

Abstract
Objectives
Differences between men and women are common in published research on aging and Alzheimer’s disease and Alzheimer’s disease-related dementias (AD/ADRD). What do these differences mean? To answer this, rigorous measurement is needed. We investigated current methods for measuring sex/gender in aging and AD/ADRD cohort studies.
Methods
An online survey was sent to National Institute on Aging-funded Alzheimer’s Disease Research Centers (n = 38) and investigator-initiated cohort studies (n = 38) to assess practices around enrollment of men and women and measurement of sex and gender.
Results
The response rate was 65.8% (n = 50). All enrolled men and all but two investigator-initiated studies enrolled women. Most cohorts (43/50) had no documented definitions for categories of “men” or “women.” Over 85% of cohorts relied solely on self-report questions to capture sex/gender data (n = 43/50). Issues with administration were also identified (n = 7).
Discussion
Our findings identify gaps in current approaches used to measure sex and gender in aging and AD/ADRD research. We discuss opportunities to bridge these gaps and advance measurement of sex and gender in aging and AD/ADRD research. Changes are needed to ensure inclusion and representation of sociocultural diversity in research samples, and consistency in data collection in aging and AD/ADRD research.
Keywords: Aging research, Alzheimer’s research, Biologic sex, Gender, Measurement
The United States has set an ambitious national goal to understand the influences of gender and biologic sex on risk, development, progression, diagnosis, and clinical presentation of Alzheimer’s disease and Alzheimer’s disease-related dementias (AD/ADRD) (Milestone 2.D, n.d.; NOT-AG-20-038: Notice of Special Interest: Sex and Gender Differences in Alzheimers Disease and Alzheimers Disease-Related Dementias (AD/ADRD), n.d.). An essential element of achieving this goal is advancing how sex and gender are considered in AD/ADRD research. Sex is a biologic concept that consists of chromosomes, sex organs, endogenous hormones, and other features encoded in DNA that typically characterize differences between men and women. Gender, by contrast, consists of enacted roles and behaviors that occur in historical and cultural contexts (Including Women and Minorities in Clinical Research Background |Office of Research on Women’s Health, 2001).
Over the last century, numerous studies have documented that older adults’ cognitive outcomes differ between men and women (Mielke et al., 2014; Snyder et al., 2016). AD/ADRD research has shown variation between men and women in how older adults protect their cognitive health, reduce their risk for cognitive decline, and manage cognitive changes (Jäncke, 2018). Moreover, emerging evidence from biomarker studies suggests neurocorrelates of disease and pathology vary with self-reported sex/gender (Armstrong et al., 2019).
What features of gender and biologic sex drive the observed differences? Answering this question could provide useful information to improve quality of life and care for persons with AD/ADRD and their families. Influences of gender and biologic sex may be apparent from the bench to bedside in AD/ADRD research. Gender and sex are well-known social and structural determinants of health (SSDoH) as they shape environmental conditions where individuals are born, live, learn, work, play, worship, and age. As SSDoH, they can affect individuals’ behavioral and environmental risks for AD/ADRD, receipt of a diagnosis, and access to treatment and the efficacy of those treatments (Hill et al., 2015). Data show that sex, for example, can have biologic influences that may explicate pathways relevant to AD/ADRD outcomes such as caregiving and physical risk factors (Iervolino et al., 2005; Ruble et al., 2006). Emerging evidence suggests gender—through its effects on interpersonal interactions and social conditions—may modify hormone levels and other biologic characteristics (Fox et al., 1997). Data also suggest the potential for complex interplays between sex and gender mechanisms that may be relevant in AD/ADRD research. Sex hormones, for example, have been shown to affect both neurologic correlates in the brain (McEwen, 2020) and also gender-role behavior (Meyer-Bahlburg, 1984).
If scientists gain understanding of specific processes that drive sex and gender effects, this knowledge may help explain heterogeneity in cognitive, functional, biomarker, and interventional outcomes in AD/ADRD research and clinical practice. In the longer term, the knowledge may help researchers optimize the efficacy and effectiveness of pharmacologic therapies and other treatment interventions. In addition, the conduct of ethically and conceptually rigorous sex and gender research may help improve inclusion and equity for sexual and gender minoritized (SGM) populations and reduce disparities in care for all patients.
For these reasons, there is a critical need to assess how gender and biologic sex are being treated in AD/ADRD research to determine whether—and to what degree—the field is adequately measuring sex and gender. Unfortunately, the conflation of sex and gender is recognized as a long-standing and widespread problem in the biomedical literature (Alex et al., 2012; Institute of Medicine (US) Committee on Understanding the Biology of Sex and Gender Differences, 2001). Further, SGM populations—those whose gender, reproductive development, or sexual orientation varies from traditional, societal, cultural, or physiological norms—are often unrepresented in research, this contributes to health disparities but also limits researchers’ ability to make scientific discoveries informed by the range of human diversity (National Institutes of Health, 2021).
The National Institutes of Health (NIH) recognize the importance of considering sex and gender in the pursuit of scientific discoveries. NIH policies underscore the roles of sex and gender in both representation in research samples (History of Women’s Participation in Clinical Research | Office of Research on Women’s Health, n.d.) and in the design, conduct, and reporting of studies (Including Women and Minorities in Clinical Research Background |Office of Research on Women’s Health, 2001; Institute of Medicine (US) Committee on Understanding the Biology of Sex and Gender Differences, 2001). There is a need for rigor in measurement of gender and biologic sex in AD/ADRD science in order to assure both adequate representation in research samples and consideration in the conduct of studies.
In this article, we report the results of a survey of National Institute on Aging (NIA)-funded Alzheimer’s Disease Research Centers (ADRCs) and investigator-initiated cohort studies. In cohort studies, a group of research participants is followed longitudinally. Such studies serve as a key resource in the investigation of AD/ADRD mechanisms. Research cohorts, particularly ADRC cohorts, account for a large proportion of the data available for understanding risk factors, symptom trajectories, pathology, and more. In addition, some AD/ADRD cohorts have operated for decades, providing a unique record of how scientific practices can change over time with advances in scholarship and technology. This is particularly relevant to measurement of sex and gender as scholarly understanding of these constructs has evolved in recent decades (Bajic et al., 2020; Dressel et al., 1997; Hurst & Peck, 1996; Montañez, 2017; Zhao & Scholar, 2019).
We describe past and current practices for collecting gender and biological sex data and then identify opportunities to advance gender and biologic sex measurement and to ensure inclusion, representation, and consistency in data collection across AD/ADRD research. Given reports that sex and gender concepts in biomedical scholarship can be ambiguous and have interchangeable usages (Alex et al., 2012; Institute of Medicine (US) Committee on Understanding the Biology of Sex and Gender Differences, 2001), we hypothesized that there may need to be changes in how the concepts are measured in order to improve the consistency and rigor in their applications in AD/ADRD science. The findings offer insights into strengths and gaps in measurement that may help advance our understanding of the impact of gender and biologic sex on trajectories of brain aging and dementia (Milestone 2.D, n.d.).
