

We read with great interest the article by Cheung et al. (1) recently published in Hepatobiliary Surgery and Nutrition, presenting a narrative review of various ablation systems for hepatocellular carcinoma (HCC) in cirrhotic patients. We would like to provide several comments. We would first like to offer our congratulations to the authors for their review, which extensively discusses radiofrequency (RFA), high-intensity focused ultrasound (HIFU) , and microwave ablation (MWA) ablation techniques. This review is a succinct summary to better understand the utility of various ablation techniques used in HCC treatment (1).
Although RFA is a well validated thermal ablation technique in the published literature, MWA has become the standard of care in treating HCC, at least in the USA. An increasing number of studies support the safety and efficacy of MWA in HCC for non-surgical candidates (2). Furthermore, there are growing efforts to determine the safety of MWA in ablating hepatic lesions located in high-risk areas. The authors mentioned the use of artificial ascites for hepatic dome lesions as an ancillary technique to minimize potential complications such as diaphragm or lung injury. We would like to offer evidence supporting MWA being a safe and effective method of treatment even in challenging locations such as peri-cardiac or sub-diaphragmatic areas without routine use of hydro-displacement (3-7). Even though continued investigation is still necessary to shed more light on the role of MWA in treating HCC in these locations, it is reassuring to see more and more studies supporting the safety and efficacy of MWA in the treatment of HCC, even in previously thought prohibitive locations and even in patients beyond early stage HCC (8-10).
In the comparison table [Tab. 4 in Ref. (1)] provided by the authors, the ablation size cut-off is reported as “5 cm” for MWA. Although there are no established guidelines for treating HCC larger than 3–3.5 cm, there is growing evidence supporting the use of adjunctive locoregional therapies such as transarterial chemoembolization (TACE) in conjunction with thermal ablation for these lesions. However, recent studies prove that lesions of up to 8 cm can be ablated with modern high power MWA probe technologies alone (2.4 GHz generators) (11). For example, the largest ablation zone that can be achieved using the Emprint™ HP ablation system (Covidien, Boulder, CO, USA) is up to 4.8 cm by 4 cm with just a one 10 minutes cycle at 150 watts using a single probe based on their reported in-vivo data. In our experience, similar to Liu et al. we have routinely been able to achieve ablation zones >5 cm using the “overlap technique”, often using the same initial access tract as can be seen in Figure 1. As the authors mentioned, MWA provides more predictable ablation zones enhancing the safety and efficacy of these larger ablations in the rather crowded liver environment. The local recurrence rate of lesions 5–8 cm was found to be comparable with recurrence rates of smaller HCC lesions after MWA in Liu et al. study (10). Also, Wang et al. achieved far higher complete ablation rates of HCC >5 cm in his study (11). Understandably, much of this literature involves retrospective small sample sizes, so large prospective studies are needed to evaluate long-term safety and efficacy of MWA of HCC lesions >5 cm, although currently published literature is very promising (8,12).
Figure 1.
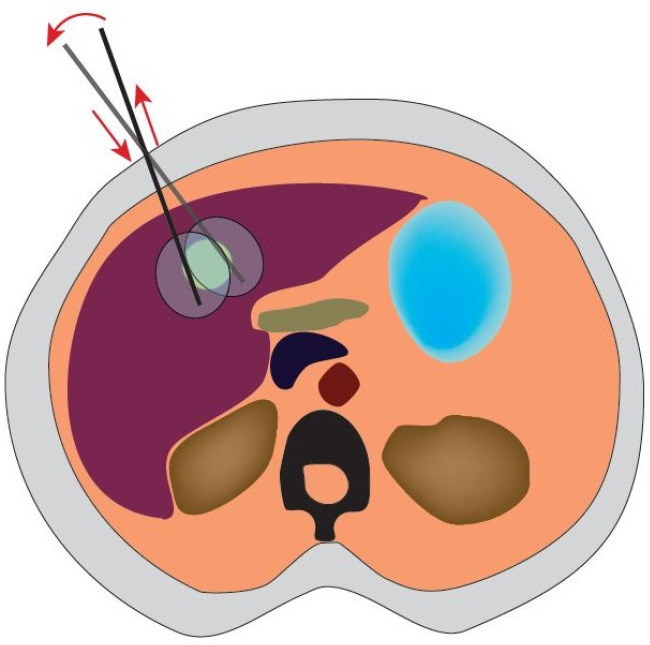
Illustration of the ‘overlap technique’ using one probe/one insertion. The needle (black line) can be retracted without exiting the liver capsule and re-advanced in a different plane as shown with red arrows to cover a larger ablation area. Adequate ablation margins can be achieved with this technique. Digital design by Sefa Ozen.
