

Abstract
Objectives
This study aimed to examine the association between infertility treatment and neurodevelopment in children at 2 and 3.5 years of age.
Design
Prospective cohort study.
Setting and participants
The study population consisted of mother–child pairs who participated in the Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study in Miyagi and Iwate Prefectures, Japan. Pregnant women were recruited in obstetric clinics or hospitals and their children were followed up by the questionnaire.
Outcome measures
The children’s neurodevelopmental outcomes were assessed at 2 and 3.5 years of age using the Ages and Stages Questionnaire, third edition (ASQ-3), which consists of questions on five developmental domains. We performed a multivariate logistic regression analysis of the association between infertility treatment (including ovulation induction (OI), artificial insemination with husband’s sperm (AIH) and assisted reproductive technology (ART)) and the clinical range of ASQ-3.
Results
Of 9655 mother–child pairs, 273 (2.8%) and 487 (5.0%) were conceived through OI/AIH and ART, respectively. The odds of having developmental delays at 2 years of age were higher in children conceived through OI/AIH (OR, 1.36; 95% CI 1.00 to 1.85) and ART (OR, 1.36; 95% CI 1.07 to 1.72) than in those conceived naturally. Additionally, OI/AIH and ART were significantly associated with communication (OR, 1.93; 95% CI 1.25 to 2.98) and gross motor (OR, 1.50; 95% CI 1.08 to 2.09) delays, respectively. There were no statistically significant differences in the odds of having developmental delays at 3.5 years of age in children conceived through OI/AIH (OR, 1.13; 95% CI 0.79 to 1.61) and ART (OR, 1.03; 95% CI 0.78 to 1.37).
Conclusion
In this study, we found a significant association between infertility treatment and children’s neurodevelopment at 2 years of age, whereas no statistically significant differences were found at 3.5 years of age.
Keywords: epidemiology, maternal medicine, developmental neurology & neurodisability
Strengths and limitations of this study.
The large sample size in this study allowed us to investigate the association between each type of infertility treatment and neurodevelopmental outcomes.
We evaluated children’s neurodevelopment at two points—2 and 3.5 years of age.
Ages and Stages Questionnaire, third edition is a screening tool (not a diagnostic tool) for developmental delays.
The number of children born through specific forms of infertility treatment, such as fresh embryo transfer, was insufficient to allow subanalysis of fresh or frozen embryo transfer.
Introduction
With the rapid progress in infertility treatment, the number of women who use infertility treatment is increasing, and more than 10% of the childbearing population has resorted to assisted reproductive technology (ART) for conception.1 In recent years, the number of fertility treatments in Japan has also been on the increase. In 2018, 56 000 newborns were conceived through ART, including in vitro fertilisation (IVF) and intracytoplasmic sperm injection (ICSI). This accounts for approximately 6% of all live births in the same year.2 Because conception using ART involves several processes (such as physical manipulation of gametes and exposure of embryos to hormones and culture media) that differ greatly from those in a natural conception, there is potential for disturbance of normal early developmental processes.3 4 Therefore, many studies have investigated the association between ART and neurodevelopmental outcomes.5–8
The findings have been almost entirely consistent in showing that singleton children conceived through ART and born at term are no different neurodevelopmentally from those born following natural conception. However, the evidence remains equivocal,8–11 and another review stated that possible associations between infertility treatment and developmental delay require further assessment in larger studies.12 The inconsistent results in the previous studies may have been due to the small sample size (fewer than 1000 children),3 and a longitudinal study with a larger sample size is needed.
This study aimed to investigate the association between infertility treatment and children’s neurodevelopment at 2 and 3.5 years of age in a Japanese birth cohort.
Methods
Study setting and participants
This study was based on data obtained by the Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study (TMM BirThree Cohort Study). The TMM BirThree Cohort Study is a prospective cohort study based in Miyagi and Iwate Prefectures, Japan and has been published elsewhere.13 14 Pregnant women and their family members were contacted in obstetric clinics or hospitals from 2013 to 2017, and 23 406 pregnant women participated in the study. Written informed consent was obtained from all participants. All participants were free to decline consent to participate in the research and were told that there was no disadvantage or risk involved with their refusal to participate. The TMM BirThree Cohort Study protocol was approved by the Tohoku University Tohoku Medical Megabank Organization’s internal review board (2013-1-103-1).
Infertility treatments
We extracted infertility treatment types from maternal medical records, and they included ovulation induction (OI), artificial insemination with husband’s sperm (AIH), IVF and ICSI; we refer to IVF and ICSI as ART in this study.
