

Abstract
There is a dearth of research examining how individual-level and systemic racism may lead to elevated diagnostic and symptom rates of paranoia in Black Americans. The present study employed item response theory methods to investigate item- and subscale-level functioning in the Schizotypal Personality Questionnaire (SPQ) in 388 Black and 450 White participants across the schizophrenia-spectrum (i.e., non-psychiatric controls, individuals with schizophrenia, schizoaffective disorder, or schizotypal personality disorder). It was predicted that (1) Black participants would score significantly higher than Whites on the Suspiciousness and Paranoid Ideation subscale of the SPQ, while controlling for total SPQ severity and relevant demographics and (2) Black participants would endorse these subscale items at a lower latent severity level (i.e., total SPQ score) compared to Whites. Generalized linear modeling showed that Black participants endorsed higher scores on subscales sampling paranoia (e.g., Suspiciousness and Paranoid Ideation), while White participants surprisingly, endorsed higher rates within disorganized/positive symptomatology subscales (e.g., Odd or Eccentric Behavior). IRT analyses showed that Black individuals also endorse items within the Suspiciousness and Paranoid Ideation subscale at lower latent severity levels, leading to inflated subscale scores when compared to their White counterparts. Results indicate prominent race effects on self-reported paranoia as assessed by the SPQ. This study provides foundational data to parse what could be normative endorsements of paranoia versus indicators of clinical risk in Black Americans. Implications and recommendations for paranoia research and assessment are discussed.
“[One problem with] being black in America is that you have to spend so much time thinking about stuff that most white people just don’t even have to think about. I worry when I get pulled over by a cop…I worry what some white cop is going to think when he walks over to our car, because he’s holding on to a gun. I worry when I walk into a store, that someone’s going to think I’m in there shoplifting. And I have to worry about that because I’m not free to ignore it. And so, that thing that’s supposed to be guaranteed to all Americans, the freedom to just be yourself is a fallacious idea.” – Feagin, 1991
Keywords: Racial Disparities, Schizotypal Personality Questionnaire, Paranoia, Stigma, Black/African American, Schizophrenia Spectrum
1. Introduction
The threats and actions of physical harm in recent national events (i.e., police profiling and excessive use of force) and histories of implicit expressions of racism in everyday environments (i.e., workplace and housing discrimination) that disproportionately impact Black Americans has garnered global attention. Ethnographic examination of the effects of implicit and explicit forms of racism on Black Americans’ thoughts and behaviors (see above quotation), brings to light the notion of racism-related vigilance, whereby marginalized individuals proactively prepare to be discriminated against based on their race and express increased worry or attention towards potential threats in their environment (Feagin, 1994; Hines, 2017). Given long-standing racism within the United States and its influence on the Black American psyche, it is perhaps unsurprising that one outcome is the development of adaptive paranoia in marginalized individuals, consisting of high levels of suspiciousness and distrustfulness of others, independent of mental or physical health status (Grier and Cobbs, 1980; Mosley et al., 2017). In fact, research on the influence of these race-based threats on behavioral, cognitive, and affective responses has yielded a common theme: a healthy cultural paranoia (adaptive paranoia) in Black individuals (Mosley et al., 2017; Sue et al., 2008; Whaley, 2001). According to Mosley and colleagues (2017), “This ‘paranoia’ reflects the heightened, yet appropriate level of awareness Blacks have regarding how they are perceived by others and the consequences of their actions given their marginalized identity.” This research, accompanied by work parsing cultural (nonclinical) from clinical paranoia in Black Americans (Combs et al., 2006), supports a framework to contextualize individual paranoia as falling along a continuum. Collectively, this literature provides compelling indications that normative levels of paranoia may be heightened in Black individuals, as an adaptive response to both individual-level and structural systems of racial oppression within America. That is, the threshold between normative and maladaptive may be shifted towards higher levels of paranoia in Black Americans.
Notably, paranoia is a feature of a variety of clinical disorders, including psychotic disorders and some personality disorders. Black Americans are 3–4 times more likely to receive a diagnosis of a psychotic disorder (2.4 times for schizophrenia specifically) (Olbert et al., 2018; Schwartz and Blankenship, 2014) and disproportionately higher rates of schizotypal personality disorder (SPD) compared to their White counterparts (Chavira et al., 2003). Generally, worry has been identified as a causal factor in the maintenance of clinical paranoia (Sheffield et al., 2021; Startup et al., 2016). In Black Americans specifically, perceived racism is a predictor of non-clinical paranoia (Combs at el., 2006). Thus, in Black Americans, worry may be compounded with racially motivated psychosocial stressors, such as major discriminatory events, which place Blacks at higher risk for psychotic experiences (Oh et al., 2016). Concerningly, there has been scarce examination of whether commonly employed assessments sampling paranoia in marginalized groups (both in research and clinical contexts) are sensitive in differentiating whether the expression of these traits is pathological or adaptive, which may have major implications for intervention targets. It is possible that the elevated diagnostic rate of psychosis in Black Americans is produced by the confluence and confusion of illness-related clinical paranoia with adaptive paranoia caused by systemic racial bias.
In an attempt to fill this gap, the current work uses a widely adopted measure of schizotypal personality to examine how race and diagnostic status may differentially impact self-reported paranoia. The Schizotypal Personality Questionnaire (SPQ) (Raine, 1991) is a commonly used self-report instrument of schizotypal personality traits in relation to the nine features of schizotypal personality disorder outlined by the DSM-III, including: Suspiciousness and Paranoid Ideation, No Close Friends, Constricted Affect, Ideas of Reference, Odd beliefs or Magical Thinking, Unusual Perceptual Experiences, Odd or Eccentric Behavior, Odd Speech, and Excessive Social Anxiety (Raine, 1991). Though originally designed as a screening tool and research instrument to assess SPD risk, the SPQ has also been implemented in study designs to characterize the underlying personality features that relate to core phenomenology expressed in psychotic disorders (Brosey and Woodward, 2015). For example, multiple studies have reported that individuals with schizophrenia and those with genetic risk for psychotic disorders have higher endorsements of SPQ items compared to controls (Moreno-Izco et al., 2015; Yaralian et al., 2000). Additional longitudinal work using other measures of schizotypal traits has shown that healthy individuals with higher endorsements of schizotypal traits are at increased risk of developing a schizophrenia-spectrum disorder later in life (Chapman et al., 1994). Although widely employed and highly impactful within the field, it should be noted that the SPQ was developed and validated using undergraduate students at an Ivy League institution and the racial breakdown of samples were not described (Raine, 1991; Raine, 1994).
Although a number of cross-cultural studies have examined item performance and measurement invariance of the SPQ across ethnic and racial groups (British/Trinidadian sample, Barron et al., 2015; Spanish/Swiss sample, Ortuno-Sierra et al., 2013; Mauritian sample, Reynolds et al., 2000), these studies did not specifically compare marginalized verses non-marginalized groups (i.e., groups that may systematically differ in their experiences of discrimination and inequality) within their respective cultural contexts. In the only known study to examine measurement invariance of the SPQ across racial groups that differ in marginalized vs. non-marginalized group affiliation within the United States, Cicero (2015) found scalar invariance in the Suspiciousness and Paranoid Ideation and Ideas of Reference domains between Whites (non-marginalized group) and Asian Pacific Islanders (marginalized group) residing in Hawaii. The dearth of research on the utility of the SPQ in Black Americans is concerning given the likelihood of individual-level and/or systemic racism driving heightened, yet adaptive, levels of paranoia in this group. This previous work is also limited by examination of subscale-level rather than item-level differences within this measure. A close inspection of item-level differences within domains of the SPQ may provide insight regarding heightened (yet normative) endorsements of paranoia and suspiciousness in marginalized racial groups within the United States, without being susceptable to potential masking effects seen in the analysis of composite subscale scores. Solely focusing on differential item functioning may be oversensitive to identifying item-specific differences across groups, with little to no practical importance at the test level (Chalmers et al., 2016; DeMars, 2011). For example, if half the items show slight bias to Group A and half show slight bias to Group B, there is likely very little practical impact when scoring. In contrast, leveraging the use of differential test functioning (DTF) allows researchers to quantify the aggregate effects of item-level bias within a subscale to examine whether the presence of bias creates a clinically meaningful difference in test level performance (Chalmers et al., 2016). Ultimately, DTF analyses provide a more robust evaluation of a given measure’s overall performance across groups and can demonstrate the practical impact of the bias uncovered in comparison to DIF.
Accordingly, the current study employed an item response theory (IRT) approach in the SPQ for Black and White Americans across the schizophrenia-spectrum to rigorously examine group differences in item parameters and the possible aggregation of bias across items within each subscale of the measure (DTF). The SPQ is well suited to explore these item- and subscale-level questions due to its content breadth (9 schizotypal features) and severity depth (i.e., ‘I get anxious when meeting people for the first time’ [low severity] vs. ‘I sometimes avoid going places where there will be many people because I will get anxious’ [high severity]). This breadth allows for the investigation of feature-specific (e.g., Suspiciousness and Paranoid Ideation, a subscale of the SPQ) effects. In tandem, the measure severity depth allows the model to capture transitions across the schizophrenia-spectrum. This allows for the examination of how possible bias influences the assessment of individuals of moderate severity levels, who are most likely to be at risk for improper classification (i.e., near diagnostic thresholds). This is particularly important, given the possibility of mischaracterized levels of psychopathology and increased rates of false positives in the identification of pathological suspiciousness and paranoia in Black individuals.
