

Abstract
Introduction
While studies have investigated influences on graduate practice locations of other health professionals, especially medicine, none have investigated practice locations of medical radiation science (MRS) graduates. This study aimed to explore factors influencing the registered principal place of practice (PPP) of diagnostic radiography, radiation therapy and nuclear medicine graduates from the University of Newcastle (UON), Australia, in their second post‐graduate year.
Methods
Data were extracted from the UON enrolment and clinical placement databases and linked to Australian Health Practitioners Regulation Agency (Ahpra) registration data for PPP location in 2019 for 187 graduates who completed their studies in 2017. Explanatory variables included age at enrolment, gender, MRS discipline, location of origin, socio‐economic index for location of origin, and locations and duration of undergraduate professional placements. Descriptive statistics, tests of association and logistic regression compared rural and non‐rural origin, and professional placement locations with Ahpra PPP.
Results
Factors related to non‐metropolitan PPP were location of origin (P = 0.002), number (P = 0.002) and duration (P = 0.007) of rural placements, and MRS discipline (P = 0.033). Controlling for other variables, location of origin and MRS discipline remained significant. Graduates of rural origin had up to 3.54 (95%CI = 1.51–8.28) times the odds of a rural PPP. Diagnostic radiography graduates had up to 5.46 (95%CI = 1.55–19.20) times the odds of nuclear medicine of a rural PPP.
Conclusion
To help reduce the gap between rural and metropolitan medical radiation service availability, there is a need for targeted recruitment of rural origin students. Further investigation of the effect of rural undergraduate MRS placements is justified.
Keywords: health workforce, medical radiation science, professional practice location, rural health, student placement
Some allied health studies identified rural origin and rural placements as influential on graduate rural practice location. This study explores the impact of such factors on MRS graduates. Data was extracted from University enrolment and clinical placement databases and linked to Australian Health Practitioners Regulation Agency (Ahpra) registration data for principal place of practice (PPP) location in 2019 for 187 graduates who completed their studies in 2017.

Introduction
The Australian health workforce is geographically maldistributed, with fewer allied health professionals, including medical radiation science (MRS) practitioners, in rural locations compared to major cities. 1 , 2 , 3 , 4 , 5 ‘Rural’ areas are classified according to their size, distance from major cities and access to services into categories that include inner and outer regional through to remote and very remote. 6 , 7 Typically, those locations have smaller populations, restricted access to healthcare, a higher proportion of Aboriginal and Torres Strait Islander people, and relatively poorer health outcomes compared to major cities, including higher rates of preventable diseases and a shorter life expectancy. 2 , 4 , 6 Rural areas characteristically have difficulty attracting and retaining health professionals, with metropolitan practice perceived to be more socially and professional desirable, with better career options. 2 , 3
Geographical health workforce distribution is well documented, 2 , 6 , 8 , 9 including all three MRS disciplines, diagnostic radiography, nuclear medicine and radiation therapy. In 2019, with a total of 14,865 registered MRS practitioners, there were 58.9 per 100,000 population in Australian major cities, 65.9 in large rural towns, 32.2 in medium rural towns, 8.0 in small rural towns, and 24.6 and 14.8 in remote and very remote communities. 5 Between 2013 and 2018, the total Australian allied health workforce increased by 21.7%, from 98,545 to 119,914. 10 In that same period, the ratio of total allied health practitioners employed in major cities compared to all other locational categories fell from 1.124 to 1.028. That decrease is encouraging, indicating a shift in allied health workforce as a whole towards rural practice. The MRS workforce trend was less encouraging for the period from 2015 to 2019, during which the number of practitioners grew by 15.9% and the ratio of major city practitioners to those employed in other, non‐metropolitan locations decreased only marginally, from 7.499 to 7.455. 5
By comparison with the overall allied health workforce, the majority of the MRS workforce practices in major cities. In 2019, 88.1% of MRS practitioners were employed in metropolitan and large regional centres. The proportion of metropolitan‐based practitioners varies across the MRS disciplines, being 86.9% in diagnostic radiography, compared to 92.1% and 91.7% in nuclear medicine and radiation therapy, respectively. 5 There is only a small proportion of nuclear medicine and radiation therapy professionals working in rural locations and none in remote and very remote areas. 5 This variation is to be expected given differences the nature of practice and types of specialised imaging and treatment equipment used across the three disciplines. While diagnostic radiography is performed even in many small rural hospitals on fixed and mobile general radiographic equipment, radiation therapy, for example, requires linear accelerators, as well as multimodality medical imaging and multidisciplinary oncology teams. Radiation therapy, therefore, is performed mainly in major metropolitan hospitals, although regional cancer care facilities, with radiation oncology and employing radiation therapists, are located in some regional population centres. 11
