

Abstract
Neurobiological heterogeneity in obsessive compulsive disorder (OCD) is understudied leading to conflicting neuroimaging findings. Therefore, we investigated objective neuroanatomical subtypes of OCD by adopting a newly proposed method based on gray matter volumes (GMVs). GMVs were derived from T1‐weighted anatomical images of patients with OCD (n = 100) and matched healthy controls (HCs; n = 106). We first inquired whether patients with OCD presented higher interindividual variability HCs in terms of GMVs. Then, we identified distinct subtypes of OCD by adopting heterogeneity through discriminative analysis (HYDRA), where regional GMVs were treated as features. Patients with OCD presented higher interindividual variability than HCs, suggesting a high structural heterogeneity of OCD. HYDRA identified two distinct robust subtypes of OCD presenting opposite neuroanatomical aberrances compared with HCs, while sharing indistinguishable clinical and demographic features. Specifically, Subtype 1 exhibited widespread increased GMVs in cortical and subcortical regions, including the orbitofrontal gyrus, right anterior insula, bilateral hippocampus, and bilateral parahippocampus and cerebellum. Subtype 2 demonstrated overall decreased GMVs in regions such as the orbitofrontal gyrus, right anterior insula, and precuneus. When mixed together, none of patients presented significant differences compared with HCs. In addition, the total intracranial volume of Subtype 2 was significantly correlated with the total score of the Yale–Brown Obsessive Compulsive Scale while that of Subtype 1 was not. These results identified two distinct neuroanatomical subtypes, providing a possible explanation for conflicting neuroimaging findings, and proposed a potential objective taxonomy contributing to precise clinical diagnosis and treatment in OCD.
Keywords: gray matter volume, heterogeneity, machine learning, OCD, subtypes of OCD
We observed high heterogeneity in terms of gray matter volume across patients with OCD and revealed two robust neuroanatomical subtypes of OCD. These two subtypes exhibited remarkably opposite gray matter volume aberrances compared to healthy controls. Our results provide a possible explanation for the conflicting neuroimaging findings and an objective taxonomy contributing to precision clinical diagnosis and treatment of OCD.

1. INTRODUCTION
It is a generally accepted notion that obsessive compulsive disorder (OCD) is a highly heterogeneous disorder reflected in its diversity of symptoms and treatment responses (Alexander, DeLong, & Strick, 1986; McKay et al., 2004). Although OCD is characterized by obsessions and compulsions, OCD symptoms present high interindividual heterogeneity. To handle this heterogeneity, OCD is further divided into various subtypes, such as washing and checking in clinical practice (Mataix‐Cols et al., 2004). Despite the great success, subtypes based on symptomatology often share overlapping patterns of aberrance (Ravindran et al., 2020; Yoo et al., 2008), have a vague diagnostic threshold in terms of how to handle sub‐threshold symptoms, and have low sensitivity (Okada et al., 2015). Moreover, there is no universally accepted taxonomy (McKay et al., 2004). The high heterogeneity obscures the discovery of biomarkers indicative of precision diagnosis and treatment (Chand et al., 2020). Recently, instead of attempting to subtyping patients based on symptom presentation, researchers turn to identify subtypes using objective neuroanatomical data such as structural magnetic resonance imaging (MRI; Abi‐Dargham & Horga, 2016; Chand et al., 2020).
Previous neuroimaging studies have mainly adopted binary case–control strategies to probe abnormal neuroanatomy in OCD. These studies identified brain structural aberrance in distributed brain regions, such as the medial frontal gyrus, middle temporal lobe, anterior insula, and anterior cingutate cortex (Endrass, Klawohn, Schuster, & Kathmann, 2008; Kwon et al., 2003; Menzies, Williams, et al., 2008). Although the cortico‐striato‐thalamo‐cortical circuit is widely accepted as the core circuit of OCD, the heterogeneity hampers reaching validated findings for application to clinical diagnosis, and treatment of OCD (Bokor & Anderson, 2014). Subtypes of OCD are accompanied by distinct genetic characterizations, comorbidities, and treatment responses (Mataix‐Cols et al., 2004; McKay et al., 2004; Starcevic & Brakoulias, 2008). Moreover, neuroimaging studies have shown reduced, increased, and even no differential gray matter volumes (GMVs) in patients with OCD (Lázaro et al., 2011; Okasha et al., 2000). In clinical practice, OCD is subjectively subdivided into subtypes according to symptom representation, because this is no universally accepted taxonomy (McKay et al., 2004). Although studies with dimensional approach demonstrate that obsessive dimensions are mediated by distinct neural systems and correspond to distinct neuropsychological deficits (Di Paola et al., 2013; Mataix‐Cols, Rosario‐Campos, & Leckman, 2005; Piras et al., 2015), and might even be indicative of treatment outcome/selection to some extent (Mataix‐Cols et al., 2005; Starcevic & Brakoulias, 2008), one of the weaknesses is that taxonomy based on phenomenology does not provide the underpinned neuroanatomical aberrance; thus, the obtained subtypes usually share overlapping patterns of aberrance (Piras et al., 2015; Ravindran et al., 2020; Xia et al., 2020; Yoo et al., 2008). In recent years, an increasing number of researchers have tried to handle the heterogeneity by identifying subtypes using objective neuroimaging data in mental disorders (Beijers, Wardenaar, van Loo, & Schoevers, 2019; Chand et al., 2020; Marquand, Wolfers, Mennes, Buitelaar, & Beckmann, 2016).
Objective identification of distinct neuroanatomical subtypes of mental disorders is a growing trend. Patients with mental disorders exhibit high heterogeneity, leading to inconsistent findings (Sun et al., 2021). To address this heterogeneity, Dwyer et al. (2018) uncovered two neuroanatomical subtypes of schizophrenia, thus improving stratification for computer‐aided diagnosis. Chand et al. adopted a semi‐supervised method and revealed two robust subtypes, where Subtype 1 presents widespread decreased GMVs, while Subtype 2 presents increased GMVs in the basal ganglia and internal capsule. These two subtypes challenge the widely accepted notion that schizophrenia is characterized by general brain volume loss (Chand et al., 2020), helping to deepen our understanding of the mechanism and move toward targeted treatment (Varol, Sotiras, & Davatzikos, 2017). Nevertheless, no study has explored the putative subtypes of OCD.