The current work examined subscale item functioning in the SPQ between Black and White participants (n= 838, 388 Black, 450 White) across the schizophrenia-spectrum. It was predicted that Black individuals would endorse SPQ Suspiciousness and Paranoid Ideation items at higher rates compared to their White counterparts when controlling for overall schizotypal personality trait severity. This would provide preliminary evidence that Black individuals may endorse paranoia due to processes not properly accounted for in our measures.
2. Methods
2.1. Participants
Analyses were performed on a total sample of 838 (388 Black, 450 White) individuals. Three hundred and thirty-two (110 Black, 222 White) individuals had no current or past psychiatric diagnosis and no familial history of psychosis. Per Structured Clinical Interviews for DSM-IV (SCID-I and SCID-II (First et al., 2002; First et al., 1997)), Mini International Neuropsychiatric Interview (MINI, (Maxwell, 1992)), and if needed medical records, 320 (185 Black, 135 White) individuals had a formal diagnosis on the schizophrenia spectrum (i.e., schizophrenia, schizoaffective disorder, or schizotypal personality disorder [SPD]), 95 (55 Black, 40 White) individuals presented with subthreshold SPD (some SPD symptoms per the SCID-II criteria, but fewer than the required 5 features to meet diagnostic threshold) and relatives of individuals with psychosis (hereto forward referred to as “high risk”), and 91 (38 Black, 53 White) individuals with a non-schizophrenia spectrum diagnosis (e.g., mood, anxiety, or substance; hereto forward referred to as “psychiatric control”) (Table 1). Inclusion/exclusion criteria followed Moussa-Tooks et al. (2020), as data from this sample was previously analyzed in order to examine the bifactor structure of the SPQ across the schizophrenia-spectrum. The high risk and psychiatric control groups were included to provide increased coverage of the full severity spectrum. Individuals who self-identified as Black/African-American or White were included in the analyses. Ninety-six individuals who listed their race as Hispanic, Asian, or Other, were not included as this small sample size would not support a well-powered analysis of these groups. Participant socioeconomic status (SES) was represented using a factor score generated from indicators of personal and maternal employment status and personal, maternal and paternal educational attainment level. Paternal employment was dropped from this measure due to low correlations with other indicators (Supplementary materials).
Table 1.
Demographics
| Full Sample Comparison | ||||
|
| ||||
| White Total (n=450) | Black Total (n=388) | Statistics (t or χ2)* | p-value * | |
| Sex (male/female) | 224/226 | 224/164 | 4.99 | 0.03 |
| Age Years, SD | 37.82(11.37) | 39.56(11.39) | 2.21 | 0.03 |
| Education Years, SD | 14.49(3.10) | 12.29(2.54) | 10.10 | < 0.01 |
|
| ||||
| White Participant Group | ||||
| Control (n=222) | SZ-Spectrum (n=135) | High Risk (n=40) | Psychiatric Control (n=53) | |
| Sex (male/female) | 96/126 | 78/57 | 15/25 | 35/18 |
| Age Years, SD | 36.50(11.21) | 37.43(11.13) | 40.78(13.05) | 42.11(10.11) |
| Education Years, SD | 15.47(2.50) | 13.39(3.27) | 15.04(4.06) | 13/68(2.60) |
| Black Participant Group | ||||
| Control (n=110) | SZ-Spectrum (n=185) | High Risk (n=55) | Psychiatric Control (n=38) | |
| Sex (male/female) | 59/51 | 116/69 | 24/31 | 25/13 |
| Age Years, SD | 37.19(11.77) | 40.08(11.07) | 40.14(12.62) | 43.03(8.71) |
| Education Years, SD | 13.42(2.98) | 11.95(2.44) | 11.69(1.88) | 12.02(1.88) |
Control = individuals with no current or past psychiatric diagnosis, SZ-Spectrum = individuals on the schizophrenia spectrum (i.e., schizophrenia, schizoaffective disorder, or schizotypal personality disorder [SPD]), High Risk = individuals with subthreshold SPD and relatives of individuals with psychosis, Psychiatric Control = individuals with a non-schizophrenia spectrum diagnosis (e.g., mood, anxiety, or substance).
Comparison between full sample within White and Black Participant groups.
2.2. Schizotypal Personality Questionnaire (SPQ)
The 74-item, yes/no paper-pencil version of the SPQ was administered. One point is designated to each ‘yes’ and 0 points to each ‘no’ response. No response, multiple responses, or written responses were considered invalid and treated as missing data (see 2.4.5.).
2.3. Statistical Analyses
R version 3.6.1 (R Core Team, 2013) was used for these analyses including the “missForest” package for data imputation (Stekhoven and Buhlmann, 2012), “lavaan” package for Confirmatory Factor Analysis (Rosseel, 2012), “mirt” package for item-response theory analysis (Chalmers, 2012), and “ggplot” package for data visualization and figure generation (Wickham, 2016).
2.3.1. Generalized Linear Models
Item response rates were examined between Black and White participant groups within each subscale. Subsequently, generalized linear models (GLM) were used to probe for race effects at the subscale-level to identify subscales to be examined in more detail with item response theory (IRT) analyses. GLM models aid in the identification of subscales with prominent race effects and subsequent IRT analyses allow for further examination of the individual items driving the effect, in addition to the schizotypal trait levels where the effects are most prominent. Each subscale score was predicted by SPQ total score, race, age, sex, and socioeconomic status (SES). These models allowed for the identification of race effects in subscale performance, while controlling for total SPQ severity and other relevant demographic factors. Subscales and total score were normalized to provide ease of comparison across subscales that contain different numbers of items. There were no significant interactions between race and SPQ total score and therefore interactions were dropped from the GLM models.
2.3.2. Selection of Anchor Items
A necessary initial step in conducting DTF analyses is the selection of “anchor” items (i.e., items that perform similarly across comparison groups) to allow estimated item parameters across different groups to be placed on a common scale to allow for meaningful comparison (Kopf et al., 2015). Subscales that did not exhibit significant race effects in the GLMs (Table 2) were therefore examined at the item-level using unidimensional IRT models, to identify items that performed nearly identically across groups (i.e., free of DIF). Selected anchor items were then used in subsequent testing of items within subscales with expected DTF across racial groups, as suggested by previous GLM results (cf. Supplementary materials for full anchor item selection description).
Table 2.
Generalized Linear Model
| Black Participant Group | ||||
|---|---|---|---|---|
|
| ||||
| Subscale | Estimated Race Effect* | Standard Error | t-value | p-value |
| Suspiciousness and Paranoid Ideation | 0.289 | 0.034 | 8.476 | <0.001 |
| Ideas of Reference | 0.226 | 0.037 | 6.143 | <0.001 |
| Odd Beliefs and Magical Thinking | −0.182 | 0.058 | −3.165 | 0.002 |
| Odd or Eccentric Behavior | −0.221 | 0.042 | −5.223 | <0.001 |
| Odd Speech | −0.219 | 0.040 | −5.477 | <0.001 |
| Social Anxiety | −0.105 | 0.046 | −2.298 | 0.022 |
| Constricted Affect | 0.051 | 0.044 | 1.142 | 0.254 |
| Unusual Perceptions | 0.007 | 0.042 | 0.171 | 0.864 |
| No Close Friends | 0.070 | 0.043 | 1.607 | 0.108 |
Subscales and total score were normalized to provide ease of comparison across subscales that contain different numbers of items.
Estimated Race Effect reflects deflection of Black participant group from White participant group. Positive values indicate that Black participants scored higher than White participants, whereas negative values indicate that White participants scored higher than Black participants.
2.3.3. Establishing Unidimensionality of IRT Models
After identification of the anchor item set, analyses were conducted to assess the appropriateness of using unidimensional IRT models (Bonifay et al., 2015). First, a series of bifactor confirmatory factor analyses (CFA) were conducted, which included the items from each subscale being examined for DTF individually and the anchor items. The bifactor CFA models had all items as indicators of a general factor and as indicators of specific orthogonal factors for each subscale. Fit indices selected to evaluate CFA models included root mean squared error of approximation (RMSEA) and Tucker-Lewis Index (TLI) (Bentler and Bonett, 1980; Cudeck and Browne, 1992). Adequate model fit is reflected in a RMSEA<0.08 and TLI>0.94.
From these models, two metrics could be used to estimate the appropriateness of using unidimensional IRT models. The first is explained common variance (ECV), which is simply the common variance explained by the general factor divided by the total common variance, therefore providing a metric of the prominence of the general factor (Reise et al., 2013). The second is percentage of uncontaminated correlations (PUC), which provides an estimate of how many model correlations are contaminated by multiple sources of variance (Reise et al., 2013). For example, in a bifactor structure, the correlations of items from the same subscale are contaminated, as their correlation can be driven both by general and specific factor variance. In contrast, correlations of items from separate subscales are uncontaminated, as their correlations are driven by the general factor alone. Importantly, research has shown that when both ECV and PUC are high (i.e., > 0.70) items can be well modeled by a unidimensional model (Reise et al., 2013). These analyses demonstrated the appropriateness of collapsing items from different subscales into a unidimensional IRT model. Employment of a unidimensional IRT model provides two benefits. Past research has demonstrated there is limited subscale-specific variance within the SPQ (Moussa-Tooks et al., 2020), which indicates any multidimensional structure is likely to have low reliability (Reise et al., 2013). Additionally, this method greatly increases ease of interpretation of the IRT parameters and information analyses.
