

Abstract
Osteoarthritis (OA) has been investigated as one of important target diseases for regenerative medicine. The concept of early OA has recently emerged under the assumption that if OA is detected and intervened early, progression of OA might be arrested or delayed before irreversible destruction of the joint occurs. This concept also matters in regenerative medicine for OA because new regenerative technologies can work better when joint damage is minimal. Diagnostic criteria for early OA have been suggested in this background to find a group of patients who have a higher possibility of developing full-blown OA. However, as currently suggested criteria of early OA are mostly expert opinions lacking higher level of evidence, clinical validations are necessary to prove their value in patient care. While new treatment methods that can suppress or prevent symptoms at an early stage of OA before progressive and irreversible changes occur are being developed, detailed definition and classification of early OA agreed upon by major stakeholders in OA field and validated by prospective studies are necessary to prove the efficacy of these methods. As clinical outcome of regenerative treatment is related to patient characteristics and the status of the whole joint, it is of critical significance to predict which patient will progress and who will be responsive to regenerative treatment. While diagnostic criteria for early OA should be highly sensitive and applicable without employing biomarkers or magnetic resonance imaging, a subclassification and comprehensive endotyping /phenotyping using these techniques might be needed to detect the population who would be responsive to regenerative medicine.
Keywords: Early osteoarthritis, Regenerative medicine, Validation
Significance of defining early osteoarthritis
Osteoarthritis (OA) is diagnosed based on history taking and physical examination plus radiographic changes, typically in those aged more than 50 years old. Joint pain is the principal symptom of OA, accompanied by joint stiffness, crepitus, and other functional limitations. Radiological changes include osteophytes and joint space narrowing, which correspond to Kellgren and Lawrence stages 2–4 [1, 2]. Diagnostic criteria for OA of hip and knee were first proposed by American College of Rheumatology (ACR), which combine clinical, laboratory, and radiographic findings [3, 4]. As these criteria were developed in order to distinguish OA from inflammatory arthropathies and thus provide a uniform system in reporting OA for interventional or epidemiological studies rather than apply for patent care, they are better suited for diagnosing late-stage OA rather than early-stage disease [5].
Considering that the progression of OA takes a long-time, a large opportunity potentially exists to change its natural courses (Fig. 1). If detected and intervened early, OA progression might be arrested or delayed well before irreversible destruction of the joint occurs. This concept for early diagnosis and treatment in OA was largely inspired by the experience in rheumatoid arthritis (RA). Early diagnosis and management strategies for RA have dramatically reduced patient illness and associated costs in the last decades. While etiologies and natural courses are of OA and RA are quite different, the strategy of early diagnosis and intervention is expected to improve outcomes and reduce disability and social burden caused by OA [5]. If OA is managed properly at an early stage when structural damage is not pronounced and the disease process is still reversible, eventual direct and indirect costs of OA might be much lower than currently ones. This concept of early OA can be important for regenerative medicine as well because new regenerative technologies can work better when the joint damage is minimal.
Fig. 1.
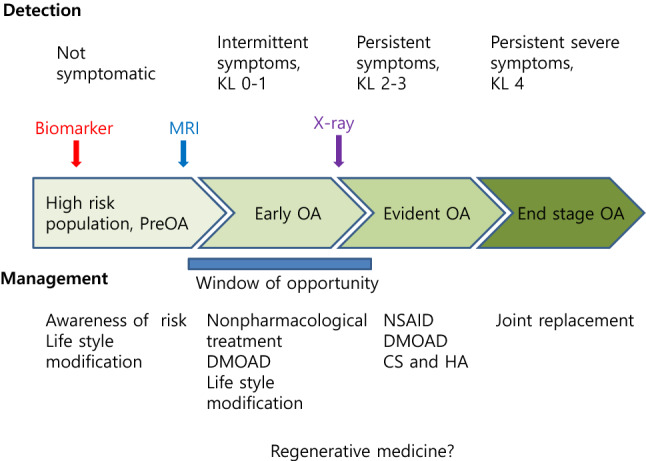
Schema showing the progression of OA. Early OA presents the window of opportunity to arrest the progression and thus change the natural course of the disease before OA becomes clinically manifest. Biochemical markers and MRI can be useful for detecting early OA. Regenerative medicine may have a role in early OA as well as in clinically evident OA
Diagnostic criteria for early OA have been suggested in this background to find a group of patients who have a higher possibility of developing overt OA. With the emergence of biological treatments including regenerative medicine, the identification of at-risk and responder populations is necessary, which will contribute to the establishment of personalized medicine in OA [6]. As is the case for early detection of other disorders, the detection of early OA should be highly sensitive with reasonable specificity.