In this study, we aimed to uncover putative neuroanatomical subtypes of OCD by adopting a newly proposed method named heterogeneity through discriminative analysis (HYDRA) from GMVs (Varol et al., 2017). HYDRA can identify subtypes by mapping differences from a normal population rather than clustering patients directly (Chand et al., 2020). Furthermore, this method excluded the effects of confounding factors, such as age and sex (Chand et al., 2020). First, we investigated whether OCD exhibited a higher structural heterogeneity than healthy controls (HCs). Then, we adopted HYDRA to reveal subtypes of OCD from GMV obtained by voxel based morphometry (VBM). There were two main hypotheses: (a) OCD would exhibit higher interindividual heterogeneity considering its various symptom representations in clinical settings and (b) HYDRA can uncover subtypes with distinct neuroanatomical aberrance.
2. MATERIALS AND METHODS
2.1. Sample
In this study, we recruited 100 patients with OCD and 106 HCs. Patients were recruited from outpatient services of the Department of Psychiatry, The First Affiliated Hospital of Zhengzhou University. The diagnosis was made by two experienced psychiatrists according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM‐V) for OCD. The patients were all drag‐naive and first‐episode. Patients were excluded if they had comorbid other mental/psychotic disorders, nervous system disease/brain trauma, or first‐degree relatives with a history of mental illness or neurological disease. The Yale–Brown Obsessive Compulsive Scale (Y‐BOCS) was used to evaluate symptom severity (Goodman et al., 1989). HCs were recruited from the community through poster advertisement. Neither of them had a history of serious medical nor neuropsychiatric illness or a family history of major psychiatric or neurological illness in their first‐degree relatives.
In addition, all participants were Han Chinese, right‐handed, and had to meet the following exclusion criteria: (a) taking drugs such as anesthetics, those that were sleep‐inducing, or analgesics in the past month; (b) substance abuse; (c) a history of a brain tumor, trauma, surgery, or other organic body diseases; (d) suffering from cardiovascular diseases, diabetes, or hypertension; (e) has contraindications for MRI scanning; and (f) has other structural brain abnormalities.
Written informed consent was obtained from all the participants before the experiment. The study was approved by the research ethics committee of the First Affiliated Hospital of Zhengzhou University and adhered to the Helsinki Declaration.
2.2. Data acquisition
High‐resolution T1‐weighted anatomical images of participants were acquired using on 3‐T GE Discovery MR750 scanner (General Electric). T1‐weighted images were obtained using the following parameters: repetition time = 8,164 ms, echo time = 3.18 ms, inversion time = 900 ms, flip angle = 7°, resolution matrix = 256 × 256, slices = 188, thickness = 1.0 mm, and voxel size = 1 × 1 × 1 mm3.
2.3. Voxel‐based morphometry analysis
CAT 12 (http://dbm.neuro.uni-jena.de/cat12/) toolbox was used to calculate voxel‐based morphometry (VBM) for each subject. We followed the recommended pipeline of CAT 12 mainly including reorientation of images, segmentation into gray matter, white matter, and cerebrospinal fluid volume. Segmented images were normalized into Montreal Neurological Institute space and resampled to 1.5 × 1.5 × 1.5 mm followed by nonlinear modulation (Ashburner, 2009; Han, Chen, et al., 2021; Han, Zheng, et al., 2021). Finally, the gray matter maps were smoothed using 6 mm full width at half maximum Gaussian kernel (FWHM). The quality of obtained gray matter maps is included in Table 1. The total intracranial volume (TIV) for each participant was estimated for the next produces.
TABLE 1.
Demographic and clinical characteristics of participants
| HC (N = 106) | OCD (N = 100) | p | |
|---|---|---|---|
| Male, no. (%) | 53 (50.00) | 53 (53.00) | .99 a |
| Age, mean (SD) [range], y | 23.09 (5.63) [16–43] | 22.93 (9.31) [12–49] | .88 b |
| Educational level, mean (SD), y | 15.18 (3.19) | 11.82 (3.16) | <.01 b |
| Duration of illness, mean (SD), m | — | 48.08 (57.61) | |
| Y‐BOCS score, mean (SD) | — | 21.92 (7.09) | |
| TIV, mean (SD), 103 cm3 | 1.55 (0.13) | 1.55 (0.14) | .70 b |
| IQR, mean (SD) | 2.09 (0.15) | 2.09 (0.16) | .98 b |
Abbreviations: HC, healthy control; OCD, obsessive–compulsive disorder; IQR, imaging quality rating; TIV, total intracranial volume; Y‐BOCS, Yale–Brown Obsessive Compulsive Scale.
χ 2 t test.
Two‐tailed two sample t test.
2.4. Heterogeneity of GMV and group difference
First, we investigated whether patients with OCD exhibited higher interindividual variability than HCs. To map the interindividual variability/distance, we extracted regional GMVs based on the brain atlas(268 brain region atlas and validated with 200 brain atlas (Craddock, James, Holtzheimer 3rd, Hu, & Mayberg, 2012; Shen, Tokoglu, Papademetris, & Constable, 2013). Thus, 1 M × 1 (M for the total number of brain regions) GMV vector for each subject was obtained. Then, the Euclidean distance between pairs of GMV vectors was calculated. An N × N (subject × subject) structural distance matrix was obtained for each group. This procedure was performed separately in OCD and HCs. For each subject, the variability value was defined as the mean value of distance values (N−1 excluding the distance to itself) representing the distance (variability) between this one and the others in the group. Thus, a heterogeneous group was expected to have larger variability values than those in the homogeneous group. A two sample t test was performed to compare variability values in OCD with that in HCs, after adjusting for age, sex, and educational level.
2.5. Subtyping with HYDRA
Thereafter, we clustered patients with OCD into subtypes using a recently proposed semi‐supervised method named HYDRA where regional GMVs were treated as features (Chand et al., 2020; Varol et al., 2017). HYDRA performed classification and subtyping simultaneously and successfully revealed two distinct neuroanatomical subtypes of schizophrenia (Chand et al., 2020). This method adaptively determines the number of clusters according to the adjusted rand index (ARI), which quantifies the similarity between clustering results of cross‐validation (Varol et al., 2017). The optimal number of clusters was determined when ARI was the largest. As done in previous studies (Chand et al., 2020, 2022; Varol et al., 2017), we identified optimal subtypes of OCD from 1 to 6 using 10‐fold cross validation where age, sex, and education level were included as covariates. The workflow is shown in Figure 1.
FIGURE 1.
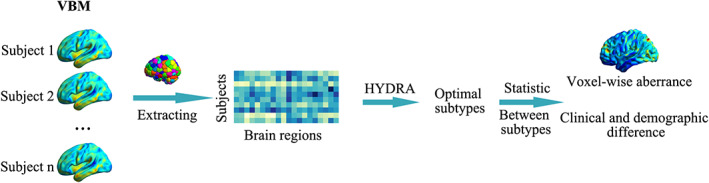
The workflow of subtyping OCD
Voxel‐wise GMV aberrance was also obtained for each subtype of OCD (and all patients vs. HC) compared with HCs using a two sample t test equipped in SPM12 where age, sex, educational level, and TIV were included as covariates. Voxel‐wise results were corrected using FDR (p < .005).