Neurodevelopmental assessments
The third edition of the Ages and Stages Questionnaire (ASQ-3) was used to evaluate child neurodevelopment.15 16 ASQ-3 is a comprehensive, reliable screening questionnaire that can be used for children aged 1 and 66 months. The guardians of children aged 2 and 3.5 years filled in the questionnaire. Each questionnaire contains 30 questions divided into five developmental domains: ‘communication’, ‘fine motor’, ‘gross motor’, ‘problemsolving’ and ‘personal-social’. Each domain has a set of six items, and each item is given a score of 10, 5 and 0 corresponding to ‘yes’, ‘sometimes’ and ‘not yet’, respectively. The total score ranges from 0 to 60 for each domain. We defined ‘developmental delay’ in a domain as when the score was greater than two SD below the mean in that domain.17 In this study, we used the validated Japanese translation of ASQ-3.16
Covariates
Considering previous studies and the characteristics of the population in this study, we included maternal age at delivery, parity, preterm birth (PTB), child sex, birth defects, multiple births, maternal education and household income as covariates of developmental outcomes.7 18 Maternal age, gestational weeks, parity, child sex, birth defect and multiple birth were obtained from medical records. Birth defects were defined in this study as follow: anencephaly, microcephaly, hydrocephalus, craniotabes, holoprosencephaly, agenesis of the corpus callosum, other head or brain abnormalities, omphalocele, abdominal fissure, epidermolysis bullosa hereditarian, incontinentia pigmenti, myelomeningocele, Down’s syndrome, trisomy 18, trisomy 13, achondroplasia, osteogenesis imperfecta, arthrogryposis multiplex congenita, other skeletal or muscle abnormalities, amniotic band syndrome and other chromosomal abnormality. Data on maternal level of education and household income were obtained using a self-report questionnaire.
Statistical analysis
Characteristics of mothers and children were compared in three groups: natural conception, OI/AIH and ART. Continuous and categorical variables were described as mean (SD) and frequency or proportion, respectively. Differences in prevalence were analysed using the χ2 test. Logistic regression analyses were performed to determine the associations between infertility treatment and each of the five domains of ASQ-3 at 2 and 3.5 years of age after adjusting for possible confounding factors. ORs and CIs were calculated. Children who were conceived naturally were used as the reference group in all analyses. For subgroup analyses, participants were classified into five groups as follows: natural conception, OI, AIH, IVF and ICSI. Furthermore, we compared developmental outcomes among children born following natural conception, fresh embryo transfer (ET) and frozen-thawed ET. Statistical significance was set at p<0.05. All statistical analyses were performed using SAS V.9.4 (SAS Institute, Cary, North Carolina).
Patient and public involvement
No participants were involved in this study because we used an existing data set for the analysis.
Results
Characteristics of the participants
We analysed data from 9655 eligible mother–child pairs who filled in ASQ-3 questionnaires (figure 1). Of the 9655 mother–child pairs, 273 (2.8%) were conceived through OI/AIH and 487 (5.0%) through ART. Maternal and child characteristics are shown in table 1. Mothers who were exposed to infertility treatment were older and had higher levels of educational and household income. Children who were conceived following infertility treatment were likely to have a lower birth weight (LBW) and gestational age.
Figure 1.
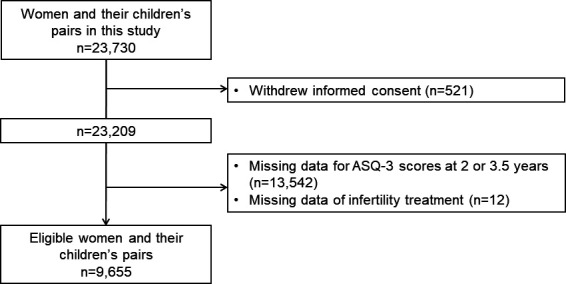
Flowchart of the exclusion criteria in the TMM BirThree Cohort Study. This flowchart describes the exclusion criteria and the number of total participants, excluded participants, and eligible participants. ASQ-3, Ages & Stages Questionnaires, Third Edition; TMM BirThree Cohort Study, Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study.
Table 1.