Method
Eligibility Criteria
Studies and centers were eligible if they were partially or fully funded by the NIA to collect longitudinal data on older adults. They also had to be based in the United States and sample individuals 65 years or older. Investigator-initiated studies were identified using a resource list from the NIA (see Supplementary Appendix Table A). We also approached all ADRCs as they are required to establish and maintain standing research cohorts of older adults (International Alzheimer’s and Related Dementias Research Portfolio, 2020; NIH-National Institute of Aging, n.d.). Included under the 38 centers we approached are 31 ADRCs “working to translate research advances into improved diagnosis and care for people with Alzheimer’s disease, as well as working to find a treatment or way to prevent Alzheimer’s and other types of dementia.” We also approached four exploratory centers that were “designed to expand and diversify research and education opportunities to new areas of the country, new populations, and new areas of science and approaches to research,” the National Alzheimer’s Disease Coordinating Center (NACC), the Alzheimer’s Disease Genetics Consortium, and the Alzheimer’s Disease Sequencing Project (International Alzheimer’s and Related Dementias Research Portfolio, 2020; NIH-National Institute of Aging, n.d.).
Survey Development
We used Dillman’s tailored design method to develop and administer a survey about sex/gender measurement (Dillman et al., 2014). This is a well-established approach that emphasizes attending all aspects of survey design and implementation procedures as experienced by recipients in order to maximize responding and reduce sources of survey error.
Survey questions asked whether cohorts enrolled men and women and, if they did, how the groups were defined. Items also asked about what sex and/or gender measures were administered and for details on each measure’s intended purpose, variable documentation, and when the measure had been added to the study protocol. We asked respondents to describe gender and biologic sex measures as documented in study protocols. We did not ask respondents to discern whether a particular measure was capturing gender or biologic sex. In this report, we use the term “sex/gender” in instances where we could not discern that a concept pertained only to “sex” or “gender.”
Survey questions included:
Does this study enroll women?
If yes, what is the study’s definition of “woman” documented in the protocol?
-
Since when has the study enrolled women?
a. Study inception (part of original design)
-
b. After study inception (later protocol modification)
i. Enter date when women were enrolled in study: _________
A parallel set of questions 1–3 was asked for men. In addition, a seventh question asked respondents to complete a table of details about how sex and/or gender were measured in the protocol. Respondents were also asked to submit the protocol with copies of the measures. To limit potential confusion or nonresponding, we asked respondents to report on measures of “sex and/or gender,” which did not require respondents to discern between the constructs. Questions were developed by the investigators and pilot-tested among a convenience sample of ADRC personnel for clarity and ease of completion (see Supplementary Appendix).
Data Gathering
All NIA-funded investigators or their delegates affiliated with a given center or study were eligible to complete the survey. Data were collected electronically in three phases. In phase I, the survey was distributed via email using Qualtrics on September 3, 2020. Our initial contact included a letter detailing the survey topic, the risks and benefits of participation, and methods for data collection and reporting. Consent was indicated by a participant’s completion of the survey. Consent to recontact was also obtained, and individuals completing the survey were given the option to remain anonymous. The email contained a hyperlink to the survey and a Microsoft Word version of the survey, which could be printed and returned. Reminder emails were sent 1 week and 2 weeks after the initial email.
In phase II, a reminder was sent to ADRCs in early November 2020. We attempted to contact study personnel through the National Alzheimer’s Coordinating Center (NACC) Director’s listserv, which includes all the Directors of the NIA-funded ADRC Program (NIH-National Institute of Aging, n.d.). In phase III, individual follow-up emails were sent to nonresponders for both ADRCs and investigator-initiated studies in late November.
In January 2021, Co-Principal Investigator (Co-PI; S. D. Stites) contacted respondents who reported sex/gender measures but had not submitted respective protocols. Study protocols were provided by six investigator-initiated cohort studies and 12 ADRCs. We were able to locate online verbatim self-report questions used to assess sex/gender for an additional 13 investigator-initiated cohort studies and one ADRC. In total, we gathered 32 study protocols. Data collection closed February 2021.
Data Quality Checks and Analyses
For two investigator-initiated studies, eight measures of sex/gender were reported. However, discussion with one of the PIs and review of study protocols showed each study had only one measure of sex/gender. The study data were updated accordingly.
Results were analyzed using descriptive statistics. The primary unit of analysis was the research center or investigator-initiated study. In five instances, more than one respondent answered for a given center or study. We analyzed all data that were submitted; however, each center or study was counted only one time in denominators and the response rate. In an analysis of duplicate responses, we tried to reconcile inconsistencies using study documentation and report inconsistencies across respondents.
To assess whether our sample included representation from throughout the geographic distribution of NIA-funded cohort studies, we examined the location of centers and study sites within geographic regions of the United States. We used the U.S. Census Bureau’s classification of five regions: the West, Midwest, South, Northeast, and the Pacific (U.S. Census Bureau, n.d.). The University of Pennsylvania Institutional Review Board approved this project.
Results
Sample Characteristics
An online survey was sent to 38 ADRCs with standing research cohorts and 38 investigator-initiated cohort studies on aging and cognition conducted in the United States. Personnel from 25 centers and 25 investigator-initiated studies completed the survey. The response rate was 65.8% (n = 50) and included representation of NIA-funded research cohorts from throughout the country.
In most cases, a PI completed the survey (56%). This category included respondents who identified as a PI, Co-PI, Multiple PI, or Site PI. The full list of respondents is shown in Table 1.
Table 1.
Sample Characteristics of Alzheimer’s Disease Research Centers (ADRCs) and Investigator-Initiated (II) Cohort Studies by Geographic Location and Respondent Role
| ADRC (n = 25) n (%) |
II cohort study (n = 25) n (%) |
Total (N = 50) n (%) |
|
|---|---|---|---|
| U.S. region | |||
| Westa | 7 (28) | 6 (24) | 13 (26) |
| Midwestb | 7 (28) | 7 (28) | 14 (28) |
| Northeastc | 6 (24) | 4 (16) | 10 (20) |
| Southd | 5 (20) | 7 (28) | 12 (24) |
| Pacifice | 0 (0) | 1 (4) | 1 (2) |
| Respondent’s role in study or center | |||
| PI and/or Program Director | 8 (32) | 20 (80) | 28 (56) |
| Core Leader or Deputy Leader | 9 (36) | 0 (0) | 9 (18) |
| Manager | 5 (20) | 2 (8) | 7 (14) |
| Researcher, Scientist, and/or Statistician | 1 (4) | 2 (8) | 3 (6) |
| Administrator | 2 (8) | 0 (0) | 2 (4) |
| Unspecified | 0 (0) | 1 (4) | 1 (2) |
Notes: Principal Investigator (PI), Co-PI, Multiple PI, Site PI.
aWest: WA, OR, ID, MT, WY, CA, NV, UT, CO, AZ, NM.
bMidwest: ND, SD, NE, KS, MN, IA, MO, MI, WI, IL IN, OH.
cNortheast: PA, NY, VT, NH, ME, MA, RI, CT, NJ.
dSouth: KY, WV, VA, DC, MD, DE, TX, OK, AR, LA, TN, NC, MS, AL, GA, SC, FL.
ePacific: AK, HI.