Currently suggested definitions of early OA
The progression of OA constitutes a continuous process from healthy condition to the earliest appearance of biomarkers from body fluids or from non-invasive imaging without any clinically relevant symptoms or signs, then to symptomatic early OA, established OA, and eventually advanced disease [7]. Defining early OA is necessary not only for identifying and treating the population properly with a high chance of progression, but also for designing clinical trials of new treatments in a better way [6]. Expectably, diagnosing early OA is trickier and more complicated than diagnosing established OA. Characteristic signs and symptoms do not fully show up in the early period. They appear rather partially and sporadically. Typical findings of established OA are not present in simple radiographs of early OA patients. Magnetic resonance imaging (MRI), an expensive technology not readily available for primary physicians, can show a wide spectrum of pathological changes of whole joint tissues in early OA. Arthroscopy is an invasive tool which is seldom used for diagnosis only. While arthroscopy is mostly out of reach for primary physicians including rheumatologists, it can nevertheless provide direct visual evidence of changes in cartilage, meniscus, and synovial tissue [8].
Luyten et al. first proposed that early knee OA was present if the following three conditions were present [6]: (1) pain in the knee, (2) Kellgren and Lawrence (K&L) grade 0 or 1 or 2 (osteophytes only) in standard radiographs, and (3) meeting at least one of the two following structural criteria: (i) arthroscopic findings of cartilage lesions, (ii) MRI findings demonstrating articular cartilage degeneration and/or meniscal degeneration and/or subchondral bone marrow lesions. Years later, in the Italian Rheumatology Association International Initiative, early symptomatic knee OA (ESKOA) was defined when a patient had one of the following: (1) two mandatory symptoms (knee pain in the absence of any recent trauma/injury and very short joint stiffness, lasting for less than 10 min at the start of movement) even in the absence of risk factors, (2) knee pain and 1 or 2 risk factors, (3) three or more risk factors in the presence of at least one mandatory symptom, with symptoms lasting less than 6 months without active inflammatory arthritis, generalized pain, KL grade > 0, any recent knee trauma or injury, and less than 40 years of age [8, 9].
In the first International Early OA Workshop held in Kyoto in 2014, more refined criteria of early OA were announced [10]. The criteria require that three classes should be met to have an early OA: (1) pain, symptoms/signs, self-reported function, and quality of life using tools such as Knee Injury and Osteoarthritis Outcome Score (KOOS): scoring ≤ 85% in at least 2 out of these 4 categories; (2) clinical examination: at least one present out of joint line tenderness or crepitus; (3) knee radiographs: KL grade of 0 or 1 (Table 1). MRI was not adopted in these criteria because of the lack of established consensus on typical findings. Biomarkers were also excluded due to poor level of evidence at that time [5, 10]. Exclusion of MRI and biomarkers makes these criteria readily available to primary care physicians. These criteria showed encouraging performance characteristics with regard to an enrichment for structural and clinical progression using longitudinal Osteoarthritis Initiative data. Inclusion of knee effusion and Heberden’s nodes enhanced the predictive performance of the originally proposed criteria [11]. Because these suggested criteria are mostly expert opinions lacking higher levels of evidence (level 5), clinical validations are necessary to prove its value in patient care. Several groups including Osteoarthritis Research Society International (OARSI) are now developing renewed criteria.
Table 1.