2.3.4. Differential Test Functioning Analyses
DTF was assessed by fitting a two-parameter unidimensional IRT model using the items from each test subscale and the identified anchor items. Two parameter IRT models provide both a discrimination parameter (analogous to factor loading), which characterize how strongly the item is related to the latent construct, in addition to a severity/ability parameter, which indexes the latent trait level at which an individual becomes more likely than not to endorse an item (i.e., 50% probability). In these models, all item parameters from the tested subscale were allowed to vary between groups, while the parameters for anchor items were constrained to be equal across groups. DTF was quantified using signed DTF (sDTF), which indicates, on the scale of the measure, the expected test score differences at a given trait level (Chalmers et al., 2016). In the current study, sDTF will provide an estimate of the expected difference in scores for the Black participants compared to the White participant group for each tested subscale.
2.3.5. Missing Data
The current sample had approximately 2% and 7% missing SPQ item and SES measure composite data, respectively. The missing SPQ and SES data was imputed using a random forest algorithm (Stekhoven and Buhlmann, 2012) using all other non-missing items within the associated measures. Random forest imputation has shown to outperform other commonly used methods of imputation and is considered highly accurate when imputing categorical data (Stekhoven and Buhlmann, 2012; Waljee et al., 2013).
3. Results
At the level of overall measure performance, Black and White participants exhibited similar schizotypal personality trait severity (means=27.93±19.51 and 26.53±17.05), respectively) as estimated by SPQ total score. In contrast, Black participants displayed higher item endorsement on most items within the Suspiciousness and Paranoid Ideation and Ideas of Reference subscales compared to their White counterparts. Unexpectedly, there was a similar pattern observed with White participants showing systematically higher rates of item endorsement in the Odd or Eccentric Behavior, Odd Beliefs or Magical Thinking, Odd Speech, and Social Anxiety subscales. The race effects described above were consistent across diagnostic groups (cf. Fig. 1 for individual item response rates per subscale by racial group and Supplementary materials Fig. 1–4 for individual item response rates per subscale by diagnostic and racial group membership).
Figure 1. Item Response Rates Across Racial Groups – Full Sample.
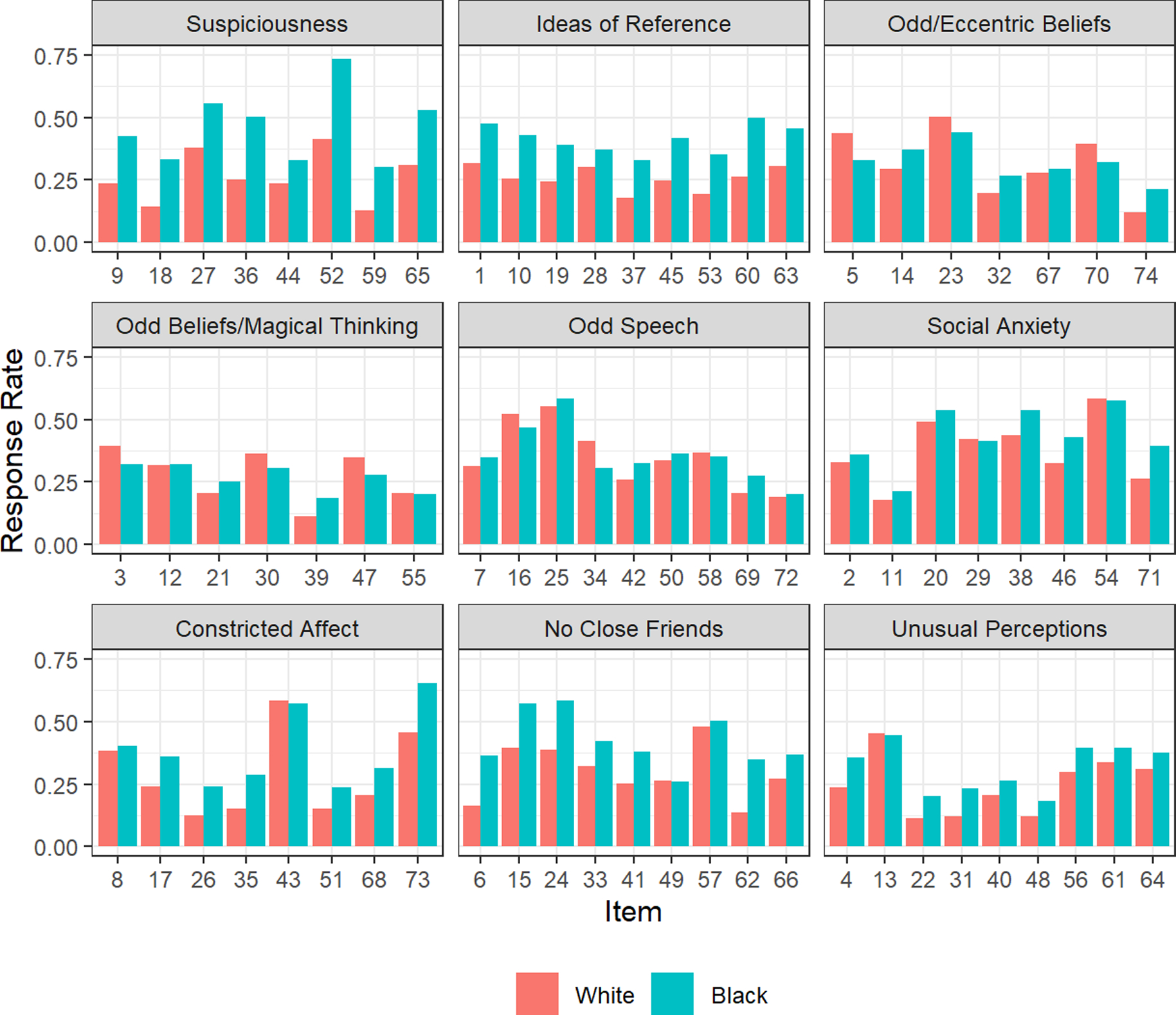
SP = Suspiciousness and Paranoia, IR = Ideas of Reference, CA = Constricted Affect, NF = No Close Friends, SA = Social Anxiety, OS = Odd Speech, OEB = Odd or Eccentric Behavior, OBMT = Odd Beliefs and Magical Thinking, UP = Unusual Perceptions
On a subscale-level, there was a significant effect of race in predicting subscale scores after controlling for overall severity (SPQ total score) and demographics in all subscales except the Constricted Affect, No Close Friends, and Unusual Perceptions subscales (Table 2). Black participants scored higher on subscales related to paranoia and negative/interpersonal symptoms, while White participants scored higher on subscales related to disorganization (e.g., Odd Speech) and positive symptoms (e.g., Odd Beliefs). There were no significant interactions between race and SPQ total score predicting subscales.
Based on GLM results, the No Close Friends, Constricted Affect, and Unusual Perceptions subscales were considered for anchor item selection; 18 items from these subscales were identified to be used as anchor items for subsequent analyses (Supplementary materials for full anchor item list).
In regards to establishing the unidimensionality of subscales prior to IRT analyses, all bifactor models fit the data well with the exception of the Odd Beliefs or Magical Thinking model, which had a fit just below the threshold for adequacy (Supplementary materials, Table 4). All models showed ECV and PUC >0.70, with the exception of the Odd Beliefs or Magical Thinking model, which had an ECV = 0.66 (Supplementary materials, Table 4). Taken together, analyses supported the use of unidimensional IRT models.
IRT models were used to carefully investigate item performance within each subscale across races. The Suspiciousness and Paranoid Ideation and Ideas of Reference subscale were selected for examination due to the significant observed race effect and the hypothesized theoretical association between race and self-reported paranoia (Table 2). The item-level parameters showed that Black participants were endorsing almost every item at a lower latent trait level compared to the White participants (Table 3, Fig. 2 & 3). Notably, at a medium latent trait severity level, the Black participant group is expected to score approximately 1.5 points (Suspiciousness and Paranoid Ideation, Fig. 2 Panel A) and 1.25 points (Ideas of Reference, Fig. 2 Panel B) higher than the White participant group. Interestingly, a subtler pattern was found for Odd or Eccentric Behavior, Odd Beliefs or Magical Thinking, Odd Speech, and Social Anxiety subscales, in which White participants scored higher at similar latent trait severity levels compared to Black individuals (Fig. 4). These findings indicate that race has a large, unaccounted influence on this measure that is especially pronounced for Black individuals on subscales related to paranoia. See Supplementary materials for correlations between subscales (Table 8) and between items within subscales (Tables 9-17).
Table 3.