Characteristics of the study population
| Total | Infertility treatment | P | |||||||
| Natural conception | OI/AIH | ART | |||||||
| n=9655 | % | n=8895 | % | n=273 | % | n=487 | % | ||
| Mother’s age, mean (SD), years | 32.7 | 4.7 | 32.4 | 4.6 | 34.3 | 3.9 | 37.2 | 3.8 | <0.0001 |
| Pre-pregnancy BMI (kg/m2) | |||||||||
| <18.5 | 1365 | 14.1 | 1279 | 14.4 | 36 | 13.2 | 50 | 10.3 | 0.0707 |
| 18.5 to <25.0 | 7204 | 74.6 | 6636 | 74.6 | 196 | 72.1 | 372 | 76.3 | |
| ≧ 25.0 | 1083 | 11.2 | 977 | 11.0 | 41 | 15.0 | 65 | 13.4 | |
| Educational level | |||||||||
| High school graduate or less | 2711 | 28.1 | 2565 | 28.8 | 49 | 18.0 | 97 | 19.9 | <0.0001 |
| Junior or vocational college graduate | 3513 | 36.4 | 3215 | 36.1 | 100 | 36.6 | 198 | 40.7 | |
| University graduate or above | 2722 | 28.2 | 2457 | 27.6 | 102 | 37.4 | 163 | 33.5 | |
| Household income (JPY/year) | |||||||||
| <4 000 000 | 3117 | 32.3 | 2974 | 33.4 | 63 | 23.1 | 80 | 16.4 | <0.0001 |
| 4 000 000 to <6 000 000 | 3063 | 31.7 | 2810 | 31.6 | 86 | 31.5 | 167 | 34.3 | |
| ≥6 000 000 | 2992 | 31.0 | 2658 | 29.9 | 111 | 40.7 | 223 | 45.8 | |
| Cigarette smoking | |||||||||
| Never | 6194 | 64.6 | 5675 | 64.3 | 195 | 71.4 | 324 | 66.7 | <0.0001 |
| Stopped before pregnancy | 2291 | 23.9 | 2075 | 23.5 | 60 | 22.0 | 156 | 32.1 | |
| Stopped after pregnancy | 950 | 9.9 | 928 | 10.5 | 17 | 6.2 | 5 | 1.0 | |
| Smoked during early pregnancy | 152 | 1.6 | 150 | 1.7 | 1 | 0.4 | 1 | 0.2 | |
| Alcohol consumption | |||||||||
| Drinking at early pregnancy | 1917 | 20.0 | 1766 | 20.0 | 57 | 21.0 | 94 | 19.3 | 0.5426 |
| Former | 3273 | 34.1 | 3023 | 34.2 | 93 | 34.2 | 157 | 32.3 | |
| Never | 3871 | 40.3 | 3568 | 40.4 | 105 | 38.6 | 198 | 40.7 | |
| Cannot drink because of constitution | 536 | 5.6 | 482 | 5.5 | 17 | 6.3 | 37 | 7.6 | |
| Parity | |||||||||
| Nullipara | 4564 | 47.3 | 4024 | 45.2 | 202 | 74.0 | 338 | 69.4 | <0.0001 |
| Multipara | 5091 | 52.7 | 4871 | 54.8 | 71 | 26.0 | 149 | 30.6 | |
| Child’s sex | |||||||||
| Male | 4958 | 51.4 | 4581 | 51.5 | 137 | 50.2 | 240 | 49.3 | 0.5874 |
| Female | 4697 | 48.7 | 4314 | 48.5 | 136 | 49.8 | 247 | 50.7 | |
| Gestational age (weeks) | |||||||||
| ≥37 | 9017 | 93.4 | 8338 | 93.7 | 245 | 89.7 | 434 | 89.1 | <0.0001 |
| 34 to <37 | 482 | 5.0 | 417 | 4.7 | 26 | 9.5 | 39 | 8.0 | |
| 29 to <34 | 113 | 1.2 | 98 | 1.1 | 2 | 0.7 | 13 | 2.7 | |
| <29 | 33 | 0.3 | 32 | 0.4 | 0 | 0.0 | 1 | 0.2 | |
| Birth weight (g) | |||||||||
| ≥2500 | 8689 | 90.0 | 8037 | 90.4 | 229 | 83.9 | 423 | 86.9 | 0.0004 |
| <2500 | 952 | 9.9 | 844 | 9.5 | 44 | 16.1 | 64 | 13.1 | |
| Birth defect | |||||||||
| No | 9477 | 98.3 | 8740 | 98.4 | 269 | 98.5 | 468 | 96.1 | 0.0033 |
| Yes | 169 | 1.8 | 146 | 1.6 | 4 | 1.5 | 19 | 3.9 | |
| Multiple birth | |||||||||
| No | 9440 | 97.8 | 8746 | 98.3 | 244 | 89.4 | 450 | 92.4 | <0.0001 |
| Yes | 215 | 2.2 | 149 | 1.7 | 29 | 10.6 | 37 | 7.6 | |
| ASQ-3 (2Y) | |||||||||
| >Mean −2SD | 8218 | 85.1 | 7626 | 85.7 | 215 | 78.8 | 377 | 77.4 | <0.0001 |
| ≤Mean −2SD | 1437 | 14.9 | 1269 | 14.3 | 58 | 21.3 | 110 | 22.6 | |
| ASQ-3 (3.5Y) | |||||||||
| >Mean −2SD | 8398 | 87.0 | 7746 | 87.1 | 233 | 85.4 | 419 | 86.0 | 0.5749 |
| ≤Mean −2SD | 1257 | 13.0 | 1149 | 12.9 | 40 | 14.7 | 68 | 14.0 | |
| Father’s age, mean (SD), y | n=4183 | n=3784 | n=142 | n=257 | |||||
| 34.5 | 5.7 | 34.2 | 5.6 | 35.1 | 4.8 | 38.8 | 5.2 | <0.0001 | |
AIH, artificial insemination with husband’s semen; ART, assisted reproductive technology; ASQ-3, Ages & Stages Questionnaires, Third Edition; BMI, body mass index; OI, ovulation induction.
