

Abstract
Episodic future thinking (EFT) is the psychological process of vividly imagining a future event, and this process has been shown to reduce overeating in the laboratory. To assess the efficacy of EFT in the natural environment, twenty-nine overweight or obese women who wanted to improve their eating habits were randomly assigned to one of two smartphone-implemented interventions – EFT or control episodic recent thinking (ERT) – while they ate dinner in a public food court. Results showed a reduction in consumption of total calories, a reduction in percent calories from fat, and an increase in percent calories from protein for EFT versus ERT. These data suggest EFT may be used to modify eating habits in natural eating environments, and may show potential as a component of behavioral obesity interventions.
Keywords: Episodic future thinking, Eating
1. Introduction
Eating involves a complex set of decisions that in part regulate body weight. One important decision is the extent to which someone resists the urge to overeat in a tempting eating environment. The choice to eat healthy may be more challenging for those who are overweight/obese. The ability to choose to eat healthy foods is complicated in overweight or obese persons by contextual factors of the eating environment. We are more likely to overeat when eating out, such as at a food court, compared to eating at home (de Castro et al., 2012). The presence of other people – friends or strangers alike – has also been shown to increase energy intake (Clendenen et al., 1994), which can make it more difficult to eat healthy when meals must be eaten outside of the home. Behaviors modeled by others influence perceived social norms around food, influencing eating behavior (Mollen et al., 2013). Furthermore, when a wide variety of foods are available in the natural environment, a person is more likely to overeat compared to when there is little or no variety (Epstein et al., 2013; Raynor and Epstein, 2001). To reduce overeating in a real world setting, the intervention must overpower contextual factors.
One method called episodic future thinking (EFT) has been shown to reduce overeating in tempting situations (Daniel et al., 2013b). EFT works by mentally projecting oneself into the future through vivid imagination of specific, personal and detailed future events. EFT reframes the temporality of decision-making in the moment. During a meal, decisions are made constantly: how much to eat, which foods to eat and when to stop eating. EFT allows people to focus on future health goals rather than the pleasure associated with a decision that is highly gratifying in the moment (Atance and O’Neill, 2001; Benoit et al., 2011; Peters and Buchel, 2010). When obese and lean women vividly imagine the future through EFT, bias towards pleasure in the moment is replaced by decisions that align with long-term goals (Daniel et al., 2013a), and engaging in EFT during an ad libitum meal reduces calorie consumption compared to a control (Daniel et al., 2013b). Because overweight persons experience more difficulty delaying gratification (Jarmolowicz et al., 2014), EFT may be even more meaningful for this population.
Current research in EFT has trained individuals to envision the future, but the content has not been specific to eating. In the present study, all the participants were overweight and indicated that they wanted to improve their eating habits. To better target behavior change, we adapted EFT to focus on future events specific to the person’s individual eating-related goals. Basic cognitive neuroscience research has shown brain regions normally involved in EFT show increased activation when compared to EFT that does not include personal goals, suggesting goal-oriented EFT may facilitate goal achievement by increasing the personal significance associated with prospection (D’Argembeau et al., 2010). EFT may help persons who are trying to eat less and lose weight amidst challenging eating situations (Sze et al., in press). To translate this laboratory research to the natural environment and test the effect of EFT on food intake and choices, we recruited overweight and obese women who were trying to eat healthier and randomized them to EFT or to an episodic recent thinking (ERT) control group Then, while engaging in EFT/ERT, the women ate dinner in a public food court with a large variety of unhealthy options as well as healthier alternatives.
An important component of translating EFT research to the field is to identify EFT delivery systems that are efficacious within the wide range of complex eating environments encountered in everyday life. In the laboratory, playing recordings of a person speaking their EFT events while eating has been shown to successfully reduce intake (Daniel et al., 2013b). In the present study, EFT and control conditions were implemented using smartphones to facilitate translation of this behavioral technique to eating in highly distracting environments outside the lab.