IRT Parameters
| Suspiciousness and Paranoid Ideation | ||||||
|
| ||||||
| Item | Item Content | White | Black | Severity Difference | ||
|
| ||||||
| † Severity | ‡ Discrim | † Severity | ‡ Discrim | |||
| 9 | I am sure I am being talked about behind my back. | 0.53 | 2.80 | 0.25 | 2.70 | −0.28 |
| 18 | Do you often feel that other people have it in for you? | 0.81 | 4.48 | 0.49 | 4.06 | −0.32 |
| 27 | Do you sometimes get concerned that friends or coworkers are not really loyal or trustworthy? | 0.12 | 1.66 | −0.15 | 2.02 | −0.27 |
| 36 | I feel I have to be on my guard even with friends. | 0.43 | 3.62 | 0.03 | 2.84 | −0.40 |
| 44 | Do you often pick up hidden threats or put-downs from what people say or do? | 0.58 | 2.32 | 0.55 | 2.63 | −0.03 |
| 52 | Have you found that it is best not to let other people know too much about you? | −0.05 | 2.83 | −0.83 | 1.81 | −0.78 |
| 59 | I often feel that others have it in for me. | 0.82 | 6.68 | 0.58 | 3.73 | −0.24 |
| 65 | Do you often have to keep an eye out to stop people from taking advantage of you? | 0.32 | 2.21 | −0.06 | 2.49 | −0.38 |
|
| ||||||
| Ideas of Reference | ||||||
|
| ||||||
| Item | Item Content | White | Black | Severity Difference | ||
|
| ||||||
| † Severity | ‡ Discrim | † Severity | ‡ Discrim | |||
| 1 | Do you sometimes feel that things you see on the TV or read in the newspaper have a special meaning for you? | 0.38 | 1.59 | 0.12 | 1.03 | −0.26 |
| 10 | I am aware that people notice me when I go out for a meal or to see a film. | 0.59 | 1.81 | 0.27 | 1.78 | −0.32 |
| 19 | Do some people drop hints about you or say things with a double meaning? | 0.60 | 2.02 | 0.36 | 2.44 | −0.24 |
| 28 | Have you ever noticed a common event or object that seemed to be a special sign for you? | 0.47 | 1.50 | 0.50 | 1.53 | 0.03 |
| 37 | Do you sometimes see special meanings in advertisements, shop windows, or in the way things are arranged around you? | 1.03 | 1.57 | 0.77 | 1.21 | −0.26 |
| 45 | When shopping do you get the feeling that other people are taking notice of you? | 0.54 | 2.36 | 0.28 | 2.70 | −0.26 |
| 53 | When you see people talking to each other, do you often wonder if they are talking about you? | 0.67 | 3.19 | 0.44 | 3.59 | −0.23 |
| 60 | Do you sometimes feel that other people are watching you? | 0.39 | 3.70 | 0.06 | 4.13 | −0.33 |
| 63 | Do you sometimes feel that people are talking about you? | 0.30 | 2.89 | 0.16 | 4.94 | −0.14 |
Severity is the latent trait level at which participant group is likely to start endorsing yes to an item above 50% likelihood.
Discrim. is the discrimination parameter (analogous to factor loading) indicates an item’s ability to differentiate participants.
Figure 2. Differential Test Functioning - Suspiciousness and Paranoid Ideation & Ideas of Reference.
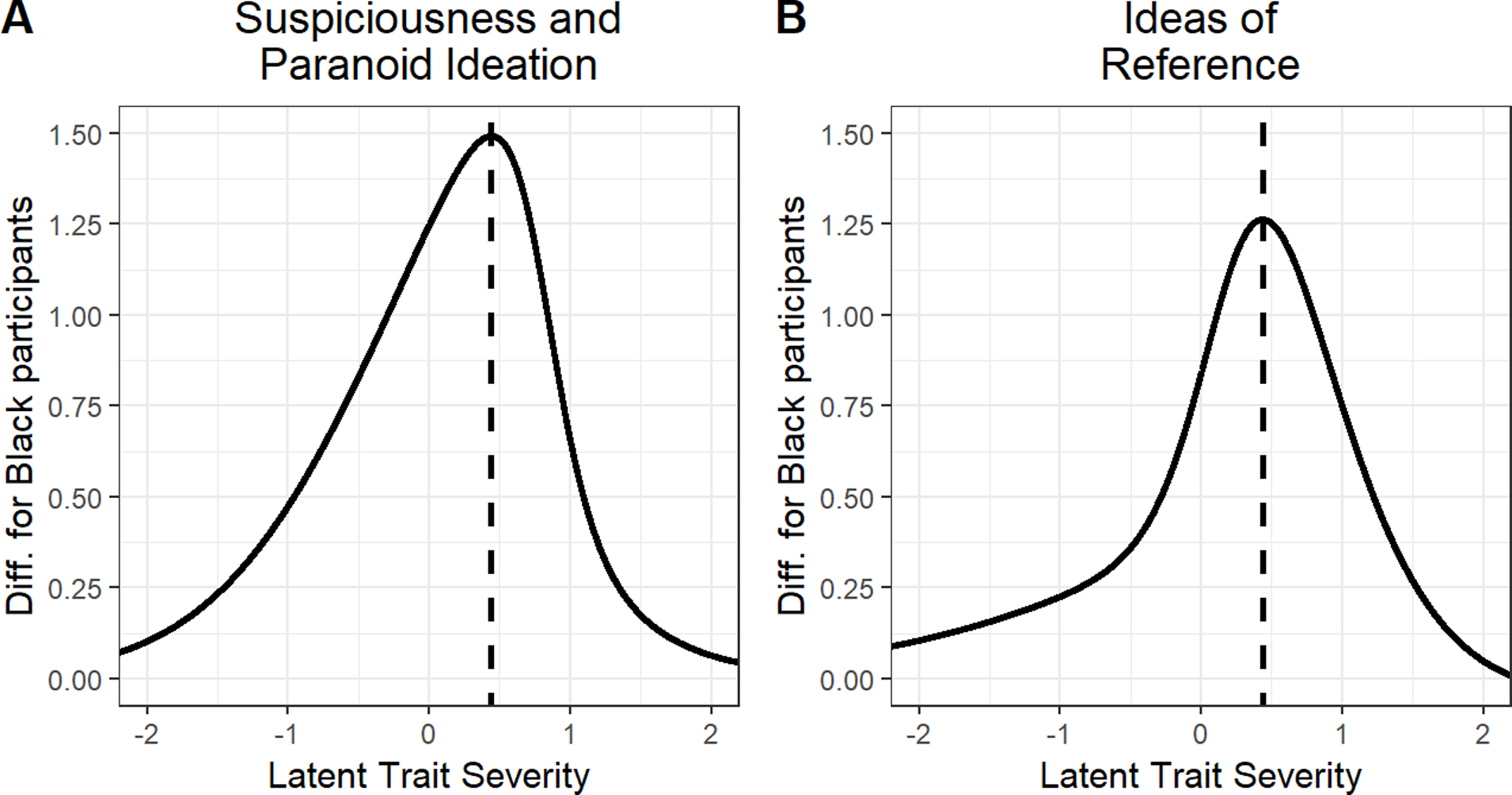
This figure provides a depiction of the subscales that showed significant increased item endorsement within the Black participant group. Dotted line indicates the latent trait level with the largest estimated difference between racial groups (i.e., peak of curves). At a medium latent trait severity level (dotted black line) the Black participant group scored approximately 1.5 points (Panel A) and 1.25 points (Panel B) higher than White participant group—reflecting a considerable difference in a 8-point and 9-point subscales respectively.
Figure 3. Schematic of Misstratification Impact on Classification.
