

Abstract
Background:
Active commuting as a contributor to daily physical activity is beneficial for cardiovascular health, but leads to more chances of exposure to ambient air pollution. This study aimed to investigate associations between active commuting to work with cardiovascular disease (CVD), mortality and life expectancy among general Chinese adults, and to further evaluate the modification effect of fine particulate matter (PM2.5) exposure on these associations.
Methods:
We included 76,176 Chinese adults without CVD from three large cohorts of the Prediction for Atherosclerotic Cardiovascular Disease Risk in China project. Information about commuting mode and physical activity were collected by unified questionnaire. Satellite-based PM2.5 concentrations at 1-km spatial resolution was used for estimating PM2.5 exposure of participants. Hazard ratios (HRs) and 95% confidence intervals (CIs) for CVD incidence, mortality and all-cause mortality were estimated using Cox proportional hazards regression models. Multiplicative interaction term of commuting mode and PM2.5 level was tested to investigate potential effect modification.
Results:
During 448,499 person-years of follow-up, 2230 CVD events and 2777 all-cause deaths were recorded. Compared with the non-active commuters, the multivariable-adjusted HRs (95% CIs) of CVD incidence and all-cause mortality were 0.95(0.85−1.05) and 0.79(0.72−0.87) for walking commuters, respectively. Corresponding HRs (95% CIs) for cycling commuters were 0.71(0.62−0.82) and 0.67(0.59−0.76). Active commuters over 45 years old were estimated to have more CVD-free years and life expectancy than non-active commuters under lower PM2.5 concentration. However, these beneficial effects of active commuting were alleviated or counteracted by long-term exposure to high PM2.5 concentration. Significant multiplicative interaction of commuting mode and PM2.5 level was showed in all-cause mortality, with the lowest risk observed in cycling participants exposed to lower level of PM2.5.
Conclusions:
Active commuting was associated with lower risk of CVD, all-cause mortality, and longer life expectancy among Chinese adults under ambient settings with lower PM2.5 level. It will be valuable to encourage active commuting among adults and develop stringent strategies on ambient PM2.5 pollution control for prevention of CVD and prolongation of life expectancy.
Keywords: Active commuting, Air pollution, Fine particulate matter, Cardiovascular disease, Cohort study
1. Introduction
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality worldwide, and more than 80% of CVD mortality take place in low- and middle-income countries including China (World Health Organization, 2021). Physical inactivity has been recognized as a risk factor for CVD and mortality (Lear et al., 2017). Active commuting modes such as walking or cycling are considerable components of daily physical activity. Previous studies about the associations of active commuting modes with CVD health showed inconsistent results, especially on the indistinct effect of walking (Celis-Morales et al., 2017; Dinu et al., 2019; Hu et al., 2007; Matthews et al., 2007; Wennberg et al., 2006). Besides, these studies were mostly conducted in developed countries. It was reported that the trend of active commuting is increasing in developed countries, while decreasing in developing countries including China (Eriksson et al., 2020; Gong et al., 2020; Hallal et al., 2012; Mäkinen et al., 2009; Ussery et al., 2018). More evidences for the benefits of active commuting in Chinese population are needed.
In addition, choosing an active commuting mode is inevitably related to higher exposure to ambient air pollution, which may counteract its favorable effect on CVD health and mortality. Studies indicated that walking or cycling commuters received greater fine particulate matter (PM2.5) uptake than those using automobiles or public transportation due to larger inhalation rates and commuting time (Cepeda et al., 2017; Chaney et al., 2017; Liu et al., 2015). Evidences from developed countries and regions indicated that the cardiovascular protective effect of active commuting and outdoor physical activity was not alleviated by exposure to air pollution (Andersen et al., 2015; Kim et al., 2020a, 2020b; Kubesch et al., 2018; Sun et al., 2020). However, air pollution is much more severe in developing countries such as China than in developed countries. Several studies indicated that exposure to ambient PM2.5 was associated with increased risks of CVD incidence and mortality among Chinese population (Li et al., 2020; Liang et al., 2020; Yang et al., 2020).
A recent study from China indicated that active commuting was associated with lower risks of ischemic heart disease independent of household air pollution, but it didn’t consider the effect of outdoor air pollution (Fan et al., 2019). However, unlike physical activity which could happen indoor or outdoor such as work or sport exercise, commuting activity happens outdoor. Thus, the air pollution closely related to commuting mode is outdoor air pollution. The effects of active commuting on CVD and mortality under high levels of ambient PM2.5 have never been reported in China. Therefore, the present study aimed to investigate the association of commuting mode with CVD incidence, mortality, and life expectancy, and to further evaluate the counteractive effect of long-term ambient PM2.5 on such associations, using large cohorts of general Chinese population from Prediction for Atherosclerotic Cardiovascular Disease Risk in China (China-PAR) project.
2. Materials and methods
2.1. Study population and data collection
Participants were from 3 cohorts of the China-PAR project, including China Multi-Center Collaborative Study of Cardiovascular Epidemiology-1998 (China MUCA (1998)), International Collaborative Study of Cardiovascular Disease in Asia (InterASIA) and Community Intervention of Metabolic Syndrome in China and Chinese Family Health Study (CIMIC). Detailed information of these cohorts has been described in the previous study (Yang et al., 2016). China MUCA (1998), InterASIA and CIMIC were established in 1998, 2000–2001 and 2007–2008, respectively. China MUCA (1998) and InterASIA were followed up twice during 2007–2008 and 2012–2015, and CIMIC was followed up once during 2012–2015 (Yang et al., 2016). Data collection was conducted by trained staffs using standard questionnaires, physical examination, and blood biochemical examinations under strict quality control. This study was approved by the institutional review board at Fuwai Hospital in Beijing and all participating institutions. Written informed consent was signed by each participant before procedures and data collection.
Information about commuting mode and physical activity was collected using a unified questionnaire for the 3 cohorts at the 2007–2008 surveys for the first time, thus data from the 2007–2008 surveys were used for baseline characteristics in the present study. A total of 104,957 participants responded at the 2007–2008 survey were initially enrolled, of which 1255 in 3 sites of InterASIA were only followed up till 2008, 7654 lost to follow-up, 2652 with CVD history, and 717 with invalid commuting information were excluded. Furthermore, the present study focused on commuting mode, thereafter 16,503 (15.7%) participants were excluded due to unemployment and retirement, and the baseline characteristics of these participants and included participants were compared in Table S1. These excluded participants were older and more inactive, with higher incidences of hypertension, diabetes, and dyslipidemia, which were in line with characteristics of unemployed and retired people. Finally, 76,176 participants were included for analysis in this study (Fig. 1).
Fig. 1.
