

Abstract
Introduction:
Laparoscopic instruments and techniques are constantly improving, as the ability to perform minimally invasive surgery is crucial in modern medicine. The progression from open surgery to minimally invasive surgery over the years eventually led to the use of robotic devices to either assist or completely replace patient-side surgery with a separate console. Though robotic surgery has been praised for its surgical outcomes, certain situations limit its use, such as cost-effectiveness or physical space constraints. The objectives of this review were to perform a search and discuss the trends in the literature.
Methods:
A literature search using keywords ((laparoscopic) OR (laparoscopy) OR (minimally invasive)) AND ((instrument) OR (instrumentation) OR (tool) OR (device) OR (apparatus)) AND ((advancement) OR (upgrade)) AND ((hysterectomy) OR (prostatectomy) OR (transoral) OR (cholecystectomy)) AND (robot) in PubMed, looking for trends in advancements or appeals for change.
Results:
This search provides a framework for these trends to facilitate discussion of ways in which laparoscopic surgery can be improved using the benefits of robotic surgical systems. This allows others to approach the successes of the current robotic systems for laparoscopic surgery with the intention of deriving advancements toward traditional laparoscopic surgery.
Keywords: Laparoscopic surgery, da Vinci, Robotic surgery
INTRODUCTION
Background
Minimally invasive surgery (MIS) has been evolving since the early 1900s, when a laparoscopic procedure was first performed by George Kelling in vivo.1 Although successful attempts in human patients were made by Kelling and other surgeons, ubiquitous application was slow. Discounting possible improvements to this field stemmed from the fear of risking complications and possibly worsening outcomes, propagated by higher incidence once laparoscopic techniques became more widespread.1 In the last century, a rise in new technology forced a change. A study in 1962 discussed the application of television to endoscopic techniques, and with further advancements in resolution and miniaturization there was promise to a future with laparoscopic surgery.2 However, it was not until the late 1970s when Dr. Camran Nezhat began to use video cameras during his procedures that laparoscopic surgery was taken more seriously, though Nezhat had described the struggle to navigate the criticism of his colleagues in his presidential address.1
Current Status of Laparoscopic Surgery
Today, performing MIS is no longer unjustifiable. Considerations for when to perform surgery via open, laparoscopic, or robotic techniques depends on various factors. The type of technique used also depends on the procedure (cholecystectomy, hysterectomy, etc.), severity of indication (disease progression, low risk/high risk), and surgical expertise. Complications during surgery can alter the technique, for example switching from laparoscopic to open surgery in the event of severe adhesions or electing to perform a different technique in the event of a complicated anatomical variation.3,4
Another consideration for laparoscopic surgery involves the instruments or tools used during the procedure. Certain tools are required in every type of surgical procedure, though some specific surgeries require specialized tools. All laparoscopic surgery techniques require the use of an illuminated scope, or laparoscope, which allows for observation of associated viscera.1 These are generally rigid, but flexible endoscopes occasionally replace them to allow for access during single-incision surgeries.5 Advancements in this area currently surround the use of three-dimensional (3D) cameras to improve surgical performance.6 Trocars are used to gain access to the abdominal cavity by puncturing the musculature and fascia of the abdominal wall with the sharp edge, allowing for other instruments to pass through a canal at the core.5 They can be disposable or reusable, wherein disposable trocars are described frequently to be of higher quality but generally less cost effective.7,8 Many different techniques are used for laparoscopic entry. The two basic techniques are open or Hasson entry, where the trocar is inserted prior to insufflation of the abdomen, and the closed or Veress needle entry, where insufflation is performed prior to trocar insertion.9
Advancements in Surgical Techniques
Laparoscopic instruments and techniques are constantly improving, as the ability to perform MIS is crucial in modern medicine. The progression from open surgery to MIS over the years eventually led to the use of robotic devices to either assist or completely replace patient-side surgery with a separate console. Robotic surgery gained traction in the 1980s, starting with Robodoc of Integrated Surgical Systems and cultivated by the US Department of Defense to reduce casualties.10 The system was not available for public use until it was introduced to private investors in 1993. The first complete surgical system was developed in 1996, known as ZEUS.10 The first clinical use of ZEUS was in 1999 for a coronary artery bypass.11 Despite ZEUS having certain advantages, it was eventually phased out in favor of the da Vinci system.10
The da Vinci Surgical System by Intuitive Surgical, Inc. is the most widely used robotic surgical system today and utilizes a master-slave console that allows the surgeon to operate remotely from the surgical field.12 This system continues to impress the medical community, and the system is being used for an increasing number of surgical procedures.13
In addition to its use in surgical procedures, the da Vinci is used in training settings as a virtual reality (VR) surgical simulator.14 This is due to the ability of the da Vinci to visualize the surgical field with 3D view at the master console. Kiely et. al. showed the application of the da Vinci in skills simulation to allow for a better transition for trainees, specifically in suturing.
The first surgery performed using the da Vinci robotic system was in Brussels, Belgium in 2000, after it had been introduced to Europe in 1997.10 A study performed in 2001 looked at the clinical feasibility of the da Vinci performed 146 surgeries with 11 types of interventions, discussing operating times and preferred trocar and slave arm positioning. The study recognized the need for improvement in both system protocols as well as system design, but highly praised the da Vinci for its ability to improve ergonomics in ways such as reducing surgeon tremor.15
Despite the predominance of the da Vinci robot, the need to improve traditional laparoscopy is required due to cost-efficacy, training, or set-up constraints. A 2017 study performed a cost assessment of robotic surgical systems and found that it has the potential to become more cost-effective; however, current financial climates are limiting.16 The da Vinci system has certain advantages that allow it to improve surgical outcomes; therefore, efforts should be made to discuss and compare specific advantages to enhance traditional laparoscopy.
The da Vinci Annual Report of 2019 states that the main clinical applications for their system are in gynecology (hysterectomy, sacrocolpopexy), urology (prostatectomy, partial nephrectomy), general surgery (hernia repair, colorectal surgery, cholecystectomy, bariatric surgery), cardiothoracic surgery (thoracic surgery, mitral valve repair), and head and neck surgery (transoral surgery).13 This review will narrow the discussion to the four most commonly researched da Vinci surgeries: cholecystectomies, hysterectomies, prostatectomies, and transoral surgeries.
One of the first noticeable advantages of the da Vinci, in a study conducted only a year after its initiation, concluded an improvement in complications with ergonomics as seen in traditional laparoscopic surgery by eliminating the need for the surgeon to keep instruments stationary.15 Other features of robotic surgery that can be extrapolated to traditional laparoscopic surgery were explored in this review.
