

Abstract
Objective
To investigate postural control related to a lower limb exoskeleton (Chairless Chair) when (a) reaching for a working tool, and (b) an external perturbation occurs.
Background
Lower limb exoskeletons aiming to reduce physical load associated with prolonged standing may impair workers’ postural control and increase the risk of falling.
Method
Forty-five males were reaching for an object (3-kg dumbbell) at the lateral end of their reaching area without the exoskeleton in upright standing (STAND) and with the exoskeleton at a high (EXOHIGH.SEAT) and low sitting position (EXOLOW.SEAT). The task was performed with the object placed in three different angles (120°, 150°, and 180°) in the transversal plane. The minimum absolute static postural stability (SSABS.MIN) as the shortest distance (mm) of the center of pressure to the base of support border was measured (zero indicates risk of falling). Additionally, eight subjects were standing without the exoskeleton or sitting on it (EXOHIGH.SEAT and EXOLOW.SEAT) while being pulled backward. The tilting moment when subjects lost their balance was assessed.
Results
SSABS.MIN was lower when using the exoskeleton (p < .05) but still about 17 mm. The location of the object to be reached had no influence. Tilting moments of less than 30 nm were sufficient to let people fall backward when sitting on the exoskeleton (50 nm for STAND).
Conclusion
Impairments in postural control by the exoskeleton may not be relevant when reaching laterally for objects up to 3 kg. When an external perturbation occurs, the risk of falling may be much higher; irrespective of factors like uneven or slippery flooring.
Application
The risk of falling using the exoskeleton seems to be low when reaching laterally for an object of up to 3 kg. In situations where, for example, a collision with coworkers is likely, this exoskeleton is not recommended.
Keywords: occupational safety, assistive device, center of pressure, risk of falling, exoskeleton
Introduction
The prevention of work-related musculoskeletal disorders (WMSDs) is one of the current challenges in occupational safety and health research. Despite existing knowledge about work-related physical risk factors (da Costa & Vieira, 2010; Punnett & Wegman, 2004), WMSDs continue to be a major health problem in the working population and a burden to economy and health care systems (Bevan, 2015; Sultan-Taïeb et al., 2017).
As a result of recent technical advances, exoskeletons that support workers performing occupational tasks have emerged and now offer a new kind of intervention to reduce physical exposures that may contribute to the prevention of WMSDs. These wearable, external, mechanical structures aim at enhancing the power of a person (de Looze et al., 2016) and reducing biomechanical loads (Huysamen et al., 2018).
A potential passive exoskeleton supporting the lower limbs is the Chairless Chair (noonee AG, Switzerland, model: mechpunk). It is designed to reduce physical load associated with prolonged standing in standing workplaces characterized by space restrictions and without the possibility of using chairs or standing aids, and in standing workplaces where the working height frequently changes and cannot be adequately adjusted to workers’ anthropometry. The Chairless Chair consists of two plastic supports worn on the lower limbs with a seating shell at the top of each support. This allows the user to sit in different sitting heights and around 60% of the physical load (i.e., body weight) carried by the lower limbs can be transferred to the ground by the exoskeleton supports (Luger et al., 2019b).
Although the use of exoskeletons in the occupational field is receiving increasing scientific attention, the focus seems to be more on exoskeletons supporting the back/trunk and upper extremities (Bosch et al., 2016; Theurel et al., 2018; Weston et al., 2018). Recent studies of back/trunk and upper extremity exoskeletons mainly address its effects on physical demands and user acceptance (Bosch et al., 2016; Huysamen et al., 2018; Rashedi et al., 2014). The few studies that deal with exoskeletons in an occupational setting for the lower extremity are mainly from our own group and focus on similar aspects including physical demands, body posture, and perceived discomfort (Luger et al., 2019a, 2019b). Besides these commonly addressed parameters, it is highly relevant to investigate safety-related aspects for a safe implementation and application of exoskeletons. In the case of the Chairless Chair, estimating the risk of falling by measures of postural stability is a reasonable safety aspect, since this exoskeleton interferes with the lower limbs of the exoskeleton user. In the field of rehabilitation, an additional risk of falling associated with using lower limb exoskeletons has already been reported (He et al., 2017). It is assumed that the interaction of the body with the environment (ground) is reduced or distorted because of an extra layer of media imposed by the exoskeleton or that the execution of certain movements cannot correctly be achieved because of the physical constraint related to the exoskeleton (He et al., 2017). These mechanisms may also put healthy workers using the Chairless Chair at a higher risk of falling.
To ensure static postural stability, the center of gravity (COG) has to be kept within the base of support (BOS) boundaries (Holbein & Redfern, 1997). Otherwise, a person could fall or has to adjust his posture to maintain or regain equilibrium. This concept can be objectively assessed by measuring the linear displacement of the center of pressure (COP) with respect to the BOS according to Holbein and Redfern (1997). For the Chairless Chair, disturbances in the posterior direction may be of special interest since the leg supports of the Chairless Chair, which are located directly behind the user’s feet, may avoid postural adjustments by changing the foot position.
In a previous paper, we already reported that static standing stability when using the Chairless Chair exoskeleton did not meaningfully decrease during a simulated repetitive industrial task. This task was characterized by an ergonomic posture and with no fast movements of the arms or the torso which could disturb balance (Luger et al., 2019b).
The present study supplements our initial experiments by investigating the risk of falling during two other typical working situations when using the Chairless Chair, which induce more disturbances to postural stability. One situation is the reaching for a tool or material; the other situation is a contact or collision that may occur when working with coworkers or robots at the same product. At ergonomically designed industrial workplaces, the workpiece is located close to the worker’s body in the so-called primary zone. Tools or materials that are only used rarely can be placed in the tertiary zone, which is characterized by maximal reaching (Canadian Centre for Occupational Health & Safety, 2020) and requires a shift of the body mass, thus affecting postural stability. Furthermore, working at an industrial production line requires the collaboration of several workers for a quick and efficient production. Also, working together with industrial robots is getting more common in the industry (Leso et al., 2018). In both cases, contacts between coworkers or between robot and human are unavoidable (Park et al., 2019). With respect to human–robot collaboration, a lot of research effort has been devoted to determine what type of contact is tolerable in order to prevent injuries (Dagalakis et al., 2016; Melia et al., 2019). Whether such collisions are sufficient to provoke a fall when workers are sitting on the Chairless Chair is unclear. In this respect, the aims were (a) to assess postural stability during a simulated occupational task where workers reach for a tool at the lateral end of their reaching area, and (b) to determine the tilting moment necessary to induce falling by an external perturbation referring to situations where a collision with coworkers or collaborating robots may occur. Aim (b) was further diversified by testing whether body weight and foot position have an influence on the tilting moments, since both factors may modify postural control (Błaszczyk et al., 2009; de Santiago et al., 2013).
