

Abstract
Background
Caffeine is widely consumed among students due to its cognitive and physical enhancing effects. However, little is known about the consumption pattern of different caffeinated products among university students in the United Arab Emirates (UAE).
Aim
To investigate the frequency of caffeine consumption among the young population of students, assess types of caffeinated products consumed, and document adverse effects and withdrawal symptoms experienced by university students.
Methods
A cross-sectional study was conducted in the UAE from December 2019 to March 2020. A random sample of 500 university students from different universities in the UAE were approached and asked to complete a self-administered online-based questionnaire. Data were analyzed using the Statistical Package for Social Science (SPSS) version 26.
Results
Of (n = 500) surveyed students, (n = 467) completed the survey 93.4%. The average level of caffeine consumption was significantly higher in females compared to male students (p < 0.005). Coffee was the highest favored source of caffeine (67.7%) followed by tea (47.3%). The average daily intake of caffeine was found to be 264 mg/day. Surprisingly, almost a third of students reported a high level of daily consumption (>400 mg/day) and more than half of them consumed less than 199 mg/day. Large proportions of students 91.1% have their caffeinated beverage after or while eating meals and 42.8% considered that this habit helped in avoiding acid reflux. Interestingly, around one third of participants have poor knowledge of caffeine-containing medical products, which seemed to affect the level of consumption in the student population (p < 0.05). The highest reported reason for caffeine intake was for studying purposes (59.4%).
Conclusion
Caffeine consumption is highly prevalent among university students in the UAE. Yet, there is insufficiency in the current knowledge of safe caffeine consumption patterns reflecting the importance of health awareness programs and nutritional lectures to decrease the long-term health issues and unintentional overdose of caffeine.
1. Introduction
Caffeine, a methylxanthine derivative, is a widely used psychoactive and cognitive enhancer substance globally [1]. In contrast to other psychoactive drugs, it is legal and available in most regions of the world. Within an hour of oral ingestion, caffeine is absorbed and distributed to all body parts, even to the placenta and blood-brain barrier [2]. It exerts various pharmacological and physiological effects on muscles, cardiovascular, renal, and respiratory systems [3]. These effects include positive inotropic and chronotropic effects on the heart, mild diuresis and many others [4]. The most prominent mechanism that explains the stimulatory activity of caffeine appears to be the antagonism of adenosine receptors in the brain, which normally cause drowsiness when activated. Consequently, caffeine promotes wakefulness, the ability to maintain intellectual activity and an improved hedonic tone [2, 5]. Apart from the psychostimulant effects of caffeine, available evidence suggests that coffee consumers are less likely to develop diabetes, coronary heart disease and stroke compared to non-coffee consumers [6]. However, conflicting results from other studies were reported [7]. For instance, a study by Liu et al. found a positive relationship between caffeine intake and all-cause mortality in the population of 55 years old and above [8].
According to the literature, there has been a global increase in caffeine intake over the past decade. In 2020/2021, individuals consumed approximately 166 million, 60 kilograms bags of coffee globally. Several reasons for caffeine consumption have been previously discussed in the literature. Its usage by surgeons to reduce fatigue [9], by athletes to enhance their performance [10], and by students to improve concentration and wakefulness [11].
Students from school and college are heavily taking caffeine nowadays. Seventy-three percent of children consume caffeine daily as stated by the journal Pediatrics by the AAP in 2014 [12]. Most of them drink soft drinks in high amounts and despite the sugar and unhealthy ingredients of these drinks, caffeine in itself can harm their health. Many studies reported various harmful effects of caffeine such as panic attacks, insomnia and chronic fatigue on students. In 2014, an 18-year-old teenager in Ohio, USA, had cardiac arrhythmia and died from an overdose of pure caffeine powder [13].
While many studies revealed similar trends in caffeine intake among students in the Gulf and the Middle East, only limited studies in the UAE highlighted this concern [14, 15]. Therefore, our study aims to investigate the frequency of caffeine consumption among the young population of students, assess types of caffeinated products consumed, and document adverse effects and symptoms of caffeine consumption experienced by university students in the UAE.