METHODS
This literature review used PubMed as a resource to search for relevant articles. The preliminary search keywords included words related to MIS (laparoscopy, laparoscopic, minimally invasive), words to describe instrumentation (instrument, instrumentation, tool, device, apparatus), words indicating an improvement (advancement, upgrade), the four procedures of focus (cholecystectomy, hysterectomy, prostatectomy, transoral), and an additional word (robot) to filter for robotic systems. The search keywords were thus be written as:
((laparoscopic) OR (laparoscopy) OR (minimally invasive)) AND ((instrument) OR (instrumentation) OR (tool) OR (device) OR (apparatus)) AND ((advancement) OR (upgrade)) AND ((hysterectomy) OR (prostatectomy) OR (transoral) OR (cholecystectomy)) AND (robot)
The search involved exclusion criteria such that only articles in English and on humans are featured. This search then was critically evaluated, and all irrelevant articles as well as reviews were eliminated from the final selection. Irrelevant articles included those only mentioning the keywords and not showing a surgical experiment, articles testing a simulation device for use in training or other academic tests, articles discussing only postoperative procedures without discussing a robotic system, and articles discussing biopsies instead of true laparoscopic procedures. A flowchart of the search is shown in Figure 1.
Figure 1.
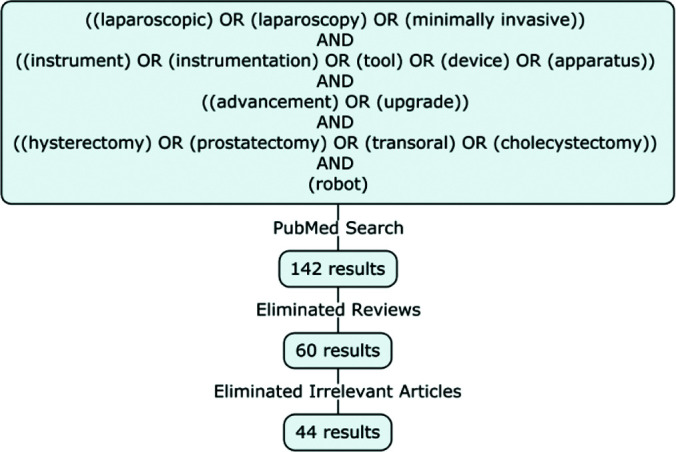
Flowchart of the search method, showing the inclusion criteria (key terms) and exclusion criteria (reviews, irrelevant articles), all from a pubmed search.
RESULTS
The search yielded 142 results when inputting the keywords into the PubMed database. Once the reviews were eliminated, 60 articles were evaluated for exclusion. Irrelevant articles were eliminated, and 44 results were included in the discussion. Table 1 shows that the search brought up 7 articles on hysterectomies, 12 on prostatectomies, 6 on cholecystectomies, 10 on transoral surgery, 2 with multiple different procedures, and 2 that were preclinical models without a specific surgical procedure. Multiple articles were included that assessed a specific procedure separate from the original search terms highlighting 4 procedures; these articles were included due to relevance to the review’s purpose. The article findings are listed in Table 2, which shows the trends that are explored in the following section.
Table 1.
Comparison of the Search Results by Surgery Type and Study Type
| Subgroups | References |
|---|---|
| Surgery Type | |
| Hysterectomies | 18, 20, 23, 43, 49, 54, 55 |
| Prostatectomies | 17, 25, 26, 27, 28, 29, 30, 51, 52, 53, 57, 59 |
| Cholecystectomies | 22, 31, 39, 41, 44, 48 |
| Transoral surgeries | 19, 21, 33, 35, 36, 37, 38, 45, 46, 63 |
| Ureteroneocystostomy | 56 |
| Gastro-oesophageal surgery | 34 |
| Roux-en-Y hepaticojejunostomy | 32 |
| Colposacropexy | 42 |
| Anterior pelvic exenteration with radical vaginectomy | 60 |
| Multiple | 15, 50 |
| N/A* | 40, 62 |
| Study Type | |
| Clinical trials | 17, 20, 59 |
| Case reports | 18, 27, 31, 32, 38, 41, 42, 43, 55, 56, 60 |
| Case studies | 15, 22, 23, 25, 26, 28, 29, 30, 33, 34, 36, 44, 45, 48, 49, 50, 53, 57 |
| Preclinical models | 19, 21, 35, 37, 39, 40, 46, 51, 52, 54, 62, 63 |
Preclinical model without definitive procedure.
Table 2.
Stratification of the Article Findings
| Article Findings | References |
|---|---|
| Evaluation of the da Vinci (multiport) | 18, 20, 21, 22, 23, 26, 27, 28, 29, 30, 31, 33, 35 |
| Criticism: haptic feedback | 19, 20, 21, 22, 28, 32, 40, 44, 46, 62, 63 |
| Acknowledgement: 3D Visual Field | 15, 17, 18, 20, 22, 23, 26, 28, 31, 32, 34, 36, 43, 46, 54, 59, 60 |
| Traditional Laparoscopic Surgery Advancements | 29, 36, 41, 42, 44, 48 |
| Adjustments made during surgery using da Vinci | 23, 26, 30, 35, 51, 54, 55, 56 |
| Novel Systems/Devices | 19, 38, 36, 39, 40, 41, 42, 43, 44, 45, 46, 60 |
| NOTES non-da Vinci devices | 38, 39 |
| Novel Robotic Manipulator | 40 |
| Percuvance™ Percutaneous Surgical System | 41, 42, 43 |
| Senhance® Surgical System | 44 |
| Medrobotics Flex™ System | 19, 45, 46 |
| Endoeye Flex 3D Videoscope | 36, 43, 60 |
| Single-site Surgery | 39, 48, 49, 50, 51, 52, 53, 54, 55, 56 |
| da Vinci SP Platform | 48, 49, 50, 51, 52, 53, 54, 55, 56 |
| Novel Single Port Device | 39 |
| Telesurgery | 62 |
| Microsurgery | 63 |
3D, three-dimensional; NOTES, natural orifice transluminal endoscopic surgery.