2. Methods
2.1. Participants
Twenty nine overweight or obese (BMI ≥ 25 kg/m2)women (median BMI = 31.14 kg/m2, Interquartile range = 29.26–33.36; mean BMI = 31.44 ± 4.68 kg/m2 (mean ± SD); mean age = 36.77 ± 12.83; 24.14% minority: average years of education = 15.38 ± 2.72 (where 12 years = high school graduate, 16 years = bachelor’s degree, 20 years = professional or graduate degree) participated in the study in exchange for a $20 check and a $10 dinner voucher. The sample size was determined based on the effect size from a previous study examining the effect of EFT on energy intake (Cohen’s d = 1.23) (Daniel et al., 2013b). Based on this effect size, power of 0.8 and alpha of .05, 12 subjects per group are required. Recruitment eligibility criteria selected participants who indicated they wanted to improve their eating habits. This was important to ensure motivation to improve eating habitswas present before implementing the intervention. Also, because health risks for different ethnicities accumulate at different BMI values, all participants were above their ethnicity-specific BMI threshold for moderate to severe health risks associated with an overweight BMI (Katzmarzyk et al., 2011). Fig. 1 details information related to recruitment and retention.
Figure 1.
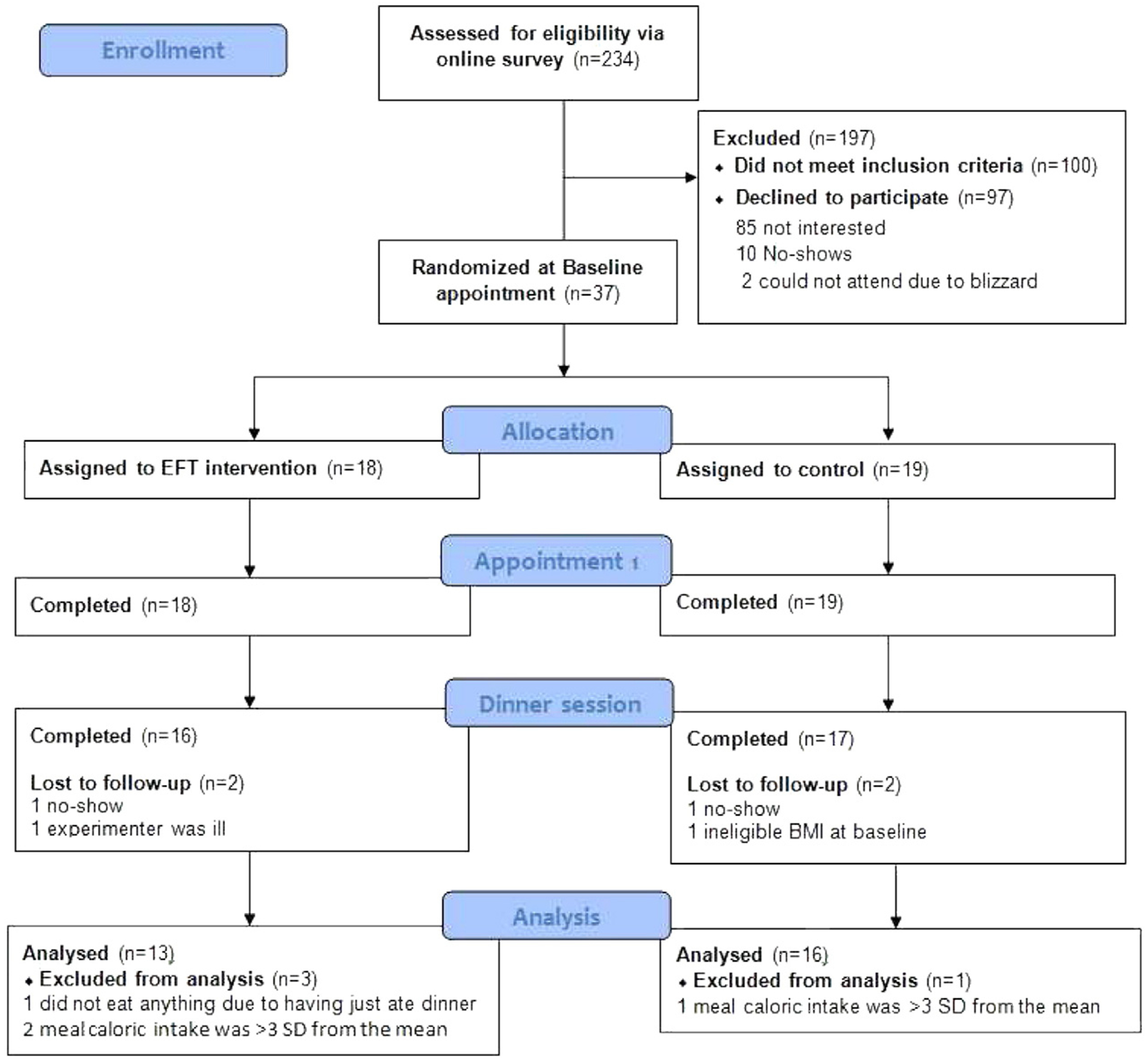
CONSORT diagram displaying information about recruitment and retention.
