highlight deviating behavior from their goals and steering users in complementary directions is a more useful approach to aid with reflection. In many ways, the above suggestions consider how data collected by ED apps can act as a reflective practicum [101, 105], a scaffold to help support the reflective process.
6.3. Opportunities to Improve Communication in ED Apps
By providing real-time self-monitoring of eating and associated behaviors, apps are well suited to communicate personal information that can help users understand the progression and severity of their ED [74]. Additionally, the persistent collection of data can support behavior change [77]. However, for reflection to occur, this data needs to be communicated to users through meaningful insights [32]. In personal informatics apps, visualizations are an appropriate method for communicating information as they can convey large quantities of information, help users spot patterns and correlations, and allow for free exploration of data [48]. However, concerning EDs, visualizations can pose several challenges, and our review revealed in Section 5.3, many of the visualization choices adopted by the apps deviated from recommended best practices for succinct and clear communication to end-users. First, visualizations of frequently logged data are challenging to interpret and may overwhelm users considering the amount of data collected [48] – this was a persistent problem noted in our review of the ED apps. Dynamic charts selected by the user can help users receive more targeted insights by aggregating the analytic activity and discovering relevant relationships among triggers, emotional and behavioral responses, and coping strategies [48]. However, the reviewed apps did not allow for such dynamic visualizations. Next, visualizations can communicate specific information about a dataset, such as numeric counts and retrieving specific values [26]. Our review showed that, while many apps did adopt these strategies, conveying information in this detailed manner may have the potential to overwhelm individuals with ED, who tend to have a preoccupation with thoughts about food and eating [91], and are therefore encouraged not to weigh themselves on a scale and misinterpret that reading [91]. As a solution, albeit in a different context, Pousman et al. recognized the challenges of traditional information visualization techniques from the perspective of enabling end-users to derive analytic insights into data [94]. Therefore they proposed expanding the definition of visualizations to include those that blur the boundaries between infovis and other domains, including ubiquitous computing, design, and art. Only two apps – Woebot [20] and 7 Cups [2] adopted such aesthetic strategies to communicate numerical data.
Design Guidelines:
Enhancing information communication’s overall usability is already recognized as an essential consideration when developing best practices for mental health apps [39]. However, beyond usability, as our review revealed, some ED apps can be cluttered with data – thus overwhelming a user in their efforts to discover insights. This is a noted critique of visualizations [100]. Understanding users’ information needs and how they derive meaningful insights through visualized data is critical in designing relevant and practical visualizations [26]. Therefore, app designers should consider the prior knowledge users have about their ED, the learning curve required to understand visualizations, and the time and effort a user might need to place in understanding the visualized data. Cuttone et al. suggest providing a simple visualization as the starting point and then allowing advanced users to increase complexity and details dynamically [48]. Providing this dynamic interaction may also prevent aggregated data from hiding important data or fostering misinterpretations in other contexts [106]. Sarikaya and Gleicher similarly find that adding user interaction elements to support showing less or more detail through zooming in/out or abstracting the data can address a common critique of scatterplots being cluttered [100]. Design attributes such as color, size, position, etc., can also enhance a visualization’s communication ability.
Drawing on these works, we further suggest that app designers employ visualizations that match the users’ information needs and consider augmenting the visualization’s design elements to convey information effectively. Standardized visualizations may have the potential to become “confronting” given their use of metrics and reminders about what, how much, and when one is eating. This may even prompt dissonance, distress, or shame between the “lived” self and the “computed” or “imagined” self [106]. Choe et al.’s study of the data practices of quantifed selfers showed that visualizations of personal data share similar informational goals as traditional info vis (e.g., examining details, identifying trends, making comparisons) but that quantifed selfers engage in activities such as self-reflection that visual representations are often not designed to support directly [44]. Therefore, for understanding users’ concerns and internal conceptions of eating behavior, choosing to employ nontraditional visualizations, as observed in Woebot [20] and 7 Cups of Tea [2], may be better suited, as they can communicate insights and support reflection to end-users in more creative and relevant ways. Nontraditional info vis may also provide opportunities to work around the limitations of standard info vis while engaging users with ED who may not be experts in reading visualizations. Further on the edge of traditional visualization systems, ED app design can draw from conceptualizations of persuasive visualizations that focus on changing peoples’ attitudes [116]. Such alternative design strategies can help users reach personal goals and improve their quality of life. In particular, captology, the study of computers as persuasive technologies [65], explores visualizations as a means to persuade [94]. This approach may be useful, especially when integrated into a positive reinforcement framework, as users, when faced with urges for disordered eating behavior, can receive targeted recommendations on how to utilize coping strategies in moments of distress [74].
6.4. Limitations and Future Research Directions
We note some limitations in this work, which constitute promising directions for future research. First, during the review process, we identified and categorized several apps using a theory-driven approach. While the apps were used exhaustively to collect large amounts of personal data, the judgment of the type of information collected and how these apps support reflection and communication on data was based on the coders’ perspective reviewing the apps. Second, the number of reviewed apps (34) may seem low at first; however, we note that this was the final set following the elimination of non-functional or inactive apps from a set of 55. While many smartphone apps address mental illnesses such as depression and anxiety, a smaller subset focuses on EDs in particular and such apps can be split based on the type of ED they target [74]. Moreover, our final count is comparable to other review studies in ED, e.g., Fairburn and Rothwell, who reviewed 39 ED apps [62]. Finally, we note that this study did not solicit directed feedback from the users of these apps or ED patients, regarding their own perceptions of data collection, reflection, and communication. As we advance, our findings can be complemented by investigations involving clinicians and patients to address several fundamental questions, including what the best practices to communicate data to mental health patients and clinicians are, as well as how can we design app interfaces that increase users’ trust in the treatment process and the therapeutic relationship. Future work can investigate, using user-centered design principles, as proposed by Graham et al. [66], the extent to which our recommended design guidelines meet the design needs of the end-users of these apps. The thorough investigation and organization of the design space presented in this paper overall provide a necessary scaffold for future empirical analysis, e.g., interview data or public community postings.
