

Abstract
To prevent the coronavirus disease 2019 (COVID-19) pandemic and aid restoration to prepandemic normality, global mass vaccination is urgently needed. Inducing herd immunity through mass vaccination has proven to be a highly effective strategy for preventing the spread of many infectious diseases, which protects the most vulnerable population groups that are unable to develop immunity, such as people with immunodeficiencies or weakened immune systems due to underlying medical or debilitating conditions. In achieving global outreach, the maintenance of the vaccine potency, transportation, and needle waste generation become major issues. Moreover, needle phobia and vaccine hesitancy act as hurdles to successful mass vaccination. The use of dissolvable microneedles for COVID-19 vaccination could act as a major paradigm shift in attaining the desired goal to vaccinate billions in the shortest time possible. In addressing these points, we discuss the potential of the use of dissolvable microneedles for COVID-19 vaccination based on the current literature.
Keywords: COVID-19 vaccine delivery, dissolvable microneedles, immunogenicity, mass vaccination
1. Introduction
One of the greatest public health threats faced by humanity in this century is the coronavirus disease 2019 (COVID-19) pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1,2,3]. While the entire world is yearning for relief from this pandemic, a ray of hope was foreseen via the approval of several COVID-19 vaccines by the Food and Drug Administration (FDA) [4,5] and other national agencies (e.g., the UK’s the Medicines and Healthcare products Regulatory Agency). However, the effectiveness of the vaccination programs and the global outreach of the vaccines for the mass population worldwide are major areas of concern [2,4,5] given the need to vaccinate billions of people in the shortest period of time. This requires the immense efficiency of the vaccination programs [6,7,8]. The vaccines require special storage conditions to remain viable during transportation and distribution [9,10,11]. The delivery of the vaccines can only be done via trained professionals using conventional vaccine delivery using hypodermic syringes [12,13]. However, the scarcity of trained professionals and the absence of adequate dosages are two of the key barriers to attaining mass vaccination [14,15]. Moreover, the vaccination programs would mean mass gatherings at specific places, which is risky, since they have the potential to facilitate the quick spread of the disease [16,17,18].
In addition, mass vaccination using hypodermic syringes will produce a massive amount of biowaste, which would create another area of concern for effective waste management [13,19,20]. In this scenario, we have to think about alternatives which would make the vaccination program much more efficient and accessible [21,22,23]. The use of novel vaccine delivery could be a potential solution to this critical challenge [24,25,26]. The use of microneedle vaccine delivery mechanisms would allow the vaccines to be delivered in a painless manner, ensuring the controlled release of drugs via a dissolvable microneedle [27,28,29,30].
The use of dissolvable microneedle patches would improve the dosing accuracy, ensuring the precise delivery of the vaccines [31,32,33].
The use of biodegradable microneedles for transdermal immunization is a fast-developing topic of study and application [34,35,36]. One of the main reasons why most individuals refuse to be vaccinated is their fear of painful needles [37,38,39]. As a result, creating a pain-free technique of immunization utilizing microneedles has been a major research challenge [40,41,42].
Microneedles contain arrays of micron-sized needles that deliver molecules across the skin without causing discomfort [43,44,45]. Microneedles have a number of benefits over traditional immunization methods (summarized in Table 1), such as intramuscular and subcutaneous injections, aside from the fact that they are painless [46,47,48]. Microneedle vaccinations elicit a strong immune response because the needles, which range in length from 25 to 1000 µm, may effectively transport the vaccine to the epidermis and dermis, which contain a large number of Langerhans and dendritic cells [36,49,50]. The microneedle array resembles band-aid patches and provides the benefits of cold-chain storage avoidance and self-administration flexibility [49,50,51]. Microneedles have the benefit of slowing the release of vaccination antigens [52,53,54]. Vaccine components in microneedles might be in solution or suspension, coated in nano or microparticles, or based on nucleic acid [55,56]. Because of the combined benefits of particulate vaccinations and pain-free vaccination, the use of microneedles to administer particle-based immunizations is growing rapidly [57,58,59]. The future of microneedle-based vaccines is bright, but certain constraints, such as dosage insufficiency, stability, and sterility, must be addressed before microneedles may be successfully used for vaccine delivery [60,61,62]. This article summarizes the current developments in COVID-19 medicaments and vaccine delivery in accordance with the field of microneedle-based immunization [61,63]. Table 1 shows a brief comparison between the limitations of needle vaccination and microneedle vaccine delivery systems. It lists the comparative differences between syringe and microneedle vaccination and shows how it is a viable and better alternative for mass COVID-19 vaccination. Given the aim of this review paper, we restrict ourselves to reviewing the literature of microneedle-based vaccine delivery methods.
Table 1.
Comparison of syringe and MN vaccination.
| Syringes and Needles (Limitations) | Microneedles in Vaccine Delivery | References | |
|---|---|---|---|
| Strengths | Weaknesses | ||
|
|
|
[45,64] |
|
|
|
[45,65] |
|
|
|
[66,67] |
|
|
|
[51,68,69] |
|
|||
1.1. Immunological Aspects of COVID-19 Medicaments
Scientists all over the world are still searching to find an effective cure for COVID-19, which might end the pandemic so that the world can go back to normalized pre-COVID-19 life [63,69,70]. Unfortunately, the search is still ongoing and will continue until a potent treatment is discovered [8,9,10]. Various therapeutic strategies are under development and are being tested worldwide [11,12]. The outcome of the treatment procedure depends on the host humoral response and the cellular immunity of the patient due to COVID-19 infection [13,14,15]. Table 2 shows the induced immunopathology of the SARS-CoV-2 virus along with the humoral response in humans. Responses from previous SARS-CoV-2 infections could act as key determinants in the development of the therapeutics, since the infection causes the production of anti-SARS-CoV-2 antibodies [16,17,18]. The antibodies produced via the immune response from the infection limits replication through the neutralization of the virus inside the body and plays a major role in controlling the disease [13,20,21]. This mechanism might also contribute to the development of COVID-19 pathogenesis due to the involvement of antibody-dependent enhancement [22,23]. Approaches such as convalescent plasma and monoclonal antibodies have enabled expeditious development in research associated with the treatment of COVID-19 in terms of distinguishing the widely varied clinical features of antibody responses in SARS-CoV-2-infected patients worldwide [24,25,26]. Clinical outcomes from numerous COVID-19 vaccine candidates have been determined, as well as the collection and characterization of a wide panel of monoclonal neutralizing antibodies and early clinical testing [27,28,30]. Figure 1 illustrates the replication process of SARS-CoV-2 and lists the therapeutic targets during the replication process.
Table 2.
SARS-CoV-2-induced immunopathology in humans: symptoms and clinical consequences.
| SL No. | Organ System | Clinical Outcomes | Clinical Manifestations | References |
|---|---|---|---|---|
| 1. | Vascular system |
|
|
[72,73] |
| 2. | Lungs |
|
|
[69,74] |
| 3. | Kidneys |
|
|
[75,76] |
| 4. | Liver |
|
|
[77,78] |
| 5. | Heart |
|
|
[73,79] |
| 6. | Intestine |
|
|
[75,80] |
| 7. | Brain |
|
|
[81,82] |
Note: NK—natural killer, LDH—lactate dehydrogenase, CRP—C-reactive protein, AST—aspartate transaminase, TNF—tumor necrosis factor, IL—interleukin, ALT—alanine transaminase.
Figure 1.
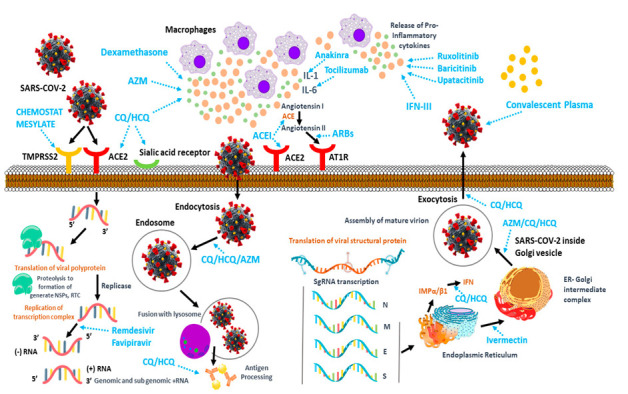
SARS-CoV-2 replication process and possible therapeutic targets (reproduced from [71]).
1.2. Structural Considerations of Coronavirus in Vaccine Development
SARS-CoV-2 is a member of the Coronaviridae family’s subgroup, which includes four species: α, β, γ, and δ. SARS-CoV and Middle East respiratory syndrome (MERS-CoV) are two more extremely deadly viruses in the Coronaviridae family that produced epidemics in 2002–2003 and 2013–present, respectively [7,8,11,13]. The spike (S), envelope (E), membrane (M), and nucleocapsid (N) structural proteins, as well as at least six auxiliary proteins (3a, 6, 7a, 7b, 8, and 10), are all encoded by the SARS-CoV-2 RNA genome [13,14,15,16]. The S protein, which consists of the S1 subunit, S2 subunit, transmembrane, and cytoplasmic domains, infects host cells [22,24,25]. The N-terminal domain (NTD), receptor-binding domain (RBD), subdomain 1 (SD1), and subdomain 2 (SD2) make up the S1 subunit (SD2) [27,28,30]. The RBD of SARS-S1 CoV-2’s subunit interacts with the cellular receptor angiotensin-converting enzyme 2. (ACE2) [83,84,85]. Virus entrance is mediated by CD147. SARS-CoV-2 enters the cytoplasm with its RNA genome and undergoes intracellular replication cycles before being discharged by exocytosis to infect new host cells. COVID-19 patients have a significant morbidity and death rate, which necessitates the rapid development of efficient preventive and treatment measures [82,86,87]. Pneumonia is the most common complication of SARS-CoV-2 infection. COVID-19 individuals who are severely sick or dangerously ill have additional organ damage [88,89]. COVID-19 initiation, amplification, and consummation are three separate stages that patients go through [90,91,92]. Rapid viral replication and the early production of dominant chemokines define the beginning stage [74,93,94]. If the viral infection is not effectively suppressed by the host’s humoral defenses, the patient enters the multiplication stage after developing both humoral and cellular immunity, during which, they produce more inflammatory mediators and recruit a large number of inflammatory cells to increase immunopathological processes [95,96,97]. COVID-19 victims eventually die as a result of persistent elevations in inflammatory mediators and extensive organ damage throughout the culmination stage [98,99,100]. Antibody-mediated humoral immune responses to SARS-CoV-2 infection are critical in the progression of COVID-19 illness [101,102]. In addition, outcomes from clinical research employing convalescent plasma and intravenous immunoglobulins (IVIG) to treat COVID-19 patients with passive antibody therapy have been published [103,104,105]. A vast number of neutralizing monoclonal antibodies have been identified, with some of them having undergone clinical testing [106,107,108]. Clinical effectiveness data from numerous vaccination studies have been published, which are significant [109,110,111]. Table 3 shows the various technologies used for the development of COVID-19 vaccines.
Table 3.
Vaccine platforms against SARS-CoV-2.
| SL No. | Vaccine Technology | Principle | Advantage | Disadvantage | References |
|---|---|---|---|---|---|
| 1. | mRNA-based | Delivery of modified mRNA |
|
|
[27,77,156] |
| 2. | DNA-based | Vector-based delivery of a viral gene |
|
|
[114,157,158] |
| 3. | Peptide-based | A fragment of whole-length viral peptide |
|
|
[159,160] |
| 4. | Live attenuated virus | De-optimization of the genome (to reduce pathogenicity) |
|
|
[157,161] |
| 5. | Inactivated virus | Chemically or UV-inactivated virus |
|
|
[92,162,163] |
Coronaviruses are single-stranded RNA viruses with an enclosed surface glycoprotein spike that facilitates receptor binding and cell penetration during infection [112,113]. Because of its functions in receptor binding and membrane fusion, the spike protein is a promising vaccination antigen [114,115,116]. Apart from entire virion-inactivated vaccines, almost all producers are targeting spike protein as an antigen [117,118,119]. Instead of incorporating the entire pathogen, new-generation vaccinations, such as recombinant protein vaccines and vector-based vaccines, only include a particular antigen or antigens from the disease, providing a superior safety profile [120,121,122]. Detailed knowledge of the pathogen’s structure and immunopathogenesis is required for the development of an effective new-generation vaccine [123,124]. Depending on the carrier of the antigen, the new-generation COVID-19 vaccines may be divided into recombinant protein vaccines and vector vaccines (for instance, mRNA vaccines, plasmid DNA vaccines, viral vector vaccines, and bacterial vector vaccines) [125,126,127]. The structural and pathobiology characteristics of the SARS-CoV-2 virus were used to choose the target antigen for new-generation vaccination [128,129,130]. The SARS-CoV-2 genome is a single-stranded, positive-sense RNA. The S proteins are found on the virus’s outer surface and can bind to ACE2 on the cell surface, allowing for receptor-mediated viral endocytosis [131,132,133]. Animal models that express human ACE2 counterparts should be utilized in challenge experiments to evaluate vaccination effectiveness, according to the ACE2-dependent mechanism [134,135]. Although the SARS-CoV S protein can employ CD209 and CD209L as alternative receptors, it is unknown if SARS-CoV-2 can as well [136,137,138]. Most COVID-19 vaccine candidates employ the S protein as the antigen since it plays such an important part in the virus’s life cycle [139,140]. The use of RNA for vaccine development is a game-changing technique that requires the adoption of a suitable delivery method to increase the oligonucleotide’s intracellular stability, and hence, translatability [141,142] The antigen of interest is encoded by non-replicating mRNA vaccines, but self-amplifying RNA leads to the translation of both the antigen and the viral replication machinery, allowing intracellular RNA amplification and protein expression [143,144,145]. Figure 2 illustrates the different stages of the pathogenesis of COVID-19 and possible targets for vaccine development.
Figure 2.
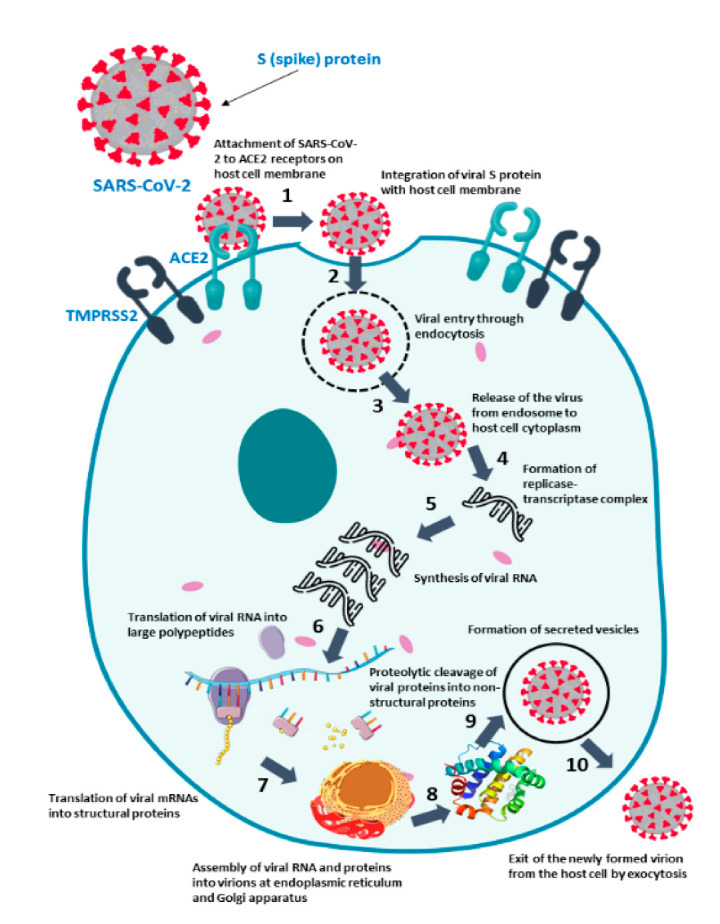
Various (numbered) stages involved in COVID-19 pathogenesis that might be used as targets for targeted treatment and vaccine development (reproduced from [155]).
While it is critical to expedite the development of these immune-mediated treatments, it is also vital to remember that there are still many unanswered issues about SARS-CoV-2 infection and its influence on host immunity [114,146]. On the one hand, this enhanced information is essential for elucidating the many processes of the host immune response involved in viral neutralization and/or the elimination of infected cells [147,148,149]. On the other hand, it will also forecast the outcome when used at a large scale in the targeted demographic [150,151,152]. As a result, the effect of gender and age on the virus’s ability to modulate host immune response, as well as the impact of SARS-CoV-2 infection on the immunity of patients with chronic diseases such as diabetes, hypertension, and chronic obstructive pulmonary disease (COPD), must be fully addressed [153,154].
1.3. Distribution Concerns of COVID-19 Vaccines
Prior to the COVID-19 pandemic, researchers did not seem to pay regular attention to the storage temperature for mRNA vaccine candidates that were under the development process. Small quantities were often frozen at −80 °C and then thawed and injected as needed [162,164,165]. Table 4 shows the current mRNA COVID-19 vaccine stability profile, dose, and dosing schedule.
Table 4.
Current mRNA COVID-19 vaccine Stability profile, dose, and dosing schedule.
| Stability Profile | Manufacturer | References | |
|---|---|---|---|
| Moderna | Pfizer-BioNTech | ||
| Frozen State | −20 °C up to 6 months | −80 °C to −60 °C up to 6 months | [78,89,109,166,167,168] |
| 2–8 °C | 30 days | Up to 5 days | |
| Room Temperature | Up to 12 h. | Up to 2 h. (up to 6 h. after dilution) | |
| Dose | 100 µg (0.5 mL) | 30 µg (0.3 mL) | [109,159,169] |
| Dosing Schedule | Day 1, Day 29 | Day 1, Day 21 | |
In addition to the rising clinical promise of mRNA-based COVID-19 vaccines, there was a growing concern that storage, transport, and administration under these conditions would pose a significant problem when hundreds of millions (if not billions) of doses were to be distributed globally [170,171]. It is critical to understand that the entire undamaged mRNA molecule is required for the vaccine’s effectiveness [172,173,174]. Even a small degradation event anywhere along an mRNA strand might significantly delay or halt that strand’s normal translation performance, resulting in inadequate antigen expression [175,176,177]. Therapeutic proteins and protein antigens, on the other hand, may undergo numerous chemical degradation processes [104,178,179]. The crucial issue of delivering mRNA into cells, as well as the critical contribution of formulation utilizing diverse delivery vehicles, must be given special consideration [80,180,181]. To safeguard our communities against worsening and future epidemics, high COVID-19 immunization rates are critical. Hundreds of millions of vaccination doses will require tremendous planning and implementation [182,183]. Despite the fact that this may be the world’s largest single vaccination attempt, best practices and lessons learned in pandemic preparedness, supply chain management, distribution, and clinical practice can help us immunize against SARS-CoV-2 [184,185,186]. To successfully manage vaccine delivery and administration to hundreds of millions of people, deliberate planning and coordination with local and international partners are essential [187,188,189]. Figure 3 shows the packaging and distribution process of the vaccines from production to use.
Figure 3.

The coronavirus disease vaccine is packaged and distributed in various levels to ensure cold storage throughout the supply chain for a successful vaccination campaign (taken from) [190].
1.4. The Need for Novel Vaccine Delivery System
Despite the extreme discomfort involved with injections, expensive prices, and difficult injection schedules, many vaccinations and medicines need multi-bolus regimens, which can cause financial and emotional burden for patients [189,191,192]. Because of their restricted access to healthcare practitioners, people in underdeveloped nations face a greater challenge [77,163,193]. Low patient compliance, as well as other needle-and-syringe-related concerns, have been identified in several global health studies as major barriers to worldwide vaccination against deadly infectious illnesses including pneumococcal pneumonia [188,194]. The idea of a single-injection vaccine, which is acknowledged by the World Health Organization (WHO) as a preferred immunization method, has been studied for many years [195,196]. Furthermore, biohazards and the potential of disease transmission from the billions of needles/syringes discarded each year continue to be major problems with injection-based systems [155,197]. As a result, a novel medication and vaccine delivery strategy that is injection-free and only requires a single dose is urgently needed [198,199].
1.5. Microneedles in Transdermal Drug and Vaccine Delivery
Transdermal microneedles, which are painless and simple to use, have been shown to be an enhanced drug-delivery technique that allows for the less invasive administration of medicinal substances [159,200]. Transdermal microneedles are useful for vaccination because the presence of a significant number of immune cells (Langerhans cells) in the dermal layer of the skin improves immunogenicity [201,202]. However, microneedles only offer either rapid or sustained release, which limits their application in vaccine administration [203,204,205]. Due to the continual presence of the vaccine antigen inside the body, immediate-release versions may cause the formation of immunological tolerance against the vaccination, whereas sustained-release variants may induce the development of immune tolerance against the vaccine [206,207]. A transdermal microneedle device with programmable delayed burst release across prolonged time periods is required to replicate the traditional immunization process’s numerous bolus injections [208,209,210] This limitation is primarily due to a lack of a manufacturing technology capable of producing microneedles with core–shell or reservoir-based microstructures, which are required to provide pulsatile or delayed burst release with various desired lag times to mimic the drug-release pattern of multiple injections [10,211,212]. Recent advances in lithography-based methods and 3D printing have made it possible to construct drug-delivery devices with unique drug-release kinetics. Current lithography-based techniques can only generate two-dimensional structures, while current three-dimensional (3D) printing significantly relies on potentially hazardous impurities (such as ultraviolet-curing agents) [213,214,215]. Dissolving microneedles result in further advantages, both for the people who are vaccinated and for logistics, through providing tiny storage and disposal sizes, low-cost manufacture, and convenience of use, allowing for self-administration at home.
2. Dissolving Microneedles in Immunization
Dissolving microneedles (DMNs) are miniature needles made of polymers such as polylactic-co-glycolic acid (PLGA), polylactic acid (PLA), and polyglycolic acid (PGA) that dissolve in the skin to deliver encapsulated medicines, leaving no sharp waste [56,216]. DMN arrays are now overlaid onto patches to aid in their implantation into the skin [10,217]. The arrays produced on the patch are often not completely implanted, and significant amounts of loaded materials are not supplied due to substantial differences in skin elasticity and the amount of hair on the skin [213,218,219]. Drugs are most commonly delivered orally or by parenteral injection, among the numerous delivery methods available [60,61,220,221]. Thus, dissolving microneedles poses a suitable vaccine delivery system and is a worthy alternative for replacing traditional needle vaccination methods. The bioavailability of many orally administrable drugs is considerably decreased because of first-pass metabolism that can be affected by varied physiological elements such as the activity of enzymes, the level of serum protein, and the gastrointestinal motility of the drug in the body, although the oral dosage form is the most convenient method for drug administration [2,31,68,222]. For delivering medicines directly into the bloodstream, hypodermic injection is more convenient and can avoid the mentioned side effects [223,224,225]. However, there are several disadvantages to hypodermic injection, including the high degree of competence necessary to deliver an injection, the trypanophobia of some patients, and the danger of infection acquired by needle sticks on occasion [37,69]. Several researchers developed microneedle (MN)-mediated drug-delivery devices to overcome these restrictions, allowing patients to self-administer therapeutic micro- and macromolecule medicines without discomfort [226,227,228].
Dissolving microneedles (DMNs) are tiny needles made of polymeric materials that contain medications. The medication is released for systemic or local administration when DMNs are injected into the skin and catalyze the breakdown of the polymeric molecule [63,229,230]. DMNs are completely biocompatible and do not produce biohazardous sharp waste, unlike hypodermic injections [231,232]. Furthermore, as compared to subcutaneous vaccinations, DMNs have been found to be more dose-effective [233,234,235].
Currently, the only DMN application technique is to superimpose an array of microneedles onto patches, which allows for easier microneedle insertion and maintenance [41,236,237]. Patches are commonly employed as supports in DMN applications, although the efficacy of drug administration that may be obtained with patches is typically considerably decreased owing to excessive skin elasticity, which can result in inadequate DMN insertion [238,239]. Furthermore, the chemicals utilized in patch materials can cause skin irritation and/or allergic responses; other patch delivery drawbacks include difficulty sticking to flexible body joint regions and hairy skin [240,241,242]. Furthermore, before the patch can be removed, patients must wait for the DMNs to entirely disintegrate [222,243,244]. Table 5 shows the usefulness of dissolving microneedles in the vaccination procedures based on several criteria. Table 6 shows the different animal models for the use of dissolving microneedles for vaccination.
Table 5.
Extent of utility of DMN in vaccination.
| SL No. | Criteria | DMN Array Patch (Score) |
|---|---|---|
| 1. | Manufacturing cost | ** |
| 2. | Mass production | *** |
| 3. | Self-administration | ***** |
| 4. | Wear time | *** |
| 5. | Material biocompatibility | *** |
| 6. | Accurate dosage delivery | *** |
| 7. | Aseptic process | *** |
| 8. | Stability against humidity | ** |
| 9. | Waste generation | ***** |
Note: *****—highest, ***—moderate, **—lowest.
Table 6.
Model animals and vaccines for dissolving microneedle array patches (DMAP).
| SL No. | Types of Vaccine | Animal Model | References |
|---|---|---|---|
| 1. | Influenza (inactivated) | Mouse | [245,246] |
| 2. | Hepatitis B (recombinant subunit) | Mouse | [78,159] |
| 3. | HIV (recombinant vector) | Mouse | [247,248] |
| 4. | Dengue virus (live attenuated) | Mouse | [63] |
| 5. | Ebola (DNA) | Mouse | [249,250] |
| 6. | Enterovirus (VLPs) | Mouse | [63] |
| 7. | Rotavirus (inactivated) | Mouse | [67] |
| 8. | Polio virus (inactivated) | Mouse | [128,251] |
| 9. | Streptococcus (inactivated) | Mouse | [63] |
| 10. | Staphylococcus (recombinant subunit) | Mouse | [63,166] |
| 11. | Shigella (BLP) | Mouse | [46,63] |
| 12. | Clostridium (toxoid) | Mouse | [46,63] |
| 13. | BCG (live attenuated) | Mouse | [107,252] |
| 14. | Neisseria gonorrhea (inactivated) | Mouse | [63,229,253,254] |
| 15. | Pseudomonas aeruginosa (inactivated) | Mouse | [64,253,254] |
| 16. | Orientia tsutsugamushi (recombinant subunit) | Mouse | [64,253,254] |
| 17. | Malaria (recombinant subunit) | Mouse | [63,253,255] |
| 18. | Influenza, DT, tetanus toxoid (inactivated) | Rat | [58,256] |
| 19. | BCG (live attenuated) | Mouse | [257] |
| 20. | Influenza (inactivated) | Guinea pig | [40,245] |
| 21. | Hepatitis B (recombinant subunit) | Pig | [258,259] |
| 22. | Hepatitis C (VLPs) | Mouse | [196,260] |
| 23. | Rabies (DNA) | Dog | [63,156] |
| 24. | IPV (inactivated) | Monkey | [261,262] |
| 25. | Measles (live attenuated) | Mouse | [63,128] |
| 26. | Hepatitis B (recombinant subunit) | Mouse | [258,259] |
| 27. | Tetanus toxoid (inactivated) | Pregnant mouse | [256,263] |
| 28. | Measles, rubella (live attenuated) | Infant monkey | [264,265] |
Note: IPV stands for inactivated poliovirus vaccine; VLPs stands for virus-like particles; BCG stands for Bacille Calmette–Guerin; HIV stands for human immunodeficiency virus; DT stands for diphtheria and tetanus vaccine; BLP stands for bacterium like particles.
2.1. Fabrication of Dissolving Microneedles
Dissolving MNs are typically made by pouring liquid mixture into a previously prepared MN mold. In most cases, a silicon wafer is used as the starting material for the mold. The wafer is then oxidized at 1000 degrees Celsius. Lithography is utilized to create a needle geometry, followed by RIE, and CVD is used to coat a wafer. A liquid polymeric solution is put into the molds that have been produced. Air gaps are eliminated with a vacuum or centrifuge after a liquid polymeric solution is put into the prepared molds. After that, the mold is dried in an oven, and the MNs are removed after they have cooled. The advantages of this technique are that it produces MNs in a reasonably easy and cost-effective manner at room temperature.
