

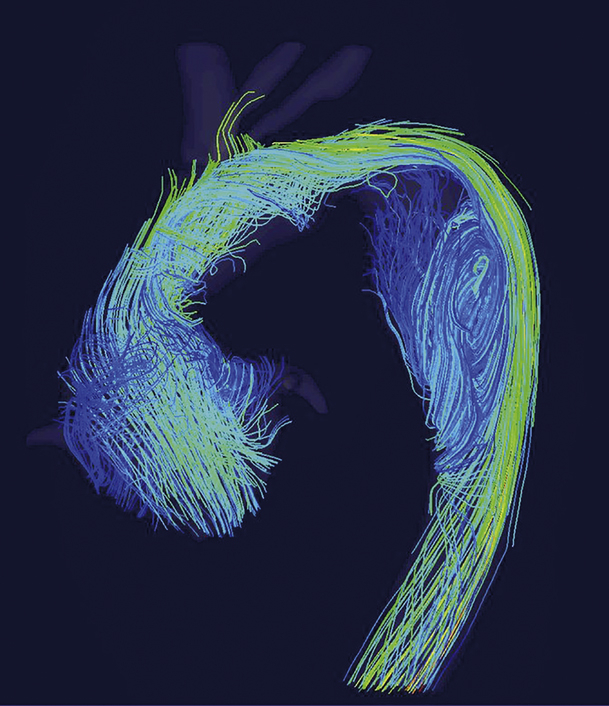
4D-flow MRI shows a vortex flow in the descending aorta, compressing the elephant trunk.
Central Message.
Dynamic obstruction of the elephant trunk may be caused by a vortex flow in the dilated proximal descending aorta outside of the trunk.
See Commentary on page 25.
Mechanical obstruction caused by kinking has been recognized as a complication of the elephant trunk (ET).1,2 We report a case of dynamic obstruction, in which a vortex flow outside of ET in the dilated proximal descending aorta compressed the trunk. This mechanism was confirmed by a 4-dimensional flow magnetic resonance imaging (MRI).
Case Report
A 48-year-old man was hospitalized for fatigue and dyspnea during less-than-ordinary activity. Blood pressure was 97/41 mm Hg. Echocardiography revealed severe aortic regurgitation (AR) with annuloaortic ectasia (50 mm). The left ventricular diastolic dimension (LVDd) was 72 mm, and left ventricular systolic dimension (LVDs) was 67 mm. The diagnosis of heart failure was made.
The patient had undergone supracoronary and total arch replacement (a 24-mm quadrifurcated graft) with an ET (18 mm in diameter, 70 mm in length) for acute type A aortic dissection 16 years ago, and percutaneous coronary intervention for left anterior descending 4 years ago with restenosis. He had no family history and no syndromes suggesting familial thoracic aortic aneurysm/dissection. At the index operation, aortic root diameter was 38 mm, and no AR was present. The descending aorta showed complete remodeling postoperatively, resulting in reduction of aortic diameter from 43 mm and true lumen expansion to 36 mm within the first 2 years. Annual follow-up by computed tomography (CT) revealed progressive dilatation of the aortic root but only mild dilatation (+2 mm) of the descending aorta thereafter (Figure 1). Moderate AR was first noted 4 years ago, and LVDd exceeded 60 mm and ejection fraction became less than 50% 1 year ago.
Figure 1.

Computed tomography scans 6 months (left), 5 years (middle), and 16 years (right) after initial operation. Solid arrow: distal anastomosis, arrowhead: elephant trunk.
CT after hospitalization showed flattening of the ET (Figure 2), which had been present since mild AR first appeared 6 years ago. Cardiac catheterization revealed pulmonary hypertension (56/27 mm Hg), high wedge pressure (24 mm Hg), low cardiac output (2.3 L/ min/m2), and systolic pressure gradient between the ascending aorta and descending aorta (42 mm Hg). Four-dimensional flow MRI showed a vortex flow in the dilated proximal descending aorta outside of ET, which flowed upward along the ventral aortic wall and turned around at the proximal blind end, compressing the ET to the greater curvature of aortic arch (Figure 2, Video 1). To relieve the pressure gradient and reduce the left ventricular afterload before the Bentall operation, we performed thoracic endovascular aortic repair (TEVAR) first.
Figure 2.