DISCUSSION
Laparoscopic surgery has evolved advantageously in many surgical endeavors, where the da Vinci surgical system provides robotic assistance and enables the surgeon to operate outside of the operating field in a comfortable setting. As the most advanced robotic surgical system currently available, it has dominated the surgical discipline. Though not every procedure significantly benefits from the use of this platform in terms of patient outcomes, many complex procedures require the da Vinci for intricate or tedious surgeries.17 There are multiple studies evaluating the da Vinci for a specific procedure, inquiring of its feasibility, or following up with multiple cases to ensure its efficacy. Many studies found multiple advantages in addition to equivalent performance to that of traditional laparoscopic surgery.
Evaluating the da Vinci Surgical System
Hysterectomies
The article by Advincula et. al. showed the ability of a robotic system to streamline hysterectomies by walking through a typical procedure using the da Vinci robot. Their da Vinci system included the EndoWrist® instruments, which provided the surgeon with greater feedback and thus reduced the fulcrum effect: a consequence of a pivot point on a surgical instrument which forces the surgeon's hand to move in the opposite direction of the end of a tool, making laparoscopic surgery unintuitive.18 Though the da Vinci is able to reduce the fulcrum effect, there are still noted limitations such as lack of haptic feedback.19–22 Some teams utilized alternative methods to correct for this particular disadvantage. In a 2005 case study looking at the da Vinci’s performance for multiple hysterectomies, a KOH™ cervical cup was used as a landmark.23 Sarlos et. al. directly compared robotic and conventional laparoscopic hysterectomies in a matched case-control study published in 2010.20 This study also used the EndoWrist® forceps in the cohort utilizing the da Vinci as a part of the established surgical technique. A part of this study was to evaluate each technique subjectively through a questionnaire given to the surgeons, which revealed that a major advantage to robotic surgery is increased ergonomics and range of motion. Operating time and total costs were the only significant differences, both showing conventional laparoscopic surgery with the advantage; however, the article mentions its limitations such as inability to truly perform a cost analysis and not accounting for the potential for learning curves. Another limitation that was mentioned is the biased nature of the questions posed, such as “Was the absence of haptic feedback a disadvantage”. It should be noted that a hysterectomy is only one common procedure in the gynecologic setting utilizing robotic or laparoscopic techniques. The major indications for robotic surgery listed for the article by Advincula et. al. were endometriosis, abnormal uterine bleeding, fibroids, chronic pelvic pain; and endometrial, ovarian, and fallopian tube cancer.18 The use of the robot for the three cancers listed were for staging of these malignancies. In a review by Truong et. al, it is also noted that robotic assistance is utilized in a variety of procedures in addition to hysterectomies since Advincula et. al, such as myomectomy, endometriosis surgery, sacrocolpopexy, adnexal surgery, tubal reanastomosis, and cerclage.24 The review discusses each of these indications and notes either equal performance with robotic assistance or improvements. Some improvements were increased ability to perform more complicated procedures, better ergonomics with obese patients, and enhanced 3D visualization of the surgical field.
Prostatectomies
Laparoscopic prostatectomies were praised initially for their minimally invasive nature but were hard to perform and constantly evolving even before robotic systems gained traction. Stolzenburg et. al. discussed a novel extraperitoneal approach to radical prostatectomies in 2003 to account for complications that occur with the conventional transperitoneal route.25 The extraperitoneal technique was utilized in the study by Esposito et. al. in their assessment of a fourth arm for robot-assisted radical prostatectomy with the da Vinci system.26 Though the 2003 study was performed with traditional laparoscopic methods, it was mentioned that the use of a robotic arm was especially important to improve ergonomics as well as remove the need for an extra assistant. The article by Lee et. al. also discussed the use of only a single assistant during robotic laparoscopic radical prostatectomies, which differed from the traditional use of two assistants in prior procedures.27 The single assistant would stand adjacent to the robot, which had three arms controlled by a surgeon seated at the console outside of the sterile field. The article discusses proper port placement when a single assistant is involved, but the protocol for this article is specific to a robotic surgical system with three arms and only for this particular surgery. Though it was only for a specific type of surgery, the article implies that the presence of a robotic system in any setting will reduce the amount of required assistants. Traditional laparoscopic procedures would be unable to do this without the advancements provided by a robotic system.27 Zorn et. al. evaluated the da Vinci in terms of error rates, measured by system failures and conversion to open surgery, and found that the system is reliable and safe in that none of the failures culminated in patient injury.28 A 2006 study by Kaufman et. al. introduced the idea of using the postoperative management defined for robotically assisted laparoscopic prostatectomies to increase postoperative outcomes for open radical prostatectomies, opening up a dialogue to continue to improve standards after the da Vinci system was implemented. The changes in management related to diet, pain medication, and drain management, and these changes correlated to decreased complications and readmissions for open prostatectomies.29 Postoperative outcomes for prostatectomies are still being evaluated; however, minor adjustments to the surgical procedure can be made to improve those outcomes. A study published in 2017 by Cestari et. al. evaluated a technique to improve robot-assisted radical prostatectomy outcomes, where a novel 6-branch autologous suburethral sling is applied during the procedure as opposed to a simple sling.30
Cholecystectomies
In 2007 Kang et. al. described a single case using the da Vinci system for a cholecystectomy in 2007, arguing for increased use of the system as the advantages were great enough to promote this system for use with more complex diseases.31 A 2008 article by Jayaraman et. al. discussed multiple cholecystectomy cases, coming to the same conclusion, as laparoscopic cholecystectomies are highly standardized and common.22 One unique disadvantage this article mentioned was the size of the robotic system, which added to difficulty for the surgical team to navigate the operating room. The search brought up an additional study that involved a Roux-en-Y hepaticojejunostomy by Prasad et. al., which was found because it was performed to correct a cholecystectomy bile duct injury.32 It was said that the da Vinci reduces the complexity of this reparatory procedure, mostly due to its 3D view rather than the 2D view of traditional laparoscopy. In addition, Prasad et. al. mentioned there is a greater mobility achieved with the da Vinci system.
