

Abstract
Objective
To examine how perceived leadership behaviours affect burnout, professional fulfilment and intent to leave the organisation among physicians.
Design
Anonymous cross-sectional survey study from November 2016 to October 2018.
Setting
12 036 attending and resident physicians at 11 healthcare organisations participating in the Physician Wellness Academic Consortium (PWAC) were surveyed to assess burnout and professional fulfilment and their drivers.
Participants
A sample of 5416 attending physicians with complete data on gender, specialty, leadership, burnout and professional fulfilment.
Main outcomes and measures
The leadership behaviour of each physician’s supervisor was assessed using the Mayo Clinic Participatory Management Leadership Index and categorised in tertiles. Multivariable logistic regression analyses examined the effect of leadership behaviour rating of each physician’s supervisor on burnout, professional fulfilment and intent to leave controlling for gender and specialty.
Results
The response rate was 45% across 11 institutions. Half of the respondents were female. Professional fulfilment increased with increasing tertiles of leadership behaviour rating (19%, 34%, 47%, p<0.001). The odds of professional fulfilment were 5.8 times higher (OR=5.8, 95% CI: 5.1 to 6.59) for physicians in the top tertile compared with those in the lowest tertile. Physicians in the top tertile were also 48% less likely to be burned out (OR=0.52, 95% CI: 0.45 to 0.61) and reported 66% lower intent to leave (OR=0.34, 95% CI: 0.26 to 0.44). Individuals who rated their supervisor’s leadership in upper tertiles relative to lower tertiles exhibited lower levels of burnout (18% vs 35% vs 47%, p<0.001), and intent to leave (16% vs 24% vs 50% p<0.001).
Conclusion
Perceived leadership behaviours have a strong relationship with burnout, professional fulfilment and intent to leave among physicians. Organisations should consider leadership development as a potential vehicle to improve physician wellness and prevent costly physician departures.
Keywords: human resource management, organisational development, quality in health care, health services administration & management
Strengths and limitations of this study.
First multicentre survey that analysed the effect of supervisor leadership behaviours on physician well-being, professional fulfilment and intent to leave.
Leadership was evaluated by 5416 physicians representing at least 12 specialties from 11 healthcare organisations.
Validated instruments were used to assess burnout, professional fulfilment and leadership behaviour.
Response rate of 45%, although relatively high for a physician survey, may still contribute to selection bias.
Respondents are from member institutions of the Physician Wellness Academic Consortium, which may limit generalisability.
Introduction
As the landscape of modern medicine continues to grow and change, physicians are increasingly becoming employed by large organisations.1 Solo or small practices are becoming less common, and up to two-thirds of physicians are now employed by large practice groups and 20% of physicians employed by a practice of greater than 100 physicians.2 The trend to group medicine exists beyond the boundaries of academic medicine or private practice, including university hospitals, health maintenance organisations, practice groups, and health systems.
Healthcare organisations have increasingly recognised the impact of occupational burnout and physician well-being on their ability to provide high-quality healthcare to their communities.3 The components of burnout include emotional exhaustion, depersonalisation and decreased personal efficacy in the context of the work environment.4 Concern for physician burnout has gained increasing attention given its implications for patient and provider health. Burnout has previously been associated with worse quality of care,5–7 physician attrition,8–10 patient satisfaction,11–13 cost of care3 14 15 and medical errors.6 16 17 Institutional factors involved in burnout and professional fulfilment act as modifiable factors that can be targeted by organisations.18–23
The impact of leadership effectiveness on burnout and workplace satisfaction for physicians is of importance for healthcare organisations.24–26 A study of 2800 physicians at the Mayo Clinic demonstrated that average leadership behaviour score of physicians’ work unit supervisor explained 11% of the variation in burnout and 47% of the variation in workplace satisfaction across 129 work units when adjusted for other factors.24 The leadership behaviours of physicians immediate supervisor have also been found to have a strong impact on physicians’ perception of values alignment with their organisation as a whole.26 Healthcare leaders face many challenges, balancing costs with ever-changing reimbursements, managing personnel and addressing dynamic quality metrics.27 However, physician training is largely focused on the individual, with an emphasis on clinical care of patients. Developing leadership skills in physician supervisors, organisations can make a large impact in the well-being of their clinicians and foster better patient care.18 25 28 29 Additionally, by understanding and targeting leadership, organisations can impact a large number of healthcare professionals and teams under each leader’s supervision. We sought to further evaluate the factors involved in physician burnout by understanding the relationship between leadership, burnout, profession fulfilment and intent to leave.
Methods
A cross-sectional study of attending physicians in the USA was performed at 11 healthcare organisations participating in the Physician Wellness Academic Consortium (PWAC: https://wellbeingconsortium.org). A standardised survey was administered at participating institutions to be distributed to physicians from all available departments. A total of 12 036 attending and resident physicians across 11 institutions were surveyed between November 2016 and October 2018 as part of their membership in the Physician Wellness Academic Consortium. Among these, 5795 attendings completed evaluation of their supervisor using the 9-item version of the Mayo Clinic Participatory Management Leadership Index. Resident physician data and incomplete data from attending physicians on gender, specialty, leadership rating scale, burnout or professional fulfilment were excluded. The dataset was deidentified by a third-party administrator prior to the analysis.
Patient and public involvement
Patients or the public were not involved in the design, conduct or reporting of the study. Given that this was an anonymous deidentified study, the results will be disseminated by publication of this study without direct contact to participants.