2.6. Reproducibility analysis
To confirm the robustness of the subtyping results, we validated the subtyping results using (a) different brain atlases (268/200 brain atlas; Craddock et al., 2012; Shen et al., 2013); and (b) to exclude the possibility that subtyping results were driven by a few subjects, we randomly selected 80% of subjects (for HCs and patients, respectively) and performed the same subtyping results on the sub‐samples. ARI was calculated between the subtyping result obtained from sub‐samples and that from the whole dataset (all HCs and patients). This procedure was repeated 100 times; (c) to investigate whether GMVs could distinguish between these two subtypes, and a linear support vector machine (SVM, equipped in LIBSVM, https://www.csie.ntu.edu.tw/~cjlin/libsvm/index.html) classifier was constructed using the same features (regional GMVs; Marquand et al., 2016). The performance of the model was evaluated using a leave‐one‐out cross‐validation strategy, and the significance was determined by a permutation test (1,000 times; Han, Chen, et al., 2021; Han et al., 2019; Li et al., 2021).
2.7. External validation
To assess clinical validity, we investigated whether these two subtypes demonstrated significant differences in clinical and demographic features, including age, sex, education level, duration of illness, and the total score of Y‐BOCS with a two‐sample t test or χ 2 test. In addition, Pearson's correlation between TIV and duration of illness/the total score of Y‐BOCS was calculated for each subtype to investigate whether the association between neuroimaging representation and severity of symptoms differed between these two subtypes.
3. RESULTS
3.1. Clinical demographics
Demographic information was included in Table 1. Patients with OCD showed no significant difference (p > .05) in terms of age, TIV, IQR, and sex, but had fewer years of education compared with HCs.
3.2. Higher heterogeneity of GMV in OCD
To depict the heterogeneity of GMV, we calculated the variability value for each subject in OCD and HCs separately. Variability values in OCD were compared with those in HCs to determine whether patients with OCD had higher heterogeneity. As a result, patients with OCD presented significantly larger variability values than those in HCs (t = 3.11, p < .01, Cohen's d = 0.43) that was confirmed with 200 regions brain atlas (t = 2.89, p < .01, Cohen's d = 0.40; Figure 2a).
FIGURE 2.
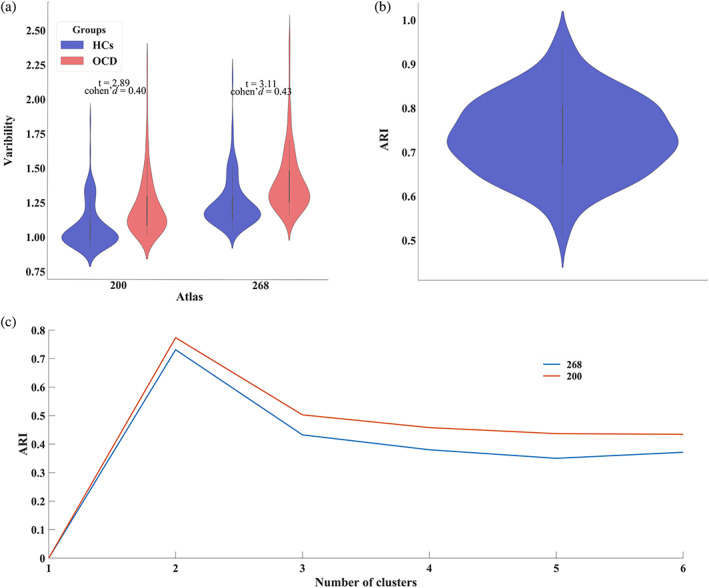
Higher heterogeneity and subtyping results of OCD. (a). Patients with OCD exhibited higher structural heterogeneity (variability) than HCs. (b). ARI values between subtyping results of the randomly selected sub‐dataset and reported one. (c). ARI values of different numbers of subtypes
3.3. Two OCD subtypes exhibit opposite GMV difference
The optimal number of subtypes was 2, where the ARI was maximum for 268 brain regions brain atlas (Figure 2c). The numbers of patients in subtypes 1 and 2 were 50 and 50, respectively.
These two subtypes exhibited opposite voxel‐wise GMV differences compared to HCs. Specifically, Subtype 1 exhibited widespread increased GMV in brain regions, including the right anterior insula, bilateral middle temporal gyrus, bilateral hippocampus, bilateral parahippocampus, precuneus, frontal gyrus, and cerebellum. Subtype 2 demonstrated overall decreased GMV in the orbitofrontal gyrus, precuneus, posterior cingulate, and putamen. The details are shown in Figure 3 and Table S1. We also obtained the GMV aberrance of OCD subtypes according to regional GMVs based on the 200 brain atlas (Figure 3). The GMV aberrance of subtypes with the 200 brain atlas was consistent with that of 268 (Subtype 1: spatial correlation r = .99, p < .01; Subtype 2: spatial correlation r = .98, p < .001). There were no significant differences between all patients with OCD and HCs.
FIGURE 3.
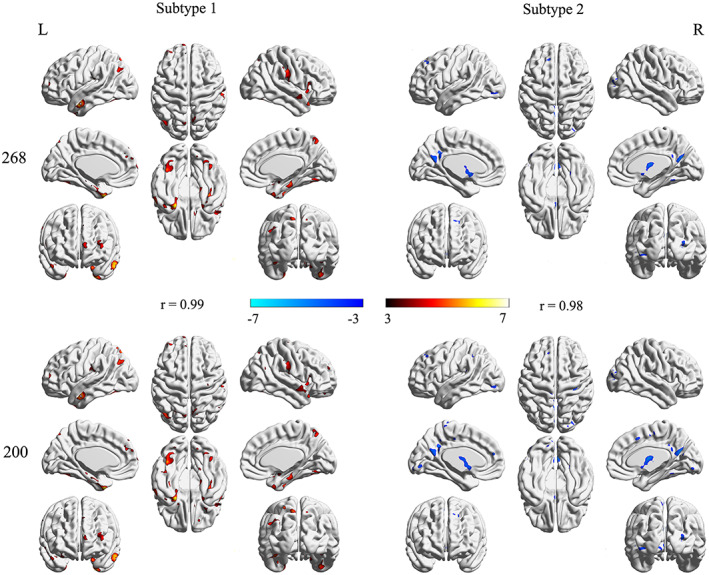
Voxel‐wise GMV aberrance in each subtype of OCD. The “r” represented the spatial correlation between the GMV aberrance of subtypes based on 268 and 200 brain atlas
3.4. Reproducibility results
Various strategies were adopted to investigate the subtype reproducibility. As a result, our subtyping results were robust and reproducible. Specifically, the optimal number of subtypes was consistently 2, and the ARI between these subtyping results obtained from different brain atlases was 0.89. The ARI values between the original subtyping result using whole samples and that based on randomly selected sub‐samples datasets were 0.74 ± 0.09 (Figure 2b). Regional GMVs could distinguish between these two subtypes (accuracy reached 87%, p < .05 for permutation). These results suggested that patients with OCD could be robustly divided into two subtypes.