Material and Methods
Lower Limb Passive Exoskeleton
The Chairless Chair (3.8 kg) consists of two plastic supports attached to the back of the workers’ legs. Each support can be adjusted in length and has a hinge joint at knee level and seat shells below the buttocks. These supports are fixed to the worker by foot brackets, thigh and hip belts, and a torso vest (Figure 1a). The worker is able to walk with the exoskelton and sit down whenever desired, applying different sitting heights. After the onset of this study, the manufacturer of the Chairless Chair developed a new foot module (EXONEW), which allowed workers to increase their supporting surface, that is, their BOS, while sitting on the EXONEW (Figure 1b). This new version of the Chairless Chair was included by a study amendment.
Figure 1.

(a) The passive lower limb exoskeleton (Chairless Chair; model: Mechpunk). (b) The enhanced foot module of the passive lower limb exoskeleton (Chairless Chair) to increase the supporting area.
Study Design
The study included three experiments of which two are reported in this paper. The third experiment was a simulated manual task with the main focus on quantifying exoskeleton induced changes in physical load, body postures, postural stability, and perceived discomfort (Luger et al., 2019a, 2019b). In the current study, the two remaining experiments addressing postural stability are reported.
Experiment I
A reaching task without external perturbations was simulated, representing occupational situations within which workers reach for an object (e.g., a working tool or material) at the lateral end of their reaching area. The position of the target object (three levels) and exoskeleton condition (three levels) were varied. The position of the target object was determined by three transversal adduction angles in the shoulder of 120°, 150°, and 180° (Figure 2(c)). These positions were chosen because they require different head or torso rotation during the reaching task, which could more or less disturb postural control. Knowledge of which object positions may increase the risk of falling when using the Chairless Chair would be important for occupational practice. Exoskeleton condition counted three levels, including standing without the exoskeleton (STAND) and sitting on the exoskeleton in a low (90° knee angle; EXOLOW.SEAT) and high configuration (120° knee angle; EXOHIGH.SEAT). We used the STAND condition for comparison with the two exoskeleton conditions since a major application of the Chairless Chairs is to substitute prolonged standing at workplaces where using a stool is not possible, for example, due to space restriction. Note that the Chairless Chair with the “old” foot module was evaluated in this experiment. The two independent variables resulted in nine experimental conditions that were offered to the subjects in a cross-over design. The order of the nine conditions was randomly allocated to the subjects using a Latin Square (double Williams) design for uneven number of conditions (Williams, 1949).
Figure 2.

Experiment I. (a) Subjects reaching for a 3-kg object at the lateral end of the reaching area. (b and c) Reaching is repeated for three different object positions based on three angles (120°, 150°, 180°) in the transversal plane.
Experiment II
The tilting moments that would induce falling were assessed, referring to situations where a collision with a coworker, robot, or workpiece may occur. In this experiment, both exoskeletons with the “old” and “new” foot module were evaluated. The difference in exoskeleton condition (five levels) was investigated using a cross-over design without randomizing the order of the conditions, including standing without the Chairless Chair (STAND), and sitting on the “old” and “new” exoskeleton in a low (90° knee angle; EXOLOW.SEAT and EXONEW.LOW.SEAT) and high configuration (120° knee angle; EXOHIGH.SEAT and EXONEW.HIGH.SEAT).
Study Population
Experiment I
Forty-five healthy male subjects were included. Exclusion criteria were musculoskeletal and systemic disorders, any known impairments in postural control or motor function, acute pain, illness or drug addiction. Inclusion criterion was age between 18 and 40 years to preclude potential age effects. No studies were available providing parameters for a sample size calculation (i.e., the effect of exoskeleton on postural control). Therefore, the sample size was based on the cross-over design including seven main conditions as applied in the main experiment (Luger et al., 2019b). Luger et al. (2019b) applied a Latin Square (double Williams) design for seven conditions to avoid first-order carry-over effects. An additional but not main independent variable in the main experiment was working distance (three levels), of which a full-factorial cross-over design includes six different orders. The seven sequences of the double William design were multiplied by six, in order to keep the variable working distance full-factorial, resulting in a minimum of 42 participants. We decided to include only male subjects to investigate the effects of the exoskeleton in a rather homogenous group of subjects, knowing that this limits the generalizability of the study results.
Experiment II
Eight subjects without age restriction participated. This small number of subjects was chosen due to the exploratory approach of this research question. Exclusion criteria were the same as in Experiment I. No sample size calculation was applied for this explorative investigation.
Subjects of both experiments gave their informed written consent prior to study inclusion. This research complied with the tenets of the declaration of Helsinki and was approved by the Ethics Committee of the University Hospital of Tübingen, Germany (project-number: 184/2017BO2). The study was registered at ClinicalTrials.gov (NCT03134144).
Experimental Procedure
Experiment I
On day one, subjects were familiarized with the exoskeleton and experimental conditions (about 30 min). After adjusting the exoskeleton to the subjects’ body size, the investigator verbally instructed each subject to place both buttocks on the sitting shell and secured the subject from behind when testing different sitting heights (about 10 min). Thereafter, each subject had to perform an industrial task (screwing, clip fitting, and cable mounting) for about 20 min while sitting on the Chairless Chair.
Additionally, inclusion and exclusion criteria were verified. On a second day, after being equipped with the measurement devices, the subjects performed the reaching task. Subjects had to reach for and transfer a 3-kg object. They grabbed the object (dumbbell) with one hand from a table next to their body at the one end of the lateral reaching area, handed it over to the other hand in front of their body, and put it down on a table next to their body at the other end of the lateral reaching area. Then, subjects performed the task the other way around. Subjects had to proceed with the task and perform fluently for a 30-s duration at a self-selected pace without changing their foot position. Prior to the task, the table height was adjusted to ensure that the dumbbell was grabbed by each subject and under each experimental condition at the same relative height. Under each exoskeleton condition, the subjects had to bring their torso in an upright position, with the upper arms vertical and an elbow flexion angle of 105°. Based on this posture, the table was adjusted to the height of the subject’s hand (for details, see Luger et al., 2019b). The reaching distance to the object was adjusted to the individual length of the horizontal and extended arm at a 180° transversal shoulder adduction angle (Figure 2). Between each experimental condition, subjects were given a 1-min rest period. Posturography using a force plate was recorded continuously.