No studies have investigated factors that influence the practice locations of MRS graduates; however, previous research has investigated factors that influence where graduates in other disciplines choose to practice and why, most studies targeting medical graduates. 1 , 2 Several studies have identified key influences on why health professionals might choose rural practice, including social, environmental, financial, personal and professional factors. 1 , 2 , 3 , 4 , 8 , 9 , 12 , 13 , 14 The two factors identified as most influential are rural background and rural placement experiences. 1 , 3 , 9 , 15 Reportedly, having a rural background approximately triples the odds of allied health graduates choosing to practice in a rural location, 13 with graduates most likely to return to their hometown or one of similar size or location. 8 , 14 , 16
Positive rural placement experiences have been shown to be beneficial in encouraging rural practice by introducing students to working and living in rural settings. 2 , 13 Previous research is contradictory regarding the optimally influential placement duration, however. Some studies have suggested longer, more frequent rural placements are positively associated with rural practice, 9 , 16 , 17 whereas Playford et al. 13 suggested that longer placements may be counterproductive, with duration of less than five weeks being optimum. That finding was associated with consequent loss of income from part‐time work, social dislocation and separation from family and friends. 13
Given the dearth of MRS‐specific research in this field, the aim of this study was to explore factors associated with graduate principal place of practice (PPP), as recorded in the Australian Health Practitioner Regulation Agency (Ahpra), of MRS graduates from the University of Newcastle (UON), Australia, in their second post‐graduate year. Specific explanatory variables included the following: student’s age at initial enrolment; gender; MRS discipline; background location of origin; relative socio‐economic index for location of origin; and location, frequency and duration of undergraduate professional placements.
Methods
This study arises from the overarching Nursing and Allied Health Graduate Outcome Tracking (NAHGOT) study,18 a prospective longitudinal cohort study involving several Australian universities and multiple disciplines. That study aims to strengthen evidence for factors influencing nursing and allied health rural workforce recruitment and retention, using a large sample size over a 10‐year period. As in the NAHGOT study, this MRS‐specific sub‐study uses student enrolment and professional placement data to explore the association with graduates’ PPP.
Participants
The target population for this study includes graduates who completed a three‐year Bachelor of MRS degree in 2017 at UON in either diagnostic radiography, nuclear medicine or radiation therapy. Students elect their MRS discipline of choice when submitting their University Admission Centre application for undergraduate entry and, if successful, enrol in a course of study in their chosen discipline. In order to establish an Australian location of origin and PPP, participants had to be domestic students who registered with Ahpra after graduating, thus excluding international students and graduates who did not register.
Data sources and collection
Data were extracted from existing databases. Data from the UON enrolment database (NUSTAR; ServiceUON, UON, NSW) included course of study, commencement and completion dates, gender, date of birth, hometown address and citizenship. Age at first enrolment was dichotomised into <21 and ≥21 years, the latter being the ‘mature‐age’ admission criterion. Undergraduate professional placement data were extracted from the UON’s placement database (SONIA online; QSR International, Burlington, MA), including the location of placements, whether a public hospital or private practice placement, and dates of all placements in 2015, 2016 and 2017. Under a data use and confidentiality agreement, graduates’ PPP was accessed from Ahpra as at September 2019, the year following the graduates’ professional development year and completion of their supervised practice program (SPP).
Data were checked manually for duplicates and missing entries. Location of origin was determined from subjects’ recorded hometown postcode when they first enrolled at UON, which was compared to Australian Bureau of Statistics data to determine the Australian Statistical Geographical Standard‐Remoteness Area (ASGS‐RA) classification category 6 and Socio‐Economic Indexes for Areas, Index of Relative Socio‐economic Disadvantage (SEIFA‐IRSD). 19 The ASGS‐RA classifications range from one to five, with RA1 being major cities and RA2‐5 being regional, rural, remote and very remote. 6 The SEIFA‐IRSD ranges from 1, most socio‐economically disadvantaged, to 10, most advantaged locations. 19 Clinical placement locations and PPP locations were also categorised using the ASGS‐RA classification, and duration of each placement was determined from recorded dates. Since each student had multiple undergraduate placements, cumulative placement days were derived across their entire degree, as either major city (RA1) or rural (RA2‐5, inclusive).
Statistical methods
Descriptive and inferential statistical analyses used Statistical Package for Social Science (SPSS; IBM Australia, Sydney) and Statistical Analysis Software (SAS, version 14.1; SAS Institute Inc., Lane Cove, NSW, Australia), PPP being the key outcome variable. Chi‐square (χ2) tests for independence, Wilcoxon rank‐sum tests and logistic regression were performed to determine associations of explanatory variables with PPP. Associations were considered significant when P < 0.05.