Participants were recruited from an existing database, Craigslist ads and flyers. Persons taking medications or living with conditions that affect appetite (e.g., ADHD medications, pregnancy) were not eligible for the study. All study procedures were approved by the University at Buffalo Social and Behavioral Sciences Institutional Review Board.
2.2. Experimental procedures
Participants attended a 90 min baseline session in the laboratory and a 60min dinner session in a nearby food court the next day. At the baseline session an informed consent form was completed, BMI was measured, their smartphone was tested for compatibility with study audio delivery methods and a basic sociodemographic form adapted from Macarthur’s sociodemographic questionnaire (Adler et al., 2000) was administered. Participants whose cell phone did not conform to study requirements were provided an iPod for the audio delivery. Participants completed a payment form for the first session and were given instructions for the next day’s dinner session. Eligible participants were randomized to either receive the study intervention (EFT) or the control task, ERT.
The dinner session occurred within 1 h of the participants’ usual dinner time and participants were instructed to “view tomorrow’s session as your dinner for the day.” Participants arrived at a private room adjacent to the food court and received a $10 food voucher for their dinner along with detailed verbal instructions. The written EFT/ERT cue was attached to their food voucher as an additional prompt. Participants practiced listening to their audio cues for 60 s and reviewed a menu with a variety of options to choose from for dinner, which included calories, grams of fat, and grams of sugar for beverage options. Some of this information were also available by signage at the food court. Participants could choose from a wide variety of options at 4 different outlets at the food court, including but not limited to: sandwiches, pizza, salads, burgers, fruit, milk (non-fat and 2%), potato chips, French fries, cottage cheese with fruit and vegetable trays.
Then, the participant went to the food court to purchase food of her choice and listen to her audio cues while eating dinner. Participants were instructed to “take as much or as little time to eat your dinner as you’d like,” to “choose whatever you would like for your dinner, as long as it is listed on the menu,” and to return with their leftovers and all trash in the plastic bag provided. Participants were also told to pay very close attention to the audio while eating their dinner. Then they returned to the private meeting room after they finished eating dinner and were debriefed. To limit participant demand expectations, all weighing equipment was hidden from view and the experimenter waited until the participant left to weigh remaining food.
2.2.1. EFT cue development interview
To begin the process of generating the audio cues, an interview process similar to a previous EFT study on eating behaviors was used (Daniel et al., 2013a). At session 1, participants were asked to list up to 5 future health goals they would like to achieve in about 3 weeks. A calendar with the highlighted future time period was provided to facilitate goal generation. Then, participants rated their health goals for feasibility and importance. Goals that were not feasible or important were not candidates for audio cue generation.
Next, participants were asked to list up to five future events they had planned or anticipated would occur in 3 weeks. The experimenter utilized open-ended questions to obtain location, time, emotion(s), and a context for the future events. One example of a future event is, “In 3 weeks, I will go to the concert with my friend. We will sit near the back so we can chat more easily. I will be feeling excited and happy to see the band play for the first time.”
Participants then rated their future events for vividness, a rating which incorporated imagination of location, time, emotion(s), and a context. Finally, the experimenter helped participants pair goals with the events to “imagine yourself achieving your health goal at the event, or imagine how you might be feeling about having achieved your health goal at the event.” This combined information comprised the EFT cue. To expand on the previous example, a complete cue including the event and goal is, “In 3 weeks, I will go to the concert with my friend. We will sit near the back so we can chat more easily. I will be feeling strong and proud of myself after having achieved my goal of going to the gym three times per week. I will be feeling excited and happy to see the band play for the first time.”