The core–shell microstructure of the dissolving microneedles is created by assembling three separate components of the microneedles, including a microneedle shell, a microneedle cap, and a dry drug or vaccine core, utilizing a 3D manufacturing method [46,55,266]. The cap and base layer, which are composed of the same biodegradable polymer, poly(d,l-lactide-co-glycolide) (PLGA), encase the medication or vaccine core [212,216]. The drug release may be precisely regulated by adjusting the PLGA shell’s disintegration [217,219]. The microneedles may easily be implanted and thoroughly lodged into the dermal layer following fast skin healing due to their small points and smooth shape [267,268]. In theory, numerous sets of microneedles with various PLGA shells may be inserted into the skin of patients at the same time in the clinical environment to produce multiple burst release across different time periods, comparable to multiple bolus injections [61,269].
When different kinds of sugars are used as the matrix for dissolving microneedles, drugs or vaccines are usually released quickly in vivo [33,68]. For example, Ito et al. (2013) [254] reported that insulin was released from microneedles very quickly, with almost all the formulated insulin being released within 1 h when dextrin was used as the matrix [36,270]. Nonetheless, in some cases, a continuous release of medicines or vaccinations is necessary [271,272,273]. A prototype of DMNs was constructed by Lee et al. [274], in which therapeutic material was encapsulated merely as a backing layer that aided as a reservoir for the controlled release of therapeutic molecules by protruding it with interstitial fluid, which prolonged the molecule diffusion into the skin through the channels formed by DMNs [63,226,275]. Figure 4 shows the strategy of the fabrication of a dissolving microneedle array via micromolding, and Figure 5 shows different fabrication methods of dissolving microneedles.
Figure 4.

Dissolving microneedle array manufacturing strategy via micromolding (taken from [276]).
Figure 5.
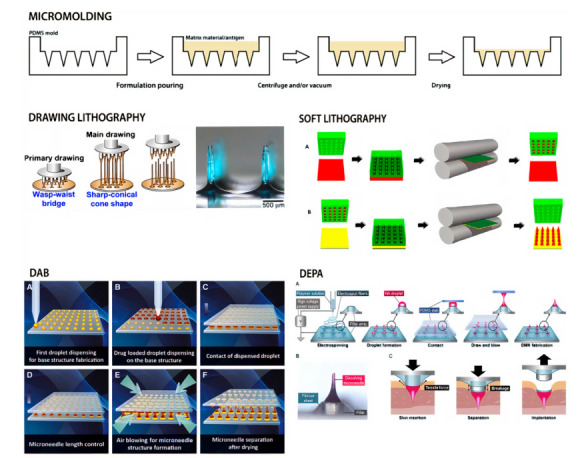
dMN manufacturing methods (taken from [277]) Micromolding with a polydimethylsiloxane (PDMS) mold is the most prevalent method for producing dMNs. Drawing lithography operates by extending two-dimensional polymeric material into a three-dimensional shape. Longitudinal extension of molten polymer by pillaring higher moving plate. In soft lithography, dMNs are produced by (A) heating a polymer sheet and a mold with microcavities. (B) The filled mold is then heated and placed on a flexible, water-soluble substrate. After mold detachment, a dMN patch remains on the substrate. Droplet-born air blowing (DAB) applies a (A) polymer solution and (B) a drug solution to two plates. (C) The upper plate is lowered until the droplets meet, (D)then withdrawn a distance equal to the two dMN lengths of the lower and top plates. (E) Drying the polymer solutions results in a dMN patch on each plate. (F) In addition, fabrication at moderate temperatures (4–25 degrees Celsius) minimizes medication and polymer waste. dMN on an electrospun pillar array (DEPA) is a variant of DAB. (A) The flat plate is replaced with a columnar array covered in a fibrous layer. (B) A PDMS slab is then utilized to draw and stretch polymer formulation droplets, resulting in microneedles. (C) Finally, the movement of air dries off the elongated droplets to form dissolving microneedles.
The manufacturing approach for fabricating dissolving MNAs with new microneedle shapes is visually depicted in Figure 5. This six-step strategy takes advantage of AM and micromolding to generate dissolving undercut MNAs while also accomplishing high-throughput fabrication: (1) MNA design in 3D CAD; (2) the direct production of a master MNA from the CAD drawing by 3D direct laser writing using a non-dissolvable resin (IP-S); (3) the high-fidelity replication of master MNA by micromolding with UV-curable resin (VeroWhite); (4) the creation of MNA master molds consisting of multiple master MNA replicas on 3D-printed MNA holders; (5) the manufacturing of elastomer (PDMS) micromolding of MNA production molds; and the spin-casting of tip-loaded, dissolving MNAs with undercut microneedles containing a vaccine or other biocargo in a water-soluble biocompatible substance (e.g., carboxymethylcellulose (CMC) and trehalose). The final step of the process varies depending on the biocargo in question, but it usually involves spin-casting cargo (e.g., vaccine) into the tip of the PDMS production molds, followed by spin-casting a dissolvable hydrogel (e.g., CMC/trehalose) into the production molds to serve as the structural material.
Biodegradable microneedles, which are made up of various biodegradable polymers such as polylactic acid, chitosan, polyglycolic acid, or poly(lactide-co-glycolide) (PLGA), break down in the skin after use, allowing the release of integrated medicines to be continued for months [230,231,232]. A recent study showed that these biodegradable microneedles might be used as a patient-friendly alternative to traditional sustained-delivery techniques [70,278,279]. However, to properly use the biodegradable polymer’s breakdown property, these microneedles must be implanted and left in the skin for several days [41,237,242]. The notable disadvantages of the fabrication of dissolving microneedles include manufacturing demanding the use of technical competence and time for the substance to dissolve. Microneedle separation into the skin was shown by Kim et al. [254] to be mediated by hydrogel swelling in reaction to contact with bodily fluid after the needles were introduced into the skin [243,280,281]. The hydrogel particles immediately absorbed water, causing the microneedles to break owing to the differential volume expansion between the needle–matrix polymer and the hydrogel particles [253,282,283]. The enlarged particles completely disintegrated the microneedles, leaving the microneedle tips in the skin of a porcine cadaver in vitro and a hairless mouse in vivo [284,285,286]. Figure 6 shows the fabrication of dissolving microneedle arrays with the PDMS micromolding technique.
Figure 6.
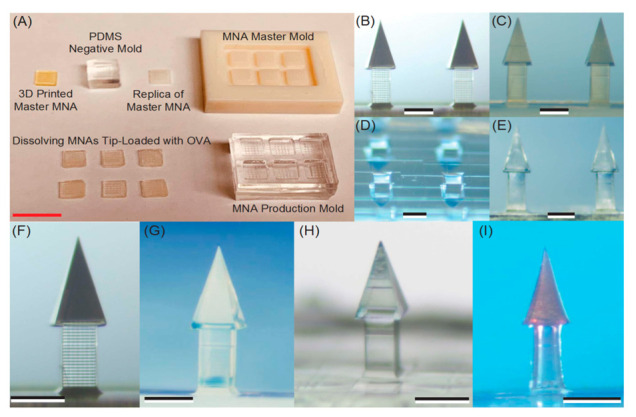
Fabrication of novel dissolving MNAs with undercut microneedles. (A) Finished items according to each stage of the production plan outlined. The scale bar measures 10 mm. (B–I). Optical stereomicroscopy was used to verify the geometric quality of the produced MNAs. The scale bars are 250 m in length. (B) Three-dimensional direct laser writing was used to generate the master MNA. (C) A two-stage micromolding approach was used to generate a replica of the master MNA (elastomer molding combined with UV-curable micromolding). (D) Wells formed like microneedles in an MNA manufacturing mold. (E) Dissolving CMC/trehalose MNA in the final stage, including a multicomponent vaccine (OVA + Poly(I:C)). (F) A closer look at a single undercut microneedle on the 3D-printed master MNA (as in B). (G) Magnification of an individual undercut microneedle on a master MNA replica at higher magnification (as in C). (H) Dissolving PVP/PVA microneedle tip filled with Alexa680-labeled OVA at the end. (I) A final dissolving CMC/trehalose microneedle tip filled with doxorubicin, a red-colored, chemotherapeutic, small-molecule medication, is shown. (Taken from [276]).
2.2. Biodegradation Kinetics of Dissolvable Microneedles
Through considering the biodegradation kinetics of a DMN array as a mathematical model, the need for exploratory in vitro experiments during the design of new biodegradable matrix-based therapeutics can be reduced [287]. The development of such a model will allow key parameters such as DMN height, shape, and patch size to be optimized in a faster and more cost-effective way than by running laboratory experiments. However, the mechanism of degradation for a particular polymer is complex, as it depends on the properties of its polymer matrix such as its chemistry, molecular weight, and morphology [141]. It also depends on both the external environment, the payload property, and the skin property, as shown in Figure 7.
Figure 7.

Schematic showing the variables which can affect the rate of drug release from a dissolvable microneedle (adapted from [289]).
It is desirable to achieve a zero-order kinetics release profile during drug delivery to result in sustained release, which is independent of the concentration of the dissolved drug, and to prevent the drug concentration falling below minimum effective levels or rising above maximum safety levels [288].
However, this has been reported as idealized and difficult to achieve, with the majority of drug release profiles from polymeric drug-delivery systems resulting in a triphasic profile [289]. Although the release profile of each polymeric microneedle system should be evaluated on a case-by-case basis, some previous efforts to model degradation-controlled release, such as from a DMN, are outlined below.
2.3. Loading Capacity of Dissolvable Microneedles
Temperature-sensitive medicines such as peptides, antibiotics, and vaccines, as well as any temperature-labile treatment, may be bulk loaded into microneedle structures using room-temperature and aqueous-based micromolding [236,290]. Adjusting the postprocessing parameters of the microneedle structures, particularly the silk protein secondary structure, allows for the controlled release of a model drug [243,291].
Due to the bulk loading of dissolvable or biodegradable systems, microneedles efficiently bypass the epidermal barrier to provide this route as a viable option to the oral and parenteral administration of therapeutics, and relatively high dosages may be given [292,293] However, there are still a number of issues to be resolved. The skin’s barrier function, for example, varies from one location to the next on the same individual, from person to person, and with age [222,294,295]. Because the variation in individual skin and the penetration depth of microneedles are related to stress on the skin, an applicator may be necessary to produce a consistent penetration depth during each microneedle administration [63,296]. Furthermore, prolonged drug or vaccine release is more difficult than bolus release, and the kinetics should be researched and confirmed [232,297]. If microneedles are used often, it is also important to evaluate if dissolved or degraded matrices have any adverse effects [298,299,300] Microneedle vaccination elicited immune responses that were equivalent to those elicited by intramuscular injection in some cases but were greater in others [222,301,302]. Overall, microneedle immunization resulted in higher recall cellular immune responses, more antibody-secreting cells, and, most importantly, more effective viral clearance [33,70]. Figure 8 shows vaccine delivery into skin and induced immunity in mice.
Figure 8.

DMN vaccine delivery to human skin and induced immunity in mice (taken from [276]). Note: OVA—ovalbumin (model antigen), IM—intramuscular, MNA—microneedle administration.
2.4. Significance of Novel Transdermal Vaccination
Most vaccines are administered through injection, either intramuscularly or subcutaneously, which can be unpleasant and uncomfortable for individuals who are scared of needles [46,68]. Additionally, the hypodermic needles used to administer the vaccine in these methods generate hazardous waste, which might result in injuries and infection when needles are reused [243,290]. Infectious diseases such as Hepatitis B and AIDS can be transmitted through the latter, particularly in underdeveloped countries [46,55,266]. Moreover, the use of new vaccine delivery techniques may give a variety of other advantages, such as antigen thermal stability, fewer booster doses, and, as a consequence, greater vaccination adherence and a lower burden on healthcare personnel [236,239,290]. Both these advantages would be especially beneficial in large-scale vaccination operations, such as in the case of an outbreak, where feasible and rapid immunization procedures are necessary [56,63,249]. Because the skin is an immune-competent organ that is also easily accessible, dermal vaccination delivery seems intriguing [41,45,50]. In the viable epidermis and dermis, many antigen-presenting cells (APCs) such as Langerhans cells (LCs) and dermal dendritic cells may be detected (dDCs) [254,303,304]. Antigen-presenting cells gather antigens and subsequently transport them to draining lymph nodes, where they transfer the antigen to T cells, activating Ag-specific T cells and B cells for a systemic immune response [41,220,286]. Microneedles penetrate the skin barrier and underneath tissue to transfer the antigen into the epidermis or dermis while staying short enough to avoid pain receptors, therefore preventing pain sensation [261,305]. Additionally, MN vaccination may not require the employment of health practitioners and will not result in sharp needle waste after immunization [37,53,305,306].
2.5. Mathematical Modeling of Microneedles
The mathematical modeling of microneedles for vaccine delivery is key in optimizing the MN performance. Currently, there are few publications involving the modeling and optimization of DMN arrays when compared with solid or hollow microneedles. Consequently, this section aims to summarize the drug-delivery mechanisms discussed within these papers along with the key parameters that have been found to affect the drug release rate from the microneedle array and the microneedle penetration depth with a view to learn the key lessons from these publications. To date, the method chosen by most studies to model DMNs was the finite element method (FEM) [158]. This is because this method is able to produce detailed diffusion or force distribution profiles [304,306,307]. Figure 9 shows a finite element analysis of the surface von Mises stress on a single microneedle.
Figure 9.

Finite element analysis of a CMC/maltose microneedle with a conical shape. (A) Surface von Mises stress when an axial load of 5 N is applied on the base. (B) Prediction of bucking mode when an axial load of 5 N is applied at the base and a fixed constraint is forced at the tip [306].
2.5.1. MN Delivery Mechanisms
This section discusses the fundamental principles used to derive the DMN mathematical models reported within the literature to date. To successfully deliver a drug, a DMN system must be applied to the skin to puncture the stratum corneum and permeate the upper dermal layers. Once the needles are “wetted” by moisture in the skin, they will dissolve to release drug molecules which are eventually adsorbed into the circulation [307]. Typically, Fick’s law can be used to simulate the diffusion profile of the drug molecules in microneedle-treated skin. Fick’s first law is used to describe steady state diffusion. Fick’s second law is used to describe transient diffusion [158].
The value of diffusion coefficient used in Fick’s law can be calculated using various methods, described in detail by Yadav et al. [141]. Chavoshi et al. [308] also reported that the drug diffusion coefficient will increase as polymer degradation occurs. Despite this, many models of DMNs assume that the drug concentration in the skin layer is uniform because the rate of diffusion is rapid compared to the dissolution of the microneedle or elimination into the bloodstream [309,310].
Ronnander et al. [309] developed a mathematical model to show the in vitro dissolution and release of sumatriptan succinate from PVP-based microneedles shaped as pyramids. To do this, governing equations were derived using material balances to relate the microneedle pyramid height and drug concentration in the skin over time.
Kim et al. [310] used a similar approach to predict the amount of drug (fentanyl) delivered into the skin via the dissolution of a water-soluble (sucrose) microneedle. More recently, this approach was used by Zoudani and Soltani [311] to create a numerical simulation of a dissolution process of a DMN in porous medium. However, Kim et al. [310]; Ronnander et al. [307]; Zoudani and Soltani [311] assumed that the ratio of needle height to the base radius remains constant throughout the dissolution process. This may not always be true; therefore, a more accurate model would consider these variables independently.
When creating their numerical simulations, Zoudani and Soltani [311] introduced a hindrance factor to investigate the effect of a drug’s molecular radius on a drug’s effective diffusion coefficient in the skin. This was not considered in the studies completed by Kim et al. [310] or Ronnander et al. [307].
2.5.2. Effect of Polymer Type
To date, there have been various studies completed to optimize the polymer used in a DMN array [306,309,312,313,314]. Each study has been undertaken with the aim of providing a formulation with optimum values for Young’s modulus, Poisson’s ratio, ultimate tensile stress, dissolution kinetics, and polymer adsorption rate. Moreover, there are a good number of articles (e.g., [47,222,315,316,317]) that discuss the varied types of materials usually used to fabricate MNs.
To study the traits of sugar MNs, Loizidou et al. [306] used finite element analyses which was the first initiative undertaken with the objective of optimizing the polymer. They evaluated the effects of sugar composition on MNs’ capability to penetrate and dispatch therapeutic materials through the skin. MNs made from CMC/maltose were found to be better than those made from CMC/trehlose and CMC/sucrose in terms of their mechanical strength and ability to deliver drugs. Loizidou et al. [306] also stated that the main mode of microneedle failure is buckling, which is positively correlated to the Young’s modulus of the microneedle array.
Amodwala et al. [318] completed a similar study to optimize the ratios of PVA to PVP and the solid content of a matrix to achieve maximum microneedle strength. The optimum patch was found to contain a 9:1 PVA to PVP ratio with 50% solid content. This formulation showed a maximum needle fracture force of 0.9N and was found to release 100% of the encapsulated drug (meloxicam) in 60 min [312]. Similarly, Ronnander et al. [309] looked at different ratios of water, sumatriptan succinate, and PVP within a DMN array and found that the formulation affects the drug release rate and time needed for the polymeric microneedle to dissolve.
Suriyaamporn et al. [314] used computer-aided rational design to optimize the formulation of Gantrez- and hyaluronic-acid-based DMNs as a potential ocular delivery system. The optimal DMN formulation was found to be 20.06% Gantrez +5% hyaluronic acid +1% Fluorescein Sodium, as it gave the optimum combination of dissolution time, insertion force, and insertion depth.
However, the simulations of drug delivery using DMN can be advanced through looking at the interactions between the polymer and drug in the microneedle structure. Hao Feng et al. [313] used molecular dynamic simulations to model the binding energy and electronegativity differences between polymer and drug molecules. This study is essential for determining compatibility between the polymer and loaded drug, therefore allowing for efficient drug delivery and minimal wastage of drugs.
2.5.3. Effect of Microneedle Array Geometric Parameters
In a microneedle array, properties such as the needle length, tip radius, base diameter, center-to-center spacing between two microneedles, the number of microneedles, and the distribution of microneedles in an array work together as a synergetic system. The needle geometry, thickness, and density are also parameters which will affect the concentration of active pharmaceutical ingredients in the blood [157].
Various publications have shown that increasing the pitch width between microneedles in an array will reduce the level of drug in the dermal layer of skin [311,312]. However, it has been further suggested that the effect of microneedle pitch on skin permeation is non-linear, and decreasing the pitch size has no significant effect on dissolution time [309]. Despite these findings, during their study on the amount of drug delivered into the skin via the dissolution of a water-soluble microneedle, Kim et al. [310] neglected the effect of the pitch and needle geometry on the deformation of skin. Therefore, these effects need to be considered to increase the accuracy of this model.
Chen et al. [319] found that polymeric microneedles with a longer length presented higher TDD efficiency. The drug used in this study was insulin, and the microneedle lengths varied between 124 µm and 445 µm. These results can be explained by considering the microneedle volume present in the viable epidermis and dermis layers of skin, which have increased transport properties when compared to the stratum corneum [320]. As the needle length increased, the percentage of needle volume present in the viable epidermis and dermis increased, leading to an increased release of insulin. Despite these findings, the author noted that using longer polymeric microneedles may not be optimal, as shorter lengths would significantly reduce the pain due to skin piercing. Gomaa et al. [321] also found that longer microneedles may require a greater insertion force for their use to be effective.
Zoudani and Soltani [311] proposed a new approach called array in array theory, a cone with an array of hemispherical convexities located in the second half of the microneedle, as shown in Figure 10. According to the numerical simulation of this design, the drug concentration left in the tissue was double the concentration left from a conical design; however, the time taken for the needle to be fully dissolved was unaffected. Therefore, the new configuration led to a more effective and economic method of drug delivery through a DMN array [322]. Despite this, a much more complicated fabrication procedure is expected for such devices.
Figure 10.
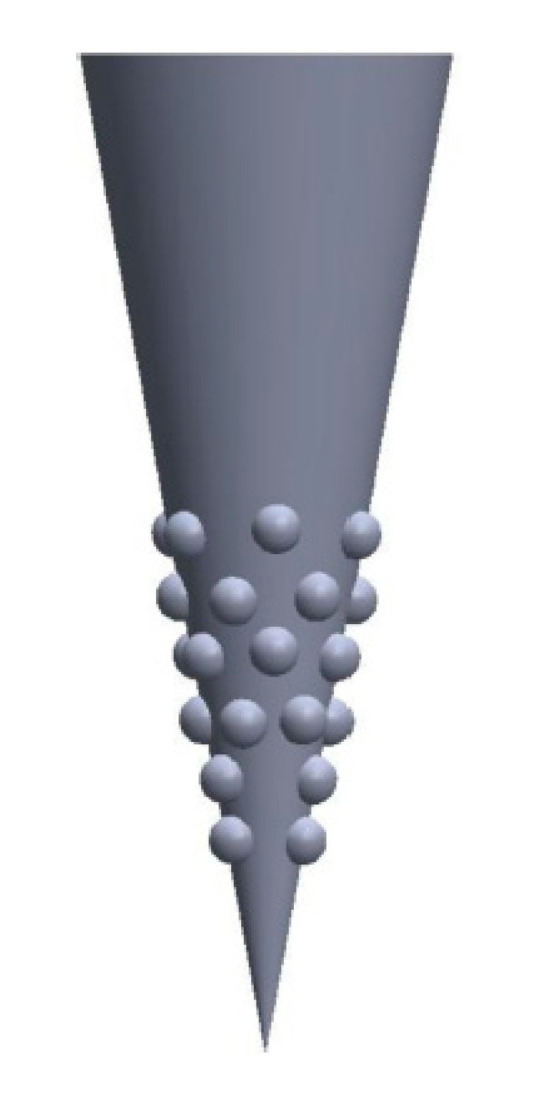
Configurations of the microneedle shape [311].
2.5.4. Effect of Skin Properties
Skin has a viscoelastic property, which must be considered when modeling the insertion behavior of a DMN array [158]. Skin thickness, Young’s modulus, porosity, and viscoelasticity are important parameters that may affect the DMN penetration depth.
As aforementioned, Loizidou et al. [306] performed experimental and finite element analyses to study the mechanical properties of sugar microneedles when inserted into skin, as shown in Figure 10. However, there are fewer publications on the insertion behavior of DMN compared to solid or hollow MNs. Although polymeric microneedles are soft compared to solid microneedles, the principles of microneedle insertion into skin remain the same.
3. Dissolving Microneedles: Some Satisfactory Aspects
Transdermal medication has become a very popular, effective, and promising administration route for drug delivery, and the concept of microneedles has intensified this [55,323]. Researchers have successfully established vaccination delivery via MNs through numerous studies [39,261,265,324,325,326,327,328], and now, DMNs have attracted immense attention for COVID-19 vaccine delivery. Researchers are optimistic about using DMNs for mass vaccination for COVID-19 due to the reasons outlined in Figure 11.
Figure 11.
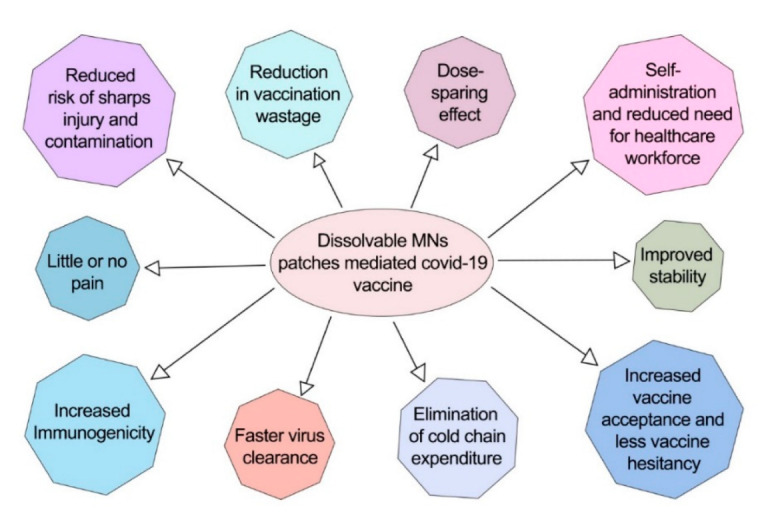
Advantages of dissolvable MN-mediated COVID-19 vaccine (information taken from [329]).
Research works that support the dissolvable-MN-patch-mediated COVID-19 vaccination system are displayed in Table 7.
Table 7.
Research works carried out to establish MN-mediated vaccine delivery.
| Targeted Molecule |
Disease Causing Microorganisms | |||||||
|---|---|---|---|---|---|---|---|---|
| Nucleic Acid | Rabies [330] | BCG [331] | Ebola [250] | Hepatitis B virus [258] | Porcine circovirus type 2 [332] | |||
| Viral Vector | SARS-CoV-2 [142] | Zika [333] | HIV [247,334,335] | |||||
| Protein-Based or VLP | SARS-CoV-2 [336] | HIV [337] | Influenza [33,233,245,338,339,340,341,342,343,344,345,346,347,348] | Hepatitis B [259,260,349] | Diphtheria [256,305,350] | HPV [65] | Tetanus [263,306,350] | Malaria [256] |
| Inactivated or Live Attenuated | Influenza [66,246,351,352,353,354] |
Polio virus [261,355] | Rubella [325,356] | Adenovirus [33,357] | Streptococcus [358] | BCG [257] |
Measles [325,356,359] | Rotavirus [67] |
3.1. Patient Compliance
MNs are safe therapeutic devices that do not require highly experienced or properly trained caregivers to administer them [360]. MN patches can be used to self-administer vaccinations [59,246]. MNs are the best possible suitable vaccination option for people with needle phobias [54]. In addition, MNs do not cause irritation after administration and are less painful than conventional syringes [34,42,298,361,362,363,364]. DMNs are the best possible substitute and hold the potential to be better than conventional syringes [346] because of the following reasons:
3.2. Overall Vaccination Cost Reduction
As DMNs are fabricated from dissolvable polymers, they have the potential to eliminate the manufacturing cost of syringe and vials [163,170,329,365]. DMNs also have the potential to reduce the storage, distribution, and overall manufacturing cost of COVID-19 vaccinations. Table 8 summarizes how DMNs will reduce the total cost of COVID-19 mass vaccination.
Table 8.
Comparison between DMNs and conventional syringes regarding cost reduction.
| SL No. | Sections Where Huge Amounts of Costs Can Be Reduced | Dissolving MNs Patch | Conventional Syringes |
|---|---|---|---|
| 1. | Maintenance cost of cold chain system for storage after manufacturing vaccine | × | √ |
| 2. | Cold chain system cost during distribution of vaccine | × | √ |
| 3. | Syringes and vials’ manufacturing cost | × | √ |
| 4. | Sharp waste disposal procedure cost | × | √ |
| 5. | Plastic and glass waste management cost | × | √ |
| 6. | Training cost (training up the caregivers for syringe and vial handling, disposal, etc.) | × | √ |
Note: √ = yes, and × = no.