For multiple logistic regression, all variables with P < 0.25 were initially included, along with possible interaction terms. Using iterative stepwise backwards elimination, 20 nonsignificant interactions were sequentially removed. Nonsignificant effects were retained if involved in significant interactions or if found to be nonsignificant confounders whose removal would have altered parameter estimates by more than 10%. Odds ratios with 95% confidence intervals were calculated. Separate models were generated for categories of ‘number of rural placements’ and ‘cumulative rural placement days’, which were used as alternative proxy measures of undergraduate rural exposure.
Ethics approval
Ethics clearance was from the UON Human Research Ethics Committee under a variation of the NAHGOT study protocol (Reference: H‐2017‐0332; 5th June 2020). Data sources were linked using a unique identifier generated from student identification numbers. Enrolment, graduation and placement data were extracted by administrative staff and de‐identified prior to access by the researchers, thus ensuring confidentiality.
Results
The UON MRS student cohort that completed in 2017 consisted of 187 students. Twenty‐three (12.3%) did not meet inclusion criteria, either because they were international students (n = 1) or had not registered with Ahpra by September 2019 (n = 22). There were no significant differences for gender, rural origin, SEIFA‐IRSD or MRS discipline studied between those included and excluded, though those excluded were generally older (P = 0.002) and less likely to have had at least one rural placement (P = 0.003). The final sample size was 164 (87.7%) graduates, with a combined total of 805 placements having been undertaken between 2015 and 2017.
Demographics and descriptive data
Table 1 shows the breakdown of variables according to the disciplines in which students were enrolled. Chosen MRS discipline showed an association with gender (χ2, P < 0.01), number of rural placements (P < 0.001), cumulative rural placement days (P < 0.001) and PPP location (P < 0.05). Categorical age, location of origin and hometown SEIFA‐IRDS score showed no association with MRS discipline.
Table 1.
Demographic factors, undergraduate placements and postgraduate principal place of practice for University of Newcastle Medical Radiation Science 2017 graduates
| Variables | Total (%) | DR (%) | NM (%) | RT (%) |
|---|---|---|---|---|
| Total participants | 164 | 84 (51.2) | 40 (24.4) | 40 (24.4) |
| Gender* | ||||
| Male | 52 (31.7) | 25 (29.8) | 20 (50.0) | 7 (17.5) |
| Female | 112 (68.3) | 59 (70.2) | 20 (50.0) | 33 (82.5) |
| Age at commencement | ||||
| <21 years | 122 (74.4) | 57 (67.9) | 31 (77.5) | 34 (85.0) |
| 21+ years (mature age) | 42 (25.6) | 27 (32.1) | 9 (22.5) | 6 (15.0) |
| Mean years (95% CI) | 20.6 (19.9–21.3) | 21.3 (20.1–22.4) | 20.5 (19.1–21.9) | 19.2 (18.6–19.8) |
| Location of origin 1 | ||||
| Major city | 115 (70.1) | 60 (71.4) | 24 (60.0) | 31 (77.5) |
| Inner regional | 42 (25.6) | 21 (25.0) | 13 (32.5) | 8 (20.0) |
| Outer regional | 7 (4.3) | 3 (3.6) | 3 (7.5) | 1 (2.5) |
| Remote/very remote | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| SEIFA‐IRDS 2 | ||||
| Most disadvantaged | 31 (18.9) | 11 (13.1) | 11 (27.5) | 9 (22.5) |
| Least disadvantaged | 133 (81.1) | 73 (86.9) | 29 (72.5) | 31 (77.5) |
| Cumulative days of rural placement* | ||||
| 0 days | 32 (19.5) | 2 (2.4) | 12 (30.0) | 18 (45.0) |
| 1–25 days | 62 (37.8) | 38 (45.2) | 17 (42.5) | 7 (17.5) |
| 26–50 days | 48 (29.3) | 30 (35.7) | 11 (27.5) | 7 (17.5) |
| 51+ days | 22 (13.4) | 14 (16.7) | 0 (0) | 8 (20.0) |
| Number of rural placements* | ||||
| 0 rural placements | 32 (19.5) | 2 (2.4) | 12 (30.0) | 18 (45.0) |
| 1 rural placement | 62 (37.8) | 38 (45.2) | 17 (42.5) | 7 (17.5) |
| 2+ rural placements | 70 (42.7) | 44 (52.4) | 11 (27.5) | 15 (37.5) |
| Principle place of practice 1 ,** | ||||
| Major city | 121 (73.8) | 56 (66.7) | 36 (90.0) | 29 (72.5) |
| Inner regional | 28 (17.1) | 15 (17.9) | 4 (10.0) | 9 (22.5) |
| Outer regional | 14 (8.5) | 12 (14.3) | 0 (0) | 2 (5.0) |
| Remote/very remote | 1 (1.6) | 1 (1.2) | 0 (0) | 0 (0) |
DR, diagnostic radiography students; NM, nuclear medicine students; RT, radiation therapy students.