Experiment II
After verifying the inclusion and exclusion criteria, subjects were tested on a single day. Extensive familiarization seemed to be unnecessary because there was no specific task to be learned. Prior to the experiment, a rope was attached to the back of the exoskeleton-vest at the level of the lumbar spine. The individual rope attachment to floor distance was measured by a folding ruler. The other end of the rope was fixed to a handheld dynamometer (Atorn ZD2, Atorn, Hahn + Kolb Werkzeuge GmbH, Lugwigsburg, Germany). Subjects were instructed to take a comfortable foot position, which resulted in the feet being positioned approximately hip-width apart (STAND) or shoulder-width apart (EXOHIGH.SEAT, EXONEW.HIGH.SEAT, EXOLOW.SEAT, and EXONEW.LOW.SEAT). When using the new prototype, subjects were instructed to maximally increase the distance between their feet and the exoskeleton’s supports to maximize the BOS. They were further asked to stiffen their body posture. In each condition, the same investigator manually pulled the dynamometer in posterior direction with the rope horizontally to the floor and slowly increased the force so that a fall was induced within 2 to 5 s. The investigator took care in applying the same slow force increment in each condition. The procedure was repeated three times per condition. Two assistants secured the subject when he would fall over. A picture of Experiment II is provided in Supplemental Appendix E.
Both experiments were performed on a plane and nonslippery underground.
Measurements and Data Analysis
Posturography
In Experiment I, a force plate (60 × 90 cm, Type 9287CA, Kistler, Toronto, Canada) was used to measure the COP with a sampling rate of 8 Hz. Data were amplified (DAQ-System, Type 5691A1, Kistler, Toronto, Canada) and processed. COP was differentiated in anteroposterior (COPAP) and mediolateral (COPML) direction and the means of the individual ranges were calculated (COPAP.RANGE and COPML.RANGE). The absolute and relative measures of static postural stability were calculated from the COPAP and COPML together with the BOS, which is defined by the surface directly surrounding the foot positions. When the exoskeleton is applied, the BOS represents the surface surrounding the foot and exoskeleton support positions. We, therefore, assessed the coordinates of the frontal part of shoe, the lateral part of the shoe at the level of distal end of the fifth metatarsal bone, and the dorsal part of the shoe at the heel, or if applicable at the exoskeleton support. The absolute static postural stability (SSABS) was determined as the absolute distance (mm) between the COP and the border of the BOS in the line from the centroid of the BOS to the COP (Supplemental Appendix A). The relative static postural stability (SSREL) was calculated using Eq. (1), where an SSREL of 100% means that the COP is exactly at the centroid of the BOS and an SSREL of 0% means that the COP is exactly on the BOS border.
| (1) |
with SOUT, the absolute distance (mm) between the COP and the BOS-border in the line from the centroid to the BOS-border; and SIN, the absolute distance (mm) between the COP and the centroid (Supplemental Appendix A). From the series of SSABS and SSREL, the minima were calculated as indicators of the risk of falling (SSABS.MIN and SSREL.MIN).
Torque measurements
In Experiment II, the peak force that induced falling was measured using a handheld dynamometer (100-Hz sampling frequency). The device is able to measure forces from 0 to 1000 N with a resolution of 0.1 N and a maximum error of 0.5 N. The mean force of the three repetitions in each experimental condition and the individual rope-to-floor distance were used to calculate the torque, further referred to as tilting moment (Eq. (2)).
| (2) |
with F [N], the peak force for each of the repetitions, and d [m], the height at which the rope was attached and the horizontal pulling force exerted.
Statistical Analysis
All dependent variables were normally distributed verified by skewness and kurtosis values (Kim, 2013), and the Shapiro–Wilk normality test.
Experiment I
Data of Experiment I were analyzed by a two-factor repeated measures analysis of variance (RM-ANOVA) with the within-subject factors exoskeleton condition (STAND, EXOHIGH.SEAT, EXOLOW.SEAT), object position further referred to as angle (120°, 150°, 180°), and the interaction term exoskeleton condition × angle. Dependent variables were: SSABS.MIN and SSREL.MIN. Significant main effects were further explored by post hoc Tukey’s Honestly Significant Difference pairwise comparisons. All statistical analyses were performed with JMP (JMP 14.2.0) at an α level of 0.05. In addition, effect sizes according to Cohen (1988) using the pooled standard deviation in the denominator were calculated (Eq. (3)) in case of significant findings. The following standard was used for effect size interpretation: <0.5 = small effect, between 0.5 and 0.8 = medium effect, >0.8 = large effect (Field, 2018).
| (3) |
In Experiment II, tilting moments were analyzed using descriptive statistics (median, quantiles, and individual subject data) and effect sizes due to its explorative character. Effect sizes were calculated according to Eq. (4) (Field, 2018) with the z-values obtained from Wilcoxon tests (applied to compare the exoskeleton conditions). The r values from 0.1 to 0.3 indicate a small effect, values between 0.3 and 0.5 are considered a medium effect and a large effect is associated with values over 0.5 (Field, 2018).
| (4) |
In addition, the relation between subjects’ body weight and tilting moments were analyzed using Pearson’s correlation coefficient (r) and linear regression.
Results
Dropouts and Extreme Values
One subject of Experiment I dropped out due to time constrictions. In three subjects, the measures of static postural stability could not be calculated due to missing data. Thus, the finally analyzed study population for Experiment I consisted of 45 healthy male subjects. None of the subjects from Experiment II dropped out (Table 1).
Table 1.
Anthropometric Data of the Study Population
| Gender | Age (Years) |
Body Height (cm) |
Body Weight (kg) |
BMI (kg/m2) |
Handedness | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| m | f | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Right | Left | |
| Experiment I | 45 | - | 24.8 | 2.9 | 182.6 | 5.5 | 78.1 | 8.7 | 23.3 | 2.1 | 39 | 6 |
| Experiment II | 6 | 2 | 33.6 | 7.9 | 177.0 | 6.1 | 77.4 | 14.7 | 24.7 | 4.5 | 6 | 2 |
Note. BMI = body mass index.
