

Abstract
An increasing number of checkpoint inhibitor-induced subacute cutaneous lupus erythematosus events have been reported. We present the first case of nivolumab-induced discoid lupus erythematosus in a patient with hepatocellular carcinoma. The patient presents with violaceous hypopigmented plaques on the pinna bilaterally, hypopigmented plaques with central hyperpigmentation on the posterior neck, and other hypopigmented plaques on the face, forearms, and hands. For management, nivolumab was held for 2 months, and Plaquenil and topical steroids were added. Nivolumab was resumed with no further progression of DLE lesions and improvement of the skin. It is important to characterize cutaneous side effects to effectively manage them.
Keywords: Nivolumab, Checkpoint inhibitors, Discoid lupus erythematosus
Introduction
Immune checkpoint inhibitors are widely used to treat various cancers, including hepatocellular carcinoma (HCC) [1]. Nivolumab is a human monoclonal antibody targeted against programmed cell death protein 1 (PD-1) [2]. The interaction between PD-1 and programmed death ligand (PD-L1) provides a suppressive signal to T cells, leading to T-cell anergy or death [2]. Tumor cells can express PD-L1 in order to evade the immune system and inhibit the activity of cytotoxic T cells [1]. Hence, the inhibition of the PD-1 and PD-L1 interaction promotes an antitumor response. Nivolumab was FDA approved in 2017 and is typically used as a second-line treatment for HCC after the failure of sorafenib [2]. We present the first case of nivolumab-induced discoid lupus erythematosus in a patient with HCC.
Case Report/Case Presentation
A 61-year-old male with HCC presented with a skin rash after 21 months of nivolumab therapy. The patient had since been with cancer-free progression. The patient did not have any other side effects of nivolumab. The past medical history included hepatitis C, coronary artery disease, myocardial infarction, hypertension, and cervical radiculopathy.
On physical examination, violaceous hypopigmented infiltrated plaques were seen on the pinna bilaterally, in the conchal bowl (Fig. 1), and on the neck (Fig. 2). Additionally, there was a 1-cm indurated plaque on the left side of the posterior neck and hypopigmented macules were seen on the left neck. Confluent, hypopigmented plaques with central areas of hyperpigmentation appeared in a photodistributed pattern on bilateral posterior forearms along with significant follicular plugging and perifollicular repigmentation.
Fig. 1.

Patient at time of drug eruption. a The pinna with violaceous hypopigmented patches. b Hypopigmented patches with significant central hyperpigmentation on the posterior neck.
Fig. 2.

Patient 3 months after initial drug eruption. a Improvement of violaceous hypopigmented patches on the pinna. b Clearing of central hyperpigmentation on the posterior neck patches. c Hypopigmented patches on the forearms and dorsal hands.
Skin biopsy demonstrated lichenoid interface inflammation with numerous dyskeratotic keratinocytes, pigment incontinence, parakeratosis, follicular plugging, and a dermal perivascular lymphocytic infiltrate (Fig. 3, 4). Direct immunofluorescence tests for antibodies to IgG, IgA, IgM, C3, and fibrinogen were negative. The ANA titer was 1:80 and the C3 and C4 antibodies were normal.
Fig. 3.