*Chi‐square test (χ 2 ) = P < 0.01 between disciplines, DR, NM & RT; **Chi‐square test (χ 2 ) = P < 0.05 between disciplines for major cities (RA1) vs rural (RA2‐RA5 combined).
Australian Statistical Geography Standard‐Remoteness Area (ASGS‐RA): RA1 = major city; RA2 = inner regional; RA3 = outer regional; RA4 = remote; RA5 = very remote. 6
Socio‐Economic Indexes for Areas (SEIFA) Index for Relative Socio‐economic Disadvantage (IRDS): Most disadvantaged = 1–2; Least disadvantaged = 3–10. 20
The majority of graduates originated from major cities (n = 115, 70.1%), with 49 (29.9%) originally from regional or rural areas. None were from remote/very remote locations. Nuclear medicine had the largest proportion of rural origin graduates and radiation therapy the least, while 18.9% were from locations classified as socio‐economically disadvantaged. Most professional placements (71.2%) were in major cities (Table 2), while thirty‐two students (19.5%) did no rural placements, as shown in Table 1.
Table 2.
Location and number of undergraduate placements undertaken by the University of Newcastle Medical Radiation Science 2017 graduates across the entirety of their degree from 2015 to 2017
| Placement location 1 | Total (%) | DR (%) | NM (%) | RT (%) |
|---|---|---|---|---|
| Total | 805 (100) | 414 (100) | 196 (100) | 195 (100) |
| Major city | 573 (71.2) | 271 (65.5) | 154 (78.6) | 148 (75.9) |
| Inner regional | 190 (23.6) | 118 (28.5) | 30 (15.3) | 42 (21.5) |
| Outer regional | 36 (4.5) | 22 (5.3) | 9 (4.5) | 5 (2.6) |
| Remote/very remote | 2 (0.2) | 2 (0.5) | 0 | 0 |
| Not available 2 | 4 (0.5) | 1 (0.2) | 3 (1.5) | 0 |
DR, diagnostic radiography students; NM, nuclear medicine students; RT, radiation therapy students.
Australian Statistical Geography Standard‐Remoteness Area (ASGS‐RA): RA1 = major city; RA2 = inner regional; RA3 = outer regional; RA4 = remote; RA5 = very remote. 6
ASGS‐RA was not available as a rural or major city status was not able to be determined from the agency name.
Principal place of practice
Of the total sample, 43 (26.2%) had a rural PPP and 121 (73.8%) were practicing in major cities in their second year after course completion (Table 1). Nuclear medicine had the highest percentage of graduates working in major cities (n = 36, 90%).
In Table 3, approximately half those working in a rural area were of rural origin (48.8%), whereas only a quarter of those working in a major city were of rural origin (23.1%) (χ2, P = 0.002). Figure 1 shows the distribution of students’ locations of origin and graduates’ PPPs across ASGS‐RA categories, showing a small overall shift away from RA2‐5 towards RA1 locations. In univariate analysis, there was also the suggestion of an association between rural PPP and undertaking rural placements, both for the number of rural placements (χ2, P = 0.002) and cumulative rural placement days (χ2, P = 0.007). Graduates who had a rural PPP had spent a median of 50 days on rural placements, higher than graduates with a major city PPP, who spent a median of 25 days on rural placements (Wilcoxon, P = 0.002). The association between MRS discipline and PPP described in the introduction of this article was also evident (χ2, P = 0.022).
Table 3.