2.2.2. ERT cue development interview
The ERT audio cue development process was identical to the EFT process, except the health goals were replaced with habitual behaviors and the future time perspective was replaced with a past 24 h time perspective. To match the cognitive load, length and complexity of the EFT procedures, participants in the ERT group were asked to “list 5 habits you do regularly and enjoy” and rated their importance. Habits that were rated as unimportant were not candidates for audio cue generation. Participants were then asked to list 5 events that occurred in the last 24 h that they enjoyed and also rated them for vividness of location, time, emotion(s), and a context.
In both groups, events that were not vivid were not candidates for audio cue generation. Finally, the experimenter asked all participants to pair the events with their goals or habits, such that they “went along together, or somehow related to that event.” All of the participants were able to pair at least 3 events with their goals or habits. After generating the EFT/ERT audio cues, participants read the cues aloud into a recorder to listen to at their dinner session the next day. Participants’ audio cues consisted of a 45 min audio file containing 3 separate cues looping in alternating order.
2.3. Measures
2.3.1. Weight and height.
Weight was measured using a digital scale (TANITA Corporation of America Inc., Arlington Heights, IL) and height was measured using a digital stadiometer (Measurement Concept and Quick Medical, North Bend, WA). Height and weight assessments were used to compute BMI (kg/m2). The weight scale was calibrated daily.
2.3.2. Demographics
Age, education level, socioeconomic status, and race/ethnicity were assessed using a questionnaire adapted from MacArthur’s sociodemographic questionnaire, which has been validated for use in women (Adler et al., 2000). To quantify socioeconomic status, the questionnaire asks participants to subjectively rate themselves on a ladder relative to other people in the United States (1 = “best off” and 10= “worst off”).
2.3.3. Calorie and macronutrient intake
Nutritional data for all study foods were obtained from the food court registered dietitian based on manufacturer-provided nutrition information after taking preparation methods and serving sizes into account. Data included serving sizes (gram weights and quantities), calories, and grams of fat, carbohydrate, and protein. Serving sizes for all foods in the cafeteria are standardized, thus allowing for an accurate estimate of the weight of foods prior to consumption. To verify intake data, participants brought their leftovers, including the packages, and verbally recalled what they ate immediately after returning to the experimenter. Then, after the participant left, the experimenter weighed all leftover foods using a KD-400 digital scale (TANITA Corporation of America Inc., Arlington Heights, IL) and subtracted each value from the initial weight of the serving provided by the cafeteria nutritionist. The scale was tared prior to each measurement.
2.3.4. Audio cue ratings
At session 1, participants rated the positivity and vividness of audio cues on a scale from 1 to 5, where 1=not at all positive/vivid and 5= very positive/vivid. Positive episodic future thinking is imagined more vividly than negative future thinking (D’Argembeau and Van der Linden, 2004) and vividness of cues enhances the effect of EFT (Peters and Buchel, 2010). Cues with ratings of 2 or lower on either of these scales were not candidates for audio cue generation.
2.4. Cost
Cost of the training was calculated in terms of graduate student time needed to train participants in EFT or ERT. Each training session took approximately 30min. At $13/h, the cost was $6.50 per subject for EFT cue development and training.
2.5. Analytical plan
Preliminary analyses were conducted to assess group differences in participant characteristics. ANOVA was used to compare continuous variables and Fisher Exact tests were used to compare categorical variables. Pearson’s correlations were used to test whether BMI, weight, or educational attainment were associated with total calories or percent of calories consumed from fat, carbohydrate and protein. Analyses of between group differences in calories or macronutrient intake were run using one-way ANOVA.
One of the participants did not adhere to the experimental protocol, and ate dinner prior to coming to the experiment. In addition, the energy intake analyses revealed three statistical outliers (3 or more standard deviations from the mean) who were also removed from analyses.
3. Results
Basic descriptive statistics are listed in Table 1. There were no significant baseline differences between groups. Additionally, Pearson’s correlations showed that BMI, weight, and educational attainment were not correlated with either total calories or percent of calories from carbohydrate, fat and protein, so covariates were not added to the model.
Table 1.
