

Abstract
Background
Being “positive” has been one of the most frustrating words anyone could hear since the end of 2019. This word had been overused globally due to the high infectious nature of SARS-CoV-2. All citizens are at risk of being infected with SARS-CoV-2, but a red warning sign has been directed towards cancer and immune-compromised patients in particular. These groups of patients are not only more prone to catch the virus but also more predisposed to its deadly consequences, something that urged the research community to seek other effective and safe solutions that could be used as a protective measurement for cancer and autoimmune patients during the pandemic.
Aim
The authors aimed to turn the spotlight on specific herbal remedies that showed potential anticancer activity, immuno-modulatory roles, and promising anti-SARS-CoV-2 actions.
Methodology
To attain the purpose of the review, the research was conducted at the States National Library of Medicine (PubMed). To search databases, the descriptors used were as follows: “COVID-19”/”SARS-CoV-2”, “Herbal Drugs”, “Autoimmune diseases”, “Rheumatoid Arthritis”, “Asthma”, “Multiple Sclerosis”, “Systemic Lupus Erythematosus” “Nutraceuticals”, “Matcha”, “EGCG”, “Quercetin”, “Cancer”, and key molecular pathways.
Results
This manuscript reviewed most of the herbal drugs that showed a triple action concerning anticancer, immunomodulation, and anti-SARS-CoV-2 activities. Special attention was directed towards “matcha” as a novel potential protective and therapeutic agent for cancer and immunocompromised patients during the SARS-CoV-2 pandemic.
Conclusion
This review sheds light on the pivotal role of “matcha” as a tri-acting herbal tea having a potent antitumorigenic effect, immunomodulatory role, and proven anti-SARS-CoV-2 activity, thus providing a powerful shield for high-risk patients such as cancer and autoimmune patients during the pandemic.
Keywords: SARS-CoV-2, herbal drugs, autoimmune diseases, nutraceuticals, cancer
Introduction
In October 2007, a warning letter was issued but no one responded (1). The warning letter was issued by Cheng and his colleagues mentioning that “Horseshoe bats resemble a large reservoir for SARS-CoV-like and the possibility of its reemergence with another novel virus should be taken into consideration because it is a time bomb” (1). The warning letter became a reality 12 years later in December 2019; the city of Wuhan in China experienced the emergence of a novel coronavirus that was initially called “Wuhan pneumonia” (2). It was further classified by the WHO on March 11, 2020 as the 5th documented pandemic since the 1918 Spanish flu pandemic (H1N1) (3).
SARS-CoV-2 has been the main cause of death in 2020 and 2021, accounting for more than 5 million deaths (4). Upon stratification of the mortality lists and the morbidity rates around the globe, several observations have been observed (5). Cancer and autoimmune patients such as those with asthma (6), rheumatoid arthritis (RA) (7), multiple sclerosis (MS) (8), and systemic lupus erythematosus (SLE) (7) were reported to be among high-risk patients during the pandemic (9).
In the case of cancer patients, their chemotherapy-induced immune-compromised status puts them at a higher risk to be easily infected by the virus, and at the same time, such patients should receive their treatment protocols to avoid complications from their oncological diseases (10, 11). Several reports from China (12–14), United States (15), and Italy (16–18) confirmed that cancer patients are at very high risk of developing severe complications upon SARS-CoV-2 infection. Among cancer patients, those with lung cancer are the least fortunate as it was reported that the highest incidence of comorbidity with SARS-CoV-2 was in lung cancer patients (19). Consequently, such patients experience severe symptoms of SARS-CoV-2 that may require intensive care admission and mechanical ventilation, or could result in loss of life (11). This issue encouraged oncological societies such as the European Association for Medical Oncology (ESMO) (20), the American Society of Clinical Oncology (ASCO), the National Comprehensive Cancer Network (NCCN), and many others to provide new guidelines for cancer patients’ treatment protocols and diagnostic tests during the pandemic (20). The main ideology behind the new guidelines is to calculate the benefit:risk ratio and categorize cancer patients into high, medium, and low priority based on Ontario Heath Cancer Care as previously reviewed in (21).
The same goes for patients suffering from autoimmune disorders where their immune-compromised status puts them at a higher risk of infection by the virus and developing more severe symptoms (22). In addition, their treatment protocols are mainly dependent on immunomodulatory disease-modifying therapies (DMTs) including glucocorticoids and immunosuppressants that are mainly prescribed to mitigate the immune attacks towards their normal body organs (22). For instance, a study focused on MS patients highlights that younger MS patients with lower socioeconomic status are at a higher risk of exposure to an unfavorable course of SARS-CoV-2 infection (23). In the case of SLE patients, it was first predicted that hydroxyl-chloroquine in their treatment protocol might provide a type of protection from COVID-19 complications (24). Yet, preliminary results from the clinics showed total opposite morbidity and mortality rates (25, 26). Mathian’s group reported that SLE patients also showed a high incidence of severe and even fatal cases of infection, confirming that, despite the co-treatment of SLE patients with antimalarial drugs, a high risk of unfavorable infection course has still been witnessed among SLE patients (25). Also, a more coherent study that included 417 SLE patients showed that the morbidity rates are moderately higher in the case of SLE patients (7).
Therefore, it is highly recommended that rheumatologists and oncologists encourage their patients to continue their ongoing treatment to avoid dangerous flare-ups of their autoimmune diseases or complications of their oncological diseases. It is imperative for those patients to have a nutritional plan that shields them from SARS-CoV-2 infection and at the same time improves their autoimmune status in the case of autoimmune patients and/or provide antitumor actions in the case of cancer patients.
In this review, we will show a glimpse of all the therapeutical trials that were carried out during the last couple of years to decrease the socioeconomic burden of such a pandemic. Yet, several failed attempts were witnessed starting from repurposing of conventional drugs, discovery of new medications that might take years of validation, to several vaccination approaches that go in parallel with the high viral mutational capacity (27, 28). However, less attention was given to the ideal remedy—”herbal drugs”—that might be the ultimate route to treat such deadly disease.
In this review, the authors will try to emphasize the significance of herbal drugs that should not be less than that of vaccines and antivirals during the pandemic. Herbal drugs have an edge regarding high-risk patients (cancer and autoimmune patients) in that they might play a dual/triple role in alleviating the primary disease and act as a protective shield during the pandemic.
Upon focusing on the herbal products with their immense roles starting from being antioxidants and holding anti-inflammatory and antiviral activities, we had a closer look at “matcha”, which we expect to have a great impact in the upcoming years because of its potent immune-modulatory capabilities and its recent validated activity against SARS-CoV-2 (29, 30). Nonetheless, matcha was also reported to hold a lot of promise for cancer (31, 32) and autoimmune patients (33, 34). Yet, in this review, the authors shed light on the research gap concerning the molecular mechanism of actions underlying matcha as a potent immunomodulatory, anticancer, and antiviral activity.
Methodology
In this review, the authors screened literature covering the therapeutic effects of “matcha” as a SARS-CoV-2 antiviral herbal drug; this review also focused on the anticancer activity and immunomodulatory role of “matcha”. To attain the purpose of the review, research was conducted at the States National Library of Medicine (PubMed). For the search in databases, the descriptors used were “COVID-19”/“SARS-CoV-2”, “Herbal Drugs”, “Autoimmune diseases”, “Rheumatoid Arthritis”, “Asthma”, “Multiple Sclerosis”, “Systemic Lupus Erythematosus” “Nutraceuticals”, “Matcha”, “Green tea”, “EGCG”, “Quercetin”, “Cancer”, and key molecular pathways. Research papers, books, and published data were reviewed for their relevance to the aim of the review and summarized. Criteria for inclusion were complete, relevant publication, available online, in English, published between 1997 and 2022, and with detailed information about participants, methods, and analyses. Data collection was performed, and data abstracted were in the form of descriptive information, covering the type of samples used, techniques, and findings or effects reported. Bias was limited through the evaluation of the studies through their internal validity rather than the conclusion.
SARS-CoV-2 Structure and Life Cycle
SARS-CoV-2 has a spherical shape with a positive single-strand RNA composed of approximately 30,000 nucleotides and enclosed inside a capsid (35). The genome encodes four structural proteins and many non-structural proteins (nsp) as previously reviewed (36, 37). The structural proteins are Spike (S) protein, Envelope (E) protein, Membrane (M) protein, and Nucleocapsid (N) protein. Inside the capsid, there is a nuclear capsid or the N protein, which is bound to the positive single-stranded RNA and coating it as demonstrated in Figure 1 . The SARS-CoV-2 life cycle is briefly described in Figure 2 , since it has been extensively discussed and reviewed in previous reviews (35, 38).
Figure 1.
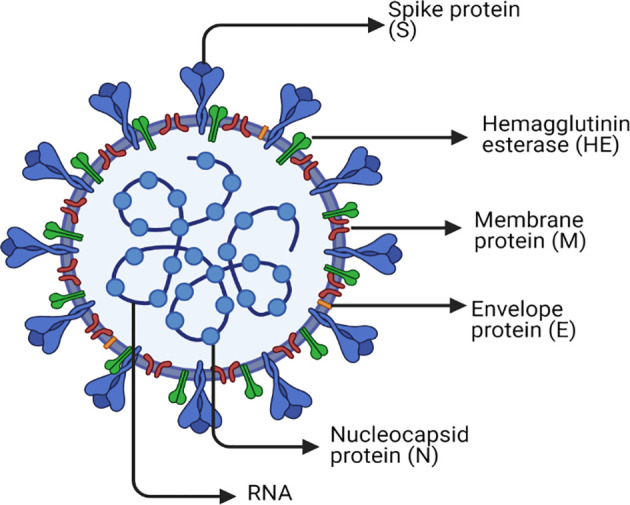
SARS-CoV-2 structure. The figure represents a graphical representation of the viral structural proteins spike (S), envelope (E), and membrane (M), which are embedded in the lipid surface. The positive single-stranded RNA is bound to the nucleocapsid protein (N) in the core of the capsid. Each one of these proteins plays a crucial role in the replication life cycle of the virus. The spike protein (S) is the master that supports the attachment and entry of host cell via fusion. The nucleocapsid protein (N) is the one used in transcription, which is included in the replication cycle. The membrane protein (M) that is most abundant on the viral surface drives the viral assembly. Furthermore, the envelope protein (E) has an indispensable role in assembly, host cell membrane permeability, and interactions between the host and virus. Another surface protein is Hemagglutinin esterase dimer (HE) that is found to play a role in cell entry and its infection without having a role in the replication process itself. Finally, the lipid envelope encircles the approximately 30,000 nucleotides, which is the genome of the virus encoding its four structural and many nonstructural proteins (nsp).
Figure 2.

SARS-CoV-2 life cycle and the repurposed drugs targeting specific stages throughout its life cycle. This figure represents a schematic description for the SARS-Cov-2 life cycle with the repurposed drugs targeting specific stages in it. ACE2 receptor on the lung cells is targeted by the RBD of the S1 region in the viral spike protein; however, this binding could be targeted by chloroquine and hydroxychloroquine, recombinant ACEII receptor, or ACEII inhibitors. After the attachment, transmembrane protease serine 2 (TMPRSS2) of the host cell makes a proteolytic cleavage between S1 and S2 subunits, thus separating RBD from the fusion domains, yet this step could be targeted by camostat mesylate and Umifenovir. Consequently, a major step is taken, which is the exposure of fusion peptide domain, enabling the virus to fuse with the cell and pave its way by endocytosis then enclosed in an acidified endosome. Proteasomes then act on the nucleocapsid protein (N), uncoating it and releasing the genetic material freely in the cytoplasm, but this can be inhibited by chloroquine and hydroxychloroquine due to rendering alkaline endosomal PH. Once the positive strand becomes free, translation of the open reading frame 1a/b and production of polyproteins pp1a and pp1ab takes place. The polyproteins undergo cleavage by the viral proteases Papain like protease (PLpro) and Chemotrypsin like protease (3C like protease or 3CLpro or Mpro). Lopinavir/Ritonavir and Darunavir/Cobicistat are the ones used to inhibit 3CLpro. On the other hand, the transcription process start since the Replication/Transcription complex (RTC) was translated, and at this point, there are many nucleoside analogue drugs that were repurposed for inhibiting RNA-dependent RNA polymerase (RdRp) such as Ribavirin, Favipiravir, Remdesivir, and Penciclovir. The RTC will supervise the formation of double membrane vesicle structures (DMV) in the cytoplasm to shield the transcription process. The positive strand is used as a template for making the negative strand, which is then transcribed to make more positive strands. Moreover, subgenomic mRNAs are produced by discontinuous transcription for the sake of being translated to form the 4 viral structural proteins. Once N protein is finished, it combines with a new positive strand for the nucleocapsid to be done. However, S, E, and M proteins proceed to the endoplasmic reticulum (ER) and then to the Golgi apparatus. Last but not least, both the nucleocapsid and structural proteins will be assembled at the ER-Golgi intermediate compartment (ERGIC) to the viral envelope followed by exocytosis of mature virions through smooth-walled vesicles. Many immune components can be released during the whole process such as IL-6, leading to a cytokine storm, so the monoclonal antibody Tocilizumab is used as well as the Toll-like receptor (TLR) inhibitors chloroquine and hydroxychloroquine.
Failed Trials to Handle the Pandemic
The current pandemic has urged the public health systems and pharmaceutical companies to develop new antiviral drugs and vaccines against SARS-CoV-2 after being the leading cause of death recently. In an attempt to find effective treatment for COVID-19 patients, enormous efforts were exerted in handling the pandemic. Several approaches were considered such as repurposing of FDA-approved drugs where the doctors were permitted to carry out such clinical trials using a combination of these drugs due to the urgent need to reduce cost, time, and risk of the drug development processes, but this was accompanied by several side effects and limitations as shown in Table 1 . Thus, not all the repurposed drugs have been approved to be used in ameliorating this pandemic, and some of them were suspended by WHO such as chloroquine, hydroxychloroquine, remdesivir, and lopinavir/ritonavir (74). It is also important to note that all clinical trials highlighted in Table 1 do not include any of the high-risk patients like cancer and autoimmune patients, who are the main concern of this review.
Table 1.
A list of currently available drugs for the treatment of SARS-CoV-2.
| Drug | No. of Clinical Trial | Clinical Trial Status | No. of Participants | Participants’ Average Age | Participants’ Status | Intervention | Results | Side Effects | Limitations | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| Ribavirin | NCT04551768 | Completed | 51 | >18 years | Hospitalized | -50 mg/ml over 1 h, 2 times/day for 6 days -100 mg/ml over 30 min 2 times/day for 6 days |
Pending | -Hemolytic anemia -Fatigue -Skin Rash -Leukopenia -Teratogenicity |
-Excision ability of false nucleotides acquired to coronaviruses by nsp14 | (39–42) |
| Favipiravir | NCT04694612 | Completed (Published Results) |
30 | 52.5 | Hospitalized | Baloxavir/Marboxil + existing treatment: 80 mg/day on days 1 and 4 Favipavir + existing treatment: 1,600 or 2,200 mg then 600 mg 3 times/day Control: existing treatment |
-No extra advantage on using Favipiravir -More vigorous clinical trials are needed to be approved for its international use |
-Elevation of liver enzymes -Nausea -Vomiting |
-Safety concerns about QT prolongation -Teratogenic potential is unclear |
(39, 43–45) |
| Remdesivir | NCT04280705 | Completed (Published Results) |
1,062 | ≥18 years | Hospitalized | Remdesivir or Placebo, 200 mg IV on day 1 then 100 mg once/day for 10 days | No notable benefit specially for mild to moderate diseased patients at day 28 | -Worsened respiratory problems -Nausea -Constipation -High alanine aminotransferase levels |
-High mortality rate -Not sufficient as sole antiviral treatment -No improvement in mortality, time of virus clearance or time of clinical improvement |
(46–48) |
| NCT04871633 | Completed | 66 | >12 years | Hospitalized | Remdesivir IV 200 mg followed by 100 mg/day for 5–10 days | Pending | N/A | N/A | ||
| Camostat mesylate | NCT04321096 | Recruiting | 580 | ≥18 years | Hospitalized/Outpatients | Placebo: 2 pills 3 times/day for 5 days Camostat mesylate: 2 × 100 mg pills 3 times daily for 5 days |
Pending | -Skin rash -Pruritus -Abdominal discomfort -Elevation of liver enzymes |
-Early treatment initiation at the first phase of infection is needed | (49–51) |
| NCT04608266 | Recruiting | 596 | ≥18 years | No initial hospitalization requirement | Placebo: 2 tablets every 8 h for 14 days Camostat mesylate: 2 × 100 mg tablets every 8 h for 14 days |
Pending | N/A | N/A | ||
| Darunavir | NCT04252274 | Recruiting | 30 | Child, Adult, Older adult | N/A | Darunavir and cobicistat one tablet/day for 5 days + conventional treatments Conventional treatment only |
Pending | -Increasing risk of cardiovascular diseases with increased exposure | -Well established pharmacological profile is needed | (49, 52, 53) |
| Lopinavir/Ritonavir | NCT04252885 | Completed | 86 | 18–80 years | N/A | -Lopinavir (200 mg) and ritonavir (50 mg) 2 tablets each, q12h, for 7-14 days +standard therapy -Arbidol (2 × 100 mg) tid, for 7-14 days +standard therapy -Standard treatment |
Pending | -Diarrhea -Nausea -Asthenia |
-Further safety profile is needed -No significant improvement in mortality rate, viral load reduction or on clinical level |
(54) |
| Chloroquine/Hydroxychloroquine | NCT04322123 | Active; not recruiting | 630 | ≥18 years | Hospitalized | Hydroxychloroquine 400 mg BID for 7 days -Hydroxychloroquine 400 mg BID + azithromycin 500 mg once a day -Standard treatment protocol |
Pending | -Cardiac arrest -QT prolongation -High rate of hospital deaths |
-Narrow therapeutic index -Cardiac toxicity -Safety and efficacy proofs are needed |
(55–59) |
| Nitazoxanide | NCT04486313 | Completed | 1,092 | 12–120 years | N/A | Nitazoxanide, 2 × 300 mg tablets BID with food for 5 days -Placebo, 2 tablets BID with food for 5 days |
Pending | -Abdominal cramps -Diarrhea |
-Further evidence is required or hepatorenal -Cardiac toxicity -Teratogenic effects |
(60) |
| Umifenovir | NCT04260594 | Completed | 236 | 18–65 years | N/A | -Arbidol 2 tablets, tid for 14–20 days -Ordinary treatment |
Pending | -Nausea -Vomiting |
-Limited safety and efficacy documents | (61) |
| ACE II inhibitors | NCT04364893 | Recruiting | 700 | ≥18 years | Hospitalized | - ACEI/ARBs discontinuation - ACEI/ARBs continuation |
Pending | -Inflammatory lung diseases -Impaired lipid and glucose metabolism -Cardiac toxicity -Renal malfunction -Impaired immunity |
-Negative impact on associated comorbidities as diabetes and hypertension | (62–64) |
| Recombinant ACE II | NCT04382950 | Not yet recruiting | 24 | 18–60 years | N/A | -rbACE2 IV 0.4 mg/kg BID for 7 days + Aerosolized 13 cis retinoic acid from 0.2 mg/kg/day to 4 mg/kg/day -Standard therapy |
Pending | -Hypotension -Acute kidney injury |
-More preclinical and clinical studies are still needed -Effective only at the early stage of infection |
(65, 66) |
| Convalescent Plasma | NCT 04343261 | Completed/Has results | 48 | 18–90 years | N/A | 2 convalescent plasma infusions (2 × 200 ml) each for 1 h | -No significant change in number of days required to discharge, between testing positive and receiving plasma and same for those who died | N/A | -No improvement for critical cases -Finding suitable donors -Disease transmission risk |
(67–70) |
| Tocilizumab | NCT04356937 | Completed/Has results | 243 | 18–85 years | Hospitalized | -IV at dose 8 mg/kg + standard therapy - IV at dose 4 mg/kg + standard therapy |
-Failure in death or intubation prevention in moderately ill hospitalized patients | -Septic shock -GIT perforations -Leukopenia -Lymphopenia |
-High cost -Opportunistic infections risk -More studies are required |
(39, 71–73) |
Throwing light on the currently available vaccines’ effectiveness, it was reported that only 30.7% protection was acquired against the new variants of concern “delta” when compared to the “alpha” variant of the virus, which has provided 48.7% protection from a single dose of either BNT162b2 or ChAdOx1 nCoV-19 vaccines (75). However, two doses from these vaccines give a 93.7% protection against alpha and 88% protection against delta for BNT162b2, while for ChAdOx1 nCoV-19, it has an efficacy of 74.5% against alpha vs. 67% for delta (76). For the Pfizer/BioNTech vaccine efficiency, it has 88% protection against the alpha variant, and this percentage has significantly decreased against delta (76). Nonetheless, it was reported that certain mutations were identified in the most recent “omicron” variant that led to higher transmission ability, higher infectivity and binding affinity to ACE2 receptors, and increase in the failure of neutralizing antibodies and immune defense (77). Therefore, relying only on the significance of vaccinations to rescue us from such virulent variants is not a wise solution, especially since it has been well documented and experienced that the vaccines developed against the wild SARS-CoV-2 have lower efficiency rates against the mutated variants (78). Collectively, it has to be recognized that at this stage, vaccine development is important, but still the nourishment of our immune systems has a greater weight in fighting this ongoing pandemic.
After shedding light onto the evolution of new variants of SARS-CoV-2, it is essential to recall the long-lasting Influenza A virus as a live example, which can be compared in parallel with SARS-CoV-2 nowadays. The Influenza A virus causes one of the annual epidemics; even so, it continues to represent a significant threat to global public health due to its very high mutation rates and its ability to cross-transmit between species (79). The same scenario applies where Influenza A rapid evolution resulted in the loss of optimal efficacy for vaccines and antiviral drugs, to which the virus became resistant and thus complete eradication was not achieved (79). As a result, the scientific communities were compelled to use natural therapies and herbal products to boost the immune system as an alternative plan, which showed great success. Some of these herbal products include licorice roots, pomegranate, guava tea, vitamin C supplements, and zinc supplements (80).
Current Status of Cancer Patients and Autoimmune Patients After the Emergence of SARS-CoV-2 Variants of Concerns
Focusing on cancer patients and patients with autoimmune diseases, there are several studies that showed impaired antibody responses following dual COVID-19 vaccination in patients with chronic lymphocytic leukemia (81) and lung cancer (82). Furthermore, it was proved that humoral protection against the delta variant is markedly impaired among chronic lymphocytic leukemia patients, indicating the urgent need for further optimization of immune protection in this patient cohort (81). Yet, not enough data were reported about the status humoral protection for patients with autoimmune diseases.
Herbal Drugs: From Passenger to Driver Seat During the Pandemic
Applying the concepts of ancient people about natural remedies in defending against colds and flu ensures that natural products were always side by side with any respiratory viral infection (83, 84). By now, most of the population had experienced the impaired protection of the currently available drugs against SARS-CoV-2 and vaccines due to the high rate of naturally occurring mutations. Consequently, a noteworthy concept is that we need an immune-modulatory and broad-spectrum antiviral agent with diverse mechanisms of action that can be readily used for the prevention of future pandemics. In this review, the authors will focus on candidates from herbal medicines exerting their immunomodulatory and antiviral effects especially for immune-compromised COVID-19 patients, and a special focus on the Japanese green tea “matcha” will be addressed. It is also worth mentioning that several reviews had shed light onto the potent role of natural compounds in the prevention of and/or as an adjunct treatment for COVID-19 (85–88). Yet, this review focuses on the tri-acting natural compounds that possess anticancer, immunomodulatory, and anti-SARS-CoV-2 activities, which were proposed as protective shields for cancer and autoimmune patients in particular during the pandemic.
Candidates from Herbal Medicine During the Pandemic
In this section, the authors will focus on candidates from the herbal medicine field that have been suggested to be used during the pandemic. During the last couple of years, a huge number of herbal medicines have been suggested as anti-SARS-CoV-2 agents, for example, purple coneflower, the bark of cinchona trees, Java turmeric, ashwagandha leaves, ginger, turmeric, garlic, flaxseed, tick berry leaves, oregano, elderberry, green tea, orange, and citrus peel as previously reviewed in (89, 90).
This review focuses on natural compounds that possess a triple action including anticancer, immunomodulatory, and anti-SARS-CoV-2 activities as listed below and as summarized in Table 2 . The inclusion criteria include natural compounds that possess the 3 activities, with a known mechanism of action and molecular targets, and entered clinical trials in the case of anti-SARS-CoV-2 herbal drugs. A detailed list of natural compounds that entered clinical trials as anti-SARS-CoV-2 agents is shown in Table 3 . The exclusion criteria used in this review include natural compounds that possess only one of the above-mentioned actions, and/or unknown mechanism of action.
Table 2.
