

Version Changes
Revised. Amendments from Version 1
The following changes were performed to respond to reviewers 1 and 2.
The novelty, relevance, and originality of the paper are emphasized further in the Introduction section.
The calculation of the minimal sample size is addressed more in detail in the Methods section to demonstrate the representativeness of our sampled population.
The acceptable Cronbach alpha values (>0.7) for the KAP part of the questionnaire (knowledge, attitude, and practice-related questions) are added under the Methods section (Questionnaire subsection).
In the discussion part, based on the observed knowledge scores (mentioned under the results section), we emphasized that our sample population expressed deficits in nutrition label-related knowledge compared to other populations in preliminary investigations.
The authors added under the discussion part the following references: Wahab RA (2018); Liuzzo G. et al. (2019); Alshukri A. et al. (2020).
Abstract
Background: Food labeling is a fundamental educational tool for advocating for public awareness. It emphasizes knowledge of the nutrient content of food and thus directs the choice towards the healthiest food products.
This cross-sectional survey aimed to assess the knowledge, attitudes, and practices (KAP) regarding nutrition label use in Lebanon through a valid questionnaire.
Methods: Overall, 768 participants (mean age: 30.8 ±12, males: 60.2%) were recruited randomly between February and May 2020. We used word of mouth and social media to recruit our sample population.
Results: Social media was the most accessed tool to attain nutrition information by responders (39.8%). More than half the participants expressed positive attitudes to check information related to sugars (66.4%), vitamins (64.9%), total fats (61.7%), proteins (59.1%), and calories (58.7%) on the food label. Expiry date, price, and brand name were the top three considerations while reading food labels. About half (46.5%) reported to “always” look at the food label. Responders reported reading labels related primarily to sugars (44.3%), calories (38.8%), and total fats (36.8%). The optimal total KAP score was 46; our findings revealed a mean KAP score of 14.46 ±7 (31.4%). When categorizing the KAP scores, 15% had high scores, and 85% scored low. Spearman’s coefficients showed positive correlations between knowledge-attitude, knowledge-practice, and attitude-practice scores, with p<0.001. The regression analysis revealed that gender, age, BMI, residency area, educational level, university degree, health and diet statuses, and activity level were significant predictors of the KAP score. Being on a diet had the highest odds (OR=3.107, CI=1.904-5.072, p<0.001).
Conclusion: The low awareness of food labels leads Lebanese people to choose unhealthy food options. A planned educational program is recommended to ease the interpretation of these labels.
Keywords: Food labels, knowledge, attitude, practices, Lebanon
Introduction
Non-communicable diseases (NCDs) account for over 35 million disease cases per year and two-thirds of the world's deaths. 1 Nutrition-related non-communicable diseases (N-NCDs), mainly diabetes, cancer, hypertension, and cardiovascular diseases, are highly prevalent in most countries in the Eastern Mediterranean Region (EMR). 2 In Lebanon, it is estimated that NCDs accounted for 91% of all deaths in 2016. 3 Thus, as a preventive action plan, the Lebanese Ministry of Public Health (MOPH) developed a national NCD prevention and control plan (NCD-PCP), that is yet to be implemented. 4 Dietary guidelines and labeling legislations are considered an effective tool for creating a healthy food environment to reduce the global burden of NCDs. 5 Moreover, the nutrition facts provided on food labels could drive favorable consumers’ behaviors. 6 In the United States of America (US), 98% of FDA-regulated packaged foods have nutrition facts panels (NFPs). 7 As for Europe, 84% of products have nutrition labels. 8 In Lebanon, nutrition labeling is regulated by mandatory standards: NL 206, NL 719 which address the labeling requirements for foods. 9 Food labeling is required for most prepared foods such as breads, cereals, canned and frozen foods, snacks, desserts, drinks, among others. Ingredients list, nutrition facts, food allergen declarations and date marking must be available as well. 9 The use of food label information is influenced by multiple elements, including comprehension difficulties, promotions, price, educational level, attention, and memorizing the information to apply it to a consequent food-related decision. 10 Thus, a combination of these factors may propel the consumer to prefer one product over another. 10 However, the presence of detailed nutrition information on the food package does not necessarily guarantee a healthy choice. 6 For example, it was found that most consumers (78%) could notice nutrient differences between food products; however, fewer (20%) were able to calculate the contribution of food nutrients to the daily intake. 10 Additionally, a recent cross-sectional study revealed that the Health Star Rating, a front-of-pack labelling system that rates the overall nutrition profile of packaged food and assigns it a rating from 0.5 to 5 stars, resulted in a greater willingness to pay for healthier products. 6 The cognitive processing model considers decision-making as a high-level cognitive process defining how people think, perceive, remember and learn. 10 In other words, it represents the acquisition and storing of knowledge related to any topic leading to a corresponding behavior. 10 As for nutrition labels, this model showed that food purchasing behaviors depend heavily on having prior knowledge via three interlinked pathways. 10 Prior knowledge could enable consumers to disregard marketing attributes. 10 Besides, it facilitates the comprehension and memory of nutrition information. 10 As a result, the stored information supports the choice of healthy food options. 10 The model concluded that consumers who are more knowledgeable about food nutrients are more likely to develop positive attitudes and use label information productively and correctly. 10 A previous study reported that two-third of the consumers with a particular interest in healthy eating actually payed attention to food labels when shopping. 11 This result suggests that across most countries, the effectiveness of food labelling varies with culture, nutritional knowledge and demographic characteristics of the population. 11 The usage and understanding of nutrition labels are inadequately registered before in Lebanon, with a current shortage of data on this topic. Thus, it is a high priority to point out the factors affecting Lebanese consumers’ interpretation of food labels, to formulate new regulations or update existing ones. The aim of this study, the first of its kind in Lebanon, was to assess consumers’ knowledge, attitudes and practices (KAP) regarding the information on food labels, and to investigate the correlates of low levels of KAP among Lebanese shoppers. The study findings could serve as an initiative to motivate the national implementation of effective food labeling approaches like the Nutri-score front-of- pack label.
Methods
Study design and data collection
This was a cross-sectional study conducted between February and May 2020. According to the Lebanese Ministry of Public Health (MOPH), the total population aged 15-64 years across all Lebanese governorates in 2020 was 3,079,431. As per the Epi-info statistical software developed by the Center for Disease Control and Prevention Version 7.2, taking an acceptable margin of error of 5% and a confidence level of 95%, the minimum representative sample size was 384. Thus, we eventually recruited 768 participants from the different Lebanese governorates. Lebanese participants aged 15 to 64 years old were eligible to participate in the study. Non-Lebanese individuals and those who did not fit our age recommendations were disregarded while collecting data. Due to the national lockdown imposed due to the COVID-19 pandemic, a self-constructed and validated questionnaire was filled online. We used word of mouth and social media to recruit our population. We gave a brief explanation of our valuable research objectives for each responder. The collected data were solely used for scientific and research purposes.
Questionnaire
A 41-item questionnaire was adapted after conducting an extensive review of the literature and based on instruments used in previous studies. 12 – 14 It was comprised of four parts: the first collected information on demographic, socio-economic and health-related data; the second part (11 questions) focused on the knowledge related to nutrition labels; the third (five questions) addressed the attitudes, and the fourth part (12 questions) investigated the responder’s practices. The questionnaire was drafted in English, subsequently translated into Arabic, the native language of the participants. It was filled online, and it took the participant around 20 minutes to fill it. The completion of the questionnaire was voluntary and anonymous. Firstly, our formulated questionnaire was piloted with 200 respondents to check its acceptability. Its internal consistency and validity were assessed using Cronbach’s alpha in a preliminary analysis after conducting the pilot study. The observed alpha values were acceptable for all the questionnaire sections (0.909 for knowledge questions, 0.841 for the attitude questions, and 0.836 for the practice questions). As the pilot study justified its validity and reproducibility (Cronbach’s alpha > 0.7 was considered acceptable), the questionnaire was then employed for further data collection. The findings from the pilot study were not considered in the final analysis.
Scoring criteria of the knowledge, attitudes, and practices
In regard to knowledge, a score of 1 point was granted for responders who answered correctly. Otherwise, those who reported a wrong answer, or failed to give any response (I don’t know response) were given no mark. For each respondent, an overall knowledge score was calculated, by adding the scores from all responses. The respondent could earn a maximum score of 14. The mean knowledge score for our sampled population was then calculated. Regarding the attitudes, and in a similar concept, one point was allocated for each appropriate response; assumed to be a positive attitude. However, a score of zero was issued for undesirable responses which were considered as negative attitudes. For each respondent, an overall attitude score was calculated, by adding the scores from all responses, with a maximum score of 16. The mean attitude score for the overall population was then derived. Likewise, the practice score was computed by adding the respondent's number of appropriate responses over a score of 16. The relevant practice warranted one score for the respondent, whereas an improper practice left the respondent with no score granted. Mean practice score for each respondent was calculated by dividing the total practice score by 16. The resulting scores for the KAP were summed up to generate individualized KAP scores. The respondents could get a maximum KAP score of 46. The KAP score, therefore, was categorized into two levels. A low KAP (<23) and a high KAP (≥23). It is worth noting that the evaluation of the appropriateness of the responders’ KAPs was literature-based, with no subjective judgment.