4. Preclinical and Stability Studies of MN Vaccination
4.1. Stability Studies of MN Vaccination
Most immunizations are currently accessible in fluid form, which must be kept refrigerated to guarantee antibody quality [342,352]. Due to this tight temperature prerequisite, immunization administration by and large utilizes a cold chain, which may be a set of temperature limitations that happen amid immunization travel, capacity, and dissemination from the point of fabricating to the point of utilization [12,87,366]. Indeed, a well-established cold chain, be that as it may, cannot guarantee immunization quality, since any accidental introduction to warmth or the unintended solidifying of immunizations amid travel and capacity can cause damage [239,249,277,361]. Due to the colossal cost of keeping up the cold chain and adapting to its issues, antibodies with thermostability that do not require refrigeration are significantly sought after [49,63,345]. Thermally steady immunizations could be distributed to populaces in nations with restricted cold-chain frameworks, and more productive and far-reaching immunization dissemination could be achieved through drugstore and mail-in techniques to combat regular and widespread episodes of maladies such as COVID-19 [233,344,355]. Table 9 shows stability studies regarding dissolving microneedles used in vaccination. Changing fluid antibodies to a dry powder frame is one approach to improve immunization toughness [232,341,350]. In terms of drying, vacuum drying, drying with a desiccant, and lyophilization are all methods of drying biopharmaceuticals such as immunizations [78,100,102]. The prescribed procedure for drying biopharmaceuticals is lyophilization [33,40,339,367]. Amid the freeze-drying process, be that as it may, the immunization particles and proteins are exposed to a number of possibly damaging stresses, including solidifying and drying stresses, which can cause changes within the antibody proteins’ auxiliary and tertiary structure as well as physical changes such as conglomeration (e.g., due to solidifying concentrations) [33,46,55,236,332]. Sugar has been utilized in studies regarding antibodies to protect immunizations against the previously mentioned types of damage during lyophilization, as often as possible within the frame of sugar glass [41,284,368,369]. In spite of the fact that the most popular way of conveying immunizations is infusion with hypodermic needles, this strategy is not favorable and our understanding of it is limited [37,67,370]. In numerous developing nations, it was assessed that more than half of all infusions are performed utilizing dangerous infusion strategies, which may be a major source of bloodborne pathogen transmission [338,368]. Microneedles, alternatives to infusion, tackle these concerns by giving a more patient-friendly and more secure conveyance strategy that infuses immunizations into the epidermis and shallow dermis layers of the skin, utilizing an easy-to-apply alternative [63,156,239,332,345]. Patients lean toward the microneedle alternative since it is easy and simple to apply, and it is more secure, since microneedles may be fabricated from secure, water-soluble excipients that break down within the skin and leave no sharp waste [46,49,55,371]. In addition, microneedle patches can be stored and dispersed in a dry, solid-state and are broken down within the skin’s interstitial liquid when utilized [63,77,345]. Further examinations have found that skin immunization is more immunogenic than muscle immunization, owing to the nearness of Langerhans and dermal dendritic cells within the skin [233,341,344]
Table 9.
Stability studies of vaccine DMAP.
| SL No. | Vaccine | Stabilizer | Temperature | Period | References |
|---|---|---|---|---|---|
| 1. | Influenza (inactivated) | Trehalose | 4 °C, 25 °C, 37 °C | 3 months | [40,69] |
| 2. | Influenza (inactivated) | Trehalose | 40 °C | 6 months | [40,69] |
| 3. | Influenza (inactivated) | Trehalose | 35 °C | 12 months | [40,69] |
| 4. | Rabies (DNA) | Sucrose | 4 °C | 3 weeks | [61,67,372] |
| 5. | Hepatitis B (recombinant subunit) | - | 4 °C | 3 months | [258,260] |
| 6. | Hepatitis B (recombinant subunit) | Sucrose | 45 °C | 6 months | [258,260] |
| 7. | Influenza (subunit) | Arginine + heptagluconate | 25 °C Freeze–thawing | 24 months5 cycles | [32,326] |
| 8. | BCG (live attenuated) | - | 25 °C | 2 months | [252] |
| 9. | Tetanus toxoid/Diphtheria toxoid (divalent subunit) | - | 4 °C | 24 weeks | [256,263] |
| 10. | Scrub typhus (recombinant subunit) | - | 25 °C | 4 weeks | [63] |
4.2. MN Patch Packaging and Storage
In a previous study [352], three alternative packing conditions were used to preserve microneedle patches carrying vaccinations [195,357,373]. The initial set of microneedle patches were put in open glass vials that were exposed to the building’s ambient air and humidity [239,351,374]. The remaining microneedle patches were put in glass vials with 1 g of desiccant (calcium sulfate, Drierite, Xenia, OH). These vials were securely capped and then parafilm-sealed. The third batch of microneedle patches was likewise packed in glass vials with desiccant and nitrogen gas instead of air [55,156,233]. Microneedle patches were kept at 4 °C in the fridge, 25 °C on a lab bench drawer, and 37 °C or 45 °C in temperature-controlled incubators [33,40,342]. At the four temperatures, fluid arrangements of inactivated flu infection in vials were kept indistinguishably with and without desiccant and oxygen [33,249,277,284,355]. After 0, 1, 7, 14, 30, 60, and 90 days, the microneedle patches and immunization arrangements were expelled, and their solidness was tested [163,355,369,370]. Table 10 shows the analytical methods used to monitor and determine the quality attributes and to test the quality attributes of mRNA vaccines.
Table 10.
Analytical methods to determine and monitor quality attributes and stability of mRNA vaccine bulk drug substance and final drug product.
| SL No. | Assay | Purpose | References |
|---|---|---|---|
| 1. | Characterizing DNA templates and RNA transcripts | ||
|
Identification of mRNA | [74,159] | |
|
Quantification—purity dependent | [203] | |
|
Quantification—purity assessment | [13] | |
|
Molecular mass, RNA integrity, and quantification | [77] | |
|
Identification and quantification of mRNA | [375] | |
|
Quality assessment | [139] | |
|
Quality assessment | [159] | |
|
Quality assessment | [13] | |
|
Quantity and quality assessment | [77] | |
| 2. | Characterizing mRNA-encoded translation products | ||
|
Translation into target protein | [156] | |
|
Translation product analysis and potential toxicity assay | [35,91] | |
| 3. | Characterizing mRNA-lipid/protein complexes | ||
|
Particle size (distribution) | [72] | |
|
Assessing bound/unbound mRNA and surface charge | [107] | |
|
Zeta potential | [77] | |
|
Quantification and integrity of carrier lipids/protein | [72] | |
|
Encapsulation efficiency | [372] | |
| 4. | General pharmaceutical tests | Appearance, pH, osmolality, endotoxin concentration, and sterility | [107] |
4.3. Preclinical Studies of Vaccine MN Array Patch
Mice were utilized in the study conducted in the article [352] to assess the viability of most immunization MAPs, whereas a monkey was utilized as an animal model in preclinical examinations of distinctive immunization MAPs [63,370]. An aluminum-type adjuvant was tested among the adjuvants; in any case, it did not illustrate high proficiency for the MAP14 immunization since it produced destitute T-cell interceded resistant reactions and was not fitting for intradermal (ID) utilization [50,63,74,202]. Nanoparticles (NPs), which can work as a station and are more effectively taken up by dendritic cells, have as of late been respected as valuable adjuvants. Bacillus anthracis inoculation NP Outlines evoked a more capable resistant reaction than an Outline without NP detailing [50,63,144,200]. Ebola immunization studies indicated a comparable advancement [63,376,377]. The Hepatitis B DNA antibody was typified in another polymer NP detailing made from pluronic-modified polyethyleneimine [63,370]. Compared to DNA MAPs, DNA NP MAPs created more prominent humoral and cellular resistance [50,63,74,202]. Utilizing an embedded Outline, the resistant reaction was upgraded by a persistent discharge of inoculation and antigen presentation to lymphoid organs [140,145,325,377]. The silk network was utilized to form a D-MAP for HIV that controlled the antigen discharge rate for two weeks, occurring in a 1300-fold increment in serum IgG titer compared to a conventional organization [33,203,303,368]. The chitosan Outline, which has an immune-enhancing impact, was utilized to extend the discharge of flu inoculation [33,97,140,156,200,325,376].
5. Microneedle Array Patch Vaccination: Clinical Trials and Human Studies
5.1. Microneedle Vaccination Clinical Trials
To address the limits and present drawbacks of hypodermic needle injection, vaccines can incorporate MAP’s innovation in stability, bioavailability, potency, and less adverse effects [74,150,208]. Using the keyword “microneedle vaccination” as a search term, seven studies were discovered on Clinical Trial.gov that used the vaccine MAP. In the registered trials, many types of MAPs were employed, and these studies were performed to assess the viability of MAP vaccination in clinical practice for some of the most severe infectious illnesses [22,68,83,208].
5.2. Vaccine Coated MN Array for Human Studies
In multiple human trials, C-MAP (NanopatchTM), a vaccine, has shown promise as a technique for effective drug delivery [63]. In a previous study [63], uncoated and excipient-coated NanopatchTM vaccines were given to 18 healthy persons for 2 min of insertion and removal [33,368,370]. On a scale of 0 to 10, 78 percent of participants reported 0 on a pain range of 0 to 10, with an average score of less than 1 on a pain scale of 0 to 10 [58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,265,266,267,268,269,270,271,272,273,274,275,276,277,278,279,280,281,282,283,284,285,286,287,288,289,290,291,292,293,294,295,296,297,298,299,300,301,302,303,304,305,306,307,308,309,310,311,312,313,314,315,316,317,318,319,320,321,322,323,324,325,326,327,328,329,330,331,332,333,334,335,336,337,338,339,340,341,342,343,344,345,346,347,348,349,350,351,352,353,354,355,356,357,358,359,360,361,362,363,364,365,366,367,368,369,370,371,372,373]. NanopatchTM had no unexpected adverse effects, and the expected erythema response faded between three and seven days after vaccination [56,61,249]. When healthy people were administered a NanopatchTM containing 15 g of inactivated influenza virus (H1N1), the side effects were low to moderate, and more than half of the people (55%) preferred the NanopatchTM method over intramuscular injection (IM) [58,209,249]. Interestingly, when employing a NanopatchTM, the antibody response was comparable to when using standard IM injection [33,56,61,368,370,373].
5.3. Vaccine Dissolvable MAP for Human Studies
There was no pain, edema, or erythema when research participants in a number of studies [63,326,368] were administered a D-MAP patch, and only mild erythema was restricted to the patch application site [35,326]. Furthermore, the great majority of participants were either somewhat or totally confident in their ability to self-administer [35,50,290,326]. As a consequence, D-MAPs were given to participants in a phase 1 research after the influenza vaccine was encapsulated in a polymer matrix [33,35,38,340]. The D-MAP that was self-administered generated antibody responses that were comparable to IM therapy [51,260,354]. Another D-MAP for the treatment of influenza was created using MicroHyala TM, a hyaluronic acid MAP [63,64]. There were hardly any significant local or systemic adverse effects, and the immunological efficacy was comparable to IM [41,43,284].
5.4. Concerns about Vaccination via MAP
5.4.1. Commercialized MAP
A few pharmaceutical companies have developed MAP devices for medication delivery systems. These companies are summarized in Table 11. OnvaxTM (a BD business) is made up of a series of plastic microprojections that stand about 200 micrometers tall [222,353]. The vaccine is transported into the epidermal layer as a result of the skin injury induced by such devices [33,43,63,326]. Vaxxas created NanopatchTM, which is a strong power microprojection grid with an influenza vaccine composition on top [50,222,353]. A spring-loaded applicator is used to apply a 250 m long NanopatchTM needle. The ZP MAP system from Zosano Pharma contains 1300 microneedles distributed out across a 2 cm2 area [36,46,63,232]. The medicine is deposited on a 190 m MAP and given through a refillable arm applicator. This technique accomplishes the intended outcome by delivering the drug formulation to the skin’s outer layers. CosMED Pharmaceutical Ltd. created a D-MAP that is built on hyaluronic acid [222,353].
Table 11.
Companies developing microneedles for vaccine delivery.
| SL No. | Company | Type of Microneedle | Disease |
|---|---|---|---|
| 1. | Micron Biomedical | Dissolving microneedle | Inactivated rotavirus |
| 2. | 3M (Kindeva) | Hollow microneedle | Cancer vaccines |
| 3. | BD Technologies (BS Soluvia) | Stainless steel microneedle | Influenza |
| 4. | Flugen | Metal microneedles | Influenza |
| 5. | Debiotech | Hollow microneedles | COVID-19 |
| 6. | Vendari (Vaxipatch) | Stainless steel microneedle | Influenza and COVID-19 |
| 7. | Nanopass (MicrojetTM) | Silicon microneedles | Influenza, Polio, Varicella-Zoster, cancers, Hepatitis B, and COVID-19 |
| 8. | BioSeren Tach Inc. | Dissolving microneedles | Vaccine |
| 9. | Sorrento Therapeutics (Solusa) | Nanotopographical imprinted microneedles (coated) | Immuno-oncology |
| 10. | Vaxxas (NanopatchTM) | Coated microneedles array patch | Influenza, COVID-19 |
| 11. | Quadmedicine | Dissolving microneedles | Influenza, Canine Influenza |
| 12. | Vaxess | Dissolving microneedles | Influenza, COVID-19, and skin cancer |
| 13. | Raphas | Dissolving microneedles | HPV, Polio, T dap, HBV, IPV, and Hepatitis B |
5.4.2. Manufacturing Issues
Dosage consistency, reasonable price, mass fabricating, and manufacturing in agreement with GMP benchmarks are all concerns in attaining successful DMN vaccination procedures [44,55,222]. In terms of cost and versatility, MAPs require the foundation of large-scale fabricating apparatus and methods [43,58,276,324]. At the beginning of mass generation, noteworthy use is required to manufacture, cast, and shape MAPs [32,68]. Once these early stages are complete, the fabrication expenses of DMNs are anticipated to be lower than that of injectables [32,33,37,46,50]. The polymer-based MAP casting technique might be low-cost since different polymers, such as cellulose derivatives, engineering plastics, and sugars, are typically affordable [41,46,66,304,369]. Scaling up handling processes, however, can be challenging due to the reliance on master molds and the necessary multi-step filling process [50,56,69,225]. Additionally, temperatures may rise due to the drying process utilized in the manufacturing of vaccine MAP [63,254,378,379]. As a result, making thermosensitive antigens may need a low-temperature technique. Special packaging or desiccants may be required to improve storage stability, although the addition of moisture-resistant material may increase package prices [36,233,236]. In addition, sterilization is essential for MAP immunization. Despite MAP’s low bioburden, the cost of the aseptic technique should be considered. The assessment of immunization MAP products should be considered in terms of cost [33,251,326]. The consistency of MAPs is also necessary for quality assurance in the marketing and production processes. Companies must establish and execute an effective pharmaceutical quality assurance system that combines GMPs and quality risk management [63,145,249]. Ultimately, for effective vaccine MAP production, current standards for conventional medications, as well as specific needs for each type of MAP, are necessary [33,63,326].
5.4.3. Regulatory Issues
An immunization Outline, agreeing to the latest report from the US Food and Drug Administration (FDA), could be an item that combines an organic item with a mechanical device [78,116,376,377]. Two or more administrative units such as the organic item and the mechanical device are combined to make up an item. This sort of item incorporates prefilled syringes, autoinjectors, and Outline patches preloaded with natural items (21 CFR 3.2e) [9,156,158,175,305]. Due to the benefits of Outline, an inoculation Outline has been focused on. Antibody and Outline were combined into one commerce [88,305,372]. The security and viability concerns related to each constituent portion and the item as an entirety ought to be considered within the direction of an immunization Outline (21 CFR Portion 4 Subpart A: Section 4.4 (b)). To move from the research facility to clinical utilization, an immunization Outline must moreover meet current GMP and post-marketing security benchmarks [61,88,163,305,370,378].
6. Challenges in Ensuring Global Access to COVID-19 Vaccines and Socio-Economic Factors
6.1. Vaccine Hesitancy
Vaccine hesitancy is defined as the delay in receiving or the refusal to receive vaccines in spite of the availability of a vaccine facility [379]. The severity of the COVID-19 pandemic cannot be minimized until communities agree to get vaccinated [380]. According to some researchers, people who prefer to receive complementary and alternative medicines (CAMs) are more prone to become vaccine hesitant [381].
In this ongoing pandemic, one of the reasons people are showing hesitancy towards the vaccine is that the COVID-19 vaccine development time period was faster than usual [153]. This has led to a fearful doubt regarding the long-term effect of the vaccine [82].
Despite this, reasons for vaccine hesitancy may vary according to country, socio-economic factors, one’s confidence towards the vaccine, and other factors [152,382]. Moreover, a lack of proper vaccination campaigning, ignorance of vaccination, and media communication have a substantial effects on people [148,205,383,384,385]. Numerous surveys have been carried out to identify the exact reason for vaccine hesitancy, and each of them included a considerable number of participants who lacked knowledge concerning the COVID-19 vaccine [5,81,89,386,387]. Media coverage regarding the adverse effect of AstraZeneca’s vaccine also led many people towards vaccine hesitancy [116,385].
To tackle the growing percentage of vaccine hesitancy during the COVID-19 pandemic, the first and foremost step is to increase awareness among the public. This involves disseminating information, educating people about the importance of vaccines, and fighting disinformation with scientific-data-based information [130,148].
Researchers have suggested the five Cs strategy to combat vaccine hesitancy, which covers: 1. Confidence, 2. Complacency, 3. Convenience, 4. Communications, and 5. Context [151].
MNs can play a vital role in reducing the percentage of vaccine-hesitant people worldwide. Because it is now proven that delivery through MNs can increase the effectiveness of a medication, not only that will lead to confidence in vaccine-hesitant people, but it also has the potential to deal with the other four components of the five Cs (see Figure 12).
Figure 12.
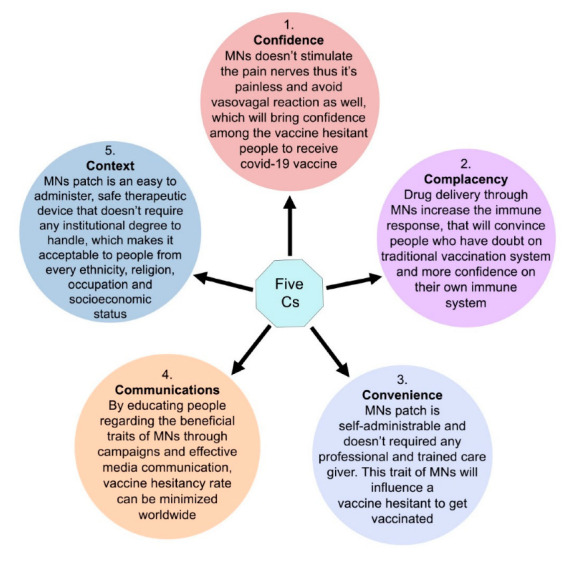
Role of MNs in dealing with vaccine hesitancy.
6.2. Needle Phobia
A needle phobia can be defined as the intense fear of medical approaches that involve needles or injections, to such extent where it causes a transformed and unaccommodating response [388]. The intensity of this phobia can reach to an extent where a patient might even refuse to accept life-saving medical help [389].
A needle-phobic human usually goes through a series of phenomena, initially starting with anxiety-associated tachycardia, and subsequently bradycardia, hypotension, diaphoresis, and shock. Eventually, all these incidents can lead a needle-phobic towards vasovagal syncope. Unfortunately, this fear of vasovagal syncope leads a treatment receiver to experience more severe needle-phobic responses than usual [389,390,391]. All these medical conditions discourage people with needle phobias to get vaccinated despite the long-term beneficial effect of vaccines.
To convince people with needle phobias to get vaccinated, the following methods could be applied:
1. Desensitization: Desensitization therapy is the most commonly applied and effective; however, it is a time-consuming technique that requires hours of compliance. In this therapy, the patient is steadily exposed to needles in a regulated and circumspect setting that eventually helps the needle-phobic to allow themselves to handle needles [390,392].
2. Topical anesthetics: The use of topical anesthetics before the administration of transdermal medications is the best possible method in the management of needle phobias, which can temporarily solve the associated issues within the shortest possible time. Local anesthetics that are cream-based mixtures have shown more efficacy in the management of needle phobias [389,393].
3. Vaccination through MNs: MNs have become popular therapeutic devices [36] for vaccine delivery due to their distinctively unique advantages [14], which can play a paramount part in alleviating the fear of needles in people. MNs are tiny, micron-sized needles that deliver the drug molecule by creating microchannels through the stratum corneum [46,364] without stimulating pain nerves [360,394]. They can penetrate the skin without pain and vasovagal reactions, making them a suitable transdermal delivery system for needle-phobic people [31,47,395].
6.3. Availability
As it has already been almost 2 years since the beginning of the COVID-19 pandemic and only 10.91% of people have been fully vaccinated as of 1 June 2021 [396], it is a challenge to fully vaccinate the rest of the 89.09% unvaccinated people (Figure 13) worldwide in spite of the remarkably rapid development of COVID-19 vaccines.
Figure 13.

Percentage of unvaccinated people worldwide as of 1 June 2021.
Based on the report of an internal investigation, the amount of vaccines supplied altogether by 37 members of the DCVMN (Developing Countries Vaccine Manufacturers Network) was about 3.5 billion doses annually [95].
According to the latest published article on 9 June, around 20 million people per day had been getting a vaccine shot manufactured by Sinopharm and Sinovac in China [397].
AstraZeneca agreed to deliver 3 billion doses of its vaccine this year; however, it was only able to deliver 40 million of the 90 million doses it had promised to provide the European Union (EU) for the first quarter of 2021 [398]. Figure 14 depicts a general estimation of the COVID-19 vaccine manufacturing capacity of leading manufacturers worldwide by the end of 2021.
Figure 14.

Manufacturing capacity by end of 2021 of lead companies producing COVID-19 vaccines. (Vaccine courses are assumed to require two doses) [399].
The COVID-19 pandemic has given rise to a humanitarian crisis throughout the world. Developing and underdeveloped countries have always been at the bottom of the priority list in the case of both technological and medical advancements, which also include vaccines and drugs [130]. For instance, the world’s poorest nations in Africa only received 0.2% of the 700 million COVID-19 vaccine doses by April 2021, whereas more than 87% of the global vaccine doses has been supplied to developed countries [176].
However, a variety of agreements with manufacturers has been launched by the COVAX Facility regarding the supply of COVID-19 vaccines, which it believes will be sufficient enough to hit its target of producing two billion doses by the end of 2021, around 50 percent of which will be reserved for distribution in developing countries [400]. Canada, France, Norway, and the UK have agreed to donate leftover vaccines from their national vaccination campaigns [398].
The pervasiveness of vaccine nationalism is a barrier to equitable vaccine distribution [400].
In an endeavor to reconcile the different perspectives, some people think that no conflict exists in terms of an even distribution of vaccines and national partiality. Having said that, it is not allowed to violate civil rights and aggravate the worldwide poverty situation. Furthermore, it is both the right and duty of each government to ensure their citizens get priority access to the COVID-19 vaccine [127].
Available Vaccines and Variants of Concern
SARS-CoV-2 is susceptible to genetic evolution that results in multiple variants that possibly have distinct characteristics in comparison to its hereditary strains. In the past year, multiple variants of SARS-CoV-2 have been originated, of which a few are considered to be a variants of concern (VOCs) [401] because of their potential to cause enhanced virulence, reduced naturalizing capacity by the help of innate immunity or vaccination, the ability to elude the detection, or the decreased effectiveness of therapeutics or vaccination [136]. Each EUA vaccine available on the market evinces a different potency and time span of effectiveness depending on the design of antigen, adjuvant molecules, vaccine delivery platforms, and immunization technique [114]. The efficacy of EUA vaccines present on the market for the different variants is as follows:
BNT162b2 vaccine: The roughly calculated effectiveness of the BNT162b2 vaccine was 89.5% (95% confidence interval (CI), 85.9 to 92.3) and 75.0% (95% CI, 70.5 to 78.9), against infection with the B.1.1.7 and B.1.351 variant, respectively, at the 14th or more day after the administration of the second dose [84,101,103,402,403,404]. BNT162b2 efficiently neutralized all SARS-CoV-2 variants in the in vitro analysis of 20 serum samples attained from 15 participants from the BNT162b2 clinical efficacy trial. The neutralization of the B.1.1.7 variant and P.1 was unceremoniously identical. The neutralization of B.1.351 was stronger but lower compared to the hereditary strain of SARS-CoV-2 [109,401,405].
Ad26.COV2.S vaccine: A single course of the vaccine offers protection from the P.2 and B.1.135 variants of COVID-19, though data have not been reported yet. It is notable that the efficacy [406] of the vaccine in the US was higher by a factor of 1.3 in comparison to South Africa, which was 72% and 57%, respectively [407].
mRNA-1273 vaccine: The percentage of effectiveness of the mRNA-1273 vaccine against the SARS-CoV-2 variants is not clear yet [27,167,169,408]. The in vitro experiment of serum samples collected from members who participated in the mRNA-1273 vaccine’s clinical efficacy trial shows that the mutations affecting the receptor-binding domain (RBD) of the B.1.1.7 strain had no remarkable effect on neutralization by serum collected from participants who received the mRNA-1273 vaccine. On the contrary, the analysis also demonstrated a reduction in titers of neutralizing antibodies against the B.1.351, B.1.1.7 + E484K, P.1, and B.1.427/B.1.429 variants. The decrease in neutralizing titers was notably lower in the B.1.351 variant [409].
ChAdOx1 nCoV-19 vaccine: A two-course [410] unit of the ChAdOx1 nCoV-19 vaccine did not give protection against the B.1.351 variant by low to moderate COVID-19 SARS-CoV-2 vaccines, according to the obtained data from a double-blind, multicenter, randomized control trial with a total of 33725432 participants. Data from another randomized control trial in regard to the ChAdOx1 nCoV-19 vaccine demonstrated that in vitro neutralization activity against the B.1.1.7 variant was decreased in comparison to a non-B.1.1.7 variant, and the clinical effectiveness of the vaccine was 70.4% and 81.5% for B.1.1.7 and non-B.1.1.7 variants, respectively [86,171].
The spike (S) protein of SARS-CoV-2 plays a vital role in the receptor recognition and cell membrane fusion process [336]. The fundamental role of the S protein in viral infection indicates that it is a potential target for vaccine development, antibody-blocking therapy, and small-molecule inhibitors (see Figure 15). Vaccines targeting various SARS-CoV-2 proteins are under development [198].
Figure 15.

Different targets for vaccine development (picture taken and modified from [114].
The mutation of the aspartate (D) at position 614 to glycine (G614) results in an intensified infective strain of SARS-CoV-2 [3,411,412], which makes it more difficult to develop antibodies or vaccines that target non-conservative regions.
To effectively prevent disease, combinations of different mAbs that identify different epitopes on the SARS-CoV-2 S surface can be assessed to neutralize a wide range of isolates, including escape mutants [413].
To avoid severe adverse events in safe and effective vaccine development, preclinical trials play a crucial role, which need to be carried out with caution. Furthermore, international organizations i.e., the WHO, CEPI, GAVI, and the Bill and Melinda Gates Foundation, need to be more cooperative with each other to ensure generous funding for vaccine development [140].
6.4. Affordability
Self-procuring middle-income countries are buying EUA (Emergency Use Authorization) vaccines with the median value of USD 5.30 (IQR 0.79–18.30), and self-procuring high-income countries are buying EUA vaccines with the median value of USD 16.3 (IQR 6.5–22.0) [153].
Countries covered by Gavi (Global Alliance for Vaccines and Immunization), which is a major buyer of vaccines for low-income countries, have paid the lowest prices per dose median value of USD 0·57 (IQR 0.16–1.90), followed by countries covered by UNICEF with the median value of USD 0.80 (IQR 0.16–2.80) and the Pan American Health Organization (PAHO) with the median value of USD 3.50 (IQR 0.87–13.0). The premarket purchasing costs of EUA vaccines (see Table 12) currently account for pandemic pricing, which might be changing [153].
Table 12.
Overview of leading companies with premarket price range [399].
| SL No. | Company | Current R&D Stage | Price Range per Course |
Platform Technology |
|---|---|---|---|---|
| 1. | AstraZeneca/Oxford University | Phase II/III | USD 6-USD 8 | Non-replicating viral vector |
| 2. | Pfizer/BioNTech | USD 37-USD 39 | mRNA | |
| 3. | Johnson & Johnson/Janssen | Phase III | USD 20 | Non-replicating viral vector |
| 4. | Moderna | USD 30-USD 74 | mRNA | |
| 5. | Novavax | USD 6-USD 32 | Protein subunit | |
| 6. | SinoVac | Undisclosed | Inactivated |
7. Discussion
Preclinical studies of the vaccine MAP have employed animal models ranging from rodents to primates. The MAP approach has been used to test a variety of vaccines, including novel outbreak pandemic vaccines, and has been demonstrated to elicit equal or superior immune responses when compared to IM and other immunization techniques. Clinical tests have been conducted to determine the vaccine MAP’s stability, safety, and immunological efficacy, with good and comparable results when compared to IM administration. However, difficulties such as mass manufacturing, pricing, an aseptic process, and reproducible quality remain. Because vaccine microneedles are an immunization product, the same standards that apply to vaccine manufacturing processes also apply to vaccine microneedle production. As a result, developing the final clinical outcome of vaccine microneedles will take a while. A suitable immunization MAP injector, as well as extra vaccine MAP packaging, are additional cost considerations. Several microneedle manufacturers with large-scale capabilities, on the other hand, have already partnered with vaccine makers to generate vaccine MAPs, with improved immunological results reported. If the restrictions mentioned above are solved, several vaccines will be combined into a microneedle system and given using MAPs. MAPs, as well as syringes and needles, will be used. In the near future, they will be used as a vaccine delivery method.