3.5. External validation results
These were no differences in age, sex, educational level, duration of illness, and total Y‐BOCS scores between these two subtypes (all p > .05). However, TIV of Subtype 2 was significantly correlated with the total Y‐BOCS scores (r = −.36, p = .01) while that of Subtype 1 was not (Figure 4).
FIGURE 4.
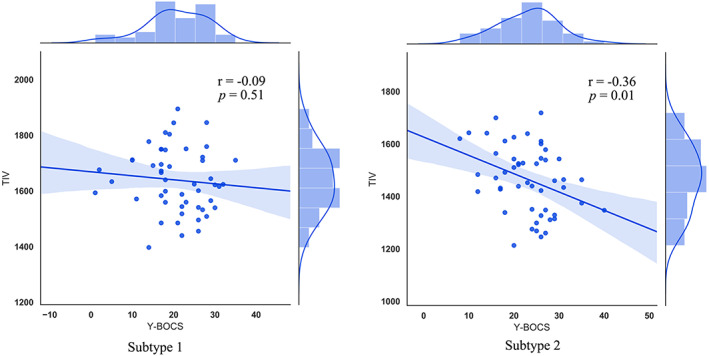
Correlation between the total intracranial volume and total Y‐BOCS scores in subtypes
4. DISCUSSION
In this study, we had two main findings: (a) patients with OCD presented higher structural heterogeneity than HCs. These results suggested a high level of structural heterogeneity in OCD for the first time and (b) we identified two remarkably distinct subtypes of OCD presenting opposite structural aberrances compared to HCs. Subtype 1 exhibited a widespread increase in GMV, whereas Subtype 2 exhibited decreased GMVs. In addition, TIV in Subtype 2 was associated with symptom severity, where TIV in Subtype 1 was not. These results revealed two neuroanatomical subtypes demonstrating opposite structural aberrances, offering an explanation for the conflicting findings in OCD. The two identified subtypes provide potential clues for the nosology of OCD.
We identified a high level of structural heterogeneity in OCD. In the clinic, patients with OCD demonstrated various symptoms and were often grouped into subtypes based on symptom representation (Starcevic & Brakoulias, 2008). These subtypes exhibited distinct neuropsychological deficits along with different symptom profiles (McKay et al., 2004; Starcevic & Brakoulias, 2008). Other mental disorders, such as schizophrenia, were found to exhibit higher interindividual variability measured using different methods (Cole, Anticevic, Repovs, & Barch, 2011; Gopal et al., 2016; Sun et al., 2021). Heterogeneity hampered the revelation of neuropathological mechanisms and the discovery of stabilized biomarkers to guide clinical diagnosis and treatment (Sun et al., 2021). However, the heterogeneity of OCD remained unclear. Knowing this was the first step in the precision diagnosis and determination of follow‐up treatment plans. Our results showed that high level of heterogeneity in OCD for the first time. This result confirmed that OCD was a highly heterogeneous disorder and highlighted the necessity of studying subtypes of OCD.
After affirming the high heterogeneity of OCD, we revealed two robust subtypes of OCD using a semi‐supervised method. To handle heterogeneity, OCD was further divided into various subtypes according to symptom presentation, such as washing and checking (Mataix‐Cols et al., 2004). However, this taxonomy based on phenomenology resulted into subtypes sharing overlapping patterns of aberrance (Ravindran et al., 2020; Xia et al., 2020; Yoo et al., 2008), and presented a vague diagnostic threshold to handle sub‐threshold symptoms, thus having low sensitivity (Okada et al., 2015). Moreover, there was no universally accepted taxonomy (McKay et al., 2004). Although studies with dimensional approach demonstrated great success, we aimed to address the heterogeneity by identifying subtypes using objective neuroimaging data. In this study, we revealed two objective subtypes using structural information derived from neuroimaging data for the first time. The exclusion criteria used in this study ruled out other factors, such as comorbidities with other mental disorders and medicine (McKay et al., 2004). These two subtypes exhibited distinct structural aberrances, providing new insights into the taxonomy of OCD. We did not observe any differences in age and illness duration between these two subtypes; however, this result did not mean that they did not affect structural aberrance in OCD. Studies found that age and illness duration drove the enlargement of striatal areas (Boedhoe et al., 2017; de Wit et al., 2014). One plausible explanation was that the effect of age/illness duration could be ignored when compared with the inherent differences between these subtypes revealed in this study. Another reason might be that there was no significant difference between children and adults with OCD (Rotge et al., 2010).
It was worth noting that these two subtypes presented opposite patterns of structural aberrances. Although the cortico‐striato‐thalamo‐cortical circuit was widely accepted as the core circuit, findings from neuroimaging studies were far from consistent in OCD (Bruin, Taylor, Thomas, & Shock, 2020; Kong et al., 2020; Yun et al., 2020). These two subtypes exhibited abnormal GMV in regions, that were consistently found, included, or beyond this circuit (Alexander et al., 1986; Boedhoe et al., 2018; Hazari, Narayanaswamy, & Venkatasubramanian, 2019; Menzies, Chamberlain, et al., 2008) while presenting remarkable opposite patterns of structural aberrances, such as the orbitofrontal gyrus and right anterior insula. Consistent with findings of hypermetabolism and increased cerebral bold flow as revealed by functional brain imaging (Saxena, Brody, Schwartz, & Baxter, 1998; Saxena & Rauch, 2000; Swedo et al., 1992), the volume of the orbitofrontal gyrus was found to be increased in OCD (Kim et al., 2001; Pujol et al., 2004; Szeszko et al., 2008). However, other studies found that gray matter volume of the orbitofrontal gyrus was decreased (van den Heuvel et al., 2009; Pujol et al., 2004). A possible explanation was that hyperactivity compensated for decreased neuronal density. Alternatively, hyperactivity lead to neurotoxic changes resulting in volume reduction (Endrass et al., 2008). As another key region in OCD, the right anterior insula was suggested to be responsible for the poor inhibitory control in OCD (Fan et al., 2016). The findings of the right anterior insula were also mixed, wherein both increased (Nishida et al., 2011; Yoo et al., 2008) and decreased (Besiroglu et al., 2011; Subirà et al., 2013) GMVs were reported, although these inconsonant results might be attributed to medical exposure, methodological differences, age, comorbidity, or illness duration. Our results showed that the main reason for this might be the high heterogeneity of OCD. Especially, Wu et al. (2021) uncovered two subgroups with distinct symptom profiles using a large sample of children with OCD, providing powerful evidence of the high heterogeneity in OCD. In fact, when mixed together, all patients presented no significant differences compared with the HCs in our study. These two distinct neuroanatomical subtypes might be related to the pathogenesis of OCD rather than those caused by other factors, such as age, illness duration, educational level, and medicine. Recently, researchers began to acknowledge this high heterogeneity and realized that group‐level differences in brain structure were not representative of every patient in mental disorders (Liu et al., 2021; Lv, Di Biase, Cash, & Cocchi, 2020; Wolfers et al., 2018; Wolfers & Beckmann, 2020). However, to the best of our knowledge, a limited number of studies focused on structural aberrance in subtypes of OCD (e.g., children vs. adults, contamination vs. aggressive; Boedhoe et al., 2018, 2017; Yoo et al., 2008). Our results indicated that future researchers might pay more attention to more homogeneous samples, and, even individualized aberrance, in the study of OCD.