Associations between demographic variables and rural undergraduate placement variables with principal place of practice of University of Newcastle Medical Radiation Science 2017 graduates
| Variable | Principal place of practice (%) | P value | |
|---|---|---|---|
| Rural 1 | Major cities 1 | ||
| Gender | |||
| Female | 27 (62.8) | 85 (70.2) | 0.367* |
| Male | 16 (37.2) | 36 (29.8) | |
| Age | |||
| <21 years | 33 (76.7) | 89 (73.6) | 0.681* |
| 21+ years | 10 (23.3) | 32 (26.4) | |
| Discipline | |||
| Diagnostic radiography | 28 (65.1) | 56 (46.2) | 0.022* |
| Nuclear medicine | 4 (9.3) | 36 (29.8) | |
| Radiation therapy | 11 (25.6) | 29 (24.0) | |
| Location of origin 1 | |||
| Major city (RA1) | 22 (51.2) | 93 (76.9) | 0.002* |
| Rural (RA2‐5) | 21 (48.8) | 28 (23.1) | |
| SEIFA‐IRDS 2 | |||
| Most disadvantaged | 7 (16.3) | 24 (19.8) | 0.609* |
| Least disadvantaged | 36 (83.7) | 97 (80.2) | |
| Cumulative days of rural placement | |||
| 0 days | 6 (14.0) | 26 (21.5) | 0.007* |
| 1–25 days | 9 (20.9) | 53 (43.8) | |
| 26–50 days | 19 (44.2) | 29 (24.0) | |
| 51+ days | 9 (20.9) | 13 (10.7) | |
| Median days (IQR) | 50 (25–50) | 25 (10–40) | 0.002** |
| Number of rural placements | |||
| 0 rural placements | 6 (14.0) | 26 (21.5) | 0.002* |
| 1 rural placements | 9 (20.9) | 53 (43.8) | |
| 2+ rural placements | 28 (65.1) | 42 (34.7) | |
*Chi square test for independence; **Wilcoxon rank‐sum test.
IQR, Interquartile range.
Australian Statistical Geography Standard‐Remoteness Area (ASGS‐RA): ‘Major cities = ASGC‐RA1. ‘Rural’ refers to ASGC‐RA categories 2–5. 6
Socio‐Economic Indexes for Areas (SEIFA) Index for Relative Socio‐economic Disadvantage (IRDS): most disadvantaged = 1–2; least disadvantaged = 3–10. 20
Figure 1.
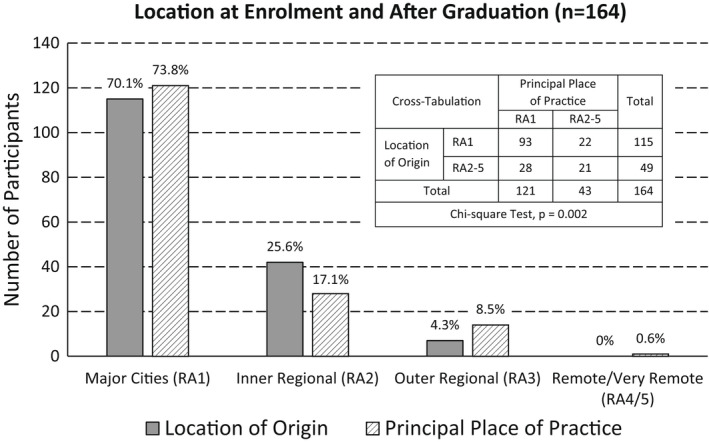
Number of University of Newcastle MRS 2017 graduates with their location of origin compared to graduate principal place of practice using the Australian Statistical Geographical Standard ‐ Remoteness Area. 6
In Table 4, before controlling for other variables, univariate regression analysis found that rural background, MRS discipline, number of rural placements and cumulative rural placement days were all significantly associated with graduates’ PPP. When controlling for other variables, only MRS discipline and location of origin remained significantly associated with rural PPP. In multivariable model 1, with categorical ‘number of rural placements’ as the measure of rural exposure, graduates from a rural background had more than three times greater odds of working in a rural location compared to those from major cities (P = 0.005; OR = 3.28, 95%CI = 1.43–7.53). Compared to nuclear medicine graduates, the odds of working in a rural location were greater for both diagnostic radiography (P = 0.007; OR = 5.47, 95%CI = 1.58–18.95) and radiation therapy (P = 0.046; OR = 3.88, 95%CI = 1.03–14.65). ‘Number of rural placements’ was no longer significant (P = 0.083) but was retained as a confounder between rural origin, discipline and PPP, improving the model fit. In multivariable model 2, the alternative measure of rural exposure, ‘cumulative rural placement days’, was a non‐significant confounder, with similar odds ratios to model 1 for both location and discipline (Table 4).
Table 4.