The benefits of DMN vaccination include dose reduction, painless immunization, and the avoidance of needle injuries. Furthermore, by increasing vaccine stability, lowering vaccine waste, and minimizing the burden on trained personnel, it has the potential to enhance vaccination coverage in disadvantaged countries. Therefore, many more advances in different areas of DMN development are needed before regulatory approval and commercial scale-up can be accomplished.
Fabrication methods must be enhanced even further to ensure minimal antigen loss, which is often promised but seldom verified in the literature and has yet to be shown on a standard laboratory level of output. Analytical challenges include potency testing and stability testing during production and storage, as well as the quantification and repeatability of antigen/adjuvant dose administered in the skin. Furthermore, the relevance of the applicator device should not be disregarded, as it has the potential to standardize DMN administration and vaccine dispersion into the skin, whereas manual application is preferred in logistical situations. DMN immunization exhibited comparable or higher antibody and cellular responses in preclinical studies than conventional vaccinations. Furthermore, cellular immune responses were evoked more strongly by sustained antigen release from nanoparticles or cross-linked structures in DMNs than by fast release from DMNs or liquid solution. While prolonged DMN delivery did not enhance the immune responses any more than rapid DMN release, further study is needed to back up this conclusion. To enhance DMN vaccination, further systematic study, such as the discovery of optimal adjuvants and the evaluation of the impact of DMN geometry, may be necessary in the future. Although the ideal DMN patch has yet to be found, substantial progress has been made. To transform DMNs into products that are safe, effective, inexpensive, and widely used, more testing is needed. To get microneedles on the market, the proper type of microneedle must be selected for (trans)dermal drug delivery (e.g., hollow, solid, geometry, material, density, and length). Microneedle application devices should also be used to provide adequate and reproducible punctures, as well as the ability to self-administer. Consequently, for each kind of vaccine formulation, new microneedle-based solutions for (trans)dermal drug administration should comprise the medicine, a stable vaccine formulation, appropriate microneedles, and a microneedle application device all in one package. Microneedle-based skin vaccination has been proven to be more dose-effective than traditional intramuscular and subcutaneous immunization in both human and animal studies. Various microneedle-based drug-delivery techniques have been used to deliver therapeutic proteins; however, protein structure was only partially explored in the articles listed above. Nothing is known about the immunological side effects of microneedle-based protein delivery. Protein structure preservation is significantly more important for therapeutic proteins than it is for vaccines during manufacture, storage, and use. Any reshaping of novel therapeutics, for example, might diminish drug efficacy while simultaneously compromising safety. However, undesirable immunogenicity may result in the full loss of a protein’s therapeutic effect owing to neutralizing antibodies, the depletion of endogenous proteins, or the collapse of the immune regulation to self-antigens. Because the skin is such a powerful immunologic organ, the latter is perhaps the most severe safety issue. This emphasizes the need to thoroughly analyze protein aggregates and subvisible particles that may be present in and released from transdermal microneedle-based formulations, since they are known to be major risk factors for undesired protein immunogenicity. However, no reports regarding the undesired immunogenicity of therapeutic protein delivery by microneedles have been published to our knowledge, and research in this area is critically needed to advance this field. This necessitates a thorough examination of protein structure in order to ensure its integrity throughout manufacturing and release, as well as immunogenicity tests in appropriate animal models. The microneedle array patch vaccines are still undergoing stability testing, although there is evidence in the literature that vaccine components, including proteins, are stable. Integration into the matrix of the polymers used in the microneedle array patch is usually used to stabilize the product, and as shown by maintenance, maintain their conformational configurations binding role of antibodies. At 25 °C, recombinant adenovirus vaccinations maintained their immunogenicity for at least a month. As a result, the vaccines delivered via the dissolvable microneedles array patch could minimize the expenses associated with the distribution and delivery of vaccines that require extreme low temperatures to maintain their viability e.g., the mRNA-based formulation in the coronavirus vaccines. Overall, microneedle-based (trans)dermal drug delivery may have a significant influence on future medicine, both for COVID-19 vaccination and for therapeutic drug delivery.
8. Conclusions
The use of dissolving microneedles for transdermal drug delivery has gained a lot of attention. This is because these devices can include medicines in polymeric matrices that break down in the skin when applied, releasing chemicals that are then delivered into the bloodstream. The requirement to impart mechanical strength while enabling rapid start of action, depending on the individual chemical being delivered, drives the diversity of designs. Micro-molding is the most common manufacturing technology, while drawing lithography and droplet-born air blowing (DAB) are becoming more popular. In this review, the progress achieved in several laboratories on the use of dissolving microneedles for the transdermal administration of a wide range of vaccinations for various illnesses was presented, including the possibility for mass immunization for COVID-19. The greatest advancements are always created at the most critical periods of adversity. Hence, to defeat this pandemic and to keep it under our control, the entire idea of mass vaccination might change due to the implementation of dissolvable microneedles for COVID-19 vaccination. Ideally, this novel vaccine delivery system will have a global outreach, and billions of people will be vaccinated to finally attain herd immunity.
Author Contributions
Conceptualization, M.J.U. and D.B.D.; resources, M.J.U. and D.B.D.; writing—original draft preparation, J.H., C.H. and T.A.; writing—review and editing, J.H., C.H., T.A., M.J.U. and D.B.D.; supervision, M.J.U. and D.B.D.; project administration, M.J.U. and D.B.D.; funding acquisition, M.J.U. and D.B.D. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
There are no additional raw data for this paper. The paper only uses secondary data from published papers, and all credits to these data have been made via citations and copyright permissions.
Conflicts of Interest
The authors declare no conflict of interest.
Funding Statement
This research received no external funding.
Footnotes
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Der Li Y., Chi W.Y., Su J.H., Ferrall L., Hung C.F., Wu T.C. Coronavirus Vaccine Development: From SARS and MERS to COVID-19. J. Biomed. Sci. 2020;27:104. doi: 10.1186/s12929-020-00695-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gaziano L., Giambartolomei C., Pereira A.C., Gaulton A., Posner D.C., Swanson S.A., Ho Y.L., Iyengar S.K., Kosik N.M., Vujkovic M., et al. Actionable Druggable Genome-Wide Mendelian Randomization Identifies Repurposing Opportunities for COVID-19. Nat. Med. 2021;27:668–676. doi: 10.1038/s41591-021-01310-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Korber B., Fischer W.M., Gnanakaran S., Yoon H., Theiler J., Abfalterer W., Hengartner N., Giorgi E.E., Bhattacharya T., Foley B., et al. Tracking Changes in SARS-CoV-2 Spike: Evidence That D614G Increases Infectivity of the COVID-19 Virus. Cell. 2020;182:812–827.e19. doi: 10.1016/j.cell.2020.06.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Baker D., Roberts C.A.K., Pryce G., Kang A.S., Marta M., Reyes S., Schmierer K., Giovannoni G., Amor S. COVID-19 Vaccine-Readiness for Anti-CD20-Depleting Therapy in Autoimmune Diseases. Clin. Exp. Immunol. 2020;202:149–161. doi: 10.1111/cei.13495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sun S., Lin D., Operario D. Interest in COVID-19 Vaccine Trials Participation among Young Adults in China: Willingness, Reasons for Hesitancy, and Demographic and Psychosocial Determinants. Prev. Med. Rep. 2021;22:101350. doi: 10.1016/j.pmedr.2021.101350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Redhead M.A., Owen C.D., Brewitz L., Collette A.H., Lukacik P., Strain-Damerell C., Robinson S.W., Collins P.M., Schäfer P., Swindells M., et al. Bispecific Repurposed Medicines Targeting the Viral and Immunological Arms of COVID-19. Sci. Rep. 2021;11:13208. doi: 10.1038/s41598-021-92416-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jeong H.J., Min S., Chae H., Kim S., Lee G., Namgoong S.K., Jeong K. Signal Amplification by Reversible Exchange for COVID-19 Antiviral Drug Candidates. Sci. Rep. 2020;10:14290. doi: 10.1038/s41598-020-71282-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Güven M., Gültekin H. The Effect of High-Dose Parenteral Vitamin D3 on COVID-19-Related Inhospital Mortality in Critical COVID-19 Patients during Intensive Care Unit Admission: An Observational Cohort Study. Eur. J. Clin. Nutr. 2021;75:1383–1388. doi: 10.1038/s41430-021-00984-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yang B., Fan J., Huang J., Guo E., Fu Y., Liu S., Xiao R., Liu C., Lu F., Qin T., et al. Clinical and Molecular Characteristics of COVID-19 Patients with Persistent SARS-CoV-2 Infection. Nat. Commun. 2021;12:3501. doi: 10.1038/s41467-021-23621-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ita K. Coronavirus Disease (COVID-19): Current Status and Prospects for Drug and Vaccine Development. Arch. Med. Res. 2021;52:15–24. doi: 10.1016/j.arcmed.2020.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cantudo-Cuenca M.D., Gutiérrez-Pizarraya A., Pinilla-Fernández A., Contreras-Macías E., Fernández-Fuertes M., Lao-Domínguez F.A., Rincón P., Pineda J.A., Macías J., Morillo-Verdugo R. Drug–Drug Interactions between Treatment Specific Pharmacotherapy and Concomitant Medication in Patients with COVID-19 in the First Wave in Spain. Sci. Rep. 2021;11:12414. doi: 10.1038/s41598-021-91953-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Prieto Curiel R., González Ramírez H. Vaccination Strategies against COVID-19 and the Diffusion of Anti-Vaccination Views. Sci. Rep. 2021;11:6626. doi: 10.1038/s41598-021-85555-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wang J., Peng Y., Xu H., Cui Z., Williams R.O., III The COVID-19 Vaccine Race: Challenges and Opportunities in Vaccine Formulation. AAPS PharmSciTech. 2020;21:225. doi: 10.1208/s12249-020-01744-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Korkmaz E., Balmert S.C., Sumpter T.L., Carey C.D., Erdos G., Falo L.D. Microarray Patches Enable the Development of Skin-Targeted Vaccines against COVID-19. Adv. Drug Deliv. Rev. 2021;171:164–186. doi: 10.1016/j.addr.2021.01.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Spencer A.J., McKay P.F., Belij-Rammerstorfer S., Ulaszewska M., Bissett C.D., Hu K., Samnuan K., Blakney A.K., Wright D., Sharpe H.R., et al. Heterologous Vaccination Regimens with Self-Amplifying RNA and Adenoviral COVID Vaccines Induce Robust Immune Responses in Mice. Nat. Commun. 2021;12:2893. doi: 10.1038/s41467-021-23173-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brady E., Oertelt-prigione S. Lack of consideration of sex and gender in COVID-19 clinical studies. Nat. Commun. 2021;12:4015. doi: 10.1038/s41467-021-24265-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rahman M.M., Bodrud-Doza M., Griffiths M.D., Mamun M.A. Biomedical Waste amid COVID-19: Perspectives from Bangladesh. Lancet Glob. Health. 2020;8:e1262. doi: 10.1016/S2214-109X(20)30349-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Xu S., Liu Y., Ding Y., Luo S., Zheng X., Wu X., Liu Z., Ilyas I., Chen S., Han S. The Zinc Fi Nger Transcription Factor, KLF2, Protects against COVID-19 Associated Endothelial Dysfunction. Signal Transduct. Target. Ther. 2021;6:266. doi: 10.1038/s41392-021-00690-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.World Bank Fast-Tracks $100 Million COVID-19 (Coronavirus) Support for Bangladesh. [(accessed on 18 July 2021)]. Available online: https://www.worldbank.org/en/news/press-release/2020/04/03/world-bank-fast-tracks-100-million-covid-19-coronavirus-support-for-bangladesh.
- 20.Watson O.J., Alhaffar M., Mehchy Z., Whittaker C., Akil Z., Brazeau N.F., Cuomo-Dannenburg G., Hamlet A., Thompson H.A., Baguelin M., et al. Leveraging Community Mortality Indicators to Infer COVID-19 Mortality and Transmission Dynamics in Damascus, Syria. Nat. Commun. 2021;12:2394. doi: 10.1038/s41467-021-22474-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Banerji A., Wickner P.G., Saff R., Stone C.A., Robinson L.B., Long A.A., Wolfson A.R., Williams P., Khan D.A., Phillips E., et al. mRNA Vaccines to Prevent COVID-19 Disease and Reported Allergic Reactions: Current Evidence and Suggested Approach. J. Allergy Clin. Immunol. Pract. 2021;9:1423–1437. doi: 10.1016/j.jaip.2020.12.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kim J.H., Marks F., Clemens J.D. Looking beyond COVID-19 Vaccine Phase 3 Trials. Nat. Med. 2021;27:205–211. doi: 10.1038/s41591-021-01230-y. [DOI] [PubMed] [Google Scholar]
- 23.Le B.L., Andreoletti G., Oskotsky T., Vallejo-Gracia A., Rosales R., Yu K., Kosti I., Leon K.E., Bunis D.G., Li C., et al. Transcriptomics-Based Drug Repositioning Pipeline Identifies Therapeutic Candidates for COVID-19. Sci. Rep. 2021;11:12310. doi: 10.1038/s41598-021-91625-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lu L., Zhang H., Zhan M., Jiang J., Yin H., Dauphars D.J., Li S.Y., Li Y., He Y.W. Antibody Response and Therapy in COVID-19 Patients: What Can Be Learned for Vaccine Development? Sci. China Life Sci. 2020;63:1833–1849. doi: 10.1007/s11427-020-1859-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dispinseri S., Secchi M., Pirillo M.F., Tolazzi M., Borghi M., Brigatti C., De Angelis M.L., Baratella M., Bazzigaluppi E., Venturi G., et al. Neutralizing Antibody Responses to SARS-CoV-2 in Symptomatic COVID-19 Is Persistent and Critical for Survival. Nat. Commun. 2021;12:6–17. doi: 10.1038/s41467-021-22958-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Saha S. Coming to Terms with COVID-19 Personally and Professionally in Bangladesh. Lancet Glob. Health. 2021;9:e1471–e1473. doi: 10.1016/S2214-109X(21)00227-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.DiPiazza A.T., Leist S.R., Abiona O.M., Moliva J.I., Werner A., Minai M., Nagata B.M., Bock K.W., Phung E., Schäfer A., et al. COVID-19 Vaccine MRNA-1273 Elicits a Protective Immune Profile in Mice That Is Not Associated with Vaccine-Enhanced Disease upon SARS-CoV-2 Challenge. Immunity. 2021;54:1869–1882.e6. doi: 10.1016/j.immuni.2021.06.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rahi M., Sharma A. Mass Vaccination against COVID-19 May Require Replays of the Polio Vaccination Drives. EClinicalMedicine. 2020;25:100501. doi: 10.1016/j.eclinm.2020.100501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Usherwood T., LaJoie Z., Srivastava V. A Model and Predictions for COVID-19 Considering Population Behavior and Vaccination. Sci. Rep. 2021;11:12051. doi: 10.1038/s41598-021-91514-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Yang J., Marziano V., Deng X., Guzzetta G., Zhang J., Trentini F., Cai J., Poletti P., Zheng W., Wang W., et al. Despite Vaccination, China Needs Non-Pharmaceutical Interventions to Prevent Widespread Outbreaks of COVID-19 in 2021. Nat. Hum. Behav. 2021;5:1009–1020. doi: 10.1038/s41562-021-01155-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Amani H., Shahbazi M.A., D’Amico C., Fontana F., Abbaszadeh S., Santos H.A. Microneedles for Painless Transdermal Immunotherapeutic Applications. J. Control. Release. 2021;330:185–217. doi: 10.1016/j.jconrel.2020.12.019. [DOI] [PubMed] [Google Scholar]
- 32.Koutsonanos D.G., Vassilieva E.V., Stavropoulou A., Zarnitsyn V.G., Esser E.S., Taherbhai M.T., Prausnitz M.R., Compans R.W., Skountzou I. Delivery of Subunit Influenza Vaccine to Skin with Microneedles Improves Immunogenicity and Long-Lived Protection. Sci. Rep. 2012;2:357. doi: 10.1038/srep00357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Vrdoljak A., Allen E.A., Ferrara F., Temperton N., Crean A., Moore A.C. Induction of Broad Immunity by Thermostabilised Vaccines Incorporated in Dissolvable Microneedles Using Novel Fabrication Methods. J. Control. Release. 2016;225:192–204. doi: 10.1016/j.jconrel.2016.01.019. [DOI] [PubMed] [Google Scholar]
- 34.Panda A., Sharma P.K., McCann T., Bloomekatz J., Repka M.A., Murthy S.N. Fabrication and Development of Controlled Release PLGA Microneedles for Macromolecular Delivery Using FITC-Dextran as Model Molecule. J. Drug Deliv. Sci. Technol. 2021;68:102712. doi: 10.1016/j.jddst.2021.102712. [DOI] [Google Scholar]
- 35.Koh K.J., Liu Y., Lim S.H., Loh X.J., Kang L., Lim C.Y., Phua K.K.L. Formulation, Characterization and Evaluation of MRNA-Loaded Dissolvable Polymeric Microneedles (RNApatch) Sci. Rep. 2018;8:11842. doi: 10.1038/s41598-018-30290-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Jeong S.Y., Park J.H., Lee Y.S., Kim Y.S., Park J.Y., Kim S.Y. The Current Status of Clinical Research Involving Microneedles: A Systematic Review. Pharmaceutics. 2020;12:1113. doi: 10.3390/pharmaceutics12111113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.McGrath M.G., Vucen S., Vrdoljak A., Kelly A., O’Mahony C., Crean A.M., Moore A. Production of Dissolvable Microneedles Using an Atomised Spray Process: Effect of Microneedle Composition on Skin Penetration. Eur. J. Pharm. Biopharm. 2014;86:200–211. doi: 10.1016/j.ejpb.2013.04.023. [DOI] [PubMed] [Google Scholar]
- 38.Frydman G.H., Olaleye D., Annamalai D., Layne K., Yang I., Kaafarani H.M.A., Fox J.G. Manuka Honey Microneedles for Enhanced Wound Healing and the Prevention and/or Treatment of Methicillin-Resistant Staphylococcus Aureus (MRSA) Surgical Site Infection. Sci. Rep. 2020;10:13229. doi: 10.1038/s41598-020-70186-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Schipper P., van der Maaden K., Groeneveld V., Ruigrok M., Romeijn S., Uleman S., Oomens C., Kersten G., Jiskoot W., Bouwstra J. Diphtheria Toxoid and N-Trimethyl Chitosan Layer-by-Layer Coated PH-Sensitive Microneedles Induce Potent Immune Responses upon Dermal Vaccination in Mice. J. Control. Release. 2017;262:28–36. doi: 10.1016/j.jconrel.2017.07.017. [DOI] [PubMed] [Google Scholar]
- 40.Choi H.J., Yoo D.G., Bondy B.J., Quan F.S., Compans R.W., Kang S.M., Prausnitz M.R. Stability of Influenza Vaccine Coated onto Microneedles. Biomaterials. 2012;33:3756–3769. doi: 10.1016/j.biomaterials.2012.01.054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Zhuang J., Rao F., Wu D., Huang Y., Xu H., Gao W., Zhang J., Sun J. Study on the Fabrication and Characterization of Tip-Loaded Dissolving Microneedles for Transdermal Drug Delivery. Eur. J. Pharm. Biopharm. 2020;157:66–73. doi: 10.1016/j.ejpb.2020.10.002. [DOI] [PubMed] [Google Scholar]
- 42.Dillon C., Hughes H., O’Reilly N.J., McLoughlin P. Formulation and Characterisation of Dissolving Microneedles for the Transdermal Delivery of Therapeutic Peptides. Int. J. Pharm. 2017;526:125–136. doi: 10.1016/j.ijpharm.2017.04.066. [DOI] [PubMed] [Google Scholar]
- 43.Mishra R., Pramanick B., Maiti T.K., Bhattacharyya T.K. Glassy Carbon Microneedles—New Transdermal Drug Delivery Device Derived from a Scalable C-MEMS Process. Microsyst. Nanoeng. 2018;4:38. doi: 10.1038/s41378-018-0039-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Leone M., Priester M.I., Romeijn S., Nejadnik M.R., Mönkäre J., O’Mahony C., Jiskoot W., Kersten G., Bouwstra J.A. Hyaluronan-Based Dissolving Microneedles with High Antigen Content for Intradermal Vaccination: Formulation, Physicochemical Characterization and Immunogenicity Assessment. Eur. J. Pharm. Biopharm. 2019;134:49–59. doi: 10.1016/j.ejpb.2018.11.013. [DOI] [PubMed] [Google Scholar]
- 45.Kim N.W., Kim S.Y., Lee J.E., Yin Y., Lee J.H., Lim S.Y., Kim E.S., Duong H.T.T., Kim H.K., Kim S., et al. Enhanced Cancer Vaccination by in Situ Nanomicelle-Generating Dissolving Microneedles. ACS Nano. 2018;12:9702–9713. doi: 10.1021/acsnano.8b04146. [DOI] [PubMed] [Google Scholar]
- 46.Menon I., Bagwe P., Gomes K.B., Bajaj L., Gala R., Uddin M.N., D’souza M.J., Zughaier S.M. Microneedles: A New Generation Vaccine Delivery System. Micromachines. 2021;12:435. doi: 10.3390/mi12040435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Zhang L., Guo R., Wang S., Yang X., Ling G., Zhang P. Fabrication, Evaluation and Applications of Dissolving Microneedles. Int. J. Pharm. 2021;604:120749. doi: 10.1016/j.ijpharm.2021.120749. [DOI] [PubMed] [Google Scholar]
- 48.Steinbach S., Jalili-Firoozinezhad S., Srinivasan S., Melo M.B., Middleton S., Konold T., Coad M., Hammond P.T., Irvine D.J., Vordermeier M., et al. Temporal Dynamics of Intradermal Cytokine Response to Tuberculin in Mycobacterium Bovis BCG-Vaccinated Cattle Using Sampling Microneedles. Sci. Rep. 2021;11:7074. doi: 10.1038/s41598-021-86398-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Kim Y.-C., Quan F.-S., Compans R.W., Kang S.-M., Prausnitz M.R. Formulation and Coating of Microneedles with Inactivated Influenza Virus to Improve Vaccine Stability and Immunogenicity. J. Control. Release. 2010;142:187–195. doi: 10.1016/j.jconrel.2009.10.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Tran K.T.M., Gavitt T.D., Farrell N.J., Curry E.J., Mara A.B., Patel A., Brown L., Kilpatrick S., Piotrowska R., Mishra N., et al. Transdermal Microneedles for the Programmable Burst Release of Multiple Vaccine Payloads. Nat. Biomed. Eng. 2020;5:998–1007. doi: 10.1038/s41551-020-00650-4. [DOI] [PubMed] [Google Scholar]
- 51.Chen Y.H., Lai K.Y., Chiu Y.H., Wu Y.W., Shiau A.L., Chen M.C. Implantable Microneedles with an Immune-Boosting Function for Effective Intradermal Influenza Vaccination. Acta Biomater. 2019;97:230–238. doi: 10.1016/j.actbio.2019.07.048. [DOI] [PubMed] [Google Scholar]
- 52.Ita K. Dissolving Microneedles for Transdermal Drug Delivery: Advances and Challenges. Biomed. Pharmacother. 2017;93:1116–1127. doi: 10.1016/j.biopha.2017.07.019. [DOI] [PubMed] [Google Scholar]
- 53.Zhu Z., Ye X., Ku Z., Liu Q., Shen C., Luo H., Luan H., Zhang C., Tian S., Lim C.Y., et al. Transcutaneous Immunization via Rapidly Dissolvable Microneedles Protects against Hand-Foot-and-Mouth Disease Caused by Enterovirus 71. J. Control. Release. 2016;243:291–302. doi: 10.1016/j.jconrel.2016.10.019. [DOI] [PubMed] [Google Scholar]
- 54.Indermun S., Luttge R., Choonara Y.E., Kumar P., Du Toit L.C., Modi G., Pillay V. Current Advances in the Fabrication of Microneedles for Transdermal Delivery. J. Control. Release. 2014;185:130–138. doi: 10.1016/j.jconrel.2014.04.052. [DOI] [PubMed] [Google Scholar]
- 55.Kim Y.-C., Park J.-H., Prausnitz M.R. Microneedles for Drug and Vaccine Delivery. Adv. Drug Deliv. Rev. 2012;64:1547. doi: 10.1016/j.addr.2012.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Deng Y., Chen J., Zhao Y., Yan X., Zhang L., Choy K., Hu J., Sant H.J., Gale B.K., Tang T. Transdermal Delivery of SiRNA through Microneedle Array. Sci. Rep. 2016;6:21422. doi: 10.1038/srep21422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Martin A., McConville A., Anderson A., McLister A., Davis J. Microneedle Manufacture: Assessing Hazards and Control Measures. Safety. 2017;3:25. doi: 10.3390/safety3040025. [DOI] [Google Scholar]
- 58.Carey J.B., Vrdoljak A., O’Mahony C., Hill A.V.S., Draper S.J., Moore A.C. Microneedle-Mediated Immunization of an Adenovirus-Based Malaria Vaccine Enhances Antigen-Specific Antibody Immunity and Reduces Anti-Vector Responses Compared to the Intradermal Route. Sci. Rep. 2014;4:6154. doi: 10.1038/srep06154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Norman J.J., Arya J.M., McClain M.A., Frew P.M., Meltzer M.I., Prausnitz M.R. Microneedle Patches: Usability and Acceptability for Self-Vaccination against Influenza. Vaccine. 2014;32:1856. doi: 10.1016/j.vaccine.2014.01.076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Than A., Liu C., Chang H., Duong P.K., Cheung C.M.G., Xu C., Wang X., Chen P. Self-Implantable Double-Layered Micro-Drug-Reservoirs for Efficient and Controlled Ocular Drug Delivery. Nat. Commun. 2018;9:4433. doi: 10.1038/s41467-018-06981-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Van Der Maaden K., Jiskoot W., Bouwstra J. Microneedle Technologies for (Trans) Dermal Drug and Vaccine Delivery. J. Control. Release. 2012;161:645–655. doi: 10.1016/j.jconrel.2012.01.042. [DOI] [PubMed] [Google Scholar]