Experiment I
Center of pressure ranges in anteroposterior and mediolateral direction
The mean ranges of COPAP were lower than for COPML, and both were influenced by exoskeleton condition (p < .0001) as shown in Table 2 and Figure 3 with medium and large effect sizes between STAND and the two exoskeleton conditions. For the COPAP direction, the position of the object (angle) had an impact on COPAP.RANGE (p < .0001) with decreasing values when transversal shoulder adduction angles increased (120° = 84.97 mm, 150° = 75.73 mm, 180° = 72.02 mm), while COPML.RANGE was not influenced (p = .69). The interaction of “exoskeleton condition × angle” was no statistically significant factor of COP ranges. For details, see Supplemental Appendices B–D.
Table 2.
Statistical Outcomes of Experiment I From the Repeated Measures Analysis of Variance
| Statistical Outcomes RM-ANOVA |
Exoskeleton Condition | Angle | Exoskeleton Condition × Angle | Subjects | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| df | F | p | df | F | p | df | F | p | N | |
| COPAP.RANGE (mm) | 2 | 73.90 | <.0001 | 2 | 22.43 | <.0001 | 4 | 2.10 | .08 | 45 |
| COPML.RANGE (mm) | 2 | 1569.72 | <.0001 | 2 | 0.37 | .69 | 4 | 1.39 | .24 | 45 |
| SSREL.MIN (%) | 2 | 252.72 | <.0001 | 2 | 4.29 | .01 | 4 | 3.85 | .005 | 42 |
| SSABS.MIN (mm) | 2 | 124.04 | <.0001 | 2 | 5.06 | .007 | 4 | 5.35 | .0003 | 42 |
Note. Angle reflects different object positions associated with three transversal shoulder adduction angles. Bold indicates statistically significant results. AP = anteroposterior; COP = center of pressure; df = degrees of freedom; ML = mediolateral; N = number of subjects; RM-ANOVA = repeated measures analysis of variance.
Figure 3.
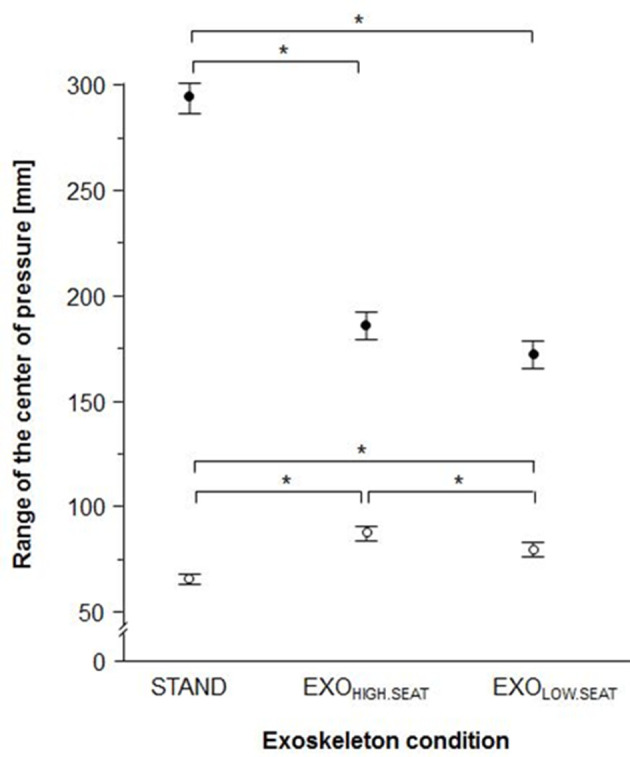
Mean ranges of the center of pressure including 95th confidence intervals in mediolateral (black filled circles) and anteroposterior (open circles) direction. STAND = standing without exoskeleton; EXOHIGH.SEAT = sitting on the exoskeleton with a knee angle of 120°; EXOLOW.SEAT = sitting on the exoskeleton with a knee angle of 90°. * indicates statistically significant differences between exoskeleton conditions.
Relative and Absolute Static Postural Stability
Exoskeleton condition and angles (position of the object) significantly influenced relative and absolute static postural stability (all p values < .01). The SSREL.MIN was highest in EXOLOW.SEAT while the SSABS.MIN was highest in STAND (SSREL.MIN: STAND = 16.71%, EXOHIGH.SEAT = 29.79%, EXOLOW.SEAT = 32.91%; SSABS.MIN: STAND = 29.31 mm, EXOHIGH-SEAT = 17.04 mm, EXOLOW.SEAT = 16.77 mm). With increasing transversal shoulder adduction angles, there was a slight decrease of SSREL.MIN (120° = 27.49%, 150° = 26.65%, 180° = 25.27%) and SSABS.MIN (120° = 22.55 mm, 150° = 20.92 mm, 180° = 19.66 mm) with statistically significant differences between 120° and 150° (p = .0289) and 120° and 180° (p < .001) for SSABS.MIN as well as between 120° and 180° for SSREL.MIN (p = .0004). Furthermore, a statistically significant interaction between exoskeleton condition and angle occurred for SSABS.MIN and SSREL.MIN (p = .0003 and p = .005, respectively). Post hoc analyses revealed that angle influenced SSABS.MIN and SSREL.MIN mainly in the standing condition without the exoskeleton. SSABS.MIN values significantly decreased from 34.0 to 28.7 and 25.2 mm when angles increased from 120° to 150° and 180°; SSREL.MIN values significantly decreased from 19.92% to 14.12% when the angles used to change the object position increased from 120° to 180° (Figure 4 and Table 2). No statistically significant changes in SSABS.MIN or SSREL.MIN were found for the EXOHIGH.SEAT or EXOLOW.SEAT conditions when the position of the object was varied. For details, see Supplemental Appendices B–D.
Figure 4.

(a) Relative and (b) absolute static postural stability with respect to exoskeleton condition and shoulder anteversion angle STAND, standing without exoskeleton. EXOHIGH.SEAT = sitting on the exoskeleton with a knee angle of 120°; EXOLOW.SEAT = sitting on the exoskeleton with a knee angle of 90°. Data are provided as means and 95th confidence intervals. † indicates statistically significant difference of EXOLOW.SEAT and EXOHIGH.SEAT compared to STAND. Angle reflects different object positions associated with three transversal shoulder adduction angles. * indicates statistically significant differences between angles within an exoskeleton condition.
