

Abstract
PURPOSE
We determined trends in life expectancy and cause-specific late mortality after autologous blood or marrow transplantation (BMT) performed over a 30-year period, using the BMT Survivor Study.
METHODS
We constructed a cohort of 4,702 individuals with hematologic neoplasms who lived ≥ 2 years after autologous BMT performed between 1981 and 2014 at three transplant centers. The end of follow-up was April 19, 2021. The primary exposure variable was autologous BMT performed in four eras: 1981-1999; 2000-2005; 2006-2010; and 2011-2014. Vital status and cause of death were obtained from National Death Index Plus program and Accurinct databases.
RESULTS
The median age at BMT was 53 years (range, 0-78 years), 58.7% were male, 67.8% were non-Hispanic White, and 28.3% had undergone transplantation between 2011 and 2014. Autologous BMT recipients experienced a 7-year reduction in life expectancy. The adjusted hazard of 5-year all-cause mortality declined over the four eras (reference: 1981-1999; hazard ratio [HR]2000-2005 = 0.77; 95% CI, 0.62 to 0.94; HR2006-2010 = 0.64; 95% CI, 0.51 to 0.79; HR2011-2014 = 0.56; 95% CI, 0.45 to 0.71; Ptrend < .001), as did years of life lost (5.0 years to 1.6 years). The reduction in all-cause mortality was most pronounced among those transplanted for Hodgkin lymphoma or plasma cell dyscrasias, but was not observed among those transplanted for non-Hodgkin lymphoma or those conditioned with total-body irradiation. We also observed a decline in late deaths because of infection (Ptrend < .0001; primarily for BMTs before 2006) and subsequent neoplasms (Ptrend = .03; confined to decline in therapy-related myeloid neoplasm–related mortality) but not because of cardiovascular or renal disease.
CONCLUSION
Late mortality among autologous BMT recipients has declined over a 30-year period. However, ongoing efforts are needed to mitigate development of infections, subsequent neoplasms, and cardiovascular and renal disease to further reduce late mortality.
INTRODUCTION
Autologous blood or marrow transplantation (BMT) is a well-established therapeutic modality for many hematologic neoplasms.1,2 Although improvements in supportive care strategies have resulted in a decline in early mortality,3 autologous BMT recipients carry a significant burden of late-occurring morbidity,4-8 placing them at high risk for late mortality.4,9-13 The leading causes of late mortality are disease recurrence or progression and subsequent malignant neoplasms (SMN).4-8 However, the cumulative effect of late-occurring morbidity and mortality on life expectancy after autologous BMT remains unknown. Furthermore, the impact of changes in transplant strategies over the past three decades (older age at transplantation, increasing proportion of patients undergoing autologous BMT for plasma cell dyscrasias (PCD), declining use of total body irradiation [TBI], and increasing use of peripheral blood stem cells [PBSCs] as a stem-cell source)14 on mortality rates and life expectancy remains unknown. We addressed these gaps using resources offered by the BMT Survivor Study.
CONTEXT
Key Objective
Determine trends in cause-specific late mortality and life expectancy after autologous blood or marrow transplantation (BMT) performed between 1981 and 2014.
Knowledge Generated
This cohort of 4,702 two-year survivors of autologous BMT experienced a 26% reduction in life expectancy, resulting in 7 years of life lost. Although the late mortality rates declined over the 30-year period, the decline was most evident in those with Hodgkin lymphoma or plasma cell dyscrasias, but not among those with non-Hodgkin lymphoma or those conditioned with total-body irradiation.
Relevance
There is a need for ongoing efforts to mitigate disease recurrence, subsequent neoplasms, infection, and cardiovascular disease after autologous BMT.
METHODS
Study Participants and Data Collection
BMT Survivor Study is a collaboration between City of Hope, the University of Minnesota, and the University of Alabama at Birmingham, designed to examine long-term outcomes in individuals who lived 2 years or more after BMT performed before 2014, regardless of remission status at cohort entry. For this report, we included patients who received an autologous BMT for Hodgkin lymphoma (HL), non-HL (NHL), PCD, or acute myeloid leukemia/myelodysplastic syndrome (AML/MDS) at one of the three sites between 1981 and 2014. Data on patient demographics (age at BMT, sex, and race/ethnicity), primary diagnosis, stem-cell source (bone marrow or PBSC), exposure to TBI for conditioning, and disease status at transplantation (high or standard risk for recurrence) were obtained from institutional transplant databases. National Death Index (NDI) Plus15 provided data regarding the date and cause of death through December 31, 2020. Additional information from medical records and Accurint databases16 was used to extend the vital status information through April 19, 2021. The Human Subjects Committee at University of Alabama at Birmingham served as the single institutional review board of record. The institutional review board granted a waiver of consent for linking the cohort to the NDI and Accurint databases. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines. Two investigators (J.W. and S.B.) independently assigned a cause of death to all deceased patients. In the event of discrepant assignment, the investigators collectively adjudicated a final cause of death. Cause of death was classified as external (suicide, homicide, or accident), recurrence-related (RRM: primary cause of death matching the pretransplant diagnosis), and non–recurrence-related (NRM: all other causes of death; Data Supplement, online only).