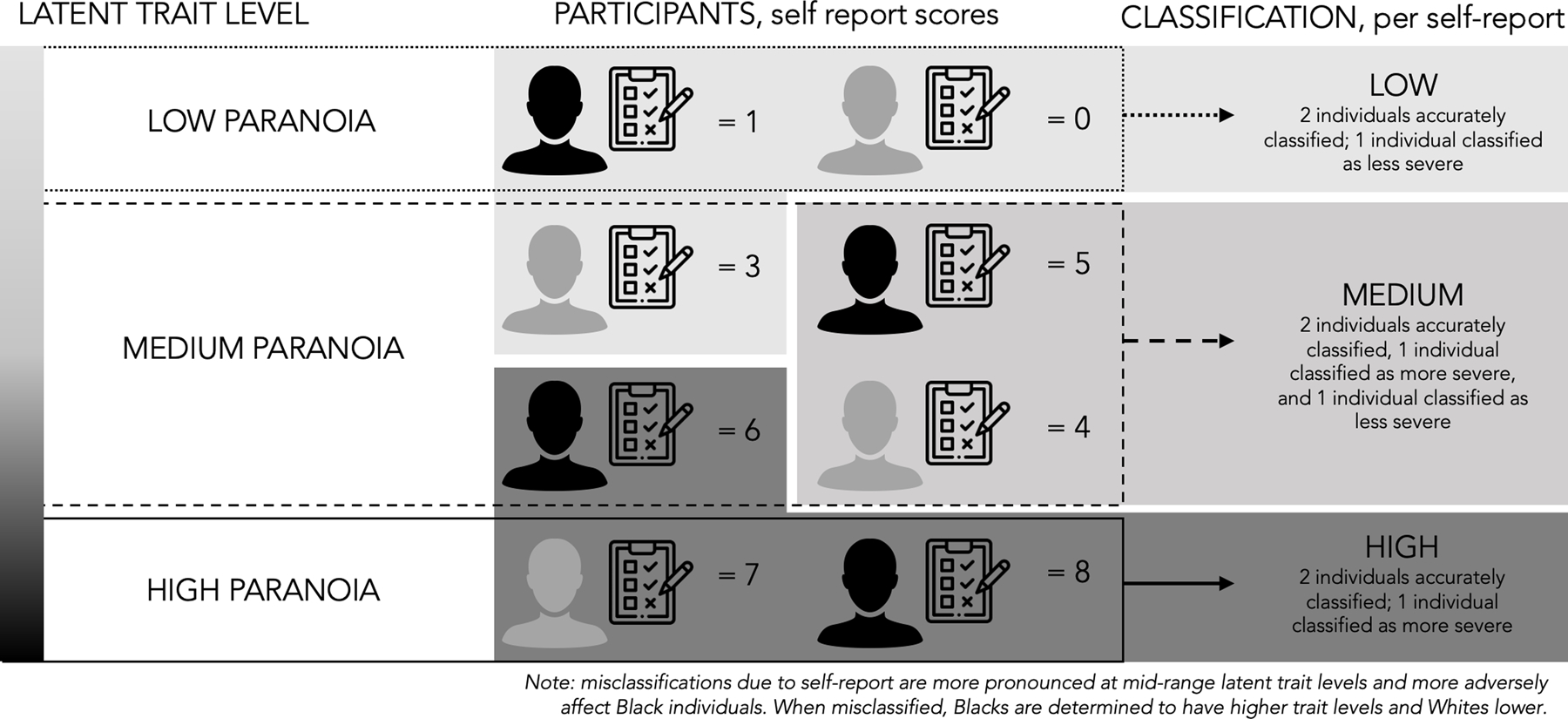
This figure provides a conceptual depiction of how the current findings of increased suspiciousness and paranoia item endorsement on the SPQ in Black individuals leads to misidentification and over-classification of Black individuals as high on a trait, specifically schizotypal traits. In this case, Black individuals self-report higher levels (right side) than White individuals on measures of suspiciousness at similar latent trait levels of schizotypal traits (right side). This can lead to inaccurate risk stratification, as Black individuals may be incorrectly classified as more severe than White individuals. Accordingly, this mis-stratification is especially problematic for individuals near measure cut-offs or diagnostic thresholds (i.e., medium schizotypal traits). For example, at the medium latent trait level, 2 individuals are correctly classified, but one Black individual is classified as more severe and one White individual is classified as less severe. Moreover, these effects may be amplified if using factor scores or other methods that combine scales with similar biases.
Figure 4. Differential Test Functioning - Odd or Eccentric Behavior, Odd Beliefs or Magical Thinking, Odd Speech, Social Anxiety.
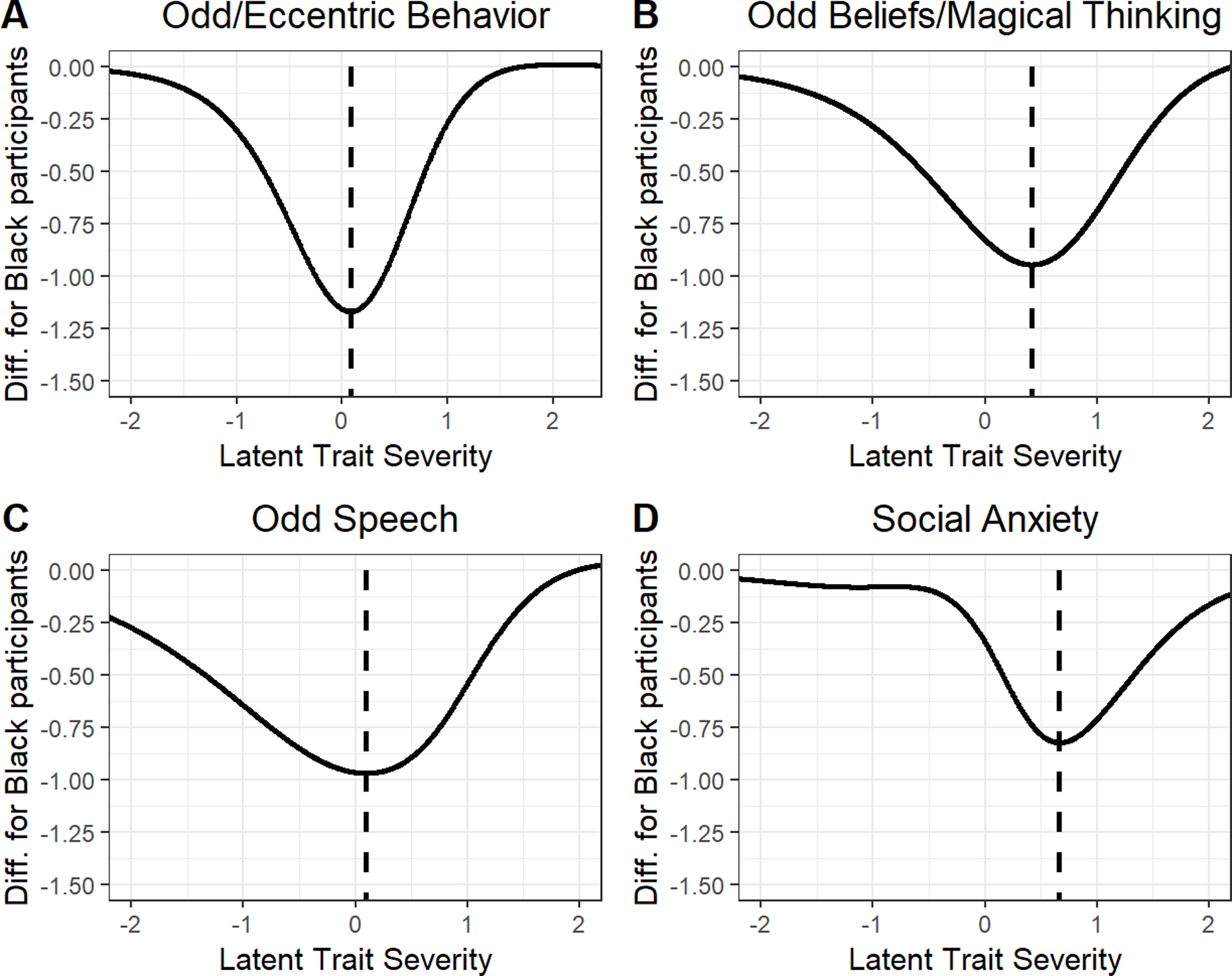
This figure provides a depiction of the subscales that showed significant increased item endorsement within the White participant group. Dotted line indicates the latent trait level with the largest estimated difference between racial groups (i.e., peak of curves). At a medium latent trait severity level (dotted black line) the White participant group scored approximately 1.15 points (Panel A), 0.90 points (Panel B), 1.00 points (Panel C), and 0.80 points (Panel D) higher than Black participant group.
4. Discussion
Given the unique experience of being Black in America (e.g., slavery, segregation, police profiling and excessive use of force, etc.) and evidence that adaptive paranoia is the manifestation of societally induced trauma associated with individual, cultural, and institutional level racism (cf. race-based traumatic stress theory; Carter, 2007), it is vital that we understand how race and diagnostic status may differentially impact item endorsement and functioning within clinically relevant measures, including suspiciousness and paranoia. Our measures assume that variability in subscales is related to the construct a given measure claims to evaluate. However, very rarely do we examine whether measures are contaminated by relevant race-specific experiential processes (i.e., those leading to adaptive paranoia).
Although overall self-reported severity levels (i.e., total SPQ score) were statistically equivalent across racial groups, subscales of the SPQ such as Suspiciousness and Paranoid Ideation showed significant item performance differences. As predicted, Black individuals endorsed a higher number of items on the Suspiciousness and Paranoid Ideation subscale at lower latent trait severity levels in comparison to Whites. This item response bias was widespread within the Suspiciousness and Paranoid Ideation subscale, as observed in each item’s lowered severity level in the Black participant group and the resulting severity differences across racial groups (Table 3). This shift across items suggests that the observed race effects on subscales were driven by more than one or two potentially dubious questions. An example of this shift is displayed prominently in the following questions within the Suspiciousness and Paranoid Ideation subscale: “Do you often feel that other people have it in for you?”, “Do you often have to keep an eye out to stop people from taking advantage of you?”, and “Have you found that it is best not to let other people know too much about you?” (Table 3, items 18, 65, 52). When viewing the wording of these items through a sociocultural lens, it is reasonable to draw conceptual links between Black individuals’ heightened fears regarding how they are viewed by others (i.e., adaptive paranoia) to normative, yet heightened self-reports of mistrust and guardedness (Fig. 3).