Enrollment of Men and Women in AD/ADRD Cohort Studies
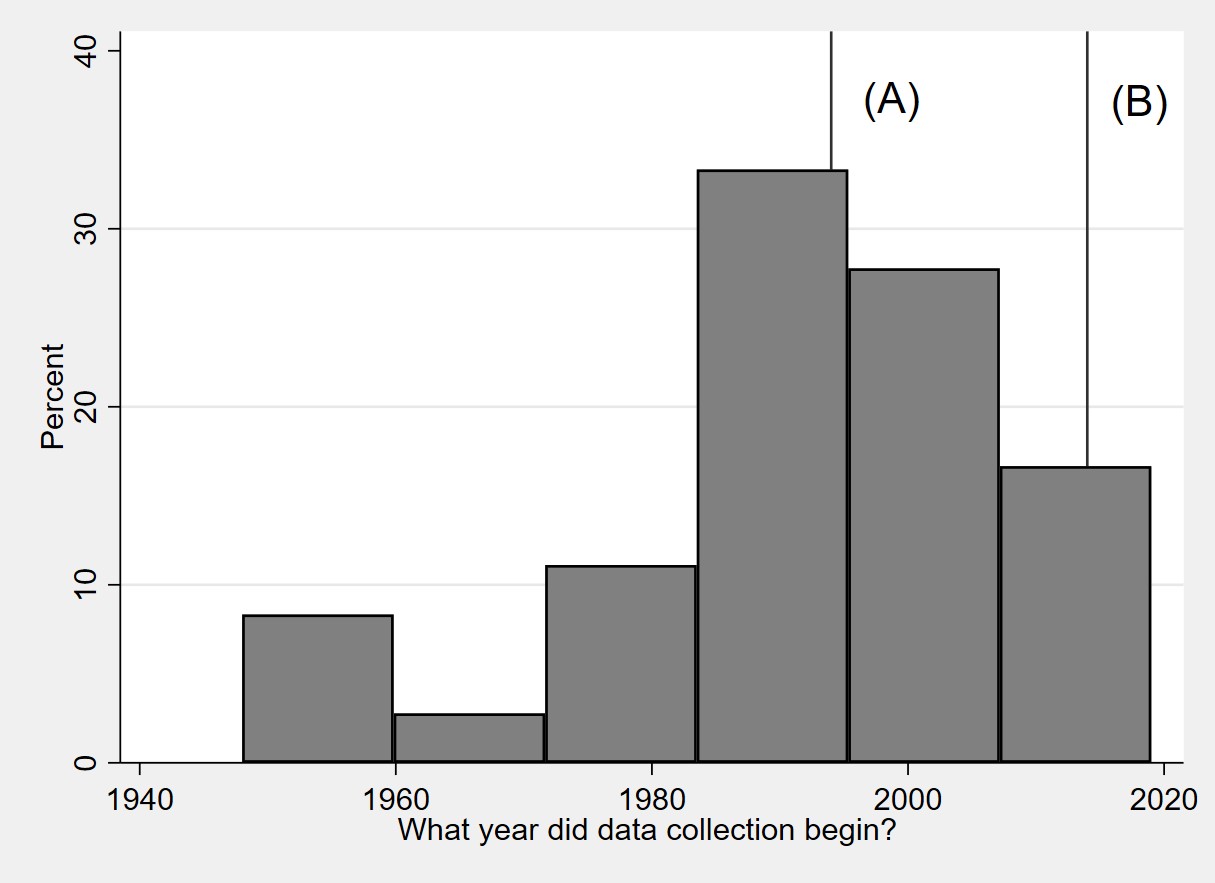
Participant recruitment in the ADRCs and investigator-initiated studies was started between 1948 and 2019 (Supplementary Appendix Figure 1). Of the cohorts maintained by the centers and investigator-initiated studies, all enrolled men and all but two enrolled women (Table 2). One investigator-initiated study underwent a protocol modification in 1978 in order to expand enrollment to women. This was well before NIH’s 1994 policy that required applicants to justify exclusion of women and minorities in clinical research.
Table 2.
Enrollment of Men and Women and Study Protocol Definitions for Sex/Gender in Alzheimer’s Disease Research Centers (ADRCs) and Investigator-Initiated (II) Cohort Studies
| ADRC (n = 25) n (%) |
II cohort study (n = 25) n (%) |
Total (N = 50) n (%) |
|
|---|---|---|---|
| Enrollment of men and women | |||
| Enrolls women | 25 (100) | 23 (92) | 48 (96) |
| From inception | 25 (100) | 22 (88) | 47 (94) |
| Modified to include | 0 (0) | 1 (4) | 1 (2) |
| Enrolls men | 25 (100) | 25 (100) | 50 (100) |
| From inception | 25 (100) | 25 (100) | 50 (100) |
| Modified to include | 0 (0) | 0 (0) | 0 (0) |
| Study protocol definitions for sex/gender | |||
| No definition is documented | 23 (92) | 20 (80) | 43 (86) |
| Definition documented (verbatim responses) | |||
| Gender: female or male | 0 (0) | 1 (4) | 1 (2) |
| Self-reported | 0 (0) | 2 (8) | 2 (4) |
| Female or male | 1 (4) | 0 (0) | 1 (2) |
| Participant-identified biological sex | 0 (0) | 1 (4) | 1 (2) |
| Per NACC forma | 1 (4) | 0 (0) | 1 (2) |
| Self-assessed | 0 (0) | 1 (4) | 1 (2) |
Note:
aNACC = National Alzheimer’s Coordinating Center.
The majority of centers and investigator-initiated studies had no documented definitions of “man” or “woman”: 23/25 (92%) for ADRCs and 20/25 (80%) for investigator-initiated studies. Of the seven reporting definitions, sex/gender definitions included the following: “male and female” (n = 2), “biologic sex” (n = 1), “self-report” (n = 3), or defined by another data source (“NACC form” n = 1).
There were five instances where two respondents from the same center or study responded. In one of these instances, one respondent reported that the variable’s name as entered into the data repository or code book was labeled “sex” while the other respondent reported that it was labeled “gender” (n = 1). The study’s documentation confirmed both terms were used interchangeably.