Statistical analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) software version 25. Demographic, socio-economic, and health-related conditions and the responses related to the knowledge, attitudes, and practices were analyzed descriptively. Data were represented as means ± standard deviation (SD) for continuous variables, and as frequencies (N) and percentages (%) for the categorical ones. The Shapiro-Wilk test indicated a non-normal distribution for the KAP scores, and thus, we used the Mann-Whitney U and Kruskal-Wallis tests to assess differences in the mean KAP scores. The Mann–Whitney U test is suitable for the independent variables with two groups (such as gender), while the Kruskal–Wallis test was used for independent variables including more than two groups (residency, for instance). We also referred to the Spearman’s rank correlation coefficient (rho) to examine the associations between KAP scores. A binary logistic regression was conducted to determine the predictors of KAP scores. A confidence interval of 95% was applied, and the level of significance was determined at 5%.
Ethical considerations
This study received approval from the ethical committee of the Lebanese University (protocol code CUER # 22-2020). The study’s design and analyses were conducted according to the guidelines of the Declaration of Helsinki. Adult respondents and minors’ families provided a written informed consent before filling the questionnaire, and their confidentiality was protected. We received written informed consent from the adult respondents and minors’ family for the publication of this data.
Results
Demographic and socio-economic characteristics
A total of 768 individuals were included in our analysis. The mean age of the overall sample was 30.8 ± 12 years. Adults (25-64 years old) represented 57.8% of the total population, while the remaining were youth (15-24 years old). Male participants constituted the dominant proportion (60.2%). More than half (59.4%) were single or divorced, while 40.6% were married. Moreover, the majority (61.3%) had no children. 49.5% of respondents were working, 35% had no job, 14.3% were housewives, and 1.2% were retired. As for the monthly wage, about half the participants (49.6%) had no salary at all, and another salient proportion (31.9%) were paid less than 1000$ a month. However, 17.3% had a salary of 1000$-3000$, and just 1.2% were earning more than 3000$ per month. Regarding their educational levels, 53.9% were university graduates or still studying at university, among which 76% had Bachelor’s degrees. Besides, 13.7% were studying at general secondary schools, 11.6% were studying at technical secondary schools, 11.2% were studying at elementary/intermediate schools, whereas 9.6% were not attending school at all. Among the final sample, around half the population (49.8%) were living in Beirut and the Mount Lebanon area. The remaining were living in South Lebanon (19%), and North Lebanon (31.2%) areas. Moreover, 45.5% of people in this study had normal BMI values, and 30.5% were overweight. Obesity and overweight status were more prevalent among the male participants (p<0.001). These findings are presented in Table 1.
Table 1. Demographic and socio-economic characteristics of the study participants.
| Variable | Category | Total | Females | Males | P-value | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Age categories | Youth (15-24) | 324 | 42.2 | 203 | 43.9 | 121 | 39.5 | 0.233 |
| Adults (25-64) | 444 | 57.8 | 259 | 56.1 | 185 | 60.5 | ||
| BMI categories | Underweight | 32 | 4.2 | 26 | 5.6 | 6 | 2 | < 0.001 |
| Normal | 350 | 45.5 | 242 | 52.5 | 106 | 34.8 | ||
| Overweight | 234 | 30.5 | 121 | 26.2 | 113 | 37 | ||
| Obese | 152 | 19.8 | 72 | 15.6 | 80 | 26.2 | ||
| Gender | Male | 462 | 60.2 | NA | NA | NA | NA | NA |
| Female | 306 | 39.8 | NA | NA | NA | NA | ||
| Residency | Beirut | 78 | 10.2 | 40 | 8.6 | 38 | 12.4 | < 0.001 |
| South Lebanon | 146 | 19 | 83 | 18 | 63 | 20.6 | ||
| North Lebanon | 240 | 31.2 | 140 | 30.3 | 100 | 32.7 | ||
| Mount Lebanon | 304 | 39.6 | 199 | 43.1 | 105 | 34.3 | ||
| Marital status | Married | 312 | 40.6 | 195 | 42.2 | 117 | 38.2 | 0.294 |
| Not Married | 456 | 59.4 | 267 | 57.8 | 189 | 61.8 | ||
| Having children | No | 471 | 61.3 | 277 | 60 | 194 | 63.4 | 0.364 |
| Yes | 297 | 38.7 | 185 | 40 | 112 | 36.6 | ||
| Unemployed | 269 | 35 | 163 | 35.3 | 106 | 34.6 | ||
| Retired | 9 | 1.2 | 0 | 0 | 9 | 2.9 | ||
| Housewife | 110 | 14.3 | 110 | 23.8 | 0 | 0 | ||
| Employed | 380 | 49.5 | 189 | 40.9 | 191 | 62.4 | ||
| Employment profession | Medical | 32 | 8.4 | 25 | 13.2 | 7 | 3.6 | <0.001 |
| Non-Medical | 348 | 91.6 | 164 | 86.7 | 184 | 96.3 | ||
| Monthly wage | <1,000$ | 245 | 31.9 | 144 | 31.2 | 101 | 33 | <0.001 |
| 1,000$ - 2,000$ | 111 | 14.4 | 39 | 8.4 | 72 | 23.5 | ||
| 2,000$ - 3,000$ | 22 | 2.9 | 7 | 1.5 | 15 | 4.9 | ||
| >3000$ | 9 | 1.2 | 0 | 0 | 9 | 2.9 | ||
| No salary | 381 | 49.6 | 272 | 58.9 | 109 | 35.6 | ||
| Educational level | Did not attend school | 74 | 9.6 | 41 | 8.9 | 331 | 10.8 | <0.001 |
| Elementary/Intermediate Schools | 86 | 11.2 | 45 | 9.7 | 41 | 13.4 | ||
| General Secondary School | 105 | 13.7 | 62 | 13.4 | 43 | 14.1 | ||
| Technical Secondary School | 89 | 11.6 | 50 | 10.8 | 39 | 12.7 | ||
| University | 414 | 53.9 | 264 | 57.10 | 150 | 49 | ||
| University degree | Bachelors’ | 315 | 76 | 189 | 71.5 | 126 | 84 | <0.001 |
| Masters’ | 91 | 22 | 72 | 27.2 | 19 | 12.6 | ||
| Ph.D. | 8 | 2 | 3 | 1.4 | 5 | 3.3 | ||
| University major | Medicine/pharmacy | 19 | 4.6 | 10 | 3.7 | 9 | 5.9 | < 0.001 |
| Business | 88 | 21.3 | 36 | 13.6 | 52 | 34.4 | ||
| Engineering | 37 | 8.9 | 14 | 5.3 | 23 | 15.2 | ||
| Agriculture | 1 | 0.2 | 1 | 0.4 | 0 | 0 | ||
| Public health | 66 | 16 | 59 | 22.3 | 7 | 4.6 | ||
| Literature | 61 | 14.7 | 50 | 18.8 | 11 | 7.3 | ||
| Tourism | 10 | 2.4 | 5 | 1.9 | 5 | 3.3 | ||
| Education | 11 | 2.7 | 10 | 3.8 | 1 | 0.6 | ||
| Law | 32 | 7.7 | 20 | 7.5 | 12 | 8 | ||
| Arts | 29 | 7 | 19 | 7.2 | 10 | 6.61 | ||
| Sciences | 58 | 14 | 39 | 14.7 | 119 | 12.6 | ||
| Religion | 2 | 0.5 | 1 | 0.4 | 1 | 0.6 | ||
Health and lifestyle conditions
As regards their health status, an appreciable proportion (42.7%) had medical conditions. Specifically, 22.9% had nutrition-related chronic diseases (diabetes, hypertension, cardiovascular and kidney disorders); 22.5% had gastrointestinal disorders (including gastroesophageal reflux disease (GERD), chronic constipation, and intolerances); 13.4% had thyroid disorders, and 3.2% were anemic. The remaining (38%) reported other health conditions (neurological, depression, polycystic ovarian syndrome, among others; Table 2). About one quarter of our sampled population were physically active (attending gym), active males (31.7%) were significantly higher than active females (20.8%), p=0.001. Additionally, 34.2% admitted that they were restricted to specific diets. It was shown that the most prevalent diets were weight loss (55.2%), low carbohydrate (15.2%), and weight gain (8.4%). Others were following intermittent fasting (6.6%), therapeutic (4.9%), low-fat (4.5%), vegan/vegetarian (4.5%), and gluten-free (0.4%) diets. More than half of the female dieters (61.4%) were following a weight loss diet, which was higher than that of males by 18.6%, p<0.001 ( Table 2).