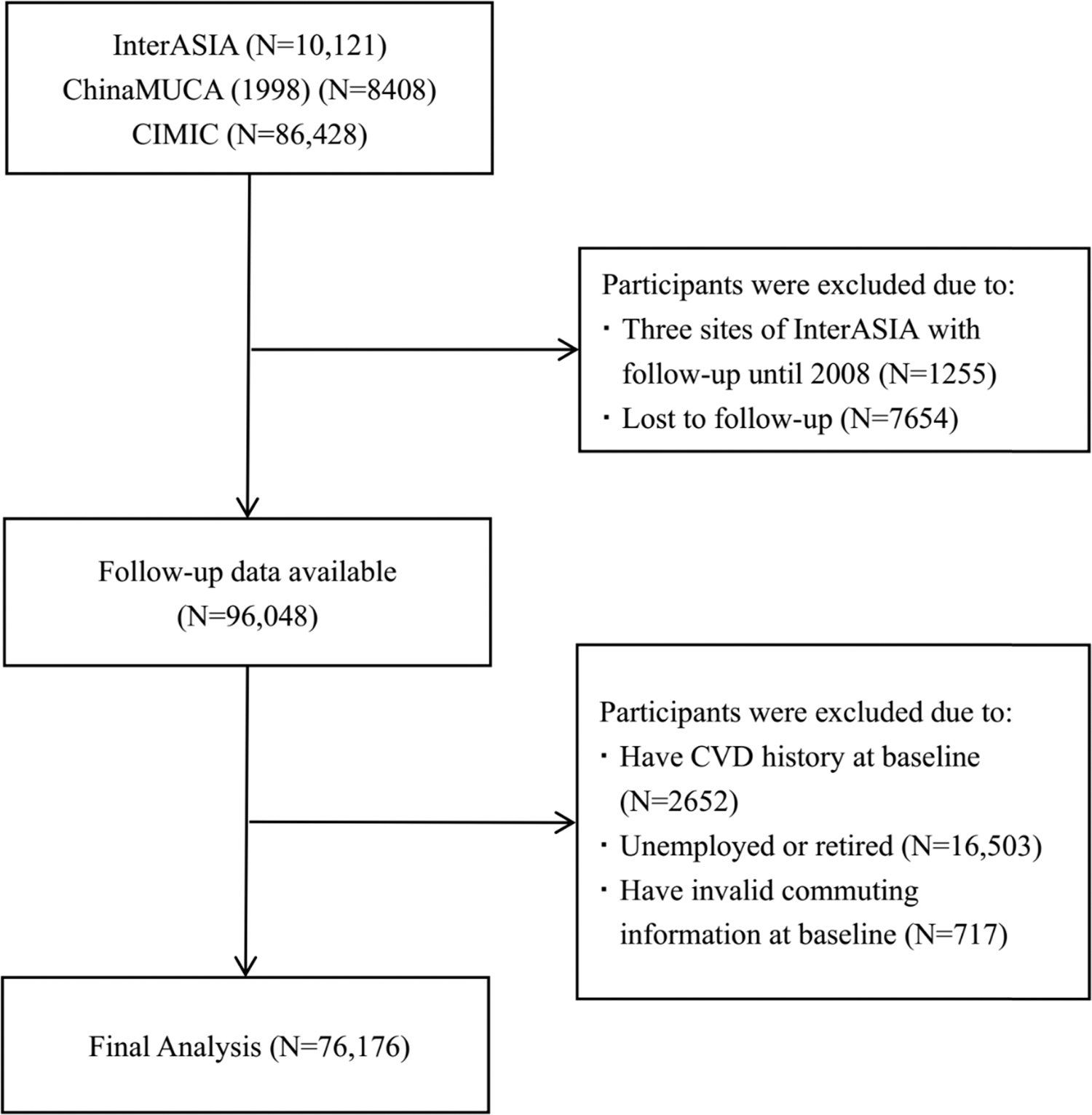
Flow chart of study participants included and excluded in the study. InterASIA, International Collaborative Study of Cardiovascular Disease in Asia; China MUCA (1998), China Multi-Center Collaborative Study of Cardiovascular Epidemiology 1998; CIMIC, Community Intervention of Metabolic Syndrome in China and Chinese Family Health Study. CVD, cardiovascular disease.
2.2. Assessment of commuting data
The information of commuting mode was collected by asking “What kind of commuting mode do you take to and from work?”, and the options were “A. Walking; B. Cycling; C. Public transportation; D. Driving (Car or motorcycle); E. No need to commute (i.e., Working at home)”. Commuting modes was categorized into three types as non-active (including public transportation, driving, and no need to commute), walking and cycling. Non-active commuting mode was served as reference in this study.
2.3. Assessment of ambient PM2.5 level
Satellite-based spatiotemporal models were applied to estimate environmental fine particulate matter (PM2.5) exposure levels. The detailed method has been published elsewhere (Ma et al., 2016). In brief, an ensemble machine learning model was developed to estimate ground PM2.5 concentration of China based on the Aerosol Optical Depth (AOD) retrieved from the National Aeronautics and Space Administration (NASA) Aqua and Terra satellites, meteorology, land use information and population density data. The most recent released 1 × 1 km resolution AOD data retrieved by the multi-angle atmospheric correction (MAIAC) algorithm were used to estimate a 1 × 1 km resolution PM2.5 level (Xiao et al., 2018). The model has been verified using the ground PM2.5 measurement results of the China Environmental Monitoring Center. The R2 of overall model fit is 0.97, and the R2 of model cross-validation is 0.93.
With the satellite-based spatiotemporal model, we obtained the monthly PM2.5 concentration in China from 2000 to 2015. The residential address of each participant was geocoded as grid cells according to latitude and longitude data. The average monthly PM2.5 concentration from 2007 to 2008 survey to 2015 were calculated for each participant.
2.4. Assessment of covariates
Data on demographics (age at baseline, gender, education attainment, per-capita household income, urban or rural resident, and geographic region), lifestyle behaviors (dietary habit, smoking status, alcohol consumption, and physical activity), physical examination (height, weight, blood pressure, fasting blood glucose, and serum lipid levels), family history of CVD, and medical history (hypertension, diabetes mellitus and dyslipidemia) were collected with standardized questionnaires and procedures by trained staffs. Current smoking status was categorized as smoker or nonsmoker by asking the participant whether he or she had smoked more than 100 cigarettes and whether he or she kept smoking till then. Alcohol drinking was defined as alcohol consumption at least 12 times in the last year. Body weight and height were measured by asking participants wearing light clothes with bare feet, and body mass index (BMI) was defined as body weight (kilograms) divided by height (square meters). Diet score was defined as the number of ideal consumptions of red meat (< 75 g/d), fish (≥ 200 g/w), fruit and vegetable (> 500 g/day), legumes (≥ 125 g/d), and tea (≥ 3 times/w) according to the Chinese dietary guideline recommendations (Han et al., 2018; Wang et al., 2016, 2020). Physical activity level and sedentary behavior were evaluated by daily time spending on moderate-vigorous physical activity (MVPA) and sitting. Family history of CVD was defined as at least a parent or a sibling having coronary heart disease (CHD) or stroke. Blood pressure (BP) was measured three times with 30 s interval in a seated position, and hypertension was defined as systolic BP ≥ 140 mmHg and/or diastolic BP ≥ 90 mmHg or use of antihypertensive medication within 2 weeks. Overnight fasting blood samples were drawn for measurements of serum lipid and glucose concentrations. Diabetes was defined as fasting glucose level ≥ 7.0 mmol/L and/or current use of hypoglycemic medicine or insulin within 2 weeks. Dyslipidemia was defined as defined as total cholesterol ≥ 240 mg/dL, triglycerides ≥ 200 mg/dL, low-density lipoprotein cholesterol ≥ 160 mg/dL, high-density lipoprotein cholesterol < 40 mg/dL and/or taking lipid-lowing medicine within 2 weeks.
2.5. Ascertain of outcomes
The 2012–2015 survey was used as the end of follow-up. In the present study, major outcomes included CVD incidence and all-cause death. CVD was defined as incident stroke, non-fatal acute myocardial infarction (AMI), or death from circulatory diseases (ICD-10 I00-I99). In addition, secondary outcomes included CHD (fatal or non-fatal CHD events), stroke (fatal or non-fatal stroke events) and death from CHD (ICD-10 I20-I25), stroke (ICD-10 I60–69), and CVD. During follow-up period, participants or their proxies were interviewed to update their latest disease or death information. Hospital records or death certificates were also checked to validate the diagnosis for validation. All outcomes were initially recorded by trained investigators at local institutes and further adjudicated by an expert outcome assessment committee at Fuwai Hospital.
2.6. Statistical analysis
Baseline characteristics were presented according to categories of commuting modes. Person-years were calculated from the date of 2007–2008 survey to the date of CVD event, death, or last follow-up, whichever occurred firstly. Participants with non-active commuting modes were served as reference, and Cox proportional hazards regression models stratified by source of cohort were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for incidences and mortality of CVD, CHD, and stroke, as well as all-cause mortality associated with commuting by walking and cycling. The analysis was performed with three models. Model 1 was adjusted for gender, age, education level (below high school, high school or above), urbanization (urban or rural), geographic region (north, northeast, east, southwest, central, south and northwest of China), per-capita household income (< 6000 or ≥ 6000 CNY/year) and PM2.5 concentration. Model 2 was further adjusted for diet score, current smoking status (yes or no), alcohol consumption (yes or no), daily time of MVPA and daily time of sitting. Model 3 was further adjusted for BMI, family history of CVD, status of hypertension, diabetes, and dyslipidemia.