Statistical Analyses
All analyses used SAS software, version 9.4 (SAS Institute Inc). Two-sided tests with P < .05 were considered statistically significant.
Mortality rate and life expectancy.
We estimated the mortality rate as deaths in a given interval of time, divided by person-years of observation in the interval among patients alive at the start of interval. We obtained smoothed estimates of mortality rates and associated CIs by fitting a Poisson regression model to the observed counts, using cubic spline terms for time. The methodology described by Martin et al17 was used for calculating life expectancy (Data Supplement). We used sex-specific 2006 US life table data from the Centers for Disease Control and Prevention18 to calculate expected population mortality rates and life expectancy (median year of BMT was 2006).
Standardized mortality ratio.
Standardized mortality ratio (SMR; ratio of observed to expected number of deaths) compared the mortality experienced by this cohort with age-, sex-, and calendar-specific mortality of the US population. The expected number of deaths was calculated by multiplying the number of person-years in each stratum by the corresponding US mortality rates obtained from the Centers for Disease Control and Prevention.18 Poisson regression method was used to calculate 95% CI of the SMR.
Risk of all-cause and cause-specific late mortality.
Kaplan-Meier techniques were used to calculate overall survival. Cox proportional hazards regression analysis with time from transplantation as the time axis was used for identifying factors associated with all-cause mortality. Cumulative incidence rates for cause-specific mortality were calculated using competing risk methods. Proportional subdistribution hazards (Fine-Gray) model for competing risk was used for identifying factors associated with cause-specific mortality. We examined the association between hazard of mortality (all-cause; cause-specific) and age at BMT, sex, race/ethnicity, primary disease, disease status at BMT, stem-cell source, use of TBI, and transplant era (1981-1999; 2000-2005; 2006-2010; and 2011-2014; on the basis of changes in transplant practices across these eras14,19,20).
Late mortality by transplant era.
The comparison across the eras was restricted to 5 years of follow-up, to ensure adequate number of patients followed during the most current era (2011-2014). We performed mediation analyses by examining whether the hazard ratios (HRs) representing the association between transplant era and mortality changed after adding a particular risk factor.
Patients transplanted in the contemporary era.
Given that the cohort included patients transplanted over three decades, we repeated these analyses in a subcohort restricted to those transplanted between 2006 and 2014 to represent a more contemporary era.
RESULTS
Patient Characteristics
Table 1 summarizes the characteristics of the 4,702 patients included in this report. The median age at BMT was 53 years (range, 0-78 years); 58.7% were male, 67.8% were non-Hispanic White, and 28.3% had undergone transplantation between 2011 and 2014. Median follow-up after BMT was 9 years (range, 2-36 years). PCD was the most common indication for BMT (42.3%). PBSCs as the stem-cell source were used in 91.6% of the transplants, and TBI was used for conditioning in 23.1%.
TABLE 1.
Patient Characteristics—Overall, and by Transplant Era in a Cohort of Patients Treated With Autologous BMT and Surviving 2 or More Years After BMT

Across the four eras, the median age at BMT increased (40 years to 58 years), as did the proportion of patients with PCD (13.7% to 60.0%) and those receiving PBSCs (66.6% to 99.5%). There was a decline in the proportion of patients conditioned with TBI (56.4% to 5.2%), as well as those transplanted for AML/MDS (15.4% to 0.2%; Table 1).
Mortality Rates
Mortality rates exceeded expected rates from 2 years to 30 years post-BMT (Fig 1A), showing a U-shaped curve, with greater divergence from expected rates among those with the shortest follow-up (mortality rate at 2 years post-BMT: 39.2/1,000 person-years) as well as among those with the longest follow-up (30 years post-BMT: 54.1/1,000 person-years). Mortality rates were higher than expected for patients transplanted at all ages, but demonstrated an increasing divergence from the general population for those transplanted at age > 30 years (Fig 1B). The cohort was at a 2.1-fold higher risk for all-cause mortality (95% CI, 2.0 to 2.2) compared with the general population (Data Supplement).