Measuring Sex/Gender in AD/ADRD Cohort Studies
About three-quarters of centers (n = 20/25) and investigator-initiated studies (n = 19/25) used one measure of sex/gender in their respective cohort (Table 3). About 14% (n = 7) had two or three measures. In four of the six instances where two measures of sex/gender were reported, the study protocols underwent modifications over time to make changes to how sex/gender were measured (1979 [n = 2], 1995 [n = 1], and 2005 [n = 1]). Three of the four underwent protocol modifications to add questions that assessed “sexual identity” and “sexual orientation.” One added a measure of “genetic sex.”
Table 3.
Counts of Sex/Gender Measures in Alzheimer’s Disease Research Centers (ADRCs) and Investigator-Initiated (II) Cohort Studies
| Count of measures used to assess sex/gender | ADRC (n = 25) n (%) |
II cohort study (n = 25) n (%) |
Total (N = 50) n (%) |
|---|---|---|---|
| 1 | 20 (80) | 19 (76) | 39 (78) |
| 2 | 3 (12) | 3 (12) | 6 (12) |
| 3 | 1 (4) | 0 (0) | 1 (2) |
| Unknown | 1 (4) | 3 (12) | 4 (8) |
We also asked how a measure was administered for data collection and labeled in related data repositories. In total, data on 52 measures of sex/gender were described by respondents. The measures are summarized in Table 4 using variable descriptions and variable names.
Table 4.
Sex and Gender Measure Variable Names and Collection Methods in Alzheimer’s Disease Research Centers (ADRCs) and Investigator-Initiated (II) Cohort Studies Protocols
| Variablea name | Sexb | Gender | IDNOc | HRTd | Genotype | Unknowne | No variable | Total |
|---|---|---|---|---|---|---|---|---|
| Source type | ||||||||
| ADRCs | 25 | 4 | 0 | 0 | 0 | 4 | 0 | 33 |
| II cohort studies | 11 | 5 | 1 | 1 | 1 | 4 | 2 | 25i |
| Total | 36 | 9 | 1 | 1 | 1 | 8 | 2 | |
| Collection method | ||||||||
| Biologic specimen | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| Direct observationf | 5 | 1 | 0 | 0 | 0 | 1 | 1 | 8 |
| Self-reportg | 32 | 8 | 1 | 1 | 0 | 1 | 0 | 43 |
| Other sourceh | 5 | 0 | 0 | 0 | 0 | 0 | 1 | 6 |
| Unknown | 0 | 0 | 0 | 0 | 0 | 7 | 0 | 7 |
| Total | 42j | 9 | 1 | 1 | 1 | 9k | 2 |
Notes:
aThe name of variable as entered into the study’s data set or code book.
bIncludes variables labeled “sex” or derivative term (i.e., subject’s sex, sexrsp).
c“Study participant identification (ID) number” intended to indicate biological sex, whereby ID numbers 1 to 4,999 were assigned to men and those 5,000 to 9,999 were assigned to women.
dA single self-report item. Female participants are asked the following question: “Did you ever take any type of estrogen hormonal medication, for example, Premarin, Ogen, or Estrace, or progesterone hormonal medication, for example, Provera?” (Hormone Replacement Therapy Variable Details | RADC, n.d.).
eUnknowns = No responses (ADRC, n = 3; II, n = 0), “self-report” (ADRC, n = 1; II, n = 1). The responses from ADRCs account for four of five instances where multiple individuals from the same institution responded to the survey.
fBased on interviewer observation (n = 1), self-report and physical examination/observation (n = 4), or no clarification was provided (n = 3).
gMay be answered by participant/subject, informant, or study personnel, as described in study procedures.
hObtained from an existing record such as medical record, insurance record, or other secondary source.
iIncludes one instance where two respondents answered on behalf of a cohort study.
jSix sex variable responses with multiple measurements (i.e., self-report and direct observation).
kOne response (“self-report”) listed two methods of measurement (direct observation and self-report).
The most common method of data collection was self-report (n = 43). Self-report measures asked research participants to report whether they identified as “male or female” or “man or woman.” Most often (n = 36) the term “sex” or a derivative term (i.e., subject’s sex, sexrsp) was used to name the variable in respective data repositories. The term “gender” was less often used to name the variable (n = 9).
In contrast to self-report, some sex/gender data were based on observations made by research coordinators or other study personnel (n = 4). In a few cases, sex/gender data were collected from existing repositories (n = 3). Sources of data included medical records, insurance records, or another secondary source. The data were documented as “sex” or related term in the data set (n = 2) or not recorded in a study data set (n = 1).
Of 43 self-report sex/gender questions, we were able to review 32 protocols associated with these questions. The most common question that was used in ADRCs and investigator-initiated cohort studies asked for the subject’s “Sex: Male or Female” (n = 23; Table 5).
Table 5.
Sex and Gender Self-Report Questions From Alzheimer’s Disease Research Centers (ADRCs) and Investigator-Initiated (II) Cohort Study Protocols
| Sex/gender question | ADRCsa (n = 13) | II cohort studiesb (n = 19) |
|---|---|---|
| Subject’s sex: | ||
| 1. Male | 10 | 14 |
| 2. Female | ||
| Subject’s sex: | ||
| What sex do you consider yourself? | 0 | 1 |
| 1. Male | ||
| 2. Female | ||
| 3. Don’t know | ||
| 4. Refused | ||
| Gender: | ||
| Please select your gender identity: | 0 | 2 |
| 1. Male | ||
| 2. Female | ||
| Genderf: | ||
| Please select your gender identity: | 1 | 0 |
| 1. Male | ||
| 2. Female | ||
| 3. Nonbinary/genderfluid | ||
| Sex at birthf: | ||
| What was your sex at birth? | 2 | 0 |
| 1. Female | ||
| 2. Male | ||
| Sexual orientationc,f: | ||
| What is your sexual orientation? | 2 | 0 |
| 1. Bisexual | ||
| 2. Gay | ||
| 3. Lesbian | ||
| 4. Straight (heterosexual) | ||
| 5. Questioning or unsure | ||
| 6. Other | ||
| 7. Prefer not to answer | ||
| No written protocol | 1 | 0 |
| Unknown/unclear | 1e | 0 |
| Secondary sourcesd | 0 | 2 |
Notes: Number of responses may exceed number of reporting entities as some ADRCs and investigator-initiated cohort studies had multiple questions in their protocols.
aTwelve protocols from ADRCs survey responses and one additional ADRCs protocols obtained via online public source.
bSix protocols from investigator-initiated cohort study personnel survey responses and 13 additional investigator-initiated cohort study protocols obtained via online public source.
cIn one instance, item was proposed but not yet included in assessment battery.
dWhile sexual orientation is a construct distinct from sex and gender, this table shows all self-report measures submitted for the current study.
eCoordinator intake: “Coordinators obtain study consent and, if applicable, brain donation consent ... Participant demographics and family history are also tabulated.”
fObtained from an existing source such as medical record, insurance record, or other secondary record.