Table 2. Health and lifestyle conditions of the study participants.
| Variable | Category | Total | Females | Males | P-value | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Medical conditions | Yes | 328 | 42.7 | 224 | 48.52 | 216 | 70.6 | <0.001 |
| No | 440 | 57.3 | 238 | 51.5 | 90 | 29.4 | ||
| Type of medical condition | Nutrition-related (diabetes, cardiovascular diseases, hypertension, Kidney disorders) | 1432 | 22.9 | 82 | 17.6 | 61 | 40.5 | <0.001 |
| Gastro-intestinal disorders | 143 | 22.5 | 101 | 21.8 | 422 | 27.9 | ||
| Thyroid gland disorders | 861 | 13.4 | 74 | 16 | 12 | 8 | ||
| Anemia | 20 | 3.2 | 20 | 4.3 | 0 | 0 | ||
| Others | 243 | 38 | 178 | 36.2 | 2242 | 3 | ||
| Physical activity | No | 575 | 74.9 | 366 | 79.2 | 209 | 68.3 | 0.001 |
| Yes | 193 | 25.1 | 96 | 20.8 | 97 | 31.7 | ||
| Diet | No | 505 | 65.8 | 286 | 61.9 | 219 | 71.6 | 0.007 |
| Yes | 263 | 34.2 | 176 | 38.1 | 87 | 28.4 | ||
| Diet type | Weight loss | 124 | 55.2 | 91 | 61.4 | 33 | 42.8 | <0.001 |
| Weight gain | 19 | 8.4 | 7 | 4.7 | 12 | 15.6 | ||
| Low carbohydrates | 39 | 15.2 | 16 | 18.9 | 23 | 29.9 | ||
| Low fat | 8 | 4.5 | 4 | 2.7 | 4 | 5.1 | ||
| Vegan/vegetarian | 8 | 4.5 | 7 | 4.7 | 1 | 1.3 | ||
| Therapeutic | 11 | 4.9 | 10 | 9.4 | 1 | 1.3 | ||
| Intermittent fasting | 15 | 6.6 | 12 | 2.6 | 3 | 3.9 | ||
| Gluten-free | 1 | 0.4 | 1 | 0.7 | 0 | 0 | ||
Knowledge related to the sources of nutritional information and reading of nutrition labels
Nutrition information may be accessed from varied sources, and therefore, we asked our participants to report their frequently used sources to obtain nutrition-related information. Our findings showed that social media platforms were used more frequently (39.8%) ( Figure 1). Almost 36.4% of Lebanese shoppers relied on Internet and magazines as data sources, based on our survey ( Figure 1). On the other hand, a salient proportion of our sampled population (31%) accessed accurate nutrition facts from specialists, such as physicians and dietitians ( Figure 1). Family (27.7%), friends (21.8%), and TV/radio channels (18.2%) were also substantial information sources. Otherwise, the minority reported referring to gym coaches (4.6%) or taking nutrition courses (3.8%) ( Figure 1).
Figure 1. Sources of nutrition information (% of participants).

Participants’ responses to knowledge questions are described in Table 3. For knowledge scoring, participants were asked to calculate the number of calories contained in 325 grams of condensed milk (calories per 100 grams were given). They also had to choose the order in which food ingredients appeared on the front of the package. Their familiarity with the “sugar-free” claims indication was also assessed. Additionally, we assessed their awareness of common food additives’ function (xylitol, sorbitol, and aspartame), and whether these sweeteners could have a laxative effect or not. Furthermore, they had to decide if monosodium glutamate (MSG) can be consumed by hypertensive patients and if hydrogenated oils were healthy or unhealthy food ingredients. Moreover, we examined their familiarity with six nutrition symbols: “vegetarian”; “non-vegetarian”; “vegan”; “gluten-free”; “trans-fat-free”; and “genetically modified organisms (GMO)” symbols. The final assessed knowledge area focused on E-numbers and their corresponding functions when added to food.
Table 3. Knowledge, attitudes, and practices of study participants (descriptive analysis).
| Appropriate answer | Positive answer* N (%) | Negative answer* N (%) | Don’t know N (%) | |
|---|---|---|---|---|
| Knowledge | ||||
| Calculation of calories present in 395 g of “Nestle” can | 1283 Kcal | 196 (25.6) | 49 (6.4) | 522 (68) |
| The order of the ingredients listed on the food package | Descending | 221 (28.8) | 155 (20.2) | 392 (50.6) |
| “Sugar Free” claim indication | No sugar, contains sweetener | 378 (48.6) | 265 (34.9) | 130 (16.5) |
| Function of Xylitol, Sorbitol, and Aspartame | Sweeteners | 174 (22.7) | 13 (1.7) | 581 (75.6) |
| Laxative effect of sweeteners | Laxative | 310 (40.4) | 26 (3.4) | 432 (56.2) |
| Monosodium glutamate (MSG) for hypertensive patients | Not allowed | 48 (6.3) | 4 (0.5) | 716 (93.2) |
| Healthfulness of hydrogenated oils | Not healthy | 322 (42) | 66 (8.6) | 379 (49.4) |
| Guess of the “Vegetarian” symbol indication (Green dotted) | Suitable for vegetarians | 18 (2.3) | 13 (1.7) | 737 (96) |
| Guess of the "Non-Vegetarian" symbol indication (Red dotted) | Not suitable for vegetarians | 8 (1) | 20 (2.6) | 740 (96.6) |
| Guess of the “Vegan” symbol indication | Suitable for vegans | 32 (4.2) | 132 (14.9) | 604 (78.9) |
| Guess of the “Gluten-Free” symbol indication | Suitable for celiac disease patients | 115 (15) | 18 (1) | 632 (84) |
| Guess the “Trans-Fat” symbol indication | Contains no trans-fat | 7 (0.9) | 68 (8.9) | 692 (90.2) |
| Guess the “GMO” symbol indication | Genetically modified product | 10 (1.3) | 45 (5.9) | 713 (92.8) |
| Familiarity with the E-labels and does each E ranges | Know what the “E”s are and their functions | 56 (7.3) | 29 (3.8) | 683 (88.9) |
| Attitudes | ||||
| The nutrition facts panel (NFP) beneficial use | Beneficial | 557 (72.5) | 211 ( 27.5) | - |
| Mandating of Nutrition Labels | Necessary | 687 (89.5) | 36 (4.7) | 45 (5.8) |
| The interest of looking over “calories” on the NFP | Interested | 451 (58.7) | 162 (21.1) | 155 (20.2) |
| The interest of looking over “carbohydrates” on the NFP | Interested | 343 (44.7) | 167 (21.7) | 258 (33.6) |
| The interest of looking over “total fats” on the NFP | Interested | 474 (61.7) | 212 (27.6) | 82 (10.7) |
| The interest of looking over “proteins” on the NFP | Interested | 454 (59.1) | 206 (26.8) | 108 (14.1) |
| The interest of looking over “sugars” on the NFP | Interested | 510 (66.4) | 246 (32) | 12 (1.6) |
| The interest of looking over “fibers” on the NFP | Interested | 358 (46.6) | 136 (17.7) | 274 (35.7) |
| The interest of looking over “saturated fat” on the NFP | Interested | 129 (16.8) | 32 (4.2) | 607 (79) |
| The interest of looking over “trans-fat” on the NFP | Interested | 96 (12.5) | 17 (2.2) | 655 (85.3) |
| The interest of looking over “cholesterol” on the NFP | Interested | 363 (47.3) | 151 (19.7) | 254 (33.1) |
| The interest of looking over “MUFA” on the NFP | Interested | 43 (5.6) | 13 ( 1.7) | 712 (92.7) |
| The interest of looking over “PUFA” on the NFP | Interested | 37 (4.8) | 11 (1.4) | 720 (93.8) |
| The interest of looking over “sodium” on the NFP | Interested | 301 (39.2) | 146 (19) | 321 (41.8) |
| The interest of looking over “vitamins” on the NFP | Interested | 498 (64.9) | 191 (24.9) | 78 (10.2) |
| The interest of looking over “minerals” on the NFP | Interested | 340 (44.3) | 181 (23.6) | 247 (32.2) |
| Practices | ||||
| Frequency of looking over nutrition labels | Always | 357 (46.5) | 411 (53.5) | - |
| Comparison between two food products based on the nutrition facts NFP panel of each | Compare | 271 (35.5) | 497 (64.7) | - |
| Looking over “calories” | Yes | 298 (38.9) | 315 (41) | 155 (20.2) |
| Looking over “carbohydrates” | Yes | 204 (26.6) | 306 (39.8) | 258 (33.6) |
| Looking over “total fats” | Yes | 283 (36.8) | 403 (52.2) | 82 (10.7) |
| Looking over “proteins” | Yes | 257 (33.5) | 403 (52.5) | 108 (14.1) |
| Looking over “saturated fats” | Yes | 88 (11.5) | 73 (9.5) | 607 (79) |
| Looking over “trans-fat” | Yes | 60 (7.8) | 53 (6.9) | 655 (85.3) |
| Looking over “cholesterol” | Yes | 203 (26.4) | 311 (40.5) | 254 (33.1) |
| Looking over “MUFA” | Yes | 23 (3) | 33 (4.3) | 712 (92.7) |
| Looking over “PUFA” | Yes | 22 (2.9) | 26 (3.4) | 720 (93.8) |
| Looking over “sugars” | Yes | 340 (44.3) | 416 (54.2) | 12 (1.6) |
| Looking over “fibers” | Yes | 192 (25) | 302 (39.3) | 274 (35.7) |
| Looking over “vitamins” | Yes | 252 (32.9) | 437 (57) | 78 (10.2) |
| Looking over “minerals” | Yes | 165 (21.5) | 356 (46.4) | 247 (32.7) |
| Looking over “sodium” | Yes | 159 (20.7) | 288 (37.5) | 321 (41.8) |
Accordingly, the understanding of nutrition labels was rated by grading an overall knowledge score for our study population, with a maximum possible score of 14. The mean ± SD knowledge score was 2.46 ± 1.93 (17.6%) for the overall population, 2.68 ± 2.07 for females, and 2.13 ± 2.68 for males, p=0.001 ( Table 4).
