


Marco Innocenti
Today, robotics has become the gold standard in the operating room for several procedures and surgical specialties. However, microsurgery has not been touched to date other than the limited application of the da Vinci Surgical System, not focused on microanastomosis. Differently from da Vinci, which aims to facilitate minimally invasive procedures by providing improved vision and dexterity to the conventional laparoscopic approach, new microsurgical robots are now designed and being introduced to provide improved precision for anastomosis. Thanks to elimination of tremor and high scaling potential, robotics in microsurgery probably will acquire increasing value as the current trend in submillimetric anastomosis will be confirmed in the clinical practice.
Currently, two dedicated robots for microsurgery have been developed: MUSA by Microsure and Symani by MMI ( Fig. 1 ). These platforms aim to increase surgeon's precision allowing for fine manipulation of very small anatomy in open surgery, rather than decrease invasiveness.
Fig. 1.
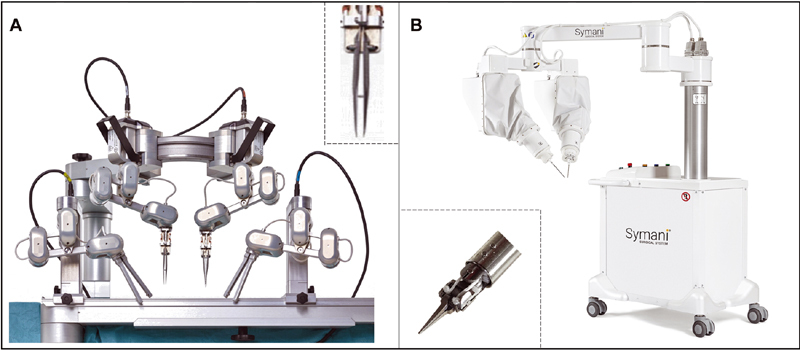
( A, B ) Robotic platforms currently available and specifically designed for microsurgery.
Although in its infancy, robotic microsurgery already has a small body of primary literature. A pilot study in lymphovenous anastomosis (LVA) using the MUSA system 1 has been recently published and a paper reporting the first human case of robotic-assisted free flap with Symani is currently in press in Plastic and Reconstructive Surgery . A comprehensive review of the potential of robotic microsurgery has recently been published in the book Robotics in Plastic and Reconstructive Surgery by Springer, 2 indicating that this subspecialty might be “here to stay.”
The Symani Surgical System saw its first clinical use in Careggi University Hospital in Florence, Italy, where both the first free flaps and LVA procedures were done. 3 This year, two more Symani Surgical Systems have been installed in Europe and are in use in the fields of plastic surgery and maxillofacial surgery at the University of Zurich and Salzburg, respectively.
Our personal experience in Florence is limited to 15 cases. These include bone flaps, soft tissue flaps including perforator-to-perforator, and three cases of LVA for lymphedema, with encouraging results. Particularly in supermicrosurgery the absence of tremor significantly increases the precision in the passage of the needle and the overall accuracy of the procedure with minimal effort by the surgeon. However, like other innovative procedures, robotic microsurgery needs to be further refined and validated on a larger scale. A multicenter postmarket clinical study has been initiated at Careggi University Hospital to provide a tool to analyze a homogeneous series of data and identify the areas of highest clinical benefit.
Most of the progress in reconstructive microsurgery over the past 30 years is substantially sustained by a tremendous improvement in the knowledge of vascular anatomy, at a size neglected by conventional anatomy. The most innovative procedures today, such as perforator flaps, propeller flaps, ultrathin flaps, lymph node transfers, and LVA, are enabled by this new vascular awareness that has come to fruition. 1 2 3 Most of these new procedures push the surgeon beyond the average manual dexterity to enter the world of supermicrosurgery.
In analogy with the operative microscope which allowed the healthy and trained eyes of the surgeons to reach magnification to an extent not replicable by the human eye, the microsurgical robot will make feasible for the average microsurgeon to execute microsutures beyond natural dexterity. Although it is unlikely that a robotic arm will replace the human hand in the near future, robotic microsurgery in my opinion is the most powerful technological innovation in reconstructive microsurgery in the past 20 years and is a promising field of application for the next generation plastic surgeons.
Footnotes
Conflict of Interest M.I. is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
References
- 1.MicroSurgical Robot Research Group . van Mulken T JM, Schols R M, Scharmga A MJ. First-in-human robotic supermicrosurgery using a dedicated microsurgical robot for treating breast cancer-related lymphedema: a randomized pilot trial. Nat Commun. 2020;11(01):757. doi: 10.1038/s41467-019-14188-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Selber J C. Switzerland: Springer International Publishing; 2021. Robotics in Plastic and Reconstructive Surgery. [Google Scholar]
- 3.Innocenti M, Malzone G, Menichini G.First-in-human free-flap tissue reconstruction using a dedicated microsurgical robotic platformPlast Reconstr Surg, In press [DOI] [PubMed]
Additional References
- 1.Hallock G G. Innovations: a dawning of a new age. Arch Plast Surg. 2021;48(02):147–148. doi: 10.5999/aps.2021.00255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hong J P. Innovation in plastic surgery-why and how? Arch Plast Surg. 2021;48(05):471–472. doi: 10.5999/aps.2021.01669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Neligan P C. The future of plastic surgery. Arch Plast Surg. 2022;49(01):1–2. doi: 10.5999/aps.2021.02278. [DOI] [PMC free article] [PubMed] [Google Scholar]