FIG 1.

(A) Mortality rate as a function of time from BMT in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. Empirical mortality rates during each year (solid circles) are shown with fitted rates from the spline-smoothed Poisson regression model (solid line) and associated pointwise 95% CIs (short-dashed lines), and the expected mortality rates for each interval on the basis of sex- and age-specific data for the US population in 2006 (long-dashed line). (B) Mortality rate as a function of age at BMT in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. Empirical annual mortality rates during each 5-year interval of age, plotted at the midpoint of each interval (blue circles), fitted rates from the spline-smoothed Poisson regression model (solid line) and associated pointwise 95% CIs (short-dashed lines), and the expected mortality rates for each interval on the basis of an average of sex-specific US population rates at each age in 2006 (long-dashed lines). BMT, blood or marrow transplantation.
Life Expectancy
Conditional on surviving ≥ 2 years after autologous BMT, patients experienced a reduction of 7.0 years in their life expectancy (25.8% reduction). Years of life lost were greatest for the youngest survivors (5 years old: 16.5 years of life lost) and smallest for the older survivors (70 years old: 0.6 years; Figs 2A and 2B).
FIG 2.

(A) Absolute reduction in life expectancy by attained age in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. (B) Percent reduction in life expectancy by attained age in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. BMT, blood or marrow transplantation.
Hazard of Late Mortality
Conditional on surviving the first 2 years after BMT, the 25-year overall survival was 41.0% for the entire cohort (Data Supplement); the overall survival by primary diagnosis and by age at BMT are shown in the Data Supplement. Factors associated with all-cause late mortality included older age at BMT (41-64 years: HR = 2.47; 95% CI, 2.14 to 2.86; ≥ 65 years: HR, 3.69; 95% CI, 3.08 to 4.42; reference: 0-40 years), male sex (HR = 1.17; 95% CI, 1.07 to 1.28), and high-risk disease (HR = 1.34; 95% CI, 1.20 to 1.50; Table 2).
TABLE 2.
Multivariable Analysis of Factors Associated With All-Cause Mortality in a Cohort of Patients Treated With Autologous BMT and Surviving 2 or More Years After Transplantation

A cause of death was available for 1,898 of the 2,132 deceased patients (89.0%). Causes of death included RRM (47.4%), NRM (44.0%), and external (1.6%). The 25-year cumulative incidence for RRM was 23.8% (95% CI, 22.5 to 25.2; Data Supplement) and for NRM was 25.9% (95% CI, 24.0 to 27.7; Data Supplement). Factors associated with RRM (Data Supplement) included older age at BMT (41-64 years: HR = 1.91; 95% CI, 1.44 to 2.53; ≥ 65 years: HR = 2.63; 95% CI, 1.88 to 3.69), primary diagnosis of PCD (HR = 2.09; 95% CI, 1.67 to 2.61; reference: NHL), and high-risk disease (HR = 1.30; 95% CI, 1.05 to 1.61). Hispanic ethnicity (HR = 0.69; 95% CI, 0.52 to 0.90; reference: non-Hispanic White) and use of PBSC as the graft source (HR = 0.64; 95% CI, 0.45 to 0.90; reference: bone marrow) were associated with a lower hazard of RRM. Factors associated with NRM (Data Supplement) included older age at BMT (41-64 years: HR = 2.07; 95% CI, 1.44 to 2.97; ≥ 65 years: HR = 3.89; 95% CI, 2.50 to 6.05) and Hispanic ethnicity (HR = 1.49; 95% CI, 1.09 to 2.04).
The most prevalent causes of NRM were infection (n = 361), SMNs (n = 346), cardiovascular disease (n = 260), and renal disease (n = 165; Data Supplement). The 25-year cumulative incidence of infection-related death was 9.7% and the SMR was 8.1. The cumulative incidence of infection-related mortality by primary disease and age are provided in the Data Supplement. Multivariable analysis identified older age at BMT, high-risk disease, and PCD as predictors of infection-related mortality (Data Supplement). Specific types of infection included bacterial (n = 42), fungal (n = 22), viral (n = 27), and unspecified (n = 270, eg, sepsis, bronchopneumonia). The 25-year cumulative incidence of SMN-related deaths was 9.8% and SMR was 5.7. Types of SMNs included hematologic SMNs (therapy-related myeloid neoplasms [t-MN: n = 124] and other [n = 23]), and solid SMNs (GI [n = 56], lung [n = 47], and other [n = 93]). The cumulative incidence of SMN-related mortality by primary disease and age are provided in the Data Supplement). Multivariable analysis identified older age at BMT for all SMN, t-MN–, and solid SMN-related mortality and male sex as predictors for solid SMN-related deaths (Data Supplement).