We would like to add our observation that most liver tumors smaller than 5 cm are rather spherical in shape, making an ablative technology that can provide high level of sphericity very desirable, as it can ensure an adequate ablation margin to the target lesion while lessening tissue damage to healthy liver parenchyma and to highly sensitive structures such as bile duct or diaphragm. In comparison, RFA, HIFU and even older generation MWA systems created more unpredictable ellipsoidal ablation zones compared to modern MWA systems limiting their safety profile and decreasing patient’s candidacy for ablative therapies. The article rightfully discusses one of the main advantages of MWA as being its significant decrease of heat sink effect, making it an ideal ablative therapy in the vascular rich liver environment and in our experience, we have found MWA to be quite effective in caudate lobe and perivascular lesions (>3 mm vessels) where heat skin is most prevalent. Also, MWA may have an inherent advantage over RFA, given its heavy reliance on active heating vs. passive heating as RFA is, possibly allowing for more effective ablation regardless of limitations imposed by local tissue environment (heat-sink, fat, fibrosis, etc.) (13,14).
In this review, ascites was described as one of the contraindications for MWA in Tab. 4 in Ref. (1). Authors mentioned that patients may be good candidates for MWA in case they are not candidates for TACE in the setting of ascites. We think these statements can be confusing for readers and would like to clarify the role of MWA in patients with ascites. Percutaneous liver ablation in the presence of ascites is considered a contraindication in many manuscripts, this is a surrogate conclusion based on surgical literature’s position in liver resection in this patient cohort. Nevertheless, there is little evidence supporting ascites as a contraindication for percutaneous thermal ablation. Some of the reasons behind this concern include worsening liver function, technical challenges and the risk of uncontrollable hemorrhage; however, the evidence for these concerns in percutaneous thermal liver ablation is frail. On the contrary, for the issue of bleeding, artificial ascites administration is recommended for lesions adjacent to gastrointestinal structures to allow a safer ablation and added fluid is drained at the end of the procedure, just like a paracentesis is performed at the end of percutaneous liver ablation in patients with ascites. We agree with Sherwani et al. that the risk of bleeding is low when performing MWA in patients with ascites given the cauterizing nature of the microwave probe, as long as the operator ensures adequate cautery of the traversed liver parenchyma all the way to the hepatic capsule (15). As for worsening liver function, most literature to date has excluded patients with cirrhosis from percutaneous thermal ablation. In our practice we use a case-by-case approach for these patients, as small and single HCCs can be safely ablated in patients with ascites and a bilirubin of <2 mg/dL. A bilirubin of <2.5 mg/dL is reported in several studies as an independent factor predicting worse outcome after liver ablation (8,12).
The authors remark that microwave provides faster ablation compared to RFA or HIFU. In-vivo and ex-vivo studies show that MWA achieves larger ablation zones and faster ablation times, thus allowing tumors to be treated with fewer probe insertion points compared to RFA (14). From a practical point of view, several advantages can be reaped; shorter MWA ablation time, shorter duration of anesthesia, and a far less “liver sticks or insertions” which in our opinion inevitably decreases complications (9).
The article does mention cryoablation as an option for liver ablation, and cites a few older studies from the surgical literature to discount it as safe option. The article also highlights cryoablation’s major advantage, the visible ice-ball, allowing for dynamic visualization of the ablation, but omits other advantages such as decreased procedure associated pain and lack of severe thermal injury to great vessels and biliary tract. However, cryoablation does seem to carry the unique risk of Cryo-Shock in larger ablations and there is a tendency towards increased post-preprocedural bleeding as shown in Rong et al. retrospective study of 1,197 HCC lesions treated by percutaneous cryoablation, but nonetheless, they found comparable efficacy, safety, and long-term survival to the reported outcomes of RFA (16). An earlier comparative study by Ei et al. confirmed aforementioned findings by Rong et al. in support of liver HCC cryoablation (17).
Lastly, it is mentioned in this narrative review, that MWA can be an alternative therapy when lesion’s location is not ideal for RFA. We believe this statement does not reflect current trend in the USA and undermines the advantages of MWA given the increasingly supportive data in the literature as discussed in this article. To the contrary, current trends show MWA to be slowly replacing RFA as the ablative method of choice in the liver; noticeable advantages of MWA over RFA include its capacity to heat the tissues without significant impedance, the lack of grounding pads that can cause skin burns, ability to use in difficult locations and faster ablation time and even a tendency towards less local tumor progression (18).
In conclusion, given these advantages, MWA seems to overcome limitations of RFA and is becoming first choice thermal-ablative therapy in HCC. Further studies are needed to support these observations.
Acknowledgments
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Open Access Statement: This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license). See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
Footnotes
Provenance and Peer Review: This article was commissioned by the editorial office, Hepatobiliary Surgery and Nutrition. The article did not undergo external peer review.
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at https://hbsn.amegroups.com/article/view/10.21037/hbsn-22-138/coif). DR reports receiving consulting fees in occasional consultations services from Medtronic, INC and Boston Scientific, Corp to develop software, artificial intelligence data mining and new medical technologies. The other author has no conflicts of interest to declare.
