

Abstract
Objective:
The Self-Medication Hypothesis (SMH) theorizes that alcohol is used to alleviate negative states. We assessed whether an acute social stressor (Trier Social Stress Test, TSST), a priming dose of alcohol, and participant sex impacted 90-minute ad libitum drinking. We expected exposure to stress to be associated with increased consumption, and this effect to be stronger following an alcohol priming dose; we also explored whether participant sex moderated these effects.
Method:
Using a 2×2 experimental design, we randomized groups of 2–3 drinkers to stress (TSST vs. no TSST) and priming beverage (alcohol vs. placebo) conditions. All participants subsequently completed the 90-min ad libitum drinking period and were instructed not to exceed more than one alcoholic beverage per hour for optimal performance to model behavioral impaired control. We examined 1) number of drinks ordered, 2) violations of the drink limit, 3) change in breath alcohol concentration (BAC), and 4) peak BAC.
Results:
Analyses showed that exposure to stress was associated with heavier ad libitum drinking. This effect was qualified by a three-way interaction; women who received a stressor and no prime dose (placebo) reached higher BACs, whereas men who received a stressor and a prime reached higher BACs.
Conclusions:
The hypothesized interaction between an alcohol priming dose and social stress was only evident among men, whereas women drank more under social stress in the absence of a priming dose. Findings suggest the importance of exploring sex differences in future studies of the SMH.
Keywords: Impaired Control over Alcohol, Social Drinking, Ad libitum, TSST, Alcohol Self-Administration, Sex Differences
Introduction
The Self-Medication Hypothesis (SMH) theorizes individuals use alcohol to alleviate negative affect particularly after stressful events (Conger, 1956; Hersh & Hussong, 2009; Livingston et al., 2021; Vogel et al., 2021). Consistent with this model, individuals who report drinking to cope with negative affective states are at greater risk for future negative alcohol-related consequences (Armeli et al., 2014; Waddell et al., 2021). Both dependent and non-dependent drinkers report drinking alcohol to cope with chronic stress (Sinha, 2007). Moreover, a review of longitudinal studies (Chassin et al., 2013) suggests causal relations between stressful life events and alcohol consumption and later development of alcohol use disorders (AUDs). In fact, stressors are widely believed to trigger uncontrolled drinking when the stress occurs prior to drinking (Sinha et al., 2016). Thus, individuals may drink in response to stress (with the goal of stress reduction) even if the context is not conducive to alcohol induced stress reduction. Yet, causal experimental studies linking stress to alcohol consumption are somewhat mixed (e.g., Cyders et al., 2016, Higgins & Marlatt, 1973; Thomas et al., 2011, McGrath et al., 2016; please see Table 1 for a summary of these experiments and their features).
Table 1.
Features of studies in which an acute stressor and/or a prime dose were used with some measure of ad libitum drinking
| Author (Year) | Sample Composition (Men/Women) | Type of Stress | Use of Full TSST | Use of Alcohol Prime | Oral vs. IV-ASA | Length of Ad-Lib | Max Alcohol Allowed | Solitary vs. Group Drinking | Drinking Environment | Analysis | Support for SMH |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patock-Peckham et al., (2021) | Social Drinkers (105/105) | Full TSST Speech + Math | Yes | .065g/kg | Oral | 90-min | .12 BAC | 2–3 person groups | Simulated Bar | MLM | Yes |
| Thomas et al. (2011) | Alcohol Dependent (39/40) | Full TSST Speech + Math | Yes | .03g/dl | Oral | 15-min | Two-drink taste test | Solitary | Lab Setting | ANOVA Linear Mixed Models | Yes |
| McGrath et al. (2016) | Heavy Drinkers (48/52) | Modified TSST 5-min Speech | No | --- | Oral | 30-min | 300ml – 3 Beer taste test | Solitary | Simulated Bar | ANOVA | Yes |
| Clay & Parker (2018) | Social Drinkers (22/17) | Full TSST Speech + Math | Yes | --- | Oral | Not Reported | BAR press earn up to 12 5 ml shots of vodka + mixer | Solitary | Lab Setting | ANOVA | Yes |
| Magrys & Olmstead (2015) | Social Drinkers – Once per month (35/40) | Full TSST Speech + Math | Yes | Alcohol expectancy, control) .03 g/kg men; .02 g/kg women | Oral | 30-min | Allowed 0.1 g/kg beverages no limit stated | One participant + 1 or more confederates | Living Room Setting | ANOVA | Yes |
| De Wit et al. (2003) | Heavy Social Drinkers 2–4 drinks per week (24/13) | Modified TSST Math in front of Audience 10-min | No | Alcohol vs. Placebo prime 0.3 g.kg men; 0.2 g/kg women | Oral | 30-min | Up to 6 0.1 g/kg ethanol drinking | 2–4 person groups | Living Room Setting | ANOVA | Yes |
| Miller et al. (1974) | AUD vs. Social Drinkers (16/00) | Disparaging Failure Feedback Regarding a 15-min Social Interaction | No (likely stronger than full TSST) | --- | Oral | 10-min | 5cm3 squirt of 30% Bourbon earned with lever press | Solitary | Lab Setting | ANOVA | Yes |
| Higgins & Marlatt (1973) | AUD vs. Social Drinkers (40/00) | Anticipate Painful vs. Mild Shock | No | .00 g/kg | Oral | 15-min | Two drink (BAC < .06) | Solitary | Lab Setting | ANOVA | No |
| Hull & Young (1983) | High vs. Low Self-Conscious Social Drinkers (120/00) | Failure Feedback Intellectual Task | No | --- | Oral | 15-min | 3 1/5 oz of wine taste test | Solitary | Lab Setting | ANOVA | Yes |
| Pratt & Davidson (2009) | Non-Treatment Seeking Alcohol Dependent (52/22) | Paced Auditory Serial Addition Test (PASAT) | No | --- | Oral | Beer available during cue-availability procedure over 40 trials | Not Reported | Solitary | Lab Setting | Correlations & T-tests | Yes* |
| Cyders et al., (2016) | Social Drinkers (15/19) | Negative Life Events Narrative + Musical Mood Induction | No | 15 mg/dl BAC after 10-min | IV-ASA | 2-hours | 150 mg/dl | Solitary | Lab Setting | ANOVA | No for women; Yes for men |
Consistent with the SMH, experiments have shown social drinkers voluntarily consume more alcohol immediately after exposure to a psychosocial stressor (de Wit et al., 2003; Magrys & Olmstead, 2015; McGrath et al., 2016). There is also evidence that subjective craving and subjective value of alcohol increase after a stress challenge in both dependent and non-dependent drinkers (Amlung & McKillop, 2014; Ramchandani et al., 2018), and laboratory studies have shown that manipulated stressors can trigger both craving and relapse (Sinha et al., 2009).
McGrath et al. (2016) examined heavy drinkers (48 men/52 women) using a modified Trier Social Stress Test (TSST; i.e. 5-minute speech only without the math component given in the full TSST; Kirschbaum et al., 1993) versus an anagram task as a control group prior to a 30-minute solitary ad libitum drinking period in a simulated bar environment. They used a 300 ml or three-beer max taste test. Stress was associated with a small but significant increase in alcohol drinking during the three-beer taste test. Sex differences were not assessed despite relatively equal numbers of men and women. Other studies have shown that males with AUDs are more likely to work (i.e. press a lever) for shots of bourbon after discouraging feedback concerning a 15-minute social confrontation situation compared to social drinkers (Miller et al., 1974; N = 16 men) and self-conscious social drinking male participants are more likely to drink more after failure feedback (Hull & Young, 1983; N= 120 men). Women were never included in these classic studies.
At the same time, some evidence from other experiments is inconsistent with the SMH. Using an ad libitum drinking paradigm, Higgins & Marlatt (1973) found that alcohol dependent men (N= 40) drank more alcohol than non-dependent men, but those who anticipated a painful shock did not differ in terms of consumption from those who anticipated a mild stimulation (Higgins & Marlatt, 1973). It is important to note that participants with a breath/blood alcohol content (BAC) of less than .06 at the start of the experiment were allowed to participate such that BACs differed across participants prior to ad libitum drinking. In addition, Pratt and Davidson (2009) used the Paced Auditory Serial Addition Test (PASAT; similar to the modified TSST with math only) as their acute stressor with beer available for 40 cue available trials. In a sample of non-treatment seeking alcohol dependent participants (52 men/ 22 women), they found that a stressor impacted cortisol levels but did not increase the urge to drink. Only those with blunted cortisol responses drank more during ad libitum drinking.
Collectively, these experiments suggest stressors involving a social evaluative component (public speaking; discouraging feedback and criticism) increase ad libitum drinking. In contrast, completing a difficult math task was effective only for those individuals with blunted cortisol responses. This may be due to the lack of the social evaluative threat component to the PASAT. Further, anticipation of painful shock did not increase ad libitum drinking during a 15-minute taste test among men (Higgins & Marlatt, 1973). Again, this stressor did not include a social evaluative component, which may be important for influencing increased alcohol consumption.
Some evidence supports the effects of social and self-evaluative stressors on ad libitum drinking. Nevertheless, the effects of stress may be stronger in the context of alcohol-related impairment. Both acute stress and alcohol consumption are associated with impaired inhibitory control, which may lead to loss of control over alcohol use (Clay & Parker, 2018; Rose & Duka, 2006). Thus, the combination of stress and alcohol may leave individuals highly dysregulated, contributing to heavy-episodic within-session drinking. Understanding continued drinking in the context of stress is critical as theoretical models of disinhibition presume that failures of inhibitory control (i.e., the ability to withhold or terminate a response such as reaching for that next drink) are linked to the development of AUDs (Baines et al., 2019; Fillmore, 2003).
Duckworth et al. (2013) suggests individuals who experience less stress exhibit greater self-control allowing them to inhibit inappropriate responses. There is also evidence that acute stress negatively impacts inhibitory control. For example, Clay and Parker’s (2018) lab experiment with social drinkers (22 men/17 women) linked physiological stress occurring after a social stressor (full TSST) to impairment of general inhibitory control using the Iowa Gambling Task. General inhibitory control and risky decision making on the Iowa Gambling task were associated with increased alcohol craving and the amount of work participants were willing to do to receive additional alcohol. Further, a robust literature supports effects of moderate doses of alcohol on inhibitory control. For example, de Wit and Chuptuape (1993) showed that social drinkers consumed more ethanol after receiving a moderate prime dose of alcohol. Similarly, Rose and Duka (2006) found that a prime dose of alcohol (0.5 g/kg) increased desire/craving for alcohol, and more disinhibited individuals have been shown to consume more beer during taste tests (Jones et al., 2011). More recently, Baines et al. (2019) found that a 0.6 g/kg prime dose of alcohol increased motivation to consume alcohol during ad libitum drinking compared to both placebo and controls.