2. Methods
2.1. Study Design, Sampling Technique, And Size
This was a quantitative, cross-sectional study with a descriptive design conducted over four months (from December 2019 to March 2020) on a random sample of university students across the UAE. The study population included females (n = 304) and males (n = 163) who were 18 years old and above and consented/agreed to participate in the study. The study received the required ethical approvals from the research ethics committee (REC) at Al-Ain University (AAU-REC-B3, Feb 2019). Convenience sampling was used as a technique to research participants.
Based on previous literature and the Raosoft sample size calculator [16], a minimum sample size of 385 students was considered representative for this study.
2.2. Study Tool
The questionnaire used in the study is a pre-validated survey. All study participants were administered this survey individually through an online link with the help of the research team who tried to reach students from different majors and universities across the seven emirates. The participants were briefly informed about the study objectives at the beginning of the questionnaire. The survey was administered in English and Arabic. It included closed-ended questions that contained four sections: Characteristics of the sample and demographics, Caffeine consumption patterns, Caffeine expectations, and social expectations and purposes of caffeine consumption.
2.3. Characteristics of the Sample and Demographics
The following information was addressed: Age, gender, college, and year of study.
2.4. Caffeine Consumption Patterns
Participants answered Yes/No questions about their caffeine consumption behaviors, their knowledge about the existence of caffeine in some medicinal products and their feedback about the use of caffeine in reliving their headaches. This section also addressed the following: When they usually take their caffeinated drink, do they prefer to drink it on an empty stomach or after their meals and if so, why do they choose after meals? What sources of caffeine do they usually consume the most, and from where do they prefer to get it?
2.5. Caffeine Expectations
Participants answered four Likert-type statements on their expectations of consuming caffeine. The Likert scale was a 5-point scale of “Highly disagree” stated as number 1, to “Highly agree” stated as number 5 on the scale. In addition, some questions were about caffeine addiction, withdrawal symptoms, and side effects. Caffeine addiction was considered as taking more than 100 mg of caffeine daily, which is about one cup of coffee. The students were given the 1 to 5 scale to report their caffeine consumption to determine their addiction level.
2.6. Social Expectations and Purposes of Caffeine Consumption
Participants were asked to answer questions about the purpose of consuming caffeinated products. The questions included a range of reasons and social habits of drinking coffee and other caffeinated products.
2.7. Validation of the Study Questionnaire
The questionnaire used for the study is pre-validated. Nevertheless, we tailored it to suit the aims of the study and the culture of the UAE. Another validation test was conducted for the edited version of the questionnaire. A draft of the questionnaire was prepared and sent to a panel of experts who were professors in the Pharmacy and Nutrition field at Al-Ain University, Ajman University and UAE University to test the content validity of the questionnaire. They examined many factors of the questionnaire including the conciseness, length, clarity, language, time consumed, bias, and appropriateness of questions. Content validation of a questionnaire should consider these factors [17].
2.8. Reliability Testing of the Study Questionnaire
The questionnaire was additionally revised based on a reliability test conducted as a pilot study on 84 students to achieve the most acceptable Cronbach's values. Also, a preliminary pilot testing was carried out to ensure the practicality and understandability of the questionnaire.
2.9. Inclusion and Exclusion Criteria
University students of both genders aged >18 years and currently studying in any university in the UAE were included in the study. The exclusion criteria were students who do not consume caffeine.
2.10. Data Collection
The final version of the questionnaire was administered through an online link sent via different social media methods to students who met the eligibility criteria and agreed to participate. The research team carried out the questionnaire distribution. Participants were first briefed about the estimated time needed to complete the survey and the study purposes; they were then directed to the questionnaire link. Furthermore, the participants were informed about the confidentiality and anonymity policy.
2.11. Statistical Analysis
Data sets were gathered by the principal investigator and the excel sheet of the online survey was downloaded and then imported to the Statistical Package for Social Science (SPSS) version 26 (IBM Corporation, Armonk, NY, USA) for data analysis. Descriptive statistical analysis was conducted and results were represented as numbers (n) with percentages (%). To assess differences in responses across categorical variables, Chi-square or Fisher exact tests were used as appropriate. A p value of <0.05 was considered to be statistically significant.