Table 4. Mean scores for the knowledge, attitudes, and practices (KAP) and the mean KAP for the overall population and by gender.
| Range of score | Overall mean ± SD | Overall mean (%) (b) | Females mean ± SD | Males mean ± SD | P-value | |
|---|---|---|---|---|---|---|
| Knowledge score | 0-14 | 2.46 ± 1.935 | 17.6% | 2.68 ± 2.071 | 2.13 ± 1.658 | 0.001 |
| Attitudes score | 0-16 | 6.24 ± 2.778 | 39% | 6.39 ± 2.834 | 6.01± 2.680 | 0.072 |
| Practices score | 0-16 | 5.76 ± 3.787 | 36% | 6.35 ± 3.982 | 4.89 ± 3.282 | <0.001 |
| Total KAP score (a) | 0-46 | 14.46 ± 7 | 31.4% | 15 ± 7 | 13 ± 6 | <0.001 |
Total KAP score is the sum of the knowledge, the attitude and the practice score.
Overall mean (%) is the product of the overall mean by hundred divided by the upper limit of each score, e.g., knowledge overall mean (%) = (2.46*100)/14 = 17.6%.
Attitudes towards nutrition labels
Participants’ responses to attitude questions are described in Table 3. We observed how our participants do perceive the beneficial use of the nutrition labels and their mandating. Also, we inquired about participants’ interests in looking over information related to calorie’s, macronutrients, and micronutrients on the nutrition facts panel. Study findings showed that the attitude of Lebanese shoppers towards nutrition facts in food product were mostly to check information related to sugars (66.4%), vitamins (64.9%), total fats (61.7%), proteins (59.1%), calories (58.7%), cholesterol (47.3%), fibers (46.6%), carbohydrates (44.7%) minerals (44.3%) among which most importantly sodium (39.2%). In contrast, they gave less consideration for information related to saturated fats (16.8%), trans-fat (12.5%), monounsaturated fatty acids (MUFA) (5.6%), and polyunsaturated fatty acids (PUFA) (4.8%).
Therefore, by responding to these questions, participants can optimally get an attitude score of 16. The mean ± SD attitude score was 6.24 ± 2.78 (39%) for the overall population, 6.39 ± 2.83 for females, and 6.01 ± 2.68 for males, p=0.072 ( Table 4).
Practices of nutrition labels use
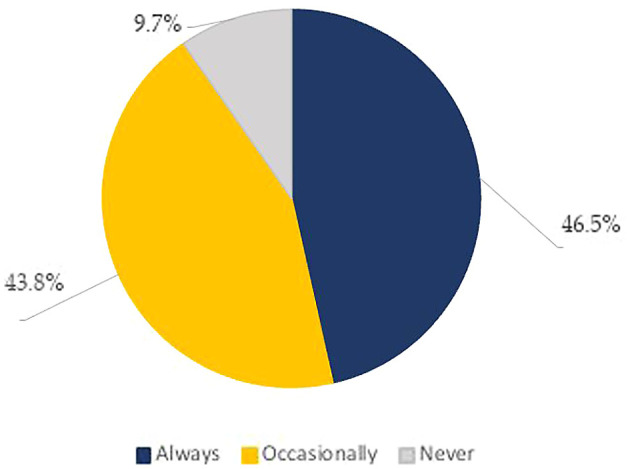
In practice, the top three information searched for when looking at the nutrition facts panel were: expiry date (75.2%), price (60.6%), and brand name (50.8%) ( Table 5). Whereas the least sought for information was: nutrition and health claims (24.8%), nutrition content (24.3%), food weight (13.6%), and presence of preparation and cooking instructions (9.4%) ( Table 5). Practice scores were based on 16 questions, including the frequency of checking nutrition labels, the act of comparing the nutrient content of food products, and looking at calories, macronutrients, and micronutrients on the food label. As for the frequency of checking the food label, about half of our sample population (46.5%) reported to “always” read the food label, whereas 43.8% of the respondents reported reading them occasionally and only 9.7% admitted not to read it at all ( Figure 2, Table 3). Besides this, when hesitating between two food products, the majority (64.7%) reported that they don’t refer to the NFP to base their choices ( Table 3).
Table 5. Considerations while reading food label.
| Considerations while reading food labels | N | % |
|---|---|---|
| Expiry date | 578 | 75.2 |
| Price | 466 | 60.6 |
| Brand name | 390 | 50.8 |
| Ingredients | 267 | 47 |
| Nutrition content | 187 | 24.3 |
| Country of origin | 257 | 33.5 |
| Food weight | 105 | 13.6 |
| Presence of preparation recipe | 72 | 9.4 |
| Presence of nutrition and health claims | 191 | 24.8 |
Figure 2. Frequency of looking at Food labels (% of participants).
In contrast to their attitudes towards the most searched information when looking at the NFP, in practice, Lebanese shoppers looked for the following nutrient information: sugars (44.3%), followed by calories (38.8%), total fats (36.8%), proteins (33.5%), and vitamins (32.9%). Others read labels related to saturated fats (11.5%), carbohydrates (26.6%), cholesterol (26.4%), fibers (25%), minerals (21.5%), sodium (20.7%), and trans-fats (7.8%). A minority were concerned to check information about monounsaturated fatty acids (MUFA) (3%), and polyunsaturated fatty acids (PUFA) (2.9%) ( Table 3).
Respectively, by responding to these questions, participants could get a maximum practice score of 16. The mean ± SD practice score was 5.76 ± 3.78 (36%) for the overall population, 6.35 ± 3.982 for females, and 4.89 ± 3.28 for males, p<0.001 ( Table 4).
Total KAP scores
The obtained knowledge, attitudes, and practices scores were summed up to determine the total KAP score. Subsequently, the respondent could get a maximum total KAP score of 46. Our findings showed a total KAP score with a mean ± SD of 14.46 ± 7 (31.4%) for the overall population, 15 ± 7 for females, and 13 ± 6 for males, p<0.001 ( Table 4).
Correlations between knowledge, attitudes, and practices scores
The Spearman’s coefficients (rho) are presented in Table 6. There was a positive correlation between knowledge and attitude scores (rho = 0.356, p<0.001). Similarly, the knowledge and practice scores were positively correlated (rho=0.38, p<0.001). Correlation findings revealed a strong positive association between attitudes and practices with a Spearman’s coefficient rho= 0.562, p<0.001. These findings demonstrate that knowledge, attitude, and practice scores increased simultaneously, and these scores were significantly correlated.
Table 6. Correlations between knowledge, attitudes, and practices scores: Spearman’s coefficients.
| Correlation coefficients (rho) | P-value | |
|---|---|---|
| Knowledge-attitude scores | 0.356 | <0.001 |
| Knowledge-practice scores | 0.380 | <0.001 |
| Attitude-practice scores | 0.562 | <0.001 |
Association of demographic, socioeconomic and health-related conditions with the KAP score based on univariate analysis
The KAP score was significantly lower for men (13 ± 6) than women (15 ± 7), p<0.001. Adults had higher scores when compared to youth (15 ± 7 vs. 14 ± 7, p=0.419). Although underweight, overweight, and obese participants had similar scores (14 ± 7), those with normal BMI had a higher mean score (15 ± 7), p<0.001. In addition, the KAP score was significantly lower for North Lebanon residents (13 ± 6, p<0.001). Further, medical sector workers had higher mean scores, as opposed to non-medical sector workers (18 ± 7 versus 14 ± 6, p=0.012). Participants earning the highest income (>3000$/month) had the highest mean score (19 ± 8), p=0.008. Non-married (15 ± 7) and childless (15 ± 7) respondents had better mean KAP scores, as opposed to their counterparts, p=0.068, and p=0.074, respectively ( Table 7).
Table 7. KAP score mean differences: Mann-Whitney U and Kruskal-Wallis tests.
| Variables | KAP score (mean ± SD) | P-value |
|---|---|---|
| Gender | ||
| Females | 15 ± 7 | <0.001 |
| Males | 13 ± 6 | |
| Age | ||
| Adults | 15 ± 7 | 0.419 |
| Youth | 14 ± 7 | |
| BMI | ||
| Underweight | 14 ± 7 | <0.001 |
| Normal | 15 ± 7 | |
| Overweight | 14 ± 7 | |
| Obese | 14 ± 7 | |
| Residency | ||
| Beirut | 17 ± 7 | <0.001 |
| North Lebanon | 13 ± 6 | |
| South Lebanon | 15 ± 7 | |
| Mount Lebanon | 14 ± 7 | |
| Employment profession | ||
| Medical sector | 18 ± 7 | 0.012 |
| Non-medical sector | 14 ± 6 | |
| Monthly wage | ||
| <1000$ | 13 ± 6 | 0.008 |
| 1000-2000$ | 15 ± 6 | |
| 2000-3000$ | 16 ± 8 | |
| >3000$ | 19 ± 8 | |
| Marital Status | ||
| Married | 14 ± 7 | 0.068 |
| Not-married | 15 ± 7 | |
| Children status | ||
| Have children | 14 ± 7 | 0.074 |
| Have no children | 15 ± 7 | |
| Education Level | ||
| Studying at university | 16 ± 7 | <0.001 |
| Low educational levels | 13 ± 6 | |
| University degree | ||
| Bachelor | 15 ± 7 | <0.001 |
| Master | 18 ± 9 | |
| Ph.D. | 22 ± 7 | |
| Diet status | ||
| On diet | 17 ± 8 | <0.001 |
| Not on diet | 13 ± 6 | |
| Physical activity status | ||
| Yes | 17 ± 7 | <0.001 |
| No | 14 ± 7 | |
| Medical conditions | ||
| Healthy | 15 ± 7 | 0.184 |
| Diseased | 14 ± 7 |
University students had a higher mean score of 16 ± 7 when compared to lower educational level students, p<0.001. Ph.D. degree holders (22 ± 7) had higher mean KAP scores than those holding Masters’ (18 ± 9) and Bachelors’ degrees (15 ± 7), p<0.001. Those who were restricted to specific diets (17 ± 8) and physically active participants (17 ± 7) had higher mean scores than their counterparts (p<0.001). Healthy respondents had a higher mean KAP score than diseased participants (15 ± 7 versus 14 ± 7, p=0.184; Table 7).