Infertility treatment and children’s neurodevelopment at 2 years of age
In total, 1437 children (14.9%) had developmental delay at 2 years of age when screened using the ASQ-3. The proportion of children with developmental delays at 2 years of age was 14.3%, 21.3% and 22.6% for natural conception, OI/AIH and ART, respectively. In the multivariable models, the odds of having developmental delays at 2 years of age were higher in children conceived through OI/AIH (OR, 1.36; 95% CI 1.00 to 1.85) and ART (OR, 1.36; 95% CI 1.07 to 1.72) than in those conceived naturally. OI/AIH and ART were significantly associated with communication (OR, 1.93; 95% CI 1.25 to 2.98) and gross motor (OR, 1.50; 95% CI 1.08 to 2.09) delays, respectively (table 2).
Table 2.
Odds ratios (95% CIs) from logistic regression models for infertility treatment and children’s neurodevelopment at the age of 2 and 3.5 years (n=9655)
| N | 2 years | 3.5 years | |||||||||||||||
| n | % | Crude | Adjusted | n | % | Crude | Adjusted | ||||||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | ||||||||||
| Lower | Upper | Lower | Upper | Lower | Upper | Lower | Upper | ||||||||||
| Total score | |||||||||||||||||
| Natural conception | 8895 | 1269 | 14.27 | ref | ref | 1149 | 12.92 | ref | ref | ||||||||
| OI/AIH | 273 | 58 | 21.25 | 1.62 | 1.21 | 2.18 | 1.36 | 1.00 | 1.85 | 40 | 14.65 | 1.16 | 0.82 | 1.63 | 1.13 | 0.79 | 1.61 |
| ART | 487 | 110 | 22.59 | 1.75 | 1.41 | 2.19 | 1.36 | 1.07 | 1.72 | 68 | 13.96 | 1.09 | 0.84 | 1.42 | 1.03 | 0.78 | 1.37 |
| Communication | |||||||||||||||||
| Natural conception | 8895 | 445 | 5.00 | ref | ref | 482 | 5.42 | ref | ref | ||||||||
| OI/AIH | 273 | 27 | 9.89 | 2.09 | 1.39 | 3.14 | 1.93 | 1.25 | 2.98 | 17 | 6.23 | 1.16 | 0.70 | 1.91 | 1.13 | 0.68 | 1.90 |
| ART | 487 | 27 | 5.54 | 1.12 | 0.75 | 1.66 | 0.95 | 0.62 | 1.45 | 29 | 5.95 | 1.11 | 0.75 | 1.63 | 1.04 | 0.69 | 1.56 |
| Gross motor | |||||||||||||||||
| Natural conception | 8895 | 483 | 5.43 | ref | ref | 367 | 4.13 | ref | ref | ||||||||
| OI/AIH | 273 | 20 | 7.33 | 1.38 | 0.87 | 2.19 | 1.15 | 0.72 | 1.85 | 16 | 5.86 | 1.45 | 0.86 | 2.42 | 1.26 | 0.74 | 2.13 |
| ART | 487 | 49 | 10.06 | 1.95 | 1.43 | 2.65 | 1.50 | 1.08 | 2.09 | 25 | 5.13 | 1.26 | 0.83 | 1.91 | 1.03 | 0.67 | 1.60 |
| Fine motor | |||||||||||||||||
| Natural conception | 8895 | 389 | 4.37 | ref | ref | 513 | 5.77 | ref | ref | ||||||||
| OI/AIH | 273 | 17 | 6.23 | 1.45 | 0.88 | 2.40 | 1.28 | 0.76 | 2.13 | 19 | 6.96 | 1.22 | 0.76 | 1.97 | 1.20 | 0.74 | 1.96 |
| ART | 487 | 34 | 6.98 | 1.64 | 1.14 | 2.36 | 1.27 | 0.86 | 1.86 | 31 | 6.37 | 1.11 | 0.76 | 1.62 | 1.05 | 0.71 | 1.56 |
| Problem solving | |||||||||||||||||
| Natural conception | 8895 | 354 | 3.98 | ref | ref | 505 | 5.68 | ref | ref | ||||||||
| OI/AIH | 273 | 13 | 4.76 | 1.21 | 0.68 | 2.13 | 0.90 | 0.50 | 1.60 | 18 | 6.59 | 1.17 | 0.72 | 1.91 | 1.20 | 0.73 | 1.99 |
| ART | 487 | 32 | 6.57 | 1.70 | 1.17 | 2.47 | 1.18 | 0.79 | 1.75 | 27 | 5.54 | 0.98 | 0.66 | 1.45 | 0.91 | 0.60 | 1.38 |
| Personal-social | |||||||||||||||||
| Natural conception | 8895 | 449 | 5.05 | ref | ref | 400 | 4.5 | ref | ref | ||||||||
| OI/AIH | 273 | 24 | 8.79 | 1.81 | 1.18 | 2.79 | 1.46 | 0.93 | 2.28 | 16 | 5.86 | 1.32 | 0.79 | 2.21 | 1.20 | 0.70 | 2.04 |
| ART | 487 | 42 | 8.62 | 1.78 | 1.28 | 2.47 | 1.25 | 0.88 | 1.77 | 28 | 5.75 | 1.30 | 0.87 | 1.92 | 1.05 | 0.69 | 1.60 |
Multivariable logistic models were adjusted for maternal age, parity, gestational week (<37 weeks), child sex, birth defect, multiple birth, maternal education level and household income.