In addition to adjusting PM2.5 as a Continuous variable in the Cox proportional hazards regression models, the joint associations of commuting modes and PM2.5 level with risks of CVD incidence and all-cause mortality were evaluated. According to our previous study on the dose-response relationship between PM2.5 and CVD, the risks of CVD incidence and CVD mortality of Chinese population started to increase dramatically while PM2.5 above around 60 μg/m3 (Li et al., 2020; Liang et al., 2020). Furthermore, 61 μg/m3 is the median of PM2.5 concentration among all study participants in the present study. Thus, participants were cross-categorized into 6 groups according to commuting modes (non-active, walking and cycling) and PM2.5 levels (< 61 μg/m3 and ≥ 61 μg/m3), and the group with non-active commuting and exposed to higher PM2.5 was used as the reference. The interaction effect was tested by introducing the multiplicative interaction term of commuting mode and PM2.5 level into the Cox models. Moreover, gain of CVD-free years and life expectancy related to active commuting modes (walking and cycling) compared with non-active commuting mode were estimated under higher of lower levels of PM2.5. The years gained were calculated by the differences of areas under the survival curves fitted by the fully-adjusted Cox proportional model with age as the timescale, from the age of 45–95 (Chudasama et al., 2019; Dehbi et al., 2017). In order to estimate the 95% CI, bootstrap simulations were applied, which generated new bootstrapped samples in equal sample size from the original data with 500 replications. The 2.5th and 97.5th percentiles of these distributions were the 95% CIs.
Subgroup analysis by selected baseline characteristics was conducted, and the interaction terms with commuting mode were tested to investigate potential effect modifications. To evaluate the robustness of results, sensitivity analysis was conducted by excluding participants who developed CVD within the first year of follow-up.
All analyses were performed with SAS (version 9.4, SAS Institute Inc., Cary, North Carolina, USA) and R software (version 3.6.0, R Foundation for Statistical Computing, Vienna, Austria). All statistical tests were two-sided, and a P-value < 0.05 was considered statistically significant.
3. Results
3.1. Baseline characteristics
Baseline characteristics among the 76,176 participants enrolled in the study by categories of commuting modes were presented in Table 1. The mean age at baseline was 51.2 ± 11.8 years old, 40.7% were male. Besides, 33,716 (44.3%) of participants taking active commuting modes to and from work. Active commuters were more likely to be urban residents, non-smokers, non-drinkers, with higher PM2.5 exposure and hypertension incidence rate.
Table 1.
Baseline characteristics of participants according to categories of commuting mode.
| Characteristics | Total | Non-active | Active Walking | Cycling |
|---|---|---|---|---|
| No. of participants | 76,176 | 42,460 | 17,771 | 15,945 |
| Age at baseline (year) | 51.2 ± 11.8 | 51.2 ± 12.4 | 52.3 ± 11.3 | 50.2 ± 10.6 |
| Male, No. (%) | 31,011(40.7) | 17,484(41.2) | 6711(37.8) | 6816(42.7) |
| Urbanization, No. (%) | 2318(3.0) | 962(2.3) | 689(3.9) | 667(4.2) |
| Education higher than high school, No. (%) | 9391(12.3) | 5329(12.6) | 2205(12.4) | 1857(11.6) |
| Current smoker, No. (%) | 16,905(22.3) | 9843(23.2) | 3502(19.7) | 3560(22.3) |
| Alcohol drinker, No. (%) | 17,128(22.5) | 10,592(24.9) | 3009(16.9) | 3527(22.1) |
| BMI (kg/m2) | 23.8 ± 3.6 | 23.8 ± 3.6 | 24.0 ± 3.6 | 23.7 ± 3.5 |
| Household income, Thousand Yuan/year | 22.5 ± 26.0 | 23.1 ± 27.0 | 17.4 ± 24.8 | 26.4 ± 23.7 |
| Daily time of MVPA, h/day | 8.4 ± 6.6 | 8.4 ± 6.6 | 8.5 ± 6.4 | 8.2 ± 6.7 |
| Daily time of sitting, h/day | 7.2 ± 2.9 | 7.0 ± 2.9 | 7.7 ± 3.0 | 7.0 ± 2.7 |
| PM2.5 concentration, yg/m3 | 67.1 ± 14.7 | 63.1 ± 13.2 | 72.4 ± 14.2 | 71.9 ± 15.8 |
| Family history of CVD, No. (%) | 8296(10.9) | 4204(9.9) | 2552(14.4) | 1540(9.7) |
| Hypertension, No. (%) | 25,226(33.1) | 12,370(29.1) | 6626(37.3) | 6230(39.1) |
| Diabetes mellitus, No. (%) | 3995(5.6) | 2106(5.0) | 1172(6.6) | 717(4.5) |
| Dyslipidemia, No. (%) | 21,701(30.2) | 12,028(28.3) | 5837(32.8) | 3836(24.1) |
Values were presented as mean with standard deviation (SD) for continuous variables and frequency with percentage for categorical variables. BMI, body mass index. MVPA, moderate-vigorous physical activity. PM2.5, fine particulate matter. CVD, cardiovascular disease.
3.2. Association of commuting modes with CVD incidence and cause-specific mortality
During 448,499 person-years (median of 5.9 years) of follow-up, we observed 2230 cases of incident CVDs including 389 CHDs and 1678 strokes; and 2777 deaths including 918 CVDs, 251 CHDs and 482 strokes. The associations of commuting modes with CVD incidence and mortality are represented in Tables 2 and 3. Generally, commuting by cycling was associated with lower risk of CVD incidence, while walking showed no significant association. Compared with non-active commuters, the multivariable-adjusted HRs (95% CIs) of incident CVD, stroke and CHD were 0.71(0.62−0.82), 0.74(0.62−0.87) and 0.81 (0.59−1.12) for cycling commuters, respectively (Table 2). The corresponding HRs (95% CIs) for walking commuters were 0.95(0.85−1.05), 0.95(0.84−1.07) and 0.98(0.77−1.25), respectively (Table 2). Furthermore, beneficial effects were observed between active commuting modes and CVD mortality and all-cause mortality. Specifically, compared with non-active commuters, the multivariable-adjusted HRs (95% CIs) of walking commuters were 0.80(0.68−0.95), 0.80 (0.64−1.00), 0.84(0.62−1.13) and 0.79(0.72−0.87) for CVD, stroke, CHD, and all-cause mortality, respectively (Table 3). The favorable effects were more apparent in cycling commuters, with corresponding HRs (95% CIs) of 0.58(0.46−0.73), 0.67(0.49−0.92), 0.54(0.34−0.84) and 0.67(0.59−0.76), respectively (Table 3).
Table 2.
Hazard ratios of cardiovascular diseases incidence associated with categories of commuting mode.
| Non-active | Active |
||
|---|---|---|---|
| Walking | Cycling | ||
|
| |||
| CVD | |||
| No. of cases | 1317 | 643 | 270 |
| Incident rate, per 100,000 Pys | 514.5 | 641.7 | 300.1 |
| Model1: HR (95% CI) | Ref. | 0.94 (0.85–1.05) | 0.74 (0.64–0.85) |
| Model2: HR (95% CI) | Ref. | 0.95 (0.85–1.05) | 0.74 (0.64–0.85) |
| Model3: HR (95% CI) Stroke |
Ref. | 0.95 (0.85–1.05) | 0.71 (0.62–0.82) |
| No. of cases | 1003 | 476 | 199 |
| Incident rate, per 100,000 Pys | 391.6 | 474.7 | 221.0 |
| Model1: HR (95% CI) | Ref. | 0.94 (0.83–1.05) | 0.78 (0.66–0.91) |
| Model2: HR (95% CI) | Ref. | 0.94 (0.84–1.06) | 0.77 (0.65–0.91) |
| Model3: HR (95% CI) | Ref. | 0.95 (0.84–1.07) | 0.74 (0.62–0.87) |
| CHD | |||
| No. of cases | 203 | 128 | 58 |
| Incident rate, per 100,000 Pys | 79.0 | 126.8 | 64.3 |
| Model1: HR (95% CI) | Ref. | 1.03 (0.81–1.30) | 0.82 (0.60–1.13) |
| Model2: HR (95% CI) | Ref. | 1.01 (0.80–1.28) | 0.83 (0.61–1.14) |
| Model3: HR (95% CI) | Ref. | 0.98 (0.77–1.25) | 0.81 (0.59–1.12) |
Model1: adjusted for age, gender, urban or rural resident, geographic region, per-capita household income, educational level, and PM2.5 concentration. Model2: Further adjusted for dietary habit, tobacco smoking, alcohol consumption, daily hours of moderate-vigorous physical activity and sitting, and BMI. Model3: Further adjusted for family history of CVD, status of diabetes mellitus, hypertension, and dyslipidemia. CVD, cardiovascular disease; Pys, person-years; HR, hazard ratio; CI, confidence interval; CHD, coronary heart disease; PM2.5, fine particulate matter; BMI, body mass index.