Experiment II
Tilting moments ranged from 14.1 to 91.6 nm with medians of 54.3 nm for STAND, 35.3 Nm for EXOHIGH.SEAT, and 28.9 Nm for EXOLOW.SEAT. Median tilting moments for the prototype with the new foot feature (possibility to increase the BOS area) were about 45%–62% higher than for the common exoskeleton (EXONEW.HIGH.SEAT = 51.1 nm and EXONEW.LOW.SEAT = 46.9 nm) and almost equal to STAND. Effect sizes ranged from 0.21 to 0.63 (Table 3). With respect to individual tilting moments, six out of eight subjects showed a similar pattern with the lowest moments for the common exoskeleton conditions (Figure 5a). Tilting moments were positively related to body weight values with higher moments for heavier subjects (Figure 5b and Table 4).
Table 3.
Effect Sizes of the Tilting Moments
| Comparison | Z Value | Effect Size, R | ||
|---|---|---|---|---|
| STAND | vs. | EXONEW.HIGH.SEAT | 0.84 | 0.21 (small) |
| STAND | vs. | EXONEW.LOW.SEAT | 1.12 | 0.28 (small) |
| STAND | vs. | EXOHIGH.SEAT | 1.82 | 0.46 (medium) |
| STAND | vs. | EXOLOW.SEAT | 2.24 | 0.56 (large) |
| EXONEW.HIGH.SEAT | vs. | EXOHIGH.SEAT | 2.52 | 0.63 (large) |
| EXONEW.LOW.SEAT | vs. | EXOLOW.SEAT | 1.68 | 0.42 (medium) |
Note. EXOHIGH.SEAT = sitting on the exoskeleton with a knee angle of 120°; EXONEW.HIGH.SEAT = sitting onthe exoskeleton with a knee angle of 120° and increased base of support area by the new foot feature; EXONEW.LOW.SEAT = sitting on the exoskeleton with a knee angle of 90° and increased base of support area by the new footfeature; STAND = standing without exoskeleton. Small effect 0.1–0.3, medium effect 0.3–0.5, large effect >0.5.
Figure 5.

(a) Tilting moments with respect to exoskeleton condition. (b) Linear regression of tilting moments with respect to body weight. STAND = standing without exoskeleton; EXOHIGH.SEAT = sitting on the exoskeleton with a knee angle of 120°; EXONEW.HIGH.SEAT = sitting on the exoskeleton with a knee angle of 120° and increased base of support area by the new foot feature; EXOLOW.SEAT = sitting on the exoskeleton with a knee angle of 90°; EXONEW.LOW.SEAT, sitting on the exoskeleton with a knee angle of 90° and increased base of support area by the new foot feature.
Table 4.
Linear Regression Equations and Correlation Coefficients of the Relationship Between Body Weight and Tilting Moment
| Posture | Foot Module | Linear Regression Equation | Correlation Coefficient (r) | R² | p Value |
|---|---|---|---|---|---|
| STAND | - | TM [Nm] = −57.47662 + 1.4713223·BW[kg] | 0.83 | 0.68 | .012 |
| EXOHIGH.SEAT | Old | TM[Nm] = −26.61612 + 0.8175775·BW[kg] | 0.71 | 0.51 | .048 |
| New | TM[Nm] = −40.21389 + 1.1908268·BW[kg] | 0.87 | 0.76 | .005 | |
| EXOLOW.SEAT | Old | TM[Nm] = −27.66195 + 0.807459·BW[kg] | 0.64 | 0.40 | .090 |
| New | TM[Nm] = −19.88268 + 0.8747171·BW[kg] | 0.85 | 0.72 | .009 |
Note. Bold indicates statistically significant results. EXOHIGH.SEAT = sitting on the exoskeleton with a knee angle of 120°; EXOLOW.SEAT = sitting on the exoskeleton with a knee angle of 90°; STAND = standing without exoskeleton; TM = tilting moment.
Discussion
The Chairless Chair is designed to reduce physical loads associated with prolonged standing or awkward postures. In this context, it has been previously shown that about 60% of the body mass can be transferred to the ground when sitting on the exoskeleton (Luger et al., 2019b). However, occupational safety aspects related to this exoskeleton have received little attention, so far. Therefore, the present study investigated static postural stability as an estimate for the risk of falling with respect to two common occupational scenarios where this exoskeleton may be utilized: reaching for a tool at the end of the lateral reaching area (Experiment I), and a potential collision with for example, collaborating workers or robots (Experiment II). We compared using the Chairless Chair at two different sitting heights with standing without exoskeleton, since the substitution of prolonged standing is a major application of the Chairless Chair.
Risk of Falling When Reaching for an Object at the Lateral End of the Reaching Area
The absolute and relative static postural stability have been used to assess postural stability (Holbein & Redfern, 1997) and to estimate the risk of falling in Experiment I. Both measures are based on the static equilibrium principle, which characterizes a stable posture when the body’s COG gravity is within the BOS area (Hayes, 1982). With respect to this principle, we decided to use the minima of SSABS and SSREL as the most suitable approach. SSABS decreased and SSREL increased while sitting on the exoskeleton compared to STAND. This incongruence is probably related to the increase in the BOS area (increase of SSREL) and a general COP shift in the posterior direction (decrease in SSABS) when sitting on the exoskeleton. The SSABS may be more important, since it is the true reflection of the safety margin that actually prevents someone from falling. With a reduced mean SSABS.MIN of about 12 mm (~44% reduction compared to standing without exoskeleton), the exoskeleton clearly lowers that safety margin.
With respect to previously published results from a simulated industrial task, no differences between standing without exoskeleton and sitting on the exoskeleton were detected in this postural stability measure (Luger et al., 2019b). The requirements of postural control strategies related to such an industrial task may be low, since the work was performed at a comfortable working height with low forces and hand-arm movements close to the body. However, when reaching for an object at the lateral end of the reaching area, requirements of postural control strategies may increase. Thus, impairments in the possibility for compensatory postural adjustments by the exoskelton may result. Compensatory postural adjustments can be achieved by rotating the body as a rigid segment around the ankle joint or by flexing the hip joints and plantar flexing the ankle joints (Afschrift et al., 2016), called the ankle and hip strategy, respectively (Nashner & McCollum, 1985). When sitting on the exoskeleton, worker’s lower limbs are attached to the exoskeleton supports, which clearly impairs ankle and hip joint movements and new strategies for restoring equilibrium may be used leading to lower SSABS.