For most self-reported sex/gender questions, explicit direction was given that the subject or research participant would answer the question (n = 25). However, in some instances (n = 7), no direction was given (n = 5) or research coordinators were expected to complete the question based on their observations (n = 2). It is not uncommon in AD/ADRD research for a proxy to complete a measure on a participant’s behalf, but this issue was only explicitly addressed in the protocol for one measure.
Discussion
Data on measurement practices of sex/gender in AD/ADRD research cohorts were gathered from 25 ADRCs and 25 investigator-initiated studies. The results provide a summary of practices covering cohorts founded from 1948 to 2019. We first discuss the implications of our findings in terms of gaps and goals in measurement practices. Then, given the strengths and limitations of current sex and gender data, we offer strategies for conducting research with currently available sex/gender data. Our overall goal is to inform ways to improve rigor in AD/ADRD science as this may, in turn, help advance research to understand the impact of sex and gender effects on trajectories of brain aging and dementia (Milestone 2.D, n.d.).
Enrollment of Socioculturally and Biologically Diverse Sex/Gender Groups
All centers and studies enrolled men and all but two investigator-initiated studies enrolled women. Given the historical overreliance of science on men and male mice, the large proportion of cohorts enrolling women was an unexpected but encouraging finding. However, most cohorts had no documented definitions for categories of “men” or “women”: 23/25 (92%) ADRCs and 20/25 (80%) investigator-initiated studies.
Cohorts that had definitions (n = 7) relied on the structure of the assessment to create that definition. In these cases, research participants self-identified with a group from a forced-choice list. The sufficiency of this as a scientific definition is a question that warrants scrutiny. The practice breaks with typical scientific methods where a measure follows from a conceptual understanding with the goal being to describe a property of that concept (Tal, 2013). An explicit understanding of what it is being measured is essential in science for operationalizing the concept in research.
Implicit in self-report sex/gender questions is the idea that the groupings reflect socially agreed upon categories to which individuals affiliate. Psychological theory poses that individuals may affiliate with social groups based on approaches of either social cohesion or social identity (Fonseca et al., 2019; Mallinson & Hatemi, 2018). None of the self-report sex/gender questions in our sample define the social category membership. To assure rigor in science, the categories should be explicitly defined. In addition, in many cases these self-affiliation questions were described as capturing biologic groupings despite their supporting principles being sociological, not biological. The degree to which self-report sex/gender questions remain acceptable and sufficiently rigorous for measuring biologic constructs, particularly in a historical period of advances in biomarkers, warrants scholarly discussion.
Second, while in many instances explicit direction was given that the research subject or participant would answer the question (n = 25, 58%), other instances seemed to challenge the implied intent that self-report questions capture an individual’s affiliation with a socially agreed upon category. In five instances, no direction was given as to who or how the questions should be completed, and in two instances research coordinators were expected to complete the question. These approaches are problematic, as they can result in inconsistent practices and incorrect information.
Even when instructions were given, they seemed insufficient. In the most commonly used assessment among ADRCs—the NACC Form A1: Subject Demographics—instructions direct that the form “be completed by the intake interviewer based on ADC scheduling records, subject interview, medicine records, and proxy co-participant report (as needed).” It offers no guidance on which method should be used to complete the sex question. When asked for clarification, the NACC helpdesk explained that “regarding the collection and reporting of gender/sex data for NACC participants. This data is all captured via self-report from NACC participants, and doesn’t have any particular guidelines around it.”
These considerations raise an important question: what would be ideal operationalization of the definitions of gender and biologic sex for clinical research? It is a question under increasing social and scientific pressure for an answer. Mounting scientific data are challenging the assumption that sex/gender is binary. Intersex people are born with differences in their chromosomes, hormones, and genitals that fall outside of a binary concept of male and female bodies (Rosenwohl-Mack et al., 2020). Moreover, social categories—like “nonbinary” and “genderqueer”—are appearing in addition to the typically accepted social categories of “man” and “woman.” The NIH definition of biologic sex includes numerous factors, many of which have continuous and multidimensional levels.
NIH policies suggest that a key purpose of gathering self-report sex/gender (identity) data is to assess and, perhaps, ensure adequate representation in research samples. Ideally, a selection criterion should approximate, to the greatest degree possible, relevant distinctions between study participants to answer a research question. Yet, if the concepts and categories that inform the selection criteria are poorly defined, do not approximate differences that matter, or fail to accurately capture social and natural categories, then it can sabotage an otherwise robust study design. Clear and representative definitions of sex and gender are needed for AD/ADRD science, as they can have important ramifications for scientific integrity. In addition to a functional definition, written procedure guidelines may help assure consistency in how protocols are administered.
Expand Measures of Sex and Gender
We examined what data on sex/gender were being gathered in AD/ADRD cohorts. Our results showed that measurement of sex/gender was conducted more consistently across centers than cohort studies. This was an expected finding given efforts to standardize data collection within the national network of centers (National Alzheimer’s Coordinating Center (NACC), n.d.). Nonetheless, both showed a heavy reliance on self-report sex/gender, with most cohorts relying exclusively on self-report sex/gender questions to measure gender and/or biologic sex (78%, n = 39/50).
While self-report identity can be useful for some purposes—such as assessing representativeness of populations in research samples—its use is also limited and can be fraught. One implication of the heavy reliance on self-report is that we cannot disambiguate effects of gender and biologic sex. But, we need to be able to disambiguate effects of sex and gender as sex-linked biology and gendered social experiences may act independently, competitively, or synergistically in AD/ADRD risk. Moreover, there can be a painful tension between self-report questions that ask about an individual’s identity based on gender—one’s experience of self as male, female, trans, or nonbinary—and sex—one’s assignment as male, female, or intersex at birth—for individuals for whom the answers to these questions may differ and a redundancy for individuals for whom the answers are similar. This raises questions that scientists should confront regarding the ethics and usefulness of parsing identity in this way.
The persistent and heavy reliance on self-report questions suggests that measurement of sex and gender in aging and AD/ADRD science has not accommodated the scientific discoveries that have been made over the past decades. Despite scientific advances in scholarly understanding of sex—in terms of genetic redistribution (Hurst & Peck, 1996), mechanisms of sex determination (Montañez, 2017), X (de)activation (Bajic et al., 2020), and Y chromosome effects (Zhao & Scholar, 2019)—and gender—in how it intersects with other SSDoH and disease (Dressel et al., 1997)—few centers or studies in our sample made updates to their original procedures for measuring gender and biologic sex.