Binary logistic regression for ‘Principal place of practice in a rural location’, for medical radiation science graduates that completed studies at the University of Newcastle in 2017
| Variables in regression models: ‘Principal place of practice in a rural location’ 1 | Univariate models (unadjusted) | Multivariable model 1 (adjusted) 4 , 9 | Multivariable model 2 (adjusted) 4 , 9 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P value | Odds ratio | Lower 95% CI | Upper 95% CI | P value | Odds ratio | Lower 95% CI | Upper 95% CI | P value | Odds ratio | Lower 95% CI | Upper 95% CI | |
| Location of origin: Rural versus major cities 2 , 3 | 0.002 | 3.17 | 1.53 | 6.60 | 0.005 | 3.28 | 1.43 | 7.53 | 0.005 | 3.31 | 1.44 | 7.63 |
| Discipline versus nuclear medicine 3 | 0.033 | 0.027 | 0.025 | |||||||||
| Diagnostic radiography | 0.009 | 4.50 | 1.46 | 13.91 | 0.007 | 5.47 | 1.58 | 18.95 | 0.007 | 5.66 | 1.62 | 19.84 |
| Radiation therapy | 0.053 | 3.41 | 0.98 | 11.85 | 0.046 | 3.88 | 1.03 | 14.65 | 0.042 | 4.12 | 1.06 | 16.10 |
| Number of rural placements 9 versus zero rural placements 3 | 0.003 | 0.083 | ||||||||||
| One rural placement | 0.596 | 0.74 | 0.24 | 2.29 | 0.290 | 0.49 | 0.13 | 1.84 | – | – | – | |
| ≥ two rural placements | 0.001 | 2.89 | 1.05 | 7.92 | 0.605 | 1.38 | 0.41 | 4.59 | – | – | – | |
| Rural placement days 9 versus no rural placement days 3 , 6 | 0.009 | 0.159 | ||||||||||
| ≤25 5 | 0.596 | 0.74 | 0.24 | 2.29 | – | – | – | 0.299 | 0.49 | 0.13 | 1.87 | |
| 26–50 7 | 0.054 | 2.84 | 0.98 | 8.19 | – | – | – | 0.532 | 1.50 | 0.42 | 5.33 | |
| >50 8 | 0.080 | 3.00 | 0.88 | 10.25 | – | – | – | 0.824 | 1.17 | 0.29 | 4.81 | |
Variables included in base multivariable model were those with P < 0.25 on univariate analysis.
Australian Standard Geographical Classification‐Remoteness Area (ASGC‐RA). ‘Major cities’ = ASGC‐RA1. ‘Rural’ refers to ASGC‐RA categories 2–5. 6
Reference group.
Odds ratios for each variable in the final model adjusts for the effect of the other remaining variables.
Constitutes 37.8% of the cohort.
19.5% of the cohort.
29.3% of the cohort.
13.4% of the cohort.
Rural placements and rural days categorical variables were considered as alternative measures of rural placement in two separate multivariable models.
Discussion
Among this study cohort, graduates with a rural background were more likely to be practicing in a rural location compared to those of major city origin. The influence of location of origin is well supported by studies of other allied health disciplines. 1 , 2 , 3 , 4 , 9 , 12 , 13 , 16 , 17 , 21 As with other disciplines, to ensure a sustained supply of rural workforce in MRS, there is a need to proactively recruit students from rural areas into universities. It is those students that are most likely to return to rural areas and become the rural practitioners of the future, whether in early post‐graduate years or later in their career.
It was apparent that a greater proportion of the diagnostic radiography graduates in this cohort had entered rural practice compared to either radiation therapy or nuclear medicine graduates, which can be readily explained. In general, more radiographers than radiation therapists or nuclear medicine scientists work in rural locations. 5 The dominant factor is the limited availability and distribution of diagnostic and treatment technologies in rural locations, 22 limiting employment opportunities for MRS graduates in those locations. Diagnostic radiography imaging modalities, such as general radiography and computed tomography, have wider applications and are relatively common in smaller population centres compared to the more specialised nuclear medicine and radiation therapy technologies, which are generally available only in RA1 and RA2 locations. 22 While much has changed in the past two decades with the opening of regional cancer care centres, rural patients still travel long distances to access nuclear medicine and radiation therapy services. 11 It could be debated that to achieve comparable health outcomes to metropolitan populations, there is a need to provide more medical radiation services for rural populations, including nuclear medicine and radiation therapy. This would enhance career pathways for MRS graduates who aspire to rural practice.
In both univariate and multivariate logistic regression, there was a trend of increasing odds that graduates had a rural PPP with both an increase in the number of rural placements and more cumulative days of rural placement. However, there was no apparent effect from a single placement or relatively short rural exposure, the trend only being evident for two or more rural placements totalling at least 25 days. While it is conceded that this is a small study sample and the associations are confounded by MRS discipline and location of origin, the trend cannot be dismissed and further investigation with a larger sample is justified. Early results from the NAHGOT study, including MRS data from two Australian universities, showed that students who had experienced 40 or more rural placement days had 4.54 times greater odds of having a rural PPP two years after graduating. 23 Moreover, similar results have been found in other studies. 9 , 16 , 17 O’Sullivan et al. 17 showed that, compared to no rural immersion, medical students who had a period of rural immersion had more than twice the odds of working in a rural area after graduation.