Participant characteristics for both groups at baseline (mean ± SD).
| EFT-GOAL | ERT | p | |
|---|---|---|---|
| N | 13 | 16 | |
| BMI (kg/m2) | 32.08 ± 5.45 | 30.91 ± 4.06 | 0.52 |
| Weight (kg) | 86.39 ± 14.9 | 80.98 ± 8.75 | 0.23 |
| Age (years) | 36.24 ± 13.24 | 37.20 ± 12.91 | 0.85 |
| Socioeconomic statusa | 4.85 ± 0.99 | 5.19 ± 1.38 | 0.46 |
| Vividness of cues | 4.46 ± 0.48 | 4.29 ± 0.50 | 0.36 |
| Positivity of cues | 4.64 ± 0.40 | 4.63 ± 0.27 | 0.90 |
| Years of education | 15.23 ± 2.95 | 15.50 ± 2.61 | 0.80 |
| Non-white/Caucasian | 23.10% | 25.00% | 0.70 |
Participants subjectively rate their SES level on a scale from 1 to 10, where 1 is the highest standing in the United States and 10 is the lowest standing.
ANOVA revealed a significant difference in calories consumed between groups (Fig. 2), where the EFT group (540.44 ± 178.20, mean ± SD), consumed significantly fewer calories than the ERT group (749.32 ± 169.90; F(1,27) = 10.38, p = 0.003). Significant differences in macronutrient percent of calories were observed for both fat (F(1,27) = 10.487, p = 0.003) and protein (F(1,27) = 6.54, p = 0.016), but not carbohydrate (F(1,27), p = 0.217). Specifically, participants in the EFT group versus ERT consumed significantly less fat (24% vs 37%) and more protein (26% vs 19%). Carbohydrate intake was similar (50% vs 44%) (Fig. 3).
Figure. 2.
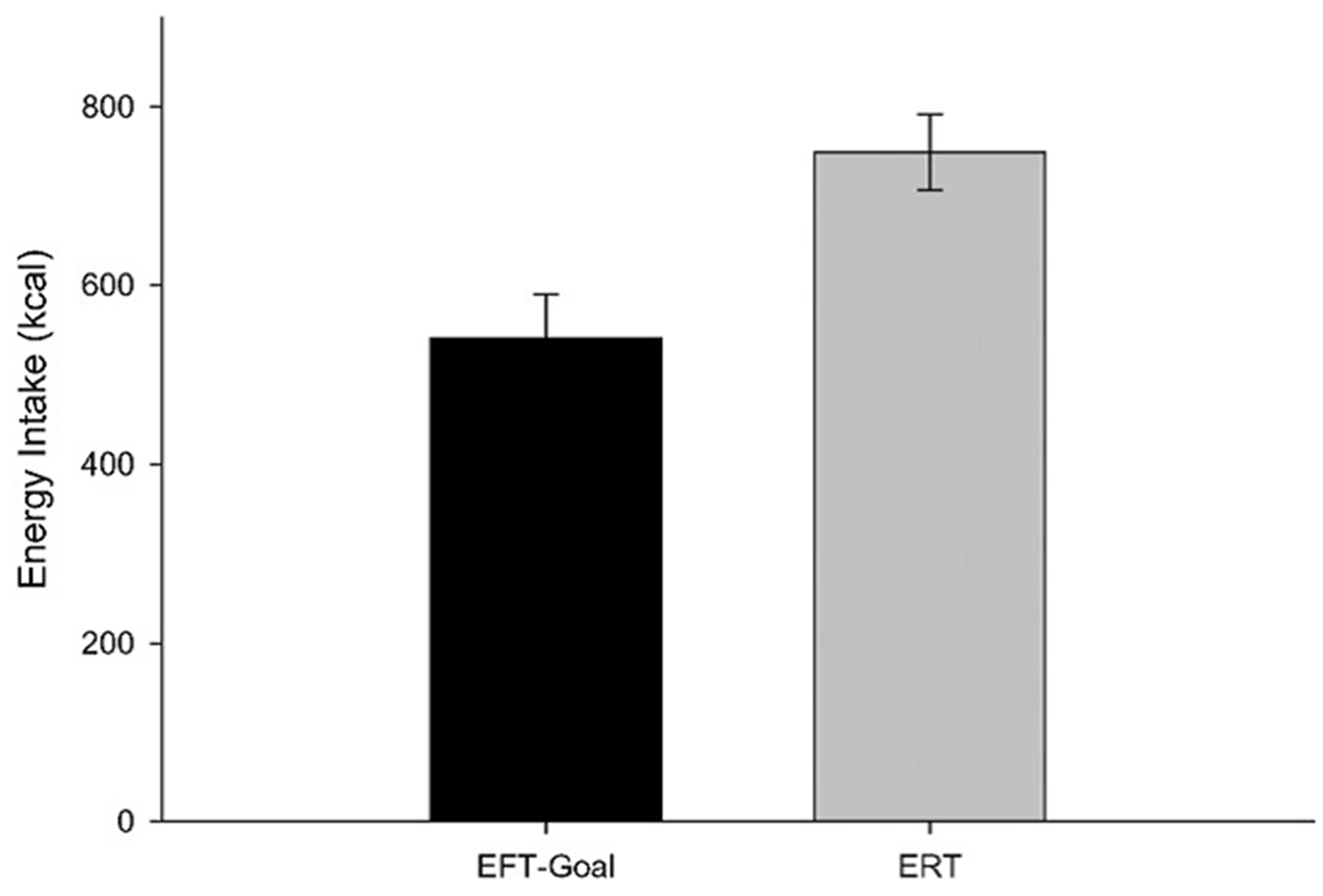
Difference in energy intake between groups (mean ± SEM).
Figure. 3.
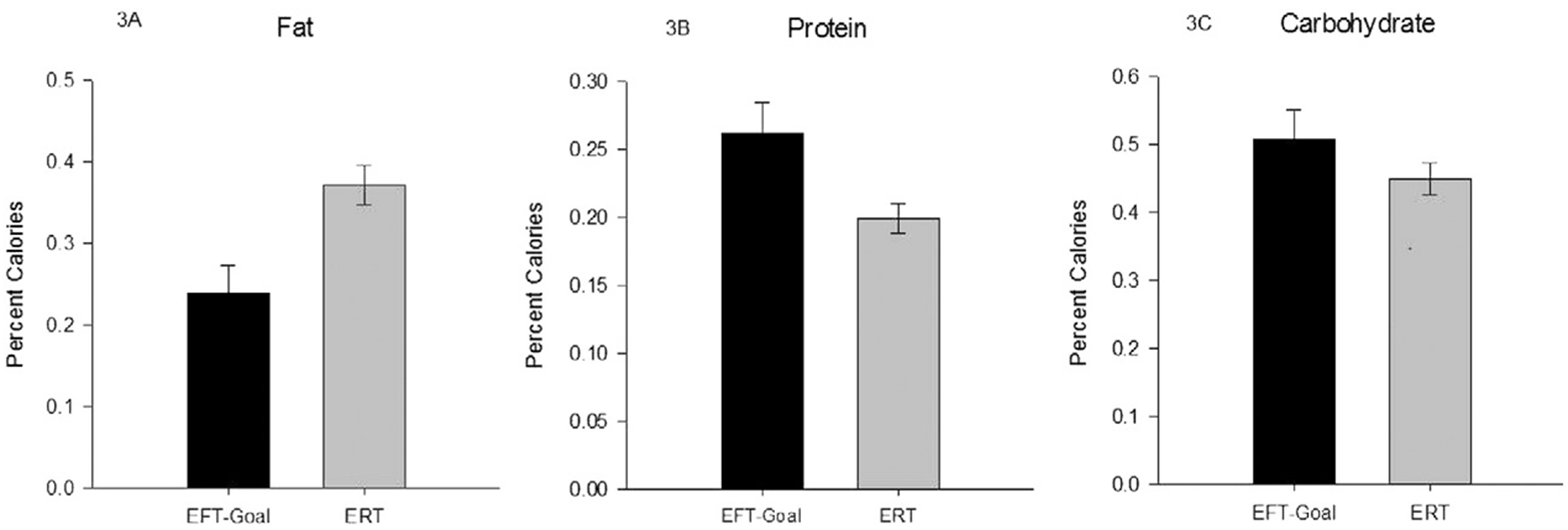
Between-group differences in percent of calories consumed from fat (3A), protein (3B) and carbohydrate (3C) (mean ± SEM).