Measures
Supervisor leadership behaviour score
Participants were asked to evaluate their leader using the organisational leadership subscale based on the revised 9-item Mayo Clinic Participatory Management Leadership Index (included in the online supplemental appendix 1, used with permission from Mayo Clinic).25 This instrument was designed to evaluate leadership behaviours associated with team member engagement, including dimensions related to inclusion (treating everyone with respect), keeping people informed, soliciting input, empowering team members, nurturing professional development and providing feedback and recognition. Each item is scored on a 5-point scale (0–4) and the scores from the individual items are summed to compute an aggregate score (with higher scores indicating more favourable ratings). The total score was then categorised into tertiles to represent groups of participants’ leadership scores in increasing order towards more favourable evaluations.
bmjopen-2021-057554supp001.pdf (30.1KB, pdf)
Professional fulfilment Index (PFI)
The PFI was used to measure professional fulfilment and burnout. The PFI includes six items for the assessment of professional fulfilment, four items for the assessment of work exhaustion and six items to assess interpersonal disengagement. The burnout score represents the mean of 10 work exhaustion and interpersonal disengagement items, scored on a Likert scale from 0 (not at all) to 4 (extremely), where 4 indicates the highest burnout score. The professional fulfilment scale assesses the degree of intrinsic positive reward the individual derives from their work, including happiness, meaningfulness, contribution, self-worth, satisfaction and feeling in control when dealing with difficult problems at work. Items are measured on a 5-point Likert scale from 0 (not at all true) to 4 (completely true). The mean score represents the mean of all six items and ranges between 0 and 4. Burnout score and professional fulfilment scores were rescaled to be between 0 and 10 to make interpretations simpler and consistent with recent reports.25 26 30 Based on the published validation studies,31 32 the established thresholds for burnout and professional fulfilment on the 0–10 scales are ≥3.25 and >7.5, respectively.
Intent to leave
Participants were asked if they intended to leave their institution within 2 years (What is the likelihood that you will leave your institution within 2 years?). The response choices were none, slight, moderate, likely and definitely. The responses were then collapsed to form a binary variable (0=none, 1 otherwise) indicating that the participants have at least ‘slight’ likelihood of leaving.
Statistical analyses
Data were summarised for the overall sample (table 1) and by tertiles of the leadership behaviour score using frequencies and percentages for categorical variables (table 2). The association between leadership behaviour score and variables of interests were statistically tested using χ2 and trend tests presented in table 2. Kramer’s V statistic was included in table 2 to show the degree of associations between categorical variables. Linear associations between continuous variables and leadership ratings were examined using correlation coefficients. Internal validity of the organisational leadership scale was assessed using Cronbach’s alpha. Multivariable logistic regression analyses were conducted to examine the association between the leadership behaviour score of each physician’s supervisor and burnout and intent to leave controlling for gender, professional fulfilment and specialty. The correlation within specialty groups was accounted for using clustering at specialty level (logistic command with cluster option in Stata V.15). Estimated ORs with 95% CIs and p values are presented in table 3. Predictive margins over leadership scale tertiles were computed based on the logistic regression models for male and female physicians and are presented in figures 1–3. All statistical analyses were conducted in Stata V.15. A p value of <0.05 was considered statistically significant.
Table 1.
Characteristics of the respondents
| Total n=5416 | N (%) |
| Gender | |
| Female | 2710 (50) |
| Male | 2706 (50) |
| Specialty | |
| Anaesthesiology | 407 (7.5) |
| Dermatology | 71 (1.3) |
| Emergency medicine | 322 (6.0) |
| Medicine | 1671 (30.9) |
| Neurology | 195 (3.6) |
| OB-GYN | 248 (4.6) |
| Pathology | 140 (2.6) |
| Paediatrics | 804 (14.9) |
| Psychiatry | 136 (2.5) |
| Radiation oncology | 77 (1.4) |
| Radiology | 317 (5.9) |
| Surgery | 630 (11.6) |
| Missing specialty | 398 (7.3) |
| Leadership behaviour mean score (0–4) (SD) | 2.7 (0.7) |
| Occupational distress and well-being | |
| Professional fulfilment | |
| Mean score (0–10) (SD)* | 6.6 (2.1) |
| Professional fulfilment present (yes) | 2280 (42) |
| Burnout | |
| Mean score (0–10) (SD)† | 3.0 (1.9) |
| Burned out (yes) | 2174 (40) |
| Intent to leave current organisation within 2 years | 1694 (32) |
*Higher score favourable.
†Higher score unfavourable.
Table 2.