Opportunities exist to expand and diversify MRS rural placement options, to develop rural immersion programs and to target rural origin students to be given their preferred placement options, considering that they are most likely to become the future rural workforce. Rural origin students may prioritise placement locations close to their home, 21 which, along with pre‐existing rural practice intentions, may be influential on their choice of graduate practice location. 21 Meanwhile, the lack of association between rural PPP and having had a single rural placement or 25 days or less of rural placement time may be explained by students who have no rural practice intentions choosing the shortest possible placement periods to meet the course requirement of doing at least one rural placement. Compelling major city origin students to undertake a single rural placement, as is currently the case, may be socially isolating and financially burdensome, while seemingly yielding limited outcomes in terms of rural health workforce capacity building. 24 It is conceded, however, that rural experience may increase urban origin students’ awareness of rural health care challenges and provide exposure to Indigenous culture.
Strengths and limitations
This study was part of the much larger NAHGOT study, which includes multiple health professions and universities. 18 It lays a methodological foundation for further MRS graduate outcome tracking for up to 10 years following graduation using the NAHGOT protocol. The data linkage method avoids self‐reporting and recall bias associated with survey data collection. 25 Longitudinal tracking of MRS graduates has not previously been performed, but in the longer term, findings for MRS graduates may be compared with different health professions and for different annual cohorts and different universities.
While this study used extensive, complementary statistical methods, the analysis included data for a relatively small sample of one graduate cohort from one university, limiting its generalisability. The cohort was the last to complete the three‐year Bachelor degree program at UON, before it transitioned to the current four‐year degree. There may be differences in practice destinations for graduates of the two different programs, a hypothesis that can be tested in subsequent analyses. Furthermore, limitations of the SONIA professional placement system mean that placement locations may not reflect students’ true preferences. Students request their top five preferences but are not guaranteed a preferred location. More research is needed to explore the influence of placement preferences on graduates’ PPP.
Conclusion
The results of this study shows that recent MRS graduates who enter rural practice are more likely to be of rural origin. In addition, results suggest a relationship between longer rural undergraduate placement experience and rural PPP, although the effect was not apparent when controlling for other variables. The findings provide a basis for future research to inform university enrolments and workforce planning and improve recruitment and retention of MRS professionals in rural locations, thus sustaining workforce supply and improving both access to care and patient health outcomes.
Even if it is their preference, there are some obvious barriers to MRS graduates entering rural practice. This study does not provide insight into the availability of jobs for graduates, which would be expected to be strongly influential on their choice of practice location, especially as early career practitioners. Under the influence of various factors, including job availability, practice location preference may change as their career progresses, hence the need for longitudinal tracking. There is a need to match such findings with reliable, publishable, longitudinal job availability and employment data as part of future MRS workforce planning.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ACKNOWLEDGEMENT
The authors thank the staff of the University of Newcastle Strategy Planning and Performance Unit, the Australian Health Practitioner Regulation Agency and the University of Newcastle Department of Rural Health for their assistance with data acquisition.
J Med Radiat Sci. 69 (2021) 182–190
REFERENCES
- 1. Playford D, Moran MC, Thompson S. Factors associated with rural work for nursing and allied health graduates 15–17 years after an undergraduate rural placement through the University Department of Rural Health program. Rural Remote Health 2020; 20: 5334. [DOI] [PubMed] [Google Scholar]
- 2. Thackrah RD, Thompson SC. Learning from follow‐up of student placements in a remote community: a small qualitative study highlights personal and workforce benefits and opportunities. BMC Med Educ 2019; 19: 331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Wolfgang R, Wakely L, Smith T, Burrows J, Little A, Brown LJ. Immersive placement experiences promote rural intent in allied health students of urban and rural origin. J Multidiscip Healthc 2019; 12: 699–710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Durey A, Haigh M, Katzenellenbogen JM. What role can the rural pipeline play in the recruitment and retention of rural allied health professionals? Rural Remote Health 2015; 15: 3438. [PubMed] [Google Scholar]