3. Results
Four hundred sixty-seven participants completed the questionnaire, of which 65.1% (n = 304) were females and more than half were between 20 and 23 years old (Table 1).
Table 1.
Demographics of students (n = 467).
| N (%) | |
|---|---|
| Total | 467 (100) |
|
| |
| Gender | |
| Male | 163 (34.9) |
| Female | 304 (65.1) |
|
| |
| Age | |
| 17–19 | 93 (19.9) |
| 20–23 | 263 (56.3) |
| 24–27 | 65 (13.9) |
| 28+ | 46 (9.9) |
|
| |
| College | |
| Medical | 201 (43) |
| Non-medical | 266 (57) |
|
| |
| Year of Study | |
| First year | 63 (13.5) |
| Second year | 93 (19.9) |
| Third year | 112 (24) |
| Fourth year | 124 (26.6) |
| Fifth year | 75 (16.1) |
Descriptive analysis was conducted.
The majority of the participants (38.5%) reported that they consume caffeine two to three times daily, and around 7% reported a consumption rate of more than 5 times per day. The vast majority of participants (90.1%) consume caffeinated drinks with or after meals. Roughly a third of them (34.7%) attributed this behavior to their knowledge of caffeine consequences on the stomach i.e. acid reflux and stomach upset, while more than half (51%) consider it a habit. Around 316 (67.7%) picked coffee as their favorite drink, 221 (47.3%) picked tea, and 172 (36.8%) picked chocolate (Table 2).
Table 2.
Caffeine consumption patterns.
| How often do you consume caffeinated beverages? N (%) | |
| Once daily | 116 (24.8) |
| 2-3 times a day | 180 (38.5) |
| 4-5 times daily | 72 (15.4) |
| More than 5 times a day | 32 (6.9) |
| 1 to 3 times weekly | 50 (10.7) |
| 4 to 6 times weekly | 17 (3.6) |
|
| |
| What time of the day do you usually consume caffeine ∗ | |
| Morning | 284 (60.8) |
| Afternoon | 187 (40.0) |
| Evening | 218 (46.7) |
|
| |
| When do you prefer to have caffeine? | |
| Before eating | 171 (36.6) |
| While eating | 106 (22.7) |
| After eating | 302 (67.4) |
|
| |
| Why do you prefer having your caffeine drink with/after meals? | |
| To help with digestion | 90 (19.3) |
| Habit | 238 (51.0) |
| To avoid acid reflux and stomach upset | 162 (34.7) |
|
| |
| Sources of caffeine ∗ | |
| Coffee | 316 (67.7) |
| Tea | 221 (47.3) |
| Caffeinated soft drinks | 124 (26.6) |
| Energy drinks | 77 (16.5) |
| Chocolate | 172 (36.8) |
|
| |
| Do you know that caffeine is added to certain pain killers\medicines? | |
| No | 157 (33.6) |
| Yes | 310 (66.4) |
|
| |
| Does a cup of coffee with Panadol relieve your pain/headache more effectively than Panadol alone? | |
| No | 204 (43.7) |
| Yes | 263 6.3) |
∗ Multiple responses allowed. Descriptive analysis was conducted.
Additionally, there were significant differences in favorite drinks across females and males. Females were more likely to prefer coffee and chocolate, whereas males were more likely to prefer tea (p < 0.005). On the other hand, there was no significant difference in caffeine consumption between the medical and non-medical colleges (p=0.149).
More than half of students (56.3%) agreed that the combination of caffeine and analgesic medications is more effective in relieving headaches. However, more than two-thirds of students (66.4%) had significantly poor knowledge about caffeine's existence in medical products and this seemed to influence their caffeine consumption rate (p < 0.05) (Table 3).
Table 3.