Table 3.
Hazard ratios of cardiovascular diseases and all-cause mortality associated with categories of commuting mode.
| Non-Active | active Walking | Cycling | |
|---|---|---|---|
| CVD-mortality | |||
| No. of cases | 556 | 257 | 105 |
| Incident rate, per 100,000 Pys | 216.1 | 254.4 | 116.4 |
| Model1: HR (95% CI) | Ref. | 0.83 (0.71–0.98) | 0.63 (0.50–0.78) |
| Model2: HR (95% CI) | Ref. | 0.84 (0.71–0.98) | 0.63 (0.50–0.79) |
| Model3: HR (95% CI) | Ref. | 0.80 (0.68–0.95) | 0.58 (0.46–0.73) |
| Stroke-mortality | |||
| No. of cases | 290 | 132 | 60 |
| Incident rate, per 100,000 Pys | 391.6 | 474.7 | 221.0 |
| Model1: HR (95% CI) | Ref. | 0.82 (0.65–1.02) | 0.76 (0.56–1.03) |
| Model2: HR (95% CI) | Ref. | 0.83 (0.67–1.04) | 0.77 (0.57–1.04) |
| Model3: HR (95% CI) | Ref. | 0.80 (0.64–1.00) | 0.67 (0.49–0.92) |
| CHD-mortality | |||
| No. of cases | 140 | 83 | 28 |
| Incident rate, per 100,000 Pys | 106.6 | 199.4 | 118.8 |
| Model1: HR (95% CI) | Ref. | 0.91 (0.68–1.22) | 0.57 (0.37–0.88) |
| Model2: HR (95% CI) | Ref. | 0.89 (0.67–1.20) | 0.57 (0.37–0.88) |
| Model3: HR (95% CI) | Ref. | 0.84 (0.62–1.13) | 0.54 (0.34–0.84) |
| All-cause mortality | |||
| No. of cases | 1734 | 687 | 356 |
| Incident rate, per 100,000 Pys | 674.1 | 680.0 | 394.5 |
| Model1: HR (95% CI) | Ref. | 0.81 (0.73–0.89) | 0.69 (0.61–0.78) |
| Model2: HR (95% CI) | Ref. | 0.80 (0.73–0.88) | 0.68 (0.60–0.77) |
| Model3: HR (95% CI) | Ref. | 0.79 (0.72–0.87) | 0.67 (0.59–0.76) |
Model1: adjusted for age, gender, urban or rural resident, geographic region, per-capita household income, educational level, and PM2.5 concentration. Model2: Further adjusted for dietary habit, tobacco smoking, alcohol consumption, daily hours of moderate-vigorous physical activity and sitting, and BMI. Model3: Further adjusted for family history of CVD, status of diabetes mellitus, hypertension, and dyslipidemia. CVD, cardiovascular disease; Pys, person-years; HR, hazard ratio; CI, confidence interval; CHD, coronary heart disease; PM2.5, fine particulate matter; BMI, body mass index.
3.3. Joint associations of commuting mode and PM2.5 level with CVD and mortality
The HRs and 95% CIs for joint associations of commuting mode and PM2.5 with CVD and all-cause mortality are shown in Fig. 2. Notably, compared with non-active commuters under higher PM2.5 level, taking active commuting modes showed no beneficial effects on either CVD incidence or all-cause mortality, with the HRs (95% CIs) of 1.02 (0.91−1.15) for walking commuters and 0.87(0.73−1.03) for cycling commuters in CVD incidence, and 0.91(0.81−1.02) and 0.98(0.84−1.15) in all-cause mortality. Compared to participants exposed to higher PM2.5 concentration, those in lower PM2.5 level had lower risk of CVD incidence and all-cause mortality. More importantly, cycling commuters had 40% and 58% lower risk of CVD and all-cause death compared to non-active commuters under lower PM2.5 level. Significant multiplicative interaction of commuting mode and PM2.5 level was observed in all-cause mortality (P for interaction < 0.001). The lowest mortality risk was observed in cycling participants exposed to lower level of PM2.5.
Fig. 2.
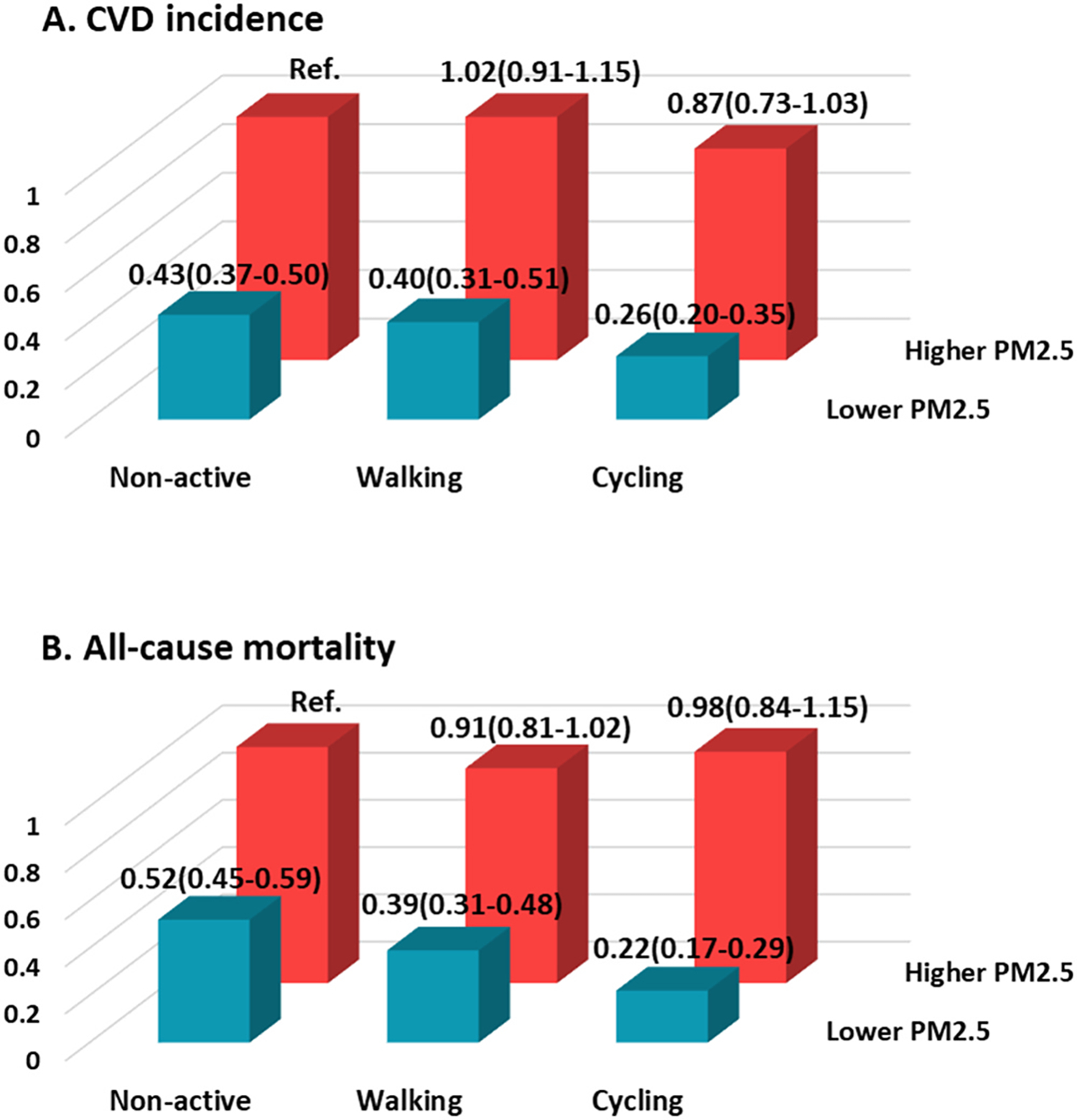
Hazard ratios and 95% confidence intervals of cardiovascular disease incidence (A) and all-cause mortality (B) for joint associations of commuting mode and PM2.5 concentration, stratified by cohort and adjusted for age, gender, urban or rural resident, geographic region, per-capita household income, educational level, dietary habit, tobacco smoking, alcohol consumption, daily hours of moderate-vigorous physical activity and sitting, BMI, family history of CVD, status of diabetes mellitus, hypertension, and dyslipidemia. Higher and lower PM2.5 was categorized by the median of PM2.5 concentration among all study participants. The P-values for interaction were 0.055 and < 0.001 for CVD incidence and all-cause mortality, respectively. CVD, cardiovascular disease; PM2.5, fine particulate matter; BMI, body mass index.