Tri-acting (anticancer, immunomodulatory, and anti-SARS-CoV-2) natural products.
| Natural Product | Active Constituent | Anti cancer Mechanism of Action | Immunomodulatory Mechanism of action | Anti-SARS-CoV-2 Mechanism of action | Ref. |
|---|---|---|---|---|---|
| Ginger | 6-gingerol 6-shogaol 10-gingerol |
-Induction of apoptosis by increasing caspase-3/7 in gastric cancer cells -Downregulation of cytosolic inhibitor of apoptosis (cIAP)-1 in gastric cancer cells -Inhibition of TRAIL-induced nuclear factor-kappaB (NF-κB) activation in gastric cancer cells |
-Inhibiting the expression of inducible nitric oxide synthase (iNOS) and cyclooxygenase-2 (COX-2) in macrophages in multiple sclerosis -Inhibiting LPS-induced NO and production of pro-inflammatory cytokines by inhibiting the NF-kB activation in BV2 microglial cells in multiple sclerosis |
-Inhibition of binding between S protein and ACE2 in silico | (91–95) |
| Turmeric | Curcumin | -Upregulation of miRNA-192-5p and suppression of PI3K/Akt signaling pathway in non-small cell lung cancer | -Reduced levels of pro-inflammatory cytokines (TNF-α and IL-1β) in the serum and synovial fluid in adjuvant-induced arthritis in rats -Regulates the cyclooxygenase (COX) and lipoxygenase (LOX) enzymes, leading to the suppression of various pro-inflammatory mediators, including MMP9 and MMP13 in arthritis -Inhibition of IL-12 signaling pathway in T cells in multiple sclerosis. |
-Inhibition of Toll-like receptors, NF-κB, inflammatory cytokines and chemokines, and bradykinin, decreasing SARS-CoV-2 symptoms | (96–104) |
| Garlic | Diallyl disulfide (DADS) Alliin |
-Proapoptotic effect by histone deacetylation, inhibition of ERK, activation of SAPK/JNK, and p38 pathways in MCF-7 breast cancer cells. | -Suppression of LPS inflammatory signals by generating an anti-inflammatory gene expression and preventing the increase in expression of pro-inflammatory cytokines IL-6 and MCP-1 in LPS induced inflammation in 3T3-L1 adipocytes. | -Attenuation of coronavirus infection by dual S-thioallylation of SARS-CoV-2 Mpro in silico | (105–113) |
| Flaxseed | Omega 3 | Upregulation of BAX, downregulation of Bcl-2 and increase in DNA fragmentation in acute myeloid leukemia. | -Reducing the level of antibodies (anti-dsDNA), interleukins (IL-1α, IL-1β, and IL-2) and TNF-α in systemic lupus erythematous. | -Incorporation of Omega-3 in phospholipid bilayer of cell membranes leading to production of less pro-inflammatory mediators. | (114–116) |
| Citrus fruits | Hesperidin | -Induction of tumor suppressor miR-486-5p and repression of oncogenic long non-coding RNA H19 in breast cancer -Repression of metastatic mediator ICAM-1 in breast cancer |
-Suppression of the levels of IL-4, IL-5, IL-13, and IgE levels in serum in mouse model for asthma -Increase the Treg cells production of interleukin IL-10, transforming growth factor (TGF-β), reduction in production of IL-17 and IL-6, decrease in the percentages of Th17 cells, % of Treg cells in the spleen and lymph nodes, reduces ROR-γt factor expression, but enhanced Foxp3 expression in mouse model for multiple sclerosis |
-Binding to the TMPRSS2 and ACE2 and block the viral entry in silico | (117–120) |
| Black tea | Theaflavins Theaflavin-3, 3’-digallate (TFDG) |
-Reduction in tumor-induced angiogenesis by downregulation of VEGF and HIF-1a in ovarian cancer cells | -Inhibiting the activation of NF-κB- and MAPK-signaling pathways in Rheumatoid arthritis. | -Blockage of viral RNA-dependent RNA-polymerase by in silico docking. | (121–125) |
| Green tea | EGCG Quercetin |
-Decrease Bcl-2 expression, increase expression of caspase 3 and Bax in esophagus cancer -Induction of apoptosis and downregulation of PI3K, PKC, COX-2, and ROS. Increased expression of p53 and Bax in liver cancer. |
-Reducing IgE and histamine levels, Decreasing FcϵRI expression, regulating the balance of Th1/Th2/Th17/Treg cells and inhibiting related transcription factors in asthma. | -Inhibition of Mpro by in silico studies -Inhibition of 3CLpro and PLpro by in silico studies |
(126–132) |
| Tripterygium wilfordii Hook. F. | Extract Triptolide |
-Accumulation has a small of p53 and apoptotic cell death in human prostatic epithelial cells - The sensitivity of gemcitabine-resistant cells to cisplatin treatment is enhanced by activation of mitochondria-initiated cell death pathway and suppression of HSP27 expression in pancreatic cells |
NF-κB, NF-κB/TNF-α/vascular cell adhesion molecule-1, and TGF-β1/α-smooth muscle/vimentin signaling pathways induced by TNFs and TLR4 in rheumatoid arthritis -Downregulation of p38 MAPK and NF-κB signaling pathways in neuroinflammation |
N/A | (133–136) |
| Eucalyptus globulus Labill. | Extract 1,8-Cineol |
-Suppresses the proliferation of human colon cancer cells by inducing apoptosis | -Reduces the expression of NF-κB target gene MUC2 in asthma | -Inhibition of Mpro in silico. | (137–139) |
Table 3.
Herbal drugs in clinical trials against SARS-CoV-2.
| Naturalcompound | Type | Dosage form | Clinical Trial No. | Results | Dose | Mechanism of action | Therapy type | Phase | No. of participants | Clinical trial state | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Echinacea purpurea | Nutraceuticals | Tablets (Echinaforce) |
NCT05002179 | Pending | Prevention: 800 mg 3 times/day Treatment: 800 mg 5 times/day |
N/A | Primary therapy | Phase IV | 122 | Completed | (140) |
| Ashwagandha, Giloy, and Tulsi combination (Ayurveda Intervention) |
Traditional medicine | Tablets | NCT04716647 | Pending | Ashwagandha: Doses range from 250 mg to 5 g Giloy: Doses range from 500 mg to 1 g Tulsi: Doses range from 500 mg to 1 g |
- Inhibitor of the main protease (Mpro or 3Clpro) - Inhibition of the TMPRSS2/ACE II complex |
Primary therapy | N/A | 28 | Completed | (141, 142) |
| Turmeric | Nutraceuticals | Tablets (NASAFYTOL) |
NCT04844658 | Pending | 1008 mg 8 times/day |
- PLpro inhibitor | Supportive therapy | N/A | 51 | Completed | (89, 143) |
| Psidii Guava’s | Herbal extract | Capsules | NCT04810728 | Pending | 2 caps 3 times/day |
- Inhibitor of 3CLpro and PLpro (mainly quercetin) | Primary therapy | Phase III | 90 | Completed | (141) |
| Flaxseed | Nutraceuticals (omega3 fatty acid) | N/A | NCT04836052 | Pending | 2 mg 2 times/day |
- Attenuate pro-inflammatory cytokines | Primary therapy | Phase III | 372 | Recruited | (144) |
| Hesperidin | Bioactive phyto-compound | Capsules | NCT04715932 | Pending | 500 mg 2 times/day |
- Inhibitor of 3CLpro and PLpro | Primary treatment | Phase II | 216 | Completed | (145) |
| Ginger | Nutraceuticals | Tablets | IRCT20200506047323N1 | Pending | 1,000 mg 3 times/day |
- Inhibitor of PLpro | Primary treatment | Phase III | 86 | Completed | (146, 147) |
| Green tea | Nutraceuticals | Capsules | IRCT20150711023153N3 | Pending | 450 mg 2 times/day |
- Inhibitor of 3CLpro and PLpro -Inhibits complex formation with the virus |
Supportive therapy | N/A | 74 | Completed | (30, 148) |
| EGCG | Nutraceuticals | Capsules | NCT04446065 | Pending | 250 mg | - Inhibitor of 3CLpro and PLpro -Inhibits complex formation with the virus |
Primary treatment (prophylaxis) | Phase II | 524 | Not yet recruiting | (30, 148) |
| Colchicine | Bioactive metabolite | Tablets | NCT04363437 | Pending | An initial dose of 1.2 mg followed by 0.6 mg after 2 h on day 1. After that, 0.6 mg of two doses up to the 14th day |
- Disruption of microtubules and thus affect viral trafficking and the formation of double-membrane viral vesicles | Primary therapy | Phase II | 70 | Recruiting | (149) |
| Quercetin | Bioactive metabolite | Tablets | NCT04377789 | Pending | 500 mg of quercetin given daily to the prophylaxis group. The quercetin treatment group had confirmed cases of COVID-19 and they were provided with 1,000 mg quercetin daily. |
- Inhibition of polymerases, proteases, and reverse transcriptase; suppressing DNA gyrase; and binding viral capsid proteins; thus, it possesses an effective antiviral activity | Primary therapy | N/A | 447 | Completed | (132) |
| Escin | Nutraceuticals | Tablets | NCT04322344 | Pending | Oral administration of standard therapy Escin tablet for 12 days (40 mg thrice a day) |
- Potent antiviral activity. Yet, the exact mechanism of action is still unknown. | Adjuvant therapy | Phase II/III | 120 | Recruiting | (150) |
| Nicotine | Bioactive phytocompound | Patches | NCT04608201 | Pending | As Nicotine patch 0.5 patch for day 1 and day 2 1 patch for day 3 and day 4 1.5 patches for day 5 and day 6 2 patches from day 7 to the day of discharge from hospital (Each patch contains 7 mg nicotine) |
- Inhibits the penetration and spread of the virus - Prophylactic effect in COVID-19 infection |
Primary therapy | Phase III | 220 | Recruiting | (151) |
Shufeng Jiedu
Shufeng Jiedu capsule (SFJDC) is an oral Chinese herbal medicine prepared from many different plants as rhizome and root of Polygonum cuspidatum, root of Isatis indigotica Fort, dried roots of Phragmites communis, and many others (53, 152). SFJDC was proven to have antibacterial, antiviral, anti-inflammatory, and antitumor effects (153). The capsule preparations are often used to cure Influenza, the thing that made these preparations to be suggested for investigating it against COVID-19 (53). Yet, it is worth mentioning that SFJDC is contraindicated in patients with known serious hypersensitivity to the product itself or any component of the dosage form.
Anticancer Activity of SFJDC
In a study held to discover the effects of combining SFJDC with doxorubicin to treat hepatocellular carcinoma cells, results showed higher incidence of apoptosis along with more inhibition in cancer migration and invasion, indicating that SFJDC could be a potential complementary anticancer medication (153).
Immunomodulatory Role of SFJDC
The anti-inflammatory action of SFJDC was studied using mouse models infected with HCoV-229E, and the study indicated the ability of SFJDC to decrease IL-6, IL-10, TNF-α, and IFN-γ in lungs. This has created the hypothesis about the ability of herbal medicines to attenuate the cytokine storm caused by COVID-19 (154). These effects could be explained by the following mechanisms in which SFJDC was found to be acting with them: the PI3K-Akt signaling pathway was attenuated and the NF-κB-mediated transcription of pro-inflammatory cytokines was inhibited as well (155, 156).
Anti-SARS-CoV-2 Activity of SFJDC
The main constituents of SFJDC are quercetin, wogonin, and polydatin, indicating their ability to bind to Mpro of SARS-CoV-2 by means of molecular docking studies (157). There are clinical data as well for the addition of SFJDC with the standard antiviral therapy, indicating the high probability of SFJDC to shorten the duration of COVID-19 symptoms in mild to moderate cases (157). Another study was conducted at Bozhou People’s hospital where the effect of combining SFJDC with arbidol hydrochloride was studied in comparison to the arbidol hydrochloride alone (158). The results revealed clinical improvements in the combined group compared to the other one (152, 159).
Ginger
Zingiber officinale or ginger belongs to the family Zingiberaceae, it is an extremely beneficial herbal medicine used in many aspects. It originated in Southeast Asia but nowadays used worldwide as a food spice (160). Ginger rhizome is used for pain, nausea, and vomiting (161). A very wide range of active constituents are available and divided into two groups: volatile and non-volatile. The volatile group is definitely responsible for the odor and taste of ginger such as sesquiterpene and monoterpenoid hydrocarbons. However, gingerols, shogaols, parasols, and zingerone are the non-volatile constituents (162). Yet, it is worth mentioning that the usage of ginger might be accompanied by several side effects such as abdominal discomfort, diarrhea, heartburn, increased bleeding tendency, and mouth or throat irritation.
Anticancer Activity of Ginger
Ginger’s active constituents 6-gingerol and 6-shogaol are the main anticancer agents. Ginger has a broad spectrum anticancer activity against an array of solid malignancies such as gastric, pancreatic, colorectal, and liver cancers as shown in Table 2 and as previously reviewed in (91). The anticancer activity of ginger is accredited to its aptitude to repress several signaling pathways simultaneously such as the PI3K/AKT/mTOR pathway, the JAK/STAT pathway, the NF-κB pathway, COX-2 signaling, and caspase molecules (91).
Immunomodulatory Role of Ginger
Ginger is now considered a perfect choice for COVID-19 patients as it has analgesic, anti-inflammatory, antiviral, and immunomodulatory effects that can have a great role in the prevention of lung damage and respiratory disorders as listed in Table 2 . Mechanistically, this analgesic effect is achieved by inhibiting prostaglandin (PG) production through cyclooxygenase (COX) and lipoxygenase (LOX) pathways. This is also achieved by its antioxidant activity where inhibition of the transcription factor Nf-ĸB occurs. It also acts as an agonist of vanilloid nociceptor, which represses the pain sensation (163). Considering the anti-inflammatory effect, several pathways are involved, but we will focus only on the effect of 6-gingerol, which inhibits the production of pro-inflammatory cytokines from LPS-stimulated macrophages as shown in Table 2 (164). In the case of immune-compromised patients such as patients with rheumatoid arthritis, its manifestations are proved to be decreased by ginger as it increases the transcription factor forkhead box protein 3 (FoxP3) gene expression and decreases retinoic acid receptor-related orphan receptor γt (RORγt) and T-box expressed in T-cell (T-bet) gene expression (165).
Anti-SARS-CoV-2 Activity of Ginger
As illustrated earlier, one of the drug targeting mechanisms for SARS-CoV-2 is a papain-like protease (PL pro) that cleaves viral polyproteins that are very important for viral replication and survival. It was recently reported that ginger has the potential to act as a PL pro inhibitor for SARS-CoV-2, expressing its antiviral effect (89). Nonetheless, ginger has proven to relieve symptoms associated with COVID-19 infection such as chest pain. Ginger has proven to reduce chest pain and induce relaxation in airway smooth muscle, hindering airway resistance and inflammation as shown in Table 3 (166).
Turmeric
Curcuma longa or turmeric is a widely known herbal medicine; its main active constituent is the polyphenolic compound curcumin. It belongs to the family Zingiberaceae and used as a food spice, same as ginger. In Asian countries, it is used as a supplement and medicine to treat many diseases such as diabetes mellitus, cardiovascular diseases, obesity, neurodegenerative diseases, inflammatory bowel disease, allergy or asthma, and psoriasis. As mentioned above, turmeric extract is known for its polyphenol curcumin, constituting up to 77%; it contains other active constituents such as demethoxy-curcumin and bis-demethoxy-curcumin (167, 168). Turmeric can be used as an antiviral, antioxidant, anti-inflammatory, and anticancer agent. It is also important to note that turmeric does not usually cause severe side effects. Some users experience mild side effects such as abdominal discomfort, nausea, diarrhea, and dizziness.
Anticancer Activity of Turmeric
Turmeric is one of the well-investigated anticancer nutraceuticals. It was named the golden spice, whose use was passed on from the kitchen to the clinic (169). Curcumin shows an anti-neoplastic activity against solid malignancies such as breast, liver, colorectal, and prostate cancers, and several types of leukemias and lymphomas as shown in Table 2 and previously reviewed in (170–172).
Immunomodulatory Role of Turmeric
Turmeric is ranked as one of the most common immunomodulatory herbal drugs as curcumin shows strong antioxidant and anti-inflammatory effects (173). Mechanistically, its anti-inflammatory effects are prominent through the inhibition of the pro-inflammatory molecules: toll-like receptor (TLR-4), phosphatidylinositol-3 kinase (PI3K), and nuclear factor-kappa B (NF-κB). Turmeric also has the potential to repress the production of an array of pro-inflammatory cytokines such as IL-6, tumor necrosis factor-alpha (TNF-α), and interleukin 1 beta (IL-1β) (174, 175).
Anti-SARS-CoV-2 Activity of Turmeric
Concerning the SARS-CoV-2 antiviral activity of turmeric, one of the proposed mechanisms of action is acting as a PL pro inhibitor, same as ginger (89). Yet, in the case of turmeric (curcumin), this is not the only known antiviral mechanism; it is also known to act as an ACE II inhibitor. As previously illustrated, the virus enters the host by its S protein binding to the ACE II receptor. ACE II expression is detected in nasal epithelial cells, alveolar epithelial type II cells (AEC type II) of lungs, and the luminal surface of intestinal epithelial cells. Consequently, it stops viral entry and invasion in these cells (176–178).
Garlic
Allium sativum or garlic is one of the world’s oldest cultivated plants and has developed a well-established reputation across many cultures for embodying promising therapeutic benefits (179). More specifically, garlic is famed for its immunomodulatory role. Garlic contains a wide range of active constituents such as allicin, alliin, ajoenes, vinyldithiins, and diallyl sulfide. S-allyl-cysteine, S-ally-mercapto cysteine, and N-acetylcysteine resemble organosulfur examples, but concerning the flavonoidal constituents, quercetin is the main active constituent. The sulfur-containing phytochemicals are mainly responsible for its immunomodulatory, anti-inflammatory, anticancer, antitumor, antidiabetic, anti-atherosclerotic, and cardioprotective features (180, 181). Similar to other herbal drugs mentioned above, some mild side effects could accompany the usage of garlic such as unpleasant mouth or body odor, nausea, vomiting, and diarrhea.
Anticancer Activity of Garlic
The anticancer properties of garlic have been well-documented in several types of neoplastic conditions such as breast, nasopharyngeal, oral, esophageal, and gastric carcinomas, which were previously reviewed in (179). Digging deeper to understand the molecular mechanism of garlic as an anticancer agent, this could be directly related to the sulfur-containing active constituents as they provide a source of hydrogen sulfide (182). In particular, our research group has recently shown the vital role of hydrogen sulfide in cancer progression in different contexts (183, 184).
Immunomodulatory Role of Garlic
As previously mentioned, the immunomodulatory role of garlic extracts has a well-documented property that is mainly related to the sulfur-containing active constituents as well (180, 181). There are extensive mechanisms for the immunomodulatory and anti-inflammatory actions of garlic, specifically alliin, which effectively suppresses the expression of several proinflammatory cytokines such as interleukin 6 (IL-6) and mature plasma cell 1 (MCP-1) (110). In the case of asthmatic patients, garlic has also a proven anti-asthmatic property through repressing IL-4, IL-5, and IL-13 secretion (185). Moreover, the S-allyl cysteine constituent of garlic has also proven to ameliorate MS-related pathology and relieve the associated symptoms through altering tumor necrosis-α level in the MS-mouse model (186). However, concerning SLE patients, no information was reported concerning the impact of garlic on the pathogenesis of the disease or its associated symptoms. Collectively, garlic has been proven to have several features that could provide a protective shield for high-risk autoimmune patients in the current pandemic.
Anti-SARS-CoV-2 Activity of Garlic
Garlic has shown potential antiviral activity against a myriad array of viruses. Its antiviral activity against SARS-CoV-2 has been estimated. It was reported to act as a chymotrypsin-like protease (3CLpro) inhibitor, resulting in hindering viral attachment to host cells. Such antiviral activity has been acknowledged to the alliin and quercetin constituents in the garlic (187). In the shadow of SARS-CoV-2-associated high risk of blood clots and increase in D-dimer levels that are directly proportional to mortality rate, it is important to decrease other risk factors for blood clots such as lipids, triglycerides, and cholesterol levels in high-risk patients in particular. In such context, black garlic extracts were proven to have an anti-atherosclerotic action, meaning to decrease the blood levels of total lipids, triglycerides, and cholesterol as they lower sterol regulatory element-binding protein 1 (SREBP-1C) mRNA expression causing downregulation of lipid and cholesterol metabolism (188).
Flaxseed
Linum usitatissimum or flaxseed has been known for its potential anticancer and anti-angiogenic properties against several solid and non-solid malignancies. Nonetheless, it has also been known for its promising immunomodulatory role and recent anti-SARS-CoV-2 activity. This has been associated with its high abundance of lignans and Omega 3. The most common lignin is secoisolariciresinol diglucoside (SDG).
Anticancer Activity of Flaxseed
Literature supports the anticancer activity of flaxseed oil and other isolated compounds from flaxseed both in vitro and in vivo (189–191). Ezzat et al. have recently validated the anticancer activity of lignin-rich fraction from flaxseed against breast cancer cell lines and mice bearing tumors as well. It was reported that lignin-rich flaxseed fractions markedly repressed vascular endothelial growth factor (VEGF) and 1-α, metalloproteinases harnessing breast cancer metastasis in vitro and in vivo (191). Moreover, it was reported to activate the caspase-3-dependent apoptosis as a mechanism of its antiproliferative activity (190, 191).
Immunomodulatory Role of Flaxseed
For a very long time, PUFA has been known to treat metabolic, cardiac, inflammatory, and autoimmune diseases and reduce the risk of cancers (192). Generally, omega 3 PUFA has a great immunomodulatory effect in cases of acute pneumonia and acute respiratory distress syndrome (ARDS) by reducing reactive oxygen species and pro-inflammatory cytokines, such as TNF-α, IL-1β, IL-6, and IL-8 (193, 194).
Anti-SARS-CoV-2 Activity of Flaxseed
Since flaxseed’s immunomodulatory role and its inhibitory impact on several cytokines that are reported to be dominant players in the cytokine storm manifested by SARS-CoV-2 patients were validated, the effect of flaxseed on SARS-CoV-2 patients was evaluated. It was found that omega 3 reduces lung inflammation caused by the SARS-CoV-2 infection by decreasing IL-6 production, extracellular signal-regulated kinases 1 and 2, COX-2 activation, and the nuclear translocation of NF-κB (144).
Citrus Fruits
Citrus fruits such as Citrus sinensis (sweet orange) are the most widely used functional food during the pandemic. This was definitely because of its highly relevant active constituents in combating SARS-CoV-2. Citrus fruits are rich in vitamin C, carotenoids, and flavanones (195). Nonetheless, even the hesperidin flavone is found in the peel and the white part (albedo) of citrus fruits (196). Hesperidin has manifold properties such as antiviral, antimicrobial, antioxidant, antitumor, antihypertensive, and immunostimulant activities (197).
Anticancer Activity of Citrus Fruits (Hesperidin)
Our research group has recently focused on the anticancer activity of hesperidin and its glycoside hesperetin, where we and others showed that hesperidin has potent anticancer properties against several hallmarks of breast cancer such as cellular viability, proliferation, colony-forming ability, migration, and invasion in vitro (198–200). Moreover, it was found to have a direct impact on the tumor microenvironment at the tumor-immune synapse through altering ICAM-1 and ULBP2 in MDA-MB-231 breast cancer cell lines.
Immunomodulatory Role of Citrus Fruits (Hesperidin)
Hesperidin has been recently reported to have a direct post immunomodulatory role on autoimmune patients. It was reported that hesperidin can reduce the neuroinflammation episodes experienced by MS victims as well as ameliorates the immunological outcome in an MS-mouse model (118). In a more comprehensive study, it was reported that hesperidin alleviates several neurological disorders including MS through its anti-inflammatory and potent antioxidant activities (201). It is also important to note that hesperidin was also found to have anti-arthritogenic effects in an experimental model of RA (202).
Anti-SARS-CoV-2 Activity of Citrus Fruits (Hesperidin)
More than one mechanism was proposed for the anti-SARS-CoV-2 activity of hesperidin; as explained before, SARS-CoV-2 is internalized by binding of the spike glycoprotein of the virus with ACE2 receptors. Hesperidin superimposes the ACE2-receptor-bidomain (RBD) complex, so it binds to the virus spike protein (197). Also, it was suggested that it binds “3Clpro” or “Mpro”, preventing the processing of viral proteins pp1a and pp1ab into functional proteins in the host cells (145). Furthermore, it is considered a powerful antioxidant as it is powerful against superoxide and hydroxyl radicals that cause oxidative stress, and it can help control specific phases of the life cycle of SARS-CoV-2 and finally prevent cell death (197, 203–205). However, the main antioxidant effect of orange peel goes back to vitamin C content. It was suggested that increasing vitamin C daily intake during the COVID-19 pandemic is a useful protective measure as it stimulates antiviral immune responses and reduces the lungs’ inflammatory status (144, 206, 207).
Echinacea purpurea
Echinacea purpurea or the purple coneflower is a well-known herb highly recommended for respiratory infectious diseases in Europe as it is already present in different forms such as extracts, tinctures, teas, and sprays, and at different dosages as well (208). The purple coneflower contains many bioactive compounds such as chicoric acid and caffeic acids, alkylamides, and polysaccharides (209). These active constituents were proven to have antiviral effects against enveloped viruses such as human coronavirus (209). Its supplements are widely recommended by naturopathic doctors for their immune support function (210). Moreover, it is well known for its various immunomodulatory, antioxidant, anti-inflammatory, and antibacterial properties (211, 212).
Anticancer Activity of Echinacea purpurea
The anticancer mechanism is still not clear, but a study showed that chicoric acid has the ability to induce apoptosis in colon cancer cells and to decrease the telomerase activity in HCT-116 cells (213). Another study done on human pancreatic cancer cells and colon cancer cells indicated the ability of the root extract to induce DNA fragmentation and increase the activity of caspase 3/7 in a dose- and time-dependent manner, thus inducing apoptosis (214).
Immunomodulatory Role of Echinacea purpurea
Extracts of E. purpurea, both aqueous and alcoholic, regulate the immune cells in both adaptive and innate systems (215–217). It works by improving CD4+ and CD8+ T lymphocyte and cytokine levels in blood. These cytokines include the three interleukins IL-6, IL-10, and IL-17 (218). To inhibit inflammation, it suppresses interleukins IL-2, IL-6, and tumor necrosis factor (TNF-α) (219).
Anti-SARS-CoV-2 Activity of Echinacea purpurea
E. purpurea seems to augment its antiviral response by influencing PRRs on the innate immune cells, pathogen-associated molecular pattern PAMPs on the virus (220). Such interaction triggers phagocytosis and initiation of other antiviral responses by the immune system (221). It was also noted that E. purpurea has an effective antiviral role against rhinoviruses (222), influenza virus (223), RSV (208), herpes virus (208), adenoviruses (208), and coronaviruses (224, 225).
Java Turmeric
Another potential candidate is Java turmeric, also known as Curcuma zanthorrhiza. It is a highly promising candidate as its major active constituent is xanthorrhizol (accounts for 44.5%) (226). Java turmeric is widely used in Southeast Asian countries and belongs to Zingiberaceae and Curcuma genus (90). This plant is usually used as an important food additive to enhance flavors (227), but as a treatment component, it is well approved for some diseases and can be used as supplements (226–229). This plant has a myriad of functions, namely, it has antimicrobial, antioxidant, antihyperglycemic, antihypertensive, antiplatelet, anticancer, and nephroprotective effects, and it can be used as a supplement in SLE (230–233). These characteristics make it a potential adjuvant therapy for COVID-19 patients and a preventive measure for high-risk patients, especially SLE patients.
Anticancer Activity of Java Turmeric (Xanthorrhizol)
The anticancer activity of Java turmeric can be due to the induction of the TP53-dependent mitochondrial pathway and thus induction of apoptosis (234–236). It can also induce caspase activation, which will lead to enzymatic proteolysis of DNA and cytoplasmic proteins leading to cell death (227). A study done on HCT166 colon cancer showed that xanthorrhizol leads to higher expression of NAG-1 and increases the activity of its promoter (237). NAG-1 (non-steroidal anti-inflammatory drug-activated gene 1) is a pro-apoptotic and is a member of (TGF-β) (237). Regulation of the MAPK pathway is another function for xanthorrhizol; it increases ROS levels intracellularly and enhances phosphorylation of p38 and JNK in SCC-15 oral squamous cell carcinoma (238).