Characteristics of the respondents by the tertiles of supervisor leadership behaviour score (scores ranked from lowest to highest)
| Total n=5416 | Tertiles of leadership behaviour score* | |||
| Lowest 1/3 (low scores: (0–2.3) N (row %) |
Middle 1/3 medium scores: (2.4–3.2) N (row %) |
Highest 1/3 high scores: (3.3–4.0) N (row %) |
(Kramer’s V) χ2 p value |
|
| Sex | ||||
| Female | 994 (37) | 972 (36) | 744 (28) | (0.07) (<0.001) |
| Male | 824 (31) | 987 (37) | 895 (33) | |
| Specialty | ||||
| Anaesthesiology | 156 (38) | 154 (38) | 97 (24) | (0.11) (<0.001) |
| Dermatology | 10 (14) | 21 (30) | 40 (56) | |
| Emergency medicine | 66 (21) | 144 (45) | 112 (35) | |
| Medicine | 625 (37) | 593 (36) | 453 (27) | |
| Neurology | 51 (26) | 72 (37) | 72 (37) | |
| OB-GYN | 98 (40) | 83 (34) | 67 (27) | |
| Pathology | 32 (23) | 51 (36) | 57 (41) | |
| Paediatrics | 241 (30) | 306 (38) | 257 (32) | |
| Psychiatry | 43 (32) | 44 (32) | 49 (36) | |
| Radiation oncology | 23 (30) | 29 (38) | 25 (33) | |
| Radiology | 89 (28) | 114 (36) | 114 (36) | |
| Surgery | 214 (34) | 209 (33) | 207 (33) | |
| Missing specialty | 170 (43) | 139 (35) | 89 (22) | |
| Professional fulfilment | ||||
| Mean score (0–10) (SD)† | 5.6 (2.1) | 6.7 (1.8) | 7.7 (1.8) | <0.001 |
| Professional fulfilment present (yes) |
438 (19) | 779 (34) | 1063(47) | (0.33) (<0.001) |
| Burned out | ||||
| Mean score (0–10) (SD)‡ | 3.7 (2.0) | 3.0 (1.7) | 2.2 (1.7) | <0.001 |
| Burned out (yes) | 1010(47) | 766 (35) | 398 (18) | (0.26) (<0.001) |
| Intent to leave (yes) | 851 (50) | 578 (34) | 265 (16) | (0.27) (<0.001) |
*Higher tertile favourable.
†Higher score favourable.
‡Higher score unfavourable.
Table 3.
Logistic regression models of professional fulfilment, burnout and intent to leave
| Model 1 Professional fulfilment (yes) n=5416 |
Model 2 Burnout status (yes) n=5416 |
Model 3 Intent to leave (yes) n=5374 |
|
| Variables | OR (95% CI) (p value) |
OR (95% CI) (p value) |
OR (95% CI) (p value) |
| Female vs male | 0.58 (0.51–0.66) (<0.001) |
1.57 (1.41–1.76) (<0.001) |
0.70 (0.60–0.83) (<0.001) |
| Leadership score Tertile 1 (lowest 1/3 of all scores) |
Reference | Reference | Reference |
| Tertile 2 (middle 1/3 of all scores) |
2.10 (1.85–2.37) (<0.001) |
0.52 (0.45–0.61) (<0.001) |
0.56 (0.48–0.65) (<0.001) |
| Tertile 3 (highest 1/3 of all scores) |
5.80 (5.10–6.59) (<0.001) |
0.26 (0.23–0.31) (<0.001) |
0.34 (0.26–0.44) (<0.001) |
| Professional fulfilment present (yes) | — | — | 0.45 (0.40–0.52) (<0.001) |
| Burned out vs not | — | — | 2.43 (2.17–2.71) (<0.001) |
| Area under the curve (ROC) | 0.71 | 0.66 | 0.74 |
Figure 1.
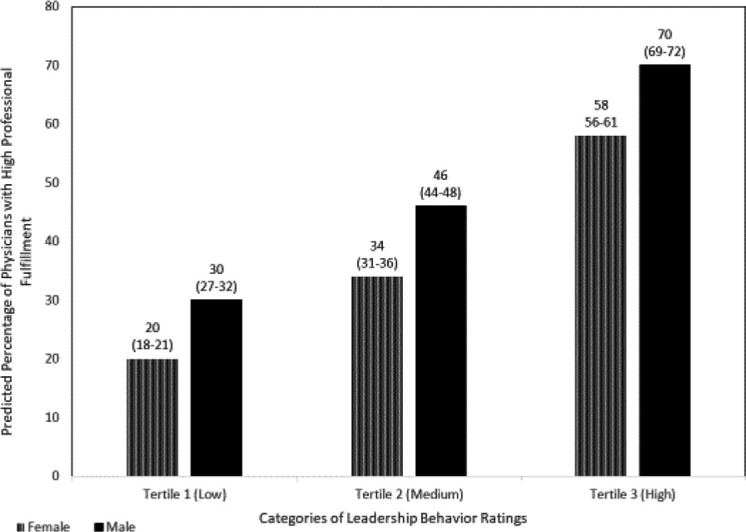
Likelihood (%, 95% CI) of professional fulfilment status by the tertiles of supervisor leadership. Behaviour score for female and male physicians.
Figure 2.
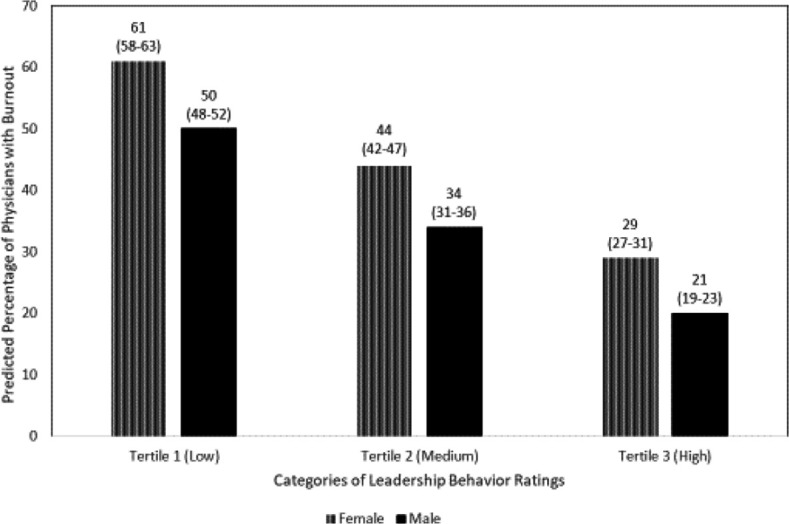
Likelihood (%, 95% CI) of burnout status by the tertiles of supervisor leadership. Behaviour score for female and male physicians.