7. CONCLUSION
Through a three-prong review, this paper contributes an analysis of the current ED app design space: how commercial app developers approach that domain, what they tend to emphasize, and what regions are underexplored. Due to the spectrum of monitored attributes in traditional ED therapy and in ED apps, we approach this from an info vis lens to uncover how user-inputted data is aggregated and presented back to users in commercial ED apps, and whether and how they facilitate reflection around ED. We find that current ED apps collect a variety of data types related to a user’s condition, and these apps vary tremendously in terms of their visualization techniques. However, the design of those visualizations rarely adheres to the best practices and guidelines put forth by prior literature in visualization and personal informatics [26, 59, 60, 80, 98, 100, 107]. Consequently, it remains unclear if the apps are adequately able to empower end-users to self-reflect on their behaviors, a process key to managing ED. By following best practices in information visualization and personal health informatics, and forming an understanding of ED treatment approaches, we discuss how designers can improve the functioning and efficacy of ED apps to ensure they are useful, provide actionable information in a timely and meaningful manner, and yield positive supports to the user in their ED journey.
CCS CONCEPTS.
• Human-centered computing → Empirical studies in HCI; • Applied computing → Health informatics.
ACKNOWLEDGMENTS
This research was supported by grant number #1816403 from the National Science Foundation, awarded to De Choudhury and Baumer.
APPENDIX
Table A1:
List of Reviewed Apps for Eating Disorder Recovery and Mental Wellness Management (as of 30 March, 2020)
| Apps | Platform | Ratings | Purpose | Target User Group | |||
|---|---|---|---|---|---|---|---|
| iOS Rating | #iOS User Ratings | Android Rating | #Android User Ratings | ||||
| Collection Only (4) | |||||||
| Kick the eating disorder out | iOS | 4 | 1 | n/a | n/a | ED Recovery Guide | ED |
| 12 Steps Overeaters Anonymous | iOS, Android | 4.7 | 83 | 4.6 | 374 | Food Journaling | ED |
| Gratitude Journal (Happiness Journal) | iOS, Android | 4.9 | 3600 | 4.8 | 9187 | Mental Wellness Management | Mental Health |
| Booster Buddy | iOS, Android | 4.6 | 97 | 4.4 | 1,431 | Mental Wellness Management | Mental Health |
| Reflection Only (13) | |||||||
| Recovery Record Clinician | iOS, Android | 4.9 | 330 | 4.5 | 31 | Eating Disorder Treatment (for Clincians) | ED |
| GG Body Image | iOS, Android | 4.6 | 41 | 4.6 | 56 | Practicing Body Image Positivity | BI |
| Anorexia Help Calendar | iOS, Android | 1 | 5 | n/a | n/a | ED Recovery Guide | AN |
| Food Addiction Calendar | iOS, Android | 2 | 4 | 2.1 | 14 | Food Addiction Recovery Guide | ED |
| Eating Disorder Guide | Android | n/a | n/a | 3.2 | 12 | ED Recovery Guide | ED |
| Anorexia Nervosa Abnormal ED | Android | n/a | n/a | 3.4 | 9 | ED Recovery Guide | AN |
| Anorexia | Android | n/a | n/a | 3.4 | 5 | ED Recovery Guide | AN |
| Anorexia Recovery Guide | Android | n/a | n/a | n/a | n/a | ED Recovery Guide | AN |
| How To Stop Binge Eating | Android | n/a | n/a | 3.2 | 6 | ED Recovery Guide | BED |
| Stop Binge Eating With Hypnosis | Android | n/a | n/a | 4.1 | 10 | ED Recovery Guide | BED |
| How to Stop Binge Eating - Complete Guide | Android | n/a | n/a | 2.8 | 6 | ED Recovery Guide | BED |
| Overeaters Anonymous Speaker Tapes | iOS | 4.8 | 442 | n/a | n/a | ED Recovery Guide | ED |
| Eating Disorders - Compulsive Overeating | Android | n/a | n/a | 1 | 1 | ED Recovery Guide | ED |
| Both Collection and Reflection (17) | |||||||
| Recovery Record | iOS, Android | 4.9 | 3900 | 4.8 | 6155 | ED Recovery Management | ED |
| Rise Up + Recover | iOS, Android | 4.7 | 177 | 4.5 | 460 | ED Recovery Management | ED |
| CBT Diary | Android | n/a | n/a | 4.2 | 249 | Mental Wellness Management | Mental Health |
| Jourvie | iOS, Android | 3 | 1 | 3.8 | 205 | ED Recovery Management | ED |
| deVicer | Android | n/a | n/a | 3.9 | 49 | ED Recovery Management | BED |
| What’s Up? | iOS, Android | 4.6 | 158 | 4.4 | 3096 | Mental Wellness Management | Mental Health |
| Mindshift CBT | iOS, Android | 4.2 | 60 | 3.9 | 1073 | Mental Wellness Management | Mental Health |
| Nourishly | iOS, Android | 4.9 | 156 | 4.7 | 67 | ED Recovery Management | ED |
| Woebot | iOS, Android | 4.7 | 1900 | 4.8 | 5523 | Mental Wellness Management | Mental Health |
| 7 Cups of Tea | iOS, Android | 3.7 | 1100 | 3.5 | 16375 | Mental Wellness Management | Mental Health |
| Eating Disorder Test | iOS, Android | 4.6 | 10 | 4 | 32 | ED Assessment Tool | ED |
| Blue Buddy | iOS | 5 | 1 | n/a | n/a | ED Recovery Management | ED |
| RealifeChange | iOS | 4.1 | 32 | n/a | n/a | Mental Wellness Management | Mental Health |
| Eating Time - meal reminder | iOS | 4.5 | 103 | n/a | n/a | Food Journaling | ED |
| New Gratitude Journal | iOS | 4.4 | 284 | n/a | n/a | Mental Wellness Management | Mental Health |
| Anorexia and Bulimia therapy - ED Help | Android | n/a | n/a | n/a | n/a | Eating Disorder Counseling | ED |
| DBT Diary Card and Skills Coach | iOS | 4.5 | 85 | n/a | n/a | Mental Wellness Management | Mental Health |
Contributor Information
Anjali Devakumar, Georgia Institute of Technology, Atlanta, GA, USA.