AD/ADRD science is experiencing a revolution in biomarkers (Jack et al., 2016). Using this momentum and technologies to expand the number and types of measures of sex/gender to include social, behavioral, and biologic markers could help characterize and quantify sex-based biological influences and cultural and historical effects of gender. This may help characterize natural variance and more directly appraise their influences in AD/ADRD mechanisms. Furthermore, this approach to measurement of biologic sex is responsive to the mounting scientific evidence showing genetic and phenotypic variations that fall outside what is typically understood as male or female (Ainsworth, 2018). It also empowers researchers to select sex measures that are conceptualized to be most directly relevant to the mechanisms under study.
Our general recommendation to expand sex/gender measures beyond a single self-report assessment can be built upon by considering opportunities posed by unique characteristics of research settings and funding mechanisms. Our findings show ADRCs and investigator-initiated studies offer two distinct pathways for conducting research on sex and gender. ADRCs prioritize harmonization of measures which facilitates investigators pooling data across multiple centers to create larger and, potentially, more geographically diverse samples. Investigator-initiated studies, in contrast, prioritize research designs and collection of measures that enable investigations of varying research questions, novel measures, and populations.
Sexual Orientation Data
In two instances, respondents submitted measures of sexual orientation. While related to constructs of gender and biologic sex, sexual orientation is a distinct paradigm that warrants independent investigation. In reporting, we included all items submitted in response to our survey when reporting our results.
The close association of sexual orientation data with gender and biologic sex serves as a reminder that sex, gender, and sexual orientation are often discussed together in terms of SGM populations. Advocates emphasize that measures that are inclusive of human experiences may help reduce disenfranchisement and other disparities experienced by SGM populations, who are underrepresented and understudied in AD/ADRD research (Barrett et al., 2015; Evans-Campbell et al., 2007; Flatt et al., 2018). While this is accurate for SGM populations, advancing measurement practices also has the potential to improve health outcomes for all patients and their families. Well-specified measures of gender and biologic sex can lead to scientific insights into disease mechanisms and modifiers that can drive innovation in prevention, treatment, and management.
Inclusive and Accurate Language
Some scholars attempt to disambiguate gender from sex by assigning them unique vernaculars (American Psychological Association, 2012, 2015). For gender, the nouns “man” and “woman” often indicate social roles (i.e., gender), and the nouns “male” and “female” denote biologic sex. However, male/female can operate as an adjective as well as noun. For example, in the expression “female participant,” it is unclear whether “female” refers to biological aspects of femaleness (i.e., biologic sex) or social and cultural presentation as being female (i.e., gender).
The above example is not intended to correct or dictate use of language but rather to draw attention to the assumptions and ambiguities around us, including those ubiquitous in our language. Written case definitions and protocols for assessing sex and gender may help mitigate some of these issues. Discussion among study teams may also be valuable to ensure shared unified vocabularies and to open opportunities to address bias, stigma, and opacity in our scientific constructs. Moreover, it underscores the need for deliberate choices to establish affirming language in aging and AD/ADRD science. To advance study of sex/gender in AD/ADRD, characterization of the constructs must be disambiguated through discourse on definitions and rigor in measurement.
Available Sex/Gender Research Data
Self-report sex/gender data are fairly routinely collected in aging and AD/ADRD research, making them often available in existing data repositories. We offer recommendations for considering these data in secondary analyses given the gaps and limitations outlined above. Recommendations and guidelines on reporting sex/gender results have been published elsewhere (Cameron & Stinson, 2019; Clayton & Tannenbaum, 2016; Thompson et al., 2019).
In considering self-report sex/gender data for inclusion in analyses, thorough review of the data collection protocol is essential. This documentation may garner insights into sociocultural groups who are represented in the data and those that could be excluded, misrepresented, and/or underrepresented. Moreover, in considering using self-report sex/gender data as a proxy measure for biologic phenotypes or social stereotypes, it is essential to explicitly recognize the limitations of this approach. Thorough reporting of conceptual models, methods, and limitations and humility are essential in order to assure future scientific directions are transparent and that ethical and social harms are avoided. In some cases, it may be prudent to forgo an analysis until appropriate data are available. In addition, researchers may want to use caution in harmonizing sex/gender data across data sources. Our results suggest that there may be important differences in how the data were collected and cataloged.
It is important readers understand the strengths and limitations of a study’s results that are based on self-report sex/gender data. Limitations that are often unmentioned include: (a) whether analyses had adequate statistical power to support conclusions drawn about sex/gender, (b) limitations of the measures in operationalizing concepts that were under study, including if and how the data were being used to proxy phenomena, and (c) whether there were unknown or problematic features of how variables were collected such as whether it was possible to know in the study documentation if the data were gathered via research participant’s self-report or study personnel’s designation.
Limitations
We report on 25 ADRCs and 25 investigator-initiated cohort studies. We invited personnel from all NIH-funded ADRCs and aging cohort studies. While most (60%) were represented in our survey, our results nonetheless represent the subset of those who responded. Particularly given how this study was carried out as a survey of research programs and projects, our results reflect the perspectives of the researchers conducting this work. There is a gap in the biomedical literature around preferences for phrasing sex/gender questions. More specifically, it would be useful to know this information among diverse, older adult populations. There is a need for community-based participatory research to gather from individuals their preferences or reactions to the phrasing of sex/gender questions.
Conclusions
Research cohorts, particularly ADRC cohorts, contribute a bulk of data to aging and AD/ADRD science. Our findings suggest that the ways sex and gender are being measured and characterized in research cohorts are impeding what researchers can understand about the influences of these factors on aging and AD/ADRD pathways and outcomes. To achieve the ambitious national goal of understanding the influences of gender and biologic sex on risk, development, progression, diagnosis, and clinical presentation of AD/ADRD, scientists may need to expand how sex and gender are considered in AD/ADRD research. Development and routine use of social, behavioral, and biologic markers of sex and gender may help characterize and quantify sex-based biological influences and cultural and historical effects of gender.
Results of our study highlight the need for foundational data sources to design and document their materials to support scientific rigor (Carter et al., 2012; Nebel et al., 2018; Snyder et al., 2016) and align with available guidance for how to report sex and gender in publications (Ferretti et al., 2020; Heidari et al., 2016). We found that few aging and AD/ADRD cohorts adequately measured and defined sex/gender. This highlights the need for reconsidering the ways in which sex and gender are currently measured in AD/ADRD and aging health research. Given that health disparities can be attributed to sex and gender differences across the life course, establishing guidelines for researchers on how to incorporate measures of sex and gender in aging and AD/ADRD health research are greatly needed to advance health equity and inclusion of sex and gender diverse people in research.
Supplementary Material
{kind=link}
Acknowledgments
The authors wish to thank Andrew Peterson, PhD, Emily Largent, PhD, Jason Karlawish, MD, and Terry Casey. The conducted research was not preregistered with an analysis plan in an independent, institutional registry. The data, analytic methods and materials may be made available to other researchers. Interested researchers are asked to contact the corresponding author with inquires.