Predictors of the KAP score: The binary logistic regression
The KAP score was categorized into two levels: a low KAP (<23) and a high KAP (≥23). The descriptive analysis revealed that 15% of our overall study population had high KAP scores, and 85% scored low for KAP ( Figure 3). Based on these findings, we determined the risk factors contributing to having either a low or a high score by running a binary logistic regression test.
Figure 3. KAP classification.

Table 8 shows the binary regression analysis findings, with no adjustment. Males (versus females, OR=0.291, CI=0.159-0.321) were less likely to have a high KAP score by 71%, p<0.001. Adult participants were 1.2 times more likely to have a high KAP score, as opposed to young participants, (OR=1.21, CI=0.727-2.013, p=0.539). In addition, being overweight (OR=1.343, CI=0.349-5.171, versus underweight) and obese (OR=1.322, CI=0.32-5.453, versus underweight) increased the possibility of having a high KAP score by 1.3 times (p=0.668 and p=0.7, respectively). Regarding the residency area, North Lebanon residents had the lowest total KAP scores. In particular, North area residents (versus Beirut residents, OR=0.359, CI=0.161-0.804) were less likely to have high scores by 64.1%, p=0.013.
Table 8. Binary logistic regression findings, with no adjustment.
| Predictors of the KAP score (0: Low KAP 1: High KAP) | Odds ratio (OR) | 95% CI | P-value | |
|---|---|---|---|---|
| Lower | Higher | |||
| Gender | ||||
| Female (reference) | 1 | - | - | - |
| Male | 0.291 | 0.159 | 0.321 | <0.001 |
| Age | ||||
| Youth (reference) | 1 | - | - | - |
| Adults | 1.210 | 0.727 | 2.013 | 0.539 |
| BMI | ||||
| Underweight (reference) | 1 | - | - | - |
| Normal | 1.072 | 0.291 | 3.949 | 0.916 |
| Overweight | 1.343 | 0.349 | 5.171 | 0.668 |
| Obese | 1.322 | 0.320 | 5.453 | 0.700 |
| Residency | ||||
| Beirut (reference) | 1 | - | - | - |
| North Lebanon | 0.359 | 0.161 | 0.804 | 0.013 |
| South Lebanon | 0.716 | 0.327 | 1.569 | 0.404 |
| Mount Lebanon | 0.514 | 0.252 | 1.050 | 0.68 |
| Studying at University | ||||
| No (reference) | 1 | - | - | - |
| Yes | 2.040 | 1.126 | 3.696 | 0.019 |
| University degree | ||||
| Undergraduate (reference) | 1 | - | - | - |
| Postgraduate | 2.068 | 1.148 | 3.725 | 0.016 |
| Dieting | ||||
| No | 1 | - | - | - |
| Yes | 3.107 | 1.904 | 5.072 | <0.001 |
| Physical activity status | ||||
| No | 1 | - | - | - |
| Yes | 2.245 | 1.364 | 3.696 | 0.001 |
| Medical condition | ||||
| No | 1 | - | - | - |
| Yes | 0.790 | 0.480 | 1.302 | 0.355 |
In terms of the educational level, university students (versus lower education level students) were two times more likely to score acceptably (OR=2.04, CI=1.126-3.696), p=0.019. Although studying at university appeared to be a significant predictor, a higher university degree contributed more significantly to the KAP score prediction. Postgraduates had had a two-fold greater probability to have a high KAP score, as opposed to undergraduates (OR=2.068, CI=1.148-3.725), p=0.016.
Interestingly, our findings show that those who were restricted to specific diets (versus non-dieters, OR=3.107, CI=1.904-5.072) and those who were physically active (versus non-actives, OR=2.245, OR=1.364-3.696) were 3 and 2.2 times more likely to score acceptably, respectively (p<0.001). For the final predictor, i.e., the health condition, it was revealed that diseased participants (versus healthy) were less likely to obtain high score by 21% (OR=0.790, CI=0.480-1.302), p=0.355.
Discussion
This study assessed the KAPs related to the reading of nutrition labels among Lebanese people, using a validated questionnaire. Overall, the mean KAP score was low (14.46 ± 7, 31.4%) which might indicate a lack of public awareness of nutrition label use. In this study, the mean knowledge score was 2.46/14 points (17.6 over 100 points). Social media were the most used platforms (39.8%) to access nutrition information. However, a lower proportion (31%) accessed accurate and reliable nutrition facts from physicians, dietitians, and other specialists. Compared to other studied populations in previous investigations, our study participants were less knowledgeable about nutrition labeling with an apparent discrepancy in the observed knowledge scores. A previous study aiming to assess the relationship between knowledge and the use of nutrition information on food packages reported that Croatian participants had an average nutrition knowledge of 70% (70 over 100 points). 15 According to Koen et al., 2018, the knowledge scores of African participants was estimated around 44%. 16 As for Italy, a mean nutrition knowledge score of 46% was observed. 17 In Arabic countries, a recent observational study by Arfaoui et al., 2021 showed that adult Saudi adult consumers had a total knowledge score of 5.8/13 points (45%), and about 77% of the Saudi participants had an average knowledge score (50th-75th percentiles using the percentile threshold method). 18 Between December 2013 and February 2014, a cross-sectional study was conducted among 748 Lebanese shoppers. 19 In a previous study, Lebanese shoppers had an average food label knowledge score of 63.1%. 19 The massive gap between our obtained knowledge score (17.6%) and that observed in a previous year (63.1%), might be partly related to the study protocol, as we carried out an online survey, which might have affected the comprehension of the questions; however, in the previous study, shoppers were surveyed in supermarkets. Moreover, the latest economic crisis might have driven the interest of Lebanese shoppers into seeking price over quality. In particular, our respondents had low knowledge scores about the E-number additives (E200, E700 …). E-numbers are the chemical names of certain food additives, and they appeared to have a bad reputation among consumers. 20 Products containing food additives are usually perceived as unhealthier products. 20 A study was conducted to compare E-number labels with “clean” labels, and showed that consumers find “clean” label ingredient lists the safest, healthiest, and the easiest to read. 20 Concerning the ability to interpret nutrition symbols on food labels, especially the vegetarian and vegan symbols, only 2.3% and 4.2% (respectively of our sample were able to do it. A study by Berich, H. (2015) done among Kent State University students found that vegetarian dieters were more familiar with such symbols. 21 It should be noted that only 1.8% of our participants were on a vegetarian/vegan diet, explaining the unfamiliarity with their corresponding food symbols. The “GMO” symbols corresponding to food containing genetically modified organisms were also unfamiliar for the majority (92.8%) of our respondents. Foods that contain genetically modified organisms was introduced to the US market and appeared on supermarket shelves in 1994. 22 Comparing Lebanon to other countries, a cross-cultural survey assessing the knowledge of consumers in the US, Japan, and Italy showed that US consumers were more familiar with GMOs (40.9%) compared with Italian (28.0%) and Japanese (33.3%) consumers. 22 Similarly, only 15% of our participants were familiar with the “gluten-free” food symbol. This finding is unsurprising, as only a few of our study population reported following a gluten-free diet. In addition, another important explanation is that we exposed our participants to the “crossed grain gluten-free” symbol, and not to worded gluten-free claims on packages. In Poland, an eye-tracking study of gluten-free cookies showed that consumers were more uncertain about the crossed grain symbol, as compared to verbal statements and gluten-free claims. 23 In contrast, about half of our sampled population agreed that “sugar-free”-labeled products are artificially sweetened. However, they had little idea about the artificial additives which act as sugar substitutes: 75.6% of the overall responders were not familiar with the role of xylitol, sorbitol, and aspartame sweeteners. In a different setting, a qualitative study exploring consumer knowledge and understanding of added sugars in the United Kingdom demonstrated that saccharin and aspartame sweeteners were correctly classified by the majority (60% and 80%, respectively) of respondents. 24 Sweeteners have been used to increase food flavor and were adopted because they contain few to no calories compared to the high caloric content of sugars. 25 Also, an important proportion of our respondents (40.4%) were aware of the laxative effect of these sweeteners. We can assume this is due to having had previous experiences with this side effect after consuming any sugar-free product. As to MSG, the majority (93.2%) of our sample population did not know whether MSG has blood pressure-elevation effects. A nutrition study on Chinese adults observed that MSG intake was associated with a significant increase in blood pressure levels, especially among patients chronically taking antihypertensive medications. 26 A previous study aimed to assess the KAP towards the use of MSG in Pakistan explored that 98.3% of the respondents were using MSGs as food flavor enhancers while cooking stews, soups, pottages, sauce, and others (6.6 g/person/week). 27 Contrarily to our findings, 42.5% of the Pakistani consumers had high knowledge levels about MSG. 27 Regarding hydrogenated vegetable oils, 42% of Lebanese shoppers in our study agreed that they caused detrimental health side effects. In Saudi Arabia, a study was conducted to assess the trans-fat-related knowledge among Saudis; its results showed that around 35.1% of the participants were familiar with the term “hydrogenated oils”, and only 4% classified these ingredients as unhealthy. 