Transoral Surgeries
Hatten et. al. retrospectively reviewed multiple cases requiring oropharyngeal reconstruction in which transoral robotic surgery (TORS) was conducted, which was required due to the difficulty in operating site accessibility for traditional laparoscopic surgery.33 In 2002, successful gastro-esophageal reflux repair using the da Vinci was performed using multiple ports, but in 2015, the da Vinci was evaluated for transoral use in the pediatric airway with cadaveric models with more limited success, owing to the confined area of operation.34,35 An alternative to TORS, transoral endoscopic ultrasonic surgery, was evaluated in oropharyngeal tumor resections and was found to be feasible as well as more cost-effective.36 This method combined traditional laparoscopic techniques with an ultrasonic scalpel, which coagulated tissues with a lower heat and thus reduction in tissue injury. This technique was described as similar to microscopic laser surgery; however, the use of the endoscope allowed the technique to be performed without an external incision. Smartt et. al. discussed the use of the da Vinci robotic system for pediatric posterior pharyngeal flap surgery, which was successful in the preclinical model.21 Their experience was overall positive, though disadvantages were noted such as diversity of equipment for use in subspecialties such as pediatric plastic surgery. The major advantage listed was the increased ergonomics during surgery, as this specific procedure is challenging. Another advantage was visualization of velopharyngeal ports, which a robotic system can manage more easily.21 Richmon et. al. describes a feasibility study within the preclinical model of TORS applied to thyroidectomies, which could possibly reduce scarring postoperatively.37
Novel Systems/Devices
Natural Orifice Transluminal Endoscopic Surgery Non-da Vinci Devices
Natural orifice transluminal endoscopic surgery (NOTES) is a specific technique that prevents scarring, as the endoscope is passed through a natural orifice such as the mouth or urethra. Limitations with NOTES are similar to the limitations in laparoscopic surgery: flexibility is restricted and procedures can be overly complex. The search brought up NOTES in five nonreview articles. Gettman et. al. discussed the use of the bladder as a possible entryway for NOTES in a single case, where a flexible ureteroscope allowed for entry and proper visualization of the peritoneal cavity.38 This study only demonstrated the feasibility of the urethra and bladder as a potential natural orifice; however, and once the new portal for NOTES was established, the surgery was then transitioned to the multiple ports using the da Vinci robotic system. An advantage to a transurethral port versus a transgastric port are decreased risk of infection, increased visualization of anatomical structures, anesthetic safety by airway proximity, and improved healing after closure.38 The 2008 article “The mechatronic support system HVSPS and the way to NOTES” discussed the possibility of improving NOTES procedures by introducing a robotic platform with three manipulators each with varying degrees of freedom.39 The goal of this device was to improve NOTES rather than improve surgical outcomes, as such this procedure is lengthy and difficult to perform. This device was first developed for laparoscopic surgery, but there have not been any further developments as of this review.
Novel Robotic Manipulator
One article was able to take lessons learned from multiport robotic surgical systems and apply it to issues regarding systems for single port surgery by applying more pivot points to the robotic arm.40 Kobayashi et. al. discussed a novel system with six degrees of freedom (DOF), which is greater than traditional single port robotic systems, allowing for greater visualization of the anatomical structures. Similarly, robotic surgical systems were built with more DOF than traditional laparoscopic techniques allowed. Extra DOF are applied with two joints within the robotic arm (2 DOF each), rotation within the end-effector (1 DOF), and translation of the base (1 DOF). The device was successful in preclinical models, and once improved could potentially change current single port devices.40 Heller et. al. also discussed the advantage of degrees of freedom with the robotic system as opposed to the laparoscopic technique and included that the camera system of the robot prevents the need to interrupt the surgery to move the camera.34
Percuvance™ Percutaneous Surgical System
Evaluation of the Percuvance™ percutaneous surgical system (PSS) was noted in three separate reports, each discussing a different type of surgery with varied techniques. Percuvance™ is a surgical instrument that can be inserted without a trocar into the skin, which allows for a decreased incision size and is generally less invasive.41 Romano et. al. discussed the use of the PSS in nerve-sparing laparoscopic colposacropexy, where a vaginal prolapse was corrected successfully, and Rossitto et. al. performed a successful total laparoscopic hysterectomy.42,43 Both these studies were early in the development of the PSS. The latest report was published in 2018, evaluating the PSS for laparoscopic cholecystectomy. This study discussed disadvantages such as prolonged operation time and instrumentation mishandling but can be overcome with product updates and learning curves.41
Senhance® Surgical System
The Senhance® system is a new robotic platform that performs similar to the da Vinci, but has an additional eye-tracking feature, where the surgeon can move the laparoscope with eye movement. The article by deBeche-Adams et. al. discussed the presence of a learning curve involved with this feature.44 They also explained the system's benefits, which include improved haptic feedback and ergonomics, as well as decreased costs with reusable instruments. They listed disadvantages such as limited number of instruments, issues with a bulky console, limitations with required calibration for eye-tracking, and procedure-specific constraints. However, the relative novelty of the system suggests the possibility of improvements with upgrades.44
Medrobotics Flex™ System
The Medrobotics Flex™ System, a computer-assisted flexible endoscope, was evaluated for transoral surgery in multiple cadaver models and surgical applications.45 Used on multiple cadaver models, its flexibility allowed for greater access to visualizing the hypopharynx and nasopharynx. It was reported that this system had better haptic feedback than other robotic systems, owing to the flexible as well as compact components.19,46 These preclinical models were shown to be feasible, and a final article by Remacle et. al. discussed the first surgical application of the system for transoral surgery.45 Though the team found the system promising, as of the article the system had not been in use and still needed improvement. More recent data was obtained on this robotic system with positive responses.47
Single-Site Surgery
Single site or single port surgery is a division of robotic surgery that only requires a single incision, for example through the umbilicus in abdominal surgery. Single site surgery can be performed in many different procedures, such as laparoendoscopic-single-site surgery (LESS), LESS-PR (radical prostatectomy), robotic-single-site radical hysterectomy, single port ureteroneocystostomy, single port cholecystectomy, and others. Traditional single-site surgery has a longer learning curve and operating times due to the limited space for laparoscopic instruments to move. Podolsky et. al. wrote an article in 2009 discussing their transumbilical approach to single port access cholecystectomy, where five cases were evaluated for operative and postoperative outcomes using this technique.48 In this instance, articulating instruments were preferred over rigid instruments to better visualize the cystohepatic triangle. Despite the initial success, without a way to improve spatial constraints or ease of technique the limitations involved in performing single-site surgery via traditional methods outweighed the benefits of increased cosmetic and other postoperative outcomes.49 The major advantage to single-site surgery is the decreased invasiveness due to the single incision, as well as its potential as an alternative to NOTES in aerodigestive surgeries, which is limited by suitable equipment. The transition to robotic single site surgery with the da Vinci S® robot was reported by Kaouk et. al. in a multipatient study, which discussed the procedures and outcomes across different surgeries (nephrectomy, pyeloplasty, etc.), all of which involved a single transumbilical port.50 This initial report of the robotic system demonstrated the ability of that system to improve the surgeon’s comfort, though the article data was not obtained in a controlled trial.