Immunomodulatory Role of Java Turmeric (Xanthorrhizol)
It was proven that it inhibits the production of inflammatory cytokines from adipose tissue by downregulation of inflammatory cytokine genes and inhibits the expression of TNF-α as well (90). For SLE patients with hypovitamin D levels, a study showed that xanthorrhizol can lower the serum level of IL-6 and increase the serum level of TGF-β (229). Another study released the same results when done on hippocampal neurons and primary culture microglia, and this inhibition of inflammation could be due to inhibition of nitric oxide synthase (iNOS), and consequently, lower levels of nitric oxide (NO) are produced (235, 239, 240). Collectively, it may play an immunosuppressant role (90).
Anti-SARS-CoV-2 Activity of Java Turmeric (Xanthorrhizol)
Xanthorrhizol was shown to have a potent antiviral activity against SARS-CoV-2 variants such as GH clade strain and delta strain, so it can be a promising antiviral plant against COVID-19 (241).
Ashwagandha
Withania somnifera is widely known for its antiviral, immunomodulatory, anti-inflammatory, anti-stress, antihypertensive, and antidiabetic effects, and many clinical trials were made to study its safety profile in humans (which eventually confirmed its safe use in humans) (242, 243). Moreover, there are scientific proofs for the ability of W. somnifera to maintain immune homeostasis in states of infection and inflammation (244, 245). The main active constituent in this plant is called Withanolides, which is a group of C28 steroidal lactone triterpinoids, including withaferin A; withanolide A, B, and D; withanoside IV and V; withasomniferin A; withanone; sitoondoside IX and X; and 12-deoxywithastramonolide. Furthermore, there are other active constituents such as catechin, naringenin, and syringic acid p-coumarin. This combination of such significant components endows W. somnifera superior protective capability (245, 246).
Anticancer Activity of Ashwagandha
Withaferin A is considered to be the principal component in W. somnifera; it works by inhibition of β-tubulin and consequently stops the proliferation of cells (247); it also inhibits tumor proteasomal chymotrypsin (248). It was also proven that withaferin A inhibits the cancer chaperon Hsp90 as it stabilizes the signaling proteins (249). Moreover, Notch1, which mediates the survival of colon cancer cells, is inhibited as well by withaferin (250).
Collectively, withaferin A and withanone promote ROS signaling, so they induce cancer killing by oxidative stress along with other pathways (251, 252). Finally, a study was carried out in a mouse model that concluded that W. somnifera alcoholic extracts inhibit tumor proliferation and growth and increase life span (253).
Immunomodulatory Role of Ashwagandha
Withanolide A encourages B- and T-cell proliferation with improvements in TH1 response as well (254–258). In mice, W. somnifera extracts led to higher counts of leukocytes and platelets (259, 260), and in chicks, the count of CD4+ and CD8+ also increased when compared to normal levels (261, 262). W. somnifera extracts were found by a study to be an immunostimulant when administered with anupana as vehicle, and the results revealed the activation of T cells and NK cells after 4 days only with BID consumption (263).
Anti-SARS-CoV-2 Activity of Ashwagandha
W. somnifera can impede the viral replication cycle. Withanone destabilizes the complex between the ACE2 receptor (host) and spike protein (virus) (264), and in addition, withaferin A and withanone are responsible for blocking Mpro and TMPRSS2 enzymes, which could interfere with the entry of the virus (142, 264, 265). Withacoagin and withanolide B have the ability to block the spike protein and also the RdRp with a high affinity (266). It was reported that they prevent virus entry to the host through inhibition of the trans-membrane protease serine 2 (TMPRSS2)/ACE II complex, thus hindering SARS-CoV-2 entrance to host cells (142).
Green and Black Tea
Tea is from the plant Camellia sinensis, which is a highly consumed beverage worldwide, with approximately 2.5 million tons produced each year. The difference between green and black tea is in the manufacturing process as green tea, once harvested, is steamed to prevent fermentation, while black tea is left as it is, causing the dimerization of catechins to theaflavins (267, 268). Although the composition of tea can change according to the climate, leaves, season, etc., the main constituent in it is considered to be polyphenols (269). Tea is not just a normal beverage, as research has turned a spotlight on it to study its various effects whether in vivo or in vitro (269). The studies revealed that polyphenols present in the tea can have a role in several diseases including cancer, diabetes, and cardiovascular diseases (269).
Black Tea
The polyphenols present in black tea are mainly theaflavins and thearubigins (269). Derivatives of theaflavins are theaflavin (TF1), theaflavin-3-gallate (TF2A), theaflavin-3’-gallate (TF2B), and theaflavin-3,3’-digallate (TF3) (270). Investigations of their biological properties found a myriad of benefits including antiviral, anti-inflammatory, antioxidant, antitumor, and antibacterial activities (271–273).
Anticancer Activity of Black Tea
Black tea shows a potential in the treatment of many types of cancer such as breast, prostate, lung, ovarian, cervical, and liver (274). In vitro studies for breast cancer showed 40% smaller tumor size for the intervention group when compared to controls (275). For prostatic cancer, significant inhibition for the androgen receptor promoter region along with inhibition of androgen receptor expression was noticed (276). Moreover, prostatic adenocarcinoma cell viability is inhibited in a dose-dependent fashion with TF1, TF2a, TF2b, and TF3 (277). A myriad of studies have proven the antiproliferative activity of theaflavins and the inhibition of survival and migration ability of cancer cells (274). There are studies that reveal the proapoptotic potential of theaflavins by observing higher levels of Bax (apoptotic protein) and lower levels of Bcl-2 (antiapoptotic protein) (274). Furthermore, P53 levels are increased by theaflavins and reduction in the levels of phosphorylated Akt, phosphorylated mTOR, and c-Myc occurs (274). Generally, theaflavins show a potential for cancer treatment and prevention (274).
Immunomodulatory Role of Black Tea
Theaflavins were proven to have the potential for inhibition of not only lipopolysaccharide (LPS)-induced intracellular adhesion molecule (ICAM)-1 but also the expression of the vascular cell adhesion molecule (VCAM)-1 by blocking pathways of NF-kB and c-Jun N-terminal kinase (JNK); this in turn will shut down the neutrophils since ICAM-1 and VCAM-1 are expressed on the endothelial cell surfaces (278–280). Theaflavins also have the capability to inhibit ROS and neutrophil elastase enzyme (the one that increases the permeability of alveolar epithelium) in a promising way (280–282).
Anti-SARS-CoV-2 Activity of Black Tea
The antiviral activity of black tea comes from TF1, TF2a, TF2b, and TF3, which were proven to have high affinity for 3CLpro and inhibit it (270). Theaflavins also showed a potential for inhibiting RNA-dependent RNA polymerase RdRp (283) and RBD in the spike at locations near the contact between ACE2 and spike protein (270). The roles of theaflavins go beyond treatment since TF3 was found to be able to bind to the ACE2 receptor, thus preventing spike RBD from attaching (284), leading to prophylaxis effects (285).
Green Tea
The main polyphenolics in green tea are quercetin and catechins, which include epigallocatechin-3-gallate (EGCG) (the most predominant one), epigallocatechin, epicatechin-3-gallate, epicatechin, gallocatechins, and gallocatechin gallate (269, 286). The main investigated biological effects were anti-inflammatory, antibacterial, antioxidant, antiproliferative, and antitumor (267), as shown in Figure 3 and briefly described below. The main prominent effect for EGCG is being a potent antiviral more than the chemically synthesized drugs (270).
Figure 3.

Significant pharmacological activities of EGCG and quercetin. Green tea, with its main two active constituents EGCG and quercetin, contributes to a wide range of medicinal activities such as antioxidant, immunomodulatory, anticancer, antiviral, and antibacterial actions. EGCG anticancer activity is produced by suppressing the NF-κB signaling in A549 and H1299 cells; activation of apoptotic cascades are also initiated, resulting in a marked hindering of cellular proliferation. On the other hand, quercetin inhibits the protein kinase C (PKC-α), a survival signaling protein, repressing several cancer hallmarks. Concerning the immunomodulatory actions, EGCG induces TLR4 and TLR2 expression levels, thus depleting the mitogen-activated protein kinase (MAPK) pathway and repression of pro-inflammatory cytokines release. As for the quercetin, it inhibits pro-inflammatory mediators such as Lipoxygenase and Phospholipase A2. Besides, both constituents share the same antiviral mechanism against SARS-CoV-2, which is binding to “3Clpro” or “Mpro”, preventing the processing of viral proteins pp1a and pp1ab into functional proteins in the host cells. Bona fida, the antioxidant effects of both EGCG and quercetin are mediated through scavenging and neutralizing the free radicals and boosting the enzymes that are responsible for detoxification such as glutathione reductase, glutathione peroxidase, and catalase. Finally, quercetin showed potential antibacterial activity through inhibiting half of the biofilm production by methicillin-resistant S. aureus (MRSA) and vancomycin-resistant S. aureus (VRSA). Similarly, EGCG showed antibacterial activities through inhibiting the B lactamase production and neutralizing the released toxins.
Regarding the scope of the review, their antiviral activity and their potential as anti-SARS-CoV-2 nutraceuticals will be the main focus especially since the anticancer activity and immunomodulatory role of EGCG and quercetin have been validated and previously reviewed (287, 288). This part will discuss some of the proposed mechanisms of EGCG (the main catechin) as an anticancer and immunomodulatory constituent of green tea as an introduction for its significance, then the spotlight on it, as well as on quercetin, will be turned on again in the matcha part.
Anticancer Activity of Green Tea
Apoptosis is the needed end result in the treatment of any cancer, so highlight was thrown on EGCG’s ability to induce apoptosis. Studies showed its ability to induce apoptosis by generating ROS and activating caspase-3 and caspase-9. Consequently, this leads to cycle arrest at the G1 phase (289, 290). NF-kB, which has a major role in apoptosis inhibition in cancer (291), was inhibited by EGCG in breast cancer, lung cancer, and human non-squamous cell carcinoma (292, 293). Activator protein-1 (AP-1), which induces proliferation, is also downregulated by EGCG (294). Actually, EGCG was proven by several studies to inhibit VEGF production through inhibition of STAT-3 and NF-kB in breast and human non-squamous cell carcinoma (292). Another study indicated the efficacy of EGCG on the inhibition of the IGF/IGF-1R axis (295, 296). Even in epigenetics, EGCG inhibits the activation of DNA methyltransferase, leading to restoration of silenced tumor suppressor genes as an end result; these genes include retinoic acid receptor- β (RARβ), p16INK4a, and O6-methylguanine-DNA methyltransferase (297).
Immunomodulatory Role of Green Tea
In an aim to investigate the effects of EGCG on cytokine level modulation, a study was done on activated human primary T cells to see the effect on atherogenesis (298). This study found that EGCG has successfully decreased the level of interleukins IL-2 and IL-4, INF-γ, and TNF-α. EGCG also decreased the level of phosphorylated c-Jun N-terminal (p-JNK) and extracellular signal-regulated kinase (p-ERK), and this could explain the mechanism used by EGCG to exert its anti-inflammatory effects (298). In addition, EGCG seems to have a role in symptoms reduction and pathology improvement in autoimmune diseases (299). Inhibition effects of EGCG on CD4+ T-cell expansion in response to stimulation was observed (299). The differentiation of naïve CD4+ T cells and that of Th1 and Th17 was also affected (299). This obstructed differentiation of Th1 and Th17 can be due to downregulation of transcription factors by EGCG, for instance, STAT1 and T-bet for Th1, while STAT3 and RORγt for Th17 (299). A study on multiple sclerosis in an animal model showed that EGCG weakened the disease severity in a dose-dependent manner and suppressed the proliferation of T cells along with reducing pro-inflammatory cytokine production (299). Besides, EGCG anti-inflammatory effects were proven as well in inflammatory arthritis disease (299).
EGCG has the ability to downregulate MAPK and NF-kb signaling pathways leading to the inhibition of pro-inflammatory cytokines as a result (300, 301). EGCG can weaken the transmigration of neutrophils through vascular endothelial cells (281) and decrease the neutrophil elastase enzyme, which increases the permeability of alveolar epithelium (302). As mentioned in black tea, EGCG in green tea can also inhibit LPS-induced ICAM-1 as well as the expression of the VCAM-1 by blocking pathways of NF-kB and c-Jun N-terminal kinase (JNK); this in turn will shut down the neutrophils since ICAM-1 and VCAM-1 are expressed on the endothelial cell surfaces (278–280). Last but not least, EGCG can scavenge for ROS and neutrophil elastase enzyme (the one that increases the permeability of alveolar epithelium) in a promising way (280–282), making it a strong immunomodulatory agent that can help fight infections that consequently will have an impact on controlling COVID-19.
Anti-SARS-CoV-2 Activity of Green Tea
EGCG was shown to possess antiviral activity against many viruses such as porcine reproductive and respiratory syndrome virus (PRRSV), hepatitis C virus (HCV), ZIKA virus, chikungunya virus, influenza virus, and HIV-1 (303–307). Consequently, this inspired researchers to evaluate its antiviral potential against SARS-CoV-2. Initially, EGCG and quercetin were reported to be among the most effective inhibitors for 3CLpro as presented in Figure 4 (148). EGCG was proven by molecular docking studies to be the most potent inhibitor for 3CLpro among all the nature-based phytochemicals (308). Then, it was reported that EGCG inhibits many structural proteins such as the HR2 domain, the post-fusion core of the S2 subunit, S protein, the RBD-ACE2 complex, and NSP15 endoribonuclease as shown in Figure 4 (270). Also, another mechanism of action mediated by EGCG was the inhibition of the complex formation between glucose-regulated protein-78 (GRP-78) and the virus (309), as shown in Figure 4 . GRP78 is a chaperone protein that is normally expressed in the lumen of the endoplasmic reticulum. Under cell stress conditions, overexpression of this protein occurs and is then translocated to the plasma membrane where SARS-CoV-2 interacts with it by the S protein, and subsequently, virus entry happens (310). Another molecular docking study was made on the binding affinity to the viral structural protein finding that EGCG has the highest affinity among the other substances that are included in the study. This study underlined a very important discovery: the affinity of EGCG to inhibition was higher than that of the well-known drugs used during the pandemic, remdesivir and chloroquine, suggesting a better antiviral activity for EGCG (270, 311).
Figure 4.

Anti-SARS-CoV-2 activities of EGCG and quercetin. This figure illustrates the anti-SARS-CoV-2 for both EGCG and quercetin. EGCG inhibits RNA-dependent RNA polymerase (RdRp), an enzyme having an important role n replication and transcription of the virus. EGCG also inhibits the binding of the S1 region of the viral spike protein to the ACE2 receptor on the lung host cells. EGCG and quercetin prevent the processing of polyproteins pp1a and pp1ab by Papain-like protease (PLpro) and Chemotrypsin-like protease (3C like protease or 3CLpro or Mpro). Finally, EGCG inhibits complex formation of the virus with GRP78 receptor and thus inhibits viral entry.
Collectively, among all the natural active constituents isolated from phytochemical plants, EGCG and quercetin showed an exceptionally potent antiviral activity harnessing the SARS-CoV-2 life cycle through a myriad of mechanisms as summarized in Figure 4 . Accordingly, our next step was to screen for herbal drugs that were reported to contain the highest phenolic contents of EGCG and quercetin. Undoubtedly, the choice was matcha, especially since it has been recently reported that several types of green tea could effectively block infection due to SARS-CoV-2 and its new variants by mainly abrogating the spike binding to the ACE2 receptor (29, 30).
Matcha: Filling the Gap During the Pandemic
Matcha powder is a herbal drug that was reported to contain at least three times higher EGCG content than green tea, providing an economic and beneficial beverage for SARS-CoV-2-infected patients and a preventive measure for high-risk patients such as cancer and autoimmune patients (312). Nowadays, matcha tea powder is widely known and used for its abundant health benefits and its exceptional quality. Matcha is the powdered form of green tea that originated in Japan (313). The high nutritional benefits of matcha come from the presence of many powerful active constituents as listed in Table 4 below. The main forms of catechins and the most active ones found in higher amounts are (-) epigallocatechin 3-gallate (EGCG), caffeine, quercetin, phenolic acids, rutin, vitamin C, chlorophyll, and theanine (313). Catechins are present in four types: (-) epicatechin (EC), (-) epicatechin 3-gallate, (-) epigallocatechin (EGC), and (-) epigallocatechin 3-gallate (EGCG) (344, 345).
Table 4.
Biological activities of matcha active constituents.
| Active constituent | Biological activity | References |
|---|---|---|
| Chlorophyll | Anti-inflammatory Antioxidant |
(314, 315) |
| Epigallocatechin 3-gallate (EGCG) |
Decreases the ROS Increases enzymes for detoxification Anti-carcinogenic Anti-bacterial Antiviral Immunomodulatory |
(300, 316–319) |
| Quercetin | Antioxidant Neuroprotective Decreases glucose absorption Increases insulin secretion and sensitivity Antiviral Immunomodulatory Anti-bacterial Anti-carcinogenic |
(320–331) |
| Vitamin C | Strong exogenous antioxidant Enforces the immune system |
(332) |
| Caffeine | Decreases the ROS Increases the antioxidant enzymes activity Increases glutathione levels Decreases pro-inflammatory cytokines |
(333, 334) |
| Theanine | Gives distinctive and non-bitter taste | (335–337) |
| Phenolic Acids | Antioxidant Anti-inflammatory Hypoglycemic Neuroprotective Regulates carbohydrates/lipid metabolism |
(333, 338–341) |
| Rutin | Antioxidant Anti-diabetic Anti-inflammatory |
(332, 342, 343) |
Matcha Main Constituents: EGCG
Catechins have an indisputable role as antioxidants by scavenging and neutralizing the free radicals and boosting the enzymes that are responsible for detoxification such as glutathione reductase, glutathione peroxidase, and catalase (346). It is also worth mentioning that the cellular redox homeostasis can be well maintained by the intake of catechins more often in the human diet (316). As previously mentioned, EGCG has a powerful antiviral effect. Compared to vitamin C, flavonoids, and glutathione, it has been proved that catechins have a higher antioxidant potential (316).
The Anti-Carcinogenic Activity of EGCG
This antioxidant effect contributes to one of the anti-carcinogenic mechanisms of EGCG, as it was previously mentioned that the catechins can quench the reactive oxygen species at any stage and consequently halt the malignant transformation process (347). Other studies have shown that the EGCG has several anticancer activities as shown in Figure 5 . EGCG exhibits antitumorigenic properties in lung cancer. It suppresses the NF-κB signaling in A549 and H1299 cells; this leads to the inhibition of cell proliferation and induces apoptosis as shown in Figure 5 (348). EGCG suppresses breast cancer progression through the tight binding of EGCG to signal transduction activator proteins of transcription 1 (STAT1) by its three hydroxyl groups of the B ring and one hydroxyl group of the D ring; this bond leads to the blockage of the phosphorylation of STAT1 by Janus Kinase 2 (JAK2) and inhibition of its carcinogenic effects since STAT1 in cancer cases can act as an oncogenic protein. It was worth noting that EGCG promotes Fas/CD95-mediated apoptosis in the neck and head squamous carcinoma by inhibiting JAK/STAT3 (317, 349).
Figure 5.

Anticancer activities of EGCG and quercetin. Epigallocatechin-3-gallate (EGCG) and quercetin modulate several canonical oncological pathways such as Wnt/β-catenin and JAK/STAT pathways. Also, they modulate the expression of several anti-apoptotic proteins such as BCL2, tumor suppressor proteins such as TP53, and oncogenic drivers such as VEGF. Both active ingredients have proven to be effective in halting the malignant transformation process in several types of cancers such as breast, lung, liver, and colorectal cancers.
Anti-Bacterial Activity of EGCG
As per the current treatment protocol for SARS-CoV-2, several antibiotics are prescribed especially in high-risk patients to avoid the complications of secondary bacterial infections, an act that would result in an antibiotic resistance catastrophe post-pandemic as described by the WHO in November 2020. As presented in Figure 3 , EGCG has promising antibacterial activity while saving the world from the antibiotic resistance dilemma that would threaten our lives enormously. EGCG has shown bactericidal activity against staphylococci. Moreover, EGCG also shows an antibiofilm activity when co-administered with other antibiotics; it gives a powerful synergistic action. EGCG also can inhibit beta-lactamase production and neutralize the released toxins. The negatively charged property of EGCG makes it more effective against Gram-positive bacteria (318).
Immunomodulatory Role of EGCG
Nutrition immunity is a new concept that has been revolutionized during the pandemic (350). Massive attack on the respiratory epithelium (host cells for SARS-CoV-2) can lead to acute respiratory distress syndrome (ARDS), characterized by the uncontrolled release of pro-inflammatory cytokines leading to damaging the host cells, a vicious process termed as cytokine storm (350). It is important to note that the cytokine storm is also a common feature in the case of chemotherapy-treated cancer patients (351). Therefore, it is a crucially important measure to protect such high-risk patients during the pandemic. SARS-CoV-2-infected patients have a reduction in IFN-α and IFN-β levels, thus increasing the chance for the virus to invade and take over the immune system (319, 352). It is noteworthy that EGCG has a dominant immunomodulatory role by inducing TLR4 and TLR2 expression levels. Such induction occurs as a result of the repression of the mitogen-activated protein kinase (MAPK) and the pro-inflammatory cytokines as presented in Figure 3 (300, 301). EGCG also modulates the immune system through inhibition of the RIG-I (acts as a RIG-I inhibitor), thus protecting the infected patient from the cytokine storm and its notorious consequences (353).
Matcha Main Constituent: Quercetin
As presented in Table 4 , one of the main matcha constituents is quercetin. Quercetin possesses an array of pharmacological activities such as neuroprotection, antioxidant, and antineoplastic activities. It also has a vital role in diabetes mellitus patients, where it inhibits glucose absorption and thus it regulates carbohydrate metabolism, thus regulating the insulin secretion and sensitivity to tissues (320, 321, 354).
Anticancer Activity of Quercetin
Our research group has recently highlighted the potential anticancer activity of quercetin and its derivatives in liver and breast cancers (355, 356). Studies show that if quercetin was ingested on a daily basis, it was found to decrease the risk of cancer incidence (326). Quercetin was also reported to retain its antitumorigenic properties against several types of leukemias, melanoma, lung, colorectal, and ovarian cancers (325). In vivo studies also supported the promising anticancer properties of quercetin in several animal models (324). Molecularly, quercetin inhibits protein kinase C signaling protein, resulting in the activation of apoptotic death signals and cell cycle arrest as shown in Figure 5 (329). It also has powerful induction effects on TP53, Fas/FADD, caspases, and suppression of vital anti-apoptotic proteins (330, 331, 357). From an immune-oncological point of view, long-term intake of quercetin was proved to improve natural killer cells’ cytotoxic activity, neutrophil chemotaxis, and lymphocyte proliferation (323, 358). In addition, quercetin induces T helper cells to produce TH1-derived interferon-gamma (IFN-γ) and downregulates TH2-derived IL-4 (327, 359). Altogether, it is quite evident that quercetin possesses potential intrinsic anticancer activity together with activating the innate and adaptive immune arms to halt oncological progression in several malignant contexts.
Antibacterial Activity of Quercetin
Similar to EGCG, quercetin has shown potent bactericidal properties against an array of bacteria, such as Enterococcus faecalis and Listeria monocytogenes. Both are resistant to several antibiotics and have a detrimental ability to produce biofilms on an artificial device such as stents. Quercetin was reported to effectively inhibit 95% of biofilm formation, also by stopping several glycolytic enzymes such as 2,3-bisphosphoglycerate-dependent phosphoglycerate mutase (GpmA) and ATP-dependent phosphofructokinase (PfkA) in L. monocytogenes. Quercetin also represses the secretion of the bacterial adhesion molecules that have a vital role in L. monocytogenes (foodborne illness bacteria) infection. Thus, the incorporation of quercetin as a food additive to minimize the adhesion, proliferation, and biofilm growth of the bacteria is a safe and economic idea (328). It is also important to note that quercetin was reported to inhibit half of the biofilm production by methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant S. aureus (VRSA), thus shedding light on its powerful antibacterial activity (328).
Immunomodulatory Role of Quercetin
Quercetin possesses an immunomodulatory role through repressing platelet aggregation, lipid peroxidation, inhibition of pro-inflammatory mediators such as lipoxygenase and phospholipase A2, and the expression levels of MHG class II and co-stimulatory molecules. Digging deeper, it was found that attenuation of several canonical and non-canonical immunomodulatory pathways such as arachidonic acid metabolism, the associated leukotriene/prostaglandins, and mTOR signaling pathways are the molecular mechanisms by which quercetin possesses its immunomodulatory role in several contexts (360, 361).
Matcha Other Constituents: Caffeine
Caffeine is one of the constituents of matcha; it has a strong antioxidant activity where it acts by neutralizing the ROS and it induces the antioxidant enzyme activities and also increases the glutathione levels, thus reducing oxidative stress. Besides the antioxidant effect, caffeine also has an anti-inflammatory activity where it reduces the secretion of pro-inflammatory cytokines. It was found that the caffeine content in matcha is greater than that in green tea, thus making matcha tea more effective (333, 334, 339).
Matcha Other Constituents: Phenolic Acids
Phenolic acids are found at their maximum levels in matcha tea. They are well known to have powerful antioxidant and anti-inflammatory effects as well as hypoglycemic and neuroprotective effects. Moreover, regulation of several metabolic disorders is controlled by some of the phenolic acids by regulating carbohydrates and lipid metabolisms (333, 338–341).
Matcha Other Constituents: Rutin
Rutin is a polyphenolic compound. Among all the kinds of tea available in the market, matcha contains very high amounts of rutin. It has several benefits such as antioxidant, antidiabetic, and anti-inflammatory effects (332, 342, 343, 362).
Matcha Other Constituents: Chlorophyll, Theanine, and Vitamin C
Chlorophyll is responsible for the bright green color of matcha. It was reported that it has powerful anti-inflammatory and antioxidant effects (314, 315). Nevertheless, the amino acid theanine provides the taste of matcha, which is distinctive and non-bitter. Also, it was found that the presence of caffeine with theanine improves efficiency rather than using them separately (335–337). Last but not least, the presence of vitamin C is also important and possesses several beneficial effects since it cannot be synthesized within the human body. It is considered a strong exogenous antioxidant, and it must be supplied via nutritional intake as it reinforces the immune system (363).
Discussion
COVID-19 has made the world face a war with a different meaning this time—a war in which the entire world population are warriors, whose main slogan was “Stay Safe”, a war whose weapons consist of open-ended practical trials that take place in research labs to find a solution to finally end the war. On one hand, the hospitals were at full capacity, and the demand for oxygen supplies was increasing. On the other hand, this virus impacted the entire globe with deleterious effects economically. The mess was escalating.
The trials for combating this virus were numerous, and carried out with different aims, whether for drug repurposing or trying to develop new antiviral agents. Vaccine development was also one of the main goals of researchers, yet many other researchers have shed light on the use of herbal medicine. In silico, in vivo, and in vitro studies were conducted all with only one aim, which is to find a solution to solve this mess. In fact, none of the studies could underestimate the significance of the others, and all can work in harmony with each other or help each other to reach the main curative goal at the end.