Summary of proposed diagnostic criteria for early OA
| Symptoms and signs | Radiographic signs in standard radiographs | Additional items | Diagnostic criteria | Reference |
|---|---|---|---|---|
| Pain in the knee | KL grade 0–2 (osteophytes only) |
(1) arthroscopic findings of cartilage lesions (2) MRI: articular cartilage degeneration and/or meniscal degeneration and/or subchondral bone marrow lesions |
Knee pain and radiological finding plus arthroscopic or MRI finding | Luyten et al. [6] |
|
Two mandatory symptoms: -knee pain in the absence of any recent trauma/injury - very short joint stiffness, lasting for less than 10 min at the start of movement |
KL grade 0 |
-Without active inflammatory arthritis or generalized pain -More than 50 years -More than 40 years if at least one risk factor present -Absence of any recent trauma or injury -Risk factors: Overweight (body mass index >25) Family history of OA Previous knee injury Malalignment Lower limbs dissymmetry OA in other sites Metabolic syndrome Not being ready to run or walk fast after a period of inactivity |
(1) Two mandatory symptoms (2) Knee pain and 1 or 2 risk factors (3) Three or more risk factors in the presence of at least one mandatory symptom |
Italian Rheumatology Association International Initiative [9] |
|
(1) Pain, symptoms/signs, self-reported function, and quality of life using tools such as KOOS (2) Clinical examination: at least one present out of joint line tenderness or crepitus; |
KL grade 0 or 1 | Patient-based questionnaires using KOOS: scoring ≤ 85% in at least 2 out of 4 subscale | KOO score, clinical examination and radiological finding | International Early OA Workshop in Kyoto [10] |
Clinical aspects of early OA
Risk factors of early OA
Any deviation from proper joint biomechanics can cause early OA. Those who have sustained anterior cruciate ligament (ACL) or meniscal injuries have a higher chance of developing early OA [6, 8]. Knee ligaments injuries cause joint instability, leading to articular cartilage (AC) damage. Even with a successful ACL reconstruction, injured patients have persistently increased risk of developing OA [12]. Meniscal injury increases the chance of AC damage and subsequent early OA due to reduced shock-absorbing function [13]. Any additional loading to the joint from strenuous physical activity, overweight, or axial malalignment can increase the risk of developing early OA [8].
Pain in early OA
Joint pain in early OA is sporadic and self-limited compared with that in established OA. Pain usually precedes radiographic changes by 2–3 years [14]. Patients typically complain of intermittent diffuse joint pain after strenuous exercise and light crepitation. They often complain of pain when climbing stairs as the first symptom. Kneeling, squatting, and repetitive loading in sports activity can cause a sensation of pain. Joint swelling is also frequently experienced [8].
Radiological findings of early OA
Evidence of definite joint space narrowing rules out the diagnosis of early OA. MRI is highly sensitive in detecting early OA. Bone marrow and soft tissue changes including meniscal degeneration, synovial thickening and loss of cruciate ligaments can be demonstrated. While visualization of AC is not very satisfactory due to a low resolution of MRI, newer techniques of detecting biochemical changes make it possible to detect early OA. Glycosaminoglycan content in AC can be assessed using T2 mapping or advanced techniques including delayed gadolinium-enhanced MRI (dGEMRIC). While the cost of MRI makes it difficult to be included in diagnostic criteria available to primary physicians at this time, it is nevertheless urgent and important to establish MRI criteria for early OA based on broad consensus and prospective observation [8].
Biomarkers in early OA
Biomarkers can reflect metabolic processes of collagen, aggrecan, and other non-collagenous proteins. As biochemical changes precede morphological changes based on imaging studies, biomarkers might have a potential to detect early OA and predict prognosis in patients without overt disease [8].
As of now, no single OA biomarker has been found to be an outstanding gold standard or has been adequately validated for clinical applications. Among various OA biomarkers, urinary C-terminal telopeptide of collagen type II (uCTX-II) and serum cartilage oligomeric protein (COMP) present possibility to be indicators for the presence, incidence, and progression of early knee OA as demonstrated from the analysis of 10 biomarkers of OA in a longitudinal cohort study of 1002 subjects in the Netherlands (CHECK, Table 2) [15]. Combination of biomarkers and imaging parameters into single diagnostic panels may be developed to screen the patients who have incipient OA.
Table 2.