The da Vinci SP® Platform
Some articles discussed single surgical techniques in case reports or studies and evaluated or reflected on the performance of the single port robotic system. The 2018 article by Garisto et. al. discussed a transperineal approach to ileal conduit and urinary diversions, where a single port was utilized.51 Port access was aided by a GelPOINT® Mini advanced access platform, where a flexible membrane surrounds the instrumentation of a single arm of the da Vinci SP1098 system. This team wrote another article in 2019, reporting a similar technique for single-port transperineal cystoprostatectomy, which included diverting urinary drainage through an ileal conduit and a lymph node dissection, all using the da Vinci SP® platform.52 Both articles included a walkthrough of a single case, discussing a successful procedure without the need to transition to multiple ports. Gaboardi et. al. studied multiple cases with the robotic laparoendoscopic single site radical prostatectomy procedure and discussed drawbacks to the da Vinci single site platform, noting the weakness of the needle holder, the lack of the EndoWrist® add-on from previous da Vinci models, and instrumentation conflicts.53 The authors recommended modified techniques until the platform was improved. The article by Escobar et. al. describes an early look at docking and suturing considerations for successful hysterectomies in a cadaveric model performed with the da Vinci single site platform; however, the article is from 2012 and there are more recent clinical studies, which were not identified in the search but have been published regarding robotic single site hysterectomies.54,55 Hye-Sung Moon published a report on how to improve single site hysterectomy, describing the best technique to avoid difficulties in vaginal cuff suturing.55 A ureteroneocystostomy was performed in 2019 by Hebert et. al. using the da Vinci SP® platform, commenting on the “snake-like” articulation of each instrument owing to their multiple joints.56 Robotic-assisted simple prostatectomy is one of multiple procedures as treatment for benign prostatic enlargement, and was also adapted to a single-port platform. Steinberg et. al. described this technique with multiple cases in 2019 and it was determined to be feasible and effective, though with low external validity as all data was acquired through one surgeon’s efforts.57 One issue encountered was limited camera mobility if all 3 robotic arms were used. Using a second robotic system was required to allow the camera and the instruments to move separately. This hindrance could suggest improvement with a traditional laparoscopic approach, where all instruments, including the laparoscope, are separate.
Novel Single Port Device
Highly versatile single port system, is a system developed by Can et. al. as a more flexible instrument to improve single-port laparoscopic surgery.39 Introduced in 2008, the system has not had any updates since. The system was last presented by Can et. al. at a conference and described the purpose of the system to be used for NOTES rather than as an improvement to more traditional laparoscopic procedures.58
Clinical Trials
In the search, only 3 clinical trials were relevant. The oldest clinical trial was conducted in 2006 regarding robotic-assisted laparoscopic prostatectomy, which is now a common procedure.59 One interesting finding was the improvement in operative time for the later surgeries by the same team, though it is mentioned that their times were longer than other publications had reported due to certain obstacles, such as a lack of initial training with the robot and a higher rate of patient obesity in their cohort. The 2011 clinical trial to compare the newer model of the da Vinci (the da Vinci S®) and the original model noted the S robot was built with improvements such as increased range of motion and newer docking system, and mentioned an exclusion criteria for the study in which the S robot was specifically requested.17 The technical advantages were not discussed further, as the article’s purpose was to show differences in postsurgical outcomes. Overall, the only statistically significant difference was the mean operative time; the S model decreased mean operating time by 22 minutes, and the author theorizes that the improved operating time is due to the docking system. The lack of improvement in other areas suggests that the newer model is primarily improving ease of use by the surgeon and patient outcomes are not affected. The newest clinical trial, conducted in 2018, looked at the feasibility and safety of robotic single site radical hysterectomy in addition to pelvic lymphadenectomy specifically, and reasoned that LESS is a procedure with cosmetic and noninvasive benefits, but is increasingly challenging due to angular constraints in regards to the surgical instruments.49 The study was prospective and applied the technique to 20 total patients, performing slightly different subtypes of the surgery and recording data such as postsurgical outcomes and other surgical parameters. Though much data was recorded, no statistical analysis was performed as this was a pilot study with a small number of patients, which limits the use of this data. However, the study discussion provided valuable insight into the surgical technique itself, referencing methods to avoid certain obstacles, such as the use of a straight needle during medialization of the umbilical arteries, which shows the potential for practical improvements as more surgeons utilize LESS as a technique.
3D Vision
One advantage of the da Vinci that has been commonly referenced is the ability to have a 3D view of the surgical field during surgery. Most agree the 3D view is an improvement over older 2D laparoscopic imaging systems, though Zorn et. al. shows that surgeons with greater experience tended toward less conversion to open surgery even when loss of the 3D view occurred.28 Three articles within the search that did not operate with the da Vinci system utilized the Endoeye Flex 3D Videoscope seemingly to compensate, which was a tool that potentially replaced 3D advantage of the da Vinci. Vizzielli et. al. discussed the use of this instrument in a laparoscopic pelvic exenteration with radical vaginectomy and found it feasible, specifically noting its potential to reduce error during surgeries performed with less experience.60
Telesurgery
Though only three articles in the initial search discussed telesurgery, only one was relevant and evaluated in this review. Telesurgery utilizes the dual platform of robotic systems and applies it to a greater distance and is becoming increasingly considered as telemedicine services have grown more prominent.61 The article by Korte et. al. discusses the impact of time delays when operating a simplified master-slave robotic system split across two separate locations.62 Their study looked at a specific task with a nonsurgical robot to prevent excessive variability with a more complex robotic system, and the console and device were in two separate buildings. They found a significant increase in the time to complete a task as artificially imposed times increased, but discussed the potential for a learning curve through novice and experienced user comparisons. Though the potential for lag within surgery is a large hurdle, the use of a robotic surgical system across two separate locations has implications for increasing the ability of international medical aid, such as in military or relief operations.
Microsurgery
Robotic systems are not only used as a replacement for traditional laparoscopy; they are frequently requested for microsurgery, requiring microscopic and precise techniques. New devices to improve this application of a robotic system are being developed. Chauhan et. al proposed a device for robotic microsurgical forceps with 2 DOF labeled RMF-2DOF to improve haptic feedback within a limited area.63 Haptic feedback is a frequently discussed criticism of the da Vinci surgical system (Table 2). Their design addressed this concern by applying a force sensor to simulate haptic feedback but showed that there was a learning curve in order to properly benefit from this addition. This device was created to be used with transoral laser microsurgery, which allows the surgeon to enter the oral cavity with a laryngoscope to access the larynx or pharynx. This is normally performed with microscopic laryngoscopy without the use of a robotic system. The article mentions previously established solutions to replace traditional LM with robotic-assistance; however, specified limitations such as inadequate sizing for tool shafts or issues with gripping force which are addressed with the RMF-2DOF device. This device was created recently, and as of this review, further evaluations of the feasibility or efficacy of this device have not been published.