References
- 1.Cheung TT, Ma KW, She WH. A review on radiofrequency, microwave and high-intensity focused ultrasound ablations for hepatocellular carcinoma with cirrhosis. Hepatobiliary Surg Nutr 2021;10:193-209. 10.21037/hbsn.2020.03.11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yang G, Xiong Y, Sun J, et al. The efficacy of microwave ablation versus liver resection in the treatment of hepatocellular carcinoma and liver metastases: A systematic review and meta-analysis. Int J Surg 2020;77:85-93. 10.1016/j.ijsu.2020.03.006 [DOI] [PubMed] [Google Scholar]
- 3.Sanampudi S, Yu Q, Raissi D. Percutaneous microwave ablation of hepatic lesions near the heart. Transl Gastroenterol Hepatol 2021;6:59. 10.21037/tgh-20-314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Birmingham E, Raissi D, Ozen M. Re: Adjunctive hydrodissection of the bare area of liver during percutaneous thermal ablation of sub-cardiac hepatic tumours. Abdom Radiol (NY) 2022;47:488-9. 10.1007/s00261-021-03280-9 [DOI] [PubMed] [Google Scholar]
- 5.Ozen M, Birmingham E, Raissi D. Re: Liver tumor ablation in difficult locations: Microwave ablation of perivascular and subdiaphragmatic hepatocellular carcinoma. Clin Imaging 2022;85:7. 10.1016/j.clinimag.2022.02.019 [DOI] [PubMed] [Google Scholar]
- 6.Filippiadis DK, Spiliopoulos S, Konstantos C, et al. Computed tomography-guided percutaneous microwave ablation of hepatocellular carcinoma in challenging locations: safety and efficacy of high-power microwave platforms. Int J Hyperthermia 2018;34:863-9. 10.1080/02656736.2017.1370728 [DOI] [PubMed] [Google Scholar]
- 7.Carberry GA, Smolock AR, Cristescu M, et al. Safety and Efficacy of Percutaneous Microwave Hepatic Ablation Near the Heart. J Vasc Interv Radiol 2017;28:490-7. 10.1016/j.jvir.2016.12.1216 [DOI] [PubMed] [Google Scholar]
- 8.Giorgio A, Gatti P, Montesarchio L, et al. Microwave Ablation in Intermediate Hepatocellular Carcinoma in Cirrhosis: An Italian Multicenter Prospective Study. J Clin Transl Hepatol 2018;6:251-7. 10.14218/JCTH.2018.00013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Raissi D, Sanampudi S, Yu Q, et al. CT-guided microwave ablation of hepatic malignancies via transpulmonary approach without ancillary techniques. J Clin Imaging Sci 2022;12:2. 10.25259/JCIS_152_2021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Liu Y, Zheng Y, Li S, et al. Percutaneous microwave ablation of larger hepatocellular carcinoma. Clin Radiol 2013;68:21-6. 10.1016/j.crad.2012.05.007 [DOI] [PubMed] [Google Scholar]
- 11.Wang T, Lu XJ, Chi JC, et al. Microwave ablation of hepatocellular carcinoma as first-line treatment: long term outcomes and prognostic factors in 221 patients. Sci Rep 2016;6:32728. 10.1038/srep32728 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Giorgio A, Merola MG, Montesarchio L, et al. Percutaneous radiofrequency ablation of hepatocellular carcinoma in cirrhosis: analysis of complications in a single centre over 20 years. Br J Radiol 2017;90:20160804. 10.1259/bjr.20160804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kapoor H, Nisiewicz MJ, Jayavarapu R, et al. Early Outcomes with Single-antenna High-powered Percutaneous Microwave Ablation for Primary and Secondary Hepatic Malignancies: Safety, Effectiveness, and Predictors of Ablative Failure. J Clin Imaging Sci 2020;10:10. 10.25259/JCIS_173_2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Poulou LS, Botsa E, Thanou I, et al. Percutaneous microwave ablation vs radiofrequency ablation in the treatment of hepatocellular carcinoma. World J Hepatol 2015;7:1054-63. 10.4254/wjh.v7.i8.1054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sherwani AK, Weis BA, Guynan J, et al. Evaluation of post-procedure hemorrhage in patients with ascites undergoing treatment of hepatic malignancy with thermal ablation utilizing microwave technology. J Clin Oncol 2016;34:e15582. 10.1200/JCO.2016.34.15_suppl.e15582 [DOI] [Google Scholar]
- 16.Rong G, Bai W, Dong Z, et al. Long-term outcomes of percutaneous cryoablation for patients with hepatocellular carcinoma within Milan criteria. PLoS One 2015;10:e0123065. 10.1371/journal.pone.0123065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ei S, Hibi T, Tanabe M, et al. Cryoablation provides superior local control of primary hepatocellular carcinomas of >2 cm compared with radiofrequency ablation and microwave coagulation therapy: an underestimated tool in the toolbox. Ann Surg Oncol 2015;22:1294-300. 10.1245/s10434-014-4114-7 [DOI] [PubMed] [Google Scholar]
- 18.Glassberg MB, Ghosh S, Clymer JW, et al. Microwave ablation compared with radiofrequency ablation for treatment of hepatocellular carcinoma and liver metastases: a systematic review and meta-analysis. Onco Targets Ther 2019;12:6407-38. 10.2147/OTT.S204340 [DOI] [PMC free article] [PubMed] [Google Scholar]