- 62.Chang H., Chew S.W.T., Zheng M., Lio D.C.S., Wiraja C., Mei Y., Ning X., Cui M., Than A., Shi P., et al. Cryomicroneedles for Transdermal Cell Delivery. Nat. Biomed. Eng. 2021;5:1008–1018. doi: 10.1038/s41551-021-00720-1. [DOI] [PubMed] [Google Scholar]
- 63.Nguyen T.T., Oh Y., Kim Y., Shin Y., Baek S.K., Park J.H. Progress in Microneedle Array Patch (MAP) for Vaccine Delivery. Hum. Vaccines Immunother. 2020;17:316–327. doi: 10.1080/21645515.2020.1767997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Rodgers A.M., McCrudden M.T.C., Vincente-Perez E.M., Dubois A.V., Ingram R.J., Larrañeta E., Kissenpfennig A., Donnelly R.F. Design and Characterisation of a Dissolving Microneedle Patch for Intradermal Vaccination with Heat-Inactivated Bacteria: A Proof of Concept Study. Int. J. Pharm. 2018;549:87–95. doi: 10.1016/j.ijpharm.2018.07.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ali A.A., McCrudden C.M., McCaffrey J., McBride J.W., Cole G., Dunne N.J., Robson T., Kissenpfennig A., Donnelly R.F., McCarthy H.O. DNA Vaccination for Cervical Cancer; a Novel Technology Platform of RALA Mediated Gene Delivery via Polymeric Microneedles. Nanomedicine. 2017;13:921–932. doi: 10.1016/j.nano.2016.11.019. [DOI] [PubMed] [Google Scholar]
- 66.Nakatsukasa A., Kuruma K., Okamatsu M., Hiono T., Suzuki M., Matsuno K., Kida H., Oyamada T., Sakoda Y. Potency of Whole Virus Particle and Split Virion Vaccines Using Dissolving Microneedle against Challenges of H1N1 and H5N1 Influenza Viruses in Mice. Vaccine. 2017;35:2855–2861. doi: 10.1016/j.vaccine.2017.04.009. [DOI] [PubMed] [Google Scholar]
- 67.Resch T.K., Wang Y., Moon S.S., Joyce J., Li S., Prausnitz M., Jiang B. Inactivated Rotavirus Vaccine by Parenteral Administration Induces Mucosal Immunity in Mice. Sci. Rep. 2018;8:561. doi: 10.1038/s41598-017-18973-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Alimardani V., Abolmaali S.S., Yousefi G., Rahiminezhad Z., Abedi M., Tamaddon A., Ahadian S. Microneedle Arrays Combined with Nanomedicine Approaches for Transdermal Delivery of Therapeutics. J. Clin. Med. 2021;10:181. doi: 10.3390/jcm10020181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Sullivan S.P., Koutsonanos D.G., Del Pilar Martin M., Lee J.W., Zarnitsyn V., Choi S.O., Murthy N., Compans R.W., Skountzou I., Prausnitz M.R. Dissolving Polymer Microneedle Patches for Influenza Vaccination. Nat. Med. 2010;16:915–920. doi: 10.1038/nm.2182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Trautmann A., Roth G.L., Nujiqi B., Walther T., Hellmann R. Towards a Versatile Point-of-Care System Combining Femtosecond Laser Generated Microfluidic Channels and Direct Laser Written Microneedle Arrays. Microsyst. Nanoeng. 2019;5:6. doi: 10.1038/s41378-019-0046-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Silveira M.M., Moreira G.M.S.G., Mendonça M. DNA vaccines against COVID-19: Perspectives and challenges. Life Sci. 2021;267:118919. doi: 10.1016/j.lfs.2020.118919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Simpson C.R., Shi T., Vasileiou E., Katikireddi S.V., Kerr S., Moore E., McCowan C., Agrawal U., Shah S.A., Ritchie L.D., et al. First-Dose ChAdOx1 and BNT162b2 COVID-19 Vaccines and Thrombocytopenic, Thromboembolic and Hemorrhagic Events in Scotland. Nat. Med. 2021;27:1290–1297. doi: 10.1038/s41591-021-01408-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Yokoyama M., Chihara N., Tanaka A., Katayama Y., Taruya A., Ishida Y., Yuzaki M., Honda K., Nishimura Y., Kondo T., et al. A Biodegradable Microneedle Sheet for Intracorporeal Topical Hemostasis. Sci. Rep. 2020;10:18831. doi: 10.1038/s41598-020-75894-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Cardozo T., Veazey R. Informed Consent Disclosure to Vaccine Trial Subjects of Risk of COVID-19 Vaccines Worsening Clinical Disease. Int. J. Clin. Pract. 2021;75:e13795. doi: 10.1111/ijcp.13795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Florindo H.F., Kleiner R., Vaskovich-Koubi D., Acúrcio R.C., Carreira B., Yeini E., Tiram G., Liubomirski Y., Satchi-Fainaro R. Immune-Mediated Approaches against COVID-19. Nat. Nanotechnol. 2020;15:630–645. doi: 10.1038/s41565-020-0732-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Rysz S., Al-Saadi J., Sjöström A., Farm M., Campoccia Jalde F., Plattén M., Eriksson H., Klein M., Vargas-Paris R., Nyrén S., et al. COVID-19 Pathophysiology May Be Driven by an Imbalance in the Renin-Angiotensin-Aldosterone System. Nat. Commun. 2021;12:2417. doi: 10.1038/s41467-021-22713-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Yang R., Deng Y., Huang B., Huang L., Lin A., Li Y., Wang W., Liu J., Lu S., Zhan Z., et al. A Core-Shell Structured COVID-19 MRNA Vaccine with Favorable Biodistribution Pattern and Promising Immunity. Signal Transduct. Target. Ther. 2021;6:213. doi: 10.1038/s41392-021-00634-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Neurath M.F. COVID-19: Biologic and Immunosuppressive Therapy in Gastroenterology and Hepatology. Nat. Rev. Gastroenterol. Hepatol. 2021;18:705–715. doi: 10.1038/s41575-021-00480-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Cho J., Lee Y.J., Kim J.H., Kim S.S., Choi B.S., Choi J.H. Antiviral Activity of Digoxin and Ouabain against SARS-CoV-2 Infection and Its Implication for COVID-19. Sci. Rep. 2020;10:16200. doi: 10.1038/s41598-020-72879-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Ahmed M.H., Hassan A. Dexamethasone for the Treatment of Coronavirus Disease (COVID-19): A Review. SN Compr. Clin. Med. 2020;2:2637–2646. doi: 10.1007/s42399-020-00610-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Batty G.D., Deary I.J., Fawns-Ritchie C., Gale C.R., Altschul D. Pre-Pandemic Cognitive Function and COVID-19 Vaccine Hesitancy: Cohort Study. Brain. Behav. Immun. 2021;96:100–105. doi: 10.1016/j.bbi.2021.05.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Robertson E., Reeve K.S., Niedzwiedz C.L., Moore J., Blake M., Green M., Katikireddi S.V., Benzeval M.J. Predictors of COVID-19 Vaccine Hesitancy in the UK Household Longitudinal Study. Brain. Behav. Immun. 2021;94:41–50. doi: 10.1016/j.bbi.2021.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Amani B., Khanijahani A., Amani B. Hydroxychloroquine plus Standard of Care Compared with Standard of Care Alone in COVID-19: A Meta-Analysis of Randomized Controlled Trials. Sci. Rep. 2021;11:11974. doi: 10.1038/s41598-021-91089-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Maneikis K., Šablauskas K., Ringelevičiūtė U., Vaitekėnaitė V., Čekauskienė R., Kryžauskaitė L., Naumovas D., Banys V., Pečeliūnas V., Beinortas T., et al. Immunogenicity of the BNT162b2 COVID-19 MRNA Vaccine and Early Clinical Outcomes in Patients with Haematological Malignancies in Lithuania: A National Prospective Cohort Study. Lancet Haematol. 2021;8:e583–e592. doi: 10.1016/S2352-3026(21)00169-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Dashtbali M., Mirzaie M. A Compartmental Model That Predicts the Effect of Social Distancing and Vaccination on Controlling COVID-19. Sci. Rep. 2021;11:8191. doi: 10.1038/s41598-021-86873-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Voysey M., Clemens S.A.C., Madhi S.A., Weckx L.Y., Folegatti P.M., Aley P.K., Angus B., Baillie V.L., Barnabas S.L., Bhorat Q.E., et al. Safety and Efficacy of the ChAdOx1 NCoV-19 Vaccine (AZD1222) against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet. 2021;397:99–111. doi: 10.1016/S0140-6736(20)32661-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Filho W.L., Voronova V., Kloga M., Paço A., Minhas A., Salvia A.L., Ferreira C.D., Sivapalan S. COVID-19 and Waste Production in Households: A Trend Analysis. Sci. Total Environ. 2021;777:145997. doi: 10.1016/j.scitotenv.2021.145997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Kreps S., Dasgupta N., Brownstein J.S., Hswen Y., Kriner D.L. Public Attitudes toward COVID-19 Vaccination: The Role of Vaccine Attributes, Incentives, and Misinformation. NPJ Vaccines. 2021;6:73. doi: 10.1038/s41541-021-00335-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Dzieciolowska S., Hamel D., Gadio S., Dionne M., Gagnon D., Robitaille L., Cook E., Caron I., Talib A., Parkes L., et al. COVID-19 Vaccine Acceptance, Hesitancy, and Refusal among Canadian Healthcare Workers: A Multicenter Survey. Am. J. Infect. Control. 2021;49:1152–1157. doi: 10.1016/j.ajic.2021.04.079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Habibi M., Taheri G., Aghdam R. A SARS-CoV-2 (COVID-19) Biological Network to Find Targets for Drug Repurposing. Sci. Rep. 2021;11:9378. doi: 10.1038/s41598-021-88427-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Chen Y., Cheng L., Lian R., Song Z., Tian J. COVID-19 Vaccine Research Focusses on Safety, Efficacy, Immunoinformatics, and Vaccine Production and Delivery: A Bibliometric Analysis Based on VOSviewer. Biosci. Trends. 2021;15:64–73. doi: 10.5582/bst.2021.01061. [DOI] [PubMed] [Google Scholar]
- 92.Kaur U., Ojha B., Pathak B.K., Singh A., Giri K.R., Singh A., Das A., Misra A., Yadav A.K., Chakrabarti S.S., et al. A Prospective Observational Safety Study on ChAdOx1 NCoV-19 Corona Virus Vaccine (Recombinant) Use in Healthcare Workers- First Results from India. eClinicalMedicine. 2021;38:101038. doi: 10.1016/j.eclinm.2021.101038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Moazzam M., Sajid M.I., Shahid H., Butt J., Bashir I., Jamshaid M., Shirazi A.N., Tiwari R.K. Understanding COVID-19: From Origin to Potential Therapeutics. Int. J. Environ. Res. Public Health. 2020;17:5904. doi: 10.3390/ijerph17165904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Orlando V., Coscioni E., Guarino I., Mucherino S., Perrella A., Trama U., Limongelli G., Menditto E. Drug-Utilisation Profiles and COVID-19. Sci. Rep. 2021;11:8913. doi: 10.1038/s41598-021-88398-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Pagliusi S., Jarrett S., Hayman B., Kreysa U., Prasad S.D., Reers M., Hong Thai P., Wu K., Zhang Y.T., Baek Y.O., et al. Emerging Manufacturers Engagements in the COVID−19 Vaccine Research, Development and Supply. Vaccine. 2020;38:5418–5423. doi: 10.1016/j.vaccine.2020.06.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Arce J.S.S., Warren S.S., Meriggi N.F., Scacco A., Mcmurry N., Voors M., Syunyaev G., Malik A.A., Aboutajdine S., Zafar B., et al. COVID-19 Vaccine Acceptance and Hesitancy in Low- and Middle-Income Countries. Nat. Med. 2021;27:1385–1394. doi: 10.1038/s41591-021-01454-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.van Riel D., de Wit E. Next-Generation Vaccine Platforms for COVID-19. Nat. Mater. 2020;19:810–812. doi: 10.1038/s41563-020-0746-0. [DOI] [PubMed] [Google Scholar]
- 98.Feng L., Wang Q., Shan C., Yang C., Feng Y., Wu J., Liu X., Zhou Y., Jiang R., Hu P., et al. An Adenovirus-Vectored COVID-19 Vaccine Confers Protection from SARS-CoV-2 Challenge in Rhesus Macaques. Nat. Commun. 2020;11:4207. doi: 10.1038/s41467-020-18077-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Aygün İ., Kaya M., Alhajj R. Identifying Side Effects of Commonly Used Drugs in the Treatment of COVID-19. Sci. Rep. 2020;10:21508. doi: 10.1038/s41598-020-78697-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Li Z., Wang Z., Dinh P.U.C., Zhu D., Popowski K.D., Lutz H., Hu S., Lewis M.G., Cook A., Andersen H., et al. Cell-Mimicking Nanodecoys Neutralize SARS-CoV-2 and Mitigate Lung Injury in a Non-Human Primate Model of COVID-19. Nat. Nanotechnol. 2021;16:942–951. doi: 10.1038/s41565-021-00923-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Abu-Raddad L.J., Chemaitelly H., Butt A.A. Effectiveness of the BNT162b2 COVID-19 Vaccine against the B.1.1.7 and B.1.351 Variants. N. Engl. J. Med. 2021;385:187–189. doi: 10.1056/NEJMc2104974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Varghese A., Kolamban S., Sherimon V., Lacap E.M., Ahmed S.S., Sreedhar J.P., Al Harthi H., Al Shuaily H.S. SEAMHCRD Deterministic Compartmental Model Based on Clinical Stages of Infection for COVID-19 Pandemic in Sultanate of Oman. Sci. Rep. 2021;11:11984. doi: 10.1038/s41598-021-91114-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Hall V.J., Foulkes S., Saei A., Andrews N., Oguti B., Charlett A., Wellington E., Stowe J., Gillson N., Atti A., et al. COVID-19 Vaccine Coverage in Health-Care Workers in England and Effectiveness of BNT162b2 MRNA Vaccine against Infection (SIREN): A Prospective, Multicentre, Cohort Study. Lancet. 2021;397:1725–1735. doi: 10.1016/S0140-6736(21)00790-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Izda V., Jeffries M.A., Sawalha A.H. COVID-19: A review of therapeutic strategies and vaccine candidates. Clin. Immunol. 2021;222:108634. doi: 10.1016/j.clim.2020.108634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Buckland M.S., Galloway J.B., Fhogartaigh C.N., Meredith L., Provine N.M., Bloor S., Ogbe A., Zelek W.M., Smielewska A., Yakovleva A., et al. Treatment of COVID-19 with Remdesivir in the Absence of Humoral Immunity: A Case Report. Nat. Commun. 2020;11:6385. doi: 10.1038/s41467-020-19761-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Dogra P., Koay E.J., Wang Z., Vahidy F.S., Ferrari M., Pasqualini R., Arap W., Boom M.L., Dirk Sostman H., Cristini V. Is the Worst of the COVID-19 Global Pandemic yet to Come? Application of Financial Mathematics as Candidate Predictive Tools. Transl. Psychiatry. 2021;11:299. doi: 10.1038/s41398-021-01429-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Fu W., Ho P.C., Liu C.L., Tzeng K.T., Nayeem N., Moore J.S., Wang L.S., Chou S.Y. Reconcile the Debate over Protective Effects of BCG Vaccine against COVID-19. Sci. Rep. 2021;11:8356. doi: 10.1038/s41598-021-87731-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Chang W.H. A Review of Vaccine Effects on Women in Light of the COVID-19 Pandemic. Taiwan. J. Obstet. Gynecol. 2020;59:812–820. doi: 10.1016/j.tjog.2020.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Polack F.P., Thomas S.J., Kitchin N., Absalon J., Gurtman A., Lockhart S., Perez J.L., Marc G.P., Moreira E.D., Zerbini C., et al. Safety and Efficacy of the BNT162b2 MRNA COVID-19 Vaccine. N. Engl. J. Med. 2020;383:2603–2615. doi: 10.1056/NEJMoa2034577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Singh N., Rai S.N., Singh V., Singh M.P. Molecular characterization, pathogen-host interaction pathway and in silico approaches for vaccine design against COVID-19. J. Chem. Neuroanat. 2020;110:101874. doi: 10.1016/j.jchemneu.2020.101874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Dai L., Gao G.F. Viral Targets for Vaccines against COVID-19. Nat. Rev. Immunol. 2021;21:73–82. doi: 10.1038/s41577-020-00480-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Wu Y., Cheng X., Jiang G., Tang H., Ming S., Tang L., Lu J. Altered Oral and Gut Microbiota and Its Association with SARS-CoV-2 Viral Load in COVID-19 Patients during Hospitalization. NPJ Biofilms Microbiomes. 2021;7:61. doi: 10.1038/s41522-021-00232-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Hillis S.D., Unwin H.J.T., Chen Y., Cluver L., Sherr L., Goldman P.S., Ratmann O., Donnelly C.A., Bhatt S., Villaveces A., et al. Global Minimum Estimates of Children Affected by COVID-19-Associated Orphanhood and Deaths of Caregivers: A Modelling Study. Lancet. 2021;398:391–402. doi: 10.1016/S0140-6736(21)01253-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Park K.S., Sun X., Aikins M.E., Moon J.J. Non-viral COVID-19 vaccine delivery systems. Adv. Drug Deliv. Rev. 2021;169:137–151. doi: 10.1016/j.addr.2020.12.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Pushparajah D., Jimenez S., Wong S., Alattas H., Nafissi N., Slavcev R.A. Advances in gene-based vaccine platforms to address the COVID-19 pandemic. Adv. Drug Deliv. Rev. 2021;170:113–141. doi: 10.1016/j.addr.2021.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Dal-Ré R., Launay O. Public Trust on Regulatory Decisions: The European Medicines Agency and the AstraZeneca COVID-19 Vaccine Label. Vaccine. 2021;39:4029–4031. doi: 10.1016/j.vaccine.2021.05.095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Xie X., Muruato A.E., Zhang X., Lokugamage K.G., Fontes-Garfias C.R., Zou J., Liu J., Ren P., Balakrishnan M., Cihlar T., et al. A Nanoluciferase SARS-CoV-2 for Rapid Neutralization Testing and Screening of Anti-Infective Drugs for COVID-19. Nat. Commun. 2020;11:5214. doi: 10.1038/s41467-020-19055-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Tan T.K., Rijal P., Rahikainen R., Keeble A.H., Schimanski L., Hussain S., Harvey R., Hayes J.W.P., Edwards J.C., McLean R.K., et al. A COVID-19 Vaccine Candidate Using SpyCatcher Multimerization of the SARS-CoV-2 Spike Protein Receptor-Binding Domain Induces Potent Neutralising Antibody Responses. Nat. Commun. 2021;12:542. doi: 10.1038/s41467-020-20654-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Biswas M., Kali M.S.K. Association of Angiotensin-Converting Enzyme Inhibitors and Angiotensin-Receptor Blockers with Risk of Mortality, Severity or SARS-CoV-2 Test Positivity in COVID-19 Patients: Meta-Analysis. Sci. Rep. 2021;11:5012. doi: 10.1038/s41598-021-84678-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Cot C., Cacciapaglia G., Islind A.S., Óskarsdóttir M., Sannino F. Impact of US Vaccination Strategy on COVID-19 Wave Dynamics. Sci. Rep. 2021;11:10960. doi: 10.1038/s41598-021-90539-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Dutta A.K. Vaccine Against COVID-19 Disease—Present Status of Development. Indian J. Pediatr. 2020;87:810–816. doi: 10.1007/s12098-020-03475-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Chauhan G., Madou M.J., Kalra S., Chopra V., Ghosh D., Martinez-Chapa S.O. Nanotechnology for COVID-19: Therapeutics and Vaccine Research. ACS Nano. 2020;14:7760–7782. doi: 10.1021/acsnano.0c04006. [DOI] [PubMed] [Google Scholar]
- 123.Koirala A., Joo Y.J., Khatami A., Chiu C., Britton P.N. Vaccines for COVID-19: The Current State of Play. Paediatr. Respir. Rev. 2020;35:43–49. doi: 10.1016/j.prrv.2020.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Burn E., You S.C., Sena A.G., Kostka K., Abedtash H., Abrahão M.T.F., Alberga A., Alghoul H., Alser O., Alshammari T.M., et al. Deep Phenotyping of 34,128 Adult Patients Hospitalised with COVID-19 in an International Network Study. Nat. Commun. 2020;11:5009. doi: 10.1038/s41467-020-18849-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Wheatley A.K., Juno J.A., Wang J.J., Selva K.J., Reynaldi A., Tan H.X., Lee W.S., Wragg K.M., Kelly H.G., Esterbauer R., et al. Evolution of Immune Responses to SARS-CoV-2 in Mild-Moderate COVID-19. Nat. Commun. 2021;12:1162. doi: 10.1038/s41467-021-21444-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Macías J., Pinilla A., Lao-Dominguez F.A., Corma A., Contreras-Macias E., González-Serna A., Gutierrez-Pizarraya A., Fernández-Fuertes M., Morillo-Verdugo R., Trigo M., et al. High Rate of Major Drug–Drug Interactions of Lopinavir–Ritonavir for COVID-19 Treatment. Sci. Rep. 2020;10:20958. doi: 10.1038/s41598-020-78029-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Bolcato M., Rodriguez D., Feola A., Mizio G.D., Bonsignore A., Ciliberti R., Tettamanti C., Aurilio M.T., Aprile A. COVID-19 Pandemic and Equal Access to Vaccines. Vaccines. 2021;9:538. doi: 10.3390/vaccines9060538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Brooks N.A., Puri A., Garg S., Nag S., Corbo J., Turabi A.E., Kaka N., Zemmel R.W., Hegarty P.K., Kamat A.M. The Association of Coronavirus Disease-19 Mortality and Prior Bacille Calmette-Guerin Vaccination: A Robust Ecological Analysis Using Unsupervised Machine Learning. Sci. Rep. 2021;11:774. doi: 10.1038/s41598-020-80787-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Meyers L.M., Gutiérrez A.H., Boyle C.M., Terry F., McGonnigal B.G., Salazar A., Princiotta M.F., Martin W.D., De Groot A.S., Moise L. Highly Conserved, Non-Human-like, and Cross-Reactive SARS-CoV-2 T Cell Epitopes for COVID-19 Vaccine Design and Validation. NPJ Vaccines. 2021;6:71. doi: 10.1038/s41541-021-00331-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Alaran A.J., Adebisi Y.A., Badmos A., Khalid-Salako F., Gaya S.K., Ilesanmi E.B., Olaoye D.Q., Bamisaiye A., Lucero-Prisno D.E., III Uneven Power Dynamics Must Be Levelled in COVID-19 Vaccines Access and Distribution. Public Health Pract. 2021;2:100096. doi: 10.1016/j.puhip.2021.100096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Ahmed Saeed AL-Japairai K., Mahmood S., Hamed Almurisi S., Reddy Venugopal J., Rebhi Hilles A., Azmana M., Raman S. Current trends in polymer microneedle for transdermal drug delivery. Int. J. Pharm. 2020;587:119673. doi: 10.1016/j.ijpharm.2020.119673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Victora C.G., Castro M.C., Gurzenda S., Barros A.J.D. Estimating the Early Impact of Immunization against COVID-19 on Deaths among Elderly People in Brazil: Analyses of Secondary Data on Vaccine Coverage and Mortality. medRxiv. 2021 doi: 10.1101/2021.04.27.21256187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Al-Metwali B.Z., Al-Jumaili A.A., Al-Alag Z.A., Sorofman B. Exploring the Acceptance of COVID-19 Vaccine among Healthcare Workers and General Population Using Health Belief Model. J. Eval. Clin. Pract. 2021;27:1112–1122. doi: 10.1111/jep.13581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Bao L., Deng W., Qi F., Lv Q., Song Z., Liu J., Gao H., Wei Q., Yu P., Xu Y., et al. Sequential Infection with H1N1 and SARS-CoV-2 Aggravated COVID-19 Pathogenesis in a Mammalian Model, and Co-Vaccination as an Effective Method of Prevention of COVID-19 and Influenza. Signal Transduct. Target. Ther. 2021;6:200. doi: 10.1038/s41392-021-00618-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Zhu H., Chen C.Z., Sakamuru S., Zhao J., Ngan D.K., Simeonov A., Hall M.D., Xia M., Zheng W., Huang R. Mining of High Throughput Screening Database Reveals AP-1 and Autophagy Pathways as Potential Targets for COVID-19 Therapeutics. Sci. Rep. 2021;11:6725. doi: 10.1038/s41598-021-86110-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Cascella M., Rajnik M., Aleem A., Dulebohn S.C., Di Napoli R. StatPearls [Internet] StatPearls Publishing; Treasure Island, FL, USA: 2022. Features, Evaluation, and Treatment of Coronavirus (COVID-19) [PubMed] [Google Scholar]
- 137.Mongia A., Saha S.K., Chouzenoux E., Majumdar A. A Computational Approach to Aid Clinicians in Selecting Anti-Viral Drugs for COVID-19 Trials. Sci. Rep. 2021;11:9047. doi: 10.1038/s41598-021-88153-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Sarkodie S.A., Owusu P.A. Impact of COVID-19 pandemic on waste management. Environ. Dev. Sustain. 2021;23:7951–7960. doi: 10.1007/s10668-020-00956-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Kumar V.M., Pandi-Perumal S.R., Trakht I., Thyagarajan S.P. Strategy for COVID-19 Vaccination in India: The Country with the Second Highest Population and Number of Cases. NPJ Vaccines. 2021;6:60. doi: 10.1038/s41541-021-00327-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Kashte S., Gulbake A., El-Amin S.F., III, Gupta A. COVID-19 Vaccines: Rapid Development, Implications, Challenges and Future Prospects. Hum. Cell. 2021;34:711. doi: 10.1007/s13577-021-00512-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Yadav P.R., Han T., Olatunji O., Pattanayek S.K. Mathematical Modelling, Simulation and Optimisation of Microneedles for Transdermal Drug Delivery: Trends and Progress. Pharmaceutics. 2020;12:693. doi: 10.3390/pharmaceutics12080693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Kuwentrai C., Yu J., Rong L., Zhang B., Hu Y., Gong H., Dou Y., Deng J., Huang J., Xu C. Intradermal Delivery of Receptor-binding Domain of SARS-CoV-2 Spike Protein with Dissolvable Microneedles to Induce Humoral and Cellular Responses in Mice. Bioeng. Transl. Med. 2021;6:e10202. doi: 10.1002/btm2.10202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Kiem C.T., Massonnaud C., Levy-Bruhl D., Poletto C., Colizza V., Bosetti P., Fontanet A., Gabet A., Olie V., Zanetti L. Short and Medium-Term Challenges for COVID-19 Vaccination: From Prioritisation to the Relaxation of Measures. eClinicalMedicine. 2021;38:101001. doi: 10.1016/j.eclinm.2021.101001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Campi G., Mazziotti M.V., Valletta A., Ravagnan G., Marcelli A., Perali A., Bianconi A. Metastable States in Plateaus and Multi-Wave Epidemic Dynamics of COVID-19 Spreading in Italy. Sci. Rep. 2021;11:12412. doi: 10.1038/s41598-021-91950-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Tregoning J.S., Brown E.S., Cheeseman H.M., Flight K.E., Higham S.L., Lemm N.M., Pierce B.F., Stirling D.C., Wang Z., Pollock K.M. Vaccines for COVID-19. Clin. Exp. Immunol. 2020;202:162–192. doi: 10.1111/cei.13517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Lanza J.S., Vucen S., Flynn O., Donadei A., Cojean S., Loiseau P., Fernandes A.P.S., Frézard F., Moore A.C. A TLR9-Adjuvanted Vaccine Formulated into Dissolvable Microneedle Patches or Cationic Liposomes Protects against Leishmaniasis after Skin or Subcutaneous Immunization. Int. J. Pharm. 2020;586:119390. doi: 10.1016/j.ijpharm.2020.119390. [DOI] [PubMed] [Google Scholar]