Future Considerations
The da Vinci surgical system is built to be able to operate within a 3D space without requiring assistants to hold instruments in place. Traditional laparoscopic surgery requires multiple assistants to at minimum hold the endoscope in place and can be physically taxing for complicated surgeries. There is a large gap between robotic and traditional laparoscopic surgery in terms of technical functions and their utilization in that some procedures may fall in the middle when seeking for an optimal procedure. As robotic systems advance, adjustments to traditional laparoscopic surgery can be made to reflect their advantages. The Endoeye Flex 3D Videoscope specifically mirrored the ability of robotic systems to view the surgical field in 3D, whether intentionally or otherwise. Similarly, the precise movements of a completely robotic system could also have implications for an application of traditional laparoscopy where a braking system is applied to each surgical instrument. In an effort to bridge the gap, an interdisciplinary team of engineering and clinical investigators are working towards a tangible semirobotic laparoscopy system that integrates critical functions of robotic technologies yet simple enough to be performed in a traditional laparoscopic surgical environment.
Limitations
The main limitation of this review is the difficulty in performing a search that selects for every relevant article. When a novel device was included in the original search, an additional search performed revealed newer articles that were inexplicably excluded though they had the same key words. Another limitation to this review is that while there is an abundance of comparative literature and case reports from the early days of the da Vinci, this system is improving so rapidly that reports on its current performance have yet to be written. In addition, though many of the reports have a high number of patient data, much of these reports are conducted by a small number of surgeons in a single setting.
CONCLUSIONS
The introduction of minimally invasive techniques in the surgical field has invited a surge of advancements in an attempt to improve both surgeon and patient experiences. A review of 44 articles within four different surgical procedures displayed a lack of improvements in traditional laparoscopic surgery and heavy reliance on robotic systems. Analysis of articles that evaluated the performance of robotic laparoscopic procedures can aid in the endeavor to improve traditional laparoscopic surgeries by learning from the advantages of the fully robotic system.
Footnotes
Acknowledgements: This work was supported by UCF College of Medicine Focused Inquiry Research Experience (FIRE) Program. Also, this material is based upon work supported by the National Science Foundation under Grant No. 2026516.
Disclosure: none.
Funding sources: UCF College of Medicine Focused Inquiry Research Experience (FIRE) Program.
Conflict of interests: none.
Informed consent: Tovah Williamson declares that written informed consent was obtained from the patient/s for publication of this study/report and any accompanying images.
Contributor Information
Tovah Williamson, University of Central Florida College of Medicine, Orlando, FL..
Sang-Eun Song, University of Central Florida, Department of Mechanical and Aerospace Engineering, Orlando, FL..
References:
- 1.Nezhat F. Triumphs and controversies in laparoscopy: the past, the present, and the future. JSLS. 2003;7(1):1–5. [PMC free article] [PubMed] [Google Scholar]
- 2.Berci G, Davids J. Endoscopy and television. BMJ. 1962;1(5292):1610–1613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Genc V, Sulaimanov M, Cipe G, et al. What necessitates the conversion to open cholecystectomy? A retrospective analysis of 5164 consecutive laparoscopic operations. Clinics (Sao Paulo, Brazil) 2011;66(3):417–420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sormaz İC, Soytaş Y, Gök AFK, Özgür İ, Avtan L. Fundus-first technique and partial cholecystectomy for difficult laparoscopic cholecystectomies. Ulus Travma Acil Cerrahi Derg. 2018;24(1):66–70. [DOI] [PubMed] [Google Scholar]
- 5.Philipose KJ, Sinha B. Laparoscopic surgery. Med J Armed Forces India. 1994;50(2):137–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bove P, Iacovelli V, Celestino F, De Carlo F, Vespasiani G, Finazzi Agrò E. 3D vs 2D laparoscopic radical prostatectomy in organ-confined prostate cancer: comparison of operative data and pentafecta rates: a single cohort study. BMC Urol. 2015;15(1):12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Alkatout I, Mettler L, Maass N, Noé GK, Elessawy M. Abdominal anatomy in the context of port placement and trocars. J Turk Ger Gynecol Assoc. 2015;16(4)241–251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Manatakis DK, Georgopoulos N. Reducing the cost of laparoscopy: reusable versus disposable laparoscopic instruments. Minim Invasive Surg. 2014:408171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ahmad G, O'Flynn H, Duffy JM, Phillips K, Watson A. Laparoscopic entry techniques. Cochrane Database Syst Rev. 2012(2):CD006583. [DOI] [PubMed] [Google Scholar]
- 10.George EI, Brand TC, LaPorta A, Marescaux J, Satava RM. Origins of robotic surgery: from skepticism to standard of care. JSLS. 2018;22(4):e2018.00039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Marescaux J, Rubino F. The ZEUS robotic system: experimental and clinical applications. Surg Clin North Am. 2003;83(6):1305–1315. [DOI] [PubMed] [Google Scholar]
- 12.Ngu JC, Tsang CB, Koh DC. The da Vinci Xi: a review of its capabilities, versatility, and potential role in robotic colorectal surgery. Robot Surg. 2017;4:77–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Intuitive Surgical Inc. Intuitive Annual Report 2019. Intuitive Surgical, Inc.; 2019. Accessed February 8, 2021. https://www.annualreports.com/HostedData/AnnualReportArchive/i/NASDAQ_ISRG_2019.pdf [Google Scholar]