- 5. Australian Government Department of Health . Fact Sheet, Allied Health 2019 – Medical Radiation Practitioners. Last updated January 2021. [cited 8 November 2021]. Available from: https://hwd.health.gov.au/resources/publications/factsheet‐alld‐medical‐radiation‐2019.pdf
- 6. Australian Government Department of Health . Australian Statistical Geography Standard‐Remoteness Area, 2019. [updated 2020 Jul 8] [cited 8 November 2021]. Available from: https://www.health.gov.au/health‐workforce/health‐workforce‐classifications/australian‐statistical‐geography‐standard‐remoteness‐area [Google Scholar]
- 7. Australian Institute of Health and Welfare . Rural & Remote Health. AIHW, Canberra, 2019. [cited 8 November 2021]. Available from: https://www.aihw.gov.au/reports/rural‐health/rural‐remote‐health/contents/rural‐health [Google Scholar]
- 8. Brown L, Smith T, Wakely L, Wolfgang R, Little A, Burrows J. Longitudinal tracking of workplace outcomes for undergraduate allied health students undertaking placements in rural Australia. J Allied Health 2017; 46: 79–87. [PubMed] [Google Scholar]
- 9. Jones MP, Bushnell JA, Humphreys JS. Are rural placements positively associated with rural intentions in medical graduates? Med Educ 2014; 48: 405–16. [DOI] [PubMed] [Google Scholar]
- 10. Australian Institute of Health and Welfare . Health Workforce. AIHW, Canberra. 2020. [cited 8 November] Available from: https://www.AIHW.gov.au/reports/australias‐health/health‐workforce [Google Scholar]
- 11. Smith T. A long way from home: Access to cancer care for rural Australians. Radiography 2012; 18: 38–42. [Google Scholar]
- 12. Brown L, Smith T, Wakely L, Little A, Wolfgang R, Burrows J. Preparing Graduates to Meet the Allied Health Workforce Needs in Rural Australia: Short‐Term Outcomes from a Longitudinal Study. Educ Sci 2017; 7: 1–14. [Google Scholar]
- 13. Playford D, Larson A, Wheatland B. Going country: rural student placement factors associated with future rural employment in nursing and allied health. Aust J Rural Health 2006; 14: 14–9. [DOI] [PubMed] [Google Scholar]
- 14. Kumar K, Jones D, Naden K, Roberts C. Rural and remote young people's health career decision making within a health workforce development program: a qualitative exploration. Rural Remote Health 2015; 15: 3303. [PubMed] [Google Scholar]
- 15. Playford D, Ngo H, Gupta S, Puddey IB. Opting for rural practice: the influence of medical student origin, intention and immersion experience. Med J Aust 2017; 207: 154–8. [DOI] [PubMed] [Google Scholar]
- 16. Schofield D, Fletcher S, Fuller J, Birden H, Page S. Where do students in the health professions want to work? Hum Resour Health 2009; 7: 74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. O'Sullivan B, McGrail M, Russell D, et al. Duration and setting of rural immersion during the medical degree relates to rural work outcomes. Med Educ 2018; 52: 803–15. [DOI] [PubMed] [Google Scholar]
- 18. Sutton KP, Beauchamp A, Smith T, et al. Rationale and protocol for the Nursing and Allied Health Graduate Outcomes Tracking (NAHGOT) study: a large‐scale longitudinal investigation of graduate practice destinations. Rural Remote Health 2021; 21: 6407. [DOI] [PubMed] [Google Scholar]
- 19. Australian Bureau of Statistics . Socioeconomic Indexes for Areas (SEIFA), 2016. [cited 8 November 2021]. Available from: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/2033.0.55.001~2016~Main%20Features~IRSD~19
- 20. Kleinbaum DG, Kupper LL, Nizam A, Muller KE. Applied Regression Analysis and Other Multivariable Methods, 4th edn. Brooks/Cole, Pacific Grove, CA, 2008. [Google Scholar]
- 21. Spencer RJ, Cardin AJ, Ranmuthugala G, Somers GT, Solarsh B. Influences on medical students' decisions to study at a rural clinical school. Aust J Rural Health 2008; 16: 262–8. [DOI] [PubMed] [Google Scholar]
- 22. Commonwealth of Australia . Availability and accessibility of diagnostic imaging equipment around Australia. Parliament of Australia, Canberra, 2018: [cited 8 November 2021]. Available from: https://www.aph.gov.au/Parliamentary_Business/Committees/Senate/Community_Affairs/Diagnosticimaging/Report [Google Scholar]
- 23. Sutton K, Depczynski J, Smith T, et al. Destinations of nursing and allied health graduates from two Australian universities: A data linkages study to inform rural placement models. Aust J Rural Health 2021; 29: 191–200. [DOI] [PubMed] [Google Scholar]
- 24. Smith T, Cross M, Waller S, et al. Ruralization of students’ horizons: insights into Australian health professional students’ rural and remote placements. J Multidiscip Healthc 2018; 11: 85–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Althubaiti A. Information bias in health research: definition, pitfalls, and adjustment methods. J Multidiscip Healthc 2016; 9: 211–7. [DOI] [PMC free article] [PubMed] [Google Scholar]