3.4. CVD-free year and life year gains of active commuter under different PM2.5 levels
To evaluate the beneficial health effect of taking active commuting modes under different air pollution conditions, we further estimate the gains of CVD-free years and life years of walking commuters and cycling commuters under overall, higher, or lower PM2.5 levels (Fig. 3). Participants were divided into higher PM2.5 group and lower PM2.5 group, with average PM2.5 concentrations of 79.5 μg/m3 and 54.7 μg/m3, respectively. Among all participants at the index age of 45, compared with non-active commuters, walking commuters were associated with 2.16 (95% CI: 1.35, 3.10) additional life years gained, with no apparent association with CVD-free years gained (0.72, 95% CI: − 0.05, 1.46); and cycling commuters were associated with an average of 3.24 (95% CI: 2.33, 4.22) and 3.71 (95% CI: 2.68, 4.61) additional CVD-free years and life years, respectively. In participants under lower PM2.5 level, the beneficial effects of active-commuting modes were more apparent, with 1.82 (0.45, 3.13) and 3.46 (1.94, 5.04) additional CVD-free years and life years (95% CI) for walking commuters, and 3.61 (2.48, 4.85) and 6.74 (5.34, 8.04) years for cycling commuters as compared with non-active commuters at the index age of 45. However, the CVD-free year gained by cycling was attenuated to 1.72(0.38, 3.14) years, and there was no significant postponement of death by taking active commuting modes for participants under higher PM2.5 level (Fig. 3).
Fig. 3.
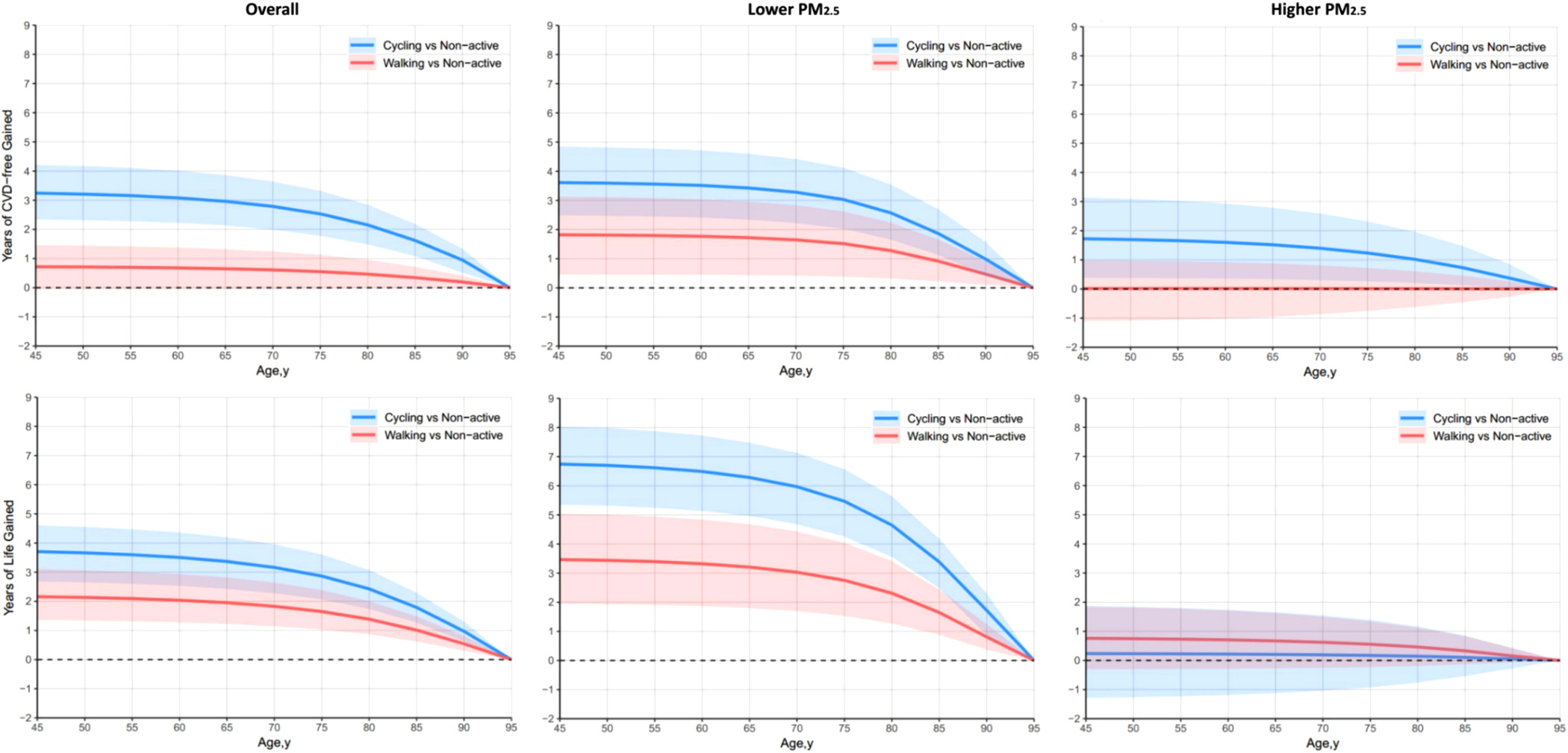
Years of CVD-free gained and years of life gained associated with walking and cycling compared with non-active commuters under different air pollution conditions. Higher and lower PM2.5 was categorized by the median of PM2.5 concentration among all study participants. Models were adjusted for cohort, age, gender, urban or rural resident, geographic region, per-capita household income, educational level, dietary habit, tobacco smoking, alcohol consumption, daily hours of moderate-vigorous physical activity and sitting, BMI, family history of CVD, status of diabetes mellitus, hypertension, and dyslipidemia. PM2.5, fine particulate matter; CVD, cardiovascular disease; BMI, body mass index.
3.5. Subgroup and sensitivity analyses
Subgroup analyses showed that the beneficial effect of active commuting mode on CVD incidence were more apparent in participants who were female, over 60 years old, non-smoker and non-drinker (P for interaction = 0.024, 0.025, 0.036 and 0.003, respectively, Table S2). The association of commuting mode and all-cause mortality was consistent across gender, status of smoking and drinking, BMI and MVPA, while significant interaction effect was observed between commuting mode and age (P for interaction = 0.025, Table S3). In addition, after excluding participants who developed CVD within the first year of follow-up, the significant associations of commuting mode with CVD incidence and all-cause mortality remained robust (Table S4).
4. Discussion
In this large prospective cohort study of general Chinese population, we observed that active commuting modes by walking and cycling were associated with lower risks of CVD and all-cause mortality, as well as postponement of incident CVD and death. Notably, we provide evidence for the first time that the protective effect of active commuting was alleviated or counteracted by higher exposure of ambient PM2.5 in China. These associations were independent of socio-demographics, lifestyle behaviors and cardio-metabolic comorbidities.
Before the 19th century, people mainly commuted by walking. With the expansion of urban and the advancement of transportation technology, the way of commuting has changed dramatically. The Finnish Adult Health Behavior Survey showed that commuting-related physical activity showed a downward trend from 1978 to 2002 (Mäkinen et al., 2009). In recent years, many developed countries have advocated commuting by walking or cycling, and the proportion of commuters choosing active commuting has increased. From 1998 to 2015, the proportion of Swedish workers who chose non-active commuting dropped from 64% to 56%, while the proportion of people who chose to commute with moderate to severe physical activity rose from 12% to 19% (Eriksson et al., 2020). In addition, the National Health Survey of the United States the proportion of walking commuters rose from 28.4% to 31.7% from 2005 to 2015 (Ussery et al., 2018). However, it was reported that the willingness of taking active commuting was decreasing among Chinese population (Gong et al., 2020). In the present study, we found that from 2007 to 2008, 55.7% of the study subjects chose an inactive way of commuting, and only 44.3% chose an active way of commuting. The prevalence and trend of commuting modes are different between China and developed countries.