Despite evidence to support effects of both acute stress and acute alcohol consumption on inhibitory control, only a few studies have examined the impact of stress following a priming dose of alcohol. For instance, Thomas et al.’s (2011) experiment examined effects of randomized acute stress on ad libitum drinking among participants who all received an alcohol prime dose .03g/dl; prime dose was not randomly manipulated. This study used the full TSST (public speaking plus math) in a sample of dependent drinkers (39 men/40 women) who were not seeking treatment. After a .03g/dl prime dose of alcohol, individuals exposed to the full TSST were twice as likely as no TSST controls to drink the maximum amount available (two beers) during a 15-minute solitary mock taste test. This investigation also examined potential interactions by participant sex; there was some graphical evidence that drinking increased more for men than women following a prime dose and a stressor, but not significantly so.
Similarly, Cyders et al. (2016) examined the impact of a negative mood induction [Negative Life Events Narrative (Abele, 1990) and Musical Mood Induction Procedure (MMIP; (Västfjäll, 2001)] on ad libitum drinking following a 15 mg/dl prime dose administered to all participants. This study used intravenous alcohol self-administration (IV-ASA) over a two-hour period (15 men/19 women). Women exposed to stress reached lower BACs than controls. In contrast, men showed a pattern of increased administration of alcohol in negative as compared to neutral mood states. Thus, both Thomas et al. (2011) and Cyders et al. (2016) found that men, relative to women, were more likely to continue drinking following a prime dose and a stressor. Yet, because all participants received the same prime dose of alcohol, it was impossible to examine potential interactions between prime doses versus placebo beverages by stress versus no stress in either study.
De Wit et al. (2003) more directly examined potential interactions between stress and an alcohol priming dose using a modified version of the TSST involving mental arithmetic in front of an audience for 10-minutes. The sample (24 men/ 13 women) included heavy social drinkers. Approximately half the participants received an alcohol prime dose of 0.3g/kg for men or 0.2g/kg for women or a placebo beverage after the stress condition. Participants were then tested during a 30-minute ad libitum drinking period with 2–4 people in a living room environment; they were allowed up to 6 ethanol drinks (0.1g/kg) during ad libitum drinking. De Wit et al. (2003) found a main effect of stress on voluntary ethanol consumption but no interaction between the modified TSST manipulation and the prime dose. Sex differences were not examined likely due to the small sample of women.
Magrys and Olmstead (2015) used a similar approach to de Wit et al. (2003), but they used the full TSST (24 TSST “stress” participants versus 51 no TSST “control” participants; 35 men/40 women) and included a no alcohol group in addition to alcohol and placebo groups. Individuals in the alcohol group were given a prime dose of alcohol (.03g/kg for men and .02g/kg for women) and all participants were allowed to order additional beverages (.01g/kg) during the ad libitum drinking period. Magrys and Olmstead (2015) found that stress was associated with greater ad libitum drinking in the alcohol prime condition, but not in the no alcohol or placebo conditions. Unfortunately, this important study did not examine potential interactions between stress and prime dose and participant sex.
Investigations of stress effects on ad libitum drinking have overall largely supported the SMH. Yet, Higgins & Marlatt (1973), Pratt and Davidson (2009) and Cyders et al. (2016) did not find main effects of stress leaving a mixed extant literature. Presumably this is due to the nature of the stressors (e.g. shock, PSAT, and negative mood induction) which were quite different from those investigations supporting the SMH which typically used social evaluative or self-evaluative feedback. Moreover, there is mixed evidence regarding potential interactions between stress and prime dose. Further, there is evidence suggesting that men may be more responsive to the combination of social stress and a priming dose than are women. Prior studies examining a prime dose and stressor have used low doses that may not impact inhibitory control, and few experiments have explicitly examined participant sex as a moderating variable.
Examining potential sex differences is critically important because women are showing dramatic rises in dysregulated binge and heavy drinking (Hingson et al., 2017; Guinle & Sinha, 2020). According to White (2020), gaps in alcohol use between cisgender women and men are narrowing. This is troubling because women progress more quickly to AUDs than men (Cheng & Anthony, 2018) and AUDs have increased by 84% in women (Grant et al., 2017). This telescoping effect in women may be tied to internalizing problems such as depression and anxiety that are more prevalent among women (Strine et al., 2008), and women are more likely to consume alcohol in response to negative emotions than are men (McCaul et al., 2019). Personality based models of AUD vulnerability also identify internalizing problems (e.g., anxiety sensitivity and depression proneness) as potential pathways to alcohol problems (Conrod et al., 2006). Furthermore, stress and negative affect appear to be associated with all phases of AUDs and disproportionately affect women with respect to drinking initiation, maintenance, and relapse (Koob & White, 2017; Peltier et al., 2019). Presumably, women may be more sensitive to social evaluative threats than men (Tops et al., 2019); this is perhaps due to their socialization towards sociotrophy (i.e., the tendency to want to maintain positive social relationships; Beck, 1983; Yang & Girgus, 2018).
It is important to understand the causal relationships between an alcohol prime dose and participant sex as potential moderators of stress effects on ad libitum drinking due to the potential for dysregulation. Thus, this current study sought to examine the excessive drinking behavior that is more closely linked to risk for alcohol-related consequences. In the absence of an incentive to control consumption (which often occurs in real-world drinking settings), participants in lab-based studies have little reason to control their drinking. Further, limits are imposed on their drinking with maximum BACs typically not exceeding a .04 - .08 BAC, and participants are held until their BACs reach a safe level. Thus, the real-world consequences that may occur from over-consumption are not well captured. This is an important limitation as drinking despite the potential for consequences (referred to as Impaired Control (IC); Heather et al., 1993) is one of the earliest signs of AUD (Leeman et al., 2009). Most prior work has been limited to trait (i.e., “retrospective” survey work; see reviews Leeman et al., 2012; 2014) rather than assessing state “in the moment” behavioral impaired control (i.e., experimental work; Leeman et al., 2013). Importantly, individuals with higher trait IC achieve higher BACs during IV-ASA protocols (Vaughn et al., 2019) suggesting trait IC may translate to state IC. Given that trait IC is correlated with stress (Leeman et al., 2007), it is important to examine effects of acute stress on state IC, and to determine if these effects are exacerbated in the context of a priming dose of alcohol that is sufficient to produce impairment of behavioral inhibition. As noted previously, it is also critical to examine potential sex differences based on evidence of potentially unique effects of stress on drinking outcomes among women.
We are aware of no prior studies examining effects of acute stress on IC in a naturalistic bar setting. Nevertheless, Leeman et al. (2013) developed a paradigm for assessing behavioral (state) IC in an experiment, providing us a useful framework for addressing this research question. Leeman et al. (2013) used an ecologically valid context (a naturalistic bar setting), studied heavy drinkers (27 men/ 12 women) in groups of 1–3 people, and allowed participants to consume alcohol to a .10 g% BAC during a 3-hour ad libitum drinking period. Leeman’s behavioral impaired control paradigm consists of instructing participants that drinking too much may negatively impact performance on subsequent cognitive tasks linked to their subject payments in a probabilistic way, yet still allowing them to continue drinking. Participants given the instructions to limit their drinking consumed less than those who did not receive this instruction (Leeman et al., 2013). Our current study utilized a similar approach by instructing, but not requiring, participants to limit their drinking.
We examined the conditions under which stress contributes to impaired control (IC) by considering participant sex, and a priming dose of alcohol (relative to placebo) as potential moderators. Based on the robustness of inhibitory control effects at .065 BAC among healthy participants (Marczinski & Fillmore, 2003) we opted for a .065 target prime dose. We also sought to increase ecological validity by conducting the study in a simulated bar (with all drinking occurring on Friday and Saturday afternoons/evenings), and we used a social drinking context with naïve rather than scripted social interactions during ad libitum drinking. This choice is consistent with the Social Attribution Perspective (Fairburn & Sayette, 2014) which presumes that alcohol will enhance mood in anticipation of uncertain social interactions with unscripted naïve participants (Bradford et al., 2017). We used the Leeman et al. (2013) behavioral impaired control paradigm which provides incentives to limit consumption, and participants could drink to a peak BAC of .12 g% to allow for heavy episodic drinking. For participants randomly assigned to the prime dose condition (.065 target BAC) prior to ad libitum, most could drink 3 standard drinks on average, while participants randomly assigned to the placebo first could drink up to six standard drinks. We also utilized a larger sample than most experiments in the existing literature so we could examine participant sex as a potential moderator.
Based upon the SMH, we hypothesized a main effect of the full TSST, such that individuals in the social stress condition would order more alcoholic drinks, be more likely to violate IC instructions, demonstrate greater changes in BAC during ad libitum drinking, and reach higher overall Peak BACs, than those in the no TSST condition. However, we hypothesized that the main effect of TSST would be modified by an alcohol prime dose such that the effect of the social stress (TSST) would be more pronounced among those given the .065 g/kg target prime dose of alcohol relative to placebo. Twice as many women with AUD have comorbid depression than men (Caetano et al., 2019), and there is some evidence suggesting unique mechanism of stress effects for women (Beck, 1983; Tops et al., 2019; Yang & Girgus, 2018). Presumably, women and men may not respond similarly to stress and priming conditions so we examined participant sex as a potential moderator.
Methods
Participants.
Two-hundred twenty-one participants were recruited through print advertisements from university campuses and the surrounding community. To be eligible, participants had to be between 21 and 35 years of age (M = 23.05; SD = 2.87) and report drinking at least 3 alcoholic beverages over a 2-hour period at least once in the last month to ensure the prime dose would not be aversive. Exclusion criteria included previous medical history contraindicating the use of alcohol (e.g., psychotropic or anti-depressant drugs). Women were also screened with a home pregnancy kit the day of their lab appointment. Further, all participants were screened with a full AUDADIS (Grant et al., 2000) battery two weeks prior to their appointment to screen out for alcohol dependence and other psychiatric disorders. We excluded 10 participants because they were more than 1.5 standard deviations above or below the target BAC within the prime condition (> .085 or < .046). We also excluded participants in solitary drinking situations (i.e., participants run individually due to no shows) and those who confessed they did not intend to drink at all the evening of the protocol. Our final sample consisted of 210 individuals (105 men, 105 women). With respect to race/ethnicity, our sample was 25% Hispanic/Latinx, and primarily White (72%). The remainder of the sample was 4% American Indian, 11% Asian, 1% Pacific Islander, 8% African American, and 4% other.