Jay Modh, Georgia Institute of Technology, Atlanta, GA, USA.
Bahador Saket, Georgia Institute of Technology, Atlanta, GA, USA.
Eric P. S. Baumer, Lehigh University, Bethlehem, PA, USA
Munmun De Choudhury, Georgia Institute of Technology, Atlanta, GA, USA.
REFERENCES
- [1].[n.d.]. 12 Steps Overeaters Anonymous on the App Store. https://apps.apple.com/us/app/12-steps-overeaters-anonymous/id708666976
- [2].[n.d.]. 7 Cups: Anxiety & Stress Chat. https://apps.apple.com/us/app/7-cups-anxiety-stress-chat/id921814681
- [3].[n.d.]. Anorexia Nervosa Abnormal Eating Disorder & Habits - Apps on Google Play. https://play.google.com/store/apps/details?id=com.OneLife2Care.AnorexiaNervosa&hl=en&gl=US
- [4].[n.d.]. Anorexia Recovery Guide - Apps on Google Play. https://play.google.com/store/apps/details?id=com.andromo.dev565055.app784133&hl=en&gl=US
- [5].[n.d.]. Blue Buddy on the App Store. https://apps.apple.com/us/app/blue-buddy/id1221007158
- [6].[n.d.]. BoosterBuddy on the App Store. https://apps.apple.com/us/app/boosterbuddy/id906538988
- [7].[n.d.]. CBT Diary - Apps on Google Play. https://play.google.com/store/apps/details?id=pl.com.continuum.cbtbasicemotionsdiary&hl=en_US&gl=US
- [8].[n.d.]. deVicer: 90-Day Binge Eating Disorder Therapy - Apps on Google Play. https://play.google.com/store/apps/details?id=life.devicer.devicer&hl=en_US&gl=US
- [9].[n.d.]. Eating Disorder Guide - Apps on Google Play. https://play.google.com/store/apps/details?id=com.andromo.dev663679.app739196&hl=en&gl=US
- [10].[n.d.]. Eating Disorder Recovery app. https://apps.apple.com/gb/app/eating-disorder-recovery-app/id1477741610
- [11].[n.d.]. GG Positive Body Image on the App Store. https://apps.apple.com/us/app/gg-positive-body-image/id1240093612
- [12].[n.d.]. Gratitude: Diary, Vision Board. https://apps.apple.com/us/app/gratitude-diary-vision-board/id1372575227
- [13].[n.d.]. HOW TO STOP BINGE EATING EFFECTIVELY - Apps on Google Play. https://play.google.com/store/apps/details?id=how.to.stop.binge.eating.hl2&hl=en&gl=US
- [14].[n.d.]. Jourvie. https://apps.apple.com/de/app/jourvie/id1076221598
- [15].[n.d.]. MindShift CBT - Anxiety Relief. https://apps.apple.com/us/app/mindshift-cbt-anxiety-relief/id634684825
- [16].[n.d.]. RealifeChange on the App Store. https://apps.apple.com/us/app/realifechange/id962955498
- [17].[n.d.]. Rise Up + Recover: An Eating Disorder Monitoring and Management Tool for Anorexia, Bulimia, Binge Eating, and EDNOS on the App Store. https://apps.apple.com/us/app/rise-up-recover-eating-disorder-monitoring-management/id509287014
- [18].[n.d.]. RR: Eating Disorder Management on the App Store. https://apps.apple.com/us/app/rr-eating-disorder-management/id457360959
- [19].[n.d.]. What’s Up? - A Mental Health App. https://apps.apple.com/us/app/whats-up-a-mental-health-app/id968251160
- [20].[n.d.]. Woebot - Your Self-Care Expert. https://apps.apple.com/us/app/woebot-your-self-care-expert/id1305375832
- [21].2017. What are Eating Disorders? https://www.nationaleatingdisorders.org/what-are-eating-disorders
- [22].Aardoom Jiska J., Dingemans Alexandra E., and Van Furth Eric F.. 2016. E-Health Interventions for Eating Disorders: Emerging Findings, Issues, and Opportunities. Current Psychiatry Reports 18, 4 (March 2016), 42. 10.1007/s11920-016-0673-6 [DOI] [PubMed] [Google Scholar]
- [23].Albrecht Urs-Vito. 2013. Transparency of health-apps for trust and decision making. Journal of medical Internet research 15, 12 (2013), e277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Ali Kathina, Farrer Louise, Fassnacht Daniel B, Gulliver Amelia, Bauer Stephanie, and Griffiths Kathleen M. 2017. Perceived barriers and facilitators towards help-seeking for eating disorders: A systematic review. International Journal of Eating Disorders 50, 1 (2017), 9–21. [DOI] [PubMed] [Google Scholar]
- [25].Altabe Madeline and Thompson J Kevin. 1996. Body image: A cognitive self-schema construct? Cognitive Therapy and Research 20, 2 (1996), 171–193. [Google Scholar]
- [26].Amar Robert, Eagan James, and Stasko John. [n.d.]. Low-Level Components of Analytic Activity in Information Visualization. ([n. d.]), 7. [Google Scholar]
- [27].Anthes Emily. 2016. Pocket psychiatry: mobile mental-health apps have exploded onto the market, but few have been thoroughly tested. Nature 532, 7597 (2016), 20–24.27078548 [Google Scholar]