Importantly, the described deflection in estimates of severity parameters was robust within the Suspiciousness and Paranoid Ideation subscale, especially at the more moderate trait levels (i.e., latent trait severity = 0.5). Black participant subscale scores were approximately 1.5 points higher compared to White participants at similar latent trait severity levels. On a 8-point subscale, this deflection reflects a meaningful difference which may be further compounded by the addition or clustering of similarly biased subscales. For example, many factor models of the SPQ cluster Suspiciousness and Paranoid Ideation and Ideas of Reference subscales into a Paranoid or Cognitive Perceptual factor (Raine et al., 1994; Stefanis et al., 2004). It is therefore likely that use of factor scores, as calculated by these models, would result in a heavily skewed interpretation of data, because both of these subscales displayed a race-based bias towards the Black group. It is important to note that the original SPQ is only one version of a now widely adopted measure. Since its development, a brief (SPQ-B, 22 items, [Raine and Benishay, 1995]) and brief-revised (SPQ-BR, 34 items, [Cohen et al., 2010]) version have been used by the research community. A notable strength of the current work is that in using the original (full) SPQ, this work captures the largest content base for this measure. The SPQ-B cognitive-perceptual factor has 4 items (28, 44, 45, and 65) and the interpersonal factor has 2 items (36 and 52) from the original Suspiciousness and Paranoia and Ideas of Reference subscales. Some of these overlapping items have high severity differences between groups (Table 3). On the SPQ-BR, 6 items from the Suspiciousness and Paranoia and Ideas of Reference subscales are retained. These 6 items compose an entire factor in the subordinate 7-factor model or covary with other symptoms (Magical Thinking, Unusual Perceptions) in the “cognitive-perceptual” factor of the super-ordinate 3-factor model. Notably, the SPQ-BR utilizes a Likert-scale, which may impact the severity differences among racial groups.
Surprisingly, the White participant group showed significant increases in item endorsement within four subscales: Excessive Social Anxiety, Odd Beliefs and Magical Thinking, Odd or Eccentric Behavior, and Odd Speech. This pattern of response suggests that common factor models (both the three and four-factor structures) of the SPQ that group both Odd Speech and Odd or Eccentric Behavior subscales under a single Disorganization factor may also be subject to similar race-based compounding effects. Though there is scant research on the relationship between stigma and self-reported psychiatric symptoms, it is well established that mental illness stigma has been a deterrence in seeking personal mental health treatment and in the formation of negative attitudes towards others with mental illnesses, particularly among individuals from marginalized backgrounds (U.S. Department of Health and Human Services, 2001; Thompson et al., 2004). Research examining the effects of race on mental illness stigma in depressed individuals found that Blacks had significantly higher levels of internalized stigma compared to Whites (Latalova et al., 2014). This is accompanied by additional work using a nationally representative sample, which showed that White participants find individuals with mental illness (both depression and schizophrenia) to be less stigmatizing compared to Black participants (Anglin et al., 2006). Collectively, this research leads to the hypothesis that White individuals may feel more comfortable self-identifying with odd or eccentric behavioral traits, because they find mental illness broadly to be less stigmatizing. In contrast, Black individuals may feel an increased internalized pressure to avoid endorsements that would suggest strange or unconventional behavior. Although further research is necessary to understand these effects, it is possible that heightened stigma towards mental illness in the Black compared to White participant groups in the present study partially accounts for this observed self-report pattern, with Blacks underreporting overtly odd and/or eccentric experiences.
Strengths of the present study include a large sample size and relatively equal distribution of Black and White participants sampled across the continuum of normal to abnormal functioning within the schizophrenia-spectrum. This facilitated the examination of group differences in endorsements across all 74 items of the SPQ. Additionally, participants were drawn from community rather than college undergraduate populations (mean age =38.62±11.41 years), making the current results more broadly generalizable than studies that primarily included participants with the privileges associated with obtaining postsecondary education.
These findings should be considered with the following limitations. First, the present study did not include additional racial and ethnic groups outside of Black Americans. Research shows that other marginalized communities, such as Hispanic and Asian Americans, experience racism within the United States of America, including increased likelihood of incarceration (U.S Department of Justice, 2020) and exposure to racially-motivated violence (Zhang et al., 2021). Accordingly, differences in subscale item functioning in the SPQ (particularly within the Suspicious and Paranoid Ideation subscale) may similarly arise in these populations. Unfortunately, the current sample was underpowered to investigate these questions in other marginalized groups. Future research will be necessary to clarify whether the manifestation of adaptive paranoia is a phenomenon shared by marginalized groups within the United States or if this outcome is specific to the Black American experience. Second, there were significant group differences in sex, age, and education between participant groups, although controlled for during analyses. While questions related to these factors were not within the scope of the present study, future research may examine potential effects of these demographic variables on item endorsement patterns within the SPQ. Third, the current study did not survey whether the sampled Black individuals immigrated to America recently or if their heritage was immersed in American multigenerational racism. Given the evidence of a considerable effect size linking migration status (both first-generation and second-generation) to psychosis risk, this area poses a notable limitation (Cantor-Graae and Selten, 2005). Lastly, urbanicity, which has been linked to increased psychosis risk (Heinz et al., 2013) was not measured in the present study. All of the listed limitations serve as crucial directions for follow-up research.
4.1. Future Directions & Recommendations to the Field
Investigators must consider how measurement error may erroneously characterize individuals from marginalized backgrounds as having elevated levels of psychopathology, especially paranoia. The racial group differences in item responses within the SPQ established in the present study may serve as a precaution regarding the generalizability and psychometric validity of assessments that have been validated using predominantly undergraduate and/or White participants. The present work is complemented by historical examinations of other personality scales, such as early versions of the Minnesota Multiphasic Personality Inventory (MMPI) that found increased endorsement of items on the Schizophrenia Proneness subscale in Blacks compared to Whites (Cowan et al., 1975; Greene, 1987; Gynther, 1972). This established work demonstrates the necessity to reexamine the practices used to establish the validity of personality and other clinical assessments that have informed schizophrenia-spectrum research. Although the SPQ is not a direct measure of psychosis risk, this work can be used as an illustration of the potential for racial bias to influence rates of paranoia symptom endorsement across other measures of schizotypal traits (e.g., MSS, Kwapil et al., 2018; O-LIFE, Mason et al., 1995) and within broader diagnostic procedures. Further investigation of this issue is particularly vital given that the examination of paranoia is central to the identification of schizophrenia-spectrum disorders, among other conditions. We must therefore consider testing our current measures across more racially diverse samples and either revising our measures or generating guidelines on thoughtful result interpretation, as necessary. At a more fundamental level, research and clinical training should continue to promote cultural competence, especially in areas of assessment and evaluation; doing so may decrease biases introduced in early stages of measure development, such as when examining the face validity of items.
On a hopeful note, assessments such as the SPQ may be improved, as was the case for subsequent MMPI revisions and the Personality Assessment Inventory. This requires that effort be dedicated to the reevaluation of these measures and purposeful recruitment of community-based samples with racial, ethnic, and socioeconomic representation that is proportional to the general population. Research may examine the appropriateness of establishing norms sensitive to the observed differences in suspiciousness and paranoid ideation between many Black and White Americans; keeping in mind that these norms would depend on a careful quantification of the personal impact of lived experiences stemming from individual, cultural, and structural racism. In other words, such norming must consider within-group variation expressed in Black American’s experiences with, and understanding of, racism (e.g., the integration of measures indexing racial identity, coping styles, personal encounters with discrimination, etc.; Carter, 2007) and the degree to which racism impacts their psychological state and adaptive responses (e.g., increased vigilance). Future work may also consider integrating IRT from the onset of assessment development to examine items and subscales that may produce biased responses in marginalized racial groups (Pedraza and Mungas, 2008). In order to fully parse potentially normative differences in paranoia endorsements across racial groups, efforts should be directed at proactively integrating measures associated with race (e.g., perceived discrimination) in research that is assessing liability for and diagnosis of schizophrenia-spectrum disorders (Nagendra et al.,2020). Research paradigms that include contextualizing measures associated with race are necessary to conduct data-driven analyses of the lived experiences that may lead to the development of heightened (and potentially normative) endorsements of paranoia in Black Americans. Auxiliary measures may need to be investigated for use in conjunction with diagnostic interviews to appropriately assess psychosis risk in individuals from marginalized backgrounds. In order to capture whether racial bias in assessment practices may drive the differential diagnostic rates of schizophrenia-spectrum disorders, measures that acknowledge the deep-rooted systemic racism impacting Black individuals must be developed and integrated into our research and assessment practices.
These race-based effects should also be closely monitored in subjective clinical decision-making (e.g., PANSS, SCID, R-GPTS). The exploration of alternative diagnoses linked to suspiciousness and paranoia (such as PTSD) in Black Americans, in addition to thoughtful consideration of the over-extrapolation of normative behavioral responses to psychopathological states must occur prior to the assignment of a psychotic-spectrum diagnosis. Further, elevated self-reports of suspiciousness and paranoia must be examined in relation to Black Americans’ expressed behavior during clinical interactions, where the potential for cultural mistrust to influence individual disposition is high. Consistent with foundational work conducted by Ridley (1984) to examine the typologies of paranoia expressed in marginalized groups, research has found that individual paranoia can be expressed in many forms (i.e., non-paranoia, cultural paranoia, pathological paranoia, or confluent paranoia), which may differentially influence symptom expression across the schizophrenia-spectrum (Whaley, 2002). It is therefore possible that normative race-based differences in paranoia and suspiciousness may pose as mediating or moderating variables for both positive and negative symptom attributions extracted from global clinical decision-making. Previous research suggests that negative symptoms (i.e., diminished social activity, flat affect, alogia, etc.) may be particularly associated with clinician-diagnosed schizophrenia-spectrum disorders in Black Americans (Trierweiler et al., 2000). This work was followed with evidence that clinician-race is linked to differential patterns of schizophrenia symptom attributions in Black Americans (Trierweiler et al., 2006). Furthermore, recent work has demonstrated that experimenter race influences task performance within domains of social cognitive functioning in non-clinical Black American men (i.e., poorer performance with White in comparison to Black experimenter; Nagendra, 2018). These social performance differences may have direct impacts on clinical interactions, exacerbating biases in assessment and evaluation, particularly within a cross-racial patient-clinician dyad. Taken together, future work would benefit from examining the intersection between Black Americans’ past experiences with race-based stressors, self-reported trait measures, and affective disposition in clinical settings.