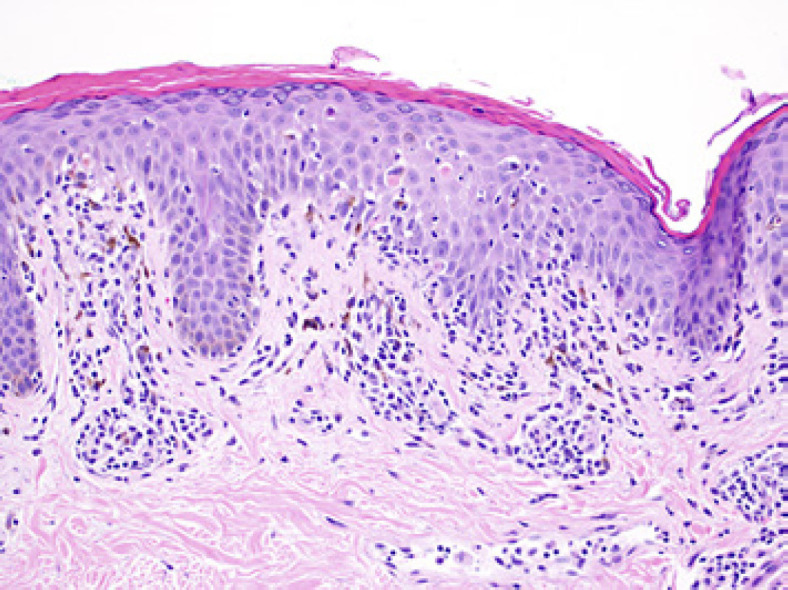
Image under 20 magnification of H and E showing lichenoid infiltrate and neutrophils in stratum corneum with thin elongated rete ridges.
Fig. 4.

Images under 10 magnification of H and E showing hyperkeratosis and follicular plugging.
Nivolumab was stopped following the drug reaction and the patient started hydroxychloroquine and topical steroids (topical clobetasol was used daily for a week followed by triamcinolone three times daily) along with sun protection. The symptoms improved by 80% after these measures. The patient was restarted on nivolumab 2 months after the initial eruption. At a follow-up visit 1 month later, there was notable clearing of the pinna and posterior neck; however, patches of hypopigmentation on the forearms and dorsal hands remained (Fig. 2). Anti-Ro and anti-histone antibodies were negative at this time.
Discussion/Conclusion
Previous case reports of nivolumab-induced subacute cutaneous lupus erythematosus (SCLE) include patients with metastatic non-small-cell lung cancer, stage IV melanoma, and ovarian carcinoma [1, 3, 4]. One case of bullous lupus was reported in a patient with lung cancer after nivolumab use [5]. In 1 case report from the UK, the use of another PD-1 inhibitor, pembrolizumab, was associated with a flare of discoid lupus erythematosus on the hands, face, and scalp that was initially diagnosed several years before [6]. We present the first case of nivolumab-induced discoid lupus erythematosus seen in a patient with HCC. Other adverse events associated with nivolumab include maculopapular rash, pruritis, vitiligo, and lichenoid skin reactions to name a few [1].
The pathogenesis of drug-induced lupus erythematosus is multifactorial, involving genetic predisposition, drug transformation, and dysregulation of adaptive immune cells [7]. Drugs implicated in triggering SCLE include calcium channel blockers, proton-pump inhibitors, hydrochlorothiazide, and terbinafine [7]. The loss of central tolerance in T and B cells can lead to autoreactive T cells or B cells, favoring an autoimmune state [7]. However, the specific mechanism of nivolumab-induced cutaneous lupus erythematosus has not been widely studied. It is proposed that generalized activation of the immune system caused by nivolumab may be associated with autoimmune disorders such as lupus erythematosus and rheumatoid arthritis [8]. The onset of general drug-induced lupus erythematosus can occur after drug exposure between a month and a decade [9]. However, the timeframe of nivolumab-induced SCLE is not well studied. Our patient presented with cutaneous symptoms 21 months after beginning nivolumab therapy. Another case series reported nivolumab-associated SCLE after 20 months in a patient with small cell lung cancer [10]. Patients treated with nivolumab may experience a long exposure before the onset of a cutaneous drug reaction; however, further research is needed to explore this.
In our patient, we used hydroxychloroquine and topical steroids along with sun protection, as is done in conventional DLE patients. This facilitated the patient to be restarted on nivolumab. Further research is warranted to understand the pathogenesis of nivolumab-induced discoid lupus erythematosus and therapeutic options. Overall, it is important for clinicians to be aware of this potential complication of nivolumab use. It is critical to biopsy skin lesions and look for serological evidence to better understand checkpoint inhibitor-induced cutaneous side effects. This also lets us use individualized therapy so that patients can continue their life-saving medications.