- [28].Ata Rheanna N., Ludden Alison Bryant, and Lally Megan M.. 2007. The Effects of Gender and Family, Friend, and Media Influences on Eating Behaviors and Body Image During Adolescence. Journal of Youth and Adolescence 36, 8 (Nov. 2007), 1024–1037. 10.1007/s10964-006-9159-x [DOI] [Google Scholar]
- [29].Bakker David, Kazantzis Nikolaos, Rickwood Debra, and Rickard Nikki. 2016. Mental health smartphone apps: review and evidence-based recommendations for future developments. JMIR mental health 3, 1 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Bauer Stephanie and Moessner Markus. 2013. Harnessing the power of technology for the treatment and prevention of eating disorders. The International Journal of Eating Disorders 46, 5 (July 2013), 508–515. 10.1002/eat.22109 [DOI] [PubMed] [Google Scholar]
- [31].Baumer Eric P. S.. 2015. Reflective Informatics: Conceptual Dimensions for Designing Technologies of Reflection. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems (CHI ‘15). Association for Computing Machinery, New York, NY, USA, 585–594. 10.1145/2702123.2702234 [DOI] [Google Scholar]
- [32].Baumer Eric P. S.. 2015. Usees. In Proc CHI. ACM Press, 3295–3298. 10.1145/2702123.2702147 [DOI] [Google Scholar]
- [33].Baumer Eric P. S., Khovanskaya Vera, Matthews Mark, Reynolds Lindsay, Sosik Victoria Schwanda, and Gay Geri. 2014. Reviewing Reflection: On the Use of Reflection in Interactive System Design. In Proceedings of the ACM Conference on Designing Interactive Systems (DIS). ACM Press, Vancouver, BC, 93–102. 10.1145/2598510.2598598 [DOI] [Google Scholar]
- [34].Ben-Zeev Dror, Brian Rachel M, Aschbrenner Kelly A, Jonathan Geneva, and Steingard Sandra. 2018. Video-based mobile health interventions for people with schizophrenia: Bringing the “pocket therapist” to life. Psychiatric rehabilitation journal 41, 1 (2018), 39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Braun Virginia and Clarke Victoria. 2006. Using thematic analysis in psychology. Qualitative research in psychology 3, 2 (2006), 77–101. [Google Scholar]
- [36].Burgess Eleanor R, Zhang Alice Renwen, Feuston Jessica L, Reddy Madhu C, Ernala Sindhu Kiranmai, De Choudhury Munmun, Schueller Stephen, Aguilera Adrian, and Czerwinski Mary. 2020. Technology Ecosystems: Rethinking Resources for Mental Health. In Extended Abstracts of the 2020 CHI Conference on Human Factors in Computing Systems. 1–8. [Google Scholar]
- [37].Burns Jane M, Durkin Lauren A, and Nicholas Jonathan. 2009. Mental health of young people in the United States: what role can the internet play in reducing stigma and promoting help seeking? Journal of Adolescent Health 45, 1 (2009), 95–97. [DOI] [PubMed] [Google Scholar]
- [38].Cavazos-Rehg Patricia A, Krauss Melissa J, Costello Shaina J, Kaiser Nina, Cahn Elizabeth S, Fitzsimmons-Craft Ellen E, and Wilfley Denise E. 2019. “I just want to be skinny.”: A content analysis of tweets expressing eating disorder symptoms. PloS one 14, 1 (2019), e0207506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Chan Steven, Torous John, Hinton Ladson, and Yellowlees Peter. 2015. Towards a Framework for Evaluating Mobile Mental Health Apps. Telemedicine Journal and E-Health: The Official Journal of the American Telemedicine Association 21, 12 (Dec. 2015), 1038–1041. 10.1089/tmj.2015.0002 [DOI] [PubMed] [Google Scholar]
- [40].Chan Steven Richard, Torous John, Hinton Ladson, and Yellowlees Peter. 2014. Mobile tele-mental health: increasing applications and a move to hybrid models of care. In Healthcare, Vol. 2. Multidisciplinary Digital Publishing Institute, 220–233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Chancellor Stevie, Hu Andrea, and De Choudhury Munmun. 2018. Norms matter: Contrasting social support around behavior change in online weight loss communities. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. 1–14. [Google Scholar]
- [42].Chancellor Stevie, Mitra Tanushree, and De Choudhury Munmun. 2016. Recovery amid pro-anorexia: Analysis of recovery in social media. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems. ACM, 2111–2123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Choe Eun Kyoung and Abdullah Saeed. 2017. A Balanced Approach for Self-Monitoring Applications. (2017), 11.