Consistent with Open Science, we have reported all conditions and data exclusions. We only reported on measures used in this specific study as there were a number of measures in the baseline survey that were not relevant to this research question. Power analyses for multi-level models are still in their early stages of development and there is not strong agreement about appropriate effect sizes to include in these analyses (Lorah, 2018; Peugh, 2010). However, the sample size for the current study was based on a priori power calculations for a MANCOVA with four groups (crossing TSST vs. no TSST and alcohol vs. placebo). Anticipated effect sizes (Cohen’s d) based on prior studies of stress and priming effects ranged from .44 to 1.6 so we estimated the number of participants per group necessary to achieve .80 power to detect a moderate effect (Cohen’s d = .50). This power analysis indicated that a sample of 128 participants was necessary to detect the proposed two-way interaction. Our study includes a larger sample of women than prior studies of stress effects on drinking behavior, albeit we were underpowered to detect small or moderate effects for three-way interactions (Hox et al., 2017).
Measurements.
We utilized four distinct outcome variables: 1) a count variable for the number of standard drinks ordered during the 90-minute ad libitum drinking period, 2) a dichotomous variable (yes/no) for whether participants followed instructions not to exceed one drink per hour to achieve an optimal cognitive performance (Behavioral Impaired Control Instruction Violations), 3) a continuous measure of change in BAC during ad libitum drinking (Peak BAC minus BAC at the start of ad libitum period) and 4) Peak BAC during the 90 minute ad libitum period. We also controlled for the following covariates in our models: 1) Usual Drinking Quantity using a single item (Wood et al., 1992), which asked, “What is your usual quantity of alcoholic beverages consumed at one drinking occasion?” 2) Center for Epidemiologic Studies Depression Scale (CES-D), which addresses past week depressive symptoms with 20 items (Radloff, 1977). Sample items included, “I felt lonely” and “I had crying spells”. The α reliability was 0.85. 3). Anxiety Sensitivity Index (ASI; Reiss et al., 1986), which is a 16-item scale that measures an individual’s concerns about negative consequences associated with anxiety-related symptoms (e.g., “It scares me when my heart beats rapidly” and “It is important to me to not appear nervous”). The α reliability was .87 for this sample. We also used the following method(s) and measures(s) as manipulation checks: 1) heart rate using wrist watches, and 2) the state scale of the State-Trait Anxiety Inventory (STAI; Spielberger et al., 1983), which is a 20-item measure of anxiety in the moment; the α reliability was 0.93.
Trier Social Stress Test (TSST).
The Trier Social Stress Test (Kirschbaum et al., 1993), is a social evaluative threat, shown to reliably induce higher distress than control manipulations (Kwako et al., 2015). The full TSST was used as our social stressor because meta-analyses have shown the full TSST robustly induces a physiological stress response (Goodman et al., 2017; Helminen et al., 2019). Both the speech and math portions of the TSST were given in front of 3 experimenters trained to express only non-reinforcing flat affect toward the participant to make it more socially evaluative. All TSST manipulations and no TSST control conditions were administered simultaneously in separate rooms away from other participants. The TSST consisted of two timed and video-taped sessions. The first part required participants to take 5- minutes by themselves to prepare for their speeches and then give a 5-minute speech about their likes and dislikes regarding their own personality, appearance, and life in front of an audience.
“Please recall that your speech is on “WHAT YOU LIKE AND DISLIKE ABOUT YOUR APPEARANCE, PERSONALITY, AND LIFE’. Your speech will be videotaped and reviewed by a team of evaluators who have been carefully trained to be evaluating you for positive and negative statements, openness, defensiveness and several other psychological factors. We will not be able to talk or answer any of your questions during your speech. You may begin.”
The second part included an arithmetic task during which the participant had to verbally count backwards from 1,022 in increments of 13 for 5 minutes. Any error resulted in the participant being asked to start over from 1,022. Participants were videotaped during both the speech and math tasks.
No TSST/Control Condition.
The no TSST condition consisted of participants rating the videotaped speech of one of our research assistant confederates posing as a previous subject. All participants in the No TSST condition received the following instructions.
“In approximately 5 minutes from now you will be required to evaluate a 5-minute speech from a previous participant. The topic of the speech was ‘WHAT YOU LIKE AND DISLIKE ABOUT YOUR APPEARANCE, PERSONALITY, AND LIFE’. Please spend the next five minutes writing about what characteristics you feel are important for people who are giving presentations to be evaluated on. We are interested in your input.”
Next, we announced the video preparation (traits/characteristics people should be evaluated on):
“You may use a sheet of paper and pen to write down your thoughts in the next five minutes. Please leave your watch on, we will take a reading after the 5 minutes elapses. We have prepared our own speech evaluation form that we are hoping to improve with your thoughts and the thoughts of other participants. However, at this time, we would like you to view this video of another participant giving a speech on ‘WHAT HE LIKES AND DISLIKES ABOUT HIS APPEARANCE, PERSONALITY AND LIFE.’ Do you have any questions?” [Answer Questions] “Please just carefully watch this video for the next 5 minutes.”
We then set a 5-minute timer and read the following instructions to the participant:
“Please evaluate this speech for positive and negative statements and check it for openness, defensiveness, and several other psychological factors. You will have five minutes to fill out this form. If you finish early, there is an additional comments section where you can write about how well you thought this participant performed based on the evaluation criteria you wrote about earlier.”
Procedures.
All participants arrived at the lab at approximately noon on Friday or Saturday afternoons in groups of 2 or 3. Each group was randomly assigned to the TSST condition or no TSST condition and a prime dose (.065 target BAC) versus a placebo (.000 target BAC) control condition. Alcoholic beverages were a cocktail of cranberry juice, sprite, and vodka (calculated by gender/height/weight; see Curtin & Fairchild, 2003; BAC calculator). Control condition beverages were a cocktail of cranberry juice, sprite, and flattened tonic water with the glasses rimmed with a negligible amount of alcohol for taste and smell cues. All bartenders were blind to the prime dose condition. The IRB approved the protocol with a Peak BAC of .12. At the start of the protocol, participants completed baseline measures on a battery of computerized cognitive tasks which were used as part of our cover story. Next, depending on stress condition, participants completed either the TSST or control task followed by completing a subset of the computerized cognitive tasks again.
After the stress condition manipulation, the alcohol administration period began. We served participants either alcohol or placebo beverages at a rate of one drink every six-minutes with a one-minute break between each drink, followed by an eight-minute absorption period (see Figure 1). Post-alcohol prime or placebo administration period, participants completed a survey and another subset of cognitive tasks. Next, participants began the 90-minute ad libitum drinking period and were instructed to limit consumption with the following language:
Figure 1.
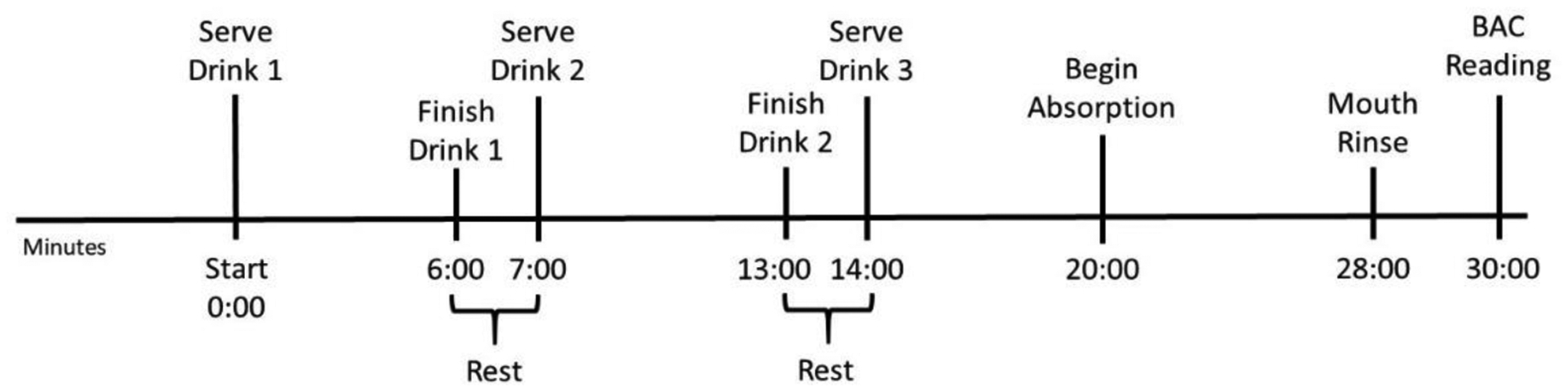
Alcohol Prime Manipulation (.00 vs .065) target dose administration timeline.
Violation of Impaired Control Instructions.
“Early this evening you completed several tasks. Later, you will repeat some of these tasks. It is very important that your performance is consistent both times you complete these tasks. If your performance on the second task falls below 80% of your performance on the baseline measure, you will be required to draw from a hat with one of three statements: 1) no loss 2) a loss of $10.00, 3) or a loss of $20.00. Thus, if you have to draw from the hat, you will have a 33% probability of losing your full $20.00 bonus payment. Remember, you have consumed alcohol this evening and alcohol does affect your performance on these tasks. It is recommended for optimal performance that you do not consume more than 1 standard drink per hour.”
The experimenter then recorded each time the participant ordered another drink (and each time they wanted another drink but were not served due to hitting the BAC limit of .12). Finally, after the ad libitum drinking period, participants completed the computerized cognitive tasks again and completed a final survey.
Ad libitum Drinking Period.