Average consumption level.
| Average caffeine consumption level | 1 to 3 times weekly | 2-3 times a day | 4 to 6 times weekly | 4-5 times daily | More than 5 times a day | Once daily | p-value | |
|---|---|---|---|---|---|---|---|---|
| Parameters | Total | |||||||
| Gender | ||||||||
| Female | 304 | 40 | 130 | 14 | 26 | 16 | 78 | 0.005 |
| Male | 163 | 10 | 50 | 3 | 46 | 16 | 38 | |
|
| ||||||||
| College | ||||||||
| Medical | 201 | 22 | 12 | 50 | 80 | 27 | 10 | 0.149 |
| Non-medical | 266 | 28 | 5 | 66 | 100 | 45 | 22 | |
|
| ||||||||
| When did you start taking caffeine (years) | ||||||||
| 13 to 17 | 210 | 27 | 92 | 9 | 31 | 9 | 42 | 0.153 |
| 8 to 12 | 77 | 4 | 28 | 2 | 16 | 6 | 21 | |
| Over 18 | 148 | 18 | 48 | 6 | 22 | 13 | 41 | |
| Under 8 | 32 | 1 | 12 | 1 | 2 | 4 | 12 | |
|
| ||||||||
| Are you aware that caffeine is added to certain pain relievers? | ||||||||
| Yes | 310 | 27 | 116 | 13 | 54 | 29 | 71 | 0.005 |
| No | 157 | 23 | 64 | 4 | 18 | 3 | 45 | |
Chi-square or fisher exact tests were used as appropriate.
The findings of this study indicated that withdrawal symptoms and side effects, such as muscle pain, shakiness, and trouble concentrating were significantly associated with the age of students (p values < 0.05). Interestingly, more than 30% of participants reported caffeine use more than 3 times a day at the age of 8–12 years, and more than 40% reported the same frequency at the age of 13–17 years (Table 4). When further exploring the expectation of caffeine consumption, we found that more than half of the participants thought it allowed them to think clearly, sharpen their memory and improve their mood (Table 5).
Table 4.
Caffeine side effects and withdrawal symptoms.
| Parameter | N (%) | At what age did you start consuming caffeine? (Years) | p-value | |||
|---|---|---|---|---|---|---|
| 8 to 12 | 13 to 17 | Over 18 | Under 8 | |||
| Withdrawal symptoms | ||||||
| Headaches | 175 (37.47) | 22 (12.57) | 81 (46.28) | 61 (34.85) | 11 (6.28) | 0.359 |
| Nausea | 42 (8.99) | 13 (30.95) | 13 (30.95) | 12 (28.57) | 4 (9.52) | 0.074 |
| Muscle pain | 37 (7.92) | 14 (37.83) | 9 (24.32) | 10 (27.02) | 4 (10.81) | 0.003 |
| Drowsiness | 127 (27.19) | 15 (11.81) | 62 (48.81) | 42 (33.07) | 7 (5.51) | 0.185 |
| Fatigue | 61 (13.06) | 4 (6.55) | 43 (47.77) | 24 (39.34) | 6 (9.83) | |
| Irritability/Poor mood | 90 (21.41) | 17 (18.88) | 19 (28.78) | 23 (25.55) | 7 (7.77) | 0.677 |
|
| ||||||
| Side effects | ||||||
| Shaky | 66 (14.13) | 15 (22.72) | 26 (41.93) | 24 (36.36) | 8 (12.12) | 0.040 |
| Tense | 62 (13.27) | 15 (24.19) | 61 (48.41) | 17 (27.41) | 4 (6.45) | 0.512 |
| Rapid heartbeat | 126 (26.98) | 19 (15.07) | 20 (4.28) | 38 (30.15) | 8 (6.34) | 0.864 |
| Anxious | 61 (13.07) | 14 (22.95) | 9 (20.45) | 22 (36.06) | 5 (3.27) | 0.310 |
| Trouble concentrating | 44 (9.42) | 11 (25.00) | 23 (43.39) | 17 (38.63) | 7 (15.90) | 0.004 |
| Restless | 53 (11.34) | 8 (15.09) | 48 (41.02) | 18 (33.96) | 4 (7.54) | 0.985 |
| Difficulty falling asleep | 117 (25.05) | 14 (11.96) | 44 (37.60) | 11 (9.40) | 0.202 | |
Bold indicates a significant result. Findings are listed as numbers. Chi-square or fisher exact.