Changing the position of the object that had to be grabbed by the subject (i.e., the three different angles in the transversal plane) did influence SSREL or SSABS. In the experimental conditition standing without the exoskeleton SSABS and SSREL decreased when the object’s position was characterized by a greater angle in the transversal plane. This position may induce disturbing torso and/or head rotations necessary when the angle increases. When sitting on the exoskeleton, the angle had no influence on SSREL or SSABS indicating that although sitting on the exoskeleton is accompanied by reduced SSABS values, the exoskeleton provides at least some stability. Therefore, after sufficient familiarization with the exoskeleton and the task, reaching for a tool (about 3 kg) with fluent and self-selected movement speed at the end of the lateral reaching area may be no exclusion criteria for the application of this exoskeleton. However, it should be noted that a further increase in postural control demands by any factor may significantly increase the risk of falling since the safety margin is lower when using the exoskeleton. This especially holds true for employees suffering from, for example, medical conditions prone to impaired postural control. A priori ergonomic evaluation of the workplace is highly recommended in order to avoid unforeseen events, abrupt changes in motion, or extreme postures leading to destabilization.
No other study assessing postural stability in a lower limb exoskeleton for occupational tasks could be found. However, impaired static balance has been reported when wearing an upper limb exoskeleton probably due to an increased effort to control the additional weight of the exoskeleton. But no evident change in trip- and slip-related fall risks during level walking occurred (Kim et al., 2018). In a different scientific context, an exoskeletons has been evaluated in terms of its potential to prevent falls in older subjects with a mild risks of falls (Verrusio et al., 2017). With respect to these few research activities, the influence of exoskeletons on postural control should be the target of future research, especially as these assistive devices seem to become more common in our daily life.
Risk of Falling Following an External Perturbation
In Experiment II, the external perturbations when subjects sat on the exoskeleton led to a higher risk of falling than in standing without exoskeleton. This interpretation can be derived from the lower tilting moments measured during the perturbation when sitting on the exoskeleton. When subjects increased their BOS area with the foot module of the new prototype, tilting moments increased to similar values like for STAND. However, as already mentioned above, when standing without exoskeleton, subjects are able to regain equilibrium by changing the foot position. When sitting on the exoskeleton either with the old or new foot module, taking a supporting step for fall prevention is restricted especially for the dorsal direction due to the supports that do not allow backward movements of the feet. Of course, tilting moments may be higher when the external force direction differs and workers may also be able to change their foot position in the forward direction while using the exoskeleton. However, in terms of a worst case consideration, since the force direction of an unforeseen external perturbation cannot be predicted, it must be recommended that every source that may induce a tilting moment on a worker using the exoskeleton should be avoided a priori.
Tilting moments decreased with decreasing body weight (Figure 5b), meaning that even lower tilting moments (<30 nm) can induce falling in lighter workers. For instance, when sitting on the exoskeleton at the lower sitting height, a tilting moment of about 21 nm was able to induce falling in the lightest subject (58 kg), while in the heaviest subject (105 kg), the necessary tilting moment was about 41 nm. Additionally, the inertia of a heavier subject is larger than that of lighter subjects. In case of dynamic forces—for example, a strike caused by a collaborative robot—the disadvantage for the subject with the low body weight would be potentiated. When these two subjects increased their BOS area by the foot module of the new prototype, tilting moments increased to about 30 (light subject) and about 70 nm (heavy subject). This new feature can lower the risk of falling and therefore has already become a standard in the currently available Chairless Chair version (2.0). However, an educational introduction and training how to use this exoskeleton is recommended to ensure that workers get familiarized with the device and know about the importance to increase their BOS (i.e., sliding the feet as far forward as possible in the new foot module) to maximize their own safety.
Another aspect indicating that tilting moments associated with falling may be higher in real-life situations than in this laboratory study is associated with the type of perturbation. The perturbation was predictable, because the subjects knew about the type and time pattern of the perturbation. Such predictable perturbations are associated with lower COP displacements due to a better arrangement of the body position prior to the impact resulting in a lower need of compensatory adjustments (Santos et al., 2010).
Limitations
In this study, only healthy and mainly young, male subjects were investigated, who had no medical history of impairments in postural control or motor function. Due to longer postural muscle response latencies and declines in the proprioceptive and visual system of older people (Ruffieux et al., 2015; Woollacott et al., 1988), it can be assumed that the risk of falling when using the Chairless Chair may increase with increasing age. Furthermore, only two occupational scenarios were investigated by the present study. Other relevant occupational scenarios such as overhead reaching, working on uneven ground, or applying high action forces while sitting on the Chairless Chair were not considered.
Both experiments have some methodological limitations that could have induced inter-individual and also between-trial differences affecting the outcomes. In the first experiment, we did not exactly control the movement speed or define how to move the arms and the torso during the reaching task. In the second experiment, subjects were manually pulled backwards until they lost their balance and we used a fixed order of experimental conditions. Although the rater who manually pulled the subjects in Experiment II used a slow increase in force so that the tilting moment occurred between 2 and 5 s after the rater started pulling, significant differences in pulling may have occurred. In addition, during a real collision with a coworker or collaborating robot, the induced torque on the body may be different in size and speed and subjects may use reactive balance strategies, which were not allowed during Experiment II.
In addition, the validity and reliability of single tests or measures to predict the risk of falls can be questioned, as indicated by a review article about on how to determine the risk of falls (Lusardi et al., 2017). In this respect, the presented data provide first insights in the influence of lower limb exoskeletons on postural control, which needs further attention in the future.
Conclusion
In a previous study, we reported that the risk of falling when using the Chairless Chair exoskeleton may not increase during a simulated repetitive industrial task (Luger et al., 2019b). The results of the current study complement this conclusion with the following three aspects: (a) reaching for a working tool of up to 3 kg at the lateral end of the reaching area is not associated with worrying impairments in postural control when using the Chairless Chair by healthy, young, male subjects; (b) the tilting moment necessary to induce falling when sitting on the Chairless Chair is fairly low, meaning that the Chairless Chair should not be used in situations where a collision may occur; (c) the new foot module that allows an increased BOS area, has the potential to increase postural stability, assuming this function is applied by the user.