The ad libitum drinking period comprised a 90-minute period during which participants could order alcoholic or non-alcohol drinks and self-administer freely until either a BAC of .12 was reached, or they voluntarily decided to stop. Participants were allowed to freely interact during the ad libitum drinking period. Once a BAC of .12 was reached, participants were barred from ordering any additional alcoholic beverages for the duration of their time in the session. To avoid interrupting the free drinking period, we used a BAC calculator (Curtin & Fairchild, 2003) to determine if a participant needed to be cut off from consuming more alcohol. BACs were only taken during the ad libitum period if a participant was likely to exceed a BAC of .12; otherwise, drinking was uninterrupted. A ride home was provided after the protocol was completed and participant BACs reached .02 or less. Participants were paid $12 per hour plus a $20 bonus for their performance on cognitive tasks performed after the ad libitum drinking period. Participants were provided with food, Netflix, and board games while waiting for BACs to return to .02 or less.
Data Analytic Strategy.
Each group of participants was randomly assigned to the same experimental condition (stress or prime). We utilized multilevel models (MLM, hierarchical model) to account for the fact that individuals were nested with groups of 2–3 (Corbin et al., 2015). Analyses were performed in SAS 9.4 (SAS Institute, Cary, NC) using the MIXED procedure for continuous outcomes (e.g., change in BAC during ad libitum drinking and peak BAC) and the GLIMMIX procedure with adaptive Gaussian quadrature for count and binary outcomes (e.g., drink orders and impaired control instruction violations). We specified a logit link function (distribution) concerning the behavioral impaired control instruction violations binary outcome variable. We used typical drinking quantity per drinking event, depression, and anxiety sensitivity as covariates in all analyses. In addition, BAC at the start of the ad libitum period was used as a covariate for Peak BAC. Intra-class correlation coefficients (ICCs) were calculated using a random intercepts model for each outcome variable. Generally, values above .05 or .10 are considered large enough to justify the use of MLM (Hox, 1998). Simple effects to decompose the interactions were calculated for the differences of least square means appropriate for models with covariates.
Results
Our calculations yielded ICCs of .36 for number of drinks ordered, .36 for violations of impaired control consequences, .42 for the BAC change score (Peak BAC minus BAC at the start of ad libitum drinking), and .47 for Peak BAC. First, we examined manipulation checks to determine if the TSST manipulation was effective in increasing stress/anxiety. Heart Rate (HR) - Figure 2 depicts mean HR as a function of the stress manipulation. Individuals in the TSST condition showed increased HR, relative to controls, beginning after the speech preparation and continuing through speech completion (e.g., HR after speech announcement F(1, 206) = 14.34, p <.001; HR after video-taped speech F(1, 206) = 37.65, p <.001). Effects of TSST condition did not interact with participant sex in the prediction of HR at any time point (all p values > = .33).
Figure 2.
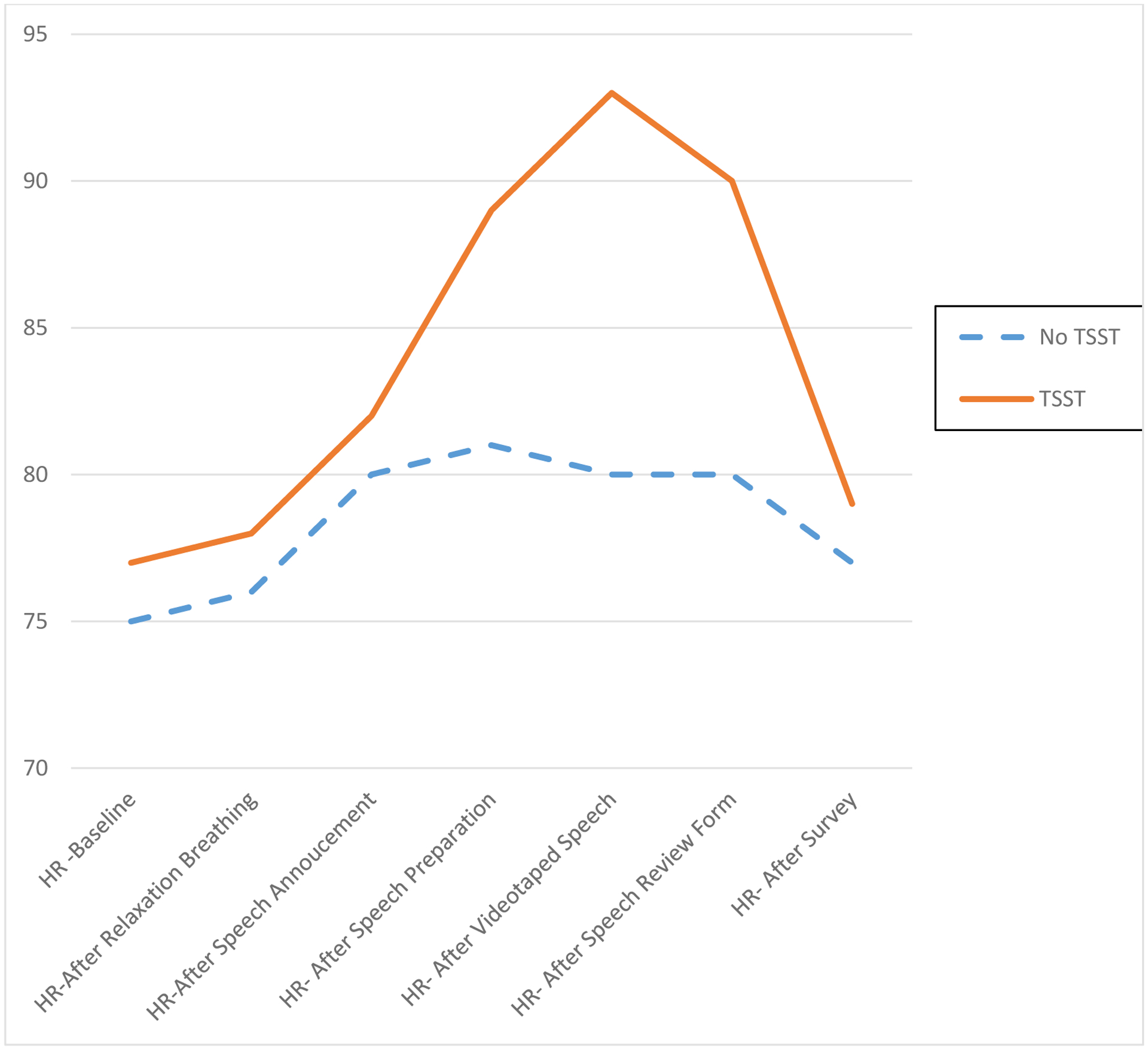
Mean Heart Rate HR as a Function of Stress Manipulation.
State Anxiety (STAI) – State anxiety was measured after the acute stressor was administered. Participants in the TSST condition had significantly higher mean State Anxiety following the TSST (M = 35.34, SD = 20.57) compared to those in the no TSST condition (M = 27.32, SD = 6.97), F(1, 209) = 42.36, p < .001. Women had significantly higher mean State Anxiety overall regardless of condition, (M = 33.59 for women; M = 28.83 for men), F(1, 198) = 26.34, p < .001. Main effects of TSST condition and participant sex were qualified by a significant TSST condition by sex interaction such that women in the TSST condition (M = 39.78) showed higher observed means post stressor than all the other conditions (M = 27.39 for women in the no TSST condition; M = 27.29 for men in the no TSST condition; M = 30.31 for men in the TSST condition), F (1, 198) = 15.62, p < .001.
Primary analyses examined effects of stress (TSST, no TSST), beverage (alcohol .065 prime dose, placebo .000 dose), and sex (women, men) and their interactions on each outcome. Table 2 contains the Type III Fixed Effects for the MLM models for each dependent variable. For number of drinks ordered during the 90-minute ad libitum drinking period, we counted a drink as ordered even if we did not serve it for safety reasons (i.e. the participant would have exceeded a .12 BAC). Results of the MLM showed a main effect of TSST condition (N = 108; TSST M = 2.41; SD = 1.23; range (0, 5), N = 102; no TSST M= 2.08; SD = 1.23; range (0, 5), such that those in the TSST condition ordered significantly more drinks than individuals in the no TSST condition, F(1, 191) = 5.65, p < .02. We also found a main effect of sex (N= 105; M= 2.65; SD = 1.36; range (0, 5) for men, N =105; M = 1.84; SD = 1.13; range (0, 4) for women), such that men ordered significantly more drinks than women, F (1, 191) = 13.52, p < .0001. For drinks ordered, the proposed social stress condition by prime condition interaction was not significant, F (1, 191) = 1.22, p = .27, nor were any interactions with participant sex.
Table 2.
Type III Fixed Effects
| Number of Drinks Ordered During 90-min Ad libitum Drinking | Impaired Control Consequence Violations During Ad libitum Drinking | Change Score (Peak BAC Minus BAC at Start of Ad libitum Drinking) | Peak BAC | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| df | F | p-value | Df | F | p-value | df | F | p-value | df | F | p-value | |||||
| Trier (TSST) | (1,191) | 5.65 | .0185* | (1,32) | 4.49 | .0420* | (1,148) | 4.69 | .0319* | (1,147) | 5.16 | .0246* | ||||
| Alcohol | (1,191) | 1.54 | .2156 | (1,32) | 0.11 | .7477 | (1,149) | 31.61 | .0001**** | (1,190) | 0.95 | .3307 | ||||
| Participant Sex | (1,191) | 13.52 | .0003*** | (1,32) | 3.89 | .0572 | (1,149) | 4.41 | .0374* | (1,150) | 2.98 | .0864 | ||||
| TSST by Sex | (1,191) | 1.27 | .2619 | (1,32) | 0.45 | .5050 | (1,146) | 0.68 | .4097 | (1,145) | 1.20 | .2752 | ||||
| Alcohol by Sex | (1,191) | 1.06 | .3056 | (1,32) | 0.23 | .6376 | (1,147) | 0.73 | .3930 | (1,148) | 0.20 | .6572 | ||||
| TSST by Alcohol | (1,191) | 1.22 | .2702 | (1,32) | 1.00 | .3240 | (1,144) | 0.02 | .8898 | (1,143) | 0.05 | .8217 | ||||
| TSST by Alcohol by Sex | (1,191) | 0.80 | .3715 | (1,32) | 2.24 | .1439 | (1,145) | 5.40 | .0215* | (1,144) | 4.60 | .0337* | ||||
| Covariates | ||||||||||||||||
| Usual Drinking Quantity | (1,191) | 6.42 | .0121* | (1,32) | 6.26 | .0176* | (1,189) | 3.22 | .0742 | (1,189) | 3.64 | .0580 | ||||
| CESD – Depression | (1,191) | 0.18 | .6729 | (1,32) | 0.04 | .8394 | (1,174) | 0.05 | .8175 | (1,174) | 0.00 | .9727 | ||||
| Anxiety Sensitivity | (1,191) | 0.74 | .3904 | (1,32) | 1.23 | .2749 | (1,190) | 0.78 | .3783 | (1,188) | 1.06 | .3057 | ||||
| BAC at start of ad lib | --- | --- | --- | --- | --- | --- | --- | --- | --- | (1,188) | 2.54 | .1128 | ||||
Note -
p<.05,
p<.01,
p<.001,
p<.0001;
Blood Alcohol Concentration (BAC) at the start of ad libitum was only used as a covariate for the Peak BAC variable.
