

Abstract
[Purpose] We analyzed the relationship between the degree of asymmetry in the shape of the thorax and postural changes in the frontal plane, and examined the mechanism that creates an asymmetry in the thoracic shape. [Participants and Methods] The participants included 19 healthy young males. We calculated the thoracic volume and lateral deviation from the amount of displacement of reflective markers attached to the thoracic area using the Vicon MX 3D-analysis system. [Results] Left-right differences were shown in each area of the thorax, and positive and negative correlations were found with the amount of lateral deviation of the thorax, which captured postural changes in the frontal plane. [Conclusion] The results of this study suggest that postural changes in the frontal plane are factors involved in the mechanism of left-right asymmetry formation in the thoracic shape.
Keywords: Thoracic shape, Lateral deviation of the thorax, Asymmetry
INTRODUCTION
In recent years, the concept of therapeutic intervention for the thorax has become widespread in physical therapy. From a clinical kinesiological perspective, we believe that intervention targeting the thorax is significant not only for respiratory diseases but also for orthopedic and central nervous system diseases. Kakizaki et al. reported a common asymmetry in the shape of the thorax, including in those who are considered healthy and those who are subject to physical therapy regardless of pathology1). These features of the thorax shape cause left-right imbalance in the muscle activities of the trunk and limbs, which are asymmetrically arranged and are thought to be the cause of various functional disorders.
As a study focusing on the asymmetry of the thorax shape, Hirayama et al. calculated the cross-sectional area of the thorax using a three-dimensional image analysis system and reported the existence of left-right differences at the same level of the thorax shape2). Shobo et al. calculated thorax volume changes using a 3D motion analysis system and also reported left-right differences in thorax shape3). Although there are differences in the measurement methods, results are consistent in healthy individuals: the left side of the thorax has a larger area and volume at the upper thoracic level, and the right side of the thorax has a larger area and volume at the lower thoracic level in healthy subjects. In addition, the degree of asymmetry in the shape of the thorax correlated with the rate of thoracic dilatation, % Vital Capacity, % Forced Expiratory, % Inspiratory Capacity, and % Expiratory Reserve Volume, and has been reported to affect the motion of the thorax and respiratory function2, 3). However, the mechanism of asymmetry in thorax shape has not yet been investigated. Examining the mechanism by which asymmetry is formed in thorax shape may add a useful assessment measure and treatment rationale in physical therapy. We hypothesized that the relationship with posture is an important factor. The thorax is easily influenced by the adjacent cervical and lumbar alignment. The respiratory muscles attached to the thorax also function as postural support muscles4). Further, deformations in the alignment of the spine, such as kyphoscoliosis and scoliosis, affect the shape and movement of the thorax. In particular, scoliosis is characterized by an asymmetrical thorax shape5, 6). In other words, changes in spinal alignment on the frontal plane may be a factor in the mechanism of asymmetry in the shape of the thorax.
The purpose of this study was to analyze the relationship between the degree of thoracic shape asymmetry and postural changes on the frontal plane and to examine the mechanism by which thoracic shape asymmetry is formed.
PARTICIPANTS AND METHODS
The participants were 19 healthy males (age: 26.9 ± 3.3 years, height: 172.0 ± 1.1 cm, body mass: 65.8 ± 7.2 kg, body mass index: 22.3 ± 2.0 kg/mg2; mean ± standard deviation [SD]). Participants had no history of smoking, respiratory diseases or traumas, anamneses of thoracotomy or laparotomy, or obvious spinal or thoracic deformations. Before commencement of the experiments, the participants were informed of and read the scientific purpose and significance of the research and signed the written informed consent form. This study was approved by the ethics committee of Bunkyo Gakuin University in accordance with the Declaration of Helsinki revised October 2013 (approval no. T2019-0004).
In this study, we measured thoracic asymmetry in the resting expiratory position and postural changes in the frontal plane. The postural change in the frontal plane was defined by the amount of lateral deviation of the thorax.
The participants were tested in an upright sitting position with a pelvic tilt of zero degrees, feet flat on the floor and 90° flexion of the hip and knee joints. The pelvic angle was defined as an angle created by an intersecting theoretical line formed by infrared reflective markers attached to the skin over the anterior and posterior superior iliac spines together with a theoretical spatial horizontal line, which was determined by using a spirit level. Before data collection, participants sat down unsupported on a stool with their knees at 90°, their feet positioned shoulder width apart, and their arms relaxed at the side of their body3, 7).