Several studies have investigated the associations of CVD incidence and mortality, but the results in other countries may not be applicable for Chinese population due to different commuting patterns, physical activity, and environmental factors (Celis-Morales et al., 2017; Fan et al., 2019; Kubesch et al., 2018). the present study indicated that choosing an active commuting mode might lead to beneficial effects on CVD health, which is in consistency with previous findings. Moreover, the advantage of cycling was consistent in previous studies, yet conflicting findings on the effect of walking were reported (Celis-Morales et al., 2017; Fan et al., 2019). Similar to other studies, our findings showed that walking commuting was associated only with CVD- and all-cause mortality, but not with CVD incidences (Celis-Morales et al., 2017; Fan et al., 2019). Daily active commuting is an important part of total physical activity, which is proved to be beneficial for cardiorespiratory fitness and overall health (Audrey et al., 2014; Liu et al., 2020; Ogilvie et al., 2007). Thus, the different effect of walking and cycling may be due to the distinction in physical activity amount (Celis-Morales et al., 2017). The 2011 Compendium of Physical Activities reported that the average intensity of commuting by walking is 4.0 metabolic equivalents (METs), lower than that of commuting by cycling which is 6.8 METs (Ainsworth et al., 2011). Besides, people with longer commuting distance were likely to choose cycling than walking, this may partly contribute to higher commuting related physical activity in cycling commuters. However, we did not observe significant high MVPA in cycling commuters than walking commuters in the present study. We speculated that because of higher occupational physical activity in Chinese population with more labor-intensive jobs compared with developed countries, the total amount of physical activity was mainly determined by work-related physical activity instead of commuting modes (Liu et al., 2020; Zang and Ng, 2016). Besides, according to previous studies, not only the amount but also the intensity had influence on the cardiovascular health effect of physical activity, and higher intensity physical activity was showed to exert better cardiovascular protective effect (Hidalgo-Santamaria et al., 2018; Ramos et al., 2015). The difference of intensity of physical activity between walking and cycling might be a potential mechanism. Furthermore, the effect of active commuting on life expectancy has been reported in other developed countries with inconsistent results (Cepeda et al., 2017; Mueller et al., 2015). This study is the first one among Chinese populations to identify that choosing an active commuting mode was related to postponement in CVD onset and death. The associations of active commuting with incidence and mortality of CVD were independent of potential confounding factors such as gender, age, socioeconomic status, diet behavior, physical activity level, smoking and alcohol consumption, air pollution exposure, family history of CVD, BMI, and comorbidity with diabetes, hypertension, and dyslipidemia. Taken together, choosing an active commuting mode, especially cycling, may deliver benefits on CVD prevention and life expectancy at the population level.
Although active commuting is beneficial for cardiovascular health, active commuters are more likely to expose to outdoor air pollution than non-active commuters who take the public transportation or driving. Our previous works revealed that long-term exposure to higher PM2.5 led to increased risks of CVD and mortality in China (Liang et al., 2020; Yang et al., 2020). Besides, recent modeling studies in both China and the US indicated that life year gains could be achieved by reducing PM2.5 concentration (Bennett et al., 2019; Qi et al., 2020). Studies from Chinese population showed that personal PM2.5 exposure levels were the highest among walking commuters, followed by cycling commuters and non-active commuters (Foraster et al., 2014), and a recent meta-analysis indicated that active commuters had higher inhalation doses of air pollutants than commuters using non-active ones (Cepeda et al., 2017). Hence, it is important to evaluate whether the beneficial effects of active commuting on cardiovascular health were reduced by exposure to air pollutants, especially in China where the ambient air pollution is more severe than many developed countries. Results of this study indicated that active commuting was associated with reduced risks of CVD, mortality, CVD-free year gained and life year gained in participants under lower exposure of PM2.5. A prospective cohort study from China Kadoorie Biobank showed that the association between active commuting modes and incident and recurrent myocardial infarction was independent of air pollution, but only indoor air-pollution by cooking and heating was considered (Fan et al., 2019). Another experimental study showed that beneficial effects in arterial stiffness were reduced in healthy and CVD participants after walking under high compared with low concentrations of traffic-related air pollution (Sinharay et al., 2018). Furthermore, Evidences from developed countries and regions indicated that the health protective effect of active commuting and outdoor physical activity was not alleviated by exposure to PM2.5, whereas the levels of PM2.5 was much lower than that in mainland China, including 26.1 μg/m3 in Taiwan, China, 35.3 μg/m3 in Hong Kong, China, and 26.2 μg/m3 in Korea (Guo et al., 2020; Kim et al., 2020a, 2020b; Sun et al., 2020). Moreover, it should be noted that the categories of PM2.5 (average PM2.5 concentrations: 79.5 ug/m3 for ’higher PM2.5’, and 54.7 ug/m3 for ’lower PM2.5’) still far exceed China’s recommended guidelines to limit average annual PM2.5 to less than 35 ug/m3 or what is generally considered as healthy PM2.5 levels. Differences in the modification effects of air pollution on the association between active commuting and CVD health may due to the level and types of airborne pollutants varying across studies. Therefore, the present study provides the first evidence in Chinese population that the advantageous effects on health of active commuting may be attenuated or counteracted by long-term exposure to a higher level of PM2.5.
These findings have important public health policy implications. Air quality is becoming better with strict air pollution control strategies in China. According to the Report on the State of the Ecology and Environment in China, the control strategies on air pollution have achieved good results. However, besides cities with low level of air pollution, the PM2.5 level of some cities still exceed the level recommended by China (35 ug/m3) and level suggested by the present study (61 ug/m3), especially among northern cities and during winter. Therefore, on one hand, in areas with lower PM2.5 level, a more active commuting mode especially cycling should be encouraged on a population level such as construction of cycle lane, allowance for bike hire and purchase and publicity of healthy life style. On the other hand, in area with higher PM2.5 level especially above 61 ug/m3, active commuting should be recommended with caution, and preventive procedure like wearing mask should be taken for active commuters to reduce the inhalation of PM2.5. Moreover, the air pollution control should be continued in China, especially in northern areas and winter season.
This is the first large prospective cohort study investigated the interaction of commuting mode and long-term exposure to ambient air pollution in CVD prevention and longevity among general Chinese population. Our study was based on a large sample size, and a long-term follow-up period with strict and comprehensive data collection, which allowed us to adjust for a wide range of potential confounding factors such as socio-demography, lifestyle behaviors and comorbidities, and to analyze subtypes of CVD. Furthermore, by using the most recent high-resolution PM2.5 data derived from the MAIAC algorithm and machine-learning approach enabled us to estimate the fine-scale PM2.5 variability for each participant.
Despite the strengths above, several limitations should be noted in the present study. First, information of commuting behavior and physical activity were self-reported instead of instrumental measurements such as pedometer, thus recall bias may introduce misclassification of commuting modes and attenuate the association of active commuting with outcomes. Second, we could not account for information about commuting time and distance in analysis due to lack of information collect. Third, through the satellite-based spatiotemporal models, we only obtained the data of ambient air PM2.5, making us incapable to analyze the health impact of other ambient air pollutants and consider the effect of work-related or indoor air pollution. Previous studies reported that the health benefits of physical activity were not affected by exposure to NO2 and PM10 in Danmark and Korea (Andersen et al., 2015; Kim et al., 2020a, 2020b; Kubesch et al., 2018), yet the level of air pollution was lower in these areas. Forth, the levels of PM2.5 exposure of participants were only dichotomized in the present study. Due to lacking participants and follow-up years to develop enough incidence cases, we could not observe significant results in more detailed stratifications in PM2.5 level. Fifth, though we had rigorous quality control, some participants may not have good access to health care and may lead to differential outcome misclassification. Sixth, although we have adjusted confounders including socio-demographics, lifestyle behaviors and cardio-metabolic comorbidities, residual confounding is still possibly existed, and associations may not imply causation for observational study. In brief, improvements are needed in future study and follow-up surveys to obtain detailed information about commuting mode and air pollution for more accurate estimates of the associations.
5. Conclusion
In summary, this large prospective cohort study revealed that active commuting is beneficial for CVD prevention and life expectancy, and discovered for the first time that long-term exposure to high level of PM2.5 could counteract the cardiovascular benefits attributable to choosing active commuting modes in Chinese population. The new findings also provided population-based evidence which is critical for policy making on environment protection and healthy lifestyle for people in China and other developing countries with severe air pollution.
Supplementary Material
Acknowledgements
The authors thank the staff and participants of the China-PAR project for their important participation and contribution.