Figure 3.
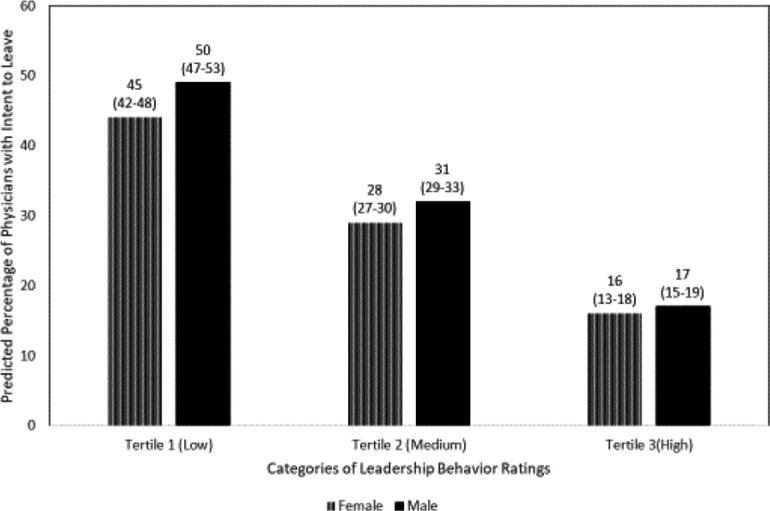
Likelihood (%, 95% CI) of reporting intent to leave by the tertiles supervisor leadership. Behaviour score for female and male physicians.
Results
The overall attending physician response rate for the PWAC survey was 45%. Fully completed surveys from 5416 attending physicians were included in the analysis. The personal and professional characteristics of responders are shown in table 1.
Table 2 presents data on the relationships between specialty distribution, burnout, professional fulfilment and intent to leave by the tertiles of the scores on the Participatory Management Leadership Index, which showed high internal consistency (Cronbach’s alpha=0.95) in this sample.
Female physicians represented 50% (2710/5416) of all participants. The percentage of female physicians who rated their immediate supervisor in the highest tertile of the leaderships scale was significantly lower than male physicians (28% vs 33%, p<0.001). Male physicians rated their leaders more favourably compared with female physicians (2.8 (1.0) vs 2.6 (1.0), p<0.001). By specialty, dermatologists (56%) and pathologists (41%) had the highest proportion who rated their immediate supervisor in the highest tertile of the leadership behaviour. In contrast, OB-GYN specialists (40%), anaesthesiologists (38%) and internal medicine physicians (31%) were least likely to rate their immediate supervisor in the highest tertile of the leaderships scale.
The leadership behaviour rating of each physician’s supervisor was negatively associated with burnout score (r=−0.34, p<0.001) and positively associated with professional fulfilment score (r=0.44, p<0.001). There was a significant positive association between professional fulfilment and leadership behaviour score. Mean professional fulfilments scores (4.6, 4.4, 4.0, p<0.001) and the percentage of those with professional fulfilment were higher at higher tertiles of leadership behaviour scores (lowest tertile: 19%, middle tertile: 34% and highest tertile: 47%, Kramer’s V: 0.33, p<0.001). The mean burnout score (3.7, 3.0, 2.2, p<0.001) and percentage of physicians who had a high burnout score decreased with increasing tertiles of leadership behaviour score (47%, 35% and 18%, Kramer’s V:0.26, p<0.001). Similarly, the percentage of those who reported an intent to leave their institution in the next 2 years decreased with increasing tertiles of leadership behaviour score (50%, 34% and 16%, Kramer’s V: 0.27, p<0.001).
Table 3 presents multivariable logistic regression models of professional fulfilment (Model 1), burnout status (Model 2) and intent to leave (Model 3) in relation to leadership behaviour rating of physician’s supervisor. The strong association between professional fulfilment and leadership behaviour score is demonstrated in Model 1. Physicians who have more favourable evaluations of their leaders were more likely to be in the professionally fulfilled category. Specifically, the odds of having high professional fulfilment increased by a factor of 2.1 for those who rated their leader in the second tertile compared with those in the lowest tertile (OR: 2.10, 95% CI: 1.85 to 2.37), while the odds increased by a factor of 5.8 for those who are in the top tertile compared with those in the lowest tertile (OR: 5.80, 95% CI: 5.10 to 6.59, Area Under the Curve (AUC): 0.71). This model also demonstrates that female physicians were significantly less likely to have high professional fulfilment after adjusting for specialty, and supervisor leadership behaviour rating (OR: 0.58, 95% CI: 0.51 to 0.66). Figure 1 illustrates the likelihood of having professional fulfilment for each leadership behaviour tertile of physician’s supervisor for female and male physicians based on the predicted probabilities obtained from Model 1. Non-overlapping CIs at each tertile show that the difference between gender groups is maintained across tertiles suggesting that the association between leadership score and professional fulfilment is not dependent on gender. This is evidenced by non-significant interaction effects between gender and leadership behaviour score tertiles in Model 1 when interaction terms are included.