AIH, artificial insemination with husband’s semen; ART, assisted reproductive technology; OI, ovulation induction.
Infertility treatment and children’s neurodevelopment at 3.5 years of age
In total, 1257 children (13.0%) had developmental delay at 3.5 years of age when screened using the ASQ-3. The proportion of children with developmental delay at 3.5 years of age was 12.9%,14.7% and 14.0% for natural conception, OI/AIH and ART, respectively. In the multivariable models, the odds of having developmental delays at 3.5 years of age were higher in children conceived through OI/AIH (OR, 1.13; 95% CI 0.79 to 1.61) and ART (OR, 1.03; 95% CI 0.78 to 1.37) than in those conceived naturally. Moreover, children conceived through infertility treatment had no statistically significant differences in any domains at 3.5 years of age (table 2).
Subgroups based on the five domains and embryo types were analysed and the results are shown in online supplemental tables S1-S4. Although the number of children conceived through each infertility treatment was less, the results, when compared within the five groups or types of ET, were similar to those within the three groups.
bmjopen-2022-060944supp001.pdf (135KB, pdf)
Discussion
We investigated the association between infertility treatment and children’s neurodevelopment, among 9655 mother–child pairs. In multivariable models, a significant association between infertility treatment and neurodevelopment was observed among the children conceived through infertility treatment, at 2 years of age; no statistically significant differences were found in them at 3.5 years of age.
Children conceived through ART are known to be at risk of LBW, PTB and birth defects,19 which are risk factors for neurodevelopmental disorders.20 21 However, the data from previous studies among children aged 1–5 years suggest that there are no developmental differences between children conceived through ART and those conceived naturally, after adjusting for confounding variables.3 19 22 Even when children with congenital anomalies or genetic syndromes and multiple births (which are known to affect development) were excluded from the study (n=9271), a significant association between infertility treatment and children’s neurodevelopment was seen at 2 years of age, while no statistically significant differences were found at 3.5 years of age (online supplemental table S5). Furthermore, we took into account very preterm (<34 weeks) or extremely preterm (<29 weeks) birth for adjusting the results for important risk factors and the similar result was obtained (online supplemental table S6). We also performed analysis adjusted for birth weight and the similar result was obtained (online supplemental table S7). A systematic review of neurodevelopmental disorders,5 neuromotor, cognitive, language, and behavioural outcomes of children born after ART showed that ART had no significant effect on children’s neuromotor and cognitive development.6 A previous study showed no significant difference in the neurodevelopmental scores between children conceived through ART and those conceived naturally; however, it showed a decrease in the score units of each scale among children conceived through ART.23 The reason for the discrepancy in results at 2 years of age between our study and the previous study might be the proportion of children conceived through infertility treatment. Because infertility treatment has become widespread owing to technological advancement, the proportion of children conceived through infertility treatment was higher in our study than in previous studies.24–26 Therefore, statistical differences might be detectable in our study. In addition, frozen-thawed embryos have been used for most ARTs in Japan.27 Frozen-thawed ET is associated with a significantly lower incidence of PTB and LBW, which are risk factors for neurodevelopmental disorders.28 Among children with developmental delay at 2 years of age, the proportion with developmental delay at 3.5 years of age was 47.3%,46.6% and 38.5% for natural conception, OI/AIH and ART, respectively. The proportion of children with developmental delay at 3.5 years of age was low, especially in those conceived through ART. Our longitudinal study demonstrated that at 2 and 3.5 years of age, the neurodevelopmental status of children conceived through infertility treatment, especially ART, might eventually catch up with that of those conceived naturally. In Japan, the health check-up for children is done at 1.5 years of age, so the counsel provided by doctors and public health nurses, which is tailored towards individual development, might also help promote the children’s development. A previous study in Japan stated that the developmental state of a child needs to be understood not only based on the characteristics of the child at one point but also on the progress of the child’s development from the results of the health check-up at 1.5 years of age. In fact, it has been suggested that it is important to conduct a follow-up health check-up at 3 years of age in relation to the development at the previous age.29
Developmental delay in the communication domain was seen at age 2 years in children conceived through OI/AIH but not in those conceived through ART. A previous study showed that compared with children conceived naturally, those conceived through OI had lower verbal ability at 3 years of age, while those conceived through ART had higher verbal ability; children conceived through infertility treatment had higher verbal ability at 5 years of age than those conceived naturally.30 A previous hospital-based cohort study in Japan showed that children conceived through ART had significantly better language development than those conceived naturally.7 Although direct comparisons with other studies assessing neurodevelopment in children conceived through infertility treatment are difficult because each researcher uses various assessment tools and control groups, the children conceived through ART might have higher verbal ability or better language development than those conceived through OI/AIH or naturally. Children conceived through infertility treatments generally enjoy advantageous socioeconomic benefits. It is possible that parents who use ART to conceive may invest more into rearing the children, which might have the greatest impact on language skills.7 30 31
Furthermore, ART was associated with developmental delays in the gross motor domain at 2 years of age. This association was not seen at 3.5 years of age. A hospital-based cohort study in Japan reported no significant difference in gross motor function (evaluated using the Ability for Basic Movement Scale for Children) at 12 months of age between the ART and control groups.32 In contrast, the Danish National Birth Cohort study showed that infertility treatment, especially ICSI, may be associated with a slight delay in gross motor development at 1.5 years of age.8 However, another study suggested no differences in motor development at 5 years of age among children conceived through ICSI, IVF and natural conception.33 These findings suggest that infertility treatment might be associated with children’s development in the early stage, but the neurodevelopment of children conceived through infertility treatment might catch up with that of those conceived naturally.