Herbal medicine was one of the major routes that were investigated throughout this pandemic by many researchers as plants have been proven to be a miracle drug throughout the generations for combating many diseases, which also gave many researchers hope for defeating COVID-19. Nature has never failed to protect us, that is why the first routine that was followed since the start of this pandemic is to eat fruits and vegetables because of their potential to strengthen our immune system and act as a preventive measure. For this reason, it was not surprising that many review articles, clinical trials, and molecular docking studies investigated the antiviral potential of many plants against SARS-CoV-2, and many of them showed a strong potential to improve the pandemic situation as previously reviewed in (364–366).
However, there was another dark side to the story, and this darkness relies mainly on the ones who were suffering every minute whether for fear of catching the virus because they know how weak their bodies are to defeat this enemy or for the difficulties they would face to follow their treatment plans in the hospitals or clinics during this pandemic. These sufferers are mainly the cancer patients and immune-compromised patients such as those with SLE, RA, and MS who have higher mortality rates and exacerbated conditions upon exposure to the virus (367) compared to other normal individuals. Although vaccines seemed to be a proper solution, there are still limitations that should be taken into consideration as regards the efficacy of the vaccine for this type of patients as well as the possible interactions between both the vaccine and their treatments or the disease condition (367). Moreover, these patients needed to be tracked routinely for any signs of unexpected adverse events or if they are on active cancer therapy, so the relation between the timing of the vaccine and its safety and efficacy with the treatments and immune deficiency should be evaluated (368). Because of this, it was logical to think of herbal medicines as an option for these people due to their potential to defend against a myriad of viruses and strengthen the immune system, and certain herbs could have a role in attacking cancer as well when compared to vaccines or synthetic drugs.
In this review, we focused on the significant role of herbal medicines in helping cancer and immune-compromised patients. A spotlight was thrown on many plants such as ginger, turmeric, garlic, flaxseed, citrus fruits, Echinacea purpurea, Java turmeric, ashwagandha, and black tea. All of the plants highlighted in this review have proven their efficacy as anticancer, immunomodulatory, and antiviral agents; many of them already show an anti-COVID-19 potential. The combination of these three actions suggests herbal medicines as a good option for these patients. Yet, it is worth mentioning that most of the herbal products’ actions mentioned in this review are dose-dependent effects. For instance, it should be noted that garlic is an anticancer agent in several oncological contexts, but it is a source of organosulfur compounds, which are hydrogen sulfide donors (182). Hydrogen sulfide is a well-known biphasic gasotransmitter molecule that, at low concentrations, plays an oncogenic role while having an anticancer activity at higher concentration (183, 184).
One of the herbal plants that were discussed in this review was green tea, and while focusing on its constituents, which were mainly EGCG and quercetin, they were found to have very potent multiple mechanisms for defending against different cancer types, acting as immunomodulatory, anti-inflammatory, and antiviral agents specifically towards COVID-19. Matcha was able to obtain these protective properties in the highest possible amount.
Matcha is a Japanese green tea in which nowadays seems to be trendy in certain populations for its claimed ability to boost health and immunity, also it has been used recently in some of the cosmetic products for its ability to participate in a healthy skin conditions. Digging deeper in the Matcha constituents, we found that it contains EGCG and quercetin, the proven ones for their efficacy, in much concentrated amounts than in the normal green tea along with other constituents that were discussed as well in this review and as shown in Figure 6 . This can explain the potential for that herbal tea in specific to be an indispensable way for cancer and immunocompromised individuals to protect themselves against COVID-19 along with alleviating their health states.
Figure 6.

Matcha beneficial effects in protecting cancer and autoimmune patients from SARS-CoV-2 infection. This figure highlights the dynamic constituents of matcha and its beneficial effects in preventing SARS-CoV-2 infection and also ameliorating SARS-CoV-2-positive patients. A special focus on cancer and autoimmune patients is presented. Patients who have caught SARS-CoV-2 were found to have a decrease in IFNs; thus, EGCG stimulates the expression of both TLR4 and TLR2, and this helps in reducing the pro-inflammatory cytokines and the cytokine storm. Since the viral nucleic acid activates the RIG-1 that increases IFN-1, EGCG showed to act as a RIG-1 inhibitor. In addition, EGCG has an antioxidant effect by neutralizing the free radicals and boosting the detoxification enzymes. Moreover, quercetin is a potent immunomodulatory in SARS-CoV-2, as it has many functions such as antiviral activity, platelet aggregation inhibition, and inhibition of proinflammatory mediators like Lipoxygenase (LOX) and Phospholipase A2. Rutin has an antioxidant and anti-inflammatory activity; thus, it is useful in the management of COVID-19. The chlorophyll content in matcha has proven to be beneficial due to its anti-inflammatory and antioxidant effect, which assists to overcome the cytokine storm. Besides, caffeine has a potential anti-inflammatory effect by decreasing proinflammatory cytokines, and its antioxidant effect is due to reduction of ROS and increase of glutathione. In addition, Vitamin C greatly stimulates antiviral immune responses and reduces the lungs’ inflammatory state. It is essential to highlight that the intake of matcha tea not only will manage COVID-19 symptoms but also can prevent the virus itself from infecting humans.
This review suggests matcha as one of the potential options that should be highlighted during this period as it offers a great amount of potential to battling the current pandemic.
Future Recommendations
Since herbal medicines have always been able to tackle many health issues throughout the past pandemics and act as prophylaxis against a myriad of diseases, this encourages us to have a wider look in generalizing herbal medicines to the entire population. As reviewed, it has been documented that with the emergence of each new mutation, the efficacy of vaccines and drugs becomes negatively affected. Such information should encourage global health organizations to tackle this issue in a different way. More in-depth studies on herbal medicines need to be conducted using more clinical trials. In vivo and in vitro studies should be carried out for much more medicinal plants as well as in silico and molecular docking studies to further study and discover new effects for secondary metabolites. Such studies and clinical trials should also include the more susceptible populations such as cancer patients, immune disease patients, and children since they are not included in the current studies. Because of this, WHO will be encouraged to advise doctors about prescribing these herbal medicines along with other synthetic drugs if needed, and the media will also play a role as they will start to encourage people to use more herbal medicines and to make them aware of such medicines’ benefits. Consequently, this can lead to the discovery of more new plants and the investigation of new research areas by pharmaceutical companies in order to meet the market need. This can be a plan for any upcoming SARS-CoV-2 outbreak or for any new pandemic for either normal or ill people, and this plan will most probably succeed. One of the herbal medicines that is highlighted by this review for future use is matcha.
Such a wide range of therapeutic potentials ofwfi 2 “matcha” constituents whether as an immunomodulatory agent or as an anti-SARS-CoV-2 agent might be the reason why “matcha” would acquire a high market share in the upcoming years, especially since SARS-CoV-2 might behave like seasonal flu (after having more than eight waves to date). Nonetheless, we should not ignore the fact that more coronaviruses might appear at any time, since bats act as a reservoir or a storage tank for them. Collectively, this might highlight the potential of “matcha” to be the stone that could hit 3 birds (cancer, autoimmune disease, and SARS-CoV-2).
Although “matcha” seems to be very promising, there are a lot of challenges that may hinder its usage. For instance, “matcha” might not be accessible for many people due to its high price especially since we are focusing on cancer and autoimmune disease patients who already have very high expenses for their medications. Therefore, it is recommended to be produced in larger amounts for the sake of reducing its price, and this could be done by pharmaceutical companies. One of the major disadvantages that might discourage people to use “matcha” is its bad taste; however, this could be masked by the addition of flavors during the production phase, which again sheds light on the importance of pharmaceutical companies in “matcha” production. Therefore, this review elucidates the importance of having a cup of “matcha” to reinforce and strengthen the immune system in cancer and autoimmune disease patients who have a higher risk of catching SARS-CoV-2. Yet, this also can be generalized for everyone as it is powerful enough to prevent and protect them from catching the virus.
Conclusion
In conclusion, this review stresses the fact that the probability of the current pandemic to continue for a long time and the probability of developing future pandemics are extremely high, especially after the emergence of several VOCs. In this review, the authors highlight the great potential held by herbal medicine especially for high-risk patients such as cancer and autoimmune patients. Also, the authors shed light onto our new norm and how herbal products are considered risk-free solutions. In this review, it was set clear that after the SARS-CoV-2 pandemic experience, it should be noted that the development of new drugs and effective vaccines will not always be the easiest option. This review presents the current herbal medicines that could be used in preventing and fighting COVID-19, which happen to have three roles: as an immunomodulatory and anticancer agent, aside from displaying anti-SARS-CoV-2 activities. A special spotlight was turned on for the Japanese green tea “matcha”. The authors elucidating the promising use of matcha as a prophylactic agent during the SARS-CoV-2 pandemic can have a significant impact on the socioeconomic and health status in general and on cancer and autoimmune patients in particular. This was mainly based on their major constituents: EGCG and quercetin and their well-reported anticancer activity, immunomodulatory effects, and their recent anti-SARS-CoV-2 activity. Yet, more detailed studies about the usage of “matcha” among cancer and autoimmune patients have to be conducted in the future.
Author Contributions
CK, MK, and MT contributed to drafting the original draft of the manuscript and data collection (literature reviewing) and sketching the figures. The conception of the work, critical revision of the article, and data interpretation were performed by the principal investigator of the work, RY. The final version of the manuscript was approved and revised by all the authors.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Glossary
| +gRNA | Positive single-stranded RNA |
| +sgRNA | Positive subgenomic RNA |
| 2019-nCoV | 2019 novel coronavirus |
| 3C like protease | Chemotrypsin-like protease |
| 3CLpro | Chemotrypsin-like protease |
| ACE II | Angiotensin-Converting Enzyme 2 |
| Ad5 | Adenovirus type 5 |
| AKT | Protein kinase B |
| ALA | Alpha linolenic acid |
| ARDS | Acute respiratory distress syndrome |
| ASCO | American Society of Clinical Oncology |
| BAD | Bcl-2-associated agonist of cell death |
| Bax | Bcl-2-associated X protein |
| Bcl-2 | B-cell lymphoma 2 |
| Bcl-xl | B-cell lymphoma extra large |
| CD 44 | Cluster of differentiation 44 |
| COVID-19 | Coronavirus disease of 2019 |
| CoVs | Coronaviruses |
| COX-2 | Cyclooxygenase 2 |
| CYP3A4 | Cytochrome P450 3A4 |
| DADS | Diallyl disulfide |
| DMTs | Disease-modifying therapies |
| DMV | Double-membrane vesicle |
| dsDNA | Double-stranded DNA |
| E | Envelope |
| EC | Epicatechin |
| EGC | Epigallocatechin |
| EGCG | Epigallocatechin 3-gallate |
| ER | Endoplasmic reticulum |
| ERGIC | Endoplasmic reticulum golgi intermediate compartment |
| ESMO | European Association for Medical Oncology |
| FADD | Fas-associated protein with death domain |
| Fas/CD95 | Cluster of differentiation 95 |
| FDA | Food and Drug Administration |
| FoxP3 | Forkhead box protein 3 |
| GIT | Gastrointestinal tract |
| GpmA | 2,3-bisphosphoglycerate-dependent phosphoglycerate mutase |
| -gRNA | Negative single-stranded RNA |
| GRP78 | 78-kDa glucose-regulated protein |
| GRP-78 | Glucose-regulated protein 78 |
| H1N1 | Hemagglutinin type 1 and neuraminidase type 1 |
| HCV | Hepatitis C virus |
| HE | Hemagglutinin esterase |
| HIV | Human immunodeficiency virus |
| ICAM-1 | Intracellular adhesion molecule 1 |
| ICTV | International Committee on Taxonomy of Viruses |
| IFN beta | Interferon beta |
| IFN gamma | Interferon gamma |
| IFN-1 | Type I interferon |
| IgE | Immunoglobulin E |
| IL-10 | Interleukin 10 |
| IL-12 | Interleukin 12 |
| IL-13 | Interleukin 13 |
| IL-1α | Interleukin 1 alpha |
| IL-1β | Interleukin 1 beta |
| IL-2 | Interleukin 2 |
| IL-4 | Interleukin 4 |
| IL-5 | Interleukin 5 |
| IL-6 | Interleukin 6 |
| IL-8 | Interleukin 8 |
| iNOS | Inducible nitric oxide synthase |
| JAK | Janus kinase |
| JAK2 | Janus kinase 2 |
| LNP | Liposomal nanoparticle |
| LOX | Lipoxygenase |
| LPS | Lipopolysaccharide |
| M | Membrane |
| MAPK | Mitogen-activated protein kinase |
| MCP 1 | Monocyte chemoattractant protein 1 |
| MCP-1 | Mature plasma cell 1 |
| MERS-CoV | Middle East Respiratory Syndrome Coronavirus |
| miRNA | MicroRNA |
| MMP13 | Matrix metallopeptidase 13 |
| MMP9 | Matrix metallopeptidase 9 |
| Mpro | Main protease |
| mRNA vaccines | Messenger RNA vaccines |
| MRSA | Methicillin-resistant S. aureus |
| MS | Multiple sclerosis |
| mTOR | Mechanistic target of rapamycin |
| MUC 2 | Mucin 2 |
| N | Nucleocapsid |
| NCCN | National Comprehensive Cancer Network |
| NF-ĸB | Nuclear factor kappa-light-chain-enhancer of activated B cells |
| NIAID | National Institute of Allergy and Infectious Disease |
| NK cell | Natural killer cell |
| NO | Nitric oxide |
| NRVV | Non-replicating viral vector |
| Nsp | Nonstructural protein |
| Nsp1 | Nonstructural protein 1 |
| Nsp12 | Nonstructural protein 12 |
| Nsp13 | Nonstructural protein 13 |
| Nsp14 | Nonstructural protein 14 |
| NSP15 | Nonstructural protein 15 |
| Nsp2 | Nonstructural protein 2 |
| Nsp2-16 | Nonstructural protein 2-16 |
| Nsp3 | Nonstructural protein 3 |
| Nsp5-16 | Nonstructural protein 5-16 |
| Nsp7 | Nonstructural protein 7 |
| Nsp8 | Nonstructural protein 8 |
| P53 | Tumor protein p53 |
| PAF | Platelet-activating factor |
| PfkA | ATP-dependent phosphofructokinase |
| PG | Prostaglandin |
| PGE2 | Prostaglandin E2 |
| PH | Potential Hydrogen |
| PI3K | Phosphoinositide 3 kinase |
| PKC-alpha | Protein kinase C-alpha |
| PKC-delta | Protein kinase C-delta |
| PLpro | Papain like protease |
| PP | Polyprotein |
| PRRSV | Procaine reproductive and respiratory syndrome virus |
| PUFA | Polyunsaturated fatty acids |
| RA | Rheumatoid arthritis |
| RBD | Region binding domain |
| RdRp | RNA-dependent RNA polymerase |
| RIG-I | Retinoic acid-inducible gene I |
| RORγt | Retinoic acid-related orphan receptor γt |
| ROS | Reactive oxygen species |
| RTC | Replication/Transcription Complex |
| S | Spike |
| saRNA | Self-amplifying messenger RNA |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome-Coronavirus-2 |
| SDG | Secoisolariciresinol diglycoside |
| -sgRNA | Negative subgenomic RNA |
| SLE | Systemic lupus erythematosus |
| SOCS3 | Suppressor of cytokine signaling 3 |
| SREBP-1C | Sterol regulatory element-binding protein 1 |
| STAT | Signal Transducer and Activator of Transcription |
| STAT1 | Signal Transducer and Activator of Transcription 1 |
| STAT3 | Signal Transducer and Activator of Transcription 3 |
| T-bet | T-box protein expressed in T cells |
| TF1 | Theaflavin |
| TF2A | Theaflavin-3-gallate |
| TF2B | Theaflavin-3’-gallate |
| TF3 or TFDG | Theaflavin-3,3’-digallate |
| TGF-β | Transforming growth factor beta |
| TH1 | T helper 1 cell |
| TH17 | T helper 17 cell |
| TH2 | T helper 2 cell |
| TLR | Toll-like receptor |
| TLR2 | Toll-like receptor 2 |
| TLR4 | Toll-like receptor 4 |
| TMPRSS2 | Transmembrane protease serine 2 |
| TNF-α | Tumor necrosis factor alpha |
| ULBP2 | UL16 binding protein 2 |
| VAERD | Vaccine-associated enhanced respiratory disease |
| VEEV | Venezuelan equine encephalitis virus |
| VEGF | Vascular endothelial growth factor |
| VRSA | Vancomycin-resistant S. aureus |
References
- 1. Cheng VC, Lau SK, Woo PC, Yuen KY. Severe Acute Respiratory Syndrome Coronavirus as an Agent of Emerging and Reemerging Infection. Clin Microbiol Rev (2007) 20(4):660–94. doi: 10.1128/CMR.00023-07 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical Features of Patients Infected With 2019 Novel Coronavirus in Wuhan, China. Lancet (2020) 395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Coronaviridae Study Group of the International Committee on Taxonomy of, V . The Species Severe Acute Respiratory Syndrome-Related Coronavirus, Classifying 2019-Ncov and Naming It SARS-CoV-2. Nat Microbiol (2020) 5(4):536–44. doi: 10.1038/s41564-020-0695-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Woolf SH, Chapman DA, Lee JH. COVID-19 as the Leading Cause of Death in the United States. JAMA (2021) 325(2):123–4. doi: 10.1001/jama.2020.24865 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Koh HK, Geller AC, VanderWeele TJ. Deaths From COVID-19. JAMA (2021) 325(2):133–4. doi: 10.1001/jama.2020.25381 [DOI] [PubMed] [Google Scholar]
- 6. Liu S, Zhi Y, Ying S. COVID-19 and Asthma, Reflection During the Pandemic. Clin Rev Allergy Immunol (2020) 59(1):78–88. doi: 10.1007/s12016-020-08797-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ramirez GA, Gerosa M, Beretta L, Bellocchi C, Argolini LM, Moroni L, et al. COVID-19 in Systemic Lupus Erythematosus, Data From a Survey on 417 Patients. Semin Arthritis Rheum (2020) 50(5):1150–7. doi: 10.1016/j.semarthrit.2020.06.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Bsteh G, Bitschnau C, Hegen H, Auer M, Di Pauli F, Rommer P, et al. Multiple Sclerosis and COVID-19, How Many Are at Risk? Eur J Neurol (2020) 28(10):3369–74. doi: 10.1111/ene.14555 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Akiyama S, Hamdeh S, Micic D, Sakuraba A. Prevalence and Clinical Outcomes of COVID-19 in Patients With Autoimmune Diseases, a Systematic Review and Meta-Analysis. Ann Rheum Dis (2021) 80(3):384–91. doi: 10.1136/annrheumdis-2020-218946 [DOI] [PubMed] [Google Scholar]
- 10. Cortiula F, Pettke A, Bartoletti M, Puglisi F, Helleday T. Managing COVID-19 in the Oncology Clinic and Avoiding the Distraction Effect. Ann Oncol (2020) 31(5):553–5. doi: 10.1016/j.annonc.2020.03.286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Rogado J, Pangua C, Serrano-Montero G, Obispo B, Marino AM, Perez-Perez M, et al. Covid-19 and Lung Cancer, A Greater Fatality Rate? Lung Cancer (2020) 146:19–22. doi: 10.1016/j.lungcan.2020.05.034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Tian J, Yuan X, Xiao J, Zhong Q, Yang C, Liu B, et al. Clinical Characteristics and Risk Factors Associated With COVID-19 Disease Severity in Patients With Cancer in Wuhan, China, a Multicentre, Retrospective, Cohort Study. Lancet Oncol (2020) 21(7):893–903. doi: 10.1016/S1470-2045(20)30309-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Yang K, Sheng Y, Huang C, Jin Y, Xiong N, Jiang K, et al. Clinical Characteristics, Outcomes, and Risk Factors for Mortality in Patients With Cancer and COVID-19 in Hubei, China, a Multicentre, Retrospective, Cohort Study. Lancet Oncol (2020) 21(7):904–13. doi: 10.1016/S1470-2045(20)30310-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Zhang L, Zhu F, Xie L, Wang C, Wang J, Chen R, et al. Clinical Characteristics of COVID-19-Infected Cancer Patients, a Retrospective Case Study in Three Hospitals Within Wuhan, China. Ann Oncol (2020) 31(7):894–901. doi: 10.1016/j.annonc.2020.03.296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dai M, Liu D, Liu M, Zhou F, Li G, Chen Z, et al. Patients With Cancer Appear More Vulnerable to SARS-CoV-2, A Multicenter Study During the COVID-19 Outbreak. Cancer Discov (2020) 10(6):783–91. doi: 10.1158/2159-8290.CD-20-0422 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Cavanna L, Citterio C, Toscani I, Franco C, Magnacavallo A, Caprioli S, et al. Cancer Patients With COVID-19, a Retrospective Study of 51 Patients in the District of Piacenza, Northern Italy. Future Sci OA (2020) 7(1):FSO645. doi: 10.2144/fsoa-2020-0157 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Di Lorenzo G, Buonerba L, Ingenito C, Crocetto F, Buonerba C, Libroia A, et al. Clinical Characteristics of Metastatic Prostate Cancer Patients Infected With COVID-19 in South Italy. Oncology (2020) 98(10):743–7. doi: 10.1159/000509434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Pietrantonio F, Garassino MC. Caring for Patients With Cancer During the COVID-19 Outbreak in Italy. JAMA Oncol (2020) 6(6):821–2. doi: 10.1001/jamaoncol.2020.1426 [DOI] [PubMed] [Google Scholar]