- [44].Choe Eun Kyoung, Lee Nicole B., Lee Bongshin, Pratt Wanda, and Kientz Julie A.. 2014. Understanding quantified-selfers’ practices in collecting and exploring personal data. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ‘14). Association for Computing Machinery, New York, NY, USA, 1143–1152. 10.1145/2556288.2557372 [DOI] [Google Scholar]
- [45].Clawson James, Pater Jessica A, Miller Andrew D, Mynatt Elizabeth D, and Mamykina Lena. 2015. No longer wearing: investigating the abandonment of personal health-tracking technologies on craigslist. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing. 647–658. [Google Scholar]
- [46].Cordeiro Felicia, Epstein Daniel A., Thomaz Edison, Bales Elizabeth, Jagannathan Arvind K., Abowd Gregory D., and Fogarty James. 2015. Barriers and Negative Nudges: Exploring Challenges in Food Journaling. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems (CHI ‘15). Association for Computing Machinery, New York, NY, USA, 1159–1162. 10.1145/2702123.2702155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Coyle David and Doherty Gavin. 2009. Clinical evaluations and collaborative design: developing new technologies for mental healthcare interventions. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems. 2051–2060. [Google Scholar]
- [48].Cuttone Andrea, Petersen Michael Kai, and Larsen Jakob Eg. 2014. Four Data Visualization Heuristics to Facilitate Reflection in Personal Informatics. In Universal Access in Human-Computer Interaction. Design for All and Accessibility Practice (Lecture Notes in Computer Science), Stephanidis Constantine and Antona Margherita (Eds.). Springer International Publishing, Cham, 541–552. 10.1007/978-3-319-07509-9_51 [DOI] [Google Scholar]
- [49].Davidson Larry and Strauss John S. 1992. Sense of self in recovery from severe mental illness. Psychology and Psychotherapy: Theory, Research and Practice 65, 2 (1992), 131–145. [DOI] [PubMed] [Google Scholar]
- [50].Davies Madlen. 2015. From healthy to tube fed in just five months: Teenager develops anorexia after becoming obsessed with calorie counting app. In Daily mail. [Google Scholar]
- [51].De Choudhury Munmun. 2015. Anorexia on Tumblr: A Characterization Study. In Proceedings of the 5th International Conference on Digital Health 2015. ACM, 43–50. [Google Scholar]
- [52].Doherty Gavin, Coyle David, and Matthews Mark. 2010. Design and evaluation guidelines for mental health technologies. Interacting with computers 22, 4 (2010), 243–252. [Google Scholar]
- [53].Donker Tara, Petrie Katherine, Proudfoot Judy, Clarke Janine, Birch Mary-Rose, and Christensen Helen. 2013. Smartphones for smarter delivery of mental health programs: a systematic review. Journal of medical Internet research 15, 11 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].Eikey Elizabeth V. 2016. Privacy and weight loss apps: a first look at how women with eating disorders use social features. In Proceedings of the 19th International Conference on Supporting Group Work. 413–415. [Google Scholar]
- [55].Eikey Elizabeth V. 2016. Providers’ Perceptions of the Impact of Weight Loss Apps on Users with Eating Disorders. In Proceedings of the 2016 ACM SIGMIS Conference on Computers and People Research. 19–20. [Google Scholar]
- [56].Eikey Elizabeth V, Chen Yunan, and Zheng Kai. 2019. Do Recovery Apps Even Exist?: Why College Women with Eating Disorders Use (But Not Recommend) Diet and Fitness Apps Over Recovery Apps. In International Conference on Information. Springer, 727–740. [Google Scholar]
- [57].Eikey Elizabeth V and Reddy Madhu C. 2017. “ It’s Definitely Been a Journey” A Qualitative Study on How Women with Eating Disorders Use Weight Loss Apps. In Proceedings of the 2017 CHI conference on human factors in computing systems. 642–654. [Google Scholar]
- [58].Eikey Elizabeth Victoria, Reddy Madhu C, Booth Kayla M, Kvasny Lynette, Blair Johnna L, Li Victor, and Poole Erika S. 2017. Desire to be underweight: Exploratory study on a weight loss app community and user perceptions of the impact on disordered eating behaviors. JMIR mHealth and uHealth 5, 10 (2017), e150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Epstein Daniel, Cordeiro Felicia, Bales Elizabeth, Fogarty James, and Munson Sean. 2014. Taming Data Complexity in Lifelogs: Exploring Visual Cuts of Personal Informatics Data. In Proceedings of the ACM Conference on Designing Interactive Systems (DIS). ACM, Vancouver, BC, 667–676. 10.1145/2598510.2598558 [DOI] [Google Scholar]
- [60].Epstein Daniel A., Ping An, Fogarty James, and Munson Sean A.. 2015. A lived informatics model of personal informatics. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing - UbiComp ‘15. ACM Press, Osaka, Japan, 731–742. [Google Scholar]
- [61].Fairburn Christopher G, Hay Phillipa J, and Welch Sarah L. 1993. Binge eating and bulimia nervosa: Distribution and determinants. (1993).