This study had some limitations. The ASQ-3 is a screening tool (not a diagnostic tool) for developmental delays; however, it is considered to be highly reliable because it has been validated in many countries worldwide and has been used in a variety of studies.18 34 35 Since we focused on children who filled in both questionnaires (at 2 and 3.5 years of age), there was the concern of bias due to the reduced number of participants and the deterioration of statistical power in the analysis. However, among the children who did not fill in the questionnaire at 3.5 years of age, the percentage of those who had neurodevelopmental delay at 2 years of age was 14.5%,10.8% and 15.0% for natural conception, OI/AIH and ART, respectively. Therefore, there was no bias such as more children with neurodevelopmental delay at 2 years of age among children who did not answer the questionnaire at 3.5 years old and the potential applicability of our results to national populations can be discussed. In the subgroup analysis with detailed classification, the number of children conceived through specific forms of infertility treatment, such as fresh ET, was insufficient to compare the ET types. Male infertility or the time to pregnancy should be taken into account when evaluating subfertility patients.36 However, it was difficult to include these factors because we did not collect them in this study. Research in this field is complex because of the need to collect various data to determine the effects of infertility treatment on offspring outcomes. As this was an observational study, residual confounding might have occurred. However, this study was a large longitudinal birth cohort with detailed information from the participants, and although continued follow-up of children born after infertility treatment is needed, this study helps to increase the understanding of the association between infertility treatment and neurodevelopmental outcomes in Japanese children.
Conclusion
In this study, we found a significant association between infertility treatment and neurodevelopment among children who were conceived through infertility treatments and those conceived naturally, at 2 years of age; however, no statistically significant differences were found at 3.5 years of age.
Supplementary Material
Acknowledgments
We are sincerely grateful to all participants of the TMM BirThree Cohort Study and the staff members of the Tohoku Medical Megabank Organization, Tohoku University. A full list of members is available at https://www.megabank.tohoku.ac.jp/english/a210901/.
Footnotes
Contributors: S.Kuri supervised this study and is the guarantor. AN, MI TaO and S.Kuri designed the study. AN, MI, TaO, KM, FU, FM, ToO, ZW, NS, NI, HH, MT, MS, JS, S.Kure, NY and S.Kuri contributed to data collection. AN, MI and TO contributed to data analysis and interpretation. AN, MI, TaO, KM, FU, FM, ToO, ZW, NS, NI, HH, TatO, MT, HT, MS, JS, S.Kure, NY and S.Kuri provided advice regarding critically important intellectual content and helped to draft the manuscript. All authors approved submission of this manuscript.
Funding: The TMM BirThree Cohort Study was supported by the Japan Agency for Medical Research and Development (AMED), Japan [grant number, JP17km0105001, JP21tm0124005, JP19gk0110039].
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available upon reasonable request. The data obtained through the TMM BirThree Cohort Study are incorporated into the TMM Biobank. All data analysed during the present study are available for research purpose with the approval by the Sample and Data Access Committee of the Biobank.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
The TMM BirThree Cohort Study protocol was approved by the Tohoku University Tohoku Medical Megabank Organization’s internal review board (2013-1-103-1). Participants gave informed consent to participate in the study before taking part.
References
- 1.Frederiksen Y, Farver-Vestergaard I, Skovgård NG, et al. Efficacy of psychosocial interventions for psychological and pregnancy outcomes in infertile women and men: a systematic review and meta-analysis. BMJ Open 2015;5:e006592. 10.1136/bmjopen-2014-006592 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Japan Society of obstetrics and gynecology (in Japanese). Available: https://plaza.umin.ac.jp/~jsog-art/2018data_20201001.pdf [Accessed 31 Dec 2021].