Funding
This study was funded by the National Key Research and Development Program of China (2017YFC0211703, 2016YFC0206503, 2018YFE0115300, and 2018YFC1311703), the National Natural Science Foundation of China (91643208 and 91843302), the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2017-I2M-1-004 and 2019-I2M-2-003), and the China Medical Board (15–220). The work of Y. Liu was supported by the MAIA science team at the JPL, California Institute of Technology (Subcontract #1588347), and the National Institute of Environmental Health Sciences of the National Institutes of Health (Award #1R01ES032140). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Abbreviations:
- CVD
Cardiovascular disease
- PM2.5
Fine particulate matter
- HRs
Hazard ratios
- CIs
Confidence intervals
- China-PAR
Prediction for Atherosclerotic Cardiovascular Disease Risk in China
- China MUCA (1998)
China Multi-Center Collaborative Study of Cardiovascular Epidemiology-1998
- InterASIA
International Collaborative Study of Cardiovascular Disease in Asia
- CIMIC
Community Intervention of Metabolic Syndrome in China and Chinese Family Health Study
- AOD
Aerosol Optical Depth
- NASA
National Aeronautics and Space Administration
- MAIAC
Multi-angle atmospheric correction
- BMI
Body mass index
- MVPA
Moderate-vigorous physical activity
- CHD
Coronary heart disease
- BP
Blood pressure
- AMI
Acute myocardial infarction
- SD
Standard deviation
Footnotes
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
CRediT authorship contribution statement
Y. Lin: performed the statistical analysis, interpreted the data, and drafted the manuscript. Y. Lin, X.Y., F. Liu, J.L., J. Ch., X. Liu, J. Ca., S.C., C.S., L.Y., F. Lu, Xia. W., L.Z., Xig. W., Y. Li, D.H., J.H. and X. Lu: collected the survey data. F. Lia, K.H. and Q.X. contributed to the estimation of PM2.5 exposures. All authors contributed to the interpretation of results and critical revision of the manuscript. Y. Liu and D.G. contributed to the concept and design of the study, and critically reviewed the manuscript.
Institutional Review Board Statement
This study was approved by the institutional review board at Fuwai Hospital in Beijing and all participating institutions. The investigations were carried out following the rules of the Declaration of Helsinki of 1975.
Appendix A. Supporting information
Supplementary data associated with this article can be found in the online version at doi:10.1016/j.ecoenv.2021.112641.
References
- Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR, Tudor-Locke C, Greer JL, Vezina J, Whitt-Glover MC, Leon AS, 2011. Compendium of physical activities: a second update of codes and MET values. Med. Sci. Sports Exerc. 43, 1575–1581. [DOI] [PubMed] [Google Scholar]
- Andersen ZJ, de Nazelle A, Mendez MA, Garcia-Aymerich J, Hertel O, Tjønneland A, Overvad K, Raaschou-Nielsen O, Nieuwenhuijsen MJ, 2015. A study of the combined effects of physical activity and air pollution on mortality in elderly urban residents: the Danish Diet, Cancer, and Health Cohort. Environ. Health Perspect. 123, 557–563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audrey S, Procter S, Cooper AR, 2014. The contribution of walking to work to adult physical activity levels: a cross sectional study. Int. J. Behav. Nutr. Phys. Act. 11, 37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennett JE, Tamura-Wicks H, Parks RM, Burnett RT, Pope CA, Bechle MJ, Marshall JD, Danaei G, Ezzati M, 2019. Particulate matter air pollution and national and county life expectancy loss in the USA: a spatiotemporal analysis. PLoS Med. 16, 1002856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Celis-Morales CA, Lyall DM, Welsh P, Anderson J, Steell L, Guo Y, Maldonado R, Mackay DF, Pell JP, Sattar N, Gill J, 2017. Association between active commuting and incident cardiovascular disease, cancer, and mortality: prospective cohort study. Bmj 357, 1456. [DOI] [PubMed] [Google Scholar]
- Cepeda M, Schoufour J, Freak-Poli R, Koolhaas CM, Dhana K, Bramer WM, Franco OH, 2017. Levels of ambient air pollution according to mode of transport: a systematic review. Lancet Public Health 2, e23–e34. [DOI] [PubMed] [Google Scholar]
- Chaney RA, Sloan CD, Cooper VC, Robinson DR, Hendrickson NR, McCord TA, Johnston JD, 2017. Personal exposure to fine particulate air pollution while commuting: an examination of six transport modes on an urban arterial roadway. PLoS One 12, 0188053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chudasama YV, Khunti KK, Zaccardi F, Rowlands AV, Yates T, Gillies CL, Davies MJ, Dhalwani NN, 2019. Physical activity, multimorbidity, and life expectancy: a UK Biobank longitudinal study. BMC Med. 17, 108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dehbi HM, Royston P, Hackshaw A, 2017. Life expectancy difference and life expectancy ratio: two measures of treatment effects in randomised trials with nonproportional hazards. Bmj 357, 2250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dinu M, Pagliai G, Macchi C, Sofi F, 2019. Active commuting and multiple health outcomes: a systematic review and meta-analysis. Sports Med. 49, 437–452. [DOI] [PubMed] [Google Scholar]
- Eriksson JS, Ekblom B, Kallings LV, Hemmingsson E, Andersson G, Wallin P, Ekblom Ö, Ekblom-Bak E, 2020. Active commuting in Swedish workers between 1998 and 2015-Trends, characteristics, and cardiovascular disease risk. Scand. J. Med. Sci. Sports 30, 370–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fan M, Lv J, Yu C, Guo Y, Bian Z, Yang S, Yang L, Chen Y, Huang Y, Chen B, Fan L, Chen J, Chen Z, Qi L, Li L, China Kadoorie Biobank Collaborative G, 2019. Association between active commuting and incident cardiovascular diseases in Chinese: a prospective cohort study. J. Am. Heart Assoc. 8, 012556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foraster M, Basagaña X, Aguilera I, Rivera M, Agis D, Bouso L, Deltell A, Marrugat J, Ramos R, Sunyer J, Vila J, Elosua R, Künzli N, 2014. Association of long-term exposure to traffic-related air pollution with blood pressure and hypertension in an adult population-based cohort in Spain (the REGICOR study). Environ. Health Perspect. 122, 404–411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gong W, Yuan F, Feng G, Ma Y, Zhang Y, Ding C, Chen Z, Liu A, 2020. Trends in transportation modes and time among Chinese population from 2002 to 2012. Int. J. Environ. Res. Public Health 17, 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo C, Zeng Y, Chang LY, Yu Z, Bo Y, Lin C, Lau AK, Tam T, Lao XQ, 2020. Independent and opposing associations of habitual exercise and chronic PM(2.5) exposures on hypertension incidence. Circulation 142, 645–656. [DOI] [PubMed] [Google Scholar]
- Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U, Lancet Physical Activity Series Working G, 2012. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet 380, 247–257. [DOI] [PubMed] [Google Scholar]
- Han C, Liu F, Yang X, Chen J, Li J, Cao J, Li Y, Shen C, Yu L, Liu Z, Wu X, Zhao L, Hu D, Lu X, Wu X, Gu D, 2018. Ideal cardiovascular health and incidence of atherosclerotic cardiovascular disease among Chinese adults: the China-PAR project. Sci. China Life Sci. 61, 504–514. [DOI] [PubMed] [Google Scholar]
- Hidalgo-Santamaria M, Bes-Rastrollo M, Martinez-Gonzalez MA, Moreno-Galarraga L, Ruiz-Canela M, Fernandez-Montero A, 2018. Physical activity intensity and cardiovascular disease prevention-from the Seguimiento Universidad de Navarra Study. Am. J. Cardiol. 122, 1871–1878. [DOI] [PubMed] [Google Scholar]