Life Expectancy and Late Mortality by Treatment Era
In an analysis restricted to 5 years of follow-up, and after adjusting for demographic and clinical variables, the years of life lost declined across the four eras (5.0 years to 1.6 years). This translated into a reduction in life expectancy of 9.4% in the most recent era (2011-2014) compared with 18.5% in the earliest era (1981-1999) (Table 2; Fig 3A). Adjusting for relevant demographic and clinical variables, the 5-year hazard of all-cause mortality declined over the four transplant eras (reference: 1981-1999; HR2000-2005 = 0.77; 95% CI, 0.62 to 0.94; HR2006-2010 = 0.64; 95% CI, 0.51 to 0.79; HR2011-2014 = 0.56; 95% CI, 0.45 to 0.71; Ptrend < .001; Fig 3B).
FIG 3.
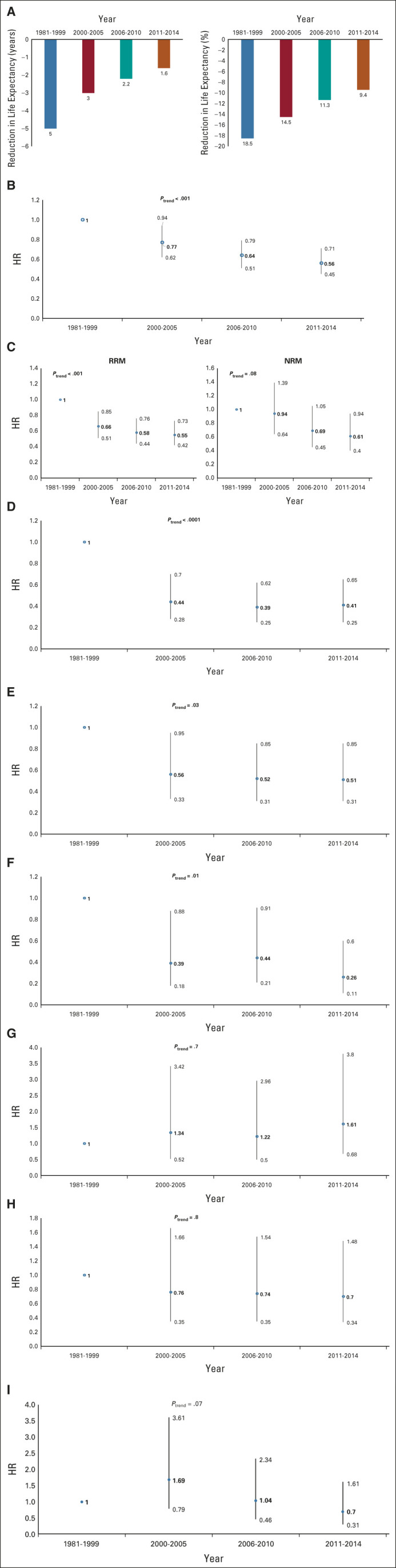
(A) Trends in reduction in life expectancy by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. (B) Trends in hazard of all-cause late mortality by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. (C) Trends in hazard of cause-specific late mortality by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. (D) Trends in hazards of infection-related late mortality by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. (E) Trends in hazards of SMN-related late mortality by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. (F) Trends in hazards of t-MN–related late mortality by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation (t-MN). The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. (G) Trends in hazards of solid SMN-related late mortality by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. (H) Trends in hazards of cardiac-related late mortality by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. (I) Trends in hazards of renal-related late mortality by transplant era in a cohort of autologous BMT recipients surviving 2 or more years after transplantation. The follow-up was truncated at 5 years post-BMT to allow comparison across the four eras. The models were adjusted for age at transplantation, sex, race/ethnicity, primary diagnosis, disease status at BMT, stem-cell source, and use of TBI. BMT, blood or marrow transplantation; HR, hazard ratio; NRM, non–recurrence-related mortality; RRM, recurrence-related mortality; SMN, subsequent malignant neoplasm; TBI, total body irradiation; t-MN, therapy-related myeloid neoplasm.