4. Discussion
EFT has been shown to reduce eating in the laboratory in overweight/obese women (Daniel et al., 2013b) and our study demonstrated that this approach is translatable to the field using a cost-effective and highly transportable technique implemented using a smartphone. Testing EFT in a food court provides the opportunity to establish that EFT can be implemented even in very distracting environments. Because eating occurs in a wide variety of environments, the transportability of cell phones or similar devices allows individuals to access EFT privately as needed, resulting in a technique that is efficient for researchers to customize and easy for people to access. Laboratory research has demonstrated that EFT reduces consumption of unhealthy foods (Daniel et al., 2013b), and this study showed women in the EFT group ate healthier by choosing foods with less fat and more protein. These switches occurred despite the fact that the experimenter did not tell participants which foods were healthy or unhealthy, though this may be common knowledge for some and nutrition information was visible on the menu and in the food court.
Food choice is deeply interwoven with the goal of eating fewer calories; people are more likely to remain on a lower calorie diet when they eat foods that contain fewer calories per gram by choosing to eat foods with fewer fat grams, such as fruits and vegetables (Raynor et al., 2011). Interestingly, foods rated highest in satiety have low fat, high protein, and low energy density (Buckland et al., 2015). In fact, a recent literature review found that eating more lean protein as part of a weight loss program results in increased weight loss, fat mass loss, and maintenance of muscle mass. In the present study, EFT directly influenced participants’ food choices to reduce calories while likely facilitating greater satiety.
One traditional approach to losing weight is counting calories, which requires researching calories for all foods eaten and is inherently difficult to accurately measure (Murakami and Livingstone, 2015). Compared to counting calories, EFT requires fewer behavioral changes, less time commitment, and possibly a lower cognitive load. Another common approach to weight loss is joining a meal replacement program. This prevents the individual from having to make difficult decisions about which foods to eat. While meal replacement programs have been shown to be successful (Kruschitz et al., 2014), the high cost may present a barrier for many individuals. In addition, meal replacement programs prevent people from eating normal meals in a social environment. Compared to these approaches, EFT is a highly portable and effective technique for reducing intake in a complex eating environment. The estimated cost for development and training of EFT was $6.50, and after the person learns EFT, the same audio cues can be re-used for multiple meals, without an increase in cost.
These findings invite further research to identify factors that can help shape EFT-based clinical interventions. It would be useful to develop a program that shapes individuals into being more future-oriented in their everyday decisions, as this may facilitate EFT in one’s everyday life, including eating times. In a culture where people are constantly “on the go,” EFT may be a particularly effective tool for reducing overeating in a wide variety of eating environments by orienting cognitive focus on long term goals rather than the short-term pleasure associated with the large variety of enticing foods commonly encountered. EFT may be an important adjunct to traditional behavioral treatments for modifying diet in those who overeat habitually.
Acknowledgments
The authors wish to express appreciation to Fathima Yasin, Zachary Dziadeszek, Jessica Messina, and Aberlee Milliron for the assistance with recruitment, data entry, and material preparations.
Role of funding sources
This research was funded in part by a grant from the National Institute of Diabetes and Digestive Diseases UO1 DK088380 awarded to Dr. Epstein.
Footnotes
Conflict of interest
Dr. Epstein is a consultant to and has equity in Kurbo. The other authors have no conflict of interest.