- Hu G, Jousilahti P, Borodulin K, Barengo NC, Lakka TA, Nissinen A, Tuomilehto J, 2007. Occupational, commuting and leisure-time physical activity in relation to coronary heart disease among middle-aged Finnish men and women. Atherosclerosis 194, 490–497. [DOI] [PubMed] [Google Scholar]
- Kim SR, Choi D, Choi S, Kim K, Lee G, Son JS, Kim KH, Park SM, 2020a. Association of combined effects of physical activity and air pollution with diabetes in older adults. Environ. Int. 145, 106161. [DOI] [PubMed] [Google Scholar]
- Kim SR, Choi S, Keum N, Park SM, 2020b. Combined effects of physical activity and air pollution on cardiovascular disease: a population-based study. J. Am. Heart Assoc. 9, e013611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kubesch NJ, Therming J. Jørgensen, Hoffmann B, Loft S, Nieuwenhuijsen MJ, Raaschou-Nielsen O, Pedersen M, Hertel O, Overvad K, Tjønneland A, Prescot E, Andersen ZJ, 2018. Effects of leisure-time and transport-related physical activities on the risk of incident and recurrent myocardial infarction and interaction with traffic-related air pollution: a cohort study. J. Am. Heart Assoc. 7, 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lear SA, Hu W, Rangarajan S, Gasevic D, Leong D, Iqbal R, Casanova A, Swaminathan S, Anjana RM, Kumar R, Rosengren A, Wei L, Yang W, Chuangshi W, Huaxing L, Nair S, Diaz R, Swidon H, Gupta R, Mohammadifard N, Lopez-Jaramillo P, Oguz A, Zatonska K, Seron P, Avezum A, Poirier P, Teo K, Yusuf S, 2017. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. Lancet 390, 2643–2654. [DOI] [PubMed] [Google Scholar]
- Liang F, Liu F, Huang K, Yang X, Li J, Xiao Q, Chen J, Liu X, Cao J, Shen C, Yu L, Lu F, Wu X, Wu X, Li Y, Hu D, Huang J, Liu Y, Lu X, Gu D, 2020. Long-term exposure to fine particulate matter and cardiovascular disease in China. J. Am. Coll. Cardiol. 75, 707–717. [DOI] [PubMed] [Google Scholar]
- Liu Q, Liu FC, Huang KY, Li JX, Yang XL, Wang XY, Chen JC, Liu XQ, Cao J, Shen C, Yu L, Lu FH, Wu XP, Zhao LC, Li Y, Hu DS, Lu XF, Huang JF, Gu DF, 2020. Beneficial effects of moderate to vigorous physical activity on cardiovascular disease among Chinese adults. J. Geriatr. Cardiol. 17, 85–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu WT, Ma CM, Liu IJ, Han BC, Chuang HC, Chuang KJ, 2015. Effects of commuting mode on air pollution exposure and cardiovascular health among young adults in Taipei, Taiwan. Int. J. Hyg. Environ. Health 218, 319–323. [DOI] [PubMed] [Google Scholar]
- Li J, Liu F, Liang F, Huang K, Yang X, Xiao Q, Chen J, Liu X, Cao J, Chen S, Shen C, Yu L, Lu F, Wu X, Zhao L, Wu X, Li Y, Hu D, Huang J, Liu Y, Lu X, Gu D, 2020. Long-term effects of high exposure to ambient fine particulate matter on coronary heart disease incidence: a population-based Chinese cohort study. Environ. Sci. Technol. 54, 6812–6821. [DOI] [PubMed] [Google Scholar]
- Mäakinen T, Borodulin K, Laatikainen T, Fogelholm M, Prättälä R, 2009. Twenty-five year socioeconomic trends in leisure-time and commuting physical activity among employed Finns. Scand. J. Med. Sci. Sports 19, 188–197. [DOI] [PubMed] [Google Scholar]
- Matthews CE, Jurj AL, Shu XO, Li HL, Yang G, Li Q, Gao YT, Zheng W, 2007. Influence of exercise, walking, cycling, and overall nonexercise physical activity on mortality in Chinese women. Am. J. Epidemiol. 165, 1343–1350. [DOI] [PubMed] [Google Scholar]
- Ma Z, Hu X, Sayer AM, Levy R, Zhang Q, Xue Y, Tong S, Bi J, Huang L, Liu Y, 2016. Satellite-based spatiotemporal trends in PM2.5 concentrations: China, 2004–2013. Environ. Health Perspect. 124, 184–192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mueller N, Rojas-Rueda D, Cole-Hunter T, de Nazelle A, Dons E, Gerike R, Götschi T, Int Panis L, Kahlmeier S, Nieuwenhuijsen M, 2015. Health impact assessment of active transportation: a systematic review. Prev. Med. 76, 103–114. [DOI] [PubMed] [Google Scholar]
- Ogilvie D, Foster CE, Rothnie H, Cavill N, Hamilton V, Fitzsimons CF, Mutrie N, Scottish Physical Activity Research C, 2007. Interventions to promote walking: systematic review. Bmj 334, 1204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qi J, Ruan Z, Qian ZM, Yin P, Yang Y, Acharya BK, Wang L, Lin H, 2020. Potential gains in life expectancy by attaining daily ambient fine particulate matter pollution standards in mainland China: a modeling study based on nationwide data. PLoS Med. 17, 1003027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ramos JS, Dalleck LC, Tjonna AE, Beetham KS, Coombes JS, 2015. The impact of high-intensity interval training versus moderate-intensity continuous training on vascular function: a systematic review and meta-analysis. Sports Med. 45, 679–692. [DOI] [PubMed] [Google Scholar]
- Sinharay R, Gong J, Barratt B, Ohman-Strickland P, Ernst S, Kelly FJ, Zhang JJ, Collins P, Cullinan P, Chung KF, 2018. Respiratory and cardiovascular responses to walking down a traffic-polluted road compared with walking in a traffic-free area in participants aged 60 years and older with chronic lung or heart disease and age-matched healthy controls: a randomised, crossover study. Lancet 391, 339–349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun S, Cao W, Qiu H, Ran J, Lin H, Shen C, Siu-Yin Lee R, Tian L, 2020. Benefits of physical activity not affected by air pollution: a prospective cohort study. Int. J. Epidemiol. 49, 142–152. [DOI] [PubMed] [Google Scholar]
- Ussery EN, Carlson SA, Whitfield GP, Watson KB, Berrigan D, Fulton JE, 2018. Transportation and leisure walking among U.S. adults: trends in reported prevalence and volume, National Health Interview Survey 2005–2015. Am. J. Prev. Med. 55, 533–540. [DOI] [PubMed] [Google Scholar]
- Wang SS, Lay S, Yu HN, Shen SR, 2016. Dietary Guidelines for Chinese Residents (2016): comments and comparisons. J. Zhejiang Univ. Sci. B 17, 649–656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang X, Liu F, Li J, Yang X, Chen J, Cao J, Wu X, Lu X, Huang J, Li Y, Zhao L, Shen C, Hu D, Yu L, Liu X, Wu X, Wu S, Gu D, 2020. Tea consumption and the risk of atherosclerotic cardiovascular disease and all-cause mortality: the China-PAR project. Eur. J. Prev. Cardiol. 27, 1956–1963, 2047487319894685. [DOI] [PubMed] [Google Scholar]
- Wennberg P, Lindahl B, Hallmans G, Messner T, Weinehall L, Johansson L, Boman K, Jansson JH, 2006. The effects of commuting activity and occupational and leisure time physical activity on risk of myocardial infarction. Eur. J. Cardiovasc. Prev. Rehabil. 13, 924–930. [DOI] [PubMed] [Google Scholar]
- World Health Organization, 2021. About cardiovascular diseases, 〈https://www.who.int/cardiovascular_diseases/about_cvd/en/〉., (Accessed 7 Feb 2021).
- Xiao Q, Chang HH, Geng G, Liu Y, 2018. An ensemble machine-learning model to predict historical PM(2.5) concentrations in China from satellite data. Environ. Sci. Technol. 52, 13260–13269. [DOI] [PubMed] [Google Scholar]
- Yang X, Liang F, Li J, Chen J, Liu F, Huang K, Cao J, Chen S, Xiao Q, Liu X, Shen C, Yu L, Lu F, Wu X, Wu X, Li Y, Zhao L, Hu D, Huang J, Lu X, Liu Y, Gu D, 2020. Associations of long-term exposure to ambient PM(2.5) with mortality in Chinese adults: a pooled analysis of cohorts in the China-PAR project. Environ. Int. 138, 105589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang X, Li J, Hu D, Chen J, Li Y, Huang J, Liu X, Liu F, Cao J, Shen C, Yu L, Lu F, Wu X, Zhao L, Wu X, Gu D, 2016. Predicting the 10-year risks of atherosclerotic cardiovascular disease in Chinese population: the China-PAR project (Prediction for ASCVD Risk in China). Circulation 134, 1430–1440. [DOI] [PubMed] [Google Scholar]
- Zang J, Ng SW, 2016. Age, period and cohort effects on adult physical activity levels from 1991 to 2011 in China. Int. J. Behav. Nutr. Phys. Act. 13, 40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.