- 14.Kiely DJ, Gotlieb WH, Lau S, et al. Virtual reality robotic surgery simulation curriculum to teach robotic suturing: a randomized controlled trial. J Robot Surg. 2015;9(3):179–186. [DOI] [PubMed] [Google Scholar]
- 15.Cadière GB, Himpens J, Germay O, et al. Feasibility of robotic laparoscopic surgery: 146 cases. World J Surg. 2001;25(11):1467–1477. [DOI] [PubMed] [Google Scholar]
- 16.Gkegkes ID, Mamais IA, Iavazzo C. Robotics in general surgery: a systematic cost assessment. J Minim Access Surg. 2017;13(4):243–255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shah K, Abaza R. Comparison of intraoperative outcomes using the new and old generation da Vinci® robot for robot-assisted laparoscopic prostatectomy. BJU Int. 2011;108(10):1642–1645. [DOI] [PubMed] [Google Scholar]
- 18.Advincula AP. Surgical techniques: robot-assisted laparoscopic hysterectomy with the da Vinci surgical system. Int J Med Robot. 2006;2(4):305–311. [DOI] [PubMed] [Google Scholar]
- 19.Richmon JD. Transoral palate-sparing nasopharyngectomy with the Flex® System: preclinical study. Laryngoscope. 2015;125(2):318–322. [DOI] [PubMed] [Google Scholar]
- 20.Sarlos D, Kots L, Stevanovic N, Schaer G. Robotic hysterectomy versus conventional laparoscopic hysterectomy: outcome and cost analyses of a matched case-control study. Eur J Obstet Gynecol Reprod Biol. 2010;150(1):92–96. [DOI] [PubMed] [Google Scholar]
- 21.Smartt JM, Jr., Gerety P, Serletti JM, Taylor JA. Application of a robotic telemanipulator to perform posterior pharyngeal flap surgery: a feasibility study. Plast Reconstr Surg. 2013;131(4):841–845. [DOI] [PubMed] [Google Scholar]
- 22.Jayaraman S, Davies W, Schlachta CM. Getting started with robotics in general surgery with cholecystectomy: the Canadian experience. Can J Surg. 2009;52(5):374–378. [PMC free article] [PubMed] [Google Scholar]
- 23.Beste TM, Nelson KH, Daucher JA. Total laparoscopic hysterectomy utilizing a robotic surgical system. JSLS. 2005;9(1):13–15. [PMC free article] [PubMed] [Google Scholar]
- 24.Truong M, Kim JH, Scheib S, Patzkowsky K. Advantages of robotics in benign gynecologic surgery. Curr Opin Obstet Gynecol. 2016;28(4):304–310. [DOI] [PubMed] [Google Scholar]
- 25.Stolzenburg JU, Truss MC, Do M, et al. Evolution of endoscopic extraperitoneal radical prostatectomy (EERPE)–technical improvements and development of a nerve-sparing, potency-preserving approach. World J Urol. 2003;21(3):147–152. [DOI] [PubMed] [Google Scholar]
- 26.Esposito MP, Ilbeigi P, Ahmed M, Lanteri V. Use of fourth arm in da Vinci robot-assisted extraperitoneal laparoscopic prostatectomy: novel technique. Urology. 2005;66(3):649–652. [DOI] [PubMed] [Google Scholar]
- 27.Lee DI, Eichel L, Skarecky DW, Ahlering TE. Robotic laparoscopic radical prostatectomy with a single assistant. Urology. 2004;63(6):1172–1175. [DOI] [PubMed] [Google Scholar]
- 28.Zorn KC, Gofrit ON, Orvieto MA, et al. Da Vinci robot error and failure rates: single institution experience on a single three-arm robot unit of more than 700 consecutive robot-assisted laparoscopic radical prostatectomies. J Endourol. 2007;21(11):1341–1344. [DOI] [PubMed] [Google Scholar]
- 29.Kaufman MR, Smith JA, Jr., Baumgartner RG, et al. Positive influence of robotically assisted laparoscopic prostatectomy on the collaborative-care pathway for open radical prostatectomy. BJU Int. 2006;97(3):473–475. [DOI] [PubMed] [Google Scholar]
- 30.Cestari A, Soranna D, Zanni G, et al. Intraoperative retrograde perfusion sphincterometry to evaluate efficacy of autologous vas deferens 6-branch suburethral sling to properly restore sphincteric apparatus during robot-assisted radical prostatectomy. J Endourol. 2017;31(9):878–885. [DOI] [PubMed] [Google Scholar]
- 31.Kang CM, Chi HS, Hyeung WJ, et al. The first Korean experience of telemanipulative robot-assisted laparoscopic cholecystectomy using the da vinci system. Yonsei Med J. 2007;48(3):540–545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Prasad A, De S, Mishra P, Tiwari A. Robotic assisted Roux-en-Y hepaticojejunostomy in a post-cholecystectomy type E2 bile duct injury. World J Gastroenterol. 2015;21(6):1703–1706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hatten KM, Brody RM, Weinstein GS, et al. Defining the role of free flaps for transoral robotic surgery. Ann Plast Surg. 2018;80(1):45–49. [DOI] [PubMed] [Google Scholar]
- 34.Heller K, Gutt C, Schaeff B, Beyer PA, Markus B. Use of the robot system Da Vinci for laparoscopic repair of gastro-oesophageal reflux in children. Eur J Pediatr Surg. 2002;12(4):239–242. [DOI] [PubMed] [Google Scholar]
- 35.Rahbar R, Ferrari LR, Borer JG, Peters CA. Robotic surgery in the pediatric airway: application and safety. Arch Otolaryngol Head Neck Surg. 2007;133(1):46–50; discussion 50. [DOI] [PubMed] [Google Scholar]
- 36.Fernández-Fernández MM, Montes-Jovellar L, Parente Arias PL, Ortega Del Alamo P. Transoral endoscopic ultraSonic surgery (TOUSS): a preliminary report of a novel robotless alternative to TORS. Eur Arch Otorhinolaryngol. 2015;272(12):3785–3791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Richmon JD, Pattani KM, Benhidjeb T, Tufano RP. Transoral robotic-assisted thyroidectomy: a preclinical feasibility study in 2 cadavers. Head Neck. 2011;33(3):330–333. [DOI] [PubMed] [Google Scholar]
- 38.Gettman MT, Blute ML. Transvesical peritoneoscopy: initial clinical evaluation of the bladder as a portal for natural orifice translumenal endoscopic surgery. Mayo Clin Proc. 2007;82(7):843–845. [DOI] [PubMed] [Google Scholar]
- 39.Can S, Fiolka A, Mayer H, et al. The mechatronic support system “HVSPS” and the way to NOTES. Minim Invasive Ther Allied Technol. 2008;17(6):341–345. [DOI] [PubMed] [Google Scholar]