- 147.Antunez Muiños P.J., López Otero D., Amat-Santos I.J., López País J., Aparisi A., Cacho Antonio C.E., Catalá P., González Ferrero T., Cabezón G., Otero García O., et al. The COVID-19 Lab Score: An Accurate Dynamic Tool to Predict in-Hospital Outcomes in COVID-19 Patients. Sci. Rep. 2021;11:9361. doi: 10.1038/s41598-021-88679-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Lazarus J.V., Ratzan S.C., Palayew A., Gostin L.O., Larson H.J., Rabin K., Kimball S., El-Mohandes A. A Global Survey of Potential Acceptance of a COVID-19 Vaccine. Nat. Med. 2021;27:225–228. doi: 10.1038/s41591-020-1124-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Castanon A., Rebolj M., Pesola F., Sasieni P. Recovery Strategies Following COVID-19 Disruption to Cervical Cancer Screening and Their Impact on Excess Diagnoses. Br. J. Cancer. 2021;124:1361–1365. doi: 10.1038/s41416-021-01275-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Ramanan A.V., Modi N., de Wildt S.N., Aurich B., Bakhtadze S., Sirvent F.J.B., Cabañas F., Campbell L., Casanova M., Charlton P., et al. Improving clinical paediatric research and learning from COVID-19: Recommendations by the Conect4Children expert advice group. Pediatr. Res. 2021 doi: 10.1038/s41390-021-01587-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Razai M.S., Oakeshott P., Esmail A., Wiysonge C.S., Viswanath K., Mills M.C. COVID-19 Vaccine Hesitancy: The Five Cs to Tackle Behavioural and Sociodemographic Factors. J. R. Soc. Med. 2021;114:295–298. doi: 10.1177/01410768211018951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Longchamps C., Ducarroz S., Crouzet L., Vignier N., Pourtau L., Allaire C., Colleville A.C., El Aarbaoui T., Melchior M. COVID-19 Vaccine Hesitancy among Persons Living in Homeless Shelters in France. Vaccine. 2021;39:3315–3318. doi: 10.1016/j.vaccine.2021.05.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Wouters O.J., Shadlen K.C., Salcher-Konrad M., Pollard A.J., Larson H.J., Teerawattananon Y., Jit M. Challenges in Ensuring Global Access to COVID-19 Vaccines: Production, Affordability, Allocation, and Deployment. Lancet. 2021;397:1023–1034. doi: 10.1016/S0140-6736(21)00306-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Wibawa T. COVID-19 Vaccine Research and Development: Ethical Issues. Trop. Med. Int. Health. 2021;26:14–19. doi: 10.1111/tmi.13503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Marian A.J. Current state of vaccine development and targeted therapies for COVID-19: Impact of basic science discoveries. Cardiovasc. Pathol. 2021;50:107278. doi: 10.1016/j.carpath.2020.107278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Crommelin D.J.A., Anchordoquy T.J., Volkin D.B., Jiskoot W., Mastrobattista E. Addressing the Cold Reality of MRNA Vaccine Stability. J. Pharm. Sci. 2021;110:997–1001. doi: 10.1016/j.xphs.2020.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Soleimanpour S., Yaghoubi A. COVID-19 Vaccine: Where Are We Now and Where Should We Go? Expert Rev. Vaccines. 2021;20:23–44. doi: 10.1080/14760584.2021.1875824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Al-kassmy J., Pedersen J., Kobinger G. Vaccine Candidates against Coronavirus Infections. Viruses. 2020;12:861. doi: 10.3390/v12080861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Ward B.J., Gobeil P., Séguin A., Atkins J., Boulay I., Charbonneau P.Y., Couture M., D’Aoust M.A., Dhaliwall J., Finkle C., et al. Phase 1 Randomized Trial of a Plant-Derived Virus-like Particle Vaccine for COVID-19. Nat. Med. 2021;27:1071–1078. doi: 10.1038/s41591-021-01370-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Santos-Beneit F., Raškevičius V., Skeberdis V.A., Bordel S. A Metabolic Modeling Approach Reveals Promising Therapeutic Targets and Antiviral Drugs to Combat COVID-19. Sci. Rep. 2021;11:11982. doi: 10.1038/s41598-021-91526-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Samaranayake L.P., Seneviratne C.J., Fakhruddin K.S. Coronavirus disease 2019 (COVID-19) vaccines: A concise review. Oral Dis. 2021:1–11. doi: 10.1111/odi.13916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Yadav T., Srivastava N., Mishra G., Dhama K., Kumar S., Puri B., Saxena S.K. Recombinant Vaccines for COVID-19. Hum. Vaccines Immunother. 2020;16:2905–2912. doi: 10.1080/21645515.2020.1820808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Sharma O., Sultan A.A., Ding H., Triggle C.R. A Review of the Progress and Challenges of Developing a Vaccine for COVID-19. Front. Immunol. 2020;11:585354. doi: 10.3389/fimmu.2020.585354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Bakadia B.M., He F., Souho T., Lamboni L., Ullah M.W., Boni B.O., Ahmed A.A.Q., Mukole B.M., Yang G. Prevention and treatment of COVID-19: Focus on interferons, chloroquine/hydroxychloroquine, azithromycin, and vaccine. Biomed. Pharmacother. 2021;133:111008. doi: 10.1016/j.biopha.2020.111008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Bøhler A.D., Strøm M.E., Sandvig K.U., Moe M.C., Jørstad Ø.K. Acute Macular Neuroretinopathy Following COVID-19 Vaccination. Eye. 2021;36:644–645. doi: 10.1038/s41433-021-01610-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Au L., Fendler A., Shepherd S.T.C., Rzeniewicz K., Cerrone M., Byrne F., Carlyle E., Edmonds K., Del Rosario L., Shon J., et al. Cytokine Release Syndrome in a Patient with Colorectal Cancer after Vaccination with BNT162b2. Nat. Med. 2021;27:1362–1366. doi: 10.1038/s41591-021-01387-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167.Holzworth A., Couchot P., Cruz-Knight W., Brucculeri M. Minimal Change Disease Following the Moderna MRNA-1273 SARS-CoV-2 Vaccine. Kidney Int. 2021;100:463. doi: 10.1016/j.kint.2021.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168.Pritchard E., Matthews P.C., Stoesser N., Eyre D.W., Gethings O., Vihta K.D., Jones J., House T., VanSteenHouse H., Bell I., et al. Impact of Vaccination on New SARS-CoV-2 Infections in the United Kingdom. Nat. Med. 2021;27:1370–1378. doi: 10.1038/s41591-021-01410-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Fisher M.J., Psevdos G. Asymptomatic SARS-CoV-2 Infection Following First Dose MRNA-1273 COVID-19 Vaccine in a Veterans Affairs Long Term Care Facility. Am. J. Infect. Control. 2021;49:1210–1211. doi: 10.1016/j.ajic.2021.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.Adetifa I.M.O., Uyoga S., Gitonga J.N., Mugo D., Otiende M., Nyagwange J., Karanja H.K., Tuju J., Wanjiku P., Aman R., et al. Temporal Trends of SARS-CoV-2 Seroprevalence during the First Wave of the COVID-19 Epidemic in Kenya. Nat. Commun. 2021;12:3966. doi: 10.1038/s41467-021-24062-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.Emary K.R.W., Golubchik T., Aley P.K., Ariani C.V., Angus B., Bibi S., Blane B., Bonsall D., Cicconi P., Charlton S., et al. Efficacy of ChAdOx1 NCoV-19 (AZD1222) Vaccine against SARS-CoV-2 Variant of Concern 202012/01 (B.1.1.7): An Exploratory Analysis of a Randomised Controlled Trial. Lancet. 2021;397:1351. doi: 10.1016/S0140-6736(21)00628-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172.Davis H.E., Assaf G.S., McCorkell L., Wei H., Low R.J., Re’em Y., Redfield S., Austin J.P., Akrami A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. eClinicalMedicine. 2021;38 doi: 10.1016/j.eclinm.2021.101019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.Kukar M., Gunčar G., Vovko T., Podnar S., Černelč P., Brvar M., Zalaznik M., Notar M., Moškon S., Notar M. COVID-19 Diagnosis by Routine Blood Tests Using Machine Learning. Sci. Rep. 2021;11:10738. doi: 10.1038/s41598-021-90265-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174.Ye T., Zhong Z., García-Sastre A., Schotsaert M., De Geest B.G. Current Status of COVID-19 (Pre)Clinical Vaccine Development. Angew. Chem.-Int. Ed. 2020;59:18885–18897. doi: 10.1002/anie.202008319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175.Bost P., De Sanctis F., Canè S., Ugel S., Donadello K., Castellucci M., Eyal D., Fiore A., Anselmi C., Barouni R.M., et al. Deciphering the State of Immune Silence in Fatal COVID-19 Patients. Nat. Commun. 2021;12:1428. doi: 10.1038/s41467-021-21702-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 176.Otu A., Osifo-Dawodu E., Atuhebwe P., Agogo E., Ebenso B. Beyond Vaccine Hesitancy: Time for Africa to Expand Vaccine Manufacturing Capacity amidst Growing COVID-19 Vaccine Nationalism. Lancet Microbe. 2021;2:e347–e348. doi: 10.1016/S2666-5247(21)00126-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Huang K., Lin S.W., Sheng W.H., Wang C.C. Influenza Vaccination and the Risk of COVID-19 Infection and Severe Illness in Older Adults in the United States. Sci. Rep. 2021;11:11025. doi: 10.1038/s41598-021-90068-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Galindez G., Matschinske J., Rose T.D., Sadegh S., Salgado-Albarrán M., Späth J., Baumbach J., Pauling J.K. Lessons from the COVID-19 Pandemic for Advancing Computational Drug Repurposing Strategies. Nat. Comput. Sci. 2021;1:33–41. doi: 10.1038/s43588-020-00007-6. [DOI] [PubMed] [Google Scholar]
- 179.Kim J., Eygeris Y., Gupta M., Sahay G. Self-assembled mRNA vaccines. Adv. Drug Deliv. Rev. 2021;170:83–112. doi: 10.1016/j.addr.2020.12.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180.Safe and Proper Sharps Disposal during the COVID-19 Mass Vaccination Campaign | CDC. [(accessed on 12 April 2021)]; Available online: https://www.cdc.gov/vaccines/covid-19/training-education/safe-proper-sharps-disposal.html.
- 181.Hodgson S.H., Mansatta K., Mallett G., Harris V., Emary K.R.W., Pollard A.J. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021;21:e26–e35. doi: 10.1016/S1473-3099(20)30773-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182.Chen J., Dai L., Barrett L., James J., Plaisance-Bonstaff K., Post S.R., Qin Z. SARS-CoV-2 Proteins and Anti-COVID-19 Drugs Induce Lytic Reactivation of an Oncogenic Virus. Commun. Biol. 2021;4:2–7. doi: 10.1038/s42003-021-02220-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183.Kwon S., Joshi A.D., Lo C.H., Drew D.A., Nguyen L.H., Guo C.G., Ma W., Mehta R.S., Shebl F.M., Warner E.T., et al. Association of Social Distancing and Face Mask Use with Risk of COVID-19. Nat. Commun. 2021;12:3737. doi: 10.1038/s41467-021-24115-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184.Toyoshima Y., Nemoto K., Matsumoto S., Nakamura Y., Kiyotani K. SARS-CoV-2 Genomic Variations Associated with Mortality Rate of COVID-19. J. Hum. Genet. 2020;65:1075–1082. doi: 10.1038/s10038-020-0808-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185.Tang Z., Kong N., Zhang X., Liu Y., Hu P., Mou S., Liljeström P., Shi J., Tan W., Kim J.S., et al. A Materials-Science Perspective on Tackling COVID-19. Nat. Rev. Mater. 2020;5:847–860. doi: 10.1038/s41578-020-00247-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 186.Wilson N., Baker M.G., Blakely T., Eichner M. Estimating the Impact of Control Measures to Prevent Outbreaks of COVID-19 Associated with Air Travel into a COVID-19-Free Country. Sci. Rep. 2021;11:10766. doi: 10.1038/s41598-021-89807-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 187.Sangkham S. Face Mask and Medical Waste Disposal during the Novel COVID-19 Pandemic in Asia. Case Stud. Chem. Environ. Eng. 2020;2:100052. doi: 10.1016/j.cscee.2020.100052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188.Calder P.C. Nutrition and Immunity: Lessons for COVID-19. Eur. J. Clin. Nutr. 2021;75:1309–1318. doi: 10.1038/s41430-021-00949-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 189.O’Donovan S.M., Imami A., Eby H., Henkel N.D., Creeden J.F., Asah S., Zhang X., Wu X., Alnafisah R., Taylor R.T., et al. Identification of Candidate Repurposable Drugs to Combat COVID-19 Using a Signature-Based Approach. Sci. Rep. 2021;11:4495. doi: 10.1038/s41598-021-84044-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 190.Ramakanth D., Singh S., Maji P.K., Lee Y.S., Gaikwad K.K. Advanced Packaging for Distribution and Storage of COVID-19 Vaccines: A Review. Environ. Chem. Lett. 2021;19:3597–3608. doi: 10.1007/s10311-021-01256-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 191.Wedlund L., Kvedar J. New Machine Learning Model Predicts Who May Benefit Most from COVID-19 Vaccination. npj Digit. Med. 2021;4:2021. doi: 10.1038/s41746-021-00425-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192.Jeyanathan M., Afkhami S., Smaill F., Miller M.S., Lichty B.D., Xing Z. Immunological Considerations for COVID-19 Vaccine Strategies. Nat. Rev. Immunol. 2020;20:615–632. doi: 10.1038/s41577-020-00434-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 193.Cannistraci C.V., Valsecchi M.G., Capua I. Age-Sex Population Adjusted Analysis of Disease Severity in Epidemics as a Tool to Devise Public Health Policies for COVID-19. Sci. Rep. 2021;11:11787. doi: 10.1038/s41598-021-89615-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.Murphy J., Vallières F., Bentall R.P., Shevlin M., McBride O., Hartman T.K., McKay R., Bennett K., Mason L., Gibson-Miller J., et al. Psychological Characteristics Associated with COVID-19 Vaccine Hesitancy and Resistance in Ireland and the United Kingdom. Nat. Commun. 2021;12:29. doi: 10.1038/s41467-020-20226-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 195.Frederiksen L.S.F., Zhang Y., Foged C., Thakur A. The Long Road Toward COVID-19 Herd Immunity: Vaccine Platform Technologies and Mass Immunization Strategies. Front. Immunol. 2020;11:1817. doi: 10.3389/fimmu.2020.01817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 196.Pawlowski C., Puranik A., Bandi H., Venkatakrishnan A.J., Agarwal V., Kennedy R., O’Horo J.C., Gores G.J., Williams A.W., Halamka J., et al. Exploratory Analysis of Immunization Records Highlights Decreased SARS-CoV-2 Rates in Individuals with Recent Non-COVID-19 Vaccinations. Sci. Rep. 2021;11:4741. doi: 10.1038/s41598-021-83641-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197.Wu J., Liang B., Chen C., Wang H., Fang Y., Shen S., Yang X., Wang B., Chen L., Chen Q., et al. SARS-CoV-2 Infection Induces Sustained Humoral Immune Responses in Convalescent Patients Following Symptomatic COVID-19. Nat. Commun. 2021;12:1813. doi: 10.1038/s41467-021-22034-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Huang Y., Yang C., Xu X., Xu W., Liu S. Structural and Functional Properties of SARS-CoV-2 Spike Protein: Potential Antivirus Drug Development for COVID-19. Acta Pharmacol. Sin. 2020;41:1141–1149. doi: 10.1038/s41401-020-0485-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199.Muruato A.E., Fontes-Garfias C.R., Ren P., Garcia-Blanco M.A., Menachery V.D., Xie X., Shi P.Y. A High-Throughput Neutralizing Antibody Assay for COVID-19 Diagnosis and Vaccine Evaluation. Nat. Commun. 2020;11:4059. doi: 10.1038/s41467-020-17892-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 200.Li Q., Lu H. Latest Updates on COVID-19 Vaccines. Biosci. Trends. 2020;14:463–466. doi: 10.5582/bst.2020.03445. [DOI] [PubMed] [Google Scholar]
- 201.Blomberg B., Mohn K.G.-I., Brokstad K.A., Zhou F., Linchausen D.W., Hansen B.-A., Lartey S., Onyango T.B., Kuwelker K., Sævik M., et al. Long COVID in a Prospective Cohort of Home-Isolated Patients. Nat. Med. 2021;27:1607–1613. doi: 10.1038/s41591-021-01433-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 202.Haynes B.F., Corey L., Fernandes P., Gilbert P.B., Hotez P.J., Rao S., Santos M.R., Schuitemaker H., Watson M., Arvin A. Prospects for a Safe COVID-19 Vaccine. Sci. Transl. Med. 2020;12:eabe0948. doi: 10.1126/scitranslmed.abe0948. [DOI] [PubMed] [Google Scholar]
- 203.Sharma A., Kumar Sharma S., Shi Y., Bucci E., Carafoli E., Melino G., Bhattacherjee A., Das G. BCG Vaccination Policy and Preventive Chloroquine Usage: Do They Have an Impact on COVID-19 Pandemic? Cell Death Dis. 2020;11:516. doi: 10.1038/s41419-020-2720-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 204.Vanderbeke L., Van Mol P., Van Herck Y., De Smet F., Humblet-Baron S., Martinod K., Antoranz A., Arijs I., Boeckx B., Bosisio F.M., et al. Monocyte-Driven Atypical Cytokine Storm and Aberrant Neutrophil Activation as Key Mediators of COVID-19 Disease Severity. Nat. Commun. 2021;12:4117. doi: 10.1038/s41467-021-24360-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 205.Silva J., Bratberg J., Lemay V. COVID-19 and Influenza Vaccine Hesitancy among College Students. J. Am. Pharm. Assoc. 2021;61:709–714.e1. doi: 10.1016/j.japh.2021.05.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 206.Nisa C.F., Bélanger J.J., Faller D.G., Buttrick N.R., Mierau J.O., Austin M.M.K., Schumpe B.M., Sasin E.M., Agostini M., Gützkow B., et al. Lives versus Livelihoods? Perceived Economic Risk Has a Stronger Association with Support for COVID-19 Preventive Measures than Perceived Health Risk. Sci. Rep. 2021;11:9669. doi: 10.1038/s41598-021-88314-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 207.Rawat K., Kumari P., Saha L. COVID-19 vaccine: A recent update in pipeline vaccines, their design and development strategies. Eur. J. Pharmacol. 2021;892:173751. doi: 10.1016/j.ejphar.2020.173751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 208.Christiansen D., Earnest-Silveira L., Grubor-Bauk B., Wijesundara D.K., Boo I., Ramsland P.A., Vincan E., Drummer H.E., Gowans E.J., Torresi J. Pre-Clinical Evaluation of a Quadrivalent HCV VLP Vaccine in Pigs Following Microneedle Delivery. Sci. Rep. 2019;9:9251. doi: 10.1038/s41598-019-45461-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 209.Pulit-Penaloza J.A., Sapkota B., Stein Esser E., Compans R.W., Pollack B.P., Skountzou I. Modulation of Influenza Vaccine Immune Responses Using an Epidermal Growth Factor Receptor Kinase Inhibitor. Sci. Rep. 2015;5:12321. doi: 10.1038/srep12321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 210.Tang S., Zhu W., Wang B.Z. Influenza Vaccines toward Universality through Nanoplatforms and given by Microneedle Patches. Viruses. 2020;12:1212. doi: 10.3390/v12111212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 211.Dixon R.V., Lau W.M., Moghimi S.M., Ng K.W. The Diagnostic Potential of Microneedles in Infectious Diseases. Precis. Nanomed. 2020;3:629–640. doi: 10.33218/001c.13658. [DOI] [Google Scholar]
- 212.Plamadeala C., Gosain S.R., Hischen F., Buchroithner B., Puthukodan S., Jacak J., Bocchino A., Whelan D., O’Mahony C., Baumgartner W., et al. Bio-Inspired Microneedle Design for Efficient Drug/Vaccine Coating. Biomed. Microdevices. 2020;22:8. doi: 10.1007/s10544-019-0456-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 213.Thakur R.R.S., Tekko I.A., Al-Shammari F., Ali A.A., McCarthy H., Donnelly R.F. Rapidly Dissolving Polymeric Microneedles for Minimally Invasive Intraocular Drug Delivery. Drug Deliv. Transl. Res. 2016;6:800–815. doi: 10.1007/s13346-016-0332-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 214.Staples M., Daniel K., Cima M.J., Langer R. Application of Micro- and Nano-Electromechanical Devices to Drug Delivery. Pharm. Res. 2006;23:847–863. doi: 10.1007/s11095-006-9906-4. [DOI] [PubMed] [Google Scholar]
- 215.Kim J.H., Song H.B., Lee K.J., Seo I.H., Lee J.Y., Lee S.M., Kim J.H., Ryu W. Impact Insertion of Transfer-Molded Microneedle for Localized and Minimally Invasive Ocular Drug Delivery. J. Control. Release. 2015;209:272–279. doi: 10.1016/j.jconrel.2015.04.041. [DOI] [PubMed] [Google Scholar]
- 216.Onesto V., Di Natale C., Profeta M., Netti P.A., Vecchione R. Engineered PLGA-PVP/VA Based Formulations to Produce Electro-Drawn Fast Biodegradable Microneedles for Labile Biomolecule Delivery. Prog. Biomater. 2020;9:203–217. doi: 10.1007/s40204-020-00143-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 217.Yang J., Liu X., Fu Y., Song Y. Recent Advances of Microneedles for Biomedical Applications: Drug Delivery and Beyond. Acta Pharm. Sin. B. 2019;9:469–483. doi: 10.1016/j.apsb.2019.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 218.Chang H., Zheng M., Chew S.W.T., Xu C. Advances in the Formulations of Microneedles for Manifold Biomedical Applications. Adv. Mater. Technol. 2020;5:1900552. doi: 10.1002/admt.201900552. [DOI] [Google Scholar]
- 219.Jung J.H., Jin S.G. Microneedle for Transdermal Drug Delivery: Current Trends and Fabrication. J. Pharm. Investig. 2021;51:503–517. doi: 10.1007/s40005-021-00512-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 220.Bok M., Zhao Z.J., Jeon S., Jeong J.H., Lim E. Ultrasonically and Iontophoretically Enhanced Drug-Delivery System Based on Dissolving Microneedle Patches. Sci. Rep. 2020;10:2027. doi: 10.1038/s41598-020-58822-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 221.Niu L., Chu L.Y., Burton S.A., Hansen K.J., Panyam J. Intradermal Delivery of Vaccine Nanoparticles Using Hollow Microneedle Array Generates Enhanced and Balanced Immune Response. J. Control. Release. 2019;294:268–278. doi: 10.1016/j.jconrel.2018.12.026. [DOI] [PubMed] [Google Scholar]
- 222.Tucak A., Sirbubalo M., Hindija L., Rahić O., Hadžiabdić J., Muhamedagić K., Čekić A., Vranić E. Microneedles: Characteristics, Materials, Production Methods and Commercial Development. Micromachines. 2020;11:961. doi: 10.3390/mi11110961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 223.Meng F., Hasan A., Mahdi Nejadi Babadaei M., Hashemi Kani P., Jouya Talaei A., Sharifi M., Cai T., Falahati M., Cai Y. Polymeric-Based Microneedle Arrays as Potential Platforms in the Development of Drugs Delivery Systems. J. Adv. Res. 2020;26:137–147. doi: 10.1016/j.jare.2020.07.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 224.Cordeiro A.S., Tekko I.A., Jomaa M.H., Vora L., McAlister E., Volpe-Zanutto F., Nethery M., Baine P.T., Mitchell N., McNeill D.W., et al. Two-Photon Polymerisation 3D Printing of Microneedle Array Templates with Versatile Designs: Application in the Development of Polymeric Drug Delivery Systems. Pharm. Res. 2020;37:174. doi: 10.1007/s11095-020-02887-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 225.Muller D.A., Henricson J., Baker S.B., Togö T., Jayashi Flores C.M., Lemaire P.A., Forster A., Anderson C.D. Innate Local Response and Tissue Recovery Following Application of High Density Microarray Patches to Human Skin. Sci. Rep. 2020;10:18468. doi: 10.1038/s41598-020-75169-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 226.Xie L., Zeng H., Sun J., Qian W. Engineering Microneedles for Therapy and Diagnosis: A Survey. Micromachines. 2020;11:271. doi: 10.3390/mi11030271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 227.Lee H., Bonfante G., Sasaki Y., Takama N., Minami T., Kim B. Porous Microneedles on a Paper for Screening Test of Prediabetes. Med. Devices Sens. 2020;3:e10109. doi: 10.1002/mds3.10109. [DOI] [Google Scholar]
- 228.Ullah A., Choi H.J., Jang M., An S., Kim G.M. Smart Microneedles with Porous Polymer Layer for Glucose-Responsive Insulin Delivery. Pharmaceutics. 2020;12:606. doi: 10.3390/pharmaceutics12070606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 229.Jamaledin R., Makvandi P., Yiu C.K.Y., Agarwal T., Vecchione R., Sun W., Maiti T.K., Tay F.R., Netti P.A. Engineered Microneedle Patches for Controlled Release of Active Compounds: Recent Advances in Release Profile Tuning. Adv. Ther. 2020;3:2000171. doi: 10.1002/adtp.202000171. [DOI] [Google Scholar]
- 230.Yeung C., Chen S., King B., Lin H., King K., Akhtar F., Diaz G., Wang B., Zhu J., Sun W., et al. A 3D-Printed Microfluidic-Enabled Hollow Microneedle Architecture for Transdermal Drug Delivery. Biomicrofluidics. 2019;13:064125. doi: 10.1063/1.5127778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 231.Larrañeta E., Lutton R.E.M., Woolfson A.D., Donnelly R.F. Microneedle Arrays as Transdermal and Intradermal Drug Delivery Systems: Materials Science, Manufacture and Commercial Development. Mater. Sci. Eng. R Rep. 2016;104:1–32. doi: 10.1016/j.mser.2016.03.001. [DOI] [Google Scholar]
- 232.Sharma S., Hatware K., Bhadane P., Sindhikar S., Mishra D.K. Recent Advances in Microneedle Composites for Biomedical Applications: Advanced Drug Delivery Technologies. Mater. Sci. Eng. C. 2019;103:109717. doi: 10.1016/j.msec.2019.05.002. [DOI] [PubMed] [Google Scholar]
- 233.Vassilieva E.V., Kalluri H., McAllister D., Taherbhai M.T., Esser E.S., Pewin W.P., Pulit-Penaloza J.A., Prausnitz M.R., Compans R.W., Skountzou I. Improved Immunogenicity of Individual Influenza Vaccine Components Delivered with a Novel Dissolving Microneedle Patch Stable at Room Temperature. Drug Deliv. Transl. Res. 2015;5:360–371. doi: 10.1007/s13346-015-0228-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 234.Chang L., Wang Y.C., Ershad F., Yang R., Yu C., Fan Y. Wearable Devices for Single-Cell Sensing and Transfection. Trends Biotechnol. 2019;37:1175–1188. doi: 10.1016/j.tibtech.2019.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 235.Xu X., Awad A., Robles-Martinez P., Gaisford S., Goyanes A., Basit A.W. Vat Photopolymerization 3D Printing for Advanced Drug Delivery and Medical Device Applications. J. Control. Release. 2020;329:743–757. doi: 10.1016/j.jconrel.2020.10.008. [DOI] [PubMed] [Google Scholar]