Table 5.
Caffeine expectations.
| Strongly disagree (%) | Disagree (%) | Neutral (%) | Agree (%) | Strongly agree (%) | ||
|---|---|---|---|---|---|---|
| Caffeine makes me | Alert, energized and less sleepy | 6.9 | 9.6 | 25.7 | 28.9 | 28.9 |
| Think clearly, pay more attention and sharpen my memory | 3.9 | 8.8 | 25.7 | 38.8 | 22.9 | |
| Relax, calm down, and improves my mood | 4.9 | 7.5 | 24.6 | 35.3 | 27.6 | |
Descriptive analysis was conducted.
More than half of the students (59.4%) reported consuming caffeine for studying and avoiding sleep (Figure 1). Lastly, we compared the average caffeine consumption per day and gender among participants and found that 28.7% (n = 134) consumed >400 mg/day which is considered a high consumption level. However, there was no difference in daily consumption among medical and non-medical students or gender (Table 6).
Figure 1.
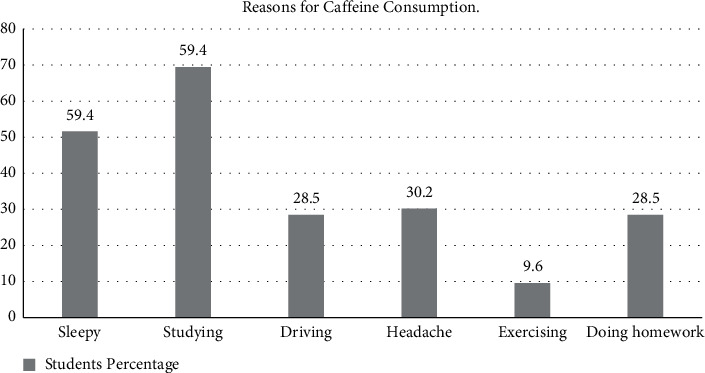
Reasons for caffeine consumption (expressed as %).
Table 6.
Caffeine average consumption.
| Caffeine consumers | % (n) |
|---|---|
| Low (≤199 mg/day) | 52.0% (n = 243) |
| Moderate (200–399 mg/day) | 19.3% (n = 90) |
| High (>400 mg/day) | 28.7% (n = 134) |
|
| |
| Caffeine average consumption per day and gender | |
| Male | 242.3 mg |
| Female | 275.1 mg |
|
| |
| Caffeine average consumption per day and college | |
| Medical | 279.7 mg |
| Non-medical | 251.5 mg |
Descriptive analysis was conducted.
4. Discussion
Little is known about caffeine's safe and healthy consumption behaviors, even though there is a rise in coffee intake by the young population. A limited number of studies conducted in the Gulf region and the UAE reported the prevalence of caffeine consumption among university students. Yet and to the best of our knowledge, no other study assessed types of caffeinated products consumed with the documentation of adverse effects and withdrawal symptoms experienced by university students. Therefore, our current study aimed to evaluate the consumption pattern of different caffeinated products among university students in the UAE, reporting caffeine's adverse effects and withdrawal symptoms and characterizing its consumption with age, gender and other characteristics. Finally, we sought to determine the motivational factors behind student's consumption of various caffeinated beverages.
Our study results indicated that more than half of the students consume less than 199 mg/day, while almost a third of the students reported a high level of daily consumption (>400 mg/day). The average daily intake of caffeine was found to be 264 mg/day. These findings were in agreement with a previous study of caffeine consumption in the UAE [18] and Bahrain universities (268 mg/day) [19]. However, the average daily consumption in our study sample was lower compared to students from Lebanon (373 mg/day during the weekdays) [20] and higher compared to caffeine intake among U.S college students who reported consuming average daily caffeine of 173 mg/day [11]. Similar results of average daily caffeine consumption in gulf universities might represent the similar habits and behaviors in these countries.