- [62].Fairburn Christopher G and Rothwell Emily R. 2015. Apps and eating disorders: A systematic clinical appraisal. International Journal of Eating Disorders 48, 7 (2015), 1038–1046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [63].Feuston Jessica L and Piper Anne Marie. 2019. Everyday experiences: small stories and mental illness on Instagram. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems. 1–14. [Google Scholar]
- [64].Fleck Rowanne and Fitzpatrick Geraldine. 2010. Reflecting on reflection: framing a design landscape. In Proceedings of the 22nd Conference of the Computer-Human Interaction Special Interest Group of Australia on Computer-Human Interaction (OZCHI ‘10). Association for Computing Machinery, New York, NY, USA, 216–223. 10.1145/1952222.1952269 [DOI] [Google Scholar]
- [65].Fogg BJ. 1998. Persuasive computers: perspectives and research directions. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ‘98). ACM Press/Addison-Wesley Publishing Co., USA, 225–232. 10.1145/274644.274677 [DOI] [Google Scholar]
- [66].Graham Andrea K, Wildes Jennifer E, Reddy Madhu, Munson Sean A, Taylor C Barr, and Mohr David C. 2019. User-centered design for technology-enabled services for eating disorders. International Journal of Eating Disorders 52, 10 (2019), 1095–1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].Griffiths Scott, Rossell Susan L, Mitchison Deborah, Murray Stuart B, and Mond Jonathan M. 2018. Pathways into treatment for eating disorders: A quantitative examination of treatment barriers and treatment attitudes. Eating disorders 26, 6 (2018), 556–574. [DOI] [PubMed] [Google Scholar]
- [68].Hart Laura M, Granillo M Teresa, Jorm Anthony F, and Paxton Susan J. 2011. Unmet need for treatment in the eating disorders: a systematic review of eating disorder specific treatment seeking among community cases. Clinical psychology review 31, 5 (2011), 727–735. [DOI] [PubMed] [Google Scholar]
- [69].Hermsen Sander, Moons Jonas, Kerkhof Peter, Wiekens Carina, and De Groot Martijn. 2017. Determinants for sustained use of an activity tracker: observational study. JMIR mHealth and uHealth 5, 10 (2017), e164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [70].Hilbert Anja, Hoek Hans W, and Schmidt Ricarda. 2017. Evidence-based clinical guidelines for eating disorders: international comparison. Current opinion in psychiatry 30, 6 (2017), 423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [71].Honary Mahsa, Bell Beth, Clinch Sarah, Wild Sarah, and McNaney Roisin. 2019. Understanding the Role of Healthy Eating and Fitness Mobile Apps in the Formation of Maladaptive Eating and Exercise Behaviors in Young People. JMIR mHealth and uHealth 7 (June 2019), e14239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [72].Hsu LK, Crisp Arthur H, and Callender John S. 1992. Recovery in anorexia nervosa—the patient’s perspective. International Journal of Eating Disorders 11, 4 (1992), 341–350. [Google Scholar]
- [73].Jacobi Corinna, Hayward Chris, de Zwaan Martina, Kraemer Helena C, and Agras W Stewart. 2004. Coming to terms with risk factors for eating disorders: application of risk terminology and suggestions for a general taxonomy. Psychological bulletin 130, 1 (2004), 19. [DOI] [PubMed] [Google Scholar]
- [74].Juarascio Adrienne S, Manasse Stephanie M, Goldstein Stephanie P, Forman Evan M, and Butryn Meghan L. 2015. Review of smartphone applications for the treatment of eating disorders. European Eating Disorders Review 23, 1 (2015), 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [75].Kay Matthew, Morris Dan, schraefel mc, and Kientz Julie A.. 2013. There’s no such thing as gaining a pound: reconsidering the bathroom scale user interface. In Proceedings of the 2013 ACM international joint conference on Pervasive and ubiquitous computing (UbiComp ‘13). Association for Computing Machinery, New York, NY, USA, 401–410. 10.1145/2493432.2493456 [DOI] [Google Scholar]
- [76].Kazdin Alan E, Fitzsimmons-Craft Ellen E, and Wilfley Denise E. 2017. Addressing critical gaps in the treatment of eating disorders. International Journal of Eating Disorders 50, 3 (2017), 170–189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [77].Kelley Christina, Lee Bongshin, and Wilcox Lauren. 2017. Self-tracking for mental wellness: understanding expert perspectives and student experiences. In Proceedings of the 2017 CHI conference on human factors in computing systems. 629–641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [78].Keski-Rahkonen Anna and Tozzi Federica. 2005. The process of recovery in eating disorder sufferers’ own words: An Internet-based study. International Journal of Eating Disorders 37, S1 (2005). [DOI] [PubMed] [Google Scholar]
- [79].Khovanskaya Vera, Baumer Eric PS, Cosley Dan, Voida Stephen, and Gay Geri. 2013. “ Everybody knows what you’re doing” a critical design approach to personal informatics. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems. 3403–3412. [Google Scholar]