Key Points
Impairments in postural control while using the Chairless Chair exoskeleton seem to be low when reaching laterally for a work tool (≤3 kg), given that there are no additional environmental influences like an uneven or slippery floor.
The risk of falling while using the Chairless Chair exoskeleton may be increased in situations when a collision with a co-worker or collaborating robot is likely.
In lighter workers, the risk of falling while using the Chairless Chair exoskeleton seems to be higher than that in heavier workers.
Supplemental Material
Supplemental material, Figure S1, for Postural Control When Using an Industrial Lower Limb Exoskeleton: Impact of Reaching for a Working Tool and External Perturbation by Benjamin Steinhilber, Robert Seibt, Monika A. Rieger and Tessy Luger in Human Factors: The Journal of Human Factors and Ergonomics Society
Acknowledgments
The authors would like to thank students Timothy J. Cobb, Theresa J. Kreidler, and Lucas Bühler for their help during the measurement preparations and data collection. We would also like to thank AUDI AG for providing us two exoskeletons, and for their input in developing the simulated tasks to adequately simulate the field situation. This work was funded by the AUDI AG and the institute´s own resources. AUDI AG was not involved in data assessment, analysis or interpretation at any time. Generally, the work of the Institute of Occupational and Social Medicine and Health Services Research is financially supported by an unrestricted grant of the employers´ association of the metal and electrical industry Baden-Württemberg (Südwestmetall). Timothy J. Cobb received a personal fellowship by Südwestmetall for conducting his medical thesis.
Author Biographies
Benjamin Steinhilber is head of the research unit “Work-related Exposures — Work Design” at the Institute of Occupational and Social Medicine and Health Services Research, University Hospital Tübingen. He received his PhD in sports science in 2013 from the Technical University of Chemnitz, Germany.
Robert Seibt is a scientific coworker at the University Hospital of Tübingen, Institute of Occupational Medicine, Social Medicine and Health Services Research, and the chief of the research and development department of THUMEDI GmbH & Co. KG. He received his diploma in biomedical engineering in 1993 from the Technical University of Chemnitz, Germany.
Monika A. Rieger is a professor of occupational and social medicine at the University of Tübingen and head of the Institute of Occupational and Social Medicine and Health Services Research, University Hospital Tübingen, Germany. She received her MD in medicine in 1995 at the University of Freiburg, Germany, and received her PhD in work physiology and occupational medicine in 2001 at the University of Wuppertal, Germany.
Tessy Luger is a scientific co-worker at the Institute of Occupational and Social Medicine and Health Services Research, University Hospital Tübingen, Germany. She received her PhD in human movement sciences in 2016 at the VU University Amsterdam, the Netherlands.
ORCID iDs
Benjamin Steinhilber https://orcid.org/0000-0001-9622-6511
Tessy Luger https://orcid.org/0000-0001-5718-251X
References
- Afschrift M., Jonkers I., De Schutter J., De Groote F. (2016). Mechanical effort predicts the selection of ankle over hip strategies in nonstepping postural responses. Journal of Neurophysiology, 116, 1937–1945. 10.1152/jn.00127.2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bevan S. (2015). Economic impact of musculoskeletal disorders (MSDs) on work in Europe. Best Practice & Research Clinical Rheumatology, 29, 356–373. 10.1016/j.berh.2015.08.002 [DOI] [PubMed] [Google Scholar]
- Błaszczyk J. W., Cieślinska-Swider J., Plewa M., Zahorska-Markiewicz B., Markiewicz A. (2009). Effects of excessive body weight on postural control. Journal of Biomechanics, 42, 1295–1300. 10.1016/j.jbiomech.2009.03.006 [DOI] [PubMed] [Google Scholar]
- Bosch T., van Eck J., Knitel K., de Looze M. (2016). The effects of a passive exoskeleton on muscle activity, discomfort and endurance time in forward bending work. Applied Ergonomics, 54, 212–217. 10.1016/j.apergo.2015.12.003 [DOI] [PubMed] [Google Scholar]
- Canadian Centre for Occupational Health & Safety . (2020). Retrieved August 20, 2003, from. https://www.ccohs.ca/oshanswers/ergonomics/sitting/sitting_basic.html;
- Cohen J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum Association. [Google Scholar]
- da Costa B. R., Vieira E. R. (2010). Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. American Journal of Industrial Medicine, 53, 285–323. 10.1002/ajim.20750 [DOI] [PubMed] [Google Scholar]
- Dagalakis N. G., Yoo J. M., Oeste T. (2016). Human-Robot collaboration dynamic impact testing and calibration instrument for disposable robot safety artifacts. Industrial Robot: An International Journal, 43, 328–337. 10.1108/IR-06-2015-0125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Looze M. P., Bosch T., Krause F., Stadler K. S., O’Sullivan L. W. (2016). Exoskeletons for industrial application and their potential effects on physical work load. Ergonomics, 59, 671–681. 10.1080/00140139.2015.1081988 [DOI] [PubMed] [Google Scholar]
- de Santiago H. A. R., Reis J. G., Gomes M. M., da Silva Herrero C. F. P., Defino H. L. A., de Abreu D. C. C. (2013). The influence of vision and support base on balance during quiet standing in patients with adolescent idiopathic scoliosis before and after posterior spinal fusion. The Spine Journal, 13, 1470–1476. 10.1016/j.spinee.2013.03.027 [DOI] [PubMed] [Google Scholar]
- Field A. (2018). Discovering Statistic using IBM SPSS Statisctics (5th edn.). SAGE. [Google Scholar]
- Hayes K. C. (1982). Biomechanics of postural control. Exercise and Sport Sciences Reviews, 10, 363–391. 10.1249/00003677-198201000-00011 [DOI] [PubMed] [Google Scholar]