Female students were found to consume more caffeinated beverages than males, with a daily average of 275 mg and 242 mg, respectively. This might be due to different lifestyles and hangouts of female students compared to males in the Arabic world. However, this finding opposes the results of a study conducted among college students of Zayed University, UAE [15], where no significant difference was reported between genders. The discrepancy between the results could be attributed to the large number of participants included in our study.
Coffee was the most commonly consumed source of caffeine by respondents, followed by tea and caffeinated soft drinks. Coffee being the primary source of caffeine, was similar to previous reports. However, according to these studies, soft drinks preceded tea consumption [19]. These results can reflect the social view of coffee as more prestigious than other drinks and thus increasing their usage trend among students in the UAE.
Forty percent of the students take caffeinated products two to three times daily and a quarter of them take it only one time, preferably in the early morning. Fortunately, more than two-thirds of the sample population take caffeinated beverages after a meal; upon asking them about the reason, half of them follow this practice to avoid stomach upset and enhance digestion. However, a study of coffee consumption among Saudi female students by H. Alfawaz mentioned that 18.7% of the students suffering from stomach pain was considered to be related to coffee consumption [21].
Our results indicated that most of the surveyed students consume caffeinated beverages to enhance their alertness and concentration while studying; sharpen their memory, and improve their mood as represented by Figure 1. A study from Korea referred reported that the motivation for caffeinated drink consumption was due to various reasons such as social factors, alertness, health, mood, daily habits as well as sensory effects. The motivation of consumption was different and depended on the source of caffeine and different kinds of caffeinated drinks [22].
The surveyed participants have reported various symptoms associated with their high caffeine consumption, such as higher levels of tension and anxiety, difficulty falling asleep, and rapid heart rate. While it is not easy to link these symptoms to the high level of caffeine consumption, many studies have shown a strong association between such symptoms and caffeine consumption [22–24]. Reports from Australia and Korea showed that caffeine consumption and energy drink intake was correlated with the poor quality of sleep among adults [25, 26]. In contrast, other reports showed no correlation between caffeine consumption and poor quality of sleep [27].
Interestingly, more than 30% of participants reported the caffeine use more than 3 times a day at the age of 8–12 years and more than 40% at the age of 13–17 years. In fact, a study published in 2010 answered the question of why should we be worried about caffeine consumption in children [28]. The results of several studies indicated that caffeine could have different effects on children and adolescents compared to those seen in adults. Indeed, childhood and adolescence is a period of speedy growth; and proper nutrition and sleep are considered essential to maximize this growth and development. Many studies concluded that caffeine use disrupts sleep patterns [28, 29]. In addition, results from animal studies indicated that caffeine could prime the brain to increase its response to subsequent drug exposure, thereby potentiating the reinforcing effects of drugs [30]. Children and adolescents can be susceptible to these effects, especially since their brains are still undergoing significant development. Thus, the results of our studies are of significance to the academic community as it increases the awareness of caffeine consumption among this population and encourage the implementation of educational platforms and workshops to educate the young population and parents about caffeine consumption among students.
5. Conclusion
Caffeine consumption is prevalent among university students in UAE (93.6%). Our study highlights the lack of knowledge of safe caffeine consumption patterns among these students and hence reflect the importance of health awareness programs and nutritional lectures to decrease the long-term health issues and unintentional overdose of caffeine. Our results can be considered baseline data to be utilized in further research about coffee consumption trends in the Arab world.
Acknowledgments
Our thanks to Al Ain University for facilitating our research. Thanks to Dr. Azza Ramadan from Al Ain University for her insightful ideas and proofreading.
Data Availability
The datasets used and analyzed during the present study are available from the corresponding author on reasonable request.
Additional Points
Strengths and weaknesses. The main study limitation is that it's a survey-based study, which can affect the accuracy of reported details. Another limitation is the unfeasibility to calculate the exact amount of caffeine content ingested by students.
Ethical Approval
The study received the required ethical approvals from the research ethics committee (REC) at Al-Ain University (AAU-REC-B3, Feb 2019).