For impaired control consequences violations (yes/no), we found that participants in the TSST condition were more likely to violate the behavioral impaired control instructions (to limit to no more than one drink per hour during the ad libitum period) with 65.74% of those who received the TSST violating the drinking limit compared to 54.90% in the no TSST control condition, F(1, 32) =4.49, p = .04. Men (68.57%) were more likely to violate IC instructions than women (52.38%), albeit this effect did not reach statistical significance, F (1, 38) = 3.80, p < .06. The proposed stress condition by prime condition interaction was not significant, F(1, 32) = 1.00, p =.32, nor were any interactions involving participant sex.
For BAC change score (Peak BAC minus BAC at the start of ad libitum drinking), our primary outcome was change in BAC rather than absolute BAC because those who received the prime dose started the ad libitum period with an average BAC of .065, SD = .012 (min .037, max .087). Thus, for these individuals, peak BAC was a function of both the prime dose and ad libitum drinking. There was a significant main effect of social stress with greater increases in BAC change score in the TSST condition relative to the no TSST condition [(N =108; M = .045; SE =.003, for stress/TSST) versus (N = 102; M = .035; SE = .003; for no TSST)], F( 1, 148) = 4.69, p = .03. As expected, there was a very large main effect of alcohol prime with participants who received a priming dose (and therefore were able to order fewer drinks before reaching the maximum) increasing their BAC less than those who did not receive the prime dose [(N = 103; M = .052; SE = .003; for the no alcohol condition) versus (N = 107; M = .027; SE= .003; for the alcohol condition)], F(1, 149) = 31.61, p = .0001. In addition, there was a main effect of participant sex with greater increases in BAC for men than women [(N=105; M =.044; SE = .003; for men) versus (N = 105; M = .035; SE = .003; for women)], F (1, 149) = 4.41, p < .04.
These main effects were qualified by a three-way interaction between stress condition, priming condition, and sex, F (1, 145) = 5.40, p = .02. For women in the no alcohol prime condition, those exposed to the social stress had greater increases in BAC (Change in BAC = .060; SE =.006) than those in the no TSST condition (Change in BAC = .038; SE =.006), t(1, 146) = 2.53, p = .01. For men in the prime condition those exposed to TSST condition had greater increases in BACs (Change in BAC = .042; SE = .006) than those in the no TSST condition (Change in BAC = .025; SE = .006), albeit not significantly so, t(1, 140) =1.93, p < .06. As depicted in Figure 3, among men who received a priming dose, those exposed to social stress experienced non-significantly greater increases in BAC change score relative to those who did not experience social stress, whereas among women who received the placebo dose the social stress was associated with greater increases in BAC change score.
Figure 3.
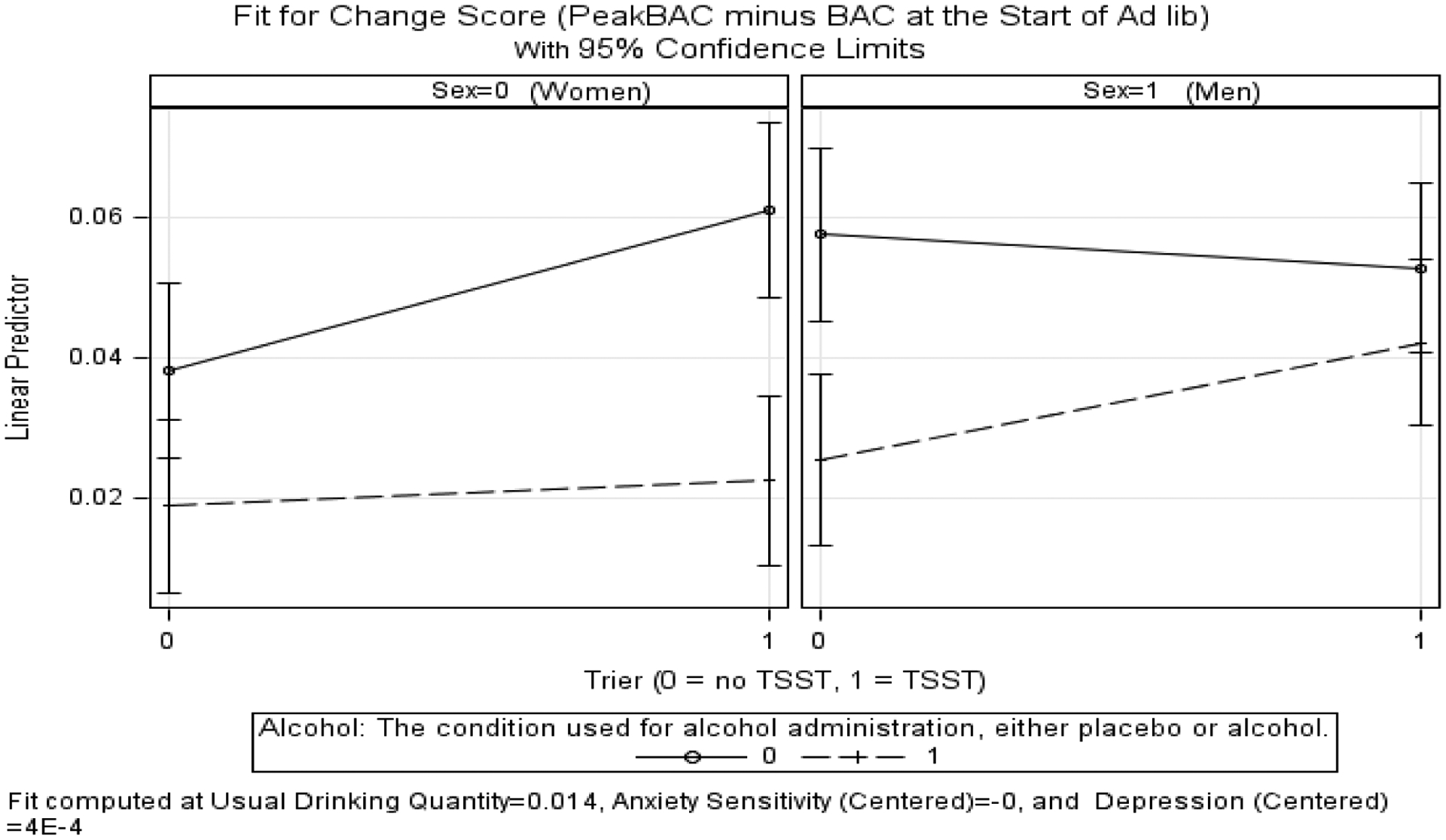
Change of BAC as a function of TSST (Stress), Alcohol Prime, and Sex.
Peak BAC during ad libitum drinking.
We also depicted the three-way interaction for absolute BACs in Figure 4 to show the extent of heavy episodic drinking despite impaired control instructions to limit alcohol use. There was a significant main effect of social stress with greater increases in Peak BAC in the TSST condition relative to the no TSST condition, [(N =108; M = .078; S.E. = .003, for stress/TSST)] versus (N = 102; M = .068; S.E. = .003; for no TSST)], F(1, 147) = 5.16, p =.02. This main effect was qualified by a three-way interaction between stress condition, priming condition, and sex, F (1, 144) = 4.60, p =.03. For women in the no alcohol prime condition, those exposed to the TSST had greater increases in Peak BACs (M = .073, S.E. = .0101) than those in the no TSST condition (Peak BAC = .050; SD = S.E. = .0101, t(1, 145) = 2.59, p =.01. For men in the alcohol prime condition those exposed to the TSST had a larger increase in Peak BACs (M = .093, S.E. = .0088) than those in the no TSST condition (M = .078, S.E. = .0093), though this effect did not reach statistical significance, t(1,139) =1.81, p =.07. See Figure 4 for a graphic depiction of the three-way interaction.
Figure 4.

Peak BAC during ad libitum as a function of TSST (Stress), Alcohol Prime, and Sex.
Discussion
Our investigation is the first to examine the effects of an acute stressor, a substantial prime dose, and participant sex on behavioral impaired control in a naturalistic bar setting. A randomized substantial prime dose (.065 target BAC) known to impair behavioral control (i.e. inhibition) was utilized (Marczinski & Fillmore, 2003). We hypothesized that greater behavioral impaired control over alcohol use (Leeman et al., 2013) would be caused by the interacting effects of an acute social stressor and prime dose. Given prior work suggesting sex differences concerning stress and risk for AUD (Guinle & Sinha, 2020; Koob & White, 2017) we used a larger sample allowing us to examine participant sex as a potential moderator.
The Self-Medication Hypothesis (SMH; Conger, 1956; Hersh & Hussong, 2009; Vogel et al., 2021), suggests the introduction of an acute stressor will increase ad libitum drinking in the moment. Our results supported this basic idea. Exposure to the TSST increased ad libitum drinking relative to the control condition by nearly half (.407) of a standard drink (i.e., equivalent to approx. 4.88 ounces of beer). This is consistent with previous research on the impact of an acute stressor on alcohol consumption (de Wit et al., 2003; Hull & Young, 1983; Magrys & Olmstead, 2015; McGrath et al., 2016; Thomas et al., 2011). Importantly, the TSST was associated with heavier drinking despite all participants receiving the specific instruction to limit their drinking to no more than one drink per hour to ensure optimal performance on cognitive tasks linked to their study payment. Individuals in the TSST condition violated instructions at a significantly greater rate than those in the no TSST condition.