The relationship between organisational leadership and physician burnout is assessed in Model 2, which is adjusted by gender, specialty and professional fulfilment. Physicians who rated the leader behaviour of their supervisor in the second tertile were 48% less likely to be burned out compared with those who are in the first tertile (OR: 0.52, 95% CI: 0.45 to 0.61); those who are in the top tertile of leadership behaviour score were 74% less likely to be burned out compared with those who are in the first tertile (OR: 0.26, 95% CI: 0.23 to 0.31). Model 2 also showed that the odds of reporting burnout are 57% higher for female physicians (OR: 1.57, 95% CI: 1.41 to 1.76, AUC: 0.77). The likelihood of burnout derived from Model 2 by the tertiles of leadership behaviour score is illustrated for male and female physicians in figure 2. The gender differences in burnout by increasing tertiles of leadership behaviour score remained similar across tertiles indicated by non-overlapping CIs at each tertile and non-significant interactions between gender and leadership behaviour score tertiles in Model 2.
Model 3 estimates the effect of leadership behaviour rating of each physician’s supervisor on the likelihood that a physician intent to leave their institution within the next 2 years. This model is adjusted by gender, specialty, burnout and professional fulfilment status as potential confounders of intent to leave. Physicians who rated the leader behaviour of their supervisor in the second tertile were 44% less likely to report an intent to leave compared with those who were in the first tertile (OR: 0.56, 95% CI: 0.48 to 0.65); those who were in the top tertile of supervisor leadership behaviour score are 66% less likely to intend to leave compared with those who were in the first tertile (OR: 0.34, 95% CI: 0.26 to 0.44). Model 3 also shows that the odds of reporting intent to leave were 30% lower for female physicians (OR: 0.70, 95% CI: 0.60 to 0.83) and 54% lower for those with high professional fulfilment (OR: 0.46, 95% CI: 0.40 to 0.52). The AUC for this model is 0.74. The likelihood of having intent to leave for male and female physicians in this model by the tertiles of supervisor leadership behaviour score is shown in figure 3. Fifty per cent (95% CI: 47% to 53%) of male physicians and 45% (95% CI: 42% to 48%) of female physicians in the lowest tertile of leadership behaviour score reported an intent to leave in 2 years compared with 17% of male physicians and 16% of female physicians in the top tertile. The difference between the gender groups in the top tertile is significantly narrower compared with that in the lower tertile evidenced by a statistically significant interaction term (gender×tertile3, OR: 0.70, 95% CI: 0.52 to 0.94, p=0.02), when interaction terms are included.
Discussion
This multi-institution study demonstrates a strong relationship between leadership evaluations and burnout, professional fulfilment and intent to leave current organisation among US physicians. These results are consistent with previous single-centre studies which have demonstrated the significant impact of leadership quality on healthcare professional burnout and professional fulfilment.24–26 33 The association between leadership and burnout remains strong even when we control for professional fulfilment, which has a well-established strong inverse relationship with burnout.34 Although the present study looks at the correlation between individuals’ rating of the leadership behaviour of their supervisor and their own well-being and professional fulfilment, previous studies have also found a strong relationship between the composite leadership behaviour score of a leader (as assessed by all individuals reporting to them) and the risk of burnout and professional fulfilment for the members of the team as a whole.24–26 Leader behaviour score also had a strong relationship with intent to leave. These results are consistent with the notion that physicians who are dissatisfied with their supervisor’s ability to lead the team are the more likely to consider other opportunities. Prior studies demonstrated physicians who report intent to leave are three times more likely to leave their institution in the next 2 years.8 9 35 This is especially important as the cost of replacing physicians is significant, and turnover and burnout can be associated with lower quality and higher cost care for patients.3 36–40
Notably, in our study, a lower percentage of female physicians rated the leadership behaviours of their supervisor in the top tertile and a higher percentage rated the behaviours of their supervisor in the lowest tertile. Previous studies have indicated female physicians report greater workplace bullying, harassment, gender discrimination and feelings of isolation.41–49 While female physicians are no longer a minority in the profession, they are often under-represented in leadership, potentially due to inequality and bias in the opportunity for promotion and reward.7 41–44 50 This also results in fewer female leaders serving as mentors and role models, which may be protective against burnout.42 45–47 50
Interestingly, in our adjusted analysis controlling for burnout, professional fulfilment and the behaviour score of their leader, female physicians reported less intent to leave than male physicians (OR: 0.7, 95% CI: 0.59 to 0.83, p<0.001). This is in contrast to prior studies demonstrating a 8%–10% higher attrition rate in female physicians.35 43 49 These observations are consistent with the possibility that higher attrition rates among women physicians may be due to lower satisfaction with their leader and higher rates of burnout. Because intent to leave describes a longer-term plan to change jobs, it is also possible that female physicians may leave their jobs more suddenly.