Biomarkers tested for early OA in CHECK study [15]
| Target OA process | Biochemical marker |
|---|---|
| Cartilage degradation | Urinary C-terminal telopeptide of collagen type II (uCTX-II), serum cartilage oligomeric protein (COMP) |
| Cartilage synthesis |
Serum N-propeptide of collagen IIA (PIIANP), Serum chondroitin sulfate 846 (sCS846) |
| Subchondral bone degradation |
Urinary C-terminal cross-linking telopeptides of type I collagen (uCTX-I), Urinary N-terminal cross-linking telopeptides of type I collagen (uNTX-I) |
| Subchondral bone synthesis | Serum procollagen type I N-terminal propeptide (sPINP), serum osteocalcin (sOC), |
| Synovial tissue synthesis | Serum N-terminal type III procollagen propeptide of (S-PIIINP), |
| Synovial tissue degradation and/or activity | Serum hyaluronic acid (sHA) |
| Cartilage and bone degradation | Serum cleavage of type I and type II collagen (sC1,2 C) |
Early OA and Pre-OA
One of the concepts that need to be distinguished from early OA is pre-osteoarthritis (pre-OA) [16]. It is different from early OA in that it is not associated with symptoms or signs of OA. The concept of preOA originated from the long-term observation of chondral lesions in sports injuries such as ACL tear and meniscal injuries [17, 18]. As it is not symptomatic, pre-OA is diagnosed from MRI or arthroscopy for sports injuries. When pre-OA becomes symptomatic, it can evolve into early OA. While it would be difficult to persuade the patient for treatment when the disease is not symptomatic, regenerative medicine may provide a possible option with the occurrence of symptoms. As not all pre-OA will become symptomatic and not all symptomatic patients develop advanced OA, it would be very helpful to predict which patients will progress from radiologic or biochemical markers. Future research should focus on the development of biomarkers that can differentiate progressors from non-progressors.
Implication of early OA to regenerative medicine
With emerging interest in regenerative medicine, new therapeutic modalities based on biological treatment are being investigated to treat OA. While the clinical outcome of regenerative treatment is not well-established and unpredictable, it is definitely related to the patient profile and the status of the whole joint. In order to find patients at risk and responders to certain treatments, it is very important and necessary to define and classify patients with early OA [7, 19]. Given that not all early OA will progress into advanced OA and that regenerative medicine has a feature of personalized medicine, it would be of utmost significance to predict which patient will progress and who will be responsive to regenerative treatment.
While diagnostic criteria for early OA should be highly sensitive and applicable without employing biomarker or MRI, a subclassification and comprehensive endotyping /phenotyping using these techniques may be employed to detect the population who would be responsive to regenerative medicine as well as rapid progressor who should be more closely monitored [7].
Currently, regenerative medicine has been applied to patients who have clinically evident, but not end-stage OA (KL2-3) with a hope that it would induce structural changes and thus reverse the progression of disease. However, there are very few evidences, available from well-controlled studies, that support the concept. It can be suggested that clinically evident OA in some patents is an already-advanced disease not quite amenable even to regenerative treatment. When combined with the concept of endotype /phenotype, the regenerative medicine may also be provided to selected patients in earlier stage disease before significant destruction of AC occurs. Considering that regenerative medicine is a costly treatment modality, choosing proper candidates (based on further endotyping /phenotyping) will be a very critical issue in the clinical application of the modality in early OA patients.
Conclusion
Regenerative medicine for OA may target and work more effectively for early stage of the disease before progressive and irreversible changes occur. Detailed definition and classification of early OA validated by prospective study will be necessary to detect the population who would be good candidates for regenerative medicine.
Acknowledgements
Funding was provided by Korea Health Industry Development Institute (Grant No. HI20C0090) and National research Foundation of Korea (Grant No. NRF-2020R1A2C2008266).
Declarations
Conflict of interest
None.