Based upon the Theory of Disinhibition (Baines et al., 2019; Fillmore, 2003), we hypothesized that a prime dose would interact with the stress manipulation such that participants would consume the most alcohol, and demonstrate higher BACs when they received both the prime dose of alcohol and the TSST condition. We found support for this prediction for men, but not for women. Women consumed more during ad libitum drinking when they received the TSST without the prime dose of alcohol. Our findings are generally consistent with Cyders et al., (2016) who showed that men, but not women self-medicated under a small prime dose of .15 mg/dl and negative mood induction using an IV alcohol self-administration paradigm. We also found evidence for the hypothesized interaction between prime dose and stressor for men only. Among men in the alcohol prime condition, those exposed to social stress (TSST) had a larger increase in BAC than those in the no TSST condition (.040 g % compared to .027 g %). Men in the alcohol prime condition also reached a higher peak BAC (.093g% for those in the TSST condition compared to .078g% for those in the no TSST condition). Thus, men in the prime and TSST condition reached peak BACs above legal limits (approx. peak BAC of .093). Among men who did not receive the alcohol prime, exposure to the TSST was not associated with significant change in BAC during ad libitum drinking (.054 TSST vs .058 no TSST). For men, both the SMH model and the Theory of Disinhibition (Baines et al., 2019; Fillmore, 2003) seem to be operating in an interactive way to get to dysregulated heavy episodic drinking levels despite incentives to limit consumption.
The existing literature on the impact of an acute stressor on ad libitum drinking is mixed. A number of investigators have not found evidence in support of the SMH after administering an acute stress manipulation (Cyders et al., 2016 -for women only; Higgins & Marlatt, 1973; Pratt & Davidson, 2009) whereas others have found evidence to support this model (de Wit et al., 2003; Hull & Young, 1983; Magrys & Olmstead, 2015; Thomas et al., 2011). We believe there are a number of plausible reasons for the mixed results in the existing literature including small sample sizes, a wide variety of acute stressors, and differences in ad libitum consumption periods [15-minutes (see Higgins & Marlatt, 1973; Hull & Young, 1983; Thomas et al., 2011) to 180-minutes (Leeman et al., 2013)]. Moreover, in some studies (McGrath et al., 2016; Thomas et al., 2011), participants have not been allowed to exceed a limit of more than two drinks, which is equivalent to .04 g%. Others (Wardell et al., 2018) have had to cut participants off at a maximum BAC of .08 g% (legal limit), which may limit the ability to adequately study dysregulated drinking. The current study used a robust social stressor, and allowed participants to reach BACs of .12 g% which may have improved our ability to detect effects of acute stress on ad libitum drinking.
Acute intoxication was an important moderator of the causal link between stress and alcohol consumption for men in the current investigation. This is consistent with literature showing a prime dose of alcohol increases desire for more alcohol (Rose & Duka, 2006) and robustly impairs inhibitory control among healthy participants (Marczinski & Fillmore, 2003). The results of the three-way interactions for both Change in BAC and Peak BAC suggest that social evaluative stress may increase any consumption among women, whereas it may uniquely impact continued consumption after initiation among men. Neither Thomas et al. (2011) or Cyders et al. (2016) manipulated prime dose, making our findings novel. Our findings regarding men seem to replicate and extend these studies in that men appear to be more impacted by a combination of stress and a more substantial level of prime dose (.065 target BAC).
The SMH (Conger, 1956; Hersh & Hussong, 2009; Livingston et al., 2021; Vogel et al., 2021) is a useful framework, but our study suggests additional research examining potential participant sex differences in response to acute stressors may be needed. This is important because women usually begin drinking at a later age compared to men but develop AUDs in a shorter time span (Cheng & Anthony, 2018; Strine et al., 2008). Further, women progress more quickly from regular drinking to intoxication to first experiencing alcohol problems and appear to go from loss of control over drinking to experiencing their “worst” alcohol problems more rapidly than men (Randall et al., 1999). Women with an AUD diagnosis are more likely to have shorter drinking histories compared to their male counter-parts seeking treatment (Cheng & Anthony, 2018). Conceivably, motivation for alcohol use may more quickly shift from using it for the positive effects of alcohol to using alcohol for negative reinforcement among women. This may be a result of physiological adaptations to stress and alcohol exposure in women. For example, Blaine and Sinha (2017) suggest stress has robust impacts on the hypothalamic-pituitary-adrenal axis (HPA) and these differences appear to precede the formation of AUDs. Tops et al., (2019) also found that women were more physiologically reactive to stress rejection challenges, than men. While men are sensitive to failure feedback, it is unclear whether women would be equally reactive; women were excluded from this classic study (Hull & Young, 1983).
Biological differences between men and women may contribute to the effects observed in the current study, but these differences may also be a result of differences in the socialization of men and women. While we could not address the role of gender identity or expression, it will be critical to evaluate in future studies. There is evidence that women may be more sensitive to socialization processes that focus on maintaining positive social relationships (Beck, 1983; Tops et al., 2019; Yang & Girgus, 2018). Further, Mayor (2015) suggests that gender roles may at least partly explain gender differences in stress responses, particularly with respect to cognitive appraisals and coping. Moreover, socialization pressures to conform to gender roles are associated with higher levels of anxiety, depression, stress and post-traumatic stress disorder in women compared to men (Anyau & Hjemdal, 2018; Mayor, 2015; Street & Dardis, 2018). Thus, gender differences in socialization processes may have led women in our study to be more sensitive to the TSST, which includes a social evaluative component.
Limitations.
Our study increases the understanding of the etiology of dysregulated drinking in social drinkers under acute stress, albeit there are some notable limitations. One limitation is that we used a non-dependent drinking sample rather than a dependent sample. Dependent drinkers are more likely to report drinking to cope with negative affect (Keyes et al., 2012) and to report higher craving in response to stress images compared to social drinkers (Ramchandani et al., 2018). Moreover, our findings may not generalize to individuals with comorbid mood and anxiety disorders and/or AUDs (Conrod et al., 2006). Another limitation is that the groups in which participants completed the study varied with respect to size (i.e., 2–3 people) and gender composition, which could have influenced the findings. Prior work suggests that dyads and groups (3 or more people) differ along a number of important characteristics that could influence outcomes (Moreland, 2010). However, Corbin et al. (2015) examined effects of group gender and size on affective responses to acute alcohol administration and found no significant effects of either on any outcomes. Further, we used multilevel models (MLM) to account for potential effects of the group in which participants completed the study. Nonetheless, it is possible that the size and composition of the groups influenced the pattern of observed findings. Therefore, much larger studies controlling for group composition would be beneficial in replications of this work. While our sample size was approximately twice as large as most self-administration studies, we were nonetheless underpowered to detect small to moderate effects for complex three-way interactions (Hox, 2010; Hox et al., 2017).
We also studied only a single prime dose of .065; effects may be dependent on the size of the initial priming dose (de Wit, 2003; Marczinski & Fillmore, 2003). Thus, future studies are needed to explore smaller and larger priming doses and their interactions with acute stress. Another limitation is lack of information regarding participants’ affect and cognition during the ad libitum period. Multi-method approaches might offer additional information regarding cognitive and affective processes. Further, we were unable to disaggregate effects of sex and gender in the current study. Future studies should include gender identity and gender expression in addition to biological sex to disaggregate these effects and examine the roles of sexual orientation, racial identity, and ability/disability status in alcohol use in response to social stress.
Another limitation is that we used a simulated bar laboratory rather than a real bar setting. Naturalistic drinking settings encourage more drinking, and the experience of more pleasurable disinhibition and stimulation relative to simulated bar settings (Wall et al., 2001). Regardless, the current study used a more ecologically valid drinking context (simulated bar) than has been used in most prior studies of the effects of an acute stressor on ad libitum consumption. Additionally, we did not examine the effect of the behavioral impaired control paradigm, independent of the stress and prime dose manipulation. Although there is evidence that individuals drink less under this type of instruction set (Leeman et al., 2013) it is possible that men and women may differentially violate these instructions independent of an acute stressor or a prime dose of alcohol. Finally, our study only experimentally examined an acute stressor prior to ad libitum drinking. The Appraisal Disruption Model (Sayette, 1993) postulates that alcohol consumed prior to (but not after) a social threat will lessen the experience of the stressor. Our study did not address an anticipatory stress paradigm, so this will need to be explored in conjunction with a behavioral impaired control paradigm in the future.
Despite these limitations, this work adds to the existing literature in several important ways. As the first experimental study to evaluate the interactive effects of a priming dose and social stressor on ad libitum drinking using a behavioral impaired control paradigm, the current study addresses important gaps in the literature. Further, our sample was larger than previous lab-based studies examining participant cisgender sex differences in the effects of stress on drinking behavior. In the current study, social stress (TSST) alone increased risk for heavy drinking among women, whereas social stress only led to heavier ad libitum drinking among men who had already consumed an alcohol dose sufficient to impact behavioral inhibitory control. Incorporating sex and gender differences in the SMH may improve our understanding of potentially unique pathways to AUD risk for men, women, and non-binary individuals. Future studies are needed to understand the mechanisms contributing to sex and gender differences in alcohol consumption under stress, and to disaggregate effects of sex and gender identity and expression. In summary, the findings of the current study pave the way for future research designed to improve our understanding of how acute stressors as well as the drinking context contribute to the development of behavioral impaired control over alcohol use and subsequent risk for alcohol-related problems. Our findings may also inform future prevention and intervention efforts, though replication of the findings is necessary to support such efforts.
Public Health Importance and Highlights of our Experiment.
This study found that women exposed to social stress drank more when given access to alcohol whereas men drank more only when exposed to both social stress and a priming dose of alcohol. This suggests the need for further attention to potential sex and gender differences in the role of self-medication in drinking behavior.
Acknowledgement
The authors would like to thank Dr.’s Daniel McNeish, Oi-man Kwok, and Craig Enders for all of their generous advice, time, and emotional and practical support for this work. We also thank Sean Noudali for his editorial advice and Dylan Bauman for scheduling our participants for this project. The National Institute on Alcohol Abuse and Alcoholism supported this work with a grant awarded to Julie A. Patock-Peckham (K01AA024160-01A1).