- 3.Wilson CL, Fisher JR, Hammarberg K, et al. Looking downstream: a review of the literature on physical and psychosocial health outcomes in adolescents and young adults who were conceived by art. Hum Reprod 2011;26:1209–19. 10.1093/humrep/der041 [DOI] [PubMed] [Google Scholar]
- 4.Sullivan-Pyke CS, Senapati S, Mainigi MA, et al. In vitro fertilization and adverse obstetric and perinatal outcomes. Semin Perinatol 2017;41:345–53. 10.1053/j.semperi.2017.07.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Djuwantono T, Aviani JK, Permadi W, et al. Risk of neurodevelopmental disorders in children born from different art treatments: a systematic review and meta-analysis. J Neurodev Disord 2020;12:33. 10.1186/s11689-020-09347-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Middelburg KJ, Heineman MJ, Bos AF, et al. Neuromotor, cognitive, language and behavioural outcome in children born following IVF or ICSI-a systematic review. Hum Reprod Update 2008;14:219–31. 10.1093/humupd/dmn005 [DOI] [PubMed] [Google Scholar]
- 7.Aoki S, Hashimoto K, Ogawa K, et al. Developmental outcomes of Japanese children born through assisted reproductive technology (art) in toddlerhood. J Obstet Gynaecol Res 2018;44:929–35. 10.1111/jog.13613 [DOI] [PubMed] [Google Scholar]
- 8.Zhu JL, Basso O, Obel C, et al. Infertility, infertility treatment and psychomotor development: the Danish national birth cohort. Paediatr Perinat Epidemiol 2009;23:98–106. 10.1111/j.1365-3016.2008.00989.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Catford SR, McLachlan RI, O'Bryan MK, et al. Long-term follow-up of intra-cytoplasmic sperm injection-conceived offspring compared with in vitro fertilization-conceived offspring: a systematic review of health outcomes beyond the neonatal period. Andrology 2017;5:610–21. 10.1111/andr.12369 [DOI] [PubMed] [Google Scholar]
- 10.Punamäki R-L, Tiitinen A, Lindblom J, et al. Mental health and developmental outcomes for children born after art: a comparative prospective study on child gender and treatment type. Hum Reprod 2016;31:100–7. 10.1093/humrep/dev273 [DOI] [PubMed] [Google Scholar]
- 11.Sutcliffe AG, Ludwig M. Outcome of assisted reproduction. Lancet 2007;370:351–9. 10.1016/S0140-6736(07)60456-5 [DOI] [PubMed] [Google Scholar]
- 12.Hvidtjørn D, Schieve L, Schendel D, et al. Cerebral palsy, autism spectrum disorders, and developmental delay in children born after assisted conception: a systematic review and meta-analysis. Arch Pediatr Adolesc Med 2009;163:72–83. 10.1001/archpediatrics.2008.507 [DOI] [PubMed] [Google Scholar]
- 13.Kuriyama S, Metoki H, Kikuya M, et al. Cohort profile: Tohoku medical Megabank project birth and three-generation cohort study (TMM BirThree cohort study): rationale, progress and perspective. Int J Epidemiol 2020;49:18–19. 10.1093/ije/dyz169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ishikuro M, Obara T, Osanai T, et al. Strategic methods for recruiting grandparents: the Tohoku medical Megabank birth and three-generation cohort study. Tohoku J Exp Med 2018;246:97–105. 10.1620/tjem.246.97 [DOI] [PubMed] [Google Scholar]
- 15.Singh A, Yeh CJ, Boone Blanchard S. Ages and stages questionnaire: a global screening scale. Bol Med Hosp Infant Mex 2017;74:5–12. 10.1016/j.bmhimx.2016.07.008 [DOI] [PubMed] [Google Scholar]
- 16.Mezawa H, Aoki S, Nakayama SF, et al. Psychometric profile of the ages and stages questionnaires, Japanese translation. Pediatr Int 2019;61:1086–95. 10.1111/ped.13990 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Squires J, Twombly E, Bricker D. B. As Q®-3 User’s Guide. 3rd ed. Baltimore, MD: Brookes, 2009. [Google Scholar]
- 18.Yeung EH, Sundaram R, Bell EM, et al. Examining infertility treatment and early childhood development in the upstate kids study. JAMA Pediatr 2016;170:251–8. 10.1001/jamapediatrics.2015.4164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vuong LN, Ly TT, Nguyen NA, et al. Development of children born from freeze-only versus fresh embryo transfer: follow-up of a randomized controlled trial. Fertil Steril 2020;114:558–66. 10.1016/j.fertnstert.2020.04.041 [DOI] [PubMed] [Google Scholar]
- 20.Helmerhorst FM, Perquin DAM, Donker D, et al. Perinatal outcome of singletons and twins after assisted conception: a systematic review of controlled studies. BMJ 2004;328:261. 10.1136/bmj.37957.560278.EE [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jackson RA, Gibson KA, Wu YW, et al. Perinatal outcomes in singletons following in vitro fertilization: a meta-analysis. Obstet Gynecol 2004;103:551–63. 10.1097/01.AOG.0000114989.84822.51 [DOI] [PubMed] [Google Scholar]