28 Even though Lebanese shoppers showed high knowledge regarding hydrogenated oils’ health impacts, practice results differed when a cross-sectional survey was conducted on 657 Lebanese adults who completed the US National Institute of Health diet history questionnaire. 29 This study found that the mean trans-fatty acids consumption among Lebanese people was double the World Health Organization (WHO) recommendations of 1 percent of total daily energy. 29 Partially hydrogenated oils have been found to contain extremely harmful fatty acids, and they cause inflammation and calcification of the arterial cells, increasing the risk of coronary heart disease (CHD). 30 When we asked our participants to calculate the energy density of a sweetened condensed milk, the majority either gave a wrong answer or failed to do any calculation (74.4%). Similarly, several studies reported a low understanding of serving size labeling among consumers. 31 A study done by Persoskie et al., 2017, showed that Americans could not determine the calorie content of a full ice-cream container. 32 Additionally, 21% could not estimate the number of servings equal to 60 g of carbohydrates, 42% could not estimate the effect on the daily calorie intake of one serving, and 41% failed to calculate the percentage daily value (DV) of calories in a single serving. 32 The mean attitude and practice scores for our population were 6.24 ± 2.778 (over 16) and 5.76 ± 3.787 (over 16), respectively. Our findings have shown that the knowledge, attitude, and practice scores were positively correlated. It is known that the better the knowledge, the better the attitudes will be, and thus, more appropriate practices will take place. 33 Although knowledge itself does not necessarily guarantee a behavior change, it shapes the attitudes towards favorable practices. 33 Considering this, our research findings highlight the importance of educating Lebanese shoppers on food labels to ease their interpretation, and this, in turn, may enhance attitudes and practices in the long term. A clear evidence-based front-of-pack label like the nutri-score could be an effective tool to help improve consumers’ diet quality and mitigate the risk of NCDs. 34 The Nutri-Score is a front-of-pack label that provides user-friendly information on the nutritional quality of food products. 34 It is based on the British Food Standards Agency nutrient profiling system (FSAm-NPS) score. 34 The higher the FSAm-NPS score, the lower the nutritional quality of the food. Nutri-score is a rating system that uses five different colours to categorize food products into five groups. 34 For example, category A (dark green) suggests higher nutritional quality; however, category E (dark orange) indicates lower nutritional quality. 34 The nutri-score is the only front-of-pack nutrition label in Europe having some strong scientific evidence for its effectiveness. 34 It has already been adopted by several European countries (Belgium, France, Germany, the Netherlands, Spain, Luxembourg and Switzerland). 34 Regarding the observed attitudes, the majority of our participants (72.5%) supported the beneficial use of the NFP. Furthermore, our participants seemed to positively perceive the nutrition labels’ importance, in contrast with a previous cross-sectional study recruiting 748 supermarket Lebanese shoppers in 2014. 19 Less than half (44.4%) of the recruited shoppers agreed that reading food labels is very important. 19 Besides, our findings are consistent with previous investigations from a cross-sectional study recruiting Iranian students from five different academic majors (including Nutrition, Public Health, Health Services Administration, Paramedical, and Engineering). 35 Among 332 students, 89.2% believed that food labels affect nutritional awareness, and 77.4% agreed with their beneficial use. 35 Similarly, a US survey aiming to examine the influence of 1990 Nutrition Labeling and Education Act food labels on college students found that 95% of participants perceived the NFP to be useful. 36 Moreover, consumers were more concerned about reading nutritional information when they planned to lose weight or follow specific dietary regimens. 36 Further, it was mentioned that 81% of participants who read the nutritional panel on product labels were on a weight-loss diet. 37 This supports our results, since 55.2% of our sample were dieters, which explains their positive attitudes towards nutrition label use. In addition, our study findings showed that female participants had higher mean attitude scores than males (6.39 ± 2.834 vs. 6.01 ± 2.680, p=0.072). This is because women experience more food-related conflict, and more dissatisfaction with their body weight and shape than men do. 38 With regards to nutrition labels mandating, the majority (89.5%) discerned the necessity of such legal actions. In addition to transparency, nutrition facts on food products enable people to determine, choose, and meet their dietary needs. 39 The FDA provides effective guidance to the food industry regarding labeling information, depending on the product type. 39 In an attempt to assess consumers’ valuation of nutrition labels, data was collected from food shoppers to observe their willingness to pay a premium cost for a box of cookies with a nutritional label. 40 Interestingly, that study found that the mean willingness to pay for a box of cookies with a nutritional label was about 11%higher than that of a cookie box without a nutritional label. 40 Moreover, expiry date marking (75.2%), price (60.6%), and brand name (50.8%) were the prioritized considerations for of our sample, whereas a smaller proportion admitted considering food ingredients (47%), and nutritional content (24.3%). Similar to our findings, the majority (84.7%) of the shoppers in Tabriz, Iran have been found to look for the expiry and production dates on the food label. 41 In addition, 51.6% were looking at food price, and only 8.7% of the participants read food labels to find information about the food additives and artificial colors. 41 Further, the date of minimum durability (i.e. best-before or use-by date) was rated the most important piece of mandatory labelling information, with 81% of Irish consumers scoring it as very important. 42 Our respondents ranking the food price as a priority consideration was a predictable finding: at the time of our data collection, Lebanon was in a financial crisis, and more than half the population lived below the poverty line. According to the latest data in July 2021, a family's budget for food was around five times the minimum monthly wage. 43 In contrast, a survey examining the awareness of food labeling among consumers in groceries in Al-Ain, United Arab Emirates reported that consumer’s responses showed general tendencies for reading the food label (89.5%); however; they read basic information related to production and expiry dates. 44 Another study in India showed that the taste, quality, convenience and ease of use were the main reasons for purchasing food among the study participants. 45 The majority (81%) looked for the expiry date, and only one third purchased food based on its nutritional value. 45 Moving to South Africa (Lesotho), an observational study reported that 40.5% of the participants were interested in reading the nutrition information on food labels, rather than facts related to price, taste, appearance, habit, convenience, or brand name. 46 When asked about the frequency at which they read nutrition labels, about half of our responders (46.5%) reported to “always” read the food labels. These findings are considered reasonable when compared to other studies in Arabic countries and worldwide and comparable to that reported among Bahraini consumers for which 42% of them reported reading the food label. 47 A research survey showed that only 27.4% of Saudi female college students stated that they always read food labels when purchasing food products. 48 In China, however, 59.2% of a survey respondents indicated to “sometimes” look at the label, and only 28.7%” always” read nutrition label. 49 Besides, only 21.6% of university Malaysian students reported to “often” use the food label during food purchasing decisions. 50 To specify, our responders claimed to read labels relating primarily to sugars (44.3%), followed by calories (38.9%), total fats (36.8%), proteins (33.5%), and vitamins (32.9%). These findings are supported by that reported in Bahrain, with the majority of shoppers reported that the amount of fat and sugar was the most important piece of information to be checked when buying a food product for the first time. 47 Chinese people had similar reading practices, and were found to look at proteins (51.5%), vitamins (49.8%), and fats (29.4%). 49 A preliminary review aimed at assessing the types of label formats that could influence the use of nutritional label among consumers showed that the majority of label users were interested in checking information related to calories, fat, sodium, and cholesterol, and in deciding whether to buy fresh fluid milk. 51 Most importantly, the majority (64.7%) of our responders reported that they did not refer to the NFP to choose between two food products. These results are not unusual in Lebanon: only 22.9% of recruited Lebanese shoppers admitted to checking the food labels every time they bought a food product. 19 On the other hand, 65% of Ghanaian consumers read food labels before purchase, and 75% based their food selection according to its nutrition content. 52 Besides, more than half of Singhalese people recruited in a cross-sectional survey could select the healthiest option with the better food label, when hesitating between two snack options. 