- 19. Yu J, Ouyang W, Chua MLK, Xie C. SARS-CoV-2 Transmission in Patients With Cancer at a Tertiary Care Hospital in Wuhan, China. JAMA Oncol (2020) 6(7):1108–10. doi: 10.1001/jamaoncol.2020.0980 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Passaro A, Addeo A, Von Garnier C, Blackhall F, Planchard D, Felip E, et al. ESMO Management and Treatment Adapted Recommendations in the COVID-19 Era, Lung Cancer. ESMO Open (2020) 5(Suppl 3). doi: 10.1136/esmoopen-2020-000820 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Gosain R, Abdou Y, Singh A, Rana N, Puzanov I, Ernstoff MS. COVID-19 and Cancer, a Comprehensive Review. Curr Oncol Rep (2020) 22(5):53. doi: 10.1007/s11912-020-00934-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Askanase AD, Khalili L, Buyon JP. Thoughts on COVID-19 and Autoimmune Diseases. Lupus Sci Med (2020) 7(1):e000396. doi: 10.1136/lupus-2020-000396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Willis MD, Robertson NP. Multiple Sclerosis and the Risk of Infection, Considerations in the Threat of the Novel Coronavirus, COVID-19/SARS-CoV-2. J Neurol (2020) 267(5):1567–9. doi: 10.1007/s00415-020-09822-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Fernandez-Ruiz R, Paredes JL, Niewold TB. COVID-19 in Patients With Systemic Lupus Erythematosus, Lessons Learned From the Inflammatory Disease. Transl Res (2021) 232:13–36. doi: 10.1016/j.trsl.2020.12.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Mathian A, Mahevas M, Rohmer J, Roumier M, Cohen-Aubart F, Amador-Borrero B, et al. Clinical Course of Coronavirus Disease 2019 (COVID-19) in a Series of 17 Patients With Systemic Lupus Erythematosus Under Long-Term Treatment With Hydroxychloroquine. Ann Rheum Dis (2020) 79(6):837–9. doi: 10.1136/annrheumdis-2020-218795 [DOI] [PubMed] [Google Scholar]
- 26. Favalli EG, Gerosa M, Murgo A, Caporali R. Are Patients With Systemic Lupus Erythematosus at Increased Risk for COVID-19? Ann Rheum Dis (2021) 80(2):e25. doi: 10.1136/annrheumdis-2020-217787 [DOI] [PubMed] [Google Scholar]
- 27. Lefebvre M, Vignier N, Pitard B, Botelho-Nevers E, Wyplosz B, Cohen R, et al. COVID-19 Vaccines, Frequently Asked Questions and Updated Answers. Infect Dis Now (2021) 51(4):319–33. doi: 10.1016/j.idnow.2021.02.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Kaptein SJF, Jacobs S, Langendries L, Seldeslachts L, Ter Horst S, Liesenborghs L, et al. Favipiravir at High Doses has Potent Antiviral Activity in SARS-CoV-2-Infected Hamsters, Whereas Hydroxychloroquine Lacks Activity. Proc Natl Acad Sci USA (2020) 117(43):26955–65. doi: 10.1073/pnas.2014441117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Liu J, Bodnar BH, Meng F, Khan AI, Wang X, Saribas S, et al. Epigallocatechin Gallate From Green Tea Effectively Blocks Infection of SARS-CoV-2 and New Variants by Inhibiting Spike Binding to ACE2 Receptor. Cell Biosci (2021) 11(1):168. doi: 10.1186/s13578-021-00680-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Henss L, Auste A, Schürmann C, Schmidt C, von Rhein C, Mühlebach MD, et al. The Green Tea Catechin Epigallocatechin Gallate Inhibits SARS-CoV-2 Infection. J Gen Virol (2021) 102(4):001574. doi: 10.1099/jgv.0.001574 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Bonuccelli G, Sotgia F, Lisanti MP. Matcha Green Tea (MGT) Inhibits the Propagation of Cancer Stem Cells (CSCs), by Targeting Mitochondrial Metabolism, Glycolysis and Multiple Cell Signalling Pathways. Aging (Albany NY) (2018) 10(8):1867–83. doi: 10.18632/aging.101483 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Keckstein S, Tilgener C, Jeschke U, Hofmann S, Vilsmaier T, Kaltofen T, et al. Effects of Matcha Tea Extract on Cell Viability and Peroxisome Proliferator-Activated Receptor γ Expression on T47D Breast Cancer Cells. Arch Gynecol Obstet (2022). doi: 10.1007/s00404-021-06381-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Westerlind H, Palmqvist I, Saevarsdottir S, Alfredsson L, Klareskog L, Di Giuseppe D. Is Tea Consumption Associated With Reduction of Risk of Rheumatoid Arthritis? A Swedish case-control study. Arthritis Res Ther (2021) 23(1):209. doi: 10.1186/s13075-021-02583-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Saleh F, Raghupathy R, Asfar S, Oteifa M, Al-Saleh N. Analysis of the Effect of the Active Compound of Green Tea (EGCG) on the Proliferation of Peripheral Blood Mononuclear Cells. BMC Complement Altern Med (2014) 14:322. doi: 10.1186/1472-6882-14-322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Kirtipal N, Bharadwaj S, Kang SG. From SARS to SARS-CoV-2, Insights on Structure, Pathogenicity and Immunity Aspects of Pandemic Human Coronaviruses. Infect Genet Evol (2020) 85:104502. doi: 10.1016/j.meegid.2020.104502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Wang MY, Zhao R, Gao LJ, Gao XF, Wang DP, Cao JM. SARS-CoV-2: Structure, Biology, and Structure-Based Therapeutics Development. Front Cell Infect Microbiol (2020) 10:587269. doi: 10.3389/fcimb.2020.587269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Kadam SB, Sukhramani GS, Bishnoi P, Pable AA, Barvkar VT. SARS-CoV-2, the Pandemic Coronavirus, Molecular and Structural Insights. J Basic Microbiol (2021) 61(3):180–202. doi: 10.1002/jobm.202000537 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Harrison AG, Lin T, Wang P. Mechanisms of SARS-CoV-2 Transmission and Pathogenesis. Trends Immunol (2020) 41(12):1100–15. doi: 10.1016/j.it.2020.10.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Elhusseiny KM, Abd-Elhay FA, Kamel MG. Possible Therapeutic Agents for COVID-19, a Comprehensive Review. Expert Rev Anti Infect Ther (2020) 18(10):1005–20. doi: 10.1080/14787210.2020.1782742 [DOI] [PubMed] [Google Scholar]
- 40. Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and Chloroquine Effectively Inhibit the Recently Emerged Novel Coronavirus (2019-Ncov) In Vitro . Cell Res (2020) 30(3):269–71. doi: 10.1038/s41422-020-0282-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Ferron F, Subissi L, Silveira De Morais AT, Le NTT, Sevajol M, Gluais L, et al. Structural and Molecular Basis of Mismatch Correction and Ribavirin Excision From Coronavirus RNA. Proc Natl Acad Sci USA (2018) 115(2):E162–71. doi: 10.1073/pnas.1718806115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Omrani AS, Saad MM, Baig K, Bahloul A, Abdul-Matin M, Alaidaroos AY, et al. Ribavirin and Interferon Alfa-2a for Severe Middle East Respiratory Syndrome Coronavirus Infection, a Retrospective Cohort Study. Lancet Infect Dis (2014) 14(11):1090–5. doi: 10.1016/S1473-3099(14)70920-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Prakash A, Singh H, Kaur H, Semwal A, Sarma P, Bhattacharyya A, et al. Systematic Review and Meta-Analysis of Effectiveness and Safety of Favipiravir in the Management of Novel Coronavirus (COVID-19) Patients. Indian J Pharmacol (2020) 52(5):414–21. doi: 10.4103/ijp.ijp_998_20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Pilkington V, Pepperrell T, Hill A. A Review of the Safety of Favipiravir - a Potential Treatment in the COVID-19 Pandemic? J Virus Erad (2020) 6(2):45–51. doi: 10.1016/S2055-6640(20)30016-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Lou Y, Liu L, Yao H, Hu X, Su J, Xu K, et al. Clinical Outcomes and Plasma Concentrations of Baloxavir Marboxil and Favipiravir in COVID-19 Patients, An Exploratory Randomized, Controlled Trial. Eur J Pharm Sci (2021) 157:105631. doi: 10.1016/j.ejps.2020.105631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the Treatment of Covid-19 - Final Report. N Engl J Med (2020) 383(19):1813–26. doi: 10.1056/NEJMc2022236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Goldman JD, Lye DCB, Hui DS, Marks KM, Bruno R, Montejano R, et al. Remdesivir for 5 or 10 Days in Patients With Severe Covid-19. N Engl J Med (2020) 383(19):1827–37. doi: 10.1056/NEJMoa2015301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Mulangu S, Dodd LE, Davey RT, Jr., Tshiani Mbaya O, Proschan M, Mukadi D, et al. A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics. N Engl J Med (2019) 381(24):2293–303. doi: 10.1056/NEJMoa1910993 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Jin Y, Yang H, Ji W, Wu W, Chen S, Zhang W, et al. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses (2020) 12(4):372. doi: 10.3390/v12040372 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Friess H, Kleeff J, Isenmann R, Malfertheiner P, Buchler MW. Adaptation of the Human Pancreas to Inhibition of Luminal Proteolytic Activity. Gastroenterology (1998) 115(2):388–96. doi: 10.1016/S0016-5085(98)70205-7 [DOI] [PubMed] [Google Scholar]
- 51. Chakraborty C, Sharma AR, Bhattacharya M, Agoramoorthy G, Lee SS. The Drug Repurposing for COVID-19 Clinical Trials Provide Very Effective Therapeutic Combinations, Lessons Learned From Major Clinical Studies. Front Pharmacol (2021) 12:704205. doi: 10.3389/fphar.2021.704205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Triant VA, Siedner MJ. Darunavir and Cardiovascular Risk, Evaluating the Data to Inform Clinical Care. J Infect Dis (2020) 221(4):498–500. doi: 10.1093/infdis/jiz482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Chen X, Yin YH, Zhang MY, Liu JY, Li R, Qu YQ. Investigating the Mechanism of ShuFeng JieDu Capsule for the Treatment of Novel Coronavirus Pneumonia (COVID-19) Based on Network Pharmacology. Int J Med Sci (2020) 17(16):2511–30. doi: 10.7150/ijms.46378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized With Severe Covid-19. N Engl J Med (2020) 382(19):1787–99. doi: 10.1056/NEJMc2008043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Saleh M, Gabriels J, Chang D, Fishbein J, Qiu M, Mountantonakis SE, et al. Safely Administering Potential QTc Prolonging Therapy Across a Large Health Care System in the COVID-19 Era. Circ Arrhythm Electrophysiol (2020) 13(11):e008937. doi: 10.1161/CIRCEP.120.008937 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Mercuro NJ, Yen CF, Shim DJ, Maher TR, McCoy CM, Zimetbaum PJ, et al. Risk of QT Interval Prolongation Associated With Use of Hydroxychloroquine With or Without Concomitant Azithromycin Among Hospitalized Patients Testing Positive for Coronavirus Disease 2019 (COVID-19). JAMA Cardiol (2020) 5(9):1036–41. doi: 10.1001/jamacardio.2020.1834 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Chorin E, Wadhwani L, Magnani S, Stefano C, Chinitz LA, Jankelson L, et al. QT Interval Prolongation and Torsade De Pointes in Patients With COVID-19 Treated With Hydroxychloroquine/Azithromycin. Heart Rhythm (2020) 17(9):1425–33. doi: 10.1016/j.hrthm.2020.05.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Touret F, de Lamballerie X. Of Chloroquine and COVID-19. Antiviral Res (2020) 177:104762. doi: 10.1016/j.antiviral.2020.104762 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Cavalcanti AB, Zampieri FG, Rosa RG, Azevedo LCP, Veiga VC, Avezum A, et al. Hydroxychloroquine With or Without Azithromycin in Mild-To-Moderate Covid-19. N Engl J Med (2020) 383(21):2041–52. doi: 10.1056/NEJMx200021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Pepperrell T, Pilkington V, Owen A, Wang J, Hill AM. Review of Safety and Minimum Pricing of Nitazoxanide for Potential Treatment of COVID-19. J Virus Erad (2020) 6(2):52–60. doi: 10.1016/S2055-6640(20)30017-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Nojomi M, Yassin Z, Keyvani H, Makiani MJ, Roham M, Laali A, et al. Effect of Arbidol (Umifenovir) on COVID-19, a Randomized Controlled Trial. BMC Infect Dis (2020) 20(1):954. doi: 10.1186/s12879-020-05698-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Estacio RO, Jeffers BW, Hiatt WR, Biggerstaff SL, Gifford N, Schrier RW. The Effect of Nisoldipine as Compared With Enalapril on Cardiovascular Outcomes in Patients With Non-Insulin-Dependent Diabetes and Hypertension. N Engl J Med (1998) 338(10):645–52. doi: 10.1056/NEJM199803053381003 [DOI] [PubMed] [Google Scholar]
- 63. Aghili R, Honardoost M, Khamseh ME. COVID-19, Case Fatality and ACE2 Inhibitors Treatment Concerns in Patients With Comorbidities. Med J Islam Repub Iran (2020) 34:147. doi: 10.47176/mjiri.34.147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Lopes RD, Macedo AVS, de Barros ESPGM, Moll-Bernardes RJ, Dos Santos TM, Mazza L, et al. Effect of Discontinuing vs Continuing Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers on Days Alive and Out of the Hospital in Patients Admitted With COVID-19, A Randomized Clinical Trial. JAMA (2021) 325(3):254–64. doi: 10.1001/jama.2020.25864 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Abd El-Aziz TM, Al-Sabi A, Stockand JD. Human Recombinant Soluble ACE2 (Hrsace2) Shows Promise for Treating Severe COVID-19. Signal Transduct Target Ther (2020) 5(1):258. doi: 10.1038/s41392-020-00374-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Ragia G, Manolopoulos VG. Inhibition of SARS-CoV-2 Entry Through the ACE2/TMPRSS2 Pathway, a Promising Approach for Uncovering Early COVID-19 Drug Therapies. Eur J Clin Pharmacol (2020) 76(12):1623–30. doi: 10.1007/s00228-020-02963-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Casadevall A, Joyner MJ, Pirofski LA. A Randomized Trial of Convalescent Plasma for COVID-19-Potentially Hopeful Signals. JAMA (2020) 324(5):455–7. doi: 10.1001/jama.2020.10218 [DOI] [PubMed] [Google Scholar]
- 68. Li L, Zhang W, Hu Y, Tong X, Zheng S, Yang J, et al. Effect of Convalescent Plasma Therapy on Time to Clinical Improvement in Patients With Severe and Life-Threatening COVID-19, A Randomized Clinical Trial. JAMA (2020) 324(5):460–70. doi: 10.1001/jama.2020.12607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. van Griensven J, Edwards T, de Lamballerie X, Semple MG, Gallian P, Baize S, et al. Evaluation of Convalescent Plasma for Ebola Virus Disease in Guinea. N Engl J Med (2016) 374(1):33–42. doi: 10.1056/NEJMoa1511812 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Dulipsingh L, Ibrahim D, Schaefer EJ, Crowell R, Diffenderfer MR, Williams K, et al. SARS-CoV-2 Serology and Virology Trends in Donors and Recipients of Convalescent Plasma. Transfus Apher Sci (2020) 59(6):102922. doi: 10.1016/j.transci.2020.102922 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Singh TU, Parida S, Lingaraju MC, Kesavan M, Kumar D, Singh RK. Drug Repurposing Approach to Fight COVID-19. Pharmacol Rep (2020) 72(6):1479–508. doi: 10.1007/s43440-020-00155-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Toniati P, Piva S, Cattalini M, Garrafa E, Regola F, Castelli F, et al. Tocilizumab for the Treatment of Severe COVID-19 Pneumonia With Hyperinflammatory Syndrome and Acute Respiratory Failure, A Single Center Study of 100 Patients in Brescia, Italy. Autoimmun Rev (2020) 19(7):102568. doi: 10.1016/j.autrev.2020.102568 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Stone JH, Frigault MJ, Serling-Boyd NJ, Fernandes AD, Harvey L, Foulkes AS, et al. Efficacy of Tocilizumab in Patients Hospitalized With Covid-19. N Engl J Med (2020) 383(24):2333–44. doi: 10.1056/NEJMoa2028836 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Alam S, Kamal TB, Sarker MMR, Zhou JR, Rahman SMA, Mohamed IN, et al. Therapeutic Effectiveness and Safety of Repurposing Drugs for the Treatment of COVID-19, Position Standing in 2021. Front Pharmacol (2021) 12:659577. doi: 10.3389/fphar.2021.659577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Shiehzadegan S, Alaghemand N, Fox M, Venketaraman V. Analysis of the Delta Variant B.1.617.2 COVID-19. Clin Pract (2021) 11(4):778–84. doi: 10.3390/clinpract11040093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Lopez Bernal J, Andrews N, Gower C, Gallagher E, Simmons R, Thelwall S, et al. Effectiveness of Covid-19 Vaccines Against the B.1.617.2 (Delta) Variant. N Engl J Med (2021) 385(7):585–94. doi: 10.1056/NEJMoa2108891 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. He X, Hong W, Pan X, Lu G, Wei X. SARS-CoV-2 Omicron Variant: Characteristics and Prevention. MedComm (2020) (2021) 2(4):838–45. doi: 10.1002/mco2.110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Pilishvili T, Gierke R, Fleming-Dutra KE, Farrar JL, Mohr NM, Talan DA, et al. Effectiveness of mRNA Covid-19 Vaccine Among U.S. Health Care Personnel N Engl J Med (2021) 385(25):e90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Lyons DM, Lauring AS. Mutation and Epistasis in Influenza Virus Evolution. Viruses (2018) 10(8):407. doi: 10.3390/v10080407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Mousa HA. Prevention and Treatment of Influenza, Influenza-Like Illness, and Common Cold by Herbal, Complementary, and Natural Therapies. J Evid Based Complement Altern Med (2017) 22(1):166–74. doi: 10.1177/2156587216641831 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Parry H, McIlroy G, Bruton R, Damery S, Tyson G, Logan N, et al. Impaired Neutralisation of SARS-CoV-2 Delta Variant in Vaccinated Patients With B Cell Chronic Lymphocytic Leukaemia. J Hematol Oncol (2022) 15(1):3. doi: 10.1186/s13045-021-01219-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Valanparambil R, Carlisle J, Linderman S, Akthar A, Millett RL, Lai L, et al. Antibody Response to SARS-CoV-2 mRNA Vaccine in Lung Cancer Patients, Reactivity to Vaccine Antigen and Variants of Concern. medRxiv (2022). doi: 10.1101/2022.01.03.22268599 [DOI] [Google Scholar]
- 83. Mirzaie A, Halaji M, Dehkordi FS, Ranjbar R, Noorbazargan H. A Narrative Literature Review on Traditional Medicine Options for Treatment of Corona Virus Disease 2019 (COVID-19). Complement Ther Clin Pract (2020) 40:101214. doi: 10.1016/j.ctcp.2020.101214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Ang L, Lee HW, Kim A, Lee JA, Zhang J, Lee MS. Herbal Medicine for Treatment of Children Diagnosed With COVID-19, A Review of Guidelines. Complement Ther Clin Pract (2020) 39:101174. doi: 10.1016/j.ctcp.2020.101174 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Kabir MT, Uddin MS, Hossain MF, Abdulhakim JA, Alam MA, Ashraf GM, et al. nCOVID-19 Pandemic, From Molecular Pathogenesis to Potential Investigational Therapeutics. Front Cell Dev Biol (2020) 8. doi: 10.3389/fcell.2020.00616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Hossain MF, Hasana S, Mamun AA, Uddin MS, Wahed MII, Sarker S, et al. COVID-19 Outbreak, Pathogenesis, Current Therapies, and Potentials for Future Management. Front Pharmacol (2020) 11. doi: 10.3389/fphar.2020.563478 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Kumar R, Srivastava JK, Singh R, Siddiqui MH, Mansouri RA, Abdulhakim JA, et al. Available Compounds With Therapeutic Potential Against COVID-19, Antimicrobial Therapies, Supportive Care, and Probable Vaccines. Front Pharmacol (2020) 11. doi: 10.3389/fphar.2020.582025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Masoud AT, Zaazouee MS, Elsayed SM, Ragab KM, Kamal EM, Alnasser YT, et al. KAP-COVIDGLOBAL, a Multinational Survey of the Levels and Determinants of Public Knowledge, Attitudes and Practices Towards COVID-19. BMJ Open (2021) 11(2):e043971. doi: 10.1136/bmjopen-2020-043971 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Huang J, Tao G, Liu J, Cai J, Huang Z, Chen JX. Current Prevention of COVID-19, Natural Products and Herbal Medicine. Front Pharmacol (2020) 11:588508. doi: 10.3389/fphar.2020.588508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Nugraha RV, Ridwansyah H, Ghozali M, Khairani AF, Atik N. Traditional Herbal Medicine Candidates as Complementary Treatments for COVID-19, A Review of Their Mechanisms, Pros and Cons. Evid Based Complement Alternat Med (2020) 2020:2560645. doi: 10.1155/2020/2560645 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Prasad S, Tyagi AK. Ginger and Its Constituents, Role in Prevention and Treatment of Gastrointestinal Cancer. Gastroenterol Res Pract (2015) 2015:142979. doi: 10.1155/2015/142979 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Mojaverrostami S, Bojnordi MN, Ghasemi-Kasman M, Ebrahimzadeh MA, Hamidabadi HG. A Review of Herbal Therapy in Multiple Sclerosis. Adv Pharm Bull (2018) 8(4):575–90. doi: 10.15171/apb.2018.066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Ali BH, Blunden G, Tanira MO, Nemmar A. Some Phytochemical, Pharmacological and Toxicological Properties of Ginger (Zingiber Officinale Roscoe), a Review of Recent Research. Food Chem Toxicol (2008) 46(2):409–20. doi: 10.1016/j.fct.2007.09.085 [DOI] [PubMed] [Google Scholar]
- 94. Ho SC, Chang KS, Lin CC. Anti-Neuroinflammatory Capacity of Fresh Ginger Is Attributed Mainly to 10-Gingerol. Food Chem (2013) 141(3):3183–91. doi: 10.1016/j.foodchem.2013.06.010 [DOI] [PubMed] [Google Scholar]
- 95. Haridas M, Sasidhar V, Nath P, Abhithaj J, Sabu A, Rammanohar P. Compounds of Citrus Medica and Zingiber Officinale for COVID-19 Inhibition, in Silico Evidence for Cues From Ayurveda. Futur J Pharm Sci (2021) 7(1):13. doi: 10.1186/s43094-020-00171-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. Giordano A, Tommonaro G. Curcumin and Cancer. Nutrients (2019) 11(10):2376. doi: 10.3390/nu11102376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Zheng Z, Sun Y, Liu Z, Zhang M, Li C, Cai H. The Effect of Curcumin and Its Nanoformulation on Adjuvant-Induced Arthritis in Rats. Drug Des Devel Ther (2015) 9:4931–42. doi: 10.2147/DDDT.S90147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Xue M, McKelvey K, Shen K, Minhas N, March L, Park SY, et al. Endogenous MMP-9 and Not MMP-2 Promotes Rheumatoid Synovial Fibroblast Survival, Inflammation and Cartilage Degradation. Rheumatol (Oxford) (2014) 53(12):2270–9. doi: 10.1093/rheumatology/keu254 [DOI] [PubMed] [Google Scholar]
- 99. Aggarwal BB, Gupta SC, Sung B. Curcumin, an Orally Bioavailable Blocker of TNF and Other Pro-Inflammatory Biomarkers. Br J Pharmacol (2013) 169(8):1672–92. doi: 10.1111/bph.12131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Shakibaei M, John T, Schulze-Tanzil G, Lehmann I, Mobasheri A, et al. Suppression of NF-KappaB Activation by Curcumin Leads to Inhibition of Expression of Cyclo-Oxygenase-2 and Matrix Metalloproteinase-9 in Human Articular Chondrocytes, Implications for the Treatment of Osteoarthritis. Biochem Pharmacol (2007) 73(9):1434–45. doi: 10.1016/j.bcp.2007.01.005 [DOI] [PubMed] [Google Scholar]
- 101. Natarajan C, Bright JJ. Curcumin Inhibits Experimental Allergic Encephalomyelitis by Blocking IL-12 Signaling Through Janus Kinase-STAT Pathway in T Lymphocytes. J Immunol (2002) 168(12):6506–13. doi: 10.4049/jimmunol.168.12.6506 [DOI] [PubMed] [Google Scholar]
- 102. Moore BA, Aznavoorian S, Engler JA, Windsor LJ. Induction of Collagenase-3 (MMP-13) in Rheumatoid Arthritis Synovial Fibroblasts. Biochim Biophys Acta (2000) 1502(2):307–18. doi: 10.1016/S0925-4439(00)00056-9 [DOI] [PubMed] [Google Scholar]
- 103. Jin H, Qiao F, Wang Y, Xu Y, Shang Y. Curcumin Inhibits Cell Proliferation and Induces Apoptosis of Human Non-Small Cell Lung Cancer Cells Through the Upregulation of miR-192-5p and Suppression of PI3K/Akt Signaling Pathway. Oncol Rep (2015) 34(5):2782–9. doi: 10.3892/or.2015.4258 [DOI] [PubMed] [Google Scholar]
- 104. Babaei F, Nassiri-Asl M, Hosseinzadeh H. Curcumin (a Constituent of Turmeric), New Treatment Option Against COVID-19. Food Sci Nutr (2020) 8(10):5215–27. doi: 10.1002/fsn3.1858 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Zhou X, Qian H, Zhang D, Zeng L. Garlic Intake and the Risk of Colorectal Cancer, A Meta-Analysis. Med (Baltimore) (2020) 99(1):e18575. doi: 10.1097/MD.0000000000018575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106. Tsubura A, Lai YC, Kuwata M, Uehara N, Yoshizawa K. Anticancer Effects of Garlic and Garlic-Derived Compounds for Breast Cancer Control. Anticancer Agents Med Chem (2011) 11(3):249–53. doi: 10.2174/187152011795347441 [DOI] [PubMed] [Google Scholar]
- 107. Lamm DL, Riggs DR. The Potential Application of Allium Sativum (Garlic) for the Treatment of Bladder Cancer. Urol Clin North Am (2000) 27(1):157–62, xi. doi: 10.1016/S0094-0143(05)70243-3 [DOI] [PubMed] [Google Scholar]