Thoracic movement during respiration was analyzed based on the changes in thoracic expansion volume. Kinematic data on respiratory thoracic motion were collected using a three-dimensional motion analyzer (Vicon MX; Vicon, Inc., Los Angeles, CA, USA) at a sampling rate of 100 Hz. Thoracic motion measurements were performed using eight cameras. A total of 70 infrared reflective markers, each with a diameter of 9.5 mm, were placed at specific points across the front of the thorax and at the back. The 70 reflective markers were used in the configuration shown in Fig. 1. Their movements were used to record changes in thoracic volume. In accordance with previous studies3, 8,9,10,11), the changes in thoracic volume were calculated from the amount of change in the movement of the infrared reflective markers attached to the body surface. The precise positioning for both the anterior and posterior markers was determined from five midline markers placed vertically in line on five levels. The anatomical landmarks for the horizontal rows were the sternal notch, 3rd rib, xiphoid process, 8th rib, and 10th rib, all of which are commonly used as guides for thoracic movement palpation. Three markers were placed on either side of a midline marker, totaling seven markers in all. This procedure was repeated on the posterior aspect of the trunk at the corresponding five levels. The distance between each marker was based on the participant’s physique and set at 15% of the distance between the left and right acromion processes. The thoracic volume was calculated by analyzing imaginary hexahedral blocks, in accordance with the method of previous studies3, 8, 11). An imaginary hexahedral block was formed using four markers each on the anterior and posterior sides. To measure changes in ventral and dorsal thoracic volumes, a virtual midpoint was set between the ventral and dorsal markers, and an anterior space was created between the ventral marker and that midpoint. Similarly, the posterior space was created between the dorsal markers and midpoints. In this study, the thoracic volumes were measured using 48 blocks. Each marker’s movement was used to record changes in thoracic volumes at a resting position. In this study, the 48 hexahedra were classified into four levels of height, and each level was divided into ventral and posterior areas (Fig. 2). The volume change was calculated by categorizing the eight areas into eight levels: the upper level front (UF) and back (UB), the middle level front (MF) and back (MB), the lower level front (LF) and back (LB), and the abdominal level front (AF) and back (AB). The volume of the thorax in each area was calculated as the ratio of left to right (right side data/left side data). The lateral deviation of the thorax was calculated by referring to the method of Homma et al.12) (Fig. 3). The thorax center point was defined as the midpoint connecting the ventral and dorsal reference points at the level of the sternal fenestra. The pelvic center point was calculated as the midpoint of the superior anterior iliac spine and the superior posterior iliac spine, and the midpoint of each of these points was recorded. The difference in the X-coordinates between the center of the thorax and the center of the pelvis was defined as the thoracic lateral deviation and normalized by the height. Negative polarity was denoted as the left side and positive polarity as the right side. In this study, to focus on the shape of the rib cage at rest, the task motion was specified only for the resting expiratory position, and the data were extracted. The Vicon Body Builder (Vicon, Inc.) and Microsoft Office Excel (Microsoft, Redmond, WA, USA) were used for the calculation of thoracic volumes and the lateral deviation of the thorax. For statistical analysis, the mean values of the left–right ratio of the thorax shape and the lateral deviation of the thorax in each area were calculated with 95% confidence intervals (95% CIs). The relationship between the left-right ratio of thorax shape in each area and the amount of lateral deviation of the thorax was examined using Pearson’s product ratio correlation coefficient. The significance level was <0.05. Evaluation and analysis of all data were performed using SPSS Statistics for Windows version 24.0 (IBM Corp., Armonk, NY, USA).
Fig. 1.

Placement of reflection markers for estimating thoracic volume.
Fig. 2.

Area classification of the thorax.
UF: upper level front; UB: upper level back; MF: middle level front; MB: middle level back; LF: lower level front; LB: lower level back; AF: Abdominal level front; AB: abdominal level back.
Fig. 3.
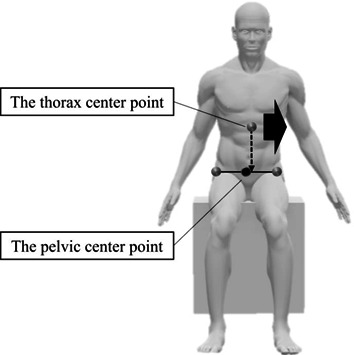
Method of calculating lateral thoracic deviation (case of left lateral deviation).
RESULTS
The thoracic expansion volume ratios at each area are summarized in Table 1. The lateral deviation of the thorax was −3.6 ± 3.2 mm/m (95% CI: −2.0 to −5.2). In this study, the thorax center point was deviated to the left side relative to the pelvic center point. The relationship between the left–right ratio of thorax shape and the amount of lateral deviation of the thorax in each area is shown in Table 2. UF and lateral thoracic deviation showed a positive correlation. LF, LB, and AF showed negative correlation.