The unadjusted hazard of 5-year all-cause mortality was comparable across all eras (HR2000-2005 = 0.99; 95% CI, 0.83 to 1.18; HR2006-2010 = 0.92; 95% CI, 0.77 to 1.09; HR2011-2014 = 0.90; 95% CI, 0.76 to 1.07; reference: 1981-1999; Data Supplement). Adjustment for age at BMT reduced the hazard of mortality (HR2000-2005 = 0.80; 95% CI, 0.67 to 0.95; HR2006-2010 = 0.70; 95% CI, 0.59 to 0.84; HR2011-2014 = 0.64; 95% CI, 0.54 to 0.77), as did adjustment for primary diagnosis (HR2000-2005 = 0.80; 95% CI, 0.67 to 0.95; HR2006-2010 = 0.67; 95% CI, 0.56 to 0.80; HR2011-2014 = 0.61; 95% CI, 0.51 to 0.73) and TBI (HR2000-2005 = 0.88; 95% CI, 0.74 to 1.05; HR2006-2010 = 0.75; 95% CI, 0.62 to 0.90; HR2011-2014 = 0.72; 95% CI, 0.60 to 0.87). Adjustment for all three (age at BMT, primary diagnosis, and TBI) resulted in further reduction in late mortality from the earliest to the most recent transplant era (HR2000-2005 = 0.69; 95% CI, 0.57 to 0.83; HR2006-2010 = 0.56; 95% CI, 0.46 to 0.68; HR2011-2014 = 0.49; 95% CI, 0.40 to 0.60). Analysis stratified by age at BMT (≤ 40 years; 41-64 years; ≥ 65 years) revealed that the decline in late mortality by transplant era was evident only among those transplanted at age < 65 years (Data Supplement). Analysis stratified by primary diagnosis revealed that the decline in all-cause mortality was evident for PCD and HL but not for NHL and AML/MDS (Data Supplement). Finally, analyses stratified by use of TBI revealed that the decline in all-cause mortality was evident among those not conditioned with TBI (Data Supplement).
The adjusted hazard of 5-year RRM (reference: 1981-1999; HR2000-2005 = 0.66; 95% CI, 0.51 to 0.85; HR2006-2010 = 0.58; 95% CI, 0.44 to 0.76; HR2011-2014 = 0.55; 95% CI, 0.42 to 0.73; Ptrend < .001) also declined (Fig 3C, Data Supplement). Mediation analysis showed that adjustment for age at BMT, primary cancer diagnosis, and TBI contributed to the observed decline in the hazard of 5-year RRM across the four eras (Data Supplement). The decline in RRM was evident for PCD and HL but not for NHL (Data Supplement).
The decline in 5-year NRM was significant only for 2011-2014 (HR = 0.61; 95% CI, 0.40 to 0.94; Fig 3C, Data Supplement). Adjustment for age at BMT, primary diagnosis, TBI, and stem-cell source explained the decline (Data Supplement). The decline in NRM was evident for HL but not for NHL or PCD (Data Supplement). The hazard of infection-related late mortality declined (Ptrend < .0001) over time (Fig 3D); the largest decline was between the oldest two eras (1981-1999 v 2000-2005). The hazard of SMN-related mortality declined over time (Ptrend = .03; Fig 3E; Data Supplement). The decline in SMN-related mortality was primarily because of a decline in t-MN–related mortality (Ptrend = .01; Fig 3F); there was no change in solid SMN-related late mortality across eras (Ptrend = .7; Fig 3G). There was no statistically significant decline in late mortality because of cardiac disease (Ptrend = .8, Fig 3H) or renal disease (Ptrend = .07, Fig 3I).
Late Mortality and Life Expectancy in Patients Transplanted in the Contemporary Era
This subcohort included 2,546 patients transplanted between 2006 and 2014. Conditional on surviving ≥ 2 years, the cohort was at a 9.1-fold higher risk for all-cause mortality (95% CI, 8.51 to 9.69) compared with the general population (Data Supplement). The 15-year overall survival was 53.4%. The 15-year cumulative incidence of RRM was 22.3% and NRM was 17.4%. Factors associated with RRM included older age at BMT, high-risk disease, and PCD (Data Supplement). Factors associated with NRM included older age at BMT, male sex, Asian race, high-risk disease, TBI, and use of bone marrow as a stem-cell source (Data Supplement). Patients experienced a 4.4-year reduction in life expectancy.
DISCUSSION
Conditional on surviving 2 years after autologous BMT, the 25-year overall survival was 41.0%. Mortality rates remained elevated for those who had survived ≥ 30 years after BMT when compared with the general population. The excess mortality translated to a 7-year reduction in life expectancy. Leading causes of death included primary disease, infection, and SMNs. The hazard of all-cause late mortality declined significantly for those transplanted after 1999, with a concomitant decline in years of life lost. The decline in late mortality was evident among those transplanted at age < 65 years, those transplanted for PCD and HL, and those transplanted with non-TBI conditioning.