5. LIMITATIONS
Several limitations should be considered when interpreting our results. First, we used multiple strategies to confirm the reliability of the results. These results were obtained in a single dataset, one more dataset was needed to confirm these results in the future. Second, we did not record the obsessive dimensions; thus, we could not investigate the association between neuroanatomical aberrance and symptom dimensions. Future studies should examine this relationship. Third, factors such as body mass index and alcohol/cigarette use were not well controlled in this study (Abramovitch et al., 2019; Abramovitch, Pizzagalli, Geller, Reuman, & Wilhelm, 2015; Torres et al., 2006), and future studies could evaluate their effects on these results. Fourth, we did not include patients with late‐onset OCD; thus, we could not determine whether our conclusion holds true for late‐onset OCD.
6. CONCLUSION
We observed high heterogeneity in terms of gray matter volume across patients with OCD and revealed two robust neuroanatomical subtypes of OCD. These two subtypes exhibited remarkably opposite gray matter volume aberrances compared to healthy controls. Our results provide a possible explanation for the conflicting neuroimaging findings and an objective taxonomy contributing to precision clinical diagnosis and treatment of OCD.
CONFLICT OF INTERESTS
The authors declare no potential conflict of interest.
AUTHOR CONTRIBUTIONS
Shaoqiang Han, Yong Zhang and Jingliang Cheng designed the study. Yinhuan Xu and Hui‐Rong Guo collected the data. Shaoqiang Han, Yarui Wei, and Keke Fang analyzed the data. Shaoqiang Han and Yong Zhang drafted the work. Liang Liu and Junying Cheng revised the draft.
Supporting information
Table S1 Altered GMVs in subtypes of OCD.
ACKNOWLEDGMENTS
This study was supported by the Natural Science Foundation of China (81601467, 81871327, and 62106229) and Medical Science and Technology Research Project of Henan province (201701011, SBGJ202102103, and SBGJ202101013).
Han, S. , Xu, Y. , Guo, H.‐R. , Fang, K. , Wei, Y. , Liu, L. , Cheng, J. , Zhang, Y. , & Cheng, J. (2022). Two distinct subtypes of obsessive compulsive disorder revealed by heterogeneity through discriminative analysis. Human Brain Mapping, 43(10), 3037–3046. 10.1002/hbm.25833
Funding information Medical science and technology research project of Henan province, Grant/Award Numbers: 201701011, SBGJ202101013, SBGJ202102103; National Natural Science Foundation of China, Grant/Award Numbers: 62106229, 81601467, 81871327
Contributor Information
Shaoqiang Han, Email: shaqianghan@163.com.
Yong Zhang, Email: zzuzhangyong2013@163.com.
Jingliang Cheng, Email: fccchengjl@zzu.edu.cn.
DATA AVAILABILITY STATEMENT
Some or all data, models, or code that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Abi‐Dargham, A. , & Horga, G. (2016). The search for imaging biomarkers in psychiatric disorders. Nature Medicine, 22(11), 1248–1255. 10.1038/nm.4190 [DOI] [PubMed] [Google Scholar]
- Abramovitch, A. , Anholt, G. E. , Cooperman, A. , van Balkom, A. , Giltay, E. J. , Penninx, B. W. , & van Oppen, P. (2019). Body mass index in obsessive‐compulsive disorder. Journal of Affective Disorders, 245, 145–151. 10.1016/j.jad.2018.10.116 [DOI] [PubMed] [Google Scholar]
- Abramovitch, A. , Pizzagalli, D. A. , Geller, D. A. , Reuman, L. , & Wilhelm, S. (2015). Cigarette smoking in obsessive‐compulsive disorder and unaffected parents of OCD patients. European Psychiatry, 30(1), 137–144. 10.1016/j.eurpsy.2013.12.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alexander, G. E. , DeLong, M. R. , & Strick, P. L. (1986). Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annual Review of Neuroscience, 9, 357–381. 10.1146/annurev.ne.09.030186.002041 [DOI] [PubMed] [Google Scholar]
- Ashburner, J. (2009). Computational anatomy with the SPM software. Magnetic Resonance Imaging, 27(8), 1163–1174. 10.1016/j.mri.2009.01.006 [DOI] [PubMed] [Google Scholar]
- Beijers, L. , Wardenaar, K. J. , van Loo, H. M. , & Schoevers, R. A. (2019). Data‐driven biological subtypes of depression: Systematic review of biological approaches to depression subtyping. Molecular Psychiatry, 24(6), 888–900. 10.1038/s41380-019-0385-5 [DOI] [PubMed] [Google Scholar]
- Besiroglu, L. , Sozen, M. , Ozbebit, O. , Avcu, S. , Selvi, Y. , Bora, A. , … Bulut, M. D. (2011). The involvement of distinct neural systems in patients with obsessive‐compulsive disorder with autogenous and reactive obsessions. Acta Psychiatrica Scandinavica, 124(2), 141–151. 10.1111/j.1600-0447.2011.01726.x [DOI] [PubMed] [Google Scholar]
- Boedhoe, P. S. W. , Schmaal, L. , Abe, Y. , Alonso, P. , Ameis, S. H. , Anticevic, A. , … van den Heuvel, O. A. (2018). Cortical abnormalities associated with pediatric and adult obsessive‐compulsive disorder: Findings from the ENIGMA obsessive‐compulsive disorder working group. The American Journal of Psychiatry, 175(5), 453–462. 10.1176/appi.ajp.2017.17050485 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boedhoe, P. S. W. , Schmaal, L. , Abe, Y. , Ameis, S. H. , Arnold, P. D. , Batistuzzo, M. C. , … van den Heuvel, O. A. (2017). Distinct subcortical volume alterations in pediatric and adult OCD: A worldwide meta‐ and mega‐analysis. The American Journal of Psychiatry, 174(1), 60–69. 10.1176/appi.ajp.2016.16020201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bokor, G. , & Anderson, P. D. (2014). Obsessive‐compulsive disorder. Journal of Pharmacy Practice, 27(2), 116–130. 10.1177/0897190014521996 [DOI] [PubMed] [Google Scholar]