References
- Adler NE, Epel ES, Castellazzo G, & Ickovics JR (2000). Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol, 19(6), 586–592. [DOI] [PubMed] [Google Scholar]
- Atance CM, & O’Neill DK (2001). Episodic future thinking. Trends Cogn. Sci, 5(12), 533–539. [DOI] [PubMed] [Google Scholar]
- Benoit RG, Gilbert SJ, & Burgess PW (2011). A neuralmechanismmediating the impact of episodic prospection on farsighted decisions. J. Neurosci, 31(18), 6771–6779. 10.1523/JNEUROSCI.6559-10.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buckland NJ, James Stubbs R, & Finlayson G (2015). Towards a satiety map of common foods: Associations between perceived satiety value of 100 foods and their objective and subjective attributes. Physiol. Behav. 10.1016/j.physbeh.2015.07.001. [DOI] [PubMed] [Google Scholar]
- Clendenen VI, Herman CP, & Polivy J (1994). Social facilitation of eating among friends and strangers. Appetite, 23(1), 1–13. 10.1006/appe.1994.1030. [DOI] [PubMed] [Google Scholar]
- Daniel TO, Stanton CM, & Epstein LH (2013a). The future is now: Comparing the effect of episodic future thinking on impulsivity in lean and obese individuals. Appetite, 71, 120–125. 10.1016/j.appet.2013.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daniel TO, Stanton CM, & Epstein LH (2013b). The future is now: Reducing impulsivity and energy intake using episodic future thinking. Psychol. Sci, 24(11), 2339–2342. 10.1177/0956797613488780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- D’Argembeau A, & Van der Linden M (2004). Phenomenal characteristics associated with projecting oneself back into the past and forward into the future: Influence of valence and temporal distance. Conscious. Cogn, 13(4), 844–858. 10.1016/j.concog.2004.07.007. [DOI] [PubMed] [Google Scholar]
- D’Argembeau A, Stawarczyk D, Majerus S, Collette F, Van der Linden M, Feyers D, … Salmon E (2010). The neural basis of personal goal processing when envisioning future events. J. Cogn. Neurosci, 22(8), 1701–1713. 10.1162/jocn.2009.21314. [DOI] [PubMed] [Google Scholar]
- de Castro JM, King GA, Duarte-Gardea M, Gonzalez-Ayala S, & Kooshian CH (2012). Overweight and obese humans overeat away from home. Appetite, 59(2), 204–211. 10.1016/j.appet.2012.04.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epstein LH, Fletcher KD, O’Neill J, Roemmich JN, Raynor H, & Bouton ME (2013). Food characteristics, long-term habituation and energy intake. Laboratory and field studies. Appetite, 60(1), 40–50. 10.1016/j.appet.2012.08.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jarmolowicz DP, Cherry JB, Reed DD, Bruce JM, Crespi JM, Lusk JL, & Bruce AS (2014). Robust relation between temporal discounting rates and bodymass. Appetite, 78, 63–67. 10.1016/j.appet.2014.02.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katzmarzyk PT, Bray GA, Greenway FL, Johnson WD, Newton RL Jr., Ravussin E, … Bouchard C (2011). Ethnic-specific BMI and waist circumference thresholds. Obesity (Silver Spring), 19(6), 1272–1278. 10.1038/oby.2010.319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kruschitz R,Wallner-Liebmann SJ, Lothaller H, Luger M, Schindler K, Hoppichler F, & Ludvik B (2014). Evaluation of a meal replacement-based weight management program in primary care settings according to the actual European Clinical Practice Guidelines for the Management of Obesity in Adults. Wien. Klin. Wochenschr, 126(19–20), 598–603. 10.1007/s00508-014-0585-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mollen S, Rimal RN, Ruiter RA, & Kok G (2013). Healthy and unhealthy social norms and food selection. Findings from a field-experiment. Appetite, 65, 83–89. 10.1016/j.appet.2013.01.020. [DOI] [PubMed] [Google Scholar]
- Murakami K, & Livingstone MB (2015). Prevalence and characteristics of misreporting of energy intake in US adults: NHANES 2003–2012. Br. J. Nutr, 1–10 10.1017/S0007114515002706. [DOI] [PubMed] [Google Scholar]
- Peters J, & Buchel C (2010). Episodic future thinking reduces reward delay discounting through an enhancement of prefrontal–mediotemporal interactions. Neuron, 66(1), 138–148. 10.1016/j.neuron.2010.03.026. [DOI] [PubMed] [Google Scholar]
- Raynor HA, & Epstein LH (2001). Dietary variety, energy regulation, and obesity. Psychol. Bull, 127(3), 325–341. [DOI] [PubMed] [Google Scholar]
- Raynor HA, Van Walleghen EL, Bachman JL, Looney SM, Phelan S, & Wing RR (2011). Dietary energy density and successful weight loss maintenance. Eat. Behav, 12(2), 119–125. 10.1016/j.eatbeh.2011.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sze YY, Daniel TO, Kilanowski CK, Collins RL, & Epstein LH (2015). Web-based delivery of an episodic future thinking intervention for overweight and obese families: A feasibility study. JMIR mHealth uHealth 10.2196/mhealth.4603 (in press). [DOI] [PMC free article] [PubMed] [Google Scholar]