Contributor Information
Shana D Stites, Department of Psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Hannah Cao, School of Social Policy and Practice, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Kristin Harkins, Department of Medicine, Division of Geriatric Medicine, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Jason D Flatt, Social and Behavioral Health Program, School of Public Health, University of Nevada, Las Vegas, Las Vegas, Nevada, USA.
Funding
This work was supported by the Research Centers Collaborative Network (RCCN) of the National Institute on Aging (NIA) (U24AG058556). Dr. Stites is supported by the Alzheimer’s Association (AARF-17-528934) and the NIA (K23AG065442). Dr. Flatt is supported by the NIA (K01AG056669). The funders had no role in the design and conduct of the study; collection, management, analysis, or interpretation of the data; preparation or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of Interest
None declared.
Human Participant Protection
The Institutional Review Board of the University of Pennsylvania approved all procedures involving human subjects.
References
- Ainsworth, C. (2018). Sex redefined: The idea of 2 sexes is overly simplistic. Scientific American. https://www.scientificamerican.com/article/sex-redefined-the-idea-of-2-sexes-is-overly-simplistic1/ [Google Scholar]
- Alex, L., Fjellman Wiklund, A., Lundman, B., Christianson, M., & Hammarström, A. (2012). Beyond a dichotomous view of the concepts of ‘sex’ and ‘gender’ focus group discussions among gender researchers at a medical faculty. PLoS One, 7(11), e50275. doi: 10.1371/journal.pone.0050275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychological Association . (2012). Guidelines for psychological practice with lesbian, gay, and bisexual clients. American Psychologist, 67(1), 10–42. doi: 10.1037/a0024659 [DOI] [PubMed] [Google Scholar]
- American Psychological Association . (2015). Guidelines for psychological practice with transgender and gender nonconforming people. American Psychologist, 70(9), 832–864. doi: 10.1037/a0039906 [DOI] [PubMed] [Google Scholar]
- Armstrong, N. M., Huang, C.-W., Williams, O. A., Bilgel, M., An, Y., Doshi, J., Erus, G., Davatzikos, C., Wong, D. F., Ferrucci, L., & Resnick, S. M. (2019). Sex differences in the association between amyloid and longitudinal brain volume change in cognitively normal older adults. NeuroImage: Clinical, 22, 101769. doi: 10.1016/j.nicl.2019.101769 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bajic, V. P., Essack, M., Zivkovic, L., Stewart, A., Zafirovic, S., Bajic, V. B., Gojobori, T., Isenovic, E., & Spremo-Potparevic, B. (2020). The X files: “The mystery of X chromosome instability in Alzheimer’s disease”. Frontiers in Genetics, 10, 1368. doi: 10.3389/fgene.2019.01368 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barrett, C., Crameri, P., Lambourne, S., Latham, J. R., & Whyte, C. (2015). Understanding the experiences and needs of lesbian, gay, bisexual and trans Australians living with dementia, and their partners. Australasian Journal on Ageing, 34, 34–38. doi: 10.1111/ajag.12271 [DOI] [PubMed] [Google Scholar]
- Cameron, J. J., & Stinson, D. A. (2019). Gender (mis)measurement: Guidelines for respecting gender diversity in psychological research. Social and Personality Psychology Compass, 13(11), 1–14. doi: 10.1111/spc3.12506 [DOI] [Google Scholar]
- Carter, C. L., Resnick, E. M., Mallampalli, M., & Kalbarczyk, A. (2012). Sex and gender differences in Alzheimer’s disease: Recommendations for future research. Journal of Women’s Health (2002), 21(10), 1018–1023. doi: 10.1089/jwh.2012.3789 [DOI] [PubMed] [Google Scholar]
- Clayton, J. A., & Tannenbaum, C. (2016). Reporting sex, gender, or both in clinical research? Journal of American Medical Association, 316(18), 1863. doi: 10.1001/jama.2016.16405 [DOI] [PubMed] [Google Scholar]
- Dillman, D. A., Smyth, J. D., & Christian, L. M. (2014). Internet, phone, mail, and mixed-mode surveys: The tailored design method. John Wiley & Sons. [Google Scholar]
- Dressel, P., Minkler, M., & Yen, I. (1997). Gender, race, class, and aging: Advances and opportunities. International Journal of Health Services: Planning, Administration, Evaluation, 27(4), 579–600. doi: 10.2190/7XAY-PYBN-AA5L-3DRC [DOI] [PubMed] [Google Scholar]
- Evans-Campbell, T., Fredriksen-Goldsen, K. I., Walters, K. L., & Stately, A. (2007). Caregiving experiences among American Indian two-spirit men and women: Contemporary and historical roles. Journal of Gay & Lesbian Social Services, 18(3–4), 75–92. doi: 10.1300/J041v18n03_05 [DOI] [Google Scholar]
- Ferretti, M. T., Martinkova, J., Biskup, E., Benke, T., Gialdini, G., Nedelska, Z., Rauen, K., Mantua, V., Religa, D., Hort, J., Santuccione Chadha, A., & Schmidt, R. (2020). Sex and gender differences in Alzheimer’s disease: Current challenges and implications for clinical practice: Position paper of the dementia and cognitive disorders panel of the European Academy of Neurology. European Journal of Neurology, 27(6), 928–943. doi: 10.1111/ene.14174 [DOI] [PubMed] [Google Scholar]
- Flatt, J. D., Johnson, J. K., Karpiak, S. E., Seidel, L., Larson, B., & Brennan-Ing, M. (2018). Correlates of subjective cognitive decline in lesbian, gay, bisexual, and transgender older adults. Journal of Alzheimer’s Disease, 64(1), 91–102. doi: 10.3233/JAD-171061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fonseca, X., Lukosch, S., & Brazier, F. (2019). Social cohesion revisited: A new definition and how to characterize it. Innovation: The European Journal of Social Science Research, 32(2), 231–253. doi: 10.1080/13511610.2018.1497480 [DOI] [Google Scholar]
- Fox, H. E., White, S. A., Kao, M. H., & Fernald, R. D. (1997). Stress and dominance in a social fish. The Journal of Neuroscience, 17(16), 6463–6469. doi: 10.1523/JNEUROSCI.17-16-06463.1997 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heidari, S., Babor, T. F., De Castro, P., Tort, S., & Curno, M. (2016). Sex and gender equity in research: Rationale for the SAGER guidelines and recommended use. Research Integrity and Peer Review, 1, 2. doi: 10.1186/s41073-016-0007-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill, C. V., Pérez-Stable, E. J., Anderson, N. A., & Bernard, M. A. (2015). The National Institute on Aging health disparities research framework. Ethnicity & Disease, 25(3), 245–254. doi: 10.18865/ed.25.3.245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- History of Women’s Participation in Clinical Research | Office of Research on Women’s Health . (n.d.). Office of Research on Women’s Health. https://orwh.od.nih.gov/toolkit/recruitment/history