Investing in the leadership development of supervising physicians may be an important strategy to mitigate burnout and promote professional fulfilment in physicians. An integrative model of Wellness-Centred Leadership incorporating the critical skills and leadership behaviours that cultivate engagement and professional fulfilment was recently published.51 When selecting and developing clinician leaders, the importance of emotional intelligence, social awareness and team communication should be considered.27 These are skills that can be developed in physicians in training, beginning in medical school and continuing through all phases of training, including communication, mindfulness and reflection.18 52 53 Leaders’ own well-being impacts their leadership effectiveness. One recent study demonstrated that 9.8% of the variation in a leader’s leadership behaviour scores, as assessed by physicians on their team, was related to their own independently assessed degree of burnout.25 This observation suggests that burnout among leaders may result in suboptimal leadership behaviour which in turn increases the risk of burnout in their team members creating a vicious cycle. This finding suggests that leadership development initiatives should include attention to the well-being of the leader in addition to cultivation of specific leadership skills.51
Our study has several limitations. First, although relatively high for a physician survey,53–56 our response rate was 45%, which raises the potential for selection bias.57 Second, the cross-sectional and survey-based design of the study allows us only to assess associations between leadership evaluations and the outcomes. Third, all physicians surveyed were from healthcare organisations participating in the PWAC. Although some PWAC institutions are non-academic institutions, most are academic medical centres, which makes the generalisability of the results to non-academic settings unclear. Finally, since the age of the respondent along with gender can help reveal the identity of the physicians in small specialties, it was not made available for the analyses and remains a limitation of the study. Our study has several strengths. It is a large multicentre study of physicians from 11 healthcare organisations representing all medical specialties with reasonably high response rate, using validated instruments to assess burnout, professional fulfilment and leadership behaviour.
Conclusion
The leadership behaviours of physician supervisors have a strong relationship to their team members’ burnout, professional fulfilment and intent to leave. Female physicians report lower satisfaction with their leaders’ leadership behaviours. Greater attention to leader selection, development and performance evaluation represents a potentially important approach to reducing occupational burnout and promoting professional fulfilment in large healthcare organisations.
Supplementary Material
Footnotes
Contributors: MM had full access to all of the study data provided by PWAC and takes responsibility for the integrity and the accuracy of the data analysis. MM, DM and TS were responsible for concept and design, acquisition, analysis or interpretation of data. Drafting of the manuscript was done by MM and CG. Critical revision of the manuscript for important intellectual content was performed by TS, DM and CG. Statistical analysis was done by MM. Administrative, technical or material support was provided by MM. MM is the guarantor.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: TS is coinventor of the Mayo Clinic Participatory Management Leadership Index and Well-being Index Instruments (Physician Well-being Index, Medical Student Well-being Index, Nurse Well-being Index, Well-being Index). Mayo Clinic holds the copyright to these instruments and has licensed them for use outside of Mayo Clinic. TS receives a portion of any royalties paid to Mayo Clinic. TS reported receiving honoraria from grand rounds or keynote lecture presentations and advising for health care organisations outside the submitted work. Other authors report no conflict of interest.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data may be obtained from a third party and are not publicly available. No additional data related to the analyses of this study are available.
Ethics statements
Patient consent for publication
Not applicable.
References
- 1.Kane C. Updated data on physician practice arrangements: for the first time, fewer physicians are owners than employees. 3. American Medical Association. AMA Economic and Health Policy Research, 2019. https://www.ama-assn.org/system/files/2019-07/prp-fewer-owners-benchmark-survey-2018.pdf [Google Scholar]
- 2.Hawkins M. Survey of America’s physicians: practice patterns and perspectives, 2016. Available: https://www.merritthawkins.com/uploadedFiles/Physicians%20Foundation%202016%20Survey%20of%20Americas%20Physicians.pdf
- 3.Shanafelt T, Goh J, Sinsky C. The business case for investing in physician well-being. JAMA Intern Med 2017;177:1826–32. 10.1001/jamainternmed.2017.4340 [DOI] [PubMed] [Google Scholar]
- 4.Maslach C, Jackson SE. The measurement of experienced burnout. J Organ Behav 1981;2:99–113. 10.1002/job.4030020205 [DOI] [Google Scholar]
- 5.Tawfik DS, Scheid A, Profit J, et al. Evidence relating health care provider burnout and quality of care: a systematic review and meta-analysis. Ann Intern Med 2019;171:555–67. 10.7326/M19-1152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg 2010;251:995–1000. 10.1097/SLA.0b013e3181bfdab3 [DOI] [PubMed] [Google Scholar]
- 7.Bohman B, Dyrbye L, Sinsky CA. Physician well-being: the reciprocity of practice efficiency, culture of wellness, and personal resilience. NJEM Catal, 2017. Available: https://catalyst.nejm.org/doi/full/10.1056/CAT.17.0429?casa_token=MlYGT-8qk_cAAAAA:1QuLaP1w5Dg6R3KqgMyc5u_MsH-y5Wa8Q3Em-rPqf2R_Vx_McVKsM3eUijpqCW8PEc6W3WB7rbSM [Accessed 20 Jan 2021].