- 22.Basatemur E, Sutcliffe A. Follow-Up of children born after art. Placenta 2008;29 Suppl B:135–40. 10.1016/j.placenta.2008.08.013 [DOI] [PubMed] [Google Scholar]
- 23.Balayla J, Sheehy O, Fraser WD, et al. Neurodevelopmental outcomes after assisted reproductive technologies. Obstet Gynecol 2017;129:265–72. 10.1097/AOG.0000000000001837 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dyer S, Chambers GM, de Mouzon J, et al. International Committee for monitoring assisted reproductive technologies world report: assisted reproductive technology 2008, 2009 and 2010. Hum Reprod 2016;31:1588–609. 10.1093/humrep/dew082 [DOI] [PubMed] [Google Scholar]
- 25.de Mouzon J, Chambers GM, Zegers-Hochschild F, et al. International Committee for monitoring assisted reproductive technologies world report: assisted reproductive technology 2012†. Hum Reprod 2020;35:1900–13. 10.1093/humrep/deaa090 [DOI] [PubMed] [Google Scholar]
- 26.Adamson GD, de Mouzon J, Chambers G. International Committee for monitoring assisted reproductive technology. world report on assisted reproductive technology. ICMART world Collab Rep assist Reprod Technol (art), 2017. Available: https://secureservercdn.net/198.71.233.206/3nz.654.myftpupload.com/wp-content/uploads/ICMART-ESHRE-WR2017-Preliminary.pdf [Accessed 31 Dec 2021].
- 27.Ishihara O, Jwa SC, Kuwahara A, et al. Assisted reproductive technology in Japan: a summary report for 2017 by the ethics Committee of the Japan Society of obstetrics and gynecology. Reprod Med Biol 2020;19:3–12. 10.1002/rmb2.12307 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ishihara O, Araki R, Kuwahara A, et al. Impact of frozen-thawed single-blastocyst transfer on maternal and neonatal outcome: an analysis of 277,042 single-embryo transfer cycles from 2008 to 2010 in Japan. Fertil Steril 2014;101:128–33. 10.1016/j.fertnstert.2013.09.025 [DOI] [PubMed] [Google Scholar]
- 29.Hongo K, Yagi S, Kono A. The Research on Follow-up Children’s Feature in Health Checkup for 3-year-old Children (in Japanese). Pediatr Health Res 2006;65:806–13. [Google Scholar]
- 30.Carson C, Kelly Y, Kurinczuk JJ, et al. Effect of pregnancy planning and fertility treatment on cognitive outcomes in children at ages 3 and 5: longitudinal cohort study. BMJ 2011;343:d4473. 10.1136/bmj.d4473 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lugo-Gil J, Tamis-LeMonda CS. Family resources and parenting quality: links to children's cognitive development across the first 3 years. Child Dev 2008;79:1065–85. 10.1111/j.1467-8624.2008.01176.x [DOI] [PubMed] [Google Scholar]
- 32.Hashimoto K, Ogawa K, Horikawa R, et al. Gross motor function and general development of babies born after assisted reproductive technology. J Obstet Gynaecol Res 2016;42:266–72. 10.1111/jog.12898 [DOI] [PubMed] [Google Scholar]
- 33.Ponjaert-Kristoffersen I, Bonduelle M, Barnes J, et al. International collaborative study of intracytoplasmic sperm injection-conceived, in vitro fertilization-conceived, and naturally conceived 5-year-old child outcomes: cognitive and motor assessments. Pediatrics 2005;115:e283–9. 10.1542/peds.2004-1445 [DOI] [PubMed] [Google Scholar]
- 34.Chong KC, Zhou VL, Tarazona D, et al. ASQ-3 scores are sensitive to small differences in age in a Peruvian infant population. Child Care Health Dev 2017;43:556–65. 10.1111/cch.12469 [DOI] [PubMed] [Google Scholar]
- 35.Agarwal PK, Xie H, Sathyapalan Rema AS, et al. Evaluation of the Ages and Stages Questionnaire (ASQ 3) as a developmental screener at 9, 18, and 24 months. Early Hum Dev 2020;147:105081. 10.1016/j.earlhumdev.2020.105081 [DOI] [PubMed] [Google Scholar]
- 36.Esteves SC, Roque M, Bedoschi G, et al. Intracytoplasmic sperm injection for male infertility and consequences for offspring. Nat Rev Urol 2018;15:535–62. 10.1038/s41585-018-0051-8 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2022-060944supp001.pdf (135KB, pdf)
Data Availability Statement
Data are available upon reasonable request. The data obtained through the TMM BirThree Cohort Study are incorporated into the TMM Biobank. All data analysed during the present study are available for research purpose with the approval by the Sample and Data Access Committee of the Biobank.