Consent
All participants consented to take part in the study.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- 1.Chin J. M., Merves M. L., Goldberger B. A., Sampson-Cone A., Cone E. J. Caffeine content of brewed teas. Journal of Analytical Toxicology . 2008;32(8):702–704. doi: 10.1093/jat/32.8.702. [DOI] [PubMed] [Google Scholar]
- 2.Nehlig A., Daval J.-L., Debry G. Caffeine and the central nervous system: mechanisms of action, biochemical, metabolic and psychostimulant effects. Brain Research Reviews . 1992;17(2):139–170. doi: 10.1016/0165-0173(92)90012-b. [DOI] [PubMed] [Google Scholar]
- 3.Frary C. D., Johnson R. K., Wang M. Q. Food sources and intakes of caffeine in the diets of persons in the United States. Journal of the American Dietetic Association . 2005;105(1):110–113. doi: 10.1016/j.jada.2004.10.027. [DOI] [PubMed] [Google Scholar]
- 4.Marx B., Scuvée É., Scuvée-Moreau J., Seutin V., Jouret F. Mécanismes de l’effet diurétique de la caféine. Médecine/Sciences . 2016;32(5):485–490. doi: 10.1051/medsci/20163205015. [DOI] [PubMed] [Google Scholar]
- 5.Nehlig A. Is caffeine a cognitive enhancer? Journal of Alzhemirs Disease . 2010;20(1):S85–S94. doi: 10.3233/jad-2010-091315. [DOI] [PubMed] [Google Scholar]
- 6.Bhatti S. K., O’Keefe J. H., Lavie C. J. Coffee and tea. Current Opinion in Clinical Nutrition and Metabolic Care . 2013;16(6):688–697. doi: 10.1097/mco.0b013e328365b9a0. [DOI] [PubMed] [Google Scholar]
- 7.Yu Z. M., Parker L., Dummer T. J. B. Associations of coffee, diet drinks, and non-nutritive sweetener use with depression among populations in Eastern Canada. Scientific Reports . 2017;7(1):p. 6255. doi: 10.1038/s41598-017-06529-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Liu J., Sui X., Lavie C. J., et al. Association of coffee consumption with all-cause and cardiovascular disease mortality. Mayo Clinic Proceedings . 2013;88(10):1066–1074. doi: 10.1016/j.mayocp.2013.06.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Franke A. G., Bagusat C., McFarlane C., Tassone-Steiger T., Kneist W., Lieb K. The use of caffeinated substances by surgeons for cognitive enhancement. Annals of Surgery . 2015;261(6):1091–1095. doi: 10.1097/sla.0000000000000830. [DOI] [PubMed] [Google Scholar]
- 10.Desbrow B., Leveritt M. Well-trained endurance athletes’ knowledge, insight, and experience of caffeine use. International Journal of Sport Nutrition and Exercise Metabolism . 2007;17(4):328–339. doi: 10.1123/ijsnem.17.4.328. [DOI] [PubMed] [Google Scholar]
- 11.Mahoney C. R., Giles G. E., Marriott B. P., et al. Intake of caffeine from all sources and reasons for use by college students. Clinical Nutrition . 2019;38(2):668–675. doi: 10.1016/j.clnu.2018.04.004. [DOI] [PubMed] [Google Scholar]
- 12.Branum A. M., Rossen L. M., Schoendorf K. C. Trends in caffeine intake among US children and adolescents. Pediatrics . 2014;133(3):386–393. doi: 10.1542/peds.2013-2877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.FDA. Bans bulk concentrated caffeine supplements | everyday health. 2021. https://www.everydayhealth.com/fda/what-ban-bulk-concentrated-caffeine-supplements-means-consumers/
- 14.Alaa Hammami M. B., Al Shaikh Y. G., Hashem A. M., et al. Caffeine consumption levels and knowledge among adults in the United Arab Emirates: insights from a nationwide survey. Journal of Caffeine and Adenosine Research . 2018;8(2):71–79. doi: 10.1089/caff.2017.0034. [DOI] [Google Scholar]
- 15.Ghali R. M. A., Shaibi H. A., Majed H. A., Haroun D. Caffeine consumption among zayed university students in Dubai, United Arab Emirates: a cross-sectional study. Arab Journal of Nutrition and Exercise . 2017;1 doi: 10.18502/ajne.v1i3.1230. [DOI] [Google Scholar]
- 16.Sample size calculator by raosoft, Inc. 2021. http://www.raosoft.com/samplesize.html .