- 108. Ryu HW, Lee SU, Lee S, Song HH, Son TH, Kim YU, et al. 3-Methoxy-Catalposide Inhibits Inflammatory Effects in Lipopolysaccharide-Stimulated RAW264.7 Macrophages. Cytokine (2017) 91:57–64. doi: 10.1016/j.cyto.2016.12.006 [DOI] [PubMed] [Google Scholar]
- 109. Arreola R, Quintero-Fabian S, Lopez-Roa RI, Flores-Gutierrez EO, Reyes-Grajeda JP, Carrera-Quintanar L, et al. Immunomodulation and Anti-Inflammatory Effects of Garlic Compounds. J Immunol Res (2015) 2015: 401630. doi: 10.1155/2015/401630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Quintero-Fabian S, Ortuno-Sahagun D, Vazquez-Carrera M, Lopez-Roa RI. Alliin, a Garlic (Allium Sativum) Compound, Prevents LPS-Induced Inflammation in 3T3-L1 Adipocytes. Mediators Inflamm (2013) 2013:381815. doi: 10.1155/2013/381815 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Lei XY, Yao SQ, Zu XY, Huang ZX, Liu LJ, Zhong M, et al. Apoptosis Induced by Diallyl Disulfide in Human Breast Cancer Cell Line MCF-7. Acta Pharmacol Sin (2008) 29(10):1233–9. doi: 10.1111/j.1745-7254.2008.00851.x [DOI] [PubMed] [Google Scholar]
- 112. Altonsy MO, Habib TN, Andrews SC. Diallyl Disulfide-Induced Apoptosis in a Breast-Cancer Cell Line (MCF-7) may be Caused by Inhibition of Histone Deacetylation. Nutr Cancer (2012) 64(8):1251–60. doi: 10.1080/01635581.2012.721156 [DOI] [PubMed] [Google Scholar]
- 113. Shekh S, Reddy KKA, Gowd KH. In Silico Allicin Induced S-Thioallylation of SARS-CoV-2 Main Protease. J Sulfur Chem (2021) 42(1):109–20. doi: 10.1080/17415993.2020.1817457 [DOI] [Google Scholar]
- 114. Tannous S, Haykal T, Dhaini J, Hodroj MH, Rizk S. The Anti-Cancer Effect of Flaxseed Lignan Derivatives on Different Acute Myeloid Leukemia Cancer Cells. BioMed Pharmacother (2020) 132:110884. doi: 10.1016/j.biopha.2020.110884 [DOI] [PubMed] [Google Scholar]
- 115. Constantin MM, Nita IE, Olteanu R, Constantin T, Bucur S, Matei C, et al. Significance and Impact of Dietary Factors on Systemic Lupus Erythematosus Pathogenesis. Exp Ther Med (2019) 17(2):1085–90. doi: 10.3892/etm.2018.6986 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116. Hathaway D, Pandav K, Patel M, Riva-Moscoso A, Singh BM, Patel A, et al. Omega 3 Fatty Acids and COVID-19, A Comprehensive Review. Infect Chemother (2020) 52(4):478–95. doi: 10.3947/ic.2020.52.4.478 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117. Cheng FJ, Huynh TK, Yang CS, Hu DW, Shen YC, Tu CY, et al. Hesperidin Is a Potential Inhibitor Against SARS-CoV-2 Infection. Nutrients (2021) 13(8):2800. doi: 10.3390/nu13082800 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Haghmorad D, Mahmoudi MB, Salehipour Z, Jalayer Z, Momtazi Brojeni AA, Rastin M, et al. Hesperidin Ameliorates Immunological Outcome and Reduces Neuroinflammation in the Mouse Model of Multiple Sclerosis. J Neuroimmunol (2017) 302:23–33. doi: 10.1016/j.jneuroim.2016.11.009 [DOI] [PubMed] [Google Scholar]
- 119. Wei D, Ci X, Chu X, Wei M, Hua S, Deng X, et al. Hesperidin Suppresses Ovalbumin-Induced Airway Inflammation in a Mouse Allergic Asthma Model. Inflammation (2012) 35(1):114–21. doi: 10.1007/s10753-011-9295-7 [DOI] [PubMed] [Google Scholar]
- 120. Abdallah RM, Elkhouly AM, Soliman RA, El Mechawy N, El Sebaei A, Motaal AA, et al. Hindering the Synchronization Between miR-486-5p and H19 lncRNA by Hesperetin Halts Breast Cancer Aggressiveness Through Tuning ICAM-1. Anticancer Agents Med Chem (2022) 22(3):586–95. doi: 10.2174/1871520621666210419093652 [DOI] [PubMed] [Google Scholar]
- 121. Pan H, Wang F, Rankin GO, Rojanasakul Y, Tu Y, Chen YC. Inhibitory Effect of Black Tea Pigments, Theaflavin3/3’-Gallate Against Cisplatin-Resistant Ovarian Cancer Cells by Inducing Apoptosis and G1 Cell Cycle Arrest. Int J Oncol (2017) 51(5):1508–20. doi: 10.3892/ijo.2017.4145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Way TD, Lee HH, Kao MC, Lin JK. Black Tea Polyphenol Theaflavins Inhibit Aromatase Activity and Attenuate Tamoxifen Resistance in HER2/neu-Transfected Human Breast Cancer Cells Through Tyrosine Kinase Suppression. Eur J Cancer (2004) 40(14):2165–74. doi: 10.1016/j.ejca.2004.06.018 [DOI] [PubMed] [Google Scholar]
- 123. Gao Y, Rankin GO, Tu Y, Chen YC. Theaflavin-3, 3’-Digallate Decreases Human Ovarian Carcinoma OVCAR-3 Cell-Induced Angiogenesis via Akt and Notch-1 Pathways, Not via MAPK Pathways. Int J Oncol (2016) 48(1):281–92. doi: 10.3892/ijo.2015.3257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124. Liu W, Li J. Theaflavin-3, 3’-Digallate Attenuates Rheumatoid Inflammation in Mice Through the Nuclear Factor-kappaB and MAPK Pathways. Arch Immunol Ther Exp (Warsz) (2019) 67(3):153–60. doi: 10.1007/s00005-019-00536-7 [DOI] [PubMed] [Google Scholar]
- 125. Banerjee A, Kanwar M, Maiti S. Theaflavin-3’-O-Gallate a Black-Tea Constituent Blocked SARS CoV-2 RNA Dependant RNA Polymerase Active-Site With Better Docking Results Than Remdesivir. Drug Res (Stuttg) (2021) 71(8):462–72. doi: 10.1055/a-1467-5828 [DOI] [PubMed] [Google Scholar]
- 126. Almatroodi SA, Almatroudi A, Khan AA, Alhumaydhi FA, Alsahli MA, Rahmani AH. Potential Therapeutic Targets of Epigallocatechin Gallate (EGCG), the Most Abundant Catechin in Green Tea, and Its Role in the Therapy of Various Types of Cancer. Molecules (2020) 25(14):3146. doi: 10.3390/molecules25143146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127. Rauf A, Imran M, Khan IA, Ur-Rehman M, Gilani SA, Mehmood Z, et al. Anticancer Potential of Quercetin, A Comprehensive Review. Phytother Res (2018) 32(11):2109–30. doi: 10.1002/ptr.6155 [DOI] [PubMed] [Google Scholar]
- 128. Li QS, Wang YQ, Liang YR, Lu JL. The Anti-Allergic Potential of Tea, a Review of Its Components, Mechanisms and Risks. Food Funct (2021) 12(1):57–69. doi: 10.1039/D0FO02091E [DOI] [PubMed] [Google Scholar]
- 129. Maurya AK, Vinayak M. Anticarcinogenic Action of Quercetin by Downregulation of Phosphatidylinositol 3-Kinase (PI3K) and Protein Kinase C (PKC) via Induction of P53 in Hepatocellular Carcinoma (HepG2) Cell Line. Mol Biol Rep (2015) 42(9):1419–29. doi: 10.1007/s11033-015-3921-7 [DOI] [PubMed] [Google Scholar]
- 130. Guan X, Gao M, Xu H, Zhang C, Liu H, Lv L, et al. Quercetin-Loaded Poly (Lactic-Co-Glycolic Acid)-D-Alpha-Tocopheryl Polyethylene Glycol 1000 Succinate Nanoparticles for the Targeted Treatment of Liver Cancer. Drug Delivery (2016) 23(9):3307–18. doi: 10.1080/10717544.2016.1176087 [DOI] [PubMed] [Google Scholar]
- 131. Ghosh R, Chakraborty A, Biswas A, Chowdhuri S. Evaluation of Green Tea Polyphenols as Novel Corona Virus (SARS CoV-2) Main Protease (Mpro) Inhibitors - an in Silico Docking and Molecular Dynamics Simulation Study. J Biomol Struct Dyn (2021) 39(12):4362–74. doi: 10.1080/07391102.2020.1779818 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Derosa G, Maffioli P, D’Angelo A, Di Pierro F. A Role for Quercetin in Coronavirus Disease 2019 (COVID-19). Phytother Res (2021) 35(3):1230–6. doi: 10.1002/ptr.6887 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Brinker AM, Ma J, Lipsky PE, Raskin I. Medicinal Chemistry and Pharmacology of Genus Tripterygium (Celastraceae). Phytochemistry (2007) 68(6):732–66. doi: 10.1016/j.phytochem.2006.11.029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Kiviharju TM, Lecane PS, Sellers RG, Peehl DM. Antiproliferative and Proapoptotic Activities of Triptolide (PG490), a Natural Product Entering Clinical Trials, on Primary Cultures of Human Prostatic Epithelial Cells. Clin Cancer Res (2002) 8(8):2666–74. [PubMed] [Google Scholar]
- 135. Zhu W, Li J, Wu S, Li S, Le L, Su X, et al. Triptolide Cooperates With Cisplatin to Induce Apoptosis in Gemcitabine-Resistant Pancreatic Cancer. Pancreas (2012) 41(7):1029–38. doi: 10.1097/MPA.0b013e31824abdc0 [DOI] [PubMed] [Google Scholar]
- 136. Gong Y, Huang X, Wang D, Li M, Liu Z. Triptolide Protects Bone Against Destruction by Targeting RANKL-Mediated ERK/AKT Signalling Pathway in the Collagen-Induced Rheumatoid Arthritis. Biomed Res (2017) 28(9):4111–6. [Google Scholar]
- 137. Teixeira A, DaCunha DC, Barros L, Caires HR, Xavier CPR, Ferreira I, et al. Eucalyptus Globulus Labill. Decoction Extract Inhibits the Growth of NCI-H460 Cells by Increasing the P53 Levels and Altering the Cell Cycle Profile. Food Funct (2019) 10(6):3188–97. doi: 10.1039/C8FO02466A [DOI] [PubMed] [Google Scholar]
- 138. Greiner JF, Muller J, Zeuner MT, Hauser S, Seidel T, Klenke C, et al. 1,8-Cineol Inhibits Nuclear Translocation of NF-kappaB P65 and NF-kappaB-Dependent Transcriptional Activity. Biochim Biophys Acta (2013) 1833(12):2866–78. doi: 10.1016/j.bbamcr.2013.07.001 [DOI] [PubMed] [Google Scholar]
- 139. Panikar S, Shoba G, Arun M, Sahayarayan JJ, Usha Raja Nanthini A, Chinnathambi A, et al. Essential Oils as an Effective Alternative for the Treatment of COVID-19, Molecular Interaction Analysis of Protease (M(pro)) With Pharmacokinetics and Toxicological Properties. J Infect Public Health (2021) 14(5):601–10. doi: 10.1016/j.jiph.2020.12.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140. Signer J, Jonsdottir HR, Albrich WC, Strasser M, Züst R, Ryter S, et al. In Vitro Virucidal Activity of Echinaforce®, an Echinacea Purpurea Preparation, Against Coronaviruses, Including Common Cold Coronavirus 229E and SARS-CoV-2. Virol J (2020) 17(1):136. doi: 10.1186/s12985-020-01401-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Shree P, Mishra P, Selvaraj C, Singh SK, Chaube R, Garg N, et al. Targeting COVID-19 (SARS-CoV-2) Main Protease Through Active Phytochemicals of Ayurvedic Medicinal Plants - Withania Somnifera (Ashwagandha), Tinospora Cordifolia (Giloy) and Ocimum Sanctum (Tulsi) - a Molecular Docking Study. J Biomol Struct Dyn (2022) 40(1):190–203. doi: 10.1080/07391102.2020.1810778 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142. Kumar V, Dhanjal JK, Bhargava P, Kaul A, Wang J, Zhang H, et al. Withanone and Withaferin-A Are Predicted to Interact With Transmembrane Protease Serine 2 (TMPRSS2) and Block Entry of SARS-CoV-2 Into Cells. J Biomol Struct Dyn (2022) 40(1):1–13. doi: 10.1080/07391102.2020.1775704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143. Rocha FAC, de Assis MR. Curcumin as a Potential Treatment for COVID-19. Phytother Res (2020) 34(9):2085–7. doi: 10.1002/ptr.6745 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144. Messina G, Polito R, Monda V, Cipolloni L, Di Nunno N, Di Mizio G, et al. Functional Role of Dietary Intervention to Improve the Outcome of COVID-19, A Hypothesis of Work. Int J Mol Sci (2020) 21(9):3104. doi: 10.3390/ijms21093104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145. Wu C, Liu Y, Yang Y, Zhang P, Zhong W, Wang Y, et al. Analysis of Therapeutic Targets for SARS-CoV-2 and Discovery of Potential Drugs by Computational Methods. Acta Pharm Sin B (2020) 10(5):766–88. doi: 10.1016/j.apsb.2020.02.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146. Yadav PK, Jaiswal A, Singh RK. In Silico Study on Spice-Derived Antiviral Phytochemicals Against SARS-CoV-2 TMPRSS2 Target. J Biomol Struct Dyn (2021) p:1–11. doi: 10.1080/07391102.2021.1965658 [DOI] [PubMed] [Google Scholar]
- 147. Oluyori AP, Olanipekun BE, Adeyemi OS, Egharevba GO, Adegboyega AE, Oladeji OS. Pharmacophore Modelling, MD Simulation and in Silico ADMET Study Reveals Bitter Cola Constituents as Potential Inhibitors of SARS-CoV-2 Main Protease and RNA Dependent-RNA Polymerase. J Biomol Struct Dyn (2022) p:1–16. doi: 10.1080/07391102.2021.2024883 [DOI] [PubMed] [Google Scholar]
- 148. Nguyen TT, Woo HJ, Kang HK, Nguyen VD, Kim YM, Kim DW, et al. Flavonoid-Mediated Inhibition of SARS Coronavirus 3C-Like Protease Expressed in Pichia Pastoris. Biotechnol Lett (2012) 34(5):831–8. doi: 10.1007/s10529-011-0845-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149. Perricone C, Bartoloni E, Gerli R. Colchicine, an Anti-Rheumatic Agent, as a Potential Compound for the Treatment of COVID-19. Reumatologia (2020) 58(5):261–4. doi: 10.5114/reum.2020.100088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150. Kim JW, Ha TK, Cho H, Kim E, Shim SH, Yang JL, et al. Antiviral Escin Derivatives From the Seeds of Aesculus Turbinata Blume (Japanese Horse Chestnut). Bioorg Med Chem Lett (2017) 27(13):3019–25. doi: 10.1016/j.bmcl.2017.05.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151. Leung JM, Yang CX, Sin DD. COVID-19 and Nicotine as a Mediator of ACE-2. Eur Respir J (2020) 55(6):2001261. doi: 10.1183/13993003.01261-2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152. Alam S, Sarker MMR, Afrin S, Richi FT, Zhao C, Zhou JR, et al. Traditional Herbal Medicines, Bioactive Metabolites, and Plant Products Against COVID-19, Update on Clinical Trials and Mechanism of Actions. Front Pharmacol (2021) 12:671498. doi: 10.3389/fphar.2021.671498 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153. Xia J, Rong L, Sawakami T, Inagaki Y, Song P, Hasegawa K, et al. Shufeng Jiedu Capsule and Its Active Ingredients Induce Apoptosis, Inhibit Migration and Invasion, and Enhances Doxorubicin Therapeutic Efficacy in Hepatocellular Carcinoma. BioMed Pharmacother (2018) 99:921–30. doi: 10.1016/j.biopha.2018.01.163 [DOI] [PubMed] [Google Scholar]
- 154. Li H, Liu L, Zhang D, Xu J, Dai H, Tang N, et al. SARS-CoV-2 and Viral Sepsis, Observations and Hypotheses. Lancet (2020) 395(10235):1517–20. doi: 10.1016/S0140-6736(20)30920-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155. Zhong W-T, Wu Y-C, Xie X-X, Zhou X, Wei M-M, Soromou L-W, et al. Phillyrin Attenuates LPS-Induced Pulmonary Inflammation via Suppression of MAPK and NF-κb Activation in Acute Lung Injury Mice. Fitoterapia (2013) 90:132–9. doi: 10.1016/j.fitote.2013.06.003 [DOI] [PubMed] [Google Scholar]
- 156. Zheng X-Y, Yang S-M, Zhang R, Wang S-M, Li G-B, Zhou S-W. Emodin-Induced Autophagy Against Cell Apoptosis Through the PI3K/AKT/mTOR Pathway in Human Hepatocytes. Drug design Dev Ther (2019) 13:3171. doi: 10.2147/DDDT.S204958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157. Xia L, Shi Y, Su J, Friedemann T, Tao Z, Lu Y, et al. Shufeng Jiedu, a Promising Herbal Therapy for Moderate COVID-19:Antiviral and Anti-Inflammatory Properties, Pathways of Bioactive Compounds, and a Clinical Real-World Pragmatic Study. Phytomedicine (2021) 85:153390. doi: 10.1016/j.phymed.2020.153390 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158. Xiao Q, Jiang Y, Wu S. Analysis of the Value of Traditional Chinese Medicine Shufeng Jiedu Capsule Combined With Arbidol in the Treatment of Mild New Coronavirus Pneumonia. Emergency (2020) 29:756–8. [Google Scholar]
- 159. Qu X-K. Observation on Clinical Effect of Shufeng Jiedu Capsule Combined With Arbidol Hydrochloride Capsule in Treatment of COVID-19. Chin Traditional Herbal Drugs (2020) p:1167–70. [Google Scholar]
- 160. Park EJ, Pezzuto JM. Botanicals in Cancer Chemoprevention. Cancer Metastasis Rev (2002) 21(3-4):231–55. doi: 10.1023/A:1021254725842 [DOI] [PubMed] [Google Scholar]
- 161. Li H, Liu Y, Luo D, Ma Y, Zhang J, Li M, et al. Ginger for Health Care: An Overview of Systematic Reviews. Complement Ther Med (2019) 45:114–23. doi: 10.1016/j.ctim.2019.06.002 [DOI] [PubMed] [Google Scholar]
- 162. Jolad SD, Lantz RC, Solyom AM, Chen GJ, Bates RB, Timmermann BN. Fresh Organically Grown Ginger (Zingiber Officinale), Composition and Effects on LPS-Induced PGE2 Production. Phytochemistry (2004) 65(13):1937–54. doi: 10.1016/j.phytochem.2004.06.008 [DOI] [PubMed] [Google Scholar]
- 163. Rondanelli M, Fossari F, Vecchio V, Gasparri C, Peroni G, Spadaccini D, et al. Clinical Trials on Pain Lowering Effect of Ginger, A Narrative Review. Phytother Res (2020) 34(11):2843–56. doi: 10.1002/ptr.6730 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164. Tripathi S, Maier KG, Bruch D, Kittur DS. Effect of 6-Gingerol on Pro-Inflammatory Cytokine Production and Costimulatory Molecule Expression in Murine Peritoneal Macrophages. J Surg Res (2007) 138(2):209–13. doi: 10.1016/j.jss.2006.07.051 [DOI] [PubMed] [Google Scholar]
- 165. Aryaeian N, Shahram F, Mahmoudi M, Tavakoli H, Yousefi B, Arablou T, et al. The Effect of Ginger Supplementation on Some Immunity and Inflammation Intermediate Genes Expression in Patients With Active Rheumatoid Arthritis. Gene (2019) 698:179–85. doi: 10.1016/j.gene.2019.01.048 [DOI] [PubMed] [Google Scholar]
- 166. Cifci A, Tayman C, Yakut HI, Halil H, Cakir E, Cakir U, et al. Ginger (Zingiber Officinale) Prevents Severe Damage to the Lungs Due to Hyperoxia and Inflammation. Turk J Med Sci (2018) 48(4):892–900. doi: 10.3906/sag-1803-223 [DOI] [PubMed] [Google Scholar]
- 167. Hewlings SJ, Kalman DS. Curcumin, A Review of Its Effects on Human Health. Foods (2017) 6(10):92. doi: 10.3390/foods6100092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168. Kocaadam B, Sanlier N. Curcumin, an Active Component of Turmeric (Curcuma Longa), and Its Effects on Health. Crit Rev Food Sci Nutr (2017) 57(13):2889–95. doi: 10.1080/10408398.2015.1077195 [DOI] [PubMed] [Google Scholar]
- 169. Gupta SC, Sung B, Kim JH, Prasad S, Li S, Aggarwal BB. Multitargeting by Turmeric, the Golden Spice, From Kitchen to Clinic. Mol Nutr Food Res (2013) 57(9):1510–28. doi: 10.1002/mnfr.201100741 [DOI] [PubMed] [Google Scholar]
- 170. Nair A, Amalraj A, Jacob J, Kunnumakkara AB, Gopi S. Non-Curcuminoids From Turmeric and Their Potential in Cancer Therapy and Anticancer Drug Delivery Formulations. Biomolecules (2019) 9(1):13. doi: 10.3390/biom9010013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171. Yeung KS, Gubili J, Mao JJ. Herb-Drug Interactions in Cancer Care. Oncol (Williston Park) (2018) 32(10):516–20. [PubMed] [Google Scholar]
- 172. Devassy JG, Nwachukwu ID, Jones PJ. Curcumin and Cancer, Barriers to Obtaining a Health Claim. Nutr Rev (2015) 73(3):155–65. doi: 10.1093/nutrit/nuu064 [DOI] [PubMed] [Google Scholar]
- 173. He Y, Yue Y, Zheng X, Zhang K, Chen S, Du Z. Curcumin, Inflammation, and Chronic Diseases, How Are They Linked? Molecules (2015) 20(5):9183–213. doi: 10.3390/molecules20059183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174. Catanzaro M, Corsini E, Rosini M, Racchi M, Lanni C. Immunomodulators Inspired by Nature, A Review on Curcumin and Echinacea. Molecules (2018) 23(11):2778. doi: 10.3390/molecules23112778 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175. Srivastava RM, Singh S, Dubey SK, Misra K, Khar A. Immunomodulatory and Therapeutic Activity of Curcumin. Int Immunopharmacol (2011) 11(3):331–41. doi: 10.1016/j.intimp.2010.08.014 [DOI] [PubMed] [Google Scholar]
- 176. Zhang H, Penninger JM, Li Y, Zhong N, Slutsky AS. Angiotensin-Converting Enzyme 2 (ACE2) as a SARS-CoV-2 Receptor, Molecular Mechanisms and Potential Therapeutic Target. Intensive Care Med (2020) 46(4):586–90. doi: 10.1007/s00134-020-05985-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177. Pang XF, Zhang LH, Bai F, Wang NP, Garner RE, McKallip RJ, et al. Attenuation of Myocardial Fibrosis With Curcumin Is Mediated by Modulating Expression of Angiotensin II AT1/AT2 Receptors and ACE2 in Rats. Drug Des Devel Ther (2015) 9:6043–54. doi: 10.2147/DDDT.S95333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178. Jia HP, Look DC, Shi L, Hickey M, Pewe L, Netland J, et al. ACE2 Receptor Expression and Severe Acute Respiratory Syndrome Coronavirus Infection Depend on Differentiation of Human Airway Epithelia. J Virol (2005) 79(23):14614–21. doi: 10.1128/JVI.79.23.14614-14621.2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179. De Greef D, Barton EM, Sandberg EN, Croley CR, Pumarol J, Wong TL, et al. Anticancer Potential of Garlic and Its Bioactive Constituents, A Systematic and Comprehensive Review. Semin Cancer Biol (2021) 73:219–64. doi: 10.1016/j.semcancer.2020.11.020 [DOI] [PubMed] [Google Scholar]
- 180. El-Saber Batiha G, Magdy Beshbishy A, Wasef LG, Elewa YHA, Al-Sagan AA, Abd El-Hack ME, et al. Chemical Constituents and Pharmacological Activities of Garlic (Allium Sativum L.), A Review. Nutrients (2020) 12(3):872. doi: 10.3390/nu12030872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181. Percival SS. Aged Garlic Extract Modifies Human Immunity. J Nutr (2016) 146(2):433S–6S. doi: 10.3945/jn.115.210427 [DOI] [PubMed] [Google Scholar]
- 182. Yagdi E, Cerella C, Dicato M, Diederich M. Garlic-Derived Natural Polysulfanes as Hydrogen Sulfide Donors, Friend or Foe? Food Chem Toxicol (2016) 95:219–33. doi: 10.1016/j.fct.2016.07.016 [DOI] [PubMed] [Google Scholar]
- 183. Youness RA, Gad AZ, Sanber K, Ahn YJ, Lee GJ, Khallaf E, et al. Targeting Hydrogen Sulphide Signaling in Breast Cancer. J Adv Res (2021) 27:177–90. doi: 10.1016/j.jare.2020.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184. Youness RA, Assal RA, Abdel Motaal A, Gad MZ. A Novel Role of sONE/NOS3/NO Signaling Cascade in Mediating Hydrogen Sulphide Bilateral Effects on Triple Negative Breast Cancer Progression. Nitric Oxide (2018) 80:12–23. doi: 10.1016/j.niox.2018.07.004 [DOI] [PubMed] [Google Scholar]
- 185. Hsieh CC, Peng WH, Tseng HH, Liang SY, Chen LJ, Tsai JC. The Protective Role of Garlic on Allergen-Induced Airway Inflammation in Mice. Am J Chin Med (2019) 47(5):1099–112. doi: 10.1142/S0192415X19500563 [DOI] [PubMed] [Google Scholar]
- 186. Escribano BM, Luque E, Aguilar-Luque M, Feijoo M, Caballero-Villarraso J, Torres LA, et al. Dose-Dependent S-Allyl Cysteine Ameliorates Multiple Sclerosis Disease-Related Pathology by Reducing Oxidative Stress and Biomarkers of Dysbiosis in Experimental Autoimmune Encephalomyelitis. Eur J Pharmacol (2017) 815:266–73. doi: 10.1016/j.ejphar.2017.09.025 [DOI] [PubMed] [Google Scholar]
- 187. Liu X, Wang XJ. Potential Inhibitors Against 2019-Ncov Coronavirus M Protease From Clinically Approved Medicines. J Genet Genomics (2020) 47(2):119–21. doi: 10.1016/j.jgg.2020.02.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188. Ha AW, Ying T, Kim WK. The Effects of Black Garlic (Allium Satvium) Extracts on Lipid Metabolism in Rats Fed a High Fat Diet. Nutr Res Pract (2015) 9(1):30–6. doi: 10.4162/nrp.2015.9.1.30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 189. Zou XG, Li J, Sun PL, Fan YW, Yang JY, Deng ZY. Orbitides Isolated From Flaxseed Induce Apoptosis Against SGC-7901 Adenocarcinoma Cells. Int J Food Sci Nutr (2020) 71(8):929–39. doi: 10.1080/09637486.2020.1750573 [DOI] [PubMed] [Google Scholar]