Several studies have described the risk of late mortality after autologous BMT.4,9-13,21,22 The composition of the cohorts has varied (disease-specific7-10,12,21-23 or all-inclusive,4,11,13 or restricted to pediatric populations13); the time to entry into the cohort has varied (from BMT,5,6,11,21,22 1 year after BMT,12 or ≥ 2 years after BMT4,7-10,13), transplant eras have varied,4-13,21-23 and methods used to determine vital status have differed (registry data,9,10,21 NDI,4,11,13 or institutional database12). Nonetheless, all studies4,9,11-13 except one10 demonstrate elevated mortality risk when compared with the general population. In our study, conditional on surviving ≥ 2 years, autologous BMT recipients were at a 2.1-fold higher risk of all-cause mortality when compared with the general population. The SMR was highest for patients with HL and those transplanted in the contemporary era and lowest for patients with AML/MDS.
We found that although the cumulative incidence of RRM plateaued at 15 years, the incidence of NRM continued to climb, with a cumulative incidence of 25.9% by 25 years post-BMT. As expected, older age at BMT and high-risk disease were associated with greater hazard of all-cause mortality, RRM, and NRM. Although the use of PBSCs in autologous BMTs is associated with faster neutrophil recovery, fewer infections, and faster immune reconstitution,24,25 its association with a lower hazard of RRM, as observed in this study, has not been previously reported and needs further investigation.
Conditional on surviving the first 2 years after BMT, we found that the life expectancy of autologous BMT survivors was 25.8% lower than expected, translating into 7 years of life lost. The only prior study to examine life expectancy did so in the setting of a single-institution cohort of allogeneic and autologous BMT recipients combined, who had survived free of primary disease for 5 or more years, where Martin et al17 reported a reduction in life expectancy of 30% across all attained ages. The lower life expectancy among BMT survivors compared with the US population likely reflects the cumulative effects of pretransplant and conditioning-related therapeutic exposures as well as post-transplant events such as disease recurrence, SMNs, infections, and other morbidities.
Transplant strategies have evolved over the past several decades with the overarching goal of improving disease control and prolonging survival. Over time, we observed an increasing number of older patients and those with a diagnosis of PCD taken for BMT, and an increase in use of PBSCs. There was a decline in the number of patients transplanted for AML/MDS and a decline in the use of TBI. Placing our findings in the context of these changes, we observed a decline in the hazard of all-cause mortality and RRM, as well as an improvement in life expectancy. We found that the reduction in late mortality was most pronounced among those who were transplanted for HL or PCDs, and among those who did not receive TBI for conditioning. The decline in NRM was restricted to patients with HL. These findings suggest that changes in transplant practice (reduction in use of TBI) and improvement in disease-specific therapeutic strategies (newer therapeutic options for PCDs and reduction in dose and volume of radiation in HL) as well as change in patient selection practice have likely contributed to the reduction in late mortality.
Similar to other studies,4,9-13 the leading causes of NRM included infection and SMNs. Risk of infection-related mortality was highest among older patients and those with PCD. Risk of SMN-related deaths was highest among older patients and those with NHL. We observed a decline in infection-related late mortality (confined to the earliest two eras, with no improvement after 2005) as well as late mortality because of SMNs (primarily because of a decline in t-MN–related mortality). However, we did not observe a decline in mortality because of cardiovascular or renal disease, suggesting a need for aggressive interventions to prevent/manage these adverse outcomes.
A possible limitation of the study stems from the reliance on NDI Plus for cause of death; we used two independent reviewers and adjudicated cause of death using algorithms to mitigate misclassification. Nevertheless, we were unable to refine the classification of the cause of death in some instances, especially infection-related deaths. Given the three decades of transplant practice, we created a contemporary cohort to provide information related to all-cause and cause-specific late mortality. Furthermore, given the disease- and age-related heterogeneity of the cohort, we provide disease-specific and age-group–specific analyses to facilitate management of specific patient populations. This study was unable to capture changes in supportive care, or patient selection strategies (eg, performance scores/pre-BMT comorbidity index) that could have resulted in improvement in outcome. Nonetheless, in this first large multi-institutional study with mature follow-up, inclusion of both adults and children, and the use of rigorous methodology to determine vital status, we describe trends in late mortality and life expectancy over three decades of autologous transplantation for hematologic neoplasms. The study finds that although late mortality among autologous BMT recipients has declined over a 30-year period, continued effort is needed to mitigate deaths because of subsequent neoplasms, infections, and cardiovascular and renal diseases in this population.