References
- Abele A (1990). Recall of positive and negative life events. Studies of mood-inducing effect and production of texts. Zeitschrift fur experimentelle und angewandte Psychologie, 37(2), 181–207. [PubMed] [Google Scholar]
- Amlung M, & MacKillop J (2014). Understanding the effects of stress and alcohol cues on motivation for alcohol via behavioral economics. Alcoholism: Clinical and Experimental Research, 38(6), 1780–1789. 10.1111/acer.12423 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anyan F, & Hjemdal O (2018). Stress of home life and gender role socializations, family cohesion, and symptoms of anxiety and depression. Women & Health, 58(5), 548–564. https://doi: 10.1080/03630242,2017.1316343. [DOI] [PubMed] [Google Scholar]
- Armeli S, Dranoff E, Tennen H, Austad CS, Fallahi CR, Raskin S, Wood R, Pearlson G. (2014). A longitudinal study of the effects of coping motives, negative affect and drinking level on drinking problems among college students. Anxiety Stress Coping, 27(5):527–541. doi: 10.1080/10615806.2014.895821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baines L, Field M, Christiansen P, & Jones A (2019). The effect of alcohol exposure and acute intoxication on inhibitory control processes and ad libitum alcohol consumption. Psychopharmacology, 236, 2187–2199. 10.1007/s00213-019-05212-4.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck AT Epstein N, Harrison RP, & Emery G (1983). Development of the sociotropy-autonomy scale: A measure of personality factors in psychopathology. University of Pennsylvania, Philadelphia: PA. [Google Scholar]
- Blaine SK, & Sinha R (2017). Alcohol, stress, and glucocorticoids: From risk to dependence and relapse in alcohol use disorders. Neuropharmacology, 122, 136–147. 10.1016/j.neuropharm.2017.01.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bradford DE, Motschman CA, Starr MJ, Curtin JJ (2017). Alcohol’s effects on emotionally motivated attention, defensive reactivity and subjective anxiety during uncertain threats, Social Cognitive and Affective Neuroscience, 12(11), 1823–1832, 10.1093/scan/nsx095 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bresin K, Mekawi Y, & Verona E (2018). The effect of laboratory manipulations of negative affect on alcohol craving and use: A meta-analysis. Psychology of addictive behaviors, 32(6), 617–627. 10.1037/adb0000383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caetano R, Vaeth P, & Canino G (2019). Comorbidity of lifetime alcohol use disorder and major depressive disorder in San Juan, Puerto Rico. Journal of Studies on Alcohol and Drugs, 80(5), 546–551. 10.15288/jsad.2019.80.546 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chassin L, Sher KJ, Hussong A, & Curran P (2013). The developmental psychopathology of alcohol use and alcohol disorders: Research achievements and future directions. Development and Psychopathology, 25(4 Pt 2), 1567–1584. 10.1017/S0954579413000771 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng HG, Anthony JC (2018). Female-male differences in alcohol dependence levels: Evidence on newly incident adolescent and young-adult drinkers in the United States, 2002–2014. Int J Methods Psychiatr Res. 27(3):e1717. doi: 10.1002/mpr.1717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chutuape MA, & de Wit H (1995). Preferences for ethanol and diazepam in anxious individuals: An evaluation of the self-medication hypothesis. Psychopharmacology, 121, 91–103. [DOI] [PubMed] [Google Scholar]
- Clay JM, & Parker MO (2018). The role of stress-reactivity, stress-recovery and risky decision-making in psychosocial stress-induced alcohol consumption in social drinkers. Psychopharmacology, 235(11):3243–3257. doi: 10.1007/s00213-018-5027-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conger JJ (1956). Reinforcement theory and the dynamics of alcoholism. Quarterly Journal of Studies on Alcohol, 17, 296–305. [PubMed] [Google Scholar]
- Conrod PJ, Stewart SH, Comeau N, & Maclean AM (2006). Efficacy of cognitive–behavioral interventions targeting personality risk factors for youth alcohol misuse. Journal of Clinical Child and Adolescent Psychology, 35(4), 550–563. 10.1207/s15374424jccp3504_6. [DOI] [PubMed] [Google Scholar]
- Corbin WR, Scott C, Boyd SJ, Menary KR, & Enders CK (2015). Contextual influences on subjective and behavioral responses to alcohol. Experimental and Clinical Psychopharmacology, 23(1), 59–70. 10.10037/a0038760. [DOI] [PubMed] [Google Scholar]
- Curtin JJ & Farchild BA (2003). Alcohol and cognitive control: Implications for regulation of behavior during response conflict. Journal of Abnormal Psychology, 112(3), 424–436. DOI: 10.1037/0021-843x.112.3.424. [DOI] [PubMed] [Google Scholar]
- Cyders MA, VanderVeen JD, Plawecki M, Millward JB, Hays J, Kareken DA, & O’Connor S (2016). Gender‐specific effects of mood on alcohol‐seeking behaviors: Preliminary findings using intravenous alcohol self‐administration. Alcoholism: Clinical and Experimental Research, 40(2), 393–400. 10.1111/acer.12955 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Wit H, & Chuptuape MA (1993). Increased ethanol choice in social drinkers following ethanol preload. Behavioral Pharmacology, 4(1), 29–36. 10.1097/00008877-199302000-00003. [DOI] [PubMed] [Google Scholar]
- de Wit H, Söderpalm AH, Nikolayev L, & Young E (2003). Effects of acute social stress on alcohol consumption in healthy subjects. Alcoholism: Clinical and Experimental Research, 27(8), 1270–1277. 10.1097/01.ALC.0000081617.37539.D6 [DOI] [PubMed] [Google Scholar]
- Duckworth AL, Kim B, & Tsukayama E (2013). Life stress impairs self-control in early adolescence. Frontiers in Psychology, 31(608), 1–12. Doi: 10.3389/fpsyg.2012.00608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairbairn CE, & Sayette MA (2014). A social-attributional analysis of alcohol response. Psychological Bulletin, 140(5), 1361–1382. 10.1037/a0037563 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fillmore MT (2003). Drug abuse as a problem of impaired control: Current approaches and findings. Behavioral and Cognitive Neuroscience Reviews, 2(3), 179–197. DOI: 10.1177/1534582303257007 [DOI] [PubMed] [Google Scholar]
- Goodman WK, Janson J, Wolf JM. (2017). Meta-analytical assessment of the effects of protocol variations on cortisol responses to the Trier Social Stress Test. Psychoneuroendocrinology, 80,26–35. doi: 10.1016/j.psyneuen.2017.02.030. [DOI] [PubMed] [Google Scholar]
- Grant BF, Chou SP, Saha TD, Pickering RP, Kerridge BT, Ruan WJ, Huang B, Jung J, Zhang H, Fan A, & Hasin DS (2017). Prevalence of 12-month alcohol use, high-risk drinking, and DSM-IV alcohol use disorder in the United States, 2001–2002 to 2012–2013: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA Psychiatry, 74(9), 911–923. 10.1001/jamapsychiatry.2017.2161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grant BF, Dawson D, & Hasin D (2000). The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV). Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, 54. [Google Scholar]
- Guinle MIB, & Sinha R (2020). The role of stress, trauma, and negative affect in alcohol misuse and alcohol use disorder in women. Alcohol Research, 40(2):5 Alcohol Research Current Reviews. 10.35946/arcr.v40.2.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heather N, Tebbutt JS, Mattick RP, & Zamir R (1993). Development of a scale for measuring impaired control over alcohol consumption: a preliminary report. Journal of Studies on Alcohol, 54(6), 700–709. 10.15288/jsa.1993.54.700 [DOI] [PubMed] [Google Scholar]
- Helminen EC, Morton ML, Wang Q, Felver JC (2019). A meta-analysis of cortisol reactivity to the Trier Social Stress Test in virtual environments. Psychoneuroendocrinology, 110, 104437. doi: 10.1016/j.psyneuen.2019.104437. [DOI] [PubMed] [Google Scholar]
- Hersh MA, & Hussong AM (2009). The association between observed parental emotion socialization and adolescent self-medication. Journal of Abnormal Child Psychology, 37(4), 493–506. 10.1007/s10802-008-9291-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins RL, & Marlatt GA (1973). Effects of anxiety arousal on the consumption of alcohol by alcoholics and social drinkers. Journal of Consulting and Clinical Psychology, 41(3), 426. 10.1037/h0035366 [DOI] [PubMed] [Google Scholar]
- Hingson R, Zha W, & Smyth D (2017). Magnitude and trends in heavy episodic drinking, alcohol-impaired driving, and alcohol-related mortality and overdose hospitalizations among emerging adults of college ages 18–24 in the United States, 1998–2014. Journal of Studies on Alcohol and Drugs, 78(4), 540–548. doi.org/ 10.15288/jsad.2017.78.540 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hox JJ (2010). Multilevel analysis: Techniques and applications. Great Britian: Routledge. [Google Scholar]
- Hox JJ Moerbeek M, & van de Schoot R (2017). Multilevel analysis: Techniques and applications. 3rd edition. New York: Routledge. 10.4324/978131560982 [DOI] [Google Scholar]
- Hox J (1998) Multilevel Modeling: When and Why. In: Balderjahn I, Mathar R, Schader M (eds) Classification, Data Analysis, and Data Highways. Studies in Classification, Data Analysis, and Knowledge Organization. Springer, Berlin, Heidelberg. 10.1007/978-3-642-72087-1_17 [DOI] [Google Scholar]
- Hull JG, & Young RD (1983). Self-consciousness, self-esteem, and success–failure as determinants of alcohol consumption in male social drinkers. Journal of Personality and Social Psychology, 44(6), 1097–1109. 10.1037/0022-3514.44.6.1097 [DOI] [PubMed] [Google Scholar]
- Jones A, Christiansen P, Nederkoorn C, Houben K, & Field M (2013). Fluctuating disinhibition: implications for the understanding and treatment of alcohol and other substance use disorders. Frontiers in psychiatry, 4, 140. 10.3389/fpsyt.2013.00140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keyes KM, Hatzenbuehler ML, Grant BF, & Hasin DS (2012). Stress and alcohol: Epidemiologic evidence. Alcohol Research: Current Reviews, 34(4), 391–400. [PMC free article] [PubMed] [Google Scholar]
- Kirschbaum C, Pirke KM, & Hellhammer DH (1993). The ‘Trier Social Stress Test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1–2), 76–81. 10.1159/000119004 [DOI] [PubMed] [Google Scholar]