- 190. Buckner AL, Buckner CA, Montaut S, Lafrenie RM. Treatment With Flaxseed Oil Induces Apoptosis in Cultured Malignant Cells. Heliyon (2019) 5(8):e02251. doi: 10.1016/j.heliyon.2019.e02251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 191. Ezzat SM, Shouman SA, Elkhoely A, Attia YM, Elsesy MS, El Senousy AS, et al. Anticancer Potentiality of Lignan Rich Fraction of Six Flaxseed Cultivars. Sci Rep (2018) 8(1):544. doi: 10.1038/s41598-017-18944-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192. Jones GJB, Roper RL. The Effects of Diets Enriched in Omega-3 Polyunsaturated Fatty Acids on Systemic Vaccinia Virus Infection. Sci Rep (2017) 7(1):15999. doi: 10.1038/s41598-017-16098-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 193. Garcia de Acilu M, Leal S, Caralt B, Roca O, Sabater J, Masclans JR. The Role of Omega-3 Polyunsaturated Fatty Acids in the Treatment of Patients With Acute Respiratory Distress Syndrome, A Clinical Review. BioMed Res Int (2015) 2015:653750. doi: 10.1155/2015/653750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194. Sharma S, Chhibber S, Mohan H, Sharma S. Dietary Supplementation With Omega-3 Polyunsaturated Fatty Acids Ameliorates Acute Pneumonia Induced by Klebsiella Pneumoniae in BALB/c Mice. Can J Microbiol (2013) 59(7):503–10. doi: 10.1139/cjm-2012-0521 [DOI] [PubMed] [Google Scholar]
- 195. Singh B, Singh JP, Kaur A, Singh N. Phenolic Composition, Antioxidant Potential and Health Benefits of Citrus Peel. Food Res Int (2020) 132:109114. doi: 10.1016/j.foodres.2020.109114 [DOI] [PubMed] [Google Scholar]
- 196. Nogata Y, Sakamoto K, Shiratsuchi H, Ishii T, Yano M, Ohta H. Flavonoid Composition of Fruit Tissues of Citrus Species. Biosci Biotechnol Biochem (2006) 70(1):178–92. doi: 10.1271/bbb.70.178 [DOI] [PubMed] [Google Scholar]
- 197. Bellavite P, Donzelli A. Hesperidin and SARS-CoV-2, New Light on the Healthy Function of Citrus Fruits. Antioxidants (Basel) (2020) 9(8):742. doi: 10.3390/antiox9080742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198. Nurhayati IP, Khumaira A, Ilmawati GPN, Meiyanto E, Hermawan A. Cytotoxic and Antimetastatic Activity of Hesperetin and Doxorubicin Combination Toward Her2 Expressing Breast Cancer Cells. Asian Pac J Cancer Prev (2020) 21(5):1259–67. doi: 10.31557/APJCP.2020.21.5.1259 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199. ElKhouly AM, Youness RA, Gad MZ. MicroRNA-486-5p and microRNA-486-3p, Multifaceted Pleiotropic Mediators in Oncological and Non-Oncological Conditions. Noncoding RNA Res (2020) 5(1):11–21. doi: 10.1016/j.ncrna.2020.01.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 200. Palit S, Kar S, Sharma G, Das PK. Hesperetin Induces Apoptosis in Breast Carcinoma by Triggering Accumulation of ROS and Activation of ASK1/JNK Pathway. J Cell Physiol (2015) 230(8):1729–39. doi: 10.1002/jcp.24818 [DOI] [PubMed] [Google Scholar]
- 201. Khan A, Ikram M, Hahm JR, Kim MO. Antioxidant and Anti-Inflammatory Effects of Citrus Flavonoid Hesperetin, Special Focus on Neurological Disorders. Antioxidants (Basel) (2020) 9(7):609. doi: 10.3390/antiox9070609 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 202. Ahmad S, Alam K, Hossain MM, Fatima M, Firdaus F, Zafeer MF, et al. Anti-Arthritogenic and Cardioprotective Action of Hesperidin and Daidzein in Collagen-Induced Rheumatoid Arthritis. Mol Cell Biochem (2016) 423(1-2):115–27. doi: 10.1007/s11010-016-2830-y [DOI] [PubMed] [Google Scholar]
- 203. Wu J. Tackle the Free Radicals Damage in COVID-19. Nitric Oxide (2020) 102:39–41. doi: 10.1016/j.niox.2020.06.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 204. Park HK, Kang SW, Park MS. Hesperidin Ameliorates Hepatic Ischemia-Reperfusion Injury in Sprague-Dawley Rats. Transplant Proc (2019) 51(8):2828–32. doi: 10.1016/j.transproceed.2019.02.059 [DOI] [PubMed] [Google Scholar]
- 205. Haggag YA, El-Ashmawy NE, Okasha KM. Is Hesperidin Essential for Prophylaxis and Treatment of COVID-19 Infection? Med Hypotheses (2020) 144:109957. doi: 10.1016/j.mehy.2020.109957 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 206. Kim H, Jang M, Kim Y, Choi J, Jeon J, Kim J, et al. Red Ginseng and Vitamin C Increase Immune Cell Activity and Decrease Lung Inflammation Induced by Influenza A Virus/H1N1 Infection. J Pharm Pharmacol (2016) 68(3):406–20. doi: 10.1111/jphp.12529 [DOI] [PubMed] [Google Scholar]
- 207. Kim Y, Kim H, Bae S, Choi J, Lim SY, Lee N, et al. Vitamin C Is an Essential Factor on the Anti-Viral Immune Responses Through the Production of Interferon-Alpha/Beta at the Initial Stage of Influenza A Virus (H3N2) Infection. Immune Netw (2013) 13(2):70–4. doi: 10.4110/in.2013.13.2.70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 208. Sharma M, Anderson SA, Schoop R, Hudson JB. Induction of Multiple Pro-Inflammatory Cytokines by Respiratory Viruses and Reversal by Standardized Echinacea, a Potent Antiviral Herbal Extract. Antiviral Res (2009) 83(2):165–70. doi: 10.1016/j.antiviral.2009.04.009 [DOI] [PubMed] [Google Scholar]
- 209. Barnes J, Anderson LA, Gibbons S, Phillipson JD. Echinacea Species (Echinacea Angustifolia (DC.) Hell., Echinacea Pallida (Nutt.) Nutt., Echinacea Purpurea (L.) Moench), a Review of Their Chemistry, Pharmacology and Clinical Properties. J Pharm Pharmacol (2005) 57(8):929–54. doi: 10.1211/0022357056127 [DOI] [PubMed] [Google Scholar]
- 210. Aucoin M, Cooley K, Saunders PR, Care J, Anheyer D, Medina DN, et al. The Effect of Echinacea Spp. On the Prevention or Treatment of COVID-19 and Other Respiratory Tract Infections in Humans, A Rapid Review. Adv Integr Med (2020) 7(4):203–17. doi: 10.1016/j.aimed.2020.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 211. Melchart D, Linde K, Worku F, Bauer R, Wagner H. Immunomodulation With Echinacea - a Systematic Review of Controlled Clinical Trials. Phytomedicine (1994) 1(3):245–54. doi: 10.1016/S0944-7113(11)80072-3 [DOI] [PubMed] [Google Scholar]
- 212. Sharifi-Rad M, Mnayer D, Morais-Braga MFB, Carneiro JNP, Bezerra CF, Coutinho HDM, et al. Echinacea Plants as Antioxidant and Antibacterial Agents, From Traditional Medicine to Biotechnological Applications. Phytother Res (2018) 32(9):1653–63. doi: 10.1002/ptr.6101 [DOI] [PubMed] [Google Scholar]
- 213. Tsai YL, Chiu CC, Yi-Fu Chen J, Chan KC, Lin SD. Cytotoxic Effects of Echinacea Purpurea Flower Extracts and Cichoric Acid on Human Colon Cancer Cells Through Induction of Apoptosis. J Ethnopharmacol (2012) 143(3):914–9. doi: 10.1016/j.jep.2012.08.032 [DOI] [PubMed] [Google Scholar]
- 214. Chicca A, Adinolfi B, Martinotti E, Fogli S, Breschi MC, Pellati F, et al. Cytotoxic Effects of Echinacea Root Hexanic Extracts on Human Cancer Cell Lines. J Ethnopharmacol (2007) 110(1):148–53. doi: 10.1016/j.jep.2006.09.013 [DOI] [PubMed] [Google Scholar]
- 215. Chaves F, Chacon M, Badilla B, Arevalo C. Effect of Echinacea Purpurea (Asteraceae) Aqueous Extract on Antibody Response to Bothrops Asper Venom and Immune Cell Response. Rev Biol Trop (2007) 55(1):113–9. doi: 10.15517/rbt.v55i1.6061 [DOI] [PubMed] [Google Scholar]
- 216. Zhai Z, Liu Y, Wu L, Senchina DS, Wurtele ES, Murphy PA, et al. Enhancement of Innate and Adaptive Immune Functions by Multiple Echinacea Species. J Med Food (2007) 10(3):423–34. doi: 10.1089/jmf.2006.257 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 217. Sadigh-Eteghad S, Khayat-Nuri H, Abadi N, Ghavami S, Golabi M, Shanebandi D. Synergetic Effects of Oral Administration of Levamisole and Echinacea Purpurea on Immune Response in Wistar Rat. Res Vet Sci (2011) 91(1):82–5. doi: 10.1016/j.rvsc.2010.07.027 [DOI] [PubMed] [Google Scholar]
- 218. Park S, Lee MS, Jung S, Lee S, Kwon O, Kreuter MH, et al. Echinacea Purpurea Protects Against Restraint Stress-Induced Immunosuppression in BALB/c Mice. J Med Food (2018) 21(3):261–8. doi: 10.1089/jmf.2017.4073 [DOI] [PubMed] [Google Scholar]
- 219. Yu D, Yuan Y, Jiang L, Tai Y, Yang X, Hu F, et al. Anti-Inflammatory Effects of Essential Oil in Echinacea Purpurea L. Pak J Pharm Sci (2013) 26(2):403–8. [PubMed] [Google Scholar]
- 220. Nagoor Meeran MF, Javed H, Sharma C, Goyal SN, Kumar S, Jha NK, et al. Can Echinacea be a Potential Candidate to Target Immunity, Inflammation, and Infection - The Trinity of Coronavirus Disease 2019. Heliyon (2021) 7(2):e05990. doi: 10.1016/j.heliyon.2021.e05990 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 221. Allegra A, Di Gioacchino M, Tonacci A, Musolino C, Gangemi S. Immunopathology of SARS-CoV-2 Infection, Immune Cells and Mediators, Prognostic Factors, and Immune-Therapeutic Implications. Int J Mol Sci (2020) 21(13):4782. doi: 10.3390/ijms21134782 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 222. Turner RB, Bauer R, Woelkart K, Hulsey TC, Gangemi JD. An Evaluation of Echinacea Angustifolia in Experimental Rhinovirus Infections. N Engl J Med (2005) 353(4):341–8. doi: 10.1056/NEJMoa044441 [DOI] [PubMed] [Google Scholar]
- 223. Pleschka S, Stein M, Schoop R, Hudson JB. Anti-Viral Properties and Mode of Action of Standardized Echinacea Purpurea Extract Against Highly Pathogenic Avian Influenza Virus (H5N1, H7N7) and Swine-Origin H1N1 (S-OIV). Virol J (2009) 6:197. doi: 10.1186/1743-422X-6-197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 224. Signer J, Jonsdottir HR, Albrich WC, Strasser M, Zust R, Ryter S, et al. In Vitro Virucidal Activity of Echinaforce(R), an Echinacea Purpurea Preparation, Against Coronaviruses, Including Common Cold Coronavirus 229E and SARS-CoV-2. Virol J (2020) 17(1):136. doi: 10.1186/s12985-020-01401-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 225. Hudson JB. Applications of the Phytomedicine Echinacea Purpurea (Purple Coneflower) in Infectious Diseases. J BioMed Biotechnol (2012) 2012:769896. doi: 10.1155/2012/769896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 226. Kim MB, Kim C, Song Y, Hwang JK. Antihyperglycemic and Anti-Inflammatory Effects of Standardized Curcuma Xanthorrhiza Roxb. Extract and Its Active Compound Xanthorrhizol in High-Fat Diet-Induced Obese Mice. Evid Based Complement Alternat Med (2014) 2014:205915. doi: 10.1155/2014/205915 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 227. Oon SF, Nallappan M, Tee TT, Shohaimi S, Kassim NK, Sa’ariwijaya MS, et al. Xanthorrhizol, a Review of Its Pharmacological Activities and Anticancer Properties. Cancer Cell Int (2015) 15:100. doi: 10.1186/s12935-015-0255-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 228. Shimizu K, Funamoto M, Sunagawa Y, Shimizu S, Katanasaka Y, Miyazaki Y, et al. Anti-Inflammatory Action of Curcumin and Its Use in the Treatment of Lifestyle-Related Diseases. Eur Cardiol (2019) 14(2):117–22. doi: 10.15420/ecr.2019.17.2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 229. Singgih Wahono C, Diah Setyorini C, Kalim H, Nurdiana N, Handono K. Effect of Curcuma Xanthorrhiza Supplementation on Systemic Lupus Erythematosus Patients With Hypovitamin D Which Were Given Vitamin D3 Towards Disease Activity (SLEDAI), IL-6, and TGF-Beta1 Serum. Int J Rheumatol (2017) 2017:7687053. doi: 10.1155/2017/7687053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 230. Maldonado C, Barnes CJ, Cornett C, Holmfred E, Hansen SH, Persson C, et al. Phylogeny Predicts the Quantity of Antimalarial Alkaloids Within the Iconic Yellow Cinchona Bark (Rubiaceae, Cinchona Calisaya). Front Plant Sci (2017) 8:391. doi: 10.3389/fpls.2017.00391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 231. Abolghasemi E, Moosa-Kazemi SH, Davoudi M, Reisi A, Satvat MT. Comparative Study of Chloroquine and Quinine on Malaria Rodents and Their Effects on the Mouse Testis. Asian Pac J Trop BioMed (2012) 2(4):311–4. doi: 10.1016/S2221-1691(12)60030-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 232. D’Alessandro S, Scaccabarozzi D, Signorini L, Perego F, Ilboudo DP, Ferrante P, et al. The Use of Antimalarial Drugs Against Viral Infection. Microorganisms (2020) 8(1):85. doi: 10.3390/microorganisms8010085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 233. Vincent MJ, Bergeron E, Benjannet S, Erickson BR, Rollin PE, Ksiazek TG, et al. Chloroquine Is a Potent Inhibitor of SARS Coronavirus Infection and Spread. Virol J (2005) 2:69. doi: 10.1186/1743-422X-2-69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 234. Handayani T, Sakinah S, Nallappan M, Pihie AH, et al. Regulation of P53-, Bcl-2- and Caspase-Dependent Signaling Pathway in Xanthorrhizol-Induced Apoptosis of HepG2 Hepatoma Cells. Anticancer Res (2007) 27(2):965–71. [PubMed] [Google Scholar]
- 235. Ismail N, Pihie AH, Nallapan M. Xanthorrhizol Induces Apoptosis via the Up-Regulation of Bax and P53 in HeLa Cells. Anticancer Res (2005) 25(3B):2221–7. [PubMed] [Google Scholar]
- 236. Cheah YH, Azimahtol HL, Abdullah NR. Xanthorrhizol Exhibits Antiproliferative Activity on MCF-7 Breast Cancer Cells via Apoptosis Induction. Anticancer Res (2006) 26(6B):4527–34. [PubMed] [Google Scholar]
- 237. Kang YJ, Park KK, Chung WY, Hwang JK, Lee SK. Xanthorrhizol, a Natural Sesquiterpenoid, Induces Apoptosis and Growth Arrest in HCT116 Human Colon Cancer Cells. J Pharmacol Sci (2009) 111(3):276–84. doi: 10.1254/jphs.09141FP [DOI] [PubMed] [Google Scholar]
- 238. Kim JY, An JM, Chung WY, Park KK, Hwang JK, Kim DS, et al. Xanthorrhizol Induces Apoptosis Through ROS-Mediated MAPK Activation in Human Oral Squamous Cell Carcinoma Cells and Inhibits DMBA-Induced Oral Carcinogenesis in Hamsters. Phytother Res (2013) 27(4):493–8. doi: 10.1002/ptr.4746 [DOI] [PubMed] [Google Scholar]
- 239. Galen EV, Kroes B. Assessment Report on Curcuma Xanthorrhiza Roxb.(C. Xanthorrhiza D. Dietrich), Rhizoma. Eur Medicines Agency (2014) 44(2). [Google Scholar]
- 240. Lim CS, Jin DQ, Mok H, Oh SJ, Lee JU, Hwang JK, et al. Antioxidant and Antiinflammatory Activities of Xanthorrhizol in Hippocampal Neurons and Primary Cultured Microglia. J Neurosci Res (2005) 82(6):831–8. doi: 10.1002/jnr.20692 [DOI] [PubMed] [Google Scholar]
- 241. Kim M, Cho H, Ahn DG, Jung HG, Seo HY, Kim JS, et al. In Vitro Replication Inhibitory Activity of Xanthorrhizol Against Severe Acute Respiratory Syndrome Coronavirus 2. Biomedicines (2021) 9(11):1725. doi: 10.3390/biomedicines9111725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 242. Saggam A, Limgaokar K, Borse S, Chavan-Gautam P, Dixit S, Tillu G, et al. Withania Somnifera (L.) Dunal, Opportunity for Clinical Repurposing in COVID-19 Management. Front Pharmacol (2021) 12:623795. doi: 10.3389/fphar.2021.623795 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 243. Mishra LC, Singh BB, Dagenais S. Scientific Basis for the Therapeutic Use of Withania Somnifera (Ashwagandha), a Review. Altern Med Rev (2000) 5(4):334–46. [PubMed] [Google Scholar]
- 244. Minhas U, Minz R, Bhatnagar A. Prophylactic Effect of Withania Somnifera on Inflammation in a Non-Autoimmune Prone Murine Model of Lupus. Drug Discov Ther (2011) 5(4):195–201. doi: 10.5582/ddt.2011.v5.4.195 [DOI] [PubMed] [Google Scholar]
- 245. Teixeira ST, Valadares MC, Goncalves SA, de Melo A, Queiroz ML. Prophylactic Administration of Withania Somnifera Extract Increases Host Resistance in Listeria Monocytogenes Infected Mice. Int Immunopharmacol (2006) 6(10):1535–42. doi: 10.1016/j.intimp.2006.03.016 [DOI] [PubMed] [Google Scholar]
- 246. Kalra R, Kaushik N. Withania Somnifera (Linn.) Dunal, a Review of Chemical and Pharmacological Diversity. Phytochem Rev (2017) 16(5):953–87. doi: 10.1007/s11101-017-9504-6 [DOI] [Google Scholar]
- 247. Antony ML, Lee J, Hahm ER, Kim SH, Marcus AI, Kumari V, et al. Growth Arrest by the Antitumor Steroidal Lactone Withaferin A in Human Breast Cancer Cells Is Associated With Down-Regulation and Covalent Binding at Cysteine 303 of Beta-Tubulin. J Biol Chem (2014) 289(3):1852–65. doi: 10.1074/jbc.M113.496844 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 248. Yang H, Shi G, Dou QP. The Tumor Proteasome Is a Primary Target for the Natural Anticancer Compound Withaferin A Isolated From “Indian Winter Cherry”. Mol Pharmacol (2007) 71(2):426–37. doi: 10.1124/mol.106.030015 [DOI] [PubMed] [Google Scholar]
- 249. Yu Y, Hamza A, Zhang T, Gu M, Zou P, Newman B, et al. Withaferin A Targets Heat Shock Protein 90 in Pancreatic Cancer Cells. Biochem Pharmacol (2010) 79(4):542–51. doi: 10.1016/j.bcp.2009.09.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 250. Koduru S, Kumar R, Srinivasan S, Evers MB, Damodaran C. Notch-1 Inhibition by Withaferin-A, a Therapeutic Target Against Colon Carcinogenesis. Mol Cancer Ther (2010) 9(1):202–10. doi: 10.1158/1535-7163.MCT-09-0771 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 251. Widodo N, Priyandoko D, Shah N, Wadhwa R, Kaul SC. Selective Killing of Cancer Cells by Ashwagandha Leaf Extract and Its Component Withanone Involves ROS Signaling. PloS One (2010) 5(10):e13536. doi: 10.1371/journal.pone.0013536 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 252. Widodo N, Takagi Y, Shrestha BG, Ishii T, Kaul SC, Wadhwa R. Selective Killing of Cancer Cells by Leaf Extract of Ashwagandha, Components, Activity and Pathway Analyses. Cancer Lett (2008) 262(1):37–47. doi: 10.1016/j.canlet.2007.11.037 [DOI] [PubMed] [Google Scholar]
- 253. Christina AJ, Joseph DG, Packialakshmi M, Kothai R, Robert SJ, Chidambaranathan N, et al. Anticarcinogenic Activity of Withania Somnifera Dunal Against Dalton’s Ascitic Lymphoma. J Ethnopharmacol (2004) 93(2-3):359–61. doi: 10.1016/j.jep.2004.04.004 [DOI] [PubMed] [Google Scholar]
- 254. Khan B, Ahmad SF, Bani S, Kaul A, Suri KA, Satti NK, et al. Augmentation and Proliferation of T Lymphocytes and Th-1 Cytokines by Withania Somnifera in Stressed Mice. Int Immunopharmacol (2006) 6(9):1394–403. doi: 10.1016/j.intimp.2006.04.001 [DOI] [PubMed] [Google Scholar]
- 255. Malik F, Singh J, Khajuria A, Suri KA, Satti NK, Singh S, et al. A Standardized Root Extract of Withania Somnifera and Its Major Constituent Withanolide-A Elicit Humoral and Cell-Mediated Immune Responses by Up Regulation of Th1-Dominant Polarization in BALB/c Mice. Life Sci (2007) 80(16):1525–38. doi: 10.1016/j.lfs.2007.01.029 [DOI] [PubMed] [Google Scholar]
- 256. Kour K, Pandey A, Suri KA, Satti NK, Gupta KK, Bani S. Restoration of Stress-Induced Altered T Cell Function and Corresponding Cytokines Patterns by Withanolide A. Int Immunopharmacol (2009) 9(10):1137–44. doi: 10.1016/j.intimp.2009.05.011 [DOI] [PubMed] [Google Scholar]
- 257. Khan S, Malik F, Suri KA, Singh J. Molecular Insight Into the Immune Up-Regulatory Properties of the Leaf Extract of Ashwagandha and Identification of Th1 Immunostimulatory Chemical Entity. Vaccine (2009) 27(43):6080–7. doi: 10.1016/j.vaccine.2009.07.011 [DOI] [PubMed] [Google Scholar]
- 258. Zhao H, Gao Z, Xie S, Han X, Sun Q. Withaferin A Attenuates Ovalbumin Induced Airway Inflammation. injury (2019) 5:6. doi: 10.2741/4737 [DOI] [PubMed] [Google Scholar]
- 259. Davis L, Kuttan G. Immunomodulatory Activity of Withania Somnifera. J Ethnopharmacol (2000) 71(1–2):193–200. doi: 10.1016/S0378-8741(99)00206-8 [DOI] [PubMed] [Google Scholar]
- 260. Agarwal R, Diwanay S, Patki P, Patwardhan B. Studies on Immunomodulatory Activity of Withania Somnifera (Ashwagandha) Extracts in Experimental Immune Inflammation. J Ethnopharmacol (1999) 67(1):27–35. doi: 10.1016/S0378-8741(99)00065-3 [DOI] [PubMed] [Google Scholar]
- 261. Latheef SK, Dhama K, Samad HA, Wani MY, Kumar MA, Palanivelu M, et al. Immunomodulatory and Prophylactic Efficacy of Herbal Extracts Against Experimentally Induced Chicken Infectious Anaemia in Chicks, Assessing the Viral Load and Cell Mediated Immunity. Virusdisease (2017) 28(1):115–20. doi: 10.1007/s13337-016-0355-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 262. Davis L, Kuttan G. Effect of Withania Somnifera on Cell Mediated Immune Responses in Mice. J Exp Clin Cancer Res (2002) 21(4):585–90. [PubMed] [Google Scholar]
- 263. Mikolai J, Erlandsen A, Murison A, Brown KA, Gregory WL, Raman-Caplan P, Zwickey HL, et al. In Vivo Effects of Ashwagandha (Withania Somnifera) Extract on the Activation of Lymphocytes. J Altern Complement Med (2009) 15(4):423–30. doi: 10.1089/acm.2008.0215 [DOI] [PubMed] [Google Scholar]
- 264. Balkrishna A, Pokhrel S, Singh H, Joshi M, Mulay VP, Haldar S, et al. Withanone From Withania Somnifera Attenuates SARS-CoV-2 RBD and Host ACE2 Interactions to Rescue Spike Protein Induced Pathologies in Humanized Zebrafish Model. Drug Design Dev Ther (2021) 15:1111. doi: 10.2147/DDDT.S292805 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 265. Sharma S, Deep S. In-Silico Drug Repurposing for Targeting SARS-CoV-2 Main Protease (Mpro). J Biomolecular Struct Dynam (2020) p:1–8. doi: 10.26434/chemrxiv.12210845 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 266. Borse S, Joshi M, Saggam A, Bhat V, Walia S, Marathe A, et al. Ayurveda Botanicals in COVID-19 Management, An in Silico Multi-Target Approach. PloS One (2021) 16(6):e0248479. doi: 10.1371/journal.pone.0248479 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 267. Chacko SM, Thambi PT, Kuttan R, Nishigaki I. Beneficial Effects of Green Tea, a Literature Review. Chin Med (2010) 5:13. doi: 10.1186/1749-8546-5-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 268. Cabrera C, Artacho R, Gimenez R. Beneficial Effects of Green Tea–a Review. J Am Coll Nutr (2006) 25(2):79–99. doi: 10.1080/07315724.2006.10719518 [DOI] [PubMed] [Google Scholar]
- 269. Khan N, Mukhtar H. Tea Polyphenols in Promotion of Human Health. Nutrients (2018) 11(1):39. doi: 10.3390/nu11010039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 270. Mhatre S, Srivastava T, Naik S, Patravale V. Antiviral Activity of Green Tea and Black Tea Polyphenols in Prophylaxis and Treatment of COVID-19, A Review. Phytomedicine (2021) 85:153286. doi: 10.1016/j.phymed.2020.153286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 271. Higdon JV, Frei B. Tea Catechins and Polyphenols, Health Effects, Metabolism, and Antioxidant Functions. Crit Rev Food Sci Nutr (2003) 43(1):89–143. doi: 10.1080/10408690390826464 [DOI] [PubMed] [Google Scholar]
- 272. Lambert JD, Yang CS. Mechanisms of Cancer Prevention by Tea Constituents. J Nutr (2003) 133(10):3262S–7S. doi: 10.1093/jn/133.10.3262S [DOI] [PubMed] [Google Scholar]
- 273. Yang CS, Landau JM. Effects of Tea Consumption on Nutrition and Health. J Nutr (2000) 130(10):2409–12. doi: 10.1093/jn/130.10.2409 [DOI] [PubMed] [Google Scholar]
- 274. O’Neill EJ, Termini D, Albano A, Tsiani E. Anti-Cancer Properties of Theaflavins. Molecules (2021) 26(4):987. doi: 10.3390/molecules26040987 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 275. Kaur S, Greaves P, Cooke DN, Edwards R, Steward WP, Gescher AJ, et al. Breast Cancer Prevention by Green Tea Catechins and Black Tea Theaflavins in the C3(1) SV40 T,t Antigen Transgenic Mouse Model Is Accompanied by Increased Apoptosis and a Decrease in Oxidative DNA Adducts. J Agric Food Chem (2007) 55(9):3378–85. doi: 10.1021/jf0633342 [DOI] [PubMed] [Google Scholar]
- 276. Ren F, Zhang S, Mitchell SH, Butler R, Young CY. Tea Polyphenols Down-Regulate the Expression of the Androgen Receptor in LNCaP Prostate Cancer Cells. Oncogene (2000) 19(15):1924–32. doi: 10.1038/sj.onc.1203511 [DOI] [PubMed] [Google Scholar]
- 277. Lee HH, Ho CT, Lin JK. Theaflavin-3,3’-Digallate and Penta-O-Galloyl-Beta-D-Glucose Inhibit Rat Liver Microsomal 5alpha-Reductase Activity and the Expression of Androgen Receptor in LNCaP Prostate Cancer Cells. Carcinogenesis (2004) 25(7):1109–18. doi: 10.1093/carcin/bgh106 [DOI] [PubMed] [Google Scholar]