- Bruin, W. B. , Taylor, L. , Thomas, R. M. , & Shock, J. P. (2020). Structural neuroimaging biomarkers for obsessive‐compulsive disorder in the ENIGMA‐OCD consortium: Medication matters. Translational Psychiatry, 10(1), 342. 10.1038/s41398-020-01013-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chand, G. B. , Dwyer, D. B. , Erus, G. , Sotiras, A. , Varol, E. , Srinivasan, D. , … Davatzikos, C. (2020). Two distinct neuroanatomical subtypes of schizophrenia revealed using machine learning. Brain, 143(3), 1027–1038. 10.1093/brain/awaa025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chand, G. B. , Singhal, P. , Dwyer, D. B. , Wen, J. , Erus, G. , Doshi, J. , … Davatzikos, C. (2022). Two schizophrenia imaging signatures and their associations with cognition, psychopathology, and genetics in the general population. medRxiv. 10.1101/2022.01.07.22268854 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole, M. W. , Anticevic, A. , Repovs, G. , & Barch, D. (2011). Variable global dysconnectivity and individual differences in schizophrenia. Biological Psychiatry, 70(1), 43–50. 10.1016/j.biopsych.2011.02.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craddock, R. C. , James, G. A. , Holtzheimer, P. E., 3rd , Hu, X. P. , & Mayberg, H. S. (2012). A whole brain fMRI atlas generated via spatially constrained spectral clustering. Human Brain Mapping, 33(8), 1914–1928. 10.1002/hbm.21333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Di Paola, M. , Luders, E. , Rubino, I. A. , Siracusano, A. , Manfredi, G. , Girardi, P. , … Spalletta, G. (2013). The structure of the corpus callosum in obsessive compulsive disorder. European Psychiatry, 28(8), 499–506. 10.1016/j.eurpsy.2012.07.001 [DOI] [PubMed] [Google Scholar]
- Dwyer, D. B. , Cabral, C. , Kambeitz‐Ilankovic, L. , Sanfelici, R. , Kambeitz, J. , Calhoun, V. , … Koutsouleris, N. (2018). Brain subtyping enhances the neuroanatomical discrimination of schizophrenia. Schizophrenia Bulletin, 44(5), 1060–1069. 10.1093/schbul/sby008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Endrass, T. , Klawohn, J. , Schuster, F. , & Kathmann, N. (2008). Overactive performance monitoring in obsessive‐compulsive disorder: ERP evidence from correct and erroneous reactions. Neuropsychologia, 46(7), 1877–1887. 10.1016/j.neuropsychologia.2007.12.001 [DOI] [PubMed] [Google Scholar]
- Fan, J. , Liu, W. , Lei, H. , Cai, L. , Zhong, M. , Dong, J. , … Zhu, X. (2016). Components of inhibition in autogenous‐ and reactive‐type obsessive‐compulsive disorder: Dissociation of interference control. Biological Psychology, 117, 117–130. 10.1016/j.biopsycho.2016.03.008 [DOI] [PubMed] [Google Scholar]
- Goodman, W. K. , Price, L. H. , Rasmussen, S. A. , Mazure, C. , Fleischmann, R. L. , Hill, C. L. , … Charney, D. S. (1989). The Yale‐Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Archives of General Psychiatry, 46(11), 1006–1011. 10.1001/archpsyc.1989.01810110048007 [DOI] [PubMed] [Google Scholar]
- Gopal, S. , Miller, R. L. , Michael, A. , Adali, T. , Cetin, M. , Rachakonda, S. , … Calhoun, V. D. (2016). Spatial variance in resting fMRI networks of schizophrenia patients: An independent vector analysis. Schizophrenia Bulletin, 42(1), 152–160. 10.1093/schbul/sbv085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Han, S. , Chen, Y. , Zheng, R. , Li, S. , Jiang, Y. , Wang, C. , … Cheng, J. (2021). The stage‐specifically accelerated brain aging in never‐treated first‐episode patients with depression. Human Brain Mapping, 42(11), 3656–3666. 10.1002/hbm.25460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Han, S. , Wang, Y. , Liao, W. , Duan, X. , Guo, J. , Yu, Y. , … Chen, H. (2019). The distinguishing intrinsic brain circuitry in treatment‐naïve first‐episode schizophrenia: Ensemble learning classification. Neurocomputing, 365, 44–53. [Google Scholar]
- Han, S. , Zheng, R. , Li, S. , Liu, L. , Wang, C. , Jiang, Y. , … Cheng, J. (2021). Progressive brain structural abnormality in depression assessed with MR imaging by using causal network analysis. Psychological Medicine. Advance online publication. 10.1017/s0033291721003986 [DOI] [PubMed] [Google Scholar]
- Hazari, N. , Narayanaswamy, J. C. , & Venkatasubramanian, G. (2019). Neuroimaging findings in obsessive‐compulsive disorder: A narrative review to elucidate neurobiological underpinnings. Indian Journal of Psychiatry, 61(Suppl 1), S9–s29. 10.4103/psychiatry.IndianJPsychiatry_525_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van den Heuvel, O. A. , Remijnse, P. L. , Mataix‐Cols, D. , Vrenken, H. , Groenewegen, H. J. , Uylings, H. B. , … Veltman, D. J. (2009). The major symptom dimensions of obsessive‐compulsive disorder are mediated by partially distinct neural systems. Brain, 132(Pt 4), 853–868. 10.1093/brain/awn267 [DOI] [PubMed] [Google Scholar]
- Kim, J. J. , Lee, M. C. , Kim, J. , Kim, I. Y. , Sun, I. K. , Han, M. H. , … Kwon, J. S. (2001). Grey matter abnormalities in obsessive–compulsive disorder: Statistical parametric mapping of segmented magnetic resonance images. British Journal of Psychiatry the Journal of Mental Science, 179(5), 330–334. [DOI] [PubMed] [Google Scholar]
- Kong, X. Z. , Boedhoe, P. S. W. , Abe, Y. , Alonso, P. , Ameis, S. H. , Arnold, P. D. , … Francks, C. (2020). Mapping cortical and subcortical asymmetry in obsessive‐compulsive disorder: Findings from the ENIGMA Consortium. Biological Psychiatry, 87(12), 1022–1034. 10.1016/j.biopsych.2019.04.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwon, J. S. , Kim, J. J. , Lee, D. W. , Lee, J. S. , Lee, D. S. , Kim, M. S. , … Lee, M. C. (2003). Neural correlates of clinical symptoms and cognitive dysfunctions in obsessive‐compulsive disorder. Psychiatry Research, 122(1), 37–47. 10.1016/s0925-4927(02)00104-x [DOI] [PubMed] [Google Scholar]