- 17.Mackison D., Wrieden W. L., Anderson A. S. Validity and reliability testing of a short questionnaire developed to assess consumers’ use, understanding and perception of food labels. European Journal of Clinical Nutrition . 2010;64(2):210–217. doi: 10.1038/ejcn.2009.126. [DOI] [PubMed] [Google Scholar]
- 18.Al Ghali R M., Al Shaibi H., Al Majed H., Haroun D. Caffeine consumption among Zayed university students in Dubai, United Arab Emirates: a cross-sectional study. Arab Journal of Nutrition and Exercise . 2017;1(3):p. 131. [Google Scholar]
- 19.Jahrami H., Al-Mutarid M., Penson P. E., Al-Islam Faris M., Saif Z., Hammad L. Intake of caffeine and its association with physical and mental health status among university students in Bahrain. Foods . 2020;9(4) doi: 10.3390/foods9040473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Khalil M., Antoun J. Knowledge and consumption of caffeinated products by university students in Beirut, Lebanon. Clinical Nutrition ESPEN . 2020;37:213–217. doi: 10.1016/j.clnesp.2020.02.014. [DOI] [PubMed] [Google Scholar]
- 21.Alfawaz H. A., Khan N., Yakout S. M., et al. Prevalence, predictors, and awareness of coffee consumption and its trend among saudi female students. International Journal of Environmental Research and Public Health . 2020;17(19) doi: 10.3390/ijerph17197020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Choi J. Motivations influencing caffeine consumption behaviors among college students in Korea: associations with sleep quality. Nutrients . 2020;12(4) doi: 10.3390/nu12040953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Richards G., Smith A. Caffeine consumption and self-assessed stress, anxiety, and depression in secondary school children. Journal of Psychopharmacology . 2015;29(12):1236–1247. doi: 10.1177/0269881115612404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Samaha A., Al Tassi A., Yahfoufi N., Gebbawi M., Rached M., Fawaz M. A. Data on the relationship between caffeine addiction and stress among Lebanese medical students in Lebanon. Data in Brief . 2020;28 doi: 10.1016/j.dib.2019.104845.104845 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Watson E. J., Coates A. M., Kohler M., Banks S. Caffeine consumption and sleep quality in Australian adults. Nutrients . 2016;8(8) doi: 10.3390/nu8080479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Park S., Lee Y., Lee J. H. Association between energy drink intake, sleep, stress, and suicidality in Korean adolescents: energy drink use in isolation or in combination with junk food consumption. Nutrition Journal . 2016;15(1):p. 87. doi: 10.1186/s12937-016-0204-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Janson C., Gislason T., De Backer W., et al. Prevalence of sleep disturbances among young adults in three European countries. Sleep . 1995;18(7):589–597. [PubMed] [Google Scholar]
- 28.Temple J. L. Caffeine use in children: what we know, what we have left to learn, and why we should worry. Neuroscience & Biobehavioral Reviews . 2009;33(6):793–806. doi: 10.1016/j.neubiorev.2009.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pollak C. P., Bright D. Caffeine consumption and weekly sleep patterns in US seventh-, eighth-, and ninth-graders. Pediatrics . 2003;111(1):42–46. doi: 10.1542/peds.111.1.42. [DOI] [PubMed] [Google Scholar]
- 30.Schenk S., Valadez A., Horger B. A., Snow S., Wellman P. J. Interactions between caffeine and cocaine in tests of self-administration. Behavioural Pharmacology . 1994;5(2):153–158. doi: 10.1097/00008877-199404000-00006. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and analyzed during the present study are available from the corresponding author on reasonable request.