Table 1. Left–right ratio of volume in each area.
| Left–Right ratio | n | |
| UF | 0.98 ± 0.03 (0.97–0.99) | 19 |
| UB | 1.00 ± 0.03 (0.98–1.01) | 19 |
| MF | 1.02 ± 0.04 (0.99–1.04) | 19 |
| MB | 1.02 ± 0.02 (1.01–1.03) | 19 |
| LF | 1.07 ± 0.04 (1.06–1.09) | 19 |
| LB | 1.06 ± 0.04 (1.04–1.08) | 19 |
| AF | 1.05 ± 0.05 (1.02–1.08) | 19 |
| AB | 1.06 ± 0.05 (1.03–1.08) | 19 |
Values are mean ± SD (95%CI), n: number of participants.
UF: upper level front; UB: upper level back; MF: middle level front; MB: middle level back; LF: lower level front; LB: lower level back; AF: Abdominal level front; AB: abdominal level back.
Table 2. Correlation between left–right ratio of thorax volume and lateral deviation of thorax.
| R | p | n | |
| UF | 0.74 | <0.01 | 19 |
| UB | 0.41 | 0.08 | 19 |
| MF | 0.20 | 0.40 | 19 |
| MB | −0.16 | 0.51 | 19 |
| LF | −0.57 | <0.05 | 19 |
| LB | −0.61 | <0.01 | 19 |
| AF | −0.47 | <0.05 | 19 |
| AB | −0.37 | 0.11 | 19 |
R: correlation coefficient; p: significance level of R; n: number of participants.
UF: upper level front, UB: upper level back, MF: middle level front, MB: middle level back, LF: lower level front, LB: lower level back, AF: Abdominal level front, AB: abdominal level back.
DISCUSSION
In this study, we focused on the asymmetry of the thorax shape and measured the volume change of the thorax using a 3-D motion analysis system. In addition, the lateral deviation of the thorax was calculated to elucidate the mechanism of the formation of asymmetry of the thorax shape. As a result, left–right differences in thorax shape were shown, and positive and negative correlations with the amount of lateral deviation of the thorax were revealed. Asymmetry of the thorax shape was investigated by dividing the thorax into eight areas and using the ratio of left to right volume change. As for the characteristics of each area, the volume on the left side of UF was large, and the volumes on the right side of MB, LF, LB, AF, and AB were large. The change in volume of the thorax using a 3-D motion analyzer indicates the lung volume level, and the increase or decrease in volume can define the forward and backward rotation of the ribs. In other words, an increase in volume indicates the backward rotation of the ribs seen in inspiration. On the other hand, a decrease in volume indicates anterior rotation of the ribs as seen in expiration. This finding suggests that the left side of UF shows more posterior rotation than the right side, and that the left side of MB, LF, LB, AF, and AB show more anterior rotation than the right side. However, UB had a 95% CI of 0.98–1.01 and MF had a 95% CI of 0.99–1.04. Since infrared reflective markers were applied on the body surface in this study, it is necessary to consider the influence of the muscle volume of the scapula and pectoralis major. The amount of lateral deviation of the thorax showed that the center point of the thorax was deviated to the left side relative to the center point of the pelvis in about 90% of the participants. Previous studies have shown that the left side of a person’s lower extremity functions as an axial leg13). In other words, it is thought that the upper body mass is brought closer to the left lower limb, which functions as the axial leg during walking, to enable the right lower limb to swing out easily. Therefore, it was suggested that the axis formation to the left side during walking affects the sitting posture. As for the relationship between the asymmetry of the thorax shape and the lateral deviation of the thorax, the more the thorax center point was deviated to the left relative to the pelvic center point, the larger the left side volume of UF, and the larger the right-side LF, LB, and AF volumes. As the thorax center point deviates laterally, the spinal column slightly changes its alignment in the frontal plane. The change in the alignment of the spine in the frontal plane is accompanied by the rotation of the vertebral column due to coupling motion, which may change the alignment of the right and left ribs at the same level, resulting in the formation of an asymmetrical thorax shape. Kouwenhoven et al. reported that even healthy individuals without spinal deformity have potential vertebral body rotation14). Therefore, we believe that a posture with a lateral deviation of the thorax in the frontal plane was observed in the present study of healthy individuals. In other words, the lateral deviation of the thorax causes a slight twisting of the thoracic vertebrae, which results in the formation of an asymmetrical shape of the thorax by establishing different directions of motion in the rib alignment at the same level. Therefore, the results of this study suggest that postural changes in the frontal plane are one of the factors in the mechanism of the formation of left-right asymmetry in thorax shape. Komuro et al. also reported asymmetry of thorax shape and lateral deviation of the thorax in healthy individuals15). However, the relationship between asymmetry of thorax shape and lateral deviation of the thorax has not been reported, and we believe this is a new finding in this study. One of the limitations of this study is the selection and age of the participants. The present study was conducted on healthy participants, and only young males were measured. Therefore, we believe that it is necessary to conduct measurements in different age groups and to examine participants with diseases. The method of calculating the lateral thoracic deviation was based on the deviation of the midpoint between the two markers attached to the ventral and dorsal sides of the sternal fenestra to the pelvic center. Therefore, we do not measure the mass of the trunk or the spinal column alignment, and we think that the future task is to grasp the leftward deviation of the thorax from various angles. In addition, in order to utilize the results in clinical practice, we would like to verify whether it is possible to reduce the asymmetry of the thorax shape and to change the muscle groups of the thorax and the respiratory function by medianizing the posture. This study demonstrated the relationship between the asymmetry of the thorax shape and the amount of lateral deviation of the thorax. Left–right differences were shown in each area of the thorax shape, and positive and negative correlations with the amount of lateral deviation of the thorax were revealed. The lateral deviation of the thorax is thought to affect the relationship between the starting and stopping of muscles, and is thought to change the length and running of muscles attached to the thorax. This feature may lead to imbalance in the muscle groups attached to the trunk. Therefore, the results of the present study may help to support the importance of therapeutic strategies for postures that are conscious of medianization.