- Lázaro, L. , Castro‐Fornieles, J. , Cullell, C. , Andrés, S. , Falcón, C. , Calvo, R. , & Bargalló, N. (2011). A voxel‐based morphometric MRI study of stabilized obsessive‐compulsive adolescent patients. Progress in Neuro‐Psychopharmacology & Biological Psychiatry, 35(8), 1863–1869. 10.1016/j.pnpbp.2011.07.016 [DOI] [PubMed] [Google Scholar]
- Li, C. , Dong, M. , Womer, F. Y. , Han, S. , Yin, Y. , Jiang, X. , … Wang, F. (2021). Transdiagnostic time‐varying dysconnectivity across major psychiatric disorders. Transdiagnostic Time‐Varying Dysconnectivity across Major Psychiatric Disorders., 42(4), 1182–1196. 10.1002/hbm.25285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, Z. , Palaniyappan, L. , Wu, X. , Zhang, K. , Du, J. , Zhao, Q. , … Lin, C. P. (2021). Resolving heterogeneity in schizophrenia through a novel systems approach to brain structure: Individualized structural covariance network analysis. Molecular Psychiatry, 26, 7719–7731. 10.1038/s41380-021-01229-4 [DOI] [PubMed] [Google Scholar]
- Lv, J. , Di Biase, M. , Cash, R. F. H. , & Cocchi, L. (2020). Individual deviations from normative models of brain structure in a large cross‐sectional schizophrenia cohort. Molecular Psychiatry, 26, 3512–3523. 10.1038/s41380-020-00882-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marquand, A. F. , Wolfers, T. , Mennes, M. , Buitelaar, J. , & Beckmann, C. F. (2016). Beyond lumping and splitting: A review of computational approaches for stratifying psychiatric disorders. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 1(5), 433–447. 10.1016/j.bpsc.2016.04.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mataix‐Cols, D. , Rosario‐Campos, M. C. , & Leckman, J. F. (2005). A multidimensional model of obsessive‐compulsive disorder. The American Journal of Psychiatry, 162(2), 228–238. 10.1176/appi.ajp.162.2.228 [DOI] [PubMed] [Google Scholar]
- Mataix‐Cols, D. , Wooderson, S. , Lawrence, N. , Brammer, M. J. , Speckens, A. , & Phillips, M. L. (2004). Distinct neural correlates of washing, checking, and hoarding symptom dimensions in obsessive‐compulsive disorder. Archives of General Psychiatry, 61(6), 564–576. 10.1001/archpsyc.61.6.564 [DOI] [PubMed] [Google Scholar]
- McKay, D. , Abramowitz, J. S. , Calamari, J. E. , Kyrios, M. , Radomsky, A. , Sookman, D. , … Wilhelm, S. (2004). A critical evaluation of obsessive‐compulsive disorder subtypes: Symptoms versus mechanisms. Clinical Psychology Review, 24(3), 283–313. 10.1016/j.cpr.2004.04.003 [DOI] [PubMed] [Google Scholar]
- Menzies, L. , Chamberlain, S. R. , Laird, A. R. , Thelen, S. M. , Sahakian, B. J. , & Bullmore, E. T. (2008). Integrating evidence from neuroimaging and neuropsychological studies of obsessive‐compulsive disorder: The orbitofronto‐striatal model revisited. Neuroscience and Biobehavioral Reviews, 32(3), 525–549. 10.1016/j.neubiorev.2007.09.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menzies, L. , Williams, G. B. , Chamberlain, S. R. , Ooi, C. , Fineberg, N. , Suckling, J. , … Bullmore, E. T. (2008). White matter abnormalities in patients with obsessive‐compulsive disorder and their first‐degree relatives. The American Journal of Psychiatry, 165(10), 1308–1315. 10.1176/appi.ajp.2008.07101677 [DOI] [PubMed] [Google Scholar]
- Nishida, S. , Narumoto, J. , Sakai, Y. , Matsuoka, T. , Nakamae, T. , Yamada, K. , … Fukui, K. (2011). Anterior insular volume is larger in patients with obsessive‐compulsive disorder. Progress in Neuro‐Psychopharmacology & Biological Psychiatry, 35(4), 997–1001. 10.1016/j.pnpbp.2011.01.022 [DOI] [PubMed] [Google Scholar]
- Okada, K. , Nakao, T. , Sanematsu, H. , Murayama, K. , Honda, S. , Tomita, M. , … Kanba, S. (2015). Biological heterogeneity of obsessive‐compulsive disorder: A voxel‐based morphometric study based on dimensional assessment. Psychiatry and Clinical Neurosciences, 69(7), 411–421. 10.1111/pcn.12269 [DOI] [PubMed] [Google Scholar]
- Okasha, A. , Rafaat, M. , Mahallawy, N. , El Nahas, G. , El Dawla, A. S. , Sayed, M. , & El Kholi, S. (2000). Cognitive dysfunction in obsessive‐compulsive disorder. Acta Psychiatrica Scandinavica, 101(4), 281–285. [PubMed] [Google Scholar]
- Piras, F. , Piras, F. , Chiapponi, C. , Girardi, P. , Caltagirone, C. , & Spalletta, G. (2015). Widespread structural brain changes in OCD: A systematic review of voxel‐based morphometry studies. Cortex, 62, 89–108. 10.1016/j.cortex.2013.01.016 [DOI] [PubMed] [Google Scholar]
- Pujol, J. , Soriano‐Mas, C. , Alonso, P. , Cardoner, N. , Menchón, J. M. , Deus, J. , & Vallejo, J. (2004). Mapping structural brain alterations in obsessive‐compulsive disorder. Archives of General Psychiatry, 61(7), 720–730. 10.1001/archpsyc.61.7.720 [DOI] [PubMed] [Google Scholar]
- Ravindran, A. , Richter, M. , Jain, T. , Ravindran, L. , Rector, N. , & Farb, N. (2020). Functional connectivity in obsessive‐compulsive disorder and its subtypes. Psychological Medicine, 50(7), 1173–1181. 10.1017/s0033291719001090 [DOI] [PubMed] [Google Scholar]
- Rotge, J. Y. , Langbour, N. , Guehl, D. , Bioulac, B. , Jaafari, N. , Allard, M. , … Burbaud, P. (2010). Gray matter alterations in obsessive‐compulsive disorder: An anatomic likelihood estimation meta‐analysis. Neuropsychopharmacology, 35(3), 686–691. 10.1038/npp.2009.175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saxena, S. , Brody, A. L. , Schwartz, J. M. , & Baxter, L. R. (1998). Neuroimaging and frontal‐subcortical circuitry in obsessive‐compulsive disorder. The British Journal of Psychiatry, 173, 26–37. [PubMed] [Google Scholar]