- 236.Lee Y., Dugansani S.R., Jeon S.H., Hwang S.H., Kim J.H., Park S.H., Jeong J.H. Drug-Delivery System Based on Salmon DNA Nano- and Micro-Scale Structures. Sci. Rep. 2017;7:9724. doi: 10.1038/s41598-017-09904-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 237.Ita K. Transdermal Delivery of Drugs with Microneedles—Potential and Challenges. Pharmaceutics. 2015;7:90–105. doi: 10.3390/pharmaceutics7030090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 238.Guillot A.J., Cordeiro A.S., Donnelly R.F., Montesinos M.C., Garrigues T.M., Melero A. Microneedle-based Delivery: An Overview of Current Applications and Trends. Pharmaceutics. 2020;12:569. doi: 10.3390/pharmaceutics12060569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 239.Zhu D.D., Zhang X.P., Yu H.L., Liu R.X., Shen C.B., Zhang W.F., Cui Y., Guo X.D. Kinetic Stability Studies of HBV Vaccine in a Microneedle Patch. Int. J. Pharm. 2019;567:118489. doi: 10.1016/j.ijpharm.2019.118489. [DOI] [PubMed] [Google Scholar]
- 240.Sarabi M.R., Ahmadpour A., Yetisen A.K., Tasoglu S. Finger-Actuated Microneedle Array for Sampling Body Fluids. Appl. Sci. 2021;11:5329. doi: 10.3390/app11125329. [DOI] [Google Scholar]
- 241.Jamaledin R., Di Natale C., Onesto V., Taraghdari Z., Zare E., Makvandi P., Vecchione R., Netti P. Progress in Microneedle-Mediated Protein Delivery. J. Clin. Med. 2020;9:542. doi: 10.3390/jcm9020542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 242.Suzuki M., Takahashi T., Aoyagi S. Fabrication and Characterization of a Biodegradable Hollow Microneedle from Chitosan. J. Robot. Mechatron. 2020;32:401–407. doi: 10.20965/jrm.2020.p0401. [DOI] [Google Scholar]
- 243.Donnelly R.F., Singh T.R.R. Novel Delivery Systems for Transdermal and Intradermal Drug Delivery. John Wiley & Sons, Ltd.; Hoboken, NJ, USA: 2015. [DOI] [Google Scholar]
- 244.Dalvi M., Kharat P., Thakor P., Bhavana V., Singh S.B., Mehra N.K. Panorama of Dissolving Microneedles for Transdermal Drug Delivery. Life Sci. 2021;284:119877. doi: 10.1016/j.lfs.2021.119877. [DOI] [PubMed] [Google Scholar]
- 245.Zhu W., Li S., Wang C., Yu G., Prausnitz M.R., Wang B.-Z. Enhanced Immune Responses Conferring Cross-Protection by Skin Vaccination With a Tri-Component Influenza Vaccine Using a Microneedle Patch. Front. Immunol. 2018;9:1705. doi: 10.3389/fimmu.2018.01705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 246.Rouphael N.G., Paine M., Mosley R., Henry S., McAllister D.V., Kalluri H., Pewin W., Frew P.M., Yu T., Thornburg N.J., et al. The Safety, Immunogenicity, and Acceptability of Inactivated Influenza Vaccine Delivered by Microneedle Patch (TIV-MNP 2015): A Randomised, Partly Blinded, Placebo-Controlled, Phase 1 Trial. Lancet. 2017;390:649–658. doi: 10.1016/S0140-6736(17)30575-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 247.Zaric M., Becker P.D., Hervouet C., Kalcheva P., Yus B.I., Cocita C., O’Neill L.A., Kwon S.-Y., Klavinskis L.S. Long-Lived Tissue Resident HIV-1 Specific Memory CD8+ T Cells Are Generated by Skin Immunization with Live Virus Vectored Microneedle Arrays. J. Control. Release. 2017;268:166–175. doi: 10.1016/j.jconrel.2017.10.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 248.Latanova A.A., Petkov S., Kilpelainen A., Jansons J., Latyshev O.E., Kuzmenko Y.V., Hinkula J., Abakumov M.A., Valuev-Elliston V.T., Gomelsky M., et al. Codon Optimization and Improved Delivery/Immunization Regimen Enhance the Immune Response against Wild-Type and Drug-Resistant HIV-1 Reverse Transcriptase, Preserving Its Th2-Polarity. Sci. Rep. 2018;8:8078. doi: 10.1038/s41598-018-26281-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 249.Liu Y., Ye L., Lin F., Gomaa Y., Flyer D., Carrion R., Patterson J.L., Prausnitz M.R., Smith G., Glenn G., et al. Intradermal Immunization by Ebola Virus GP Subunit Vaccines Using Microneedle Patches Protects Mice against Lethal EBOV Challenge. Sci. Rep. 2018;8:11193. doi: 10.1038/s41598-018-29135-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 250.Yang H.-W., Ye L., Guo X.D., Yang C., Compans R.W., Prausnitz M.R. Ebola Vaccination Using a DNA Vaccine Coated on PLGA-PLL/ΓPGA Nanoparticles Administered Using a Microneedle Patch. Adv. Healthc. Mater. 2017;6:1600750. doi: 10.1002/adhm.201600750. [DOI] [PubMed] [Google Scholar]
- 251.Kaur S.P., Gupta V. COVID-19 Vaccine: A comprehensive status report. Virus Res. 2020;288:198114. doi: 10.1016/j.virusres.2020.198114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 252.Hensel J., McAndrews K.M., McGrail D.J., Dowlatshahi D.P., LeBleu V.S., Kalluri R. Protection against SARS-CoV-2 by BCG Vaccination Is Not Supported by Epidemiological Analyses. Sci. Rep. 2020;10:18377. doi: 10.1038/s41598-020-75491-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 253.Bariya S.H., Gohel M.C., Mehta T.A., Sharma O.P. Microneedles: An Emerging Transdermal Drug Delivery System. J. Pharm. Pharmacol. 2012;64:11–29. doi: 10.1111/j.2042-7158.2011.01369.x. [DOI] [PubMed] [Google Scholar]
- 254.Hong X., Wei L., Wu F., Wu Z., Chen L., Liu Z., Yuan W. Dissolving and Biodegradable Microneedle Technologies for Transdermal Sustained Delivery of Drug and Vaccine. Drug Des. Devel. Ther. 2013;7:945–952. doi: 10.2147/DDDT.S44401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 255.Liu T., Luo G., Xing M. Biomedical Applications of Polymeric Microneedles for Transdermal Therapeutic Delivery and Diagnosis: Current Status and Future Perspectives. Adv. Ther. 2020;3:1900140. doi: 10.1002/adtp.201900140. [DOI] [Google Scholar]
- 256.Matsuo K., Hirobe S., Yokota Y., Ayabe Y., Seto M., Quan Y.-S., Kamiyama F., Tougan T., Horii T., Mukai Y., et al. Transcutaneous Immunization Using a Dissolving Microneedle Array Protects against Tetanus, Diphtheria, Malaria, and Influenza. J. Control. Release. 2012;160:495–501. doi: 10.1016/j.jconrel.2012.04.001. [DOI] [PubMed] [Google Scholar]
- 257.Chen F., Yan Q., Yu Y., Wu M.X. BCG Vaccine Powder-Laden and Dissolvable Microneedle Arrays for Lesion-Free Vaccination. J. Control. Release. 2017;255:36–44. doi: 10.1016/j.jconrel.2017.03.397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 258.Qiu Y., Guo L., Zhang S., Xu B., Gao Y., Hu Y., Hou J., Bai B., Shen H., Mao P. DNA-Based Vaccination against Hepatitis B Virus Using Dissolving Microneedle Arrays Adjuvanted by Cationic Liposomes and CpG ODN. Drug Deliv. 2016;23:2391–2398. doi: 10.3109/10717544.2014.992497. [DOI] [PubMed] [Google Scholar]
- 259.Poirier D., Renaud F., Dewar V., Strodiot L., Wauters F., Janimak J., Shimada T., Nomura T., Kabata K., Kuruma K., et al. Hepatitis B Surface Antigen Incorporated in Dissolvable Microneedle Array Patch Is Antigenic and Thermostable. Biomaterials. 2017;145:256–265. doi: 10.1016/j.biomaterials.2017.08.038. [DOI] [PubMed] [Google Scholar]
- 260.Cuevas M.B.P., Kodani M., Choi Y., Joyce J., O’Connor S.M., Kamili S., Prausnitz M.R. Hepatitis B Vaccination Using a Dissolvable Microneedle Patch Is Immunogenic in Mice and Rhesus Macaques. Bioeng. Transl. Med. 2018;3:186–196. doi: 10.1002/btm2.10098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 261.Edens C., Dybdahl-Sissoko N.C., Weldon W.C., Oberste M.S., Prausnitz M.R. Inactivated Polio Vaccination Using a Microneedle Patch Is Immunogenic in the Rhesus Macaque. Vaccine. 2015;33:4683–4690. doi: 10.1016/j.vaccine.2015.01.089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 262.Muller D.A., Fernando G.J.P., Owens N.S., Agyei-Yeboah C., Wei J.C.J., Depelsenaire A.C.I., Forster A., Fahey P., Weldon W.C., Oberste M.S., et al. High-Density Microprojection Array Delivery to Rat Skin of Low Doses of Trivalent Inactivated Poliovirus Vaccine Elicits Potent Neutralising Antibody Responses. Sci. Rep. 2017;7:12644. doi: 10.1038/s41598-017-13011-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 263.Esser E.S., Romanyuk A., Vassilieva E.V., Jacob J., Prausnitz M., Compans R.W., Skountzou I. Tetanus Vaccination with a Dissolving Microneedle Patch Confers Protective Immune Responses in Pregnancy. J. Control. Release. 2016;236:47–56. doi: 10.1016/j.jconrel.2016.06.026. [DOI] [PubMed] [Google Scholar]
- 264.De Swart R.L., De Vries R.D., Rennick L.J., Van Amerongen G., McQuaid S., Verburgh R.J., Yüksel S., De Jong A., Lemon K., Nguyen D.T., et al. Needle-Free Delivery of Measles Virus Vaccine to the Lower Respiratory Tract of Non-Human Primates Elicits Optimal Immunity and Protection. NPJ Vaccines. 2017;2:22. doi: 10.1038/s41541-017-0022-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 265.Edens C., Collins M.L., Ayers J., Rota P.A., Prausnitz M.R. Measles Vaccination Using a Microneedle Patch. Vaccine. 2013;31:3403–3409. doi: 10.1016/j.vaccine.2012.09.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 266.Bhatnagar S., Dave K., Venuganti V.V.K. Microneedles in the Clinic. J. Control. Release. 2017;260:164–182. doi: 10.1016/j.jconrel.2017.05.029. [DOI] [PubMed] [Google Scholar]
- 267.Chiang B., Wang K., Ross Ethier C., Prausnitz M.R. Clearance Kinetics and Clearance Routes of Molecules from the Suprachoroidal Space after Microneedle Injection. Investig. Ophthalmol. Vis. Sci. 2017;58:545–554. doi: 10.1167/iovs.16-20679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 268.Jiang X., Lillehoj P.B. Microneedle-Based Skin Patch for Blood-Free Rapid Diagnostic Testing. Microsyst. Nanoeng. 2020;6:96. doi: 10.1038/s41378-020-00206-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 269.Rad Z.F., Nordon R.E., Anthony C.J., Bilston L., Prewett P.D., Arns J.Y., Arns C.H., Zhang L., Davies G.J. High-Fidelity Replication of Thermoplastic Microneedles with Open Microfluidic Channels. Microsyst. Nanoeng. 2017;3:17034. doi: 10.1038/micronano.2017.34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 270.Xiang Z., Liu J., Lee C. A Flexible Three-Dimensional Electrode Mesh: An Enabling Technology for Wireless Brain–Computer Interface Prostheses. Microsyst. Nanoeng. 2016;2:16012. doi: 10.1038/micronano.2016.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 271.Pireddu R., Schlich M., Marceddu S., Valenti D., Pini E., Fadda A.M., Lai F., Sinico C. Nanosuspensions and Microneedles Roller as a Combined Approach to Enhance Diclofenac Topical Bioavailability. Pharmaceutics. 2020;12:1140. doi: 10.3390/pharmaceutics12121140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 272.Lutton R.E.M., Moore J., Larrañeta E., Ligett S., Woolfson A.D., Donnelly R.F. Microneedle Characterisation: The Need for Universal Acceptance Criteria and GMP Specifications When Moving towards Commercialisation. Drug Deliv. Transl. Res. 2015;5:313–331. doi: 10.1007/s13346-015-0237-z. [DOI] [PubMed] [Google Scholar]
- 273.Rezaei Nejad H., Sadeqi A., Kiaee G., Sonkusale S. Low-Cost and Cleanroom-Free Fabrication of Microneedles. Microsyst. Nanoeng. 2018;4:17073. doi: 10.1038/micronano.2017.73. [DOI] [Google Scholar]
- 274.Lahiji S.F., Dangol M., Jung H. A Patchless Dissolving Microneedle Delivery System Enabling Rapid and Efficient Transdermal Drug Delivery. Sci. Rep. 2015;5:7914. doi: 10.1038/srep07914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 275.Park J.H., Allen M.G., Prausnitz M.R. Polymer Microneedles for Controlled-Release Drug Delivery. Pharm. Res. 2006;23:1008–1019. doi: 10.1007/s11095-006-0028-9. [DOI] [PubMed] [Google Scholar]
- 276.Balmert S.C., Carey C.D., Falo G.D., Sethi S.K., Erdos G., Korkmaz E., Falo L.D. Dissolving Undercut Microneedle Arrays for Multicomponent Cutaneous Vaccination. J. Control. Release. 2020;317:336–346. doi: 10.1016/j.jconrel.2019.11.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 277.Leone M., Mönkäre J., Bouwstra J.A., Kersten G. Dissolving Microneedle Patches for Dermal Vaccination. Pharm. Res. 2017;34:2223–2240. doi: 10.1007/s11095-017-2223-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 278.Ren L., Xu S., Gao J., Lin Z., Chen Z., Liu B., Liang L., Jiang L. Fabrication of Flexible Microneedle Array Electrodes for Wearable Bio-Signal Recording. Sensors. 2018;18:1191. doi: 10.3390/s18041191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 279.Ghosh U., Ning S., Wang Y., Kong Y.L. Addressing Unmet Clinical Needs with 3D Printing Technologies. Adv. Healthc. Mater. 2018;7:e1800417. doi: 10.1002/adhm.201800417. [DOI] [PubMed] [Google Scholar]
- 280.Lee K.J., Lee J.Y., Lee S.G., Park S.H., Yang D.S., Lee J.J., Khademhosseini A., Kim J.S., Ryu W.H. Microneedle Drug Eluting Balloon for Enhanced Drug Delivery to Vascular Tissue. J. Control. Release. 2020;321:174–183. doi: 10.1016/j.jconrel.2020.02.012. [DOI] [PubMed] [Google Scholar]
- 281.Satti A.T., Park J., Park J., Kim H., Cho S. Fabrication of Parylene-Coated Microneedle Array Electrode for Wearable ECG Device. Sensors. 2020;20:5183. doi: 10.3390/s20185183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 282.Tekko I.A., Raj Singh T.R. Microneedles for Drug and Vaccine Delivery and Patient Monitoring. John Wiley & Sons, Ltd; Hoboken, NJ, USA: 2018. Microneedles for Ocular Drug Delivery and Targeting: Challenges and Opportunities; pp. 283–306. [DOI] [Google Scholar]
- 283.Maqsood M., Maqsood H., Kousar R., Jabeen C., Waqas A., Gillani S. Effects of Hospital Service Quality on Patients Satisfaction and Behavioural Intention of Doctors and Nurses. Saudi J. Med. Pharm. Sci. 2017;3:772–776. doi: 10.21276/sjmps. [DOI] [Google Scholar]
- 284.Kusama S., Sato K., Matsui Y., Kimura N., Abe H., Yoshida S., Nishizawa M. Transdermal Electroosmotic Flow Generated by a Porous Microneedle Array Patch. Nat. Commun. 2021;12:658. doi: 10.1038/s41467-021-20948-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 285.Lee K.J., Goudie M.J., Tebon P., Sun W., Luo Z., Lee J., Zhang S., Fetah K., Kim H.J., Xue Y., et al. Non-Transdermal Microneedles for Advanced Drug Delivery. Adv. Drug Deliv. Rev. 2020;165–166:41–59. doi: 10.1016/j.addr.2019.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 286.Jung C.R., Lahiji S.F., Jung H., Kim Y., Kim H. Rapidly Separable Micropillar Integrated Dissolving Microneedles. Pharmaceutics. 2020;12:581. doi: 10.3390/pharmaceutics12060581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 287.Rothstein S.N., Federspiel W.J., Little S.R. A simple model framework for the prediction of controlled release from bulk eroding polymer matrices. J. Mater. Chem. 2008;16:1873–1880. doi: 10.1039/b718277e. [DOI] [Google Scholar]
- 288.Langer R.S., Peppas N.A. Present and future applications of biomaterials in controlled drug delivery systems. Biomaterials. 1981;2:201–214. doi: 10.1016/0142-9612(81)90059-4. [DOI] [PubMed] [Google Scholar]
- 289.Kamaly N., Yameen B., Wu J., Farokhzad O.C. Degradable controlled-release polymers and polymeric nanoparticles: Mechanisms of controlling drug release. Chem. Rev. 2016;116:2602–2663. doi: 10.1021/acs.chemrev.5b00346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 290.Shin M.D., Shukla S., Chung Y.H., Beiss V., Chan S.K., Ortega-Rivera O.A., Wirth D.M., Chen A., Sack M., Pokorski J.K., et al. COVID-19 Vaccine Development and a Potential Nanomaterial Path Forward. Nat. Nanotechnol. 2020;15:646–655. doi: 10.1038/s41565-020-0737-y. [DOI] [PubMed] [Google Scholar]
- 291.Roy G., Galigama R.D., Thorat V.S., Garg P., Venuganti V.V.K. Microneedle Ocular Patch: Fabrication, Characterization, and Ex-Vivo Evaluation Using Pilocarpine as Model Drug. Drug Dev. Ind. Pharm. 2020;46:1114–1122. doi: 10.1080/03639045.2020.1776317. [DOI] [PubMed] [Google Scholar]
- 292.Ye R., Yang J., Li Y., Zheng Y., Yang J., Li Y., Liu B., Jiang L. Fabrication of Tip-Hollow and Tip-Dissolvable Microneedle Arrays for Transdermal Drug Delivery. ACS Biomater. Sci. Eng. 2020;6:2487–2494. doi: 10.1021/acsbiomaterials.0c00120. [DOI] [PubMed] [Google Scholar]
- 293.Yuzhakov V.V. Microneedle Array, Patch, and Applicator for Transdermal Drug Delivery. 7658728 B2. U.S. Patent. 2010 February 9;
- 294.Dardano P., De Martino S., Battisti M., Miranda B., Rea I., De Stefano L. One-Shot Fabrication of Polymeric Hollow Microneedles by Standard Photolithography. Polymers. 2021;13:520. doi: 10.3390/polym13040520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 295.Yang J., Li Y., Ye R., Zheng Y., Li X., Chen Y., Xie X., Jiang L. Smartphone-Powered Iontophoresis-Microneedle Array Patch for Controlled Transdermal Delivery. Microsyst. Nanoeng. 2020;6:112. doi: 10.1038/s41378-020-00224-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 296.Chinnadayyala S.R., Cho S. Porous Platinum Black-Coated Minimally Invasive Microneedles for Non-Enzymatic Continuous Glucose Monitoring in Interstitial Fluid. Nanomaterials. 2021;11:37. doi: 10.3390/nano11010037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 297.Wang Q.L., Zhu D.D., Liu X.B., Chen B.Z., Guo X.D. Microneedles with Controlled Bubble Sizes and Drug Distributions for Efficient Transdermal Drug Delivery. Sci. Rep. 2016;6:38755. doi: 10.1038/srep38755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 298.Wen F., He T., Liu H., Chen H.Y., Zhang T., Lee C. Advances in Chemical Sensing Technology for Enabling the Next-Generation Self-Sustainable Integrated Wearable System in the IoT Era. Nano Energy. 2020;78:105155. doi: 10.1016/j.nanoen.2020.105155. [DOI] [Google Scholar]
- 299.Economidou S.N., Pere C.P.P., Reid A., Uddin M.J., Windmill J.F.C., Lamprou D.A., Douroumis D. 3D Printed Microneedle Patches Using Stereolithography (SLA)for Intradermal Insulin Delivery. Mater. Sci. Eng. C. 2019;102:743–755. doi: 10.1016/j.msec.2019.04.063. [DOI] [PubMed] [Google Scholar]
- 300.Thakur R.R.S., Fallows S.J., McMillan H.L., Donnelly R.F., Jones D.S. Microneedle-Mediated Intrascleral Delivery of in Situ Forming Thermoresponsive Implants for Sustained Ocular Drug Delivery. J. Pharm. Pharmacol. 2014;66:584–595. doi: 10.1111/jphp.12152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 301.Lutton R.E.M., Larrañeta E., Kearney M.C., Boyd P., Woolfson A.D., Donnelly R.F. A Novel Scalable Manufacturing Process for the Production of Hydrogel-Forming Microneedle Arrays. Int. J. Pharm. 2015;494:417–429. doi: 10.1016/j.ijpharm.2015.08.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 302.Eum J., Kim Y., Um D.J., Shin J., Yang H., Jung H. Solvent-Free Polycaprolactone Dissolving Microneedles Generated via the Thermal Melting Method for the Sustained Release of Capsaicin. Micromachines. 2021;12:167. doi: 10.3390/mi12020167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 303.Prausnitz M.R., Langer R. Transdermal Drug Delivery. Nat. Biotechnol. 2008;26:1261–1268. doi: 10.1038/nbt.1504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 304.Leone M., Romeijn S., Du G., Le Dévédec S., Vrieling H., O’Mahony C., Bouwstra J., Kersten G. Diphtheria Toxoid Dissolving Microneedle Vaccination: Adjuvant Screening and Effect of Repeated-Fractional Dose Administration. Int. J. Pharm. 2020;580:119182. doi: 10.1016/j.ijpharm.2020.119182. [DOI] [PubMed] [Google Scholar]
- 305.Hirobe S., Azukizawa H., Matsuo K., Zhai Y., Quan Y.-S., Kamiyama F., Suzuki H., Katayama I., Okada N., Nakagawa S. Development and Clinical Study of a Self-Dissolving Microneedle Patch for Transcutaneous Immunization Device. Pharm. Res. 2013;30:2664–2674. doi: 10.1007/s11095-013-1092-6. [DOI] [PubMed] [Google Scholar]
- 306.Loizidou E.Z., Williams N.A., Barrow D.A., Eaton M.J., McCrory J., Evans S.L., Allender C.J. Structural characteristics and transdermal delivery studies on sugar microneedles: Experimental and finite element modelling analyses. Eur. J. Pharm. Biopharm. 2015;89:224–231. doi: 10.1016/j.ejpb.2014.11.023. [DOI] [PubMed] [Google Scholar]
- 307.Ronnander P., Simon L., Koch A. Experimental and mathematical study of the transdermal delivery of sumatriptan succinate from polyvinylpyrrolidone-based microneedles. Eur. J. Pharm. Biopharm. 2020;146:32–40. doi: 10.1016/j.ejpb.2019.11.007. [DOI] [PubMed] [Google Scholar]
- 308.Chavoshi S., Rabiee M., Rafizadeh M., Rabiee N., Shamsabadi A.S., Bagherzadeh M., Salarian R., Tahriri M., Tayebi L. Mathematical modeling of drug release from biodegradable polymeric microneedles. Bio-Des. Manuf. 2019;2:96–107. doi: 10.1007/s42242-019-00041-y. [DOI] [Google Scholar]
- 309.Ronnander P., Simon L., Spilgies H., Koch A. Modelling the in-vitro dissolution and release of sumatriptan succinate from polyvinylpyrrolidone-based microneedles. Eur. J. Pharm. Sci. 2018;125:54–63. doi: 10.1016/j.ejps.2018.09.010. [DOI] [PubMed] [Google Scholar]
- 310.Kim K.S., Ita K., Simon L. Modelling of dissolving microneedles for transdermal drug delivery: Theoretical and experimental aspects. Eur. J. Pharm. Sci. 2015;68:137–143. doi: 10.1016/j.ejps.2014.12.008. [DOI] [PubMed] [Google Scholar]
- 311.Zoudani E.L., Soltani M. A New Computational Method of Modeling and Evaluation of Dissolving Microneedle for Drug Delivery Applications: Extension to Theoretical Modeling of a Novel Design of Microneedle (Array in Array) for Efficient Drug Delivery. Eur. J. Pharm. Sci. 2020;150:105339. doi: 10.1016/j.ejps.2020.105339. [DOI] [PubMed] [Google Scholar]
- 312.Edens C., Collins M.L., Goodson J.L., Rota P.A., Prausnitz M.R. A Microneedle Patch Containing Measles Vaccine Is Immunogenic in Non-Human Primates. Vaccine. 2015;33:4712–4718. doi: 10.1016/j.vaccine.2015.02.074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 313.Feng Y.H., Liu J.L., Zhu D.D., Hao Y.Y., Guo X.D. Multiscale simulations of drug distributions in polymer dissolvable microneedles. Colloids Surf. B Biointerfaces. 2020;189:110844. doi: 10.1016/j.colsurfb.2020.110844. [DOI] [PubMed] [Google Scholar]
- 314.Suriyaamporn P., Opanasopit P., Ngawhirunpat T., Rangsimawong W. Computer-aided rational design for optimally Gantrez® S-97 and hyaluronic acid-based dissolving microneedles as a potential ocular delivery system. J. Drug Deliv. Sci. Technol. 2021;61:102319. doi: 10.1016/j.jddst.2020.102319. [DOI] [Google Scholar]
- 315.Aldawood F.K., Andar A., Desai S. A Comprehensive Review of Microneedles: Types, Materials, Processes, Characterizations and Applications. Polymers. 2021;13:2815. doi: 10.3390/polym13162815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 316.Moore L.E., Vucen S., Moore A.C. Trends in Drug- and Vaccine-Based Dissolvable Microneedle Materials and Methods of Fabrication. Eur. J. Pharm. Biopharm. 2022;173:54–72. doi: 10.1016/j.ejpb.2022.02.013. [DOI] [PubMed] [Google Scholar]
- 317.Koyani R.D. Synthetic Polymers for Microneedle Synthesis: From Then to Now. J. Drug Deliv. Sci. Technol. 2020;60:102071. doi: 10.1016/j.jddst.2020.102071. [DOI] [Google Scholar]
- 318.Amodwala S., Kumar P., Thakkar H.P. Statistically Optimized Fast Dissolving Microneedle Transdermal Patch of Meloxicam: A Patient Friendly Approach to Manage Arthritis. Eur. J. Pharm. Sci. 2017;104:114–123. doi: 10.1016/j.ejps.2017.04.001. [DOI] [PubMed] [Google Scholar]
- 319.Chen S., Wu D., Liu Y., Huang Y., Xu H., Gao W., Zhang J., Sun J., Zhuang J. Optimal scaling analysis of polymeric microneedle length and its effect on transdermal insulin delivery. J. Drug Deliv. Sci. Technol. 2020;56:101547. doi: 10.1016/j.jddst.2020.101547. [DOI] [Google Scholar]
- 320.Andrews S.N., Jong E., Prausnitz M.R. Transdermal delivery of molecules is limited by full epidermis, not just stratum corneum. Pharm. Res. 2013;30:1099–1109. doi: 10.1007/s11095-012-0946-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 321.Gomaa Y.A., Morrow D.I.J., Garland M.J., Donnelly R.F., El-Khordagui L.K., Meidan V.M. Effects of microneedle length, density, insertion time and multiple applications on human skin barrier function: Assessments by transepidermal water loss. Toxicol. In Vitro. 2010;24:1971–1978. doi: 10.1016/j.tiv.2010.08.012. [DOI] [PubMed] [Google Scholar]
- 322.Wang C., Han B., Zhao T., Liu H., Liu B., Chen L., Xie M., Liu J., Zheng H., Zhang S., et al. Vaccination Willingness, Vaccine Hesitancy, and Estimated Coverage at the First Round of COVID-19 Vaccination in China: A National Cross-Sectional Study. Vaccine. 2021;39:2833–2842. doi: 10.1016/j.vaccine.2021.04.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 323.He X., Sun J., Zhuang J., Xu H., Liu Y., Wu D. Microneedle System for Transdermal Drug and Vaccine Delivery: Devices, Safety, and Prospects. Dose-Response. 2019;17:1559325819878585. doi: 10.1177/1559325819878585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 324.Prausnitz M.R., Mikszta J.A., Cormier M., Andrianov A.K. Microneedle-Based Vaccines. Curr. Top. Microbiol. Immunol. 2009;333:369–393. doi: 10.1007/978-3-540-92165-3_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 325.Prausnitz M.R., Goodson J.L., Rota P.A., Orenstein W.A. A Microneedle Patch for Measles and Rubella Vaccination: A Game Changer for Achieving Elimination. Curr. Opin. Virol. 2020;41:68–76. doi: 10.1016/j.coviro.2020.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 326.Ellison T.J., Talbott G.C., Henderson D.R. VaxiPatchTM, a Novel Vaccination System Comprised of Subunit Antigens, Adjuvants and Microneedle Skin Delivery: An Application to Influenza B/Colorado/06/2017. Vaccine. 2020;38:6839–6848. doi: 10.1016/j.vaccine.2020.07.040. [DOI] [PubMed] [Google Scholar]