53 Interestingly, a study in Kenya revealed that consumers found some difficulties while reading food labels, including the technical language used, small font size when reading a food label, unfamiliar language, and incomplete labeling information. 54 Consistent findings were obtained from our univariate analysis and binary regression analysis regarding the mean KAP score. Our findings revealed that female (15 ± 7), adult (15 ± 7), healthy (15 ± 7), and overweight/obese participants (14 ± 7) were more likely to have a high KAP score. In addition, those with higher educational levels (university level), and those who had completed higher university studies (Master, Ph.D.) had higher KAP scores. Other interesting findings are that those who were restricted to certain diets and the physically active participants had better KAP scores than their counterparts. On the other hand, North Lebanon residents had a lower KAP score (13 ± 6), as opposed to other residency areas. Supporting our findings, a sex-specific analysis of nutrition label use in the US showed that females used nutrition labels more than males (40.7% versus 54.3%, p<0.001). 55 Similarly, another study in Malaysia reported that females, adults, tertiary level-educated, and physically active participants had increased odds of nutrition label use. 56 Also, Libyan respondents who had university degree or equivalent of it expressed better awareness on food labeling. 57 The same study showed that participants who had no health problems had better reading practices for the nutrition labels than diseased respondents, coming in confirmation with the findings of the present study. 57 Going back to the cognitive processing model, it revealed that some complex tasks related to reading food labels demand high comprehension and interpretation skills. 10 Thus, this model explains why a higher educational level was a significant predictor of better KAP in our study findings. 10 In addition, knowing more about food labels and consulting them before food purchase can help dieters and those who care about their body shape to pick healthy food options. 58 Upon this, having better knowledge about nutrition labels can protect from many NCDs, which explains why our healthy responders had higher KAP scores than diseased participants. This study has identified the KAP scores and the associated factors of KAP related to nutrition label use among the Lebanese public. The findings of this study might advocate for future educational programs clarifying the meaning of crucial nutrition claims and symbols. Although increasing consumers’ awareness is key in leading to better KAP, food manufacturers should also invest in simplifying their nutrition labels presentation to attract more consumers. As discussed before, concerning the nutri-score’s promising application, epidemiological findings among European cohorts found that people who consume more food with higher FSAm-NPS scores (lower nutritional quality) had a higher risk of developing cancers, and a 6% increase in the risk of overall mortality. 59 In France, seven out of 10 people check the Nutri-Score, and 84% say they are very likely to pick food products with higher scores. 60 Besides, a cross-sectional study recruiting 501,594 adults from ten European countries mentioned that a FSAm-NPS score was calculated for each participant based on the nutritional quality of the food they consume. 61 Individuals with a higher score revealed an increased risk of all-cause mortality as well as the incidence of circulatory and gastrointestinal diseases. 61
Limitations and strengths
Our study includes some limitations. Firstly, the cross-sectional design of the survey itself limited the ability to reach causal inference. In addition, the online distribution of the questionnaire in the second period of the study (after COVID-19 pandemic emergence) may pose information and selection biases. Thus, the self-reported data may overestimate the understanding, the positive attitudes, and the appropriate practices regarding nutrition label use. On the other hand, this study has critical strengths. It is the first study in Lebanon adopting a valid and reliable questionnaire to assess the knowledge, attitudes, and practices of Lebanese consumers regarding nutrition label use. Besides, responders were recruited from different areas, had different educational levels, and were of various ages so that the study’s findings could be generalized to the whole population.
Conclusion
The low awareness of nutrition labels leads Lebanese people to choose unhealthy food options. This study showed an association between the participants’ attitudes, practices and self-reported knowledge. Because nutrition and chronic diseases are interrelated, a planned educational program is recommended to help Lebanese people pick healthy options mindfully. It is necessary to establish educational campaigns about the association between reading nutrition labels and health outcomes. The Food and Drug Administration (FDA) has implemented a “Read the Label” campaign to support children, families, and community leaders in analyzing nutrition labels and to use them effectively. In conclusion, advocating for a nutrition rating system like Nutri-Score in Lebanon is fundamental to mitigate obesity and chronic disease burden. However, one should take into account that nutrition labeling is only one approach to a public health nutrition policy, and it should be complementary with other public health measures and, in particular, nutrition education and communication.
Data availability
OSF: Assessment of the Knowledge, attitudes and practices (KAP) of Lebanese shoppers towards food labeling: The first steps in the Nutri-score roadmap, https://osf.io/3nh5 62
This project contains the following underlying data:
-
•
Data-Excel-Nutrition Label.xlsx
Data are available under the terms of the Creative Commons Zero “No rights reserved” data waiver (CC0 1.0 Public domain dedication).
Funding Statement
The author(s) declared that no grants were involved in supporting this work.
[version 2; peer review: 2 approved]
References
- 1. World Health Organization: Non communicable Diseases. 2021. October 16, 2021. Reference Source
- 2. World Health Organization, Regional Office of East Mediterranean: Regional data on non-communicable diseases risk factors. 2016. Reference Source
- 3. World Health Organization: Lebanon 2016 total population: 2016 total deaths. 2016. Reference Source
- 4. Ministry of Public Health Republic of Lebanon: Non-Communicable Diseases Prevention and Control Plan (NCD-PCP) 2016-2020. 2016. Reference Source
- 5. Branca F, Lartey A, Oenema S, et al. : Transforming the food system to fight non-communicable diseases. BMJ 2019;364:l296. 10.1136/bmj.l296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Talati Z, Norman R, Pettigrew S, et al. : The impact of interpretive and reductive front-of-pack labels on Food Choice and willingness to pay. International Journal of Behavioral Nutrition and Physical Activity 2017;14(1):171. 10.1186/s12966-017-0628-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Center for Food Safety and Applied Nutrition: The New Nutrition Facts Label U.S. Food and Drug Administration;2020. November 4, 2021. Reference Source [Google Scholar]
- 8. SGS Société Générale de Surveillance SA: New EU Food Labelling Requirements. 2014. November 4, 2021. Reference Source
- 9. Ministry of Economy and Trade: An ABC Guide on EU Food Packaging and Labelling Requirements. 2008. November 4, 2021. Reference Source
- 10. Miller LM, Cassady DL: The effects of nutrition knowledge on food label use. A review of the literature. Appetite 2015;92:207–216. 10.1016/j.appet.2015.05.029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Grunert KG, Wills JM, Fernández-Celemín L: Nutrition knowledge, and use and understanding of nutrition information on food labels among consumers in the UK. Appetite 2010;55(2):177–189. 10.1016/j.appet.2010.05.045 [DOI] [PubMed] [Google Scholar]
- 12. Nurliyana G, Norazmir MN, Khairil MI: Knowledge, attitude and practices of university students regarding the use of nutritional information and food labels. Asian Journal of Clinical Nutrition 2011;3(3):79–91. 10.3923/ajcn.2011.79.91.1 [DOI] [Google Scholar]
- 13. Lin C-TJ: How do consumers interpret health messages on food labels? Nutrition Today 2008;43(6):267–272. 10.1097/01.nt.0000342701.19798.25 [DOI] [Google Scholar]
- 14. Wojcicki JM, Heyman MB: Adolescent nutritional awareness and use of food labels: Results from the National Nutrition Health and Examination Survey. BMC Pediatrics 2012;12(1). 10.1186/1471-2431-12-55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kresic G, Mrduljas N: The relationship between knowledge and the use of nutrition information on food package. 2016. November 6, 2021. Reference Source
- 16. Koen N, Wentzel-Viljoen E, Nel D, et al. : Consumer knowledge and use of food and nutrition labelling in South Africa: A cross-sectional descriptive study. International Journal of Consumer Studies 2018;42(3):335–346. 10.1111/ijcs.12422 [DOI] [Google Scholar]
- 17. Scalvedi ML, Gennaro L, Saba A, et al. : Relationship between nutrition knowledge and dietary intake: An assessment among a sample of Italian adults. Frontiers in Nutrition 2021;8. 10.3389/fnut.2021.714493 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Arfaoui L, Alkhaldy A, Alareeshi A, et al. : Assessment of knowledge and self-reported use of Nutrition Facts label: JMDH. Journal of Multidisciplinary Healthcare 2021;14:2959–2972. October 25, 2021. 10.2147/JMDH.S327700 Reference Source [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hassan HF, Dimassi H: Usage and understanding of food labels among Lebanese shoppers. International Journal of Consumer Studies 2017;41(5):570–575. 10.1111/ijcs.12368 [DOI] [Google Scholar]