- Saxena, S. , & Rauch, S. L. (2000). Functional neuroimaging and the neuroanatomy of obsessive‐compulsive disorder. The Psychiatric Clinics of North America, 23(3), 563–586. 10.1016/s0193-953x(05)70181-7 [DOI] [PubMed] [Google Scholar]
- Shen, X. , Tokoglu, F. , Papademetris, X. , & Constable, R. T. (2013). Groupwise whole‐brain parcellation from resting‐state fMRI data for network node identification. NeuroImage, 82, 403–415. 10.1016/j.neuroimage.2013.05.081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Starcevic, V. , & Brakoulias, V. (2008). Symptom subtypes of obsessive‐compulsive disorder: Are they relevant for treatment? The Australian and New Zealand Journal of Psychiatry, 42(8), 651–661. 10.1080/00048670802203442 [DOI] [PubMed] [Google Scholar]
- Subirà, M. , Alonso, P. , Segalàs, C. , Real, E. , López‐Solà, C. , Pujol, J. , … Soriano‐Mas, C. (2013). Brain structural alterations in obsessive‐compulsive disorder patients with autogenous and reactive obsessions. PLoS One, 8(9), e75273. 10.1371/journal.pone.0075273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun, X. , Liu, J. , Ma, Q. , Duan, J. , Wang, X. , Xu, Y. , … Xia, M. (2021). Disrupted intersubject variability architecture in functional connectomes in schizophrenia. Schizophrenia Bulletin, 47(3), 837–848. 10.1093/schbul/sbaa155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swedo, S. E. , Pietrini, P. , Leonard, H. L. , Schapiro, M. B. , Rettew, D. C. , Goldberger, E. L. , … Grady, C. L. (1992). Cerebral glucose metabolism in childhood‐onset obsessive‐compulsive disorder. Revisualization during pharmacotherapy. Archives of General Psychiatry, 49(9), 690–694. 10.1001/archpsyc.1992.01820090018003 [DOI] [PubMed] [Google Scholar]
- Szeszko, P. R. , Christian, C. , Macmaster, F. , Lencz, T. , Mirza, Y. , Taormina, S. P. , … Rosenberg, D. R. (2008). Gray matter structural alterations in psychotropic drug‐naive pediatric obsessive‐compulsive disorder: An optimized voxel‐based morphometry study. The American Journal of Psychiatry, 165(10), 1299–1307. 10.1176/appi.ajp.2008.08010033 [DOI] [PubMed] [Google Scholar]
- Torres, A. R. , Prince, M. J. , Bebbington, P. E. , Bhugra, D. , Brugha, T. S. , Farrell, M. , … Singleton, N. (2006). Obsessive‐compulsive disorder: Prevalence, comorbidity, impact, and help‐seeking in the British National Psychiatric Morbidity Survey of 2000. The American Journal of Psychiatry, 163(11), 1978–1985. 10.1176/ajp.2006.163.11.1978 [DOI] [PubMed] [Google Scholar]
- Varol, E. , Sotiras, A. , & Davatzikos, C. (2017). HYDRA: Revealing heterogeneity of imaging and genetic patterns through a multiple max‐margin discriminative analysis framework. NeuroImage, 145(Pt B), 346–364. 10.1016/j.neuroimage.2016.02.041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Wit, S. J. , Alonso, P. , Schweren, L. , Mataix‐Cols, D. , Lochner, C. , Menchón, J. M. , … van den Heuvel, O. A. (2014). Multicenter voxel‐based morphometry mega‐analysis of structural brain scans in obsessive‐compulsive disorder. The American Journal of Psychiatry, 171(3), 340–349. 10.1176/appi.ajp.2013.13040574 [DOI] [PubMed] [Google Scholar]
- Wolfers, T. , & Beckmann, C. F. (2020). Individual differences v. the average patient: Mapping the heterogeneity in ADHD using normative models. Psychological Medicine, 50(2), 314–323. 10.1017/s0033291719000084 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolfers, T. , Doan, N. T. , Kaufmann, T. , Alnæs, D. , Moberget, T. , Agartz, I. , … Marquand, A. F. (2018). Mapping the heterogeneous phenotype of schizophrenia and bipolar disorder using normative models. JAMA Psychiatry, 75(11), 1146–1155. 10.1001/jamapsychiatry.2018.2467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu, X. , Yu, G. , Zhang, K. , Feng, J. , Zhang, J. , Sahakian, B. J. , & Robbins, T. W. (2021). Symptom‐based profiling and multimodal neuroimaging of a large preteenage population identifies distinct obsessive‐compulsive disorder‐like subtypes with neurocognitive differences. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging. Advance online publication. 10.1016/j.bpsc.2021.06.011 [DOI] [PubMed] [Google Scholar]
- Xia, J. , Fan, J. , Liu, W. , Du, H. , Zhu, J. , Yi, J. , … Zhu, X. (2020). Functional connectivity within the salience network differentiates autogenous‐ from reactive‐type obsessive‐compulsive disorder. Progress in Neuro‐Psychopharmacology & Biological Psychiatry, 98, 109813. 10.1016/j.pnpbp.2019.109813 [DOI] [PubMed] [Google Scholar]
- Yoo, S. Y. , Roh, M. S. , Choi, J. S. , Kang, D. H. , Ha, T. H. , Lee, J. M. , … Kwon, J. S. (2008). Voxel‐based morphometry study of gray matter abnormalities in obsessive‐compulsive disorder. Journal of Korean Medical Science, 23(1), 24–30. 10.3346/jkms.2008.23.1.24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yun, J. Y. , Boedhoe, P. S. W. , Vriend, C. , Jahanshad, N. , Abe, Y. , Ameis, S. H. , … Kwon, J. S. (2020). Brain structural covariance networks in obsessive‐compulsive disorder: A graph analysis from the ENIGMA Consortium. Brain, 143(2), 684–700. 10.1093/brain/awaa001 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1 Altered GMVs in subtypes of OCD.
Data Availability Statement
Some or all data, models, or code that support the findings of this study are available from the corresponding author upon reasonable request.