5. Conclusion
The present study provides evidence that Black Americans across the schizophrenia-spectrum self-report significantly higher levels of paranoia and suspiciousness on the SPQ compared to their White counterparts. It is likely that the measure is unable to distinguish adaptive (cultural) paranoia from paranoia indicating psychopathological risk. This work necessitates a closer investigation of whether adaptive paranoia expressed in Black Americans may contribute to the increased diagnostic rates of psychotic disorders. Current clinical assessment measures and global decision-making may overattribute potentially normative cultural variations in the expression of paranoia in Black Americans, as indicators of pathological states.
Supplementary Material
Acknowledgements
We wish to thank the patients and their families for participation in this study as well as the support from Mahogany A. Monette in providing feedback on the manuscript.
Role of the funding source
This work was supported by the National Institutes of Health (grant number T32 MH103213 to W.P.H., JW., and A.B.M.; R01 MH074983 and R21 MH118617 to W.P.H.; T32 DA024628 to A.J.B.; R21 MH091774 to B.F.O; Indiana Clinical and Translational Sciences Institute award TL1 TR001107 and UL1 TR001108 to A.B.M.).
Footnotes
Declaration of competing interest
None of the authors have conflicts to report.
References
- Anglin DM, Link BG, & Phelan JC (2006). Racial differences in stigmatizing attitudes toward people with mental illness. Psychiatric Services, 57(6), 857–862. 10.1176/ps.2006.57.6.857 [DOI] [PubMed] [Google Scholar]
- Barron D, Swami V, Towell T, Hutchinson G, & Morgan KD (2015). Examination of the factor structure of the Schizotypal Personality Questionnaire among British and Trinidadian adults. Biomed Research International, 2015, 258–275. 10.1155/2015/258275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bentler PM, & Bonett DG (1980). Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin, 88(3), 588–606. 10.1037/0033-2909.88.3.588 [DOI] [Google Scholar]
- Bonifay WE, Reise SP, Scheines R, & Meijer RR (2015). When Are Multidimensional Data Unidimensional Enough for Structural Equation Modeling? An Evaluation of the DETECT Multidimensionality Index. Structural Equation Modeling: A Multidisciplinary Journal, 22(4), 504–516. 10.1080/10705511.2014.938596 [DOI] [Google Scholar]
- Brosey E, & Woodward ND (2015). Schizotypy and clinical symptoms, cognitive function, and quality of life in individuals with a psychotic disorder. Schizophrenia Reearchs, 166(1), 92–97. 10.1016/j.schres.2015.04.038 [DOI] [PubMed] [Google Scholar]
- Cantor-Graae E, & Selten J-P (2005). Schizophrenia and Migration- A Meta-Analysis and Review. American Journal of Psychiatry, 162(1), 12–24. 10.1176/appi.ajp.162.1.12 [DOI] [PubMed] [Google Scholar]
- Carter RT (2007). Racism and Psychological and Emotional Injury: Recognizing and Assessing Race-Based Traumatic Stress. The Counseling Psychologist, 35(1), 13–105. 10.1177/0011000006292033 [DOI] [Google Scholar]
- Chalmers RP (2012). A Multidimensional Item Response Theory Package for the {R} Environment. Journal of Statistical Software. [Google Scholar]
- Chalmers RP, Counsell A, & Flora DB (2016). It Might Not Make a Big DIF: Improved Differential Test Functioning Statistics That Account for Sampling Variability. Educational and Psychological Measurement, 76(1), 114–140. 10.1177/0013164415584576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chapman LJ, Chapman JP, Kwapil TR, Eckblad M, & Zinser MC (1994). Putatively Psychosis-Prone Subjects 10 Years Later. Journal of Abnormal Psychology, 103(2), 171–183. 10.1037//0021-843x.103.2.171 [DOI] [PubMed] [Google Scholar]
- Chavira DA, Grilo CM, Shea MT, Yen S, Gunderson JG, Morey LC, Skodol AE, Stout RL, Zanarini MC, & McGlashan TH (2003). Ethnicity and four personality disorders. Comprehensive Psychiatry, 44(6), 483–491. 10.1016/s0010-440x(03)00104-4 [DOI] [PubMed] [Google Scholar]
- Cicero DC (2015). Measurement invariance of the Schizotypal Personality Questionnaire in Asian, Pacific Islander, White, and multiethnic populations. Psychological Assessment, 28(4), 351–361. 10.1037/pas0000180 [DOI] [PubMed] [Google Scholar]
- Cohen AS, Matthews RA, Najolia GM, & Brown LA (2010). Toward a more psychometrically sound brief measure of schizotypal traits: introducing the SPQ- Brief Revised. Journal of personality disorders, 24(4), 516–537. 10.1521/pedi.2010.24.4.516 [DOI] [PubMed] [Google Scholar]
- Combs DR, Penn DL, Cassisi J, Michael C, Wood T, Wanner J, & Adams S (2006). Perceived Racism as a Predictor of Paranoia Among African Americans. Journal of Black Psychology, 32(1), 87–104. 10.1177/0095798405283175 [DOI] [Google Scholar]
- Cowan MA, Watkins BA, & Davis WE (1975). Level of education, diagnosis and race-related differences in MMPI performance. Journal of Clinical Psychology. 31(3), 442–444. 10.1002/1097-4679(197507)31:3 [DOI] [PubMed] [Google Scholar]
- Cudeck R, & Browne MW (1992). Constructing a covariance matrix that yields a specified minimizer and a specified minimum discrepancy function value Psychometrika, 57(3), 357–369. 10.1007/BF02295424 [DOI] [Google Scholar]
- DeMars CE (2011). An Analytic Comparison of Effect Sizes for Differential Item Functioning. Applied Measurement in Education, 24(3), 189–209. 10.1080/08957347.2011.580255 [DOI] [Google Scholar]
- Feagin JR (1991). The continuing significance of race: AntiBlack discrimination in public places. American Sociological Review, 56(1), 101–116. 10.2307/2095676 [DOI] [Google Scholar]
- Feagin JR, Sikes MP (1994). Living with racism: The black middle-class experience. Boston: Beacon Press. [Google Scholar]
- First MB, Spitzer RL, Gibbon M, & Williams JBW (2002). Structured clinical interview for DSM-IV-TR axis I disorders, research version, patient edition (SCID-I/P). New York: Biometrics Research. [Google Scholar]
- First MB, Gibbon M, Spitzer RL, Williams JBW, & Benjamin LS (1997). Structured clinical interview for DSM-IV Axis II personality disorders. American Psychiatric Press. [Google Scholar]
- Greene RL (1987). Ethnicity and MMPI performance: A review. Journal of Consulting and Clinical Psychology, 55(4), 497–512. 10.1037/0022-006X.55.4.497 [DOI] [PubMed] [Google Scholar]
- Grier WH, & Cobbs PM (1980). Black Rage. New York: Basic Books, Inc. [Google Scholar]
- Gynther MD (1972). White norms and black MMPIs: A prescription for discrimination? Psychological Bulletin,, 78(5), 386–402. 10.1037/h0033555 [DOI] [PubMed] [Google Scholar]
- Heinz A, Deserno L, & Reininghaus U (2013). Urbanicity, social adversity and psychosis. World Psychiatry, 12, 187–197. 10.1002/wps.20056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hines AL, Pollack CE, LaVeist TA, & Thorpe RJ, Jr (2018). Race, Vigilant Coping Strategy, and Hypertension in an Integrated Community. American journal of hypertension, 31(2), 197–204. 10.1093/ajh/hpx164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kopf J, Zeileis A, & Strobl C (2015). Anchor Selection Strategies for DIF Analysis: Review, Assessment, and New Approaches. Educational Psychological Measurement, 75(1), 22–56. 10.1177/0013164414529792 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwapil TR, Gross GM, Silvia PJ, Raulin ML, & Barrantes-Vidal N (2018). Development and psychometric properties of the Multidimensional Schizotypy Scale: A new measure for assessing positive, negative, and disorganized schizotypy. Schizophrenia Research, 193, 209–217. 10.1016/j.schres.2017.07.001 [DOI] [PubMed] [Google Scholar]
- Latalova K, Kamaradova D, & Prasko J (2014). Perspectives on perceived stigma and self-stigma in adult male patients with depression. Neuropsychiatric Disease and Treatment, 10, 1399–1405. 10.2147/NDT.S54081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason O, & Claridge G (2006). The Oxford-Liverpool Inventory of Feelings and Experiences (O-LIFE): further description and extended norms. Schizophrenia research, 82(2–3), 203–211. 10.1016/j.schres.2005.12.845 [DOI] [PubMed] [Google Scholar]
- Maxwell ME, 1992. Family Interview for Genetic Studies (FIGS): a manual for FIGS. Clinical Neurogenetics Branch, Intramural Research Program, National Institute of Mental Health, Bethesda, MD. [Google Scholar]