- 278. Chowdhury P, Barooah AK. Tea Bioactive Modulate Innate Immunity, In Perception to COVID-19 Pandemic. Front Immunol (2020) 11:590716. doi: 10.3389/fimmu.2020.590716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 279. Song YA, Park YL, Yoon SH, Kim KY, Cho SB, Lee WS, et al. Black Tea Polyphenol Theaflavin Suppresses LPS-Induced ICAM-1 and VCAM-1 Expression via Blockage of NF-kappaB and JNK Activation in Intestinal Epithelial Cells. Inflammation Res (2011) 60(5):493–500. doi: 10.1007/s00011-010-0296-z [DOI] [PubMed] [Google Scholar]
- 280. Li J, Ye L, Wang X, Liu J, Wang Y, Zhou Y, et al. (-)-Epigallocatechin Gallate Inhibits Endotoxin-Induced Expression of Inflammatory Cytokines in Human Cerebral Microvascular Endothelial Cells. J Neuroinflamm (2012) 9:161. doi: 10.1186/1742-2094-9-161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 281. Dona M, Dell’Aica I, Calabrese F, Benelli R, Morini M, Albini A, et al. Neutrophil Restraint by Green Tea, Inhibition of Inflammation, Associated Angiogenesis, and Pulmonary Fibrosis. J Immunol (2003) 170(8):4335–41. doi: 10.4049/jimmunol.170.8.4335 [DOI] [PubMed] [Google Scholar]
- 282. Sartor L, Pezzato E, Garbisa S. (-)Epigallocatechin-3-Gallate Inhibits Leukocyte Elastase, Potential of the Phyto-Factor in Hindering Inflammation, Emphysema, and Invasion. J Leukoc Biol (2002) 71(1):73–9. [PubMed] [Google Scholar]
- 283. Lung J, Lin YS, Yang YH, Chou YL, Shu LH, Cheng YC, et al. The Potential Chemical Structure of Anti-SARS-CoV-2 RNA-Dependent RNA Polymerase. J Med Virol (2020) 92(6):693–7. doi: 10.1002/jmv.25761 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 284. Maiti S, Banerjee A. Epigallocatechin Gallate and Theaflavin Gallate Interaction in SARS-CoV-2 Spike-Protein Central Channel With Reference to the Hydroxychloroquine Interaction, Bioinformatics and Molecular Docking Study. Drug Dev Res (2021) 82(1):86–96. doi: 10.1002/ddr.21730 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 285. Zhang J-J, Shen X, Yan Y-M, Yan W, Cheng Y-X. Discovery of Anti-SARS-CoV-2 Agents From Commercially Available Flavor via Docking Screening. (2020). doi: 10.31219/osf.io/vjch2 [DOI] [Google Scholar]
- 286. Green Tea, in Drugs and Lactation Database (LactMed). Bethesda (MD) (2006). [Google Scholar]
- 287. Aparicio-Soto M, Sanchez-Hidalgo M, Alarcon-de-la-Lastra C. An Update on Diet and Nutritional Factors in Systemic Lupus Erythematosus Management. Nutr Res Rev (2017) 30(1):118–37. doi: 10.1017/S0954422417000026 [DOI] [PubMed] [Google Scholar]
- 288. Gan RY, Li HB, Sui ZQ, Corke H. Absorption, Metabolism, Anti-Cancer Effect and Molecular Targets of Epigallocatechin Gallate (EGCG), An Updated Review. Crit Rev Food Sci Nutr (2018) 58(6):924–41. doi: 10.1080/10408398.2016.1231168 [DOI] [PubMed] [Google Scholar]
- 289. Shankar S, Ganapathy S, Hingorani SR, Srivastava RK. EGCG Inhibits Growth, Invasion, Angiogenesis and Metastasis of Pancreatic Cancer. Front Biosci (2008) 13:440–52. doi: 10.2741/2691 [DOI] [PubMed] [Google Scholar]
- 290. Shankar S, Suthakar G, Srivastava RK. Epigallocatechin-3-Gallate Inhibits Cell Cycle and Induces Apoptosis in Pancreatic Cancer. Front Biosci (2007) 12:5039–51. doi: 10.2741/2446 [DOI] [PubMed] [Google Scholar]
- 291. Kaltschmidt B, Greiner JFW, Kadhim HM, Kaltschmidt C. Subunit-Specific Role of NF-KappaB in Cancer. Biomedicines (2018) 6(2):44. doi: 10.3390/biomedicines6020044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 292. Masuda M, Suzui M, Lim JT, Deguchi A, Soh JW, Weinstein IB. Epigallocatechin-3-Gallate Decreases VEGF Production in Head and Neck and Breast Carcinoma Cells by Inhibiting EGFR-Related Pathways of Signal Transduction. J Exp Ther Oncol (2002) 2(6):350–9. doi: 10.1046/j.1359-4117.2002.01062.x [DOI] [PubMed] [Google Scholar]
- 293. Fujiki H, Suganuma M, Okabe S, Sueoka N, Komori A, Sueoka E, et al. Cancer Inhibition by Green Tea. Mutat Res/Fundam Mol Mech Mutagenesis (1998) 402(1-2):307–10. doi: 10.1016/S0027-5107(97)00310-2 [DOI] [PubMed] [Google Scholar]
- 294. Shirakami Y, Shimizu M. Possible Mechanisms of Green Tea and Its Constituents Against Cancer. Molecules (2018) 23(9):2284. doi: 10.3390/molecules23092284 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 295. Shimizu M, Deguchi A, Hara Y, Moriwaki H, Weinstein IB. EGCG Inhibits Activation of the Insulin-Like Growth Factor-1 Receptor in Human Colon Cancer Cells. Biochem Biophys Res Commun (2005) 334(3):947–53. doi: 10.1016/j.bbrc.2005.06.182 [DOI] [PubMed] [Google Scholar]
- 296. Shimizu M, Shirakami Y, Sakai H, Tatebe H, Nakagawa T, Hara Y, et al. EGCG Inhibits Activation of the Insulin-Like Growth Factor (IGF)/IGF-1 Receptor Axis in Human Hepatocellular Carcinoma Cells. Cancer Lett (2008) 262(1):10–8. doi: 10.1016/j.canlet.2007.11.026 [DOI] [PubMed] [Google Scholar]
- 297. Fang M, Chen D, Yang CS. Dietary Polyphenols may Affect DNA Methylation. J Nutr (2007) 137(1 Suppl):223S–8S. doi: 10.1093/jn/137.1.223S [DOI] [PubMed] [Google Scholar]
- 298. Huang SC, Kao YH, Shih SF, Tsai MC, Lin CS, Chen LW, et al. Epigallocatechin-3-Gallate Exhibits Immunomodulatory Effects in Human Primary T Cells. Biochem Biophys Res Commun (2021) 550:70–6. doi: 10.1016/j.bbrc.2021.02.132 [DOI] [PubMed] [Google Scholar]
- 299. Wu D, Wang J, Pae M, Meydani SN. Green tea EGCG, T Cells, and T Cell-Mediated Autoimmune Diseases. Mol Aspects Med (2012) 33(1):107–18. doi: 10.1016/j.mam.2011.10.001 [DOI] [PubMed] [Google Scholar]
- 300. Byun EH, Omura T, Yamada K, Tachibana H. Green Tea Polyphenol Epigallocatechin-3-Gallate Inhibits TLR2 Signaling Induced by Peptidoglycan Through the Polyphenol Sensing Molecule 67-kDa Laminin Receptor. FEBS Lett (2011) 585(5):814–20. doi: 10.1016/j.febslet.2011.02.010 [DOI] [PubMed] [Google Scholar]
- 301. Byun EB, Choi HG, Sung NY, Byun EH. Green Tea Polyphenol Epigallocatechin-3-Gallate Inhibits TLR4 Signaling Through the 67-kDa Laminin Receptor on Lipopolysaccharide-Stimulated Dendritic Cells. Biochem Biophys Res Commun (2012) 426(4):480–5. doi: 10.1016/j.bbrc.2012.08.096 [DOI] [PubMed] [Google Scholar]
- 302. Xiaokaiti Y, Wu H, Chen Y, Yang H, Duan J, Li X, et al. EGCG Reverses Human Neutrophil Elastase-Induced Migration in A549 Cells by Directly Binding to HNE and by Regulating Alpha1-AT. Sci Rep (2015) 5:11494. doi: 10.1038/srep11494 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 303. Mekky RY, El-Ekiaby N, El Sobky SA, Elemam NM, Youness RA, El-Sayed M, et al. Epigallocatechin Gallate (EGCG) and miR-548m Reduce HCV Entry Through Repression of CD81 Receptor in HCV Cell Models. Arch Virol (2019) 164(6):1587–95. doi: 10.1007/s00705-019-04232-x [DOI] [PubMed] [Google Scholar]
- 304. Ge M, Xiao Y, Chen H, Luo F, Du G, Zeng F. Multiple Antiviral Approaches of (-)-Epigallocatechin-3-Gallate (EGCG) Against Porcine Reproductive and Respiratory Syndrome Virus Infection In Vitro. Antiviral Res (2018) 158:52–62. doi: 10.1016/j.antiviral.2018.07.012 [DOI] [PubMed] [Google Scholar]
- 305. Lu JW, Hsieh PS, Lin CC, Hu MK, Huang SM, Wang YM, et al. Synergistic Effects of Combination Treatment Using EGCG and Suramin Against the Chikungunya Virus. Biochem Biophys Res Commun (2017) 491(3):595–602. doi: 10.1016/j.bbrc.2017.07.157 [DOI] [PubMed] [Google Scholar]
- 306. Yang J, Li L, Tan S, Jin H, Qiu J, Mao Q, et al. A Natural Theaflavins Preparation Inhibits HIV-1 Infection by Targeting the Entry Step, Potential Applications for Preventing HIV-1 Infection. Fitoterapia (2012) 83(2):348–55. doi: 10.1016/j.fitote.2011.11.016 [DOI] [PubMed] [Google Scholar]
- 307. Song JM, Lee KH, Seong BL. Antiviral Effect of Catechins in Green Tea on Influenza Virus. Antiviral Res (2005) 68(2):66–74. doi: 10.1016/j.antiviral.2005.06.010 [DOI] [PubMed] [Google Scholar]
- 308. Khaerunnisa S, Kurniawan H, Awaluddin R, Suhartati S, Soetjipto S. Potential Inhibitor of COVID-19 Main Protease (Mpro) From Several Medicinal Plant Compounds by Molecular Docking Study. Preprints (2020) 2020:2020030226. doi: 10.20944/preprints202003.0226.v1 [DOI] [Google Scholar]
- 309. Ibrahim IM, Abdelmalek DH, Elfiky AA. GRP78, A Cell’s Response to Stress. Life Sci (2019) 226:156–63. doi: 10.1016/j.lfs.2019.04.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 310. Khomari F, Nabi-Afjadi M, Yarahmadi S, Eskandari H, Bahreini E. Effects of Cell Proteostasis Network on the Survival of SARS-CoV-2. Biol Proced Online (2021) 23(1):8. doi: 10.1186/s12575-021-00145-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 311. Khan M, Khan M, Khan Z, Ahamad T, Ansari W. Identification of Dietary Molecules as Therapeutic Agents to Combat COVID-19 Using Molecular Docking Studies. Res Sq (2020). doi: 10.21203/rs.3.rs-19560/v1 [DOI] [Google Scholar]
- 312. Weiss DJ, Anderton CR. Determination of Catechins in Matcha Green Tea by Micellar Electrokinetic Chromatography. J Chromatogr A (2003) 1011(1-2):173–80. doi: 10.1016/S0021-9673(03)01133-6 [DOI] [PubMed] [Google Scholar]
- 313. Kochman J, Jakubczyk K, Antoniewicz J, Mruk H, Janda K. Health Benefits and Chemical Composition of Matcha Green Tea, A Review. Molecules (2020) 26(1):85. doi: 10.3390/molecules26010085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 314. Kang YR, Park J, Jung SK, Chang YH. Synthesis, Characterization, and Functional Properties of Chlorophylls, Pheophytins, and Zn-Pheophytins. Food Chem (2018) 245:943–50. doi: 10.1016/j.foodchem.2017.11.079 [DOI] [PubMed] [Google Scholar]
- 315. Suzuki Y, Shioi Y. Identification of Chlorophylls and Carotenoids in Major Teas by High-Performance Liquid Chromatography With Photodiode Array Detection. J Agric Food Chem (2003) 51(18):5307–14. doi: 10.1021/jf030158d [DOI] [PubMed] [Google Scholar]
- 316. Grzesik M, Naparlo K, Bartosz G, Sadowska-Bartosz I. Antioxidant Properties of Catechins: Comparison With Other Antioxidants. Food Chem (2018) 241:480–92. doi: 10.1016/j.foodchem.2017.08.117 [DOI] [PubMed] [Google Scholar]
- 317. Menegazzi M, Mariotto S, Dal Bosco M, Darra E, Vaiana N, Shoji K, et al. Direct Interaction of Natural and Synthetic Catechins With Signal Transducer Activator of Transcription 1 Affects Both Its Phosphorylation and Activity. FEBS J (2014) 281(3):724–38. doi: 10.1111/febs.12618 [DOI] [PubMed] [Google Scholar]
- 318. Steinmann J, Buer J, Pietschmann T, Steinmann E. Anti-Infective Properties of Epigallocatechin-3-Gallate (EGCG), a Component of Green Tea. Br J Pharmacol (2013) 168(5):1059–73. doi: 10.1111/bph.12009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 319. Channappanavar R, Zhao J, Perlman S. T Cell-Mediated Immune Response to Respiratory Coronaviruses. Immunol Res (2014) 59(1-3):118–28. doi: 10.1007/s12026-014-8534-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 320. Babaei F, Mirzababaei M, Nassiri-Asl M. Quercetin in Food, Possible Mechanisms of Its Effect on Memory. J Food Sci (2018) 83(9):2280–7. doi: 10.1111/1750-3841.14317 [DOI] [PubMed] [Google Scholar]
- 321. Costa LG, Garrick JM, Roque PJ, Pellacani C. Mechanisms of Neuroprotection by Quercetin, Counteracting Oxidative Stress and More. Oxid Med Cell Longev (2016) 2016:2986796. doi: 10.1155/2016/2986796 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 322. Senggunprai L, Kukongviriyapan V, Prawan A, Kukongviriyapan U. Quercetin and EGCG Exhibit Chemopreventive Effects in Cholangiocarcinoma Cells via Suppression of JAK/STAT Signaling Pathway. Phytother Res (2014) 28(6):841–8. doi: 10.1002/ptr.5061 [DOI] [PubMed] [Google Scholar]
- 323. Alvarez P, Alvarado C, Puerto M, Schlumberger A, Jimenez L, de la Fuente M. Improvement of Leukocyte Functions in Prematurely Aging Mice After Five Weeks of Diet Supplementation With Polyphenol-Rich Cereals. Nutrition (2006) 22(9):913–21. doi: 10.1016/j.nut.2005.12.012 [DOI] [PubMed] [Google Scholar]
- 324. Hashemzaei M, Delarami Far A, Yari A, Heravi RE, Tabrizian K, Taghdisi SM, et al. Anticancer and Apoptosisinducing Effects of Quercetin In Vitro and In Vivo . Oncol Rep (2017) 38(2):819–28. doi: 10.3892/or.2017.5766 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 325. Spagnuolo C, Russo M, Bilotto S, Tedesco I, Laratta B, Russo GL. Dietary Polyphenols in Cancer Prevention, the Example of the Flavonoid Quercetin in Leukemia. Ann N Y Acad Sci (2012) 1259:95–103. doi: 10.1111/j.1749-6632.2012.06599.x [DOI] [PubMed] [Google Scholar]
- 326. Araujo JR, Goncalves P, Martel F. Chemopreventive Effect of Dietary Polyphenols in Colorectal Cancer Cell Lines. Nutr Res (2011) 31(2):77–87. doi: 10.1016/j.nutres.2011.01.006 [DOI] [PubMed] [Google Scholar]
- 327. Nair MP, Kandaswami C, Mahajan S, Chadha KC, Chawda R, Nair H, et al. The Flavonoid, Quercetin, Differentially Regulates Th-1 (IFNgamma) and Th-2 (IL4) Cytokine Gene Expression by Normal Peripheral Blood Mononuclear Cells. Biochim Biophys Acta (2002) 1593(1):29–36. doi: 10.1016/S0167-4889(02)00328-2 [DOI] [PubMed] [Google Scholar]
- 328. Wang S, Yao J, Zhou B, Yang J, Chaudry MT, Wang M, et al. Bacteriostatic Effect of Quercetin as an Antibiotic Alternative In Vivo and Its Antibacterial Mechanism In Vitro . J Food Prot (2018) 81(1):68–78. doi: 10.4315/0362-028X.JFP-17-214 [DOI] [PubMed] [Google Scholar]
- 329. Sahpazidou D, Geromichalos GD, Stagos D, Apostolou A, Haroutounian SA, Tsatsakis AM, et al. Anticarcinogenic Activity of Polyphenolic Extracts From Grape Stems Against Breast, Colon, Renal and Thyroid Cancer Cells. Toxicol Lett (2014) 230(2):218–24. doi: 10.1016/j.toxlet.2014.01.042 [DOI] [PubMed] [Google Scholar]
- 330. Vargas AJ, Burd R. Hormesis and Synergy, Pathways and Mechanisms of Quercetin in Cancer Prevention and Management. Nutr Rev (2010) 68(7):418–28. doi: 10.1111/j.1753-4887.2010.00301.x [DOI] [PubMed] [Google Scholar]
- 331. Hsu CL, Yen GC. Phenolic Compounds, Evidence for Inhibitory Effects Against Obesity and Their Underlying Molecular Signaling Mechanisms. Mol Nutr Food Res (2008) 52(1):53–61. doi: 10.1002/mnfr.200700393 [DOI] [PubMed] [Google Scholar]
- 332. Jakubczyk K, Kochman J, Kwiatkowska A, Kaldunska J, Dec K, Kawczuga D, et al. Antioxidant Properties and Nutritional Composition of Matcha Green Tea. Foods (2020) 9(4):483. doi: 10.3390/foods9040483 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 333. Kolackova T, Kolofikova K, Sytarova I, Snopek L, Sumczynski D, Orsavova J. Matcha Tea: Analysis of Nutritional Composition, Phenolics and Antioxidant Activity. Plant Foods Hum Nutr (2020) 75(1):48–53. doi: 10.1007/s11130-019-00777-z [DOI] [PubMed] [Google Scholar]
- 334. Mitani T, Nagano T, Harada K, Yamashita Y, Ashida H. Caffeine-Stimulated Intestinal Epithelial Cells Suppress Lipid Accumulation in Adipocytes. J Nutr Sci Vitaminol (Tokyo) (2017) 63(5):331–8. doi: 10.3177/jnsv.63.331 [DOI] [PubMed] [Google Scholar]
- 335. Unno K, Furushima D, Hamamoto S, Iguchi K, Yamada H, Morita A, et al. Stress-Reducing Effect of Cookies Containing Matcha Green Tea, Essential Ratio Among Theanine, Arginine, Caffeine and Epigallocatechin Gallate. Heliyon (2019) 5(5):e01653. doi: 10.1016/j.heliyon.2019.e01653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 336. Ku KM, Choi JN, Kim J, Kim JK, Yoo LG, Lee SJ, et al. Metabolomics Analysis Reveals the Compositional Differences of Shade Grown Tea (Camellia Sinensis L.). J Agric Food Chem (2010) 58(1):418–26. doi: 10.1021/jf902929h [DOI] [PubMed] [Google Scholar]
- 337. Kaneko S, Kumazawa K, Masuda H, Henze A, Hofmann T. Molecular and Sensory Studies on the Umami Taste of Japanese Green Tea. J Agric Food Chem (2006) 54(7):2688–94. doi: 10.1021/jf0525232 [DOI] [PubMed] [Google Scholar]
- 338. Bialecka-Florjanczyk E, Fabiszewska A, Zieniuk B. Phenolic Acids Derivatives - Biotechnological Methods of Synthesis and Bioactivity. Curr Pharm Biotechnol (2018) 19(14):1098–113. doi: 10.2174/1389201020666181217142051 [DOI] [PubMed] [Google Scholar]
- 339. Stefanello N, Spanevello RM, Passamonti S, Porciuncula L, Bonan CD, Olabiyi AA, et al. Coffee, Caffeine, Chlorogenic Acid, and the Purinergic System. Food Chem Toxicol (2019) 123:298–313. doi: 10.1016/j.fct.2018.10.005 [DOI] [PubMed] [Google Scholar]
- 340. Naveed M, Hejazi V, Abbas M, Kamboh AA, Khan GJ, Shumzaid M, et al. Chlorogenic Acid (CGA): A Pharmacological Review and Call for Further Research. BioMed Pharmacother (2018) 97:67–74. doi: 10.1016/j.biopha.2017.10.064 [DOI] [PubMed] [Google Scholar]
- 341. Weng CJ, Yen GC. Chemopreventive Effects of Dietary Phytochemicals Against Cancer Invasion and Metastasis, Phenolic Acids, Monophenol, Polyphenol, and Their Derivatives. Cancer Treat Rev (2012) 38(1):76–87. doi: 10.1016/j.ctrv.2011.03.001 [DOI] [PubMed] [Google Scholar]
- 342. Ghorbani A. Mechanisms of Antidiabetic Effects of Flavonoid Rutin. BioMed Pharmacother (2017) 96:305–12. doi: 10.1016/j.biopha.2017.10.001 [DOI] [PubMed] [Google Scholar]
- 343. Hosseinzadeh H, Nassiri-Asl M. Review of the Protective Effects of Rutin on the Metabolic Function as an Important Dietary Flavonoid. J Endocrinol Invest (2014) 37(9):783–8. doi: 10.1007/s40618-014-0096-3 [DOI] [PubMed] [Google Scholar]
- 344. Reygaert WC. Green Tea Catechins: Their Use in Treating and Preventing Infectious Diseases. BioMed Res Int (2018) 2018:9105261. doi: 10.1155/2018/9105261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 345. Ohishi T, Goto S, Monira P, Isemura M, Nakamura Y. Anti-Inflammatory Action of Green Tea. Antiinflamm Antiallergy Agents Med Chem (2016) 15(2):74–90. doi: 10.2174/1871523015666160915154443 [DOI] [PubMed] [Google Scholar]
- 346. Miura Y, Chiba T, Tomita I, Koizumi H, Miura S, Umegaki K, et al. Tea Catechins Prevent the Development of Atherosclerosis in Apoprotein E-Deficient Mice. J Nutr (2001) 131(1):27–32. doi: 10.1093/jn/131.1.27 [DOI] [PubMed] [Google Scholar]
- 347. Yang CS, Wang H. Cancer Preventive Activities of Tea Catechins. Molecules (2016) 21(12):1679. doi: 10.3390/molecules21121679 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 348. Zhang L, Xie J, Gan R, Wu Z, Luo H, Chen X, et al. Synergistic Inhibition of Lung Cancer Cells by EGCG and NF-kappaB Inhibitor BAY11-7082. J Cancer (2019) 10(26):6543–56. doi: 10.7150/jca.34285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 349. Lin HY, Hou SC, Chen SC, Kao MC, Yu CC, Funayama S, et al. (-)-Epigallocatechin Gallate Induces Fas/CD95-Mediated Apoptosis Through Inhibiting Constitutive and IL-6-Induced JAK/STAT3 Signaling in Head and Neck Squamous Cell Carcinoma Cells. J Agric Food Chem (2012) 60(10):2480–9. doi: 10.1021/jf204362n [DOI] [PubMed] [Google Scholar]
- 350. Calder PC. Nutrition, Immunity and COVID-19. BMJ Nutr Prev Health (2020) 3(1):74–92. doi: 10.1136/bmjnph-2020-000085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 351. Filippou PS, Karagiannis GS. Cytokine Storm During Chemotherapy, a New Companion Diagnostic Emerges? Oncotarget (2020) 11(3):213–5. doi: 10.18632/oncotarget.27442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 352. Hadjadj J, Yatim N, Barnabei L, Corneau A, Boussier J, Smith N, et al. Impaired Type I Interferon Activity and Inflammatory Responses in Severe COVID-19 Patients. Science (2020) 369(6504):718–24. doi: 10.1126/science.abc6027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 353. Ranjith-Kumar CT, Lai Y, Sarisky RT, Cheng Kao C. Green Tea Catechin, Epigallocatechin Gallate, Suppresses Signaling by the dsRNA Innate Immune Receptor RIG-I. PloS One (2010) 5(9):e12878. doi: 10.1371/journal.pone.0012878 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 354. Eid HM, Haddad PS. The Antidiabetic Potential of Quercetin, Underlying Mechanisms. Curr Med Chem (2017) 24(4):355–64. doi: 10.2174/0929867323666160909153707 [DOI] [PubMed] [Google Scholar]
- 355. Abdel-Latif M, Afifi A, Soliman R, Elkhouly A, Abdelmotaal A, Youness RA. A New Quercetin Glycoside Enhances TNBC Immunological Profile Through TP53/miR-155/MICA/Ulbp2. Ann Oncol (2019) 30:vii7–8. doi: 10.1093/annonc/mdz413.028 [DOI] [Google Scholar]
- 356. Ahmed Youness R, Amr Assal R, Mohamed Ezzat S, Zakaria Gad M, Abdel Motaal A. A Methoxylated Quercetin Glycoside Harnesses HCC Tumor Progression in a TP53/miR-15/miR-16 Dependent Manner. Nat Prod Res (2020) 34(10):1475–80. doi: 10.1080/14786419.2018.1509326 [DOI] [PubMed] [Google Scholar]
- 357. Kuo PC, Liu HF, Chao JI. Survivin and P53 Modulate Quercetin-Induced Cell Growth Inhibition and Apoptosis in Human Lung Carcinoma Cells. J Biol Chem (2004) 279(53):55875–85. doi: 10.1074/jbc.M407985200 [DOI] [PubMed] [Google Scholar]
- 358. Bae JH, Kim JY, Kim MJ, Chang SH, Park YS, Son CH, et al. Quercetin Enhances Susceptibility to NK Cell-Mediated Lysis of Tumor Cells Through Induction of NKG2D Ligands and Suppression of HSP70. J Immunother (2010) 33(4):391–401. doi: 10.1097/CJI.0b013e3181d32f22 [DOI] [PubMed] [Google Scholar]
- 359. Ha EJ, Kim KY, Kim CE, Jun DY, Kim YH. Enhancement of Quercetin-Induced Apoptosis by Cotreatment With Autophagy Inhibitor Is Associated With Augmentation of BAK-Dependent Mitochondrial Pathway in Jurkat T Cells. Oxid Med Cell Longev (2019) 2019:7989276. doi: 10.1155/2019/7989276 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 360. Begum R, Sharma M, Pillai KK, Aeri V, Sheliya MA. Inhibitory Effect of Careya Arborea on Inflammatory Biomarkers in Carrageenan-Induced Inflammation. Pharm Biol (2015) 53(3):437–45. doi: 10.3109/13880209.2014.923005 [DOI] [PubMed] [Google Scholar]
- 361. Erden Inal M, Kahraman A. The Protective Effect of Flavonol Quercetin Against Ultraviolet a Induced Oxidative Stress in Rats. Toxicology (2000) 154(1-3):21–9. doi: 10.1016/S0300-483X(00)00268-7 [DOI] [PubMed] [Google Scholar]
- 362. Habtemariam S. Rutin as a Natural Therapy for Alzheimer’s Disease, Insights Into Its Mechanisms of Action. Curr Med Chem (2016) 23(9):860–73. doi: 10.2174/0929867323666160217124333 [DOI] [PubMed] [Google Scholar]
- 363. Nadi E, Tavakoli F, Zeraati F, Goodarzi MT, Hashemi SH. Effect of Vitamin C Administration on Leukocyte Vitamin C Level and Severity of Bronchial Asthma. Acta Med Iran (2012) 50(4):233–8. [PubMed] [Google Scholar]
- 364. Khanna K, Kohli SK, Kaur R, Bhardwaj A, Bhardwaj V, Ohri P, et al. Herbal Immune-Boosters, Substantial Warriors of Pandemic Covid-19 Battle. Phytomedicine (2021) 85:153361. doi: 10.1016/j.phymed.2020.153361 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 365. Panyod S, Ho CT, Sheen LY. Dietary Therapy and Herbal Medicine for COVID-19 Prevention, A Review and Perspective. J Tradit Complement Med (2020) 10(4):420–7. doi: 10.1016/j.jtcme.2020.05.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 366. Du HZ, Hou XY, Miao YH, Huang BS, Liu DH. Traditional Chinese Medicine: an Effective Treatment for 2019 Novel Coronavirus Pneumonia (NCP). Chin J Nat Med (2020) 18(3):206–10. doi: 10.1016/S1875-5364(20)30022-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 367. Han HJ, Nwagwu C, Anyim O, Ekweremadu C, Kim S, et al. COVID-19 and Cancer, From Basic Mechanisms to Vaccine Development Using Nanotechnology. Int Immunopharmacol (2021) 90:107247. doi: 10.1016/j.intimp.2020.107247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 368. Kuderer NM, Hill JA, Carpenter PA, Lyman GH. Challenges and Opportunities for COVID-19 Vaccines in Patients With Cancer. Cancer Invest (2021) 39(3):205–13. doi: 10.1080/07357907.2021.1885596 [DOI] [PubMed] [Google Scholar]