Multiplanar reconstruction of computed tomography scans 5 years after index operation (left), before thoracic endovascular aortic repair (middle left), and after TEVAR and Bentall operation (right), and 4-dimsneional flow magnetic resonance imaging before thoracic endovascular aortic repair (middle right). Elephant trunk flattening was not present 5 years after the index operation. A vortex flow was present in the proximal descending aorta outside of the elephant trunk, compressing the trunk to the greater curvature of aortic arch. Broken arrow: proximal anastomosis, solid arrow: distal anastomosis, arrowhead: elephant trunk. TEVAR, Thoracic endovascular aortic repair.
TEVAR was performed via a femoral artery using the wire pull-through technique. A 31-mm conformable TAG device 15 cm in length (W. L. Gore & Associates, Flagstaff, Ariz) was deployed from the aortic arch graft to the seventh vertebral level. The pressure gradient disappeared after deployment. Together with the optimal medical therapy, LVDd was reduced to 61 mm and LVDs to 44 mm 4 weeks after TEVAR. Bentall operation with coronary artery bypass grafting to left anterior descending was successfully performed. Seventeen months later, echocardiography revealed further improvement of the left ventricular function; LVDd 57 mm, LVDs 38 mm.
The patient provided written informed consent.
Discussion
Pressure gradient across the ET may develop when its diameter is too small or when mechanical obstruction is present. In the present case, although the diameter of ET was 18 mm, the size itself was not likely to be a cause, since the pressure gradient disappeared after TEVAR. There was no mechanical obstruction. Due to true lumen expansion caused by obliteration of the thoracic false lumen, there was a size mismatch between the native aorta and ET. This mismatch, together with the curvature of aortic arch, seemed to form the basis for dynamic obstruction. AR due to progressive root dilatation seemed to have played a pivotal role in the development of dynamic obstruction, possibly through retrograde diastolic aortic flow, since the appearance of ET flattening coincided with progression of AR. The fact that ET was already flattened 6 years ago suggests that primary cause of heart failure was AR, and pressure gradient across the ET was an exacerbating factor. TEVAR was effective to relieve the dynamic obstruction, suggesting that such a complication could be avoided when ET was frozen. However, the frozen ET is also not free from the risk of mechanical obstruction.3, 4, 5 The present case indicates the importance of postoperative surveillance imaging after surgery with an ET. While multiplanar reconstruction CT images can provide morphologic information to find complications of ET, 4-dimensional flow MRI may provide useful information to determine the mechanism of obstruction.
Footnotes
Disclosures: The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Supplementary Data
Four-dimensional flow magnetic resonance imaging before thoracic endovascular aortic repair. A vortex flow in the proximal descending aorta outside of the elephant trunk flowed upward along the ventral aortic wall and turned around at the proximal blind end, compressing the elephant trunk to the greater curvature of aortic arch. Video available at: https://www.jtcvs.org/article/S2666-2507(22)00124-9/fulltext.
{kind=link}
References
- 1.Heinemann M., Buehner B., Jurmann M., Borst H. Use of the “elephant trunk technique” in aortic surgery. Ann Thorac Surg. 1995;60:2–7. [PubMed] [Google Scholar]
- 2.Wallet F., Perbet S., Fleron M.H., De Castro V., Godet G., Bertrand M., et al. Elephant trunk prosthesis kinking: transesophageal echocardiography diagnosis. Anesth Analg. 2008;106:67–69. doi: 10.1213/01.ane.0000297295.55058.0c. [DOI] [PubMed] [Google Scholar]
- 3.Pacini D., Armaro A., Di Marco L., Russo V., Di Bartolomeo R. Stent graft coarctation after frozen elephant trunk procedure: an unusual complication. J Thorac Cardiovasc Surg. 2009;137:1027–1029.e1. doi: 10.1016/j.jtcvs.2008.03.036. [DOI] [PubMed] [Google Scholar]
- 4.Uchida T., Kuroda Y., Yamashita A., Sadahiro M. Unexpected intraoperative obstruction of frozen elephant trunk in patients who underwent total arch replacement. J Card Surg. 2019;34:1673–1675. doi: 10.1111/jocs.14261. [DOI] [PubMed] [Google Scholar]
- 5.Dalal A.R., Pedroza A.J., Iwakoshi S., Lee J.T., Fleischmann D., Watkins A.C. Endovascular aortic repair after proximal stent graft migration of a modified frozen elephant trunk. Innovations (Phila) 2020;15:169–172. doi: 10.1177/1556984520902839. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Four-dimensional flow magnetic resonance imaging before thoracic endovascular aortic repair. A vortex flow in the proximal descending aorta outside of the elephant trunk flowed upward along the ventral aortic wall and turned around at the proximal blind end, compressing the elephant trunk to the greater curvature of aortic arch. Video available at: https://www.jtcvs.org/article/S2666-2507(22)00124-9/fulltext.