- Moreno-Izco L, Sanchez-Torres AM, Lorente-Omenaca R, Fananas L, Rosa A, Salvatore P, Peralta V, & Cuesta MJ (2015). Ten-year stability of self-reported schizotypal personality features in patients with psychosis and their healthy siblings. Psychiatry Researcg, 227(2–3), 283–289. 10.1016/j.psychres.2015.02.020 [DOI] [PubMed] [Google Scholar]
- Mosley DV, Owen KH, Rostosky SS, & Reese RJ (2017). Contextualizing behaviors associated with paranoia: Perspectives of Black men. Psychology of Men & Masculinity, 18(2), 165–175. 10.1037/men0000052 [DOI] [Google Scholar]
- Moussa-Tooks AB, Bailey AJ, Bolbecker AR, Viken RJ, O’Donnell BF, & Hetrick WP (2020). Bifactor Structure of the Schizotypal Personality Questionnaire Across the Schizotypy Spectrum. Journal of Personality Disorders, 34, 1–25. 10.1521/pedi_2020_34_466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nagendra A, Twery BL, Neblett EW, Mustafic H, Jones TS, Gatewood D, & Penn DL (2018). Social cognition and African American men: The roles of perceived discrimination and experimenter race on task performance. Psychiatry Research, 259, 21–26. 10.1016/j.psychres.2017.09.074 [DOI] [PubMed] [Google Scholar]
- Nagendra A, Orleans-Pobee M, Spahnn R, Monette M, Sosoo EE, Pinkham AE, & Penn DL (2020). How often do US-based schizophrenia papers published in high-impact psychiatric journals report on race and ethnicity?: A 20-year update of Lewine and Caudle (1999). Journal of mental health (Abingdon, England), 1–8. 10.1080/09638237.2020.1837356 [DOI] [PubMed] [Google Scholar]
- Oh H, Cogburn CD, Anglin D, Lukens E, & DeVylder J (2016). Major discriminatory events and risk for psychotic experiences among Black Americans. The American journal of Orthopsychiatry, 86(3), 277–285. 10.1037/ort0000158 [DOI] [PubMed] [Google Scholar]
- Olbert CM, Nagendra A, & Buck B (2018). Meta-analysis of Black vs. White racial disparity in schizophrenia diagnosis in the United States: Do structured assessments attenuate racial disparities? Journal of Abnormal Psychology, 127(1), 104–115. 10.1037/abn0000309 [DOI] [PubMed] [Google Scholar]
- Ortuno-Sierra J, Badoud D, Knecht F, Paino M, Eliez S, Fonseca-Pedrero E, & Debbane M (2013). Testing measurement invariance of the schizotypal personality questionnaire-brief scores across Spanish and Swiss adolescents. PLoS One, 8(12), e82041. 10.1371/journal.pone.0082041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedraza O, & Mungas D (2008). Measurement in cross-cultural neuropsychology. Neuropsychol Rev, 18(3), 184–193. 10.1007/s11065-008-9067-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raine A (1991). The SPQ: A Scale for the Assessment of Schizotypal Personality Based on DSM-III-R Criteria Schizophrenia Bulletin, 17(4). 10.1093/schbul/17.4.555 [DOI] [PubMed] [Google Scholar]
- Raine A, Reynolds C, Lencz T, Scerbo A, Triphon N, & Kim D (1994). Cognitive-Perceptual, Interpersonal, and Disorganized Features of Schizotypal Personality. Schizophrenia Bulletin, 20(1), 191–201. 10.1093/schbul/20.1.191 [DOI] [PubMed] [Google Scholar]
- Raine A, & Benishay D (1995). The SPQ-B: A brief screening instrument for schizotypal personality disorder. Journal of Personality Disorders, 9(4), 346–355. 10.1521/pedi.1995.9.4.346 [DOI] [Google Scholar]
- Reise SP, Scheines R, Widaman KF, & Haviland MG (2013). Multidimensionality and Structural Coefficient Bias in Structural Equation Modeling. Educational and Psychological Measurement, 73(1), 5–26. 10.1177/0013164412449831 [DOI] [Google Scholar]
- Reynolds CA, Raine A, Mellingen K, Venables PH, & Mednick SA (2000). Three-Factor Model of Schizotypal Personality- Invariance Across Culture, Gender, Religious Affiliation, Family Adversity, and Psychopathology. Shizophrenia Bulletin. 26(3), 603–618. 10.1093/oxfordjournals.schbul.a033481 [DOI] [PubMed] [Google Scholar]
- Rosseel Y (2012). Lavaan: An R package for structural equation modeling and more. Version 0.5–12 (BETA). Journal of Statistical Software, 48(2), 1–36. [Google Scholar]
- Schwartz RC, & Blankenship DM (2014). Racial disparities in psychotic disorder diagnosis: A review of empirical literature. World Journal of Psychiatry, 4(4), 133–140. 10.5498/wjp.v4.i4.133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheffield JM, Brinen AP, & Freeman D (2021). Paranoia and Grandiosity in the General Population: Differential Associations With Putative Causal Factors. Frontiers in Psychiatry, 12, 668152. 10.3389/fpsyt.2021.668152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Startup H, Pugh K, Dunn G, Cordwell J, Mander H, Černis E, Wingham G, Shirvell K, Kingdon D, & Freeman D (2016). Worry processes in patients with persecutory delusions. The British Journal of Clinical Psychology, 55(4), 387–400. 10.1111/bjc.12109 [DOI] [PubMed] [Google Scholar]
- Stefanis NC, Smyrnis N, Avramopoulos D, Evdokimidis l., Ntzoufrasy l., & Stefanis CN (2004). Factorial Composition of Self-Rated Schizotypal Traits Among Young Males Undergoing Military Training. Schizophrenia Bulletin, 30(2), 335–350. 10.1093/oxfordjournals.schbul.a007083 [DOI] [PubMed] [Google Scholar]
- Stekhoven DJ, & Buhlmann P (2012). MissForest--non-parametric missing value imputation for mixed-type data. Bioinformatics, 28(1), 112–118. 10.1093/bioinformatics/btr597 [DOI] [PubMed] [Google Scholar]
- Sue DW, Capodilupo CM, & Holder AMB (2008). Racial microaggressions in the life experience of Black Americans. Professional Psychology: Research and Practice, 39(3), 329–336. 10.1037/0735-7028.39.3.329 [DOI] [Google Scholar]
- Thompson VLS, Bazile A, & Akbar M (2004). African Americans’ Perceptions of Psychotherapy and Psychotherapists. Professional Psychology: Research and Practice, 35(1), 19–26. 10.1037/0735-7028.35.1.19 [DOI] [Google Scholar]
- Trierweiler SJ, Neighbors HW, Munday C, Jackson EETJS, & Binion VJ (2006). Differences in Patterns of Symptom Attribution in Diagnosing Schizophrenia Between African American and Non-African American Clinicians. American Journal of Orthopsychiatry 76(2), 154–160. 10.1037/0002-9432.76.2.154 [DOI] [PubMed] [Google Scholar]
- Trierweiler SJ, Neighbors HW, Munday C, Thompson EE, Binion VJ, & Gomez JP (2000). Clinician Attributions Associated With the Diagnosis of Schizophrenia in African American and Non-African American Patients. Journal of Consulting and Clinical Psychology, 68(1), 171–175. 10.I037//0022-006X.68.1.171 [DOI] [PubMed] [Google Scholar]
- U.S Department of Health and Human Services Services. (2001). Mental Health: Culture, Race, and Ethnicity—A Supplement to Mental Health: A Report of the Surgeon General. https://www.ncbi.nlm.nih.gov/books/NBK44243/ [PubMed]
- U.S Department of Justice. (2020). Prisoners in 2019. 1–37. https://doi.org/https://bjs.ojp.gov/content/pub/pdf/p19.pdf
- Waljee AK, Mukherjee A, Singal AG, Zhang Y, Warren J, Balis U, Marrero J, Zhu J, & Higgins PD (2013). Comparison of imputation methods for missing laboratory data in medicine. BMJ Open, 3(8). 10.1136/bmjopen-2013-002847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whaley AL (2001). Cultural Mistrust and Mental Health Services for African Americans: A Review and Meta-Analysis. The Counseling Psychologist, 29(4). 10.1177/0011000001294003 [DOI] [Google Scholar]
- Whaley AL (2002). Confluent paranoia in African American psychiatric patients: An empirical study of Ridley’s typology. Journal of Abnormal Psychology, 111(4), 568–577. 10.1037/0021-843X.111.4.568 [DOI] [PubMed] [Google Scholar]
- Wickham H (2016). ggplot2: Elegant Graphics for Data Analysis. In Springer-Verlag New York. https://ggplot2.tidyverse.org [Google Scholar]
- Yaralian PS, Raine A, Lencz T, Hooley JM, Bihrle SE, Mills S, & Ventura J (2000). Elevated levels of cognitive-perceptual deficits in individuals with a family history of schizophrenia spectrum disorders. Schizophrenia Research, 46(57–63). 10.1016/s0920-9964(99)00239-x [DOI] [PubMed] [Google Scholar]
- Zhang Y, Zhang L, & Benton F (2021). Hate Crimes against Asian Americans. American Journal of Criminal Justice, 1–21. 10.1007/s12103-020-09602-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.