- 40.Kobayashi Y, Sekiguchi Y, Noguchi T, et al. Development of a robotic system with six-degrees-of-freedom robotic tool manipulators for single-port surgery. Int J Med Robot. 2015;11(2):235–246. [DOI] [PubMed] [Google Scholar]
- 41.Sapalidis K, Katsaounis A, Mantalovas S, et al. Complete percutaneous laparoscopic cholecystectomy by employing the Percuvance Percutaneous Surgical System. Ann Transl Med. 2019;7(7):139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Romano F, Legge F, Scambia G, Guido M. Nerve-sparing laparoscopic colposacropexy using a percutaneous surgical system: a case report. J Minim Invasive Gynecol. 2017;24(4):536–537. [DOI] [PubMed] [Google Scholar]
- 43.Rossitto C, Gueli Alletti S, Costantini B, Fanfani F, Scambia G. Total laparoscopic hysterectomy with percutaneous (Percuvance) instruments: new frontier of minimally invasive gynecological surgery. J Minim Invasive Gynecol. 2016;23(1):14–15. [DOI] [PubMed] [Google Scholar]
- 44.deBeche-Adams T, Eubanks WS, de la Fuente SG. Early experience with the Senhance®-laparoscopic/robotic platform in the US. J Robot Surg. 2019;13(2):357–359. [DOI] [PubMed] [Google Scholar]
- 45.Remacle M, M N Prasad V, Lawson G, Plisson L, Bachy V, Van der Vorst S. Transoral robotic surgery (TORS) with the Medrobotics Flex™ System: first surgical application on humans. Eur Arch Otorhinolaryngol. 2015;272(6):1451–1455. [DOI] [PubMed] [Google Scholar]
- 46.Friedrich DT, Scheithauer MO, Greve J, et al. Application of a computer-assisted flexible endoscope system for transoral surgery of the hypopharynx and upper esophagus. Eur Arch Otorhinolaryngol. 2017;274(5):2287–2293. [DOI] [PubMed] [Google Scholar]
- 47.Sethi N, Gouzos M, Padhye V, et al. Transoral robotic surgery using the Medrobotic Flex® system: the Adelaide experience. J Robot Surg. 2020;14(1):109–113. [DOI] [PubMed] [Google Scholar]
- 48.Podolsky ER, Rottman SJ, Poblete H, King SA, Curcillo PG. Single port access (SPA) cholecystectomy: a completely transumbilical approach. J Laparoendosc Adv Surg Tech A. 2009;19(2):219–222. [DOI] [PubMed] [Google Scholar]
- 49.Vizza E, Chiofalo B, Cutillo G, et al. Robotic single site radical hysterectomy plus pelvic lymphadenectomy in gynecological cancers. J Gynecol Oncol. 2018;29(1):e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Kaouk JH, Goel RK, Haber GP, Crouzet S, Stein RJ. Robotic single-port transumbilical surgery in humans: initial report. BJU Int. 2009;103(3):366–369. [DOI] [PubMed] [Google Scholar]
- 51.Garisto J, Bertolo R, Kaouk J. Transperineal approach for intracorporeal ileal conduit urinary diversion using a purpose-built single-port robotic system: step-by-step. Urology. 2018;122:179–184. [DOI] [PubMed] [Google Scholar]
- 52.Garisto J, Bertolo R, Chan E, Kaouk J. Single-port trans-perineal approach to cystoprostatectomy with intracorporeal ileal conduit urinary diversion and lymph-nodes dissection using a purpose-built robotic system: surgical steps in a preclinical model. International Braz j Urol: official Journal of the Brazilian Society of Urology. 2019;45(4):854–855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Gaboardi F, Pini G, Suardi N, Montorsi F, Passaretti G, Smelzo S. Robotic laparoendoscopic single-site radical prostatectomy (R-LESS-RP) with daVinci Single-Site® platform. Concept and evolution of the technique following an IDEAL phase 1. J Robot Surg. 2019;13(2):215–226. [DOI] [PubMed] [Google Scholar]
- 54.Escobar PF, Knight J, Rao S, Weinberg L. da Vinci® single-site platform: anthropometrical, docking and suturing considerations for hysterectomy in the cadaver model. Int J Med Robot. 2012;8(2):191–195. [DOI] [PubMed] [Google Scholar]
- 55.Moon HS. Tips on robotic single-site surgery suture technique: screwing and clockwise direction suture technique for robotic single-site surgery. Taiwan J Obstet Gynecol. 2018;57(3):432–434. [DOI] [PubMed] [Google Scholar]
- 56.Hebert KJ, Joseph J, Gettman M, Tollefson M, Frank I, Viers BR. Technical considerations of single port ureteroneocystostomy utilizing da Vinci SP platform. Urology. 2019;129:236. [DOI] [PubMed] [Google Scholar]
- 57.Steinberg RL, Passoni N, Garbens A, Johnson BA, Gahan JC. Initial experience with extraperitoneal robotic-assisted simple prostatectomy using the da Vinci SP surgical system. J Robot Surg. 2020;14(4):601–607. [DOI] [PubMed] [Google Scholar]
- 58.Can S, Staub C, Knoll A, Fiolka A, Schneider A, Feussner H. Design, development and evaluation of a highly versatile robot platform for minimally invasive single-port surgery. 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob). 2012, Rome, Italy. [Google Scholar]
- 59.Mikhail AA, Orvieto MA, Billatos ES, et al. Robotic-assisted laparoscopic prostatectomy: first 100 patients with one year of follow-up. Urology. 2006;68(6):1275–1279. [DOI] [PubMed] [Google Scholar]
- 60.Vizzielli G, Perrone E, Pizzacalla S, Scambia G, Ercoli A. Laparoscopic pelvic exenteration with radical vaginectomy using 3-dimensional vision and multifunction instrument. Int J Gynecol Cancer. 2018;28(9):1805–1806. [DOI] [PubMed] [Google Scholar]
- 61.Koonin LM, Hoots B, Tsang CA, et al. Trends in the use of telehealth during the emergence of the COVID-19 pandemic - United States, January-March 2020. MMWR Morb Mortal Wkly Rep. 2020;69(43):1595-1599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Korte C, Nair SS, Nistor V, Low TP, Doarn CR, Schaffner G. Determining the threshold of time-delay for teleoperation accuracy and efficiency in relation to telesurgery. Telemed J E Health. 2014;20(12):1078–1086. [DOI] [PubMed] [Google Scholar]
- 63.Chauhan M, Deshpande N, Pacchierotti C, et al. A robotic microsurgical forceps for transoral laser microsurgery. Int J Comput Assist Radiol Surg. 2019;14(2):321–333. [DOI] [PubMed] [Google Scholar]