- 20. Meijer A: Comparing clean labels versus labels including E-numbers from a consumer perspective. Master Thesis. 2020. October 17, 2021. Reference Source
- 21. Berish HM: Knowledge and perceptions of vegetarian diets among college-aged students. Thesis. 2015. October 17, 2021. Reference Source
- 22. Schouteten JJ, Gellynck X, De Steur H: Consumers’ perceptions of GM-free labelled foods: A sensory experiment. International Journal of Consumer Studies 2018;42(3):347–357. 10.1111/ijcs.12424 [DOI] [Google Scholar]
- 23. Sielicka-Różyńska M, Jerzyk E, Gluza N: Consumer perception of packaging: An Eye-Tracking Study of gluten-Free Cookies. International Journal of Consumer Studies 2020;45(1):14–27. 10.1111/ijcs.12600 [DOI] [Google Scholar]
- 24. Tierney M, Gallagher A, Giotis E, et al. : An online survey on consumer knowledge and understanding of added sugars. Nutrients 2017;9(1):37. 10.3390/nu9010037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Saraiva A, Carrascosa C, Raheem D, et al. : Natural sweeteners: The relevance of food naturalness for consumers, food security aspects, sustainability and health impacts. International Journal of Environmental Research and Public Health 2020;17(17):6285. 10.3390/ijerph17176285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Shi Z, Yuan B, Taylor AW, et al. : Monosodium glutamate is related to a higher increase in blood pressure over 5 years: Findings from the Jiangsu Nutrition Study of Chinese adults. Journal of Hypertension 2011;29(5):846–853. 10.1097/hjh.0b013e328344da8e [DOI] [PubMed] [Google Scholar]
- 27. Henry-Unae HN: Consumer knowledge, attitude and practice towards the use of monosodium glutamate and food grade bullion cubes as dietary constituents. Pakistan Journal of Nutrition 2009;9(1):76–80. 10.3923/pjn.2010.76.80 [DOI] [Google Scholar]
- 28. Kamel S: Trans-Fats Declaration, Awareness and Consumption in Saudi Arabia. Current Research in Nutrition and Food Science 2018;6(3):748–756. 10.12944/CRNFSJ.6.3.17.4 [DOI] [Google Scholar]
- 29. Farhat AG, Jaalouk D, Moukarzel SR, et al. : Consumption of trans fatty acid and omega 6 to omega 3 ratio in Lebanese adults. Nutrition & Food Science 2016;46(1):120–129. 10.1108/nfs-07-2015-0089 [DOI] [Google Scholar]
- 30. Kummerow FA: The negative effects of hydrogenated trans fats and what to do about them. Atherosclerosis 2009;205(2):458–465. 10.1016/j.atherosclerosis.2009.03.009 [DOI] [PubMed] [Google Scholar]
- 31. Bucher T, Duncanson K, Murawski B, Van der Horst K, et al. : Consumer understanding, perception and interpretation of serving size information on food labels: A scoping review. 2018. 10.20944/preprints201801.0212.v1 [DOI] [PMC free article] [PubMed]
- 32. Persoskie A, Hennessy E, Nelson WL: US consumers’ understanding of nutrition labels in 2013: The Importance of Health Literacy. Preventing Chronic Disease 2017;14:E86. 10.5888/pcd14.170066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Karuniawati H, Hassali MA, Suryawati S, et al. : Assessment of knowledge, attitude, and practice of antibiotic use among the population of Boyolali, Indonesia: A cross-sectional study. International Journal of Environmental Research and Public Health 2021;18(16):8258. 10.3390/ijerph18168258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. World Health Organization. International Agency for Research on Cancer: The nutri-score: A science-based front-of-pack nutrition label. 2021. November 5, 2021. Reference Source
- 35. Mahdavi AM, Abdolahi P, Mahdavi R: Knowledge, Attitude and Practice between Medical and Non-Medical Sciences Students about Food Labeling. Health Promotion Perspectives 2012;2(2):173–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Marietta A, Welshimer K, Anderson S: Knowledge, attitudes, and behaviors of college students regarding the 1990 nutrition labeling education act food labels. Journal of the American Dietetic Association 1999;99(4):445–449. 10.1016/s0002-8223(99)00108-x [DOI] [PubMed] [Google Scholar]
- 37. Group, T. H: Nutrition 101: Consumers actually do read product labels. Forbes. 2016, July 20. October 17, 2021. Reference Source [Google Scholar]
- 38. Rolls BJ, Fedoroff IC, Guthrie JF: Gender differences in eating behavior and body weight regulation. Health Psychology 1991;10(2):133–142. 10.1037/0278-6133.10.2.133 [DOI] [PubMed] [Google Scholar]
- 39. Team, M. S: The benefits of labeling: Featuring you’re off the shelf food products and Nutrition Facts. MenUSno;2021, August 26. October 17, 2021. Reference Source [Google Scholar]
- 40. Loureiro ML, Gracia A, Nayga RM: Do consumers value nutritional labels? OUP Academic;2006, June 1. January 5, 2022. Reference Source [Google Scholar]
- 41. Pourmoradian S, Kermanshahi M, Chaeipeima M, et al. : Consumers' knowledge, attitude, and practice regarding front-of-package (FOP) labels at the point of Purchase. 2020. 10.21203/rs.3.rs-129608/v1 [DOI]
- 42. Food Safety Authority of Ireland: A research study into consumers’ attitudes to food labeling. 2009. October 19, 2021. Reference Source
- 43. Al Arabiya English: Lebanon families spend 'five times minimum wage' on food alone: Study Al Arabiya English;2021. October 19, 2021. Reference Source [Google Scholar]
- 44. Washi S: Awareness of Food Labeling among Consumers in Groceries in Al-Ain, United Arab Emirates. International Journal of Marketing Studies 2012;4(1). 10.5539/ijms.v4n1p38 [DOI] [Google Scholar]
- 45. Vemula SR, Gavaravarapu SM, Mendu VV, et al. : Use of food label information by urban consumers in India – a study among supermarket shoppers. Public Health Nutrition 2013;17(9):2104–2114. 10.1017/s1368980013002231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Mahgoub S, Lesoli PP, Gobotswang K: Awareness and use of nutrition information on food packages among consumers in Maseru (Lesotho). African Journal of Food, Agriculture, Nutrition and Development 2007;07(06):001–016. 10.18697/ajfand.17.2585 [DOI] [Google Scholar]
- 47. Wahab RA: Food Label Use and Awareness of Nutritional Information Among Consumers in Bahrain: An Exploratory Study. KnE Life Sciences [Internet]. 2018 Oct 15 [cited 2022 Mar 24];4(6):26. 10.18502/kls.v4i6.3088 [DOI] [Google Scholar]
- 48. Al-Barqi R, Al-Salem Y, Mahrous L, et al. : Understanding barriers towards the use of food labels among Saudi Female College Students. Malaysian Journal of Nutrition 2020;26(1):019–030. 10.31246/mjn-2019-0117 [DOI] [Google Scholar]
- 49. Barreiro-Hurle J, Gracia A, De-Magistris T: The effects of multiple health and nutrition labels on Consumer Food Choices. Journal of Agricultural Economics 2010;61(2):426–443. 10.1111/j.1477-9552.2010.00247.x [DOI] [Google Scholar]
- 50. Nurliyana G, Norazmir MN, Khairil an MI: Knowledge, attitude and practices of university students regarding the use of nutritional information and food labels. Asian Journal of Clinical Nutrition 2011;3(3):79–91. 10.3923/ajcn.2011.79.91 [DOI] [Google Scholar]
- 51. Azman N, Sahak SZ: Nutritional label and consumer buying decision: A preliminary review. Procedia - Social and Behavioral Sciences 2014;130:490–498. 10.1016/j.sbspro.2014.04.057 [DOI] [Google Scholar]
- 52. Darkwa S: Knowledge of Nutrition Facts on food labels and their impact on food choices on consumers in Koforidua, Ghana: A case study. South African Journal of Clinical Nutrition 2014;27(1):13–17. 10.1080/16070658.2014.11734479 [DOI] [Google Scholar]
- 53. Talagala IA, Arambepola C: Use of food labels by adolescents to make healthier choices on snacks: A cross-sectional study from Sri Lanka. BMC Public Health 2016;16(1):739. 10.1186/s12889-016-3422-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Liuzzo G, Rolandi S, Serraino A, et al. : Pre-packaged food products Business to Consumer (B2C) distance selling and information obligations in Italian mass market retailers. Italian Journal of Food Safety [Internet]. 2019 Oct 1 [cited 2022 Mar 24];8(3). 10.4081/ijfs.2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Su D, Zhou J, Jackson HL, et al. : A sex-specific analysis of Nutrition Label Use and Health, Douglas County, Nebraska, 2013. Preventing Chronic Disease 2015;12:E158. 10.5888/pcd12.150167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Cheah YK, Moy FM, Loh DA: Socio-demographic and lifestyle factors associated with nutrition label use among Malaysian adults. British Food Journal 2015;117(11):2777–2787. 10.1108/bfj-01-2015-0001 [DOI] [Google Scholar]
- 57. Alshukri A, Elramli S, Albkoush H: Study of knowledge, attitude and awareness of the information of food labeling among consumers in Tripoli municipality Libya. 2020. Retrieved March 24, 2022. Reference Source [Google Scholar]
- 58. Mayo Foundation for Medical Education and Research: Decoding the New Nutrition Facts Label. Mayo Clinic;2019, July 20. October 25, 2021. Reference Source [Google Scholar]
- 59. Southey F: Nutri-score for cancer prevention: IARC backs EU-wide roll out of Nutrition Labelling Scheme. 2021. November 5, 2021. Reference Source Reference Source
- 60. Tate & Lyle: What is nutri-score and why should food and drink manufacturers work towards better ratings. 2020. November 5, 2021. Reference Source
- 61. Deschasaux M, Huybrechts I, Julia C, et al. : Association between nutritional profiles of foods underlying nutri-score front-of-pack labels and mortality: Epic cohort study in 10 European countries. BMJ 2020;370. 10.1136/bmj.m3173 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Hoteit M: Assessment of the Knowledge, attitudes and practices (KAP) of Lebanese shoppers towards food labeling: The first steps in the Nutri-score roadmap. 2022, January 4. 10.17605/OSF.IO/3NH5F [DOI] [PMC free article] [PubMed]