- 327.Van Der Maaden K., Varypataki E.M., Yu H., Romeijn S., Jiskoot W., Bouwstra J. Parameter Optimization toward Optimal Microneedle-Based Dermal Vaccination. Eur. J. Pharm. Sci. 2014;64:18–25. doi: 10.1016/j.ejps.2014.08.004. [DOI] [PubMed] [Google Scholar]
- 328.Arya J., Prausnitz M.R. Microneedle Patches for Vaccination in Developing Countries. J. Control. Release. 2016;240:135–141. doi: 10.1016/j.jconrel.2015.11.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 329.O’Shea J., Prausnitz M.R., Rouphael N. Dissolvable Microneedle Patches to Enable Increased Access to Vaccines against SARS-CoV-2 and Future Pandemic Outbreaks. Vaccines. 2021;9:320. doi: 10.3390/vaccines9040320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 330.Arya J.M., Dewitt K., Scott-Garrard M., Chiang Y.-W., Prausnitz M.R. Rabies Vaccination in Dogs Using a Dissolving Microneedle Patch. J. Control. Release. 2016;239:19–26. doi: 10.1016/j.jconrel.2016.08.012. [DOI] [PubMed] [Google Scholar]
- 331.Yan Q., Liu H., Cheng Z., Xue Y., Cheng Z., Dai X., Shan W., Chen F. Immunotherapeutic Effect of BCG-Polysaccharide Nucleic Acid Powder on Mycobacterium Tuberculosis-Infected Mice Using Microneedle Patches. Drug Deliv. 2017;24:1648–1653. doi: 10.1080/10717544.2017.1391892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 332.Liao J.-F., Lee J.-C., Lin C.-K., Hung-Wei Y., Chen P.-Y., Yang H.-W. Self-Assembly DNA Polyplex Vaccine inside Dissolving Microneedles for High-Potency Intradermal Vaccination. Theranostics. 2017;7:2593–2605. doi: 10.7150/thno.19894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 333.Kim E., Erdos G., Huang S., Kenniston T., Falo L.D., Jr., Gambotto A. Preventative Vaccines for Zika Virus Outbreak: Preliminary Evaluation. EBioMedicine. 2016;13:315. doi: 10.1016/j.ebiom.2016.09.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 334.Becker P.D., Hervouet C., Mason G.M., Kwon S.-Y., Klavinskis L.S. Skin Vaccination with Live Virus Vectored Microneedle Arrays Induce Long Lived CD8(+) T Cell Memory. Vaccine. 2015;33:4691–4698. doi: 10.1016/j.vaccine.2015.04.046. [DOI] [PubMed] [Google Scholar]
- 335.Bachy V., Hervouet C., Becker P.D., Chorro L., Carlin L.M., Herath S., Papagatsias T., Barbaroux J.-B., Oh S.-J., Benlahrech A., et al. Langerin Negative Dendritic Cells Promote Potent CD8+ T-Cell Priming by Skin Delivery of Live Adenovirus Vaccine Microneedle Arrays. Proc. Natl. Acad. Sci. USA. 2013;110:3041–3046. doi: 10.1073/pnas.1214449110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 336.Kim E., Erdos G., Huang S., Kenniston T.W., Balmert S.C., Carey C.D., Raj V.S., Epperly M.W., Klimstra W.B., Haagmans B.L., et al. Microneedle Array Delivered Recombinant Coronavirus Vaccines: Immunogenicity and Rapid Translational Development. EBioMedicine. 2020;55:102743. doi: 10.1016/j.ebiom.2020.102743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 337.Pattani A., McKay P., Garland M.J., Curran R.M., Migalska K., Cassidy C.M., Malcolm K., Shattock R.J., McCarthy H., Donnelly R.F. Microneedle Mediated Intradermal Delivery of Adjuvanted Recombinant HIV-1 CN54gp140 Effectively Primes Mucosal Boost Inoculations. J. Control. Release. 2012;162:529–537. doi: 10.1016/j.jconrel.2012.07.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 338.Zhu W., Pewin W., Wang C., Luo Y., Gonzalez G.X., Mohan T., Prausnitz M., Wang B.-Z. A Boosting Skin Vaccination with Dissolving Microneedle Patch Encapsulating M2e Vaccine Broadens the Protective Efficacy of Conventional Influenza Vaccines. J. Control. Release. 2017;261:1–9. doi: 10.1016/j.jconrel.2017.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 339.Deng L., Chang T.Z., Wang Y., Li S., Wang S., Matsuyama S., Yu G., Compans R.W., Li J.-D., Prausnitz M.R., et al. Heterosubtypic Influenza Protection Elicited by Double-Layered Polypeptide Nanoparticles in Mice. Proc. Natl. Acad. Sci. USA. 2018;115:E7758–E7767. doi: 10.1073/pnas.1805713115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 340.Allen E.A., O’Mahony C., Cronin M., O’Mahony T., Moore A.C., Crean A.M. Dissolvable Microneedle Fabrication Using Piezoelectric Dispensing Technology. Int. J. Pharm. 2016;500:1–10. doi: 10.1016/j.ijpharm.2015.12.052. [DOI] [PubMed] [Google Scholar]
- 341.Kommareddy S., Baudner B.C., Oh S., Kwon S.-Y., Singh M., O’Hagan D.T. Dissolvable Microneedle Patches for the Delivery of Cell-Culture-Derived Influenza Vaccine Antigens. J. Pharm. Sci. 2012;101:1021–1027. doi: 10.1002/jps.23019. [DOI] [PubMed] [Google Scholar]
- 342.Mistilis M.J., Bommarius A.S., Prausnitz M.R. Development of a Thermostable Microneedle Patch for Influenza Vaccination. J. Pharm. Sci. 2015;104:740–749. doi: 10.1002/jps.24283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 343.Wang J., Li B., Wu M.X. Effective and Lesion-Free Cutaneous Influenza Vaccination. Proc. Natl. Acad. Sci. USA. 2015;112:5005–5010. doi: 10.1073/pnas.1500408112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 344.Hirobe S., Azukizawa H., Hanafusa T., Matsuo K., Quan Y.-S., Kamiyama F., Katayama I., Okada N., Nakagawa S. Clinical Study and Stability Assessment of a Novel Transcutaneous Influenza Vaccination Using a Dissolving Microneedle Patch. Biomaterials. 2015;57:50–58. doi: 10.1016/j.biomaterials.2015.04.007. [DOI] [PubMed] [Google Scholar]
- 345.Long-Term Stability of Influenza Vaccine in a Dissolving Microneedle Patch. [(accessed on 29 April 2021)]; doi: 10.1007/s13346-016-0282-2. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5003766/ [DOI] [PMC free article] [PubMed]
- 346.Littauer E.Q., Mills L.K., Brock N., Esser E.S., Romanyuk A., Pulit-Penaloza J.A., Vassilieva E.V., Beaver J.T., Antao O., Krammer F., et al. Stable Incorporation of GM-CSF into Dissolvable Microneedle Patch Improves Skin Vaccination against Influenza. J. Control. Release. 2018;276:1–16. doi: 10.1016/j.jconrel.2018.02.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 347.Esser E.S., Pulit-Penaloza J.A., Kalluri H., McAllister D., Vassilieva E.V., Littauer E., Lelutiu N., Prausnitz M., Compans R.W., Skountzou I. Microneedle Patch Delivery of Influenza Vaccine during Pregnancy Enhances Maternal Immune Responses Promoting Survival and Long-Lasting Passive Immunity to Offspring. Sci. Rep. 2017;7:5705. doi: 10.1038/s41598-017-05940-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 348.Vassilieva E.V., Wang S., Li S., Prausnitz M.R., Compans R.W. Skin Immunization by Microneedle Patch Overcomes Statin-Induced Suppression of Immune Responses to Influenza Vaccine. Sci. Rep. 2017;7:17855. doi: 10.1038/s41598-017-18140-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 349.Wang T., Zhen Y., Ma X., Wei B., Li S., Wang N. Mannosylated and Lipid A-Incorporating Cationic Liposomes Constituting Microneedle Arrays as an Effective Oral Mucosal HBV Vaccine Applicable in the Controlled Temperature Chain. Colloids Surf. B. Biointerfaces. 2015;126:520–530. doi: 10.1016/j.colsurfb.2015.01.005. [DOI] [PubMed] [Google Scholar]
- 350.Hiraishi Y., Nakagawa T., Quan Y.-S., Kamiyama F., Hirobe S., Okada N., Nakagawa S. Performance and Characteristics Evaluation of a Sodium Hyaluronate-Based Microneedle Patch for a Transcutaneous Drug Delivery System. Int. J. Pharm. 2013;441:570–579. doi: 10.1016/j.ijpharm.2012.10.042. [DOI] [PubMed] [Google Scholar]
- 351.Chu L.Y., Ye L., Dong K., Compans R.W., Yang C., Prausnitz M.R. Enhanced Stability of Inactivated Influenza Vaccine Encapsulated in Dissolving Microneedle Patches. Pharm. Res. 2016;33:868–878. doi: 10.1007/s11095-015-1833-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 352.Chu L.Y., Prausnitz M.R. Separable Arrowhead Microneedles. J. Control. Release. 2011;149:242–249. doi: 10.1016/j.jconrel.2010.10.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 353.Raphael A.P., Prow T.W., Crichton M.L., Chen X., Fernando G.J.P., Kendall M.A.F. Targeted, Needle-Free Vaccinations in Skin Using Multilayered, Densely-Packed Dissolving Microprojection Arrays. Small. 2010;6:1785–1793. doi: 10.1002/smll.201000326. [DOI] [PubMed] [Google Scholar]
- 354.Donadei A., Kraan H., Ophorst O., Flynn O., O’Mahony C., Soema P.C., Moore A.C. Skin Delivery of Trivalent Sabin Inactivated Poliovirus Vaccine Using Dissolvable Microneedle Patches Induces Neutralizing Antibodies. J. Control. Release. 2019;311–312:96–103. doi: 10.1016/j.jconrel.2019.08.039. [DOI] [PubMed] [Google Scholar]
- 355.Kolluru C., Gomaa Y., Prausnitz M.R. Development of a Thermostable Microneedle Patch for Polio Vaccination. Drug Deliv. Transl. Res. 2019;9:192–203. doi: 10.1007/s13346-018-00608-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 356.Joyce J.C., Carroll T.D., Collins M.L., Chen M.-H., Fritts L., Dutra J.C., Rourke T.L., Goodson J.L., McChesney M.B., Prausnitz M.R., et al. A Microneedle Patch for Measles and Rubella Vaccination Is Immunogenic and Protective in Infant Rhesus Macaques. J. Infect. Dis. 2018;218:124–132. doi: 10.1093/infdis/jiy139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 357.Erdos G., Balmert S.C., Carey C.D., Falo G.D., Patel N.A., Zhang J., Gambotto A., Korkmaz E., Falo L.D. Improved Cutaneous Genetic Immunization by Microneedle Array Delivery of an Adjuvanted Adenovirus Vaccine. J. Invest. Dermatol. 2020;140:2528–2531.e2. doi: 10.1016/j.jid.2020.03.966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 358.Hsueh K.-J., Chen M.-C., Cheng L.-T., Lee J.-W., Chung W.-B., Chu C.-Y. Transcutaneous Immunization of Streptococcus Suis Bacterin Using Dissolving Microneedles. Comp. Immunol. Microbiol. Infect. Dis. 2017;50:78–87. doi: 10.1016/j.cimid.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 359.Schepens B., Vos P.J., Saelens X., van der Maaden K. Vaccination with Influenza Hemagglutinin-Loaded Ceramic Nanoporous Microneedle Arrays Induces Protective Immune Responses. Eur. J. Pharm. Biopharm. 2019;136:259–266. doi: 10.1016/j.ejpb.2019.02.002. [DOI] [PubMed] [Google Scholar]
- 360.Uddin M.J., Scoutaris N., Economidou S.N., Giraud C., Chowdhry B.Z., Donnelly R.F., Douroumis D. 3D Printed Microneedles for Anticancer Therapy of Skin Tumours. Mater. Sci. Eng. C. 2020;107:110248. doi: 10.1016/j.msec.2019.110248. [DOI] [PubMed] [Google Scholar]
- 361.Gill H.S., Denson D.D., Burris B.A., Prausnitz M.R. Effect of Microneedle Design on Pain in Human Subjects. Clin. J. Pain. 2008;24:585. doi: 10.1097/AJP.0b013e31816778f9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 362.Uddin M.J., Scoutaris N., Klepetsanis P., Chowdhry B., Prausnitz M.R., Douroumis D. Inkjet Printing of Transdermal Microneedles for the Delivery of Anticancer Agents. Int. J. Pharm. 2015;494:593–602. doi: 10.1016/j.ijpharm.2015.01.038. [DOI] [PubMed] [Google Scholar]
- 363.He B., Liu S., Wang Y., Xu M., Cai W., Liu J., Bai W., Ye S., Ma Y., Hu H., et al. Rapid Isolation and Immune Profiling of SARS-CoV-2 Specific Memory B Cell in Convalescent COVID-19 Patients via LIBRA-Seq. Signal Transduct. Target. Ther. 2021;6:195. doi: 10.1038/s41392-021-00610-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 364.Das A.K., Islam M.N., Billah M.M., Sarker A. COVID-19 Pandemic and Healthcare Solid Waste Management Strategy—A Mini-Review. Sci. Total Environ. 2021;778:146220. doi: 10.1016/j.scitotenv.2021.146220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 365.Mills J.L.S., Jayashi C.M.F., Reynolds S., Wun C., Calcutt A., Baker S.B., Murugappan S., Depelsenaire A.C.I., Dooley J., Fahey P.V., et al. M-Protein Based Vaccine Induces Immunogenicity and Protection from Streptococcus Pyogenes When Delivered on a High-Density Microarray Patch (HD-MAP) NPJ Vaccines. 2020;5:74. doi: 10.1038/s41541-020-00222-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 366.Pulit-Penaloza J.A., Esser E.S., Vassilieva E.V., Lee J.W., Taherbhai M.T., Pollack B.P., Prausnitz M.R., Compans R.W., Skountzou I. A Protective Role of Murine Langerin+ Cells in Immune Responses to Cutaneous Vaccination with Microneedle Patches. Sci. Rep. 2014;4:6094. doi: 10.1038/srep06094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 367.Jeong H.R., Bae J.Y., Park J.H., Baek S.K., Kim G., Park M.S., Park J.H. Preclinical Study of Influenza Bivalent Vaccine Delivered with a Two Compartmental Microneedle Array. J. Control. Release. 2020;324:280–288. doi: 10.1016/j.jconrel.2020.05.024. [DOI] [PubMed] [Google Scholar]
- 368.Wong Y.-L., Sampson S., Germishuizen W.A., Goonesekera S., Caponetti G., Sadoff J., Bloom B.R., Edwards D. Drying a Tuberculosis Vaccine without Freezing. Proc. Natl. Acad. Sci. USA. 2007;104:2591–2595. doi: 10.1073/pnas.0611430104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 369.Bardel E., Doucet-Ladeveze R., Mathieu C., Harandi A.M., Dubois B., Kaiserlian D. Intradermal Immunisation Using the TLR3-Ligand Poly (I:C) as Adjuvant Induces Mucosal Antibody Responses and Protects against Genital HSV-2 Infection. npj Vaccines. 2016;1:16010. doi: 10.1038/npjvaccines.2016.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 370.Muller D.A., Pearson F.E., Fernando G.J.P., Agyei-Yeboah C., Owens N.S., Corrie S.R., Crichton M.L., Wei J.C.J., Weldon W.C., Oberste M.S., et al. Inactivated Poliovirus Type 2 Vaccine Delivered to Rat Skin via High Density Microprojection Array Elicits Potent Neutralising Antibody Responses. Sci. Rep. 2016;6:22094. doi: 10.1038/srep22094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 371.Frolov V.G., Seid R.C., Odutayo O., Al-Khalili M., Yu J., Frolova O.Y., Vu H., Butler B.A., Look J.L., Ellingsworth L.R., et al. Transcutaneous Delivery and Thermostability of a Dry Trivalent Inactivated Influenza Vaccine Patch. Influenza Other Respir. Viruses. 2008;2:53–60. doi: 10.1111/j.1750-2659.2008.00040.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 372.Nakagami H., Hayashi H., Shimamura M., Rakugi H., Morishita R. Therapeutic Vaccine for Chronic Diseases after the COVID-19 Era. Hypertens. Res. 2021;44:1047–1053. doi: 10.1038/s41440-021-00677-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 373.Lofano G., Mallett C.P., Bertholet S., O’Hagan D.T. Technological Approaches to Streamline Vaccination Schedules, Progressing towards Single-Dose Vaccines. NPJ Vaccines. 2020;5:88. doi: 10.1038/s41541-020-00238-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 374.Brüssow H. Efforts towards a COVID-19 Vaccine. Environ. Microbiol. 2020;22:4071–4084. doi: 10.1111/1462-2920.15225. [DOI] [PubMed] [Google Scholar]
- 375.Creighton R.L., Phan J., Woodrow K.A. In Situs 3D-Patterning of Electrospun Fibers Using Two-Layer Composite Materials. Sci. Rep. 2020;10:7949. doi: 10.1038/s41598-020-64846-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 376.Vargason A.M., Anselmo A.C., Mitragotri S. The Evolution of Commercial Drug Delivery Technologies. Nat. Biomed. Eng. 2021;5:951–967. doi: 10.1038/s41551-021-00698-w. [DOI] [PubMed] [Google Scholar]
- 377.Serr I., Fürst R.W., Achenbach P., Scherm M.G., Gökmen F., Haupt F., Sedlmeier E.M., Knopff A., Shultz L., Willis R.A., et al. Type 1 Diabetes Vaccine Candidates Promote Human Foxp3+ Treg Induction in Humanized Mice. Nat. Commun. 2016;7:10991. doi: 10.1038/ncomms10991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 378.Yazie T.D., Tebeje M.G., Chufa K.A. Healthcare Waste Management Current Status and Potential Challenges in Ethiopia: A Systematic Review. BMC Res. Notes. 2019;12:285. doi: 10.1186/s13104-019-4316-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 379.MacDonald N.E., The SAGE Working Group on Vaccine Hesitancy Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine. 2015;33:4161–4164. doi: 10.1016/j.vaccine.2015.04.036. [DOI] [PubMed] [Google Scholar]
- 380.Salmon D.A., Dudley M.Z., Glanz J.M., Omer S.B. Vaccine Hesitancy: Causes, Consequences, and a Call to Action. Am. J. Prev. Med. 2015;49:S391–S398. doi: 10.1016/j.amepre.2015.06.009. [DOI] [PubMed] [Google Scholar]
- 381.Hornsey M.J., Lobera J., Díaz-Catalán C. Vaccine Hesitancy Is Strongly Associated with Distrust of Conventional Medicine, and Only Weakly Associated with Trust in Alternative Medicine. Soc. Sci. Med. 2020;255:113019. doi: 10.1016/j.socscimed.2020.113019. [DOI] [PubMed] [Google Scholar]
- 382.Stoeckel F., Carter C., Lyons B.A., Reifler J. Association of Vaccine Hesitancy and Immunization Coverage Rates in the European Union. Vaccine. 2021;39:3935–3939. doi: 10.1016/j.vaccine.2021.05.062. [DOI] [PubMed] [Google Scholar]
- 383.Abu Hammour K., Abu Farha R., Manaseer Q., Al-Manaseer B. Factors Affecting Public Knowledge about COVID-19 Vaccines and the Influence of Knowledge on Their Acceptance to Get Vaccinated. J. Am. Pharm. Assoc. 2021;62:309–316. doi: 10.1016/j.japh.2021.06.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 384.Luk T.T., Zhao S., Wu Y., Wong J.Y.H., Wang M.P., Lam T.H. Prevalence and Determinants of SARS-CoV-2 Vaccine Hesitancy in Hong Kong: A Population-Based Survey. Vaccine. 2021;39:3602–3607. doi: 10.1016/j.vaccine.2021.05.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 385.Paris C., Bénézit F., Geslin M., Polard E., Baldeyrou M., Turmel V., Tadié É., Garlantezec R., Tattevin P. COVID-19 Vaccine Hesitancy among Healthcare Workers. Infect. Dis. Now. 2021;51:484–487. doi: 10.1016/j.idnow.2021.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 386.Pullan S., Dey M. Vaccine Hesitancy and Anti-Vaccination in the Time of COVID-19: A Google Trends Analysis. Vaccine. 2021;39:1877–1881. doi: 10.1016/j.vaccine.2021.03.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 387.Verger P., Dualé C., Lenzi N., Scronias D., Pulcini C., Launay O. Vaccine Hesitancy among Hospital Staff Physicians: A Cross-Sectional Survey in France in 2019. Vaccine. 2021;39:4481–4488. doi: 10.1016/j.vaccine.2021.06.053. [DOI] [PubMed] [Google Scholar]
- 388.Andrews G.J. ‘I Had to Go to the Hospital and It Was Freaking Me out’: Needle Phobic Encounter Space. Health Place. 2011;17:875–884. doi: 10.1016/j.healthplace.2011.04.012. [DOI] [PubMed] [Google Scholar]
- 389.Jenkins K., II Needle Phobia: A Psychological Perspective. Br. J. Anaesth. 2014;113:4–6. doi: 10.1093/bja/aeu013. [DOI] [PubMed] [Google Scholar]
- 390.Fernandes P.P. Rapid Desensitization for Needle Phobia. Psychosomatics. 2003;44:253–254. doi: 10.1176/appi.psy.44.3.253. [DOI] [PubMed] [Google Scholar]
- 391.Win N.N., Kohase H., Miyamoto T., Umino M. Decreased Bispectral Index as an Indicator of Syncope before Hypotension and Bradycardia in Two Patients with Needle Phobia. Br. J. Anaesth. 2003;91:749–752. doi: 10.1093/bja/aeg238. [DOI] [PubMed] [Google Scholar]
- 392.Turnage J.R., Logan D.L. Treatment of a Hypodermic Needle Phobia by in Vivo Systematic Desensitization. J. Behav. Ther. Exp. Psychiatry. 1974;5:67–69. doi: 10.1016/0005-7916(74)90017-2. [DOI] [Google Scholar]
- 393.Sokolowski C.J., Giovannitti J.A., Boynes S.G. Needle Phobia: Etiology, Adverse Consequences, and Patient Management. Dent. Clin. N. Am. 2010;54:731–744. doi: 10.1016/j.cden.2010.06.012. [DOI] [PubMed] [Google Scholar]
- 394.Noh I., Lee K., Rhee Y.S. Microneedle Systems for Delivering Nucleic Acid Drugs. J. Pharm. Investig. 2022;1:273–292. doi: 10.1007/s40005-021-00558-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 395.Nagarkar R., Singh M., Nguyen H.X., Jonnalagadda S. A Review of Recent Advances in Microneedle Technology for Transdermal Drug Delivery. J. Drug Deliv. Sci. Technol. 2020;59:101923. doi: 10.1016/j.jddst.2020.101923. [DOI] [Google Scholar]
- 396.Jiang P., Klemeš J.J., Van Fan Y., Fu X., Tan R.R., You S., Foley A.M. Energy, Environmental, Economic and Social Equity (4E) Pressures of COVID-19 Vaccination Mismanagement: A Global Perspective. Energy. 2021;235:121315. doi: 10.1016/j.energy.2021.121315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 397.Mallapaty S. China Is Vaccinating a Staggering 20 Million People a Day. Nature. 2021 doi: 10.1038/d41586-021-01545-3. [DOI] [PubMed] [Google Scholar]
- 398.Burki T.K. Challenges in the Rollout of COVID-19 Vaccines Worldwide. Lancet. Respir. Med. 2021;9:e42. doi: 10.1016/S2213-2600(21)00129-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 399.So A.D., Woo J. Special Paper: Reserving Coronavirus Disease 2019 Vaccines for Global Access: Cross Sectional Analysis. BMJ. 2020;371:m4750. doi: 10.1136/bmj.m4750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 400.Eccleston-Turner M., Upton H. International Collaboration to Ensure Equitable Access to Vaccines for COVID-19: The ACT-Accelerator and the COVAX Facility. Milbank Q. 2021;99:426–449. doi: 10.1111/1468-0009.12503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 401.Zaqout A., Daghfal J., Alaqad I., Hussein S.A.N., Aldushain A., Almaslamani M.A., Abukhattab M., Omrani A.S. The Initial Impact of a National BNT162b2 MRNA COVID-19 Vaccine Rollout. Int. J. Infect. Dis. 2021;108:116–118. doi: 10.1016/j.ijid.2021.05.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 402.Herishanu Y., Avivi I., Aharon A., Shefer G., Levi S., Bronstein Y., Morales M., Ziv T., Shorer Arbel Y., Scarfò L., et al. Efficacy of the BNT162b2 MRNA COVID-19 Vaccine in Patients with Chronic Lymphocytic Leukemia. Blood. 2021;137:3165–3173. doi: 10.1182/blood.2021011568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 403.Tauzin A., Nayrac M., Benlarbi M., Gong S.Y., Gasser R., Beaudoin-Bussières G., Brassard N., Laumaea A., Vézina D., Prévost J., et al. A Single Dose of the SARS-CoV-2 Vaccine BNT162b2 Elicits Fc-Mediated Antibody Effector Functions and T Cell Responses. Cell Host Microbe. 2021;29:1137–1150.e6. doi: 10.1016/j.chom.2021.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 404.Pellini R., Venuti A., Pimpinelli F., Abril E., Blandino G., Campo F., Conti L., De Virgilio A., De Marco F., Di Domenico E.G., et al. Initial Observations on Age, Gender, BMI and Hypertension in Antibody Responses to SARS-CoV-2 BNT162b2 Vaccine. EClinicalMedicine. 2021;36:100928. doi: 10.1016/j.eclinm.2021.100928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 405.Liu Y., Liu J., Xia H., Zhang X., Fontes-Garfias C.R., Swanson K.A., Cai H., Sarkar R., Chen W., Cutler M., et al. Neutralizing Activity of BNT162b2-Elicited Serum. N. Engl. J. Med. 2021;384:1466–1468. doi: 10.1056/NEJMc2102017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 406.He X., Chandrashekar A., Zahn R., Wegmann F., Yu J., Mercado N.B., McMahan K., Martinot A.J., Piedra-Mora C., Beecy S., et al. Low-Dose Ad26.COV2.S Protection against SARS-CoV-2 Challenge in Rhesus Macaques. Cell. 2021;184:3467–3473.e11. doi: 10.1016/j.cell.2021.05.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 407.Karim S.S.A., de Oliveira T. New SARS-CoV-2 Variants—Clinical, Public Health, and Vaccine Implications. N. Engl. J. Med. 2021;384:1866–1868. doi: 10.1056/NEJMc2100362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 408.Rodríguez-Espinosa D., Broseta J.J., Maduell F., Bedini J.L., Vera M. Humoral Response of the MRNA-1273 SARS-CoV-2 Vaccine in Peritoneal Dialysis Patients. Kidney Int. 2021;100:476. doi: 10.1016/j.kint.2021.05.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 409.Wu K., Werner A.P., Koch M., Choi A., Narayanan E., Stewart-Jones G.B.E., Colpitts T., Bennett H., Boyoglu-Barnum S., Shi W., et al. Serum Neutralizing Activity Elicited by MRNA-1273 Vaccine. N. Engl. J. Med. 2021;384:1468–1470. doi: 10.1056/NEJMc2102179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 410.Silva-Cayetano A., Foster W.S., Innocentin S., Belij-Rammerstorfer S., Spencer A.J., Burton O.T., Fra-Bidó S., Le Lee J., Thakur N., Conceicao C., et al. A Booster Dose Enhances Immunogenicity of the COVID-19 Vaccine Candidate ChAdOx1 NCoV-19 in Aged Mice. Med. 2021;2:243–262.e8. doi: 10.1016/j.medj.2020.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 411.Becerra-Flores M., Cardozo T. SARS-CoV-2 Viral Spike G614 Mutation Exhibits Higher Case Fatality Rate. Int. J. Clin. Pract. 2020;74:e13525. doi: 10.1111/ijcp.13525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 412.Zhang L., Jackson C.B., Mou H., Ojha A., Peng H., Quinlan B.D., Rangarajan E.S., Pan A., Vanderheiden A., Suthar M.S., et al. SARS-CoV-2 Spike-Protein D614G Mutation Increases Virion Spike Density and Infectivity. Nat. Commun. 2020;11:6013. doi: 10.1038/s41467-020-19808-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 413.Zhou G., Zhao Q. Perspectives on Therapeutic Neutralizing Antibodies against the Novel Coronavirus SARS-CoV-2. Int. J. Biol. Sci. 2020;16:1718–1723. doi: 10.7150/ijbs.45123. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
There are no additional raw data for this paper. The paper only uses secondary data from published papers, and all credits to these data have been made via citations and copyright permissions.