- He Y., Eguren D., Luu T. P., Contreras-Vidal J. L. (2017). Risk management and regulations for lower limb medical exoskeletons: A review. Medical Devices, 10, 89–107. 10.2147/MDER.S107134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holbein M. A., Redfern M. S. (1997). Functional stability limits while holding loads in various positions. International Journal of Industrial Ergonomics, 19, 387–395. 10.1016/S0169-8141(96)00023-6 [DOI] [PubMed] [Google Scholar]
- Huysamen K., de Looze M., Bosch T., Ortiz J., Toxiri S., O’Sullivan L. W. (2018). Assessment of an active industrial exoskeleton to aid dynamic lifting and lowering manual handling tasks. Applied Ergonomics, 68, 125–131. 10.1016/j.apergo.2017.11.004 [DOI] [PubMed] [Google Scholar]
- Kim H.-Y. (2013). Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restorative Dentistry & Endodontics, 38, 52–54. 10.5395/rde.2013.38.1.52 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim S., Nussbaum M. A., Mokhlespour Esfahani M. I., Alemi M. M., Jia B., Rashedi E. (2018). Assessing the influence of a passive, upper extremity exoskeletal vest for tasks requiring arm elevation: Part II - "Unexpected" effects on shoulder motion, balance, and spine loading. Applied Ergonomics, 70, 323–330. [DOI] [PubMed] [Google Scholar]
- Leso V., Fontana L., Iavicoli I. (2018). The occupational health and safety dimension of industry 4.0. La Medicina del lavoro, 110, 327–338. 10.23749/mdl.v110i5.7282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luger T., Cobb T. J., Seibt R., Rieger M. A., Steinhilber B. (2019. a). Subjective evaluation of a passive lower-limb industrial exoskeleton used during simulated assembly. IISE Transactions on Occupational Ergonomics and Human Factors, 7, 175–184. 10.1080/24725838.2018.1560376 [DOI] [Google Scholar]
- Luger T., Seibt R., Cobb T. J., Rieger M. A., Steinhilber B. (2019. b). Influence of a passive lower-limb exoskeleton during simulated industrial work tasks on physical load, upper body posture, postural control and discomfort. Applied Ergonomics, 80, 152–160. 10.1016/j.apergo.2019.05.018 [DOI] [PubMed] [Google Scholar]
- Lusardi M. M., Fritz S., Middleton A., Allison L., Wingood M., Phillips E., Criss M., Verma S., Osborne J., Chui K. K. (2017). Determining risk of falls in community Dwelling older adults: A systematic review and meta-analysis using Posttest probability. Journal of Geriatric Physical Therapy, 40, 1–36. 10.1519/JPT.0000000000000099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melia M., Geissler B., König J., Ottersbach H. J., Umbreit M., Letzel S., Muttray A. (2019). Pressure pain thresholds: Subject factors and the meaning of peak pressures. European Journal of Pain, 23, 167–182. 10.1002/ejp.1298 [DOI] [PubMed] [Google Scholar]
- Nashner L. M., McCollum G. (1985). The organization of human postural movements: A formal basis and experimental synthesis. Behavioral and Brain Sciences, 8, 135–150. 10.1017/S0140525X00020008 [DOI] [Google Scholar]
- Park M. Y., Choi J. S., Kim K. S., Rhim S., Park H. J., Shin M. K. (2019). Identification of a closed cutaneous injury after mechanical trauma caused by collision. Skin Research and Technology, 25, 440–446. 10.1111/srt.12670 [DOI] [PubMed] [Google Scholar]
- Punnett L., Wegman D. H. (2004). Work-related musculoskeletal disorders: The epidemiologic evidence and the debate. Journal of Electromyography and Kinesiology, 14, 13–23. 10.1016/j.jelekin.2003.09.015 [DOI] [PubMed] [Google Scholar]
- Rashedi E., Kim S., Nussbaum M. A., Agnew M. J. (2014). Ergonomic evaluation of a wearable assistive device for overhead work. Ergonomics, 57, 1864–1874. 10.1080/00140139.2014.952682 [DOI] [PubMed] [Google Scholar]
- Ruffieux J., Keller M., Lauber B., Taube W. (2015). Changes in standing and walking performance under Dual-task conditions across the lifespan. Sports Medicine, 45, 1739–1758. 10.1007/s40279-015-0369-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Santos M. J., Kanekar N., Aruin A. S. (2010). The role of anticipatory postural adjustments in compensatory control of posture: 2. biomechanical analysis. Journal of Electromyography and Kinesiology, 20, 398–405. 10.1016/j.jelekin.2010.01.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sultan-Taïeb H., Parent-Lamarche A., Gaillard A., Stock S., Nicolakakis N., Hong Q. N., Vezina M., Coulibaly Y., Vézina N., Berthelette D. (2017). Economic evaluations of ergonomic interventions preventing work-related musculoskeletal disorders: A systematic review of organizational-level interventions. BMC Public Health, 17, 935. 10.1186/s12889-017-4935-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Theurel J., Desbrosses K., Roux T., Savescu A. (2018). Physiological consequences of using an upper limb exoskeleton during manual handling tasks. Applied Ergonomics, 67, 211–217. 10.1016/j.apergo.2017.10.008 [DOI] [PubMed] [Google Scholar]
- Verrusio W., Gianturco V., Cacciafesta M., Marigliano V., Troisi G., Ripani M. (2017). Fall prevention in the young old using an exoskeleton human body posturizer: A randomized controlled trial. Aging Clinical and Experimental Research, 29, 207–214. 10.1007/s40520-016-0540-7 [DOI] [PubMed] [Google Scholar]
- Weston E. B., Alizadeh M., Knapik G. G., Wang X., Marras W. S. (2018). Biomechanical evaluation of exoskeleton use on loading of the lumbar spine. Applied Ergonomics, 68, 101–108. 10.1016/j.apergo.2017.11.006 [DOI] [PubMed] [Google Scholar]
- Williams E. J. (1949). Experimental designs balanced for the estimation of residual effects of treatments. Australian Journal of Chemistry, 2, 149–168. 10.1071/CH9490149 [DOI] [Google Scholar]
- Woollacott M., Inglin B., Manchester D. (1988). Response preparation and posture control. neuromuscular changes in the older adult. Annals of the New York Academy of Sciences, 515, 42–53. 10.1111/j.1749-6632.1988.tb32964.x [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, Figure S1, for Postural Control When Using an Industrial Lower Limb Exoskeleton: Impact of Reaching for a Working Tool and External Perturbation by Benjamin Steinhilber, Robert Seibt, Monika A. Rieger and Tessy Luger in Human Factors: The Journal of Human Factors and Ergonomics Society