- 8.Hamidi MS, Bohman B, Sandborg C, et al. Estimating institutional physician turnover attributable to self-reported burnout and associated financial burden: a case study. BMC Health Serv Res 2018;18:851. 10.1186/s12913-018-3663-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jackson TN, Pearcy CP, Khorgami Z, et al. The physician attrition crisis: a cross-sectional survey of the risk factors for reduced job satisfaction among US surgeons. World J Surg 2018;42:1285–92. 10.1007/s00268-017-4286-y [DOI] [PubMed] [Google Scholar]
- 10.Shanafelt TD, Mungo M, Schmitgen J, et al. Longitudinal study evaluating the association between physician burnout and changes in professional work effort. Mayo Clin Proc 2016;91:422–31. 10.1016/j.mayocp.2016.02.001 [DOI] [PubMed] [Google Scholar]
- 11.Haas JS, Cook EF, Puopolo AL, et al. Is the professional satisfaction of general internists associated with patient satisfaction? J Gen Intern Med 2000;15:122–8. 10.1046/j.1525-1497.2000.02219.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Welle D, Trockel MT, Hamidi MS, et al. Association of occupational distress and sleep-related impairment in physicians with unsolicited patient complaints. Mayo Clin Proc 2020;95:719–26. 10.1016/j.mayocp.2019.09.025 [DOI] [PubMed] [Google Scholar]
- 13.Windover AK, Martinez K, Mercer MB, et al. Correlates and outcomes of physician burnout within a large academic medical center. JAMA Intern Med 2018;178:856–8. 10.1001/jamainternmed.2018.0019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Han S, Shanafelt TD, Sinsky CA, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med 2019;170:784–90. 10.7326/M18-1422 [DOI] [PubMed] [Google Scholar]
- 15.Dyrbye LN, West CP, Hunderfund AL, et al. Relationship between burnout, professional behaviors, and cost-conscious attitudes among US physicians. J Gen Intern Med 2020;35:1465–76. 10.1007/s11606-019-05376-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA 2006;296:1071–8. 10.1001/jama.296.9.1071 [DOI] [PubMed] [Google Scholar]
- 17.Menon NK, Shanafelt TD, Sinsky CA, et al. Association of physician burnout with suicidal ideation and medical errors. JAMA Netw Open 2020;3:e2028780. 10.1001/jamanetworkopen.2020.28780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shanafelt TD, Noseworthy JH. Executive leadership and physician well-being: nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc 2017;92:129–46. 10.1016/j.mayocp.2016.10.004 [DOI] [PubMed] [Google Scholar]
- 19.Andolsek KM, Km A. Physician well-being: organizational strategies for physician burnout. FP Essent 2018;471:20–4. [PubMed] [Google Scholar]
- 20.Mari S, Meyen R, Kim B. Resident-led organizational initiatives to reduce burnout and improve wellness. BMC Med Educ 2019;19:437. 10.1186/s12909-019-1756-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.DeChant PF, Acs A, Rhee KB, et al. Effect of organization-directed workplace interventions on physician burnout: a systematic review. Mayo Clin Proc Innov Qual Outcomes 2019;3:384–408. 10.1016/j.mayocpiqo.2019.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Shanafelt T, Stolz S, Springer J, et al. A blueprint for organizational strategies to promote the well-being of health care professionals. NEJM Catalyst 2020;1. 10.1056/CAT.20.0266 [DOI] [Google Scholar]
- 23.Swensen SJ, Shanafelt TD. Mayo clinic strategies to reduce burnout: 12 actions to create the idea workplace. Oxford University Press, 2020. [Google Scholar]
- 24.Shanafelt TD, Gorringe G, Menaker R, et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc 2015;90:432–40. 10.1016/j.mayocp.2015.01.012 [DOI] [PubMed] [Google Scholar]
- 25.Shanafelt TD, Makowski MS, Wang H, et al. Association of burnout, professional fulfillment, and self-care practices of physician leaders with their independently rated leadership effectiveness. JAMA Netw Open 2020;3:e207961. 10.1001/jamanetworkopen.2020.7961 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Shanafelt TD, Wang H, Leonard M, et al. Assessment of the association of leadership behaviors of supervising physicians with personal-organizational values alignment among staff physicians. JAMA Netw Open 2021;4:e2035622. 10.1001/jamanetworkopen.2020.35622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Stoller JK. Help wanted: developing clinician leaders. Perspect Med Educ 2014;3:233–7. 10.1007/s40037-014-0119-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Edelmann CM, Boen F, Fransen K. The power of Empowerment: predictors and benefits of shared leadership in organizations. Front Psychol 2020;11:582894. 10.3389/fpsyg.2020.582894 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.White BAA, Bledsoe C, Hendricks R, et al. A leadership education framework addressing relationship management, burnout, and team trust. Proc 2019;32:298–300. 10.1080/08998280.2018.1550346 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Trockel MT, Menon NK, Rowe SG, et al. Assessment of physician sleep and wellness, burnout, and clinically significant medical errors. JAMA Netw Open 2020;3:e2028111. 10.1001/jamanetworkopen.2020.28111 [DOI] [PubMed] [Google Scholar]
- 31.Trockel M, Bohman B, Lesure E, et al. A brief instrument to assess both burnout and professional fulfillment in physicians: reliability and validity, including correlation with self-reported medical errors, in a sample of resident and practicing physicians. Acad Psychiatry 2018;42:11–24. 10.1007/s40596-017-0849-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Trockel MT, Hamidi MS, Menon NK, et al. Self-valuation: attending to the most important instrument in the practice of medicine. Mayo Clin Proc 2019;94:2022–31. 10.1016/j.mayocp.2019.04.040 [DOI] [PubMed] [Google Scholar]