Smita Bhatia
This author is an Associate Editor for Journal of Clinical Oncology. Journal policy recused the author from having any role in the peer review of this manuscript.
Wendy Landier
Research Funding: Merck Sharp & Dohme (Inst)
Stephen J. Forman
Stock and Other Ownership Interests: MustangBio, Lixte Biotechnology
Consulting or Advisory Role: Alimera Sciences, Lixte Biotechnology, MustangBio
Research Funding: MustangBio
Patents, Royalties, Other Intellectual Property: MustangBio
Daniel J. Weisdorf
Consulting or Advisory Role: Incyte, Fate Therapeutics
Research Funding: Incyte
Mukta Arora
Consulting or Advisory Role: Fate Therapeutics
Research Funding: Syndax (Inst), Kadmon (Inst), Pharmacyclics (Inst)
No other potential conflicts of interest were reported.
See accompanying editorial on page 1971
DISCLAIMER
The opinions expressed in this paper are those of the authors and do not necessarily represent those of the organizations providing funding for this study. The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
PRIOR PRESENTATION
Presented in part at the American Society of Hematology annual meeting, Atlanta, GA, December 12, 2021.
SUPPORT
Supported in part by the National Cancer Institute (R01 CA078938 [S.B.]; U01 CA213140 [S.B.]), and the Leukemia and Lymphoma Society (R6502-16 [S.B.]).
AUTHOR CONTRIBUTIONS
Conception and design: Smita Bhatia
Financial support: Smita Bhatia
Administrative support: Smita Bhatia, Wendy Landier, Lindsey Hageman, Elizabeth Schlichting, Nora Balas, Stephen J. Forman
Provision of study materials or patients: Smita Bhatia, Arianna Siler, Donna Salzman, Saro H. Armenian, Mukta Arora
Collection and assembly of data: Smita Bhatia, Lindsey Hageman, Jessica Wu, Elizabeth Schlichting, Arianna Siler, Erin Funk, Jessica Hicks, Shawn Lim, Nora Balas, Alysia Bosworth, Hok Sreng Te, Liton Francisco, Frederick D. Goldman, Saro H. Armenian, Mukta Arora
Data analysis and interpretation: Smita Bhatia, Chen Dai, Wendy Landier, Jessica Wu, Ravi Bhatia, Donna Salzman, Stephen J. Forman, Daniel J. Weisdorf, F. Lennie Wong, Saro H. Armenian, Mukta Arora
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Trends in Late Mortality and Life Expectancy After Autologous Blood or Marrow Transplantation Over Three Decades: A BMTSS Report
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Smita Bhatia
This author is an Associate Editor for Journal of Clinical Oncology. Journal policy recused the author from having any role in the peer review of this manuscript.
Wendy Landier
Research Funding: Merck Sharp & Dohme (Inst)
Stephen J. Forman
Stock and Other Ownership Interests: MustangBio, Lixte Biotechnology
Consulting or Advisory Role: Alimera Sciences, Lixte Biotechnology, MustangBio
Research Funding: MustangBio
Patents, Royalties, Other Intellectual Property: MustangBio
Daniel J. Weisdorf
Consulting or Advisory Role: Incyte, Fate Therapeutics
Research Funding: Incyte
Mukta Arora
Consulting or Advisory Role: Fate Therapeutics
Research Funding: Syndax (Inst), Kadmon (Inst), Pharmacyclics (Inst)
No other potential conflicts of interest were reported.