Conflicts of interest
The authors declare that there is no conflict of interest regarding the publication of this article.
REFERENCES
- 1.Kakizaki F, editor: Methods for reconstruction of thoracic movement system. Tokyo: Human Press, 2017, pp 2–7 (in Japanese). [Google Scholar]
- 2.Hirayama T, Homma Y, Mohara A, et al. : Effects of the features of thoracic shape at rest on thoracic mobility and respiratory function. Rigakuryoho Kagaku, 2018, 33: 513–518 (in Japanese with English abstract). [Google Scholar]
- 3.Shōbo A, Kakizaki F: The relationship between thoracic configuration and changes in volumes of hemithoraces in upright sitting. J Phys Ther Sci, 2016, 28: 3205–3208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hodges PW, Butler JE, McKenzie DK, et al. : Contraction of the human diaphragm during rapid postural adjustments. J Physiol, 1997, 505: 539–548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Carrier J, Aubin CE, Villemure, et al.: Long-term correction resulting from rib length modifications in adolescent idiopathic scoliosis. In: Sawatzky BJ (ed.), lnternational Research Society of Spinal Deforrnities, Symposium 2004, Vancouver, University of British Columbia Press, 2004, pp 286–289.
- 6.Kasai Y, Takegami K, Uchida A: Length of the ribs in patients with idiopathic scoliosis. Arch Orthop Trauma Surg, 2002, 122: 161–162. [DOI] [PubMed] [Google Scholar]
- 7.Lin F, Parthasarathy S, Taylor SJ, et al. : Effect of different sitting postures on lung capacity, expiratory flow, and lumbar lordosis. Arch Phys Med Rehabil, 2006, 87: 504–509. [DOI] [PubMed] [Google Scholar]
- 8.Ferrigno G, Carnevali P, Aliverti A, et al. : Three-dimensional optical analysis of chest wall motion. J Appl Physiol, 1994, 77: 1224–1231. [DOI] [PubMed] [Google Scholar]
- 9.Nakabo T, Yamamoto S: Influence of kyphosis on chest wall motion—comparison of slump sitting and straight sitting. Rigakuryoho Kagaku, 2009, 24: 697–701 (in Japanese with English abstract). [Google Scholar]
- 10.Aliverti A, Ghidoli G, Dellacà RL, et al. : Chest wall kinematic determinants of diaphragm length by optoelectronic plethysmography and ultrasonography. J Appl Physiol, 2003, 94: 621–630. [DOI] [PubMed] [Google Scholar]
- 11.Aramaki Y, Kakizaki F, Kawata S, et al. : Effects of the posterior pelvic tilt sitting posture on thoracic morphology and respiratory function. J Phys Ther Sci, 2021, 33: 118–124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Homma Y, Hirayama T, Mohara A, et al. : Relations of bilateral symmetry in the cross-sectional area of the quadratus lumborum muscles to posture in the frontal plane and respiratory function in forced breathing. Rigakuryoho Kagaku, 2018, 33: 501–506 (in Japanese with English abstract). [Google Scholar]
- 13.Hirasawa Y: Lateralization of a left human foot and a right from a viewpoint of stasiogy. Shinkeishinpo, 1980, 24: 623–632 (in Japanese with English abstract). [Google Scholar]
- 14.Kouwenhoven JW, Vincken KL, Bartels LW, et al. : Analysis of preexistent vertebral rotation in the normal spine. Spine, 2006, 31: 1467–1472. [DOI] [PubMed] [Google Scholar]
- 15.Komuro N, Homma Y, Adachi R, et al. : Relationships among thoracic lateral deviation, thoracic shape, and lateral tilt angle of the shank in the stance phase of gait. Rigakuryoho Kagaku, 2020, 35: 187–191 (in Japanese with English abstract). [Google Scholar]