- Hormone Replacement Therapy Variable Details | RADC . (n.d.). RADC Research Resource Sharing Hub. https://www.radc.rush.edu/docs/var/detail.htm?category=Female+Reproductive+History&subcategory=Hormone+replacement+therapy&variable=hormones
- Hurst, L. D., & Peck, J. R. (1996). Recent advances in understanding of the evolution and maintenance of sex. Trends in Ecology & Evolution, 11(2), 46–52. doi: 10.1016/0169-5347(96)81041-x [DOI] [PubMed] [Google Scholar]
- Iervolino, A. C., Hines, M., Golombok, S. E., Rust, J., & Plomin, R. (2005). Genetic and environmental influences on sex-typed behavior during the preschool years. Child Development, 76(4), 826–840. doi: 10.1111/j.1467-8624.2005.00880.x [DOI] [PubMed] [Google Scholar]
- Including Women and Minorities in Clinical Research Background | Office of Research on Women’s Health . (2001). Office of Research on Women’s Health National Institutes of Health. https://orwh.od.nih.gov/research/clinical-research-trials/nih-inclusion-policy/including-women-and-minorities-clinical
- Institute of Medicine (US) Committee on Understanding the Biology of Sex and Gender Differences . (2001). Exploring the biological contributions to human health: Does sex matter? National Academies Press (US), 1–10. doi: 10.17226/10028 [DOI] [PubMed] [Google Scholar]
- International Alzheimer’s and Related Dementias Research Portfolio . (2020, December 15). Category D. Population studies—List of cohorts and studies.https://iadrp.nia.nih.gov/about/cadro/Population-Studies-Cohorts-and-Studies
- Jack, C. R., Bennett, D. A., Blennow, K., Carrillo, M. C., Feldman, H. H., Frisoni, G. B., Hampel, H., Jagust, W. J., Johnson, K. A., Knopman, D. S., Petersen, R. C., Scheltens, P., Sperling, R. A., & Dubois, B. (2016). A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology, 87(5), 539–547. doi: 10.1212/WNL.0000000000002923 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jäncke, L. (2018). Sex/gender differences in cognition, neurophysiology, and neuroanatomy. F1000Research, 7. doi: 10.12688/f1000research.13917.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallinson, D. J., & Hatemi, P. K. (2018). The effects of information and social conformity on opinion change. PLoS One, 13(5), e0196600. doi: 10.1371/journal.pone.0196600 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McEwen, B. S. (2020). Hormones and behavior and the integration of brain–body science. Hormones and Behavior, 119, 104619. doi: 10.1016/j.yhbeh.2019.104619 [DOI] [PubMed] [Google Scholar]
- Meyer-Bahlburg, H. F. (1984). Psychoendocrine research on sexual orientation. Current status and future options. Progress in Brain Research, 61, 375–398. doi: 10.1016/S0079-6123(08)64448-9 [DOI] [PubMed] [Google Scholar]
- Mielke, M. M., Vemuri, P., & Rocca, W. A. (2014). Clinical epidemiology of Alzheimer’s disease: Assessing sex and gender differences. Clinical Epidemiology, 6, 37–48. doi: 10.2147/CLEP.S37929 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milestone 2.D. (n.d.). National Institute on Aging. http://www.nia.nih.gov/research/milestones/disease-mechanisms/milestone-2-d [Google Scholar]
- Montañez, A. (2017). Beyond XX and XY. Scientific American, 317(3), 50–51. doi: 10.1038/scientificamerican0917-50 [DOI] [PubMed] [Google Scholar]
- National Alzheimer’s Coordinating Center (NACC) . (n.d.). National Institute on Aging. http://www.nia.nih.gov/research/dn/national-alzheimers-coordinating-center-nacc [Google Scholar]
- National Institutes of Health . (2021). Strategic plan to advance research on the health and well-being of sexual & gender minorities (p. 19). https://dpcpsi.nih.gov/sites/default/files/SGMStrategicPlan_2021_2025.pdf
- Nebel, R. A., Aggarwal, N. T., Barnes, L. L., Gallagher, A., Goldstein, J. M., Kantarci, K., Mallampalli, M. P., Mormino, E. C., Scott, L., Yu, W. H., Maki, P. M., & Mielke, M. M. (2018). Understanding the impact of sex and gender in Alzheimer’s disease: A call to action. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, 14(9), 1171–1183. doi: 10.1016/j.jalz.2018.04.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- NIH-National Institute of Aging . (n.d.). Alzheimer’s disease research centers. National Institute on Aging. http://www.nia.nih.gov/health/alzheimers-disease-research-centers [Google Scholar]
- NOT-AG-20-038: Notice of Special Interest: Sex and Gender Differences in Alzheimers Disease and Alzheimers Disease-Related Dementias (AD/ADRD) . (n.d.). https://grants.nih.gov/grants/guide/notice-files/NOT-AG-20-038.html
- Rosenwohl-Mack, A., Tamar-Mattis, S., Baratz, A. B., Dalke, K. B., Ittelson, A., Zieselman, K., & Flatt, J. D. (2020). A national study on the physical and mental health of intersex adults in the U.S. PLoS One, 15(10), e0240088. doi: 10.1371/journal.pone.0240088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruble, D. N., Martin, C. L., & Berenbaum, S. A. (2006). Gender development. In Eisenberg, N., Damon, W., Lerner, R. M. (Eds.), Handbook of child psychology: Social, emotional, and personality development (Vol. 3, 6th ed., pp. 858–932). John Wiley & Sons, Inc. [Google Scholar]
- Snyder, H. M., Asthana, S., Bain, L., Brinton, R., Craft, S., Dubal, D. B., Espeland, M. A., Gatz, M., Mielke, M. M., Raber, J., Rapp, P. R., Yaffe, K., & Carrillo, M. C. (2016). Sex biology contributions to vulnerability to Alzheimer’s disease: A think tank convened by the Women’s Alzheimer’s Research Initiative. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, 12(11), 1186–1196. doi: 10.1016/j.jalz.2016.08.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tal, E. (2013). Old and new problems in philosophy of measurement: Old and new problems in philosophy of measurement. Philosophy Compass, 8(12), 1159–1173. doi: 10.1111/phc3.12089 [DOI] [Google Scholar]
- Thompson, K., Peters, S., Woodward, M., Carcel, C., & Norton, R. (2019). Reporting sex and gender in medical research. Lancet (London, England), 393(10185), 2038. doi: 10.1016/S0140-6736(19)31041-4 [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau . (n.d.). Census regions and divisions of the United States. US Census Bureau. [Google Scholar]
- Zhao, R. F., & Scholar, P. D. N. M. D. (2019, February 26). The Y chromosome: Beyond gender determination. National Human Genome Research Institute (NHGRI). https://www.genome.gov/27557513/the-y-chromosome-beyond-gender-determination/ [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.