- Koob GF, & White A (2017). Alcohol and the female brain. Presented at 2017 National Conference on Alcohol and Opioid Use in Women & Girls: Advances in Prevention, Treatment, and Recovery Research. Washington DC, MA. [Google Scholar]
- Kwako LE, Spagnolo PA, Schwandt ML, Thorsell A, George DT, Momenan R, Rio DE, Huestis M, Anizan S, Concheiro M, Sinha R, & Heilig M (2015). The corticotropin releasing hormone-1 (CRH1) receptor antagonist pexacerfont in alcohol dependence: a randomized controlled experimental medicine study. Neuropsychopharmacology, 40(5), 1053–1063. 10.1038/npp.2014.306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leeman RF, Corbin WR, Nogueira C, Krishnan-Sarin S, Potenza MN, & O’Malley SS (2013). A human alcohol self-administration paradigm to model individual differences in impaired control over alcohol use. Experimental and Clinical Psychopharmacology, 21(4), 303–314. 10.1037/a0033438 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leeman RF, Fenton M, & Volpicelli JR (2007) Impaired control and undergraduate problem drinking. Alcohol, 42(1):42–8. doi: 10.1093/alcalc/agl095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leeman RF, Patock-Peckham JA, & Potenza MN (2012). Impaired control over alcohol use: An under-addressed risk factor for problem drinking in young adults? Experimental and Clinical Psychopharmacology, 20(2), 92–106. 10.1037/a0026463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leeman RF, Toll BA, Taylor LA, & Volpicelli JR (2009). Alcohol-induced disinhibition expectancies and impaired control as prospective predictors of problem drinking in undergraduates. Psychology of Addictive Behaviors, 23, 553–563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leeman RF, Beseler CL, Helms CM, Patock-Peckham JA, Wakeling VA, & Kahler CW (2014). A brief, critical review of research on impaired control over alcohol use and suggestions for future studies. Alcoholism, clinical and experimental research, 38(2), 301–308. 10.1111/acer.12269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Livingston NA, Lee DJ, Mahoney CT, Farmer SL, Cole T, Marx BP, Keane TM (2021). Longitudinal assessment of PTSD and illicit drug use among male and female OEF-OIF veterans. Addictive Behaviors, 118, 106870. 10.1016/j.addbeh.2021.106870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorah J (2018). Effect size measures for multilevel models: Definition, interpretation, and TIMSS example. Large-scale Assessments in Education, 6:8 10.1186/s40536-018-0061-2 [DOI] [Google Scholar]
- Magrys SA, & Olmstead MC (2015). Acute stress increases voluntary consumption of alcohol in undergraduates. Alcohol and Alcoholism, 50(2), 213–218. 10.1093/alcalc/agu101 [DOI] [PubMed] [Google Scholar]
- Marczinski CA, & Fillmore MT (2003). Preresponse cues reduce the impairing effects of alcohol on the execution and suppression of responses. Experimental and Clinical Psychopharmacology, 11(1), 110–117. 10.1037/1064-1297.11.1.110 [DOI] [PubMed] [Google Scholar]
- Mayor E (2015). Gender roles and traits in stress and health. Frontiers in Psychology, 6, 7. doi:http://dx.doi.org.ezproxy1.lib.asu.edu/10.3389/fpsyg.2015.00779 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCaul ME, Roach D, Hasin DS, Weisner C, Chang G, & Sinha R (2019). Alcohol and women: A brief overview. Alcoholism: Clinical and Experimental Research, 43(5), 774–779. doi:http://dx.doi.org.ezproxy1.lib.asu.edu/10.1111/acer.13985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGrath E, Jones A, & Field M (2016). Acute stress increases ad libitum alcohol consumption in heavy drinkers, but not through impaired inhibitory control. Psychopharmacology, 233, 1227–1234. 10.1007/s00213-016-4205-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller PM Hersen M, Eisler RM, & Hilsman G (1974). Effects of stress on operant drinking of alcoholics and social drinkers. Behavior Research & Therapy, 12, 67–72. doi: 10.1016/0005-7967(74)90094-1. [DOI] [PubMed] [Google Scholar]
- Moreland RL, (2010). Are dyads really groups? Small Group Research, 41(2), 251–267. https://doi: 10.1177/1046496409358618. [DOI] [Google Scholar]
- Peltier MR, Verplaetse TL, Mineur YS, Petrakis IL, Cosgrove KP, Picciotto MR, & McKee SA (2019). Sex differences in stress-related alcohol use. Neurobiology of Stress, 10, 100149. 10.1016/j.ynstr.2019.100149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peugh JL (2010). A practical guide to multilevel modeling. Journal of School Psychology, 48(1), 85–112. doi:http://dx.doi.org.ezproxy1.lib.asu.edu/10.1016/j.jsp.2009.09.002 [DOI] [PubMed] [Google Scholar]
- Pratt WM, & Davidson D (2009). Role of the HPA axis and the A118G polymorphism of the μ-opioid receptor in stress-induced drinking behavior. Alcohol & Alcoholism, 44(4), 358–365. 10.1093/alcalc/agp007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self report depression scale for research in the general population. Applied Psychological Measurements, 1, 385–401. [Google Scholar]
- Randall CL, Roberts JS, Del Boca FK, Carroll KM, Connors GJ, & Mattson ME (1999). Telescoping of landmark events associated with drinking: A gender comparison. Journal of Studies on Alcohol, 60(2), 252–260. 10.15288/jsa.1999.60.252 [DOI] [PubMed] [Google Scholar]
- Ramchandani VA, Stangl BL, Blaine SK, Plawecki MH, Schwandt ML, Kwako LE, Sinha R, Cyders MA, O’Connor S, & Zakhari S (2018). Stress vulnerability and alcohol use and consequences: From human laboratory studies to clinical outcomes. Alcohol, 72, 75–88. 10.1016/j.alcohol.2018.06.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reiss S, Peterson RA, Gursky DM, & McNally RJ (1986). Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behaviour Research and Therapy, 24(1):1–8. https://doi: 10.1016/0005-7967(86)90143-9. [DOI] [PubMed] [Google Scholar]
- Rose AK, & Duka T (2006). Effects of dose and time on the ability of alcohol to prime social drinkers. Behavioural Pharmacology, 17(1), 61–70. 10.1097/01.fbp.0000189814.61802.92 [DOI] [PubMed] [Google Scholar]
- Sayette MA (1993). An appraisal-disruption model of alcohol’s effects on stress responses in social drinkers. Psychological Bulletin, 114(3), 459–476. [DOI] [PubMed] [Google Scholar]
- Sinha R (2007). The role of stress in addiction relapse. Current Psychiatry Reports, 9(5), 388–395. 10.1007/s11920-007-0050-6 [DOI] [PubMed] [Google Scholar]
- Sinha R (2009). Modeling stress and drug craving in the laboratory: Implications for addiction treatment development. Addiction Biology, 14(1), 84–98. 10.1111/j.1369-1600.2008.00134.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sinha R, Lacadie CM, Constable RT, & Seo D (2016). Dynamic neural activity during stress signals resilient coping. PNAS, 113(31), 8837–8842. 10.1073/pnas.1600965113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, & Jacobs GA (1983). Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press. [Google Scholar]
- Street AE, & Daris CM, (2018). Using a social construction of gender lens to understand gender differences in PTSD. Clinical Psychology Review, 66, 97–105. 10.1016/j.cpr.c018.03.001. [DOI] [PubMed] [Google Scholar]
- Strine TW, Mokdad AH, Balluz LS, Gonzalez O, Crider R, Berry JT, & Kroenke K (2008). Depression and anxiety in the United States: Findings from the 2006 behavioral risk factor surveillance system. Psychiatric Services, 59(12), 1383–1390. [DOI] [PubMed] [Google Scholar]
- Thomas SE, Bacon AK, Randall PK, Brady KT, & See RE (2011). An acute psychosocial stressor increases drinking in non-treatment-seeking alcoholics. Psychopharmacology, 218(1), 19–28. 10.1007/s00213-010-2163-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tops S, Habel U, Abel T, Derntl B, Radke S (2019). The verbal interaction social threat task: a new paradigm investigating the effects of social rejection in men and women. Frontiers in Neuroscience, 7;13:830. doi: 10.3389/fnins.2019.00830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Västfjäll D (2001). Emotion induction through music: A review of the musical mood induction procedure. Musicae Scientiae, 5(1_suppl), 173–211. [Google Scholar]
- Vaughan CL, Stangl BL, Schwandt ML, Corey KM, Hendershot CS, & Ramchandani VA (2019). The relationship between impaired control, impulsivity, and alcohol self-administration in nondependent drinkers. Experimental and Clinical Psychopharmacology, 27(3), 236. 10.1037/pha0000247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vogel L, Koller G, & Ehring T (2021). The relationship between posttraumatic stress symptoms and craving in patients with substance use disorder attending detoxification. Drug and Alcohol Dependence, 223, 1–6. doi: 10.1016/j.drugalcdep.2021.108709. [DOI] [PubMed] [Google Scholar]
- Waddell JT, Corbin WR, & Marohnic SD (2021). Putting things in context: Longitudinal relations between drinking contexts, drinking motives, and negative alcohol consequences. Psychology of Addictive Behaviors, 35(2), 148–159. 10.1037/adb0000653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wall A, Hinson RE, McKee SA, & Goldstein A (2001). Examining alcohol outcome expectancies in laboratory and naturalistic bar settings: A within-subject experimental analysis. Psychology of Addictive Behaviors, 15, 219–226. 10.1037/0893-164X.15.3.219 [DOI] [PubMed] [Google Scholar]
- Wardell JD, Le Foll B, & Hendershot CS (2018). Preliminary evaluation of a human laboratory model of impaired control over alcohol using intravenous alcohol self-administration. Journal of Psychopharmacology, 32(1), 105–115. 10.1177/0269881117723000 [DOI] [PubMed] [Google Scholar]
- White AM (2020). Gender differences in the epidemiology of alcohol use and related harms in the United States. Alcohol Research Current Reviews, 40(2):01 10.35946/arcr.v40.2.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wood MD, Nagoshi CT, & Dennis DA (1992). Alcohol norms and expectations as predictors of alcohol use and problems in a college student sample. The American Journal of Drug and Alcohol Abuse, 18(4), 461–467 10.3109/00952999209051042 [DOI] [PubMed] [Google Scholar]
- Yang K, Girgus JS Are women more likely than men are to care excessively about maintaining positive social relationships? A meta-analytic review of the gender difference in sociotropy. Sex Roles 81, 157–172 (2019). 10.1007/s11199-018-0980-y [DOI] [Google Scholar]