Statement of Ethics
A case report involving no more than one individual is not a systematic investigation and does not meet the Federal Policy for the Protection of Human Subjects definition of “research.” Hence, this case report did not require IRB and ethical approval in accordance with guidelines. Written informed consent was obtained from the patient for publication of the medical case and accompanying images.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
There were no funding sources utilized.
Author Contributions
Jaya Manjunath, Mark Mochel, and FNU Nutan participated in the interpretation of the case, drafting of the case report, and critical revisions.
Data Availability Statement
All data generated or analyzed during this study have been included in this article. Any further inquiries can be directed to the corresponding author.
References
- 1.Zitouni NB, Arnault J-P, Dadban A, Attencourt C, Lok CC, Chaby G. Subacute cutaneous lupus erythematosus induced by nivolumab: two case reports and a literature review. Melanoma Res. 2019;29((2)):212–5. doi: 10.1097/CMR.0000000000000536. [DOI] [PubMed] [Google Scholar]
- 2.Finkelmeier F, Waidmann O, Trojan J. Nivolumab for the treatment of hepatocellular carcinoma. Expert Rev Anticancer Ther. 2018;18((12)):1169–75. doi: 10.1080/14737140.2018.1535315. [DOI] [PubMed] [Google Scholar]
- 3.Liu RC, Sebaratnam DF, Jackett L, Kao S, Lowe PM. Subacute cutaneous lupus erythematosus induced by nivolumab. Australas J Dermatol. 2018;59((2)):e152–4. doi: 10.1111/ajd.12681. [DOI] [PubMed] [Google Scholar]
- 4.Kosche C, Owen JL, Choi JN. Widespread subacute cutaneous lupus erythematosus in a patient receiving checkpoint inhibitor immunotherapy with ipilimumab and nivolumab. Dermatol Online J. 2019;25((10)) [PubMed] [Google Scholar]
- 5.Wouters A, Durieux V, Kolivras A, Meert A-P, Sculier J-P. Bullous lupus under nivolumab treatment for lung cancer: a case report with systematic literature review. Anticancer Res. 2019;39((6)):3003–8. doi: 10.21873/anticanres.13432. [DOI] [PubMed] [Google Scholar]
- 6.Blakeway EA, Elshimy N, Muinonen-Martin A, Marples M, Mathew B, Mitra A. Cutaneous lupus associated with pembrolizumab therapy for advanced melanoma: a report of three cases. Melanoma Res. 2019 Jun;29((3)):338–41. doi: 10.1097/CMR.0000000000000587. [DOI] [PubMed] [Google Scholar]
- 7.He Y, Sawalha AH. Drug-induced lupus erythematosus: an update on drugs and mechanisms. Curr Opin Rheumatol. 2018;30((5)):490–7. doi: 10.1097/BOR.0000000000000522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aburahma A, Aljariri Alhesan N, Elounais F, Abu Sitta E. Antiphospholipid antibody induced by nivolumab. Case Rep Hematol. 2018 Jan 11;2018:3106852. doi: 10.1155/2018/3106852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dalle Vedove C, Simon JC, Girolomoni G. Drug-induced lupus erythematosus with emphasis on skin manifestations and the role of anti-TNFα agents. J Dtsch Dermatol Ges. 2012;10((12)):889–97. doi: 10.1111/j.1610-0387.2012.08000.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bui AN, Hirner J, Singer SB, Eberly-Puleo A, Larocca C, Lian CG, et al. De novo subacute cutaneous lupus erythematosus-like eruptions in the setting of programmed death-1 or programmed death ligand-1 inhibitor therapy: clinicopathological correlation. Clin Exp Dermatol. 2021 Mar;46((2)):328–37. doi: 10.1111/ced.14449. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study have been included in this article. Any further inquiries can be directed to the corresponding author.