- [80].Kim Younghoon and Heer Jeffrey. 2018. Assessing Effects of Task and Data Distribution on the Effectiveness of Visual Encodings. Computer Graphics Forum 37, 3 (June 2018), 157–167. 10.1111/cgf.13409 [DOI] [Google Scholar]
- [81].Koshy Kiron, Limb Christopher, Gundogan Buket, Whitehurst Katharine, and Jafree Daniyal J. 2017. Reflective practice in health care and how to reflect effectively. International journal of surgery. Oncology 2, 6 (2017), e20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [82].Li Ian, Dey Anind, and Forlizzi Jodi. 2010. A Stage-Based Model of Personal Informatics Systems. In Proc CHI. Atlanta, GA, 557–566. [Google Scholar]
- [83].Mackinlay Jock. 1986. Automating the design of graphical presentations of relational information. ACM Transactions on Graphics 5, 2 (April 1986), 110–141. 10.1145/22949.22950 [DOI] [Google Scholar]
- [84].Mahdawi Arwa. 2014. The unhealthy side of wearable fitness devices. The Guardian 3 (2014). [Google Scholar]
- [85].Mann Karen, Gordon Jill, and MacLeod Anna. 2009. Reflection and reflective practice in health professions education: a systematic review. Advances in health sciences education 14, 4 (2009), 595–621. [DOI] [PubMed] [Google Scholar]
- [86].McMaster Rose, Beale Barbara, Hillege Sharon, and Nagy Sue. 2004. The Parent Experience of Eating Disorders: Interactions with Health Professionals. International Journal of Mental Health Nursing 13, 1 (March 2004), 67–73. 10.1111/j.1447-0349.2004.00310.x [DOI] [PubMed] [Google Scholar]
- [87].Mercurio Andrea and Rima Brandi. 2011. Watching My Weight: Self-Weighing, Body Surveillance, and Body Dissatisfaction. Sex Roles 65, 1–2 (July 2011), 47–55. 10.1007/s11199-011-9980-x [DOI] [Google Scholar]
- [88].Mohr David C, Burns Michelle Nicole, Schueller Stephen M, Clarke Gregory, and Klinkman Michael. 2013. Behavioral intervention technologies: evidence review and recommendations for future research in mental health. General hospital psychiatry 35, 4 (2013), 332–338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [89].Mohr David C, Weingardt Ken R, Reddy Madhu, and Schueller Stephen M. 2017. Three problems with current digital mental health research… and three things we can do about them. Psychiatric services 68, 5 (2017), 427–429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [90].Murnane Elizabeth L, Huffaker David, and Kossinets Gueorgi. 2015. Mobile health apps: adoption, adherence, and abandonment. In Adjunct Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2015 ACM International Symposium on Wearable Computers. 261–264. [Google Scholar]
- [91].Murphy Rebecca, Straebler Suzanne, Cooper Zafra, and Fairburn Christopher G.. 2010. Cognitive Behavioral Therapy for Eating Disorders. The Psychiatric Clinics of North America 33, 3 (Sept. 2010), 611–627. 10.1016/j.psc.2010.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [92].Neary Martha and Schueller Stephen M. 2018. State of the field of mental health apps. Cognitive and Behavioral Practice 25, 4 (2018), 531–537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [93].Pater Jessica A, Haimson Oliver L, Andalibi Nazanin, and Mynatt Elizabeth D. 2016. “Hunger Hurts but Starving Works” Characterizing the Presentation of Eating Disorders Online. In Proceedings of the 19th ACM Conference on Computer-Supported Cooperative Work & Social Computing. 1185–1200. [Google Scholar]
- [94].Pousman Zachary, Stasko John, and Mateas Michael. 2007. Casual Information Visualization: Depictions of Data in Everyday Life. IEEE Transactions on Visualization and Computer Graphics 13, 6 (Nov. 2007), 1145–1152. 10.1109/TVCG.2007.70541 [DOI] [PubMed] [Google Scholar]
- [95].Powell Adam C, Landman Adam B, and Bates David W. 2014. In search of a few good apps. Jama 311, 18 (2014), 1851–1852. [DOI] [PubMed] [Google Scholar]
- [96].Powell Adam C, Torous John, Chan Steven, Raynor Geoffrey Stephen, Shwarts Erik, Shanahan Meghan, and Landman Adam B. 2016. Interrater Reliability of mHealth App Rating Measures: Analysis of Top Depression and Smoking Cessation Apps. JMIR mHealth and uHealth 4, 1 (Feb. 2016). 10.2196/mhealth.5176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [97].Rathbone Amy Leigh, Clarry Laura, and Prescott Julie. 2017. Assessing the efficacy of mobile health apps using the basic principles of cognitive behavioral therapy: systematic review. Journal of medical Internet research 19, 11 (2017), e399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [98].Saket Bahador, Endert Alex, and Demiralp Cagatay. 2019. Task-Based Effectiveness of Basic Visualizations. IEEE Transactions on Visualization and Computer Graphics 25, 7 (July 2019), 2505–2512. https://ieeexplore.ieee.org/document/8354901/ [DOI] [PubMed] [Google Scholar]
- [99].Saraiya Purvi, North Chris, and Duca Karen. 2005. An insight-based methodology for evaluating bioinformatics visualizations. IEEE transactions on visualization and computer graphics 11, 4 (2005), 443–456. [DOI] [PubMed] [Google Scholar]