Ethical Statement
There are no animal experiements carried out for this article.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494–502. doi: 10.1136/ard.16.4.494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Risberg MA, Holm I, Tjomsland O, Ljunggren E, Ekeland A. Prospective study of changes in impairments and disabilities after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1999;29:400–12. doi: 10.2519/jospt.1999.29.7.400. [DOI] [PubMed] [Google Scholar]
- 3.Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and therapeutic criteria committee of the American Rheumatism Association. Arthritis Rheum. 1986;29:1039–49. doi: 10.1002/art.1780290816. [DOI] [PubMed] [Google Scholar]
- 4.Altman R, Alarcón G, Appelrouth D, Bloch D, Borestein D, Brandt K, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991;34:505–14. doi: 10.1002/art.1780340502. [DOI] [PubMed] [Google Scholar]
- 5.Kanamoto T, Mae T, Yokoyama T, Tanaka H, Ebina K, Nakata K. Significance and definition of early knee osteoarthritis. Ann Joint. 2020;5:4. doi: 10.21037/aoj.2019.09.02. [DOI] [Google Scholar]
- 6.Luyten FP, Denti M, Filardo G, Kon E, Engebretsen L. Definition and classification of early osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc. 2012;20:401–6. doi: 10.1007/s00167-011-1743-2. [DOI] [PubMed] [Google Scholar]
- 7.Mahmoudian A, Lohmander LS, Mobasheri A, Englund M, Luyten FP. Early-stage symptomatic osteoarthritis of the knee - time for action. Nat Rev Rheumatol. 2021;17:621–32. doi: 10.1038/s41584-021-00673-4. [DOI] [PubMed] [Google Scholar]
- 8.Madry H, Kon E, Condello V, Giuseppe M, Peretti GM, Steinwachs M, et al. Early osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc. 2016;24:1753–62. doi: 10.1007/s00167-016-4068-3. [DOI] [PubMed] [Google Scholar]
- 9.Migliore A, Scirè CA, Carmona L, Herrero-Beaumont G, Bizzi E, Branco J, et al. The challenge of the definition of early symptomatic knee osteoarthritis: a proposal of criteria and red flags from an international initiative promoted by the Italian Society for Rheumatology. Rheumatol Int. 2017;37:1237–8. doi: 10.1007/s00296-017-3742-1. [DOI] [PubMed] [Google Scholar]
- 10.Luyten FP, Bierma-Zeinstra S, Dell’Accio F, Kraus VB, Nakata K, Sekiya I, et al. Toward classification criteria for early osteoarthritis of the knee. Semin Arthritis Rheum. 2018;47:457–63. doi: 10.1016/j.semarthrit.2017.08.006. [DOI] [PubMed] [Google Scholar]
- 11.Mahmoudian A, Lohmander LS, Jafari H, Luyten FP. Towards classification criteria for early-stage knee osteoarthritis: a population-based study to enrich for progressors. Semin Arthritis Rheum. 2021;51:285–91. doi: 10.1016/j.semarthrit.2020.11.002. [DOI] [PubMed] [Google Scholar]
- 12.Culvenor AG, Collins NJ, Guermazi A, Cook JL, Vicenzino B, Khan KM, et al. Early knee osteoarthritis is evident one year following anterior cruciate ligament reconstruction: a magnetic resonance imaging evaluation. Arthritis Rheumatol. 2015;67:946–55. doi: 10.1002/art.39005. [DOI] [PubMed] [Google Scholar]
- 13.Madry H, Luyten FP, Facchini A. Biological aspects of early osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2012;20:407–22. doi: 10.1007/s00167-011-1705-8. [DOI] [PubMed] [Google Scholar]
- 14.Case R, Thomas E, Clarke E, Peat G. Prodromal symptoms in knee osteoarthritis: a nested case-control study using data from the osteoarthritis initiative. Osteoarthritis Cartilage. 2015;23:1083–9. doi: 10.1016/j.joca.2014.12.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Van Spil WE, Welsing PM, Bierma-Zeinstra SM, Bijlsma JW, Roorda LD, Cats HA, et al. The ability of systemic biochemical markers to reflect presence, incidence, and progression of early-stage radiographic knee and hip osteoarthritis: data from CHECK. Osteoarthritis Cartilage. 2015;23:1388–97. doi: 10.1016/j.joca.2015.03.023. [DOI] [PubMed] [Google Scholar]
- 16.Chu CR, Williams AA, Coyle CH, Bowers ME. Early diagnosis to enable early treatment of pre-osteoarthritis. Arthritis Res Ther. 2012;14:212. doi: 10.1186/ar3845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gelber AC, Hochberg MC, Mead LA, Wang NY, Wigley FM, Klag MJ. Joint injury in young adults and risk for subsequent knee and hip osteoarthritis. Ann Intern Med. 2000;133:321–8. doi: 10.7326/0003-4819-133-5-200009050-00007. [DOI] [PubMed] [Google Scholar]
- 18.Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequences of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007;35:1756–69. doi: 10.1177/0363546507307396. [DOI] [PubMed] [Google Scholar]
- 19.Hawker GA, Lohmander LS. What an earlier recognition of osteoarthritis can do for OA prevention. Osteoarthritis Cartilage. 2021;29:1632–4. [DOI] [PubMed]