- 33.Dyrbye LN, Major-Elechi B, Hays JT, et al. Relationship between organizational leadership and health care employee burnout and satisfaction. Mayo Clin Proc 2020;95:698–708. 10.1016/j.mayocp.2019.10.041 [DOI] [PubMed] [Google Scholar]
- 34.Siegel TR, Nagengast AK. Mitigating burnout. Surg Clin North Am 2019;99:1029–35. 10.1016/j.suc.2019.06.015 [DOI] [PubMed] [Google Scholar]
- 35.Rittenhouse DR, Mertz E, Keane D, et al. No exit: an evaluation of measures of physician attrition. Health Serv Res 2004;39:1571–88. 10.1111/j.1475-6773.2004.00304.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gill JM, Mainous AG. The role of provider continuity in preventing hospitalizations. Arch Fam Med 1998;7:352–7. 10.1001/archfami.7.4.352 [DOI] [PubMed] [Google Scholar]
- 37.Raddish M, Horn SD, Sharkey PD. Continuity of care: is it cost effective? Am J Manag Care 1999;5:727–34. [PubMed] [Google Scholar]
- 38.Buchbinder SB, Wilson M, Melick CF, et al. Estimates of costs of primary care physician turnover. Am J Manag Care 1999;5:1431–8. [PubMed] [Google Scholar]
- 39.Misra-Hebert AD, Kay R, Stoller JK. A review of physician turnover: rates, causes, and consequences. Am J Med Qual 2004;19:56–66. 10.1177/106286060401900203 [DOI] [PubMed] [Google Scholar]
- 40.Atkinson W, Misra-Hebert A, Stoller JK. The impact on revenue of physician turnover: an assessment model and experience in a large healthcare center. J Med Pract Manage 2006;21:351–5. [PubMed] [Google Scholar]
- 41.Person SD, Jordan CG, Allison JJ. Measuring diversity and inclusion in academic medicine: the diversity engagement survey (des). Acad Med J Assoc Am Med Coll 2015;90:1675–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Tesch BJ, Wood HM, Helwig AL, et al. Promotion of women physicians in academic medicine. glass ceiling or sticky floor? JAMA 1995;273:1022–5. [PubMed] [Google Scholar]
- 43.Frank E, Zhao Z, Sen S, et al. Gender disparities in work and parental status among early career physicians. JAMA Netw Open 2019;2:e198340. 10.1001/jamanetworkopen.2019.8340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mueller CM, Gaudilliere DK, Kin C, et al. Gender disparities in scholarly productivity of US academic surgeons. J Surg Res 2016;203:28–33. 10.1016/j.jss.2016.03.060 [DOI] [PubMed] [Google Scholar]
- 45.Cochran A, Hauschild T, Elder WB, et al. Perceived gender-based barriers to careers in academic surgery. Am J Surg 2013;206:263–8. 10.1016/j.amjsurg.2012.07.044 [DOI] [PubMed] [Google Scholar]
- 46.Zhuge Y, Kaufman J, Simeone DM, et al. Is there still a glass ceiling for women in academic surgery? Ann Surg 2011;253:637–43. 10.1097/SLA.0b013e3182111120 [DOI] [PubMed] [Google Scholar]
- 47.Liang R, Dornan T, Nestel D. Why do women leave surgical training? A qualitative and feminist study. Lancet 2019;393:541–9. 10.1016/S0140-6736(18)32612-6 [DOI] [PubMed] [Google Scholar]
- 48.Bingmer K, Wojnarski CM, Brady JT, et al. A model for a formal mentorship program in surgical residency. J Surg Res 2019;243:64–70. 10.1016/j.jss.2019.04.068 [DOI] [PubMed] [Google Scholar]
- 49.Khoushhal Z, Hussain MA, Greco E, et al. Prevalence and causes of attrition among surgical residents: a systematic review and meta-analysis. JAMA Surg 2017;152:265–72. 10.1001/jamasurg.2016.4086 [DOI] [PubMed] [Google Scholar]
- 50.Templeton K, Bernstein CA, Sukhera J, et al. Gender-Based differences in burnout: issues faced by women physicians. NAM Perspect 2019. 10.31478/201905a [DOI] [Google Scholar]
- 51.Shanafelt T, Trockel M, Rodriguez A, et al. Wellness-centered leadership: equipping health care leaders to cultivate physician well-being and professional fulfillment. Acad Med 2021;96:641–51. 10.1097/ACM.0000000000003907 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Smith CD, Balatbat C, Corbridge S, et al. Implementing optimal team-based care to reduce clinician burnout. NAM Perspect 2018;8. Discussion Paper, National Academy of Medicine, Washington, DC. 10.31478/201809c [DOI] [Google Scholar]
- 53.Shanafelt T, Swensen S. Leadership and physician burnout: using the annual review to reduce burnout and promote engagement. Am J Med Qual 2017;32:563–5. 10.1177/1062860617691605 [DOI] [PubMed] [Google Scholar]
- 54.Allegra CJ, Hall R, Yothers G. Prevalence of burnout in the U.S. oncology community: results of a 2003 survey. J Oncol Pract 2005;1:140–7. 10.1200/jop.2005.1.4.140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Kuerer HM, Eberlein TJ, Pollock RE, et al. Career satisfaction, practice patterns and burnout among surgical oncologists: report on the quality of life of members of the Society of surgical oncology. Ann Surg Oncol 2007;14:3043–53. 10.1245/s10434-007-9579-1 [DOI] [PubMed] [Google Scholar]
- 56.Shanafelt TD, Balch CM, Bechamps GJ, et al. Burnout and career satisfaction among American surgeons. Ann Surg 2009;250:463–71. 10.1097/SLA.0b013e3181ac4dfd [DOI] [PubMed] [Google Scholar]
- 57.Asch DA, Jedrziewski MK, Christakis NA. Response rates to mail surveys published in medical journals. J Clin Epidemiol 1997;50:1129–36. 10.1016/S0895-4356(97)00126-1 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2021-057554supp001.pdf (30.1KB, pdf)
Data Availability Statement
Data may be obtained from a third party and are not publicly available. No additional data related to the analyses of this study are available.