- [100].Sarikaya Alper and Gleicher Michael. 2018. Scatterplots: Tasks, Data, and Designs. IEEE Transactions on Visualization and Computer Graphics 24, 1 (Jan. 2018), 402–412. 10.1109/TVCG.2017.2744184 [DOI] [PubMed] [Google Scholar]
- [101].Schön Donald A.. 1983. The Reflective Practitioner. Basic Books, New York. [Google Scholar]
- [102].Shafran Roz, Fairburn Christopher G., Robinson Paul, and Lask Bryan. 2004. Body Checking and Its Avoidance in Eating Disorders. International Journal of Eating Disorders 35, 1 (Jan. 2004), 93–101. 10.1002/eat.10228 [DOI] [PubMed] [Google Scholar]
- [103].Shen Nelson, Levitan Michael-Jane, Johnson Andrew, Bender Jacqueline Lorene, Hamilton-Page Michelle, Jadad Alejandro Alex R., and Wiljer David. 2015. Finding a depression app: a review and content analysis of the depression app marketplace. JMIR mHealth and uHealth 3, 1 (Feb. 2015), e16. 10.2196/mhealth.3713 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [104].Shingleton Rebecca M., Richards Lauren K., and Thompson-Brenner Heather. 2013. Using Technology Within the Treatment of Eating Disorders: A Clinical Practice Review. Psychotherapy (Chicago, Ill.) 50, 4 (Dec. 2013). 10.1037/a0031815 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [105].Slovák Petr, Frauenberger Christopher, and Fitzpatrick Geraldine. 2017. Reflective Practicum: A Framework of Sensitising Concepts to Design for Transformative Reflection. In Proceedings of the ACM Conference on Human Factors in Computing Systems (CHI). ACM, Denver, CO, 2696–2707. 10.1145/3025453.3025516 [DOI] [Google Scholar]
- [106].Snyder Jaime, Murnane Elizabeth, Lustig Caitie, and Voida Stephen. 2019. Visually Encoding the Lived Experience of Bipolar Disorder. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems. ACM, Glasgow Scotland Uk, 1–14. 10.1145/3290605.3300363 [DOI] [Google Scholar]
- [107].Spence Ian and Lewandowsky Stephan. 1991. Displaying proportions and percentages. Applied Cognitive Psychology 5, 1 (1991), 61–77. 10.1002/acp.2350050106 [DOI] [Google Scholar]
- [108].Spruijt-Metz Donna, Hekler Eric, Saranummi Niilo, Intille Stephen, Korhonen Ilkka, Nilsen Wendy, Rivera Daniel E, Spring Bonnie, Michie Susan, Asch David A, et al. 2015. Building new computational models to support health behavior change and maintenance: new opportunities in behavioral research. Translational behavioral medicine 5, 3 (2015), 335–346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [109].Stice Eric. 2002. Risk and maintenance factors for eating pathology: a meta-analytic review. Psychological bulletin 128, 5 (2002), 825. [DOI] [PubMed] [Google Scholar]
- [110].Stice Eric, Marti C. Nathan, and Rohde Paul. 2013. Prevalence, Incidence, Impairment, and Course of the Proposed DSM-5 Eating Disorder Diagnoses in an 8-Year Prospective Community Study of Young Women. Journal of abnormal psychology 122, 2 (May 2013), 445–457. 10.1037/a0030679 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [111].Tiller Jane M., Sloane Gaynor, Schmidt Ulrike, Troop Nicholas, Power Michael, and Treasure Janet L.. 1997. Social Support in Patients with Anorexia Nervosa and Bulimia Nervosa. International Journal of Eating Disorders 21, 1 (Jan. 1997), 31–38. [DOI] [PubMed] [Google Scholar]
- [112].Torous John, Andersson Gerhard, Bertagnoli Andrew, Christensen Helen, Cuijpers Pim, Firth Joseph, Haim Adam, Hsin Honor, Hollis Chris, Lewis Shôn, et al. 2019. Towards a consensus around standards for smartphone apps and digital mental health. World Psychiatry 18, 1 (2019), 97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [113].Torous John and Firth Joseph. 2016. The digital placebo effect: mobile mental health meets clinical psychiatry. The Lancet Psychiatry 3, 2 (2016), 100–102. [DOI] [PubMed] [Google Scholar]
- [114].Torous John, Nicholas Jennifer, Larsen Mark E, Firth Joseph, and Christensen Helen. 2018. Clinical review of user engagement with mental health smartphone apps: evidence, theory and improvements. Evidence-based mental health 21, 3 (2018), 116–119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [115].Tregarthen Jenna P., Lock James, and Darcy Alison M.. 2015. Development of a smartphone application for eating disorder self-monitoring. The International Journal of Eating Disorders 48, 7 (Nov. 2015), 972–982. 10.1002/eat.22386 [DOI] [PubMed] [Google Scholar]
- [116].Valle A. 2005. The Persuasive Mirror : computerized persuasion for healthy living.
- [117].Vandereycken Walter. 2006. Denial of Illness in Anorexia Nervosa—a Conceptual Review: Part 1 Diagnostic Significance and Assessment. European Eating Disorders Review 14, 5 (Sept. 2006), 341–351. 10.1002/erv.721 [DOI] [Google Scholar]
- [118].Walker Morgan, Thornton Laura, De Choudhury Munmun, Teevan Jaime, Bulik Cynthia M, Levinson Cheri A, and Zerwas Stephanie. 2015. Facebook use and disordered eating in college-aged women. Journal of Adolescent Health 57, 2 (2015), 157–163. [DOI] [PMC free article] [PubMed] [Google Scholar]