REFERENCES
- 1.Jantunen E, Varmavuo V, Pelkonen J, et al. Importance of early immune recovery after autologous hematopoietic cell transplantation in lymphoma patients Leuk Lymphoma 602115–21212019 [DOI] [PubMed] [Google Scholar]
- 2. Al Hamed R, Bazarbachi AH, Malard F, et al. Current status of autologous stem cell transplantation for multiple myeloma. Blood Cancer J. 2019;9:44. doi: 10.1038/s41408-019-0205-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jantunen E, Itälä M, Lehtinen T, et al. Early treatment-related mortality in adult autologous stem cell transplant recipients: A nation-wide survey of 1482 transplanted patients Eur J Haematol 76245–2502006 [DOI] [PubMed] [Google Scholar]
- 4.Bhatia S, Robison LL, Francisco L, et al. Late mortality in survivors of autologous hematopoietic-cell transplantation: Report from the Bone Marrow Transplant Survivor Study Blood 1054215–42222005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.André M, Henry-Amar M, Blaise D, et al. Treatment-related deaths and second cancer risk after autologous stem-cell transplantation for Hodgkin's disease Blood 921933–19401998 [PubMed] [Google Scholar]
- 6.Micallef IN, Lillington DM, Apostolidis J, et al. Therapy-related myelodysplasia and secondary acute myelogenous leukemia after high-dose therapy with autologous hematopoietic progenitor-cell support for lymphoid malignancies J Clin Oncol 18947–9552000 [DOI] [PubMed] [Google Scholar]
- 7.Majhail NS, Ness KK, Burns LJ, et al. Late effects in survivors of Hodgkin and non-Hodgkin lymphoma treated with autologous hematopoietic cell transplantation: A report from the bone marrow transplant survivor study Biol Blood Marrow Transpl 131153–11592007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Arora M, Chen Y, Hageman L, et al. Morbidity burden in survivors of multiple myeloma who underwent autologous transplantation: A Bone Marrow Transplantation Survivor Study Cancer 1263322–33292020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Majhail NS, Bajorunaite R, Lazarus HM, et al. Long-term survival and late relapse in 2-year survivors of autologous haematopoietic cell transplantation for Hodgkin and non-Hodgkin lymphoma Br J Haematol 147129–1392009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Majhail NS, Bajorunaite R, Lazarus HM, et al. High probability of long-term survival in 2-year survivors of autologous hematopoietic cell transplantation for AML in first or second CR Bone Marrow Transplant 46385–3922011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vanderwalde AM, Sun CL, Laddaran L, et al. Conditional survival and cause-specific mortality after autologous hematopoietic cell transplantation for hematological malignancies Leukemia 271139–11452013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.El-Asmar J, Rybicki L, Bolwell BJ, et al. Conditional long-term survival after autologous hematopoietic cell transplantation for diffuse large B cell lymphoma Biol Blood Marrow Transplant 252522–25262019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Holmqvist AS, Chen Y, Wu J, et al. Late mortality after autologous blood or marrow transplantation in childhood: A Blood or Marrow Transplant Survivor Study-2 report Blood 1312720–27292018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.D'Souza A, Fretham C, Lee SJ, et al. Current use of and trends in hematopoietic cell transplantation in the United States Biol Blood Marrow Transplant 26e177–e1822020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.National Death Index. https://www.cdc.gov/nchs/ndi/index.htm
- 16.Accurint: LexisNexis risk solutions. http://www.accurint.com
- 17.Martin PJ, Counts GW, Appelbaum FR, et al. Life expectancy in patients surviving more than 5 years after hematopoietic cell transplantation J Clin Oncol 281011–10162010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Centers for Disease Control and Prevention: Data access - Compressed mortality file. https://www.cdc.gov/nchs/data_access/cmf.htm [Google Scholar]
- 19.Auner HW, Szydlo R, Hoek J, et al. Trends in autologous hematopoietic cell transplantation for multiple myeloma in Europe: Increased use and improved outcomes in elderly patients in recent years Bone Marrow Transplant 50209–2152015 [DOI] [PubMed] [Google Scholar]
- 20.McCarthy PL, Hahn T, Hassebroek A, et al. Trends in use of and survival after autologous hematopoietic cell transplantation in North America, 1995-2005: Significant improvement in survival for lymphoma and myeloma during a period of increasing recipient age Biol Blood Marrow Transplant 191116–11232013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Costa LJ, Zhang MJ, Zhong X, et al. Trends in utilization and outcomes of autologous transplantation as early therapy for multiple myeloma Biol Blood Marrow Transplant 191615–16242013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Costa LJ, Iacobelli S, Pasquini MC, et al. Long-term survival of 1338 MM patients treated with tandem autologous vs. autologous-allogeneic transplantation Bone Marrow Transplant 551810–18162020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Badar T, Epperla N, Szabo A, et al. Trends in postrelapse survival in classic Hodgkin lymphoma patients after experiencing therapy failure following auto-HCT Blood Adv 447–542020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Vellenga E, van Agthoven M, Croockewit AJ, et al. Autologous peripheral blood stem cell transplantation in patients with relapsed lymphoma results in accelerated haematopoietic reconstitution, improved quality of life and cost reduction compared with bone marrow transplantation: The Hovon 22 study Br J Haematol 114319–3262001 [DOI] [PubMed] [Google Scholar]
- 25.Schwinger W, Weber-Mzell D, Zois B, et al. Immune reconstitution after purified autologous and allogeneic blood stem cell transplantation compared with unmanipulated bone marrow transplantation in children Br J Haematol 13576–842006 [DOI] [PubMed] [Google Scholar]