

Abstract
The Theory of Planned Behavior posits that behaviors are predicted by one’s intention to perform them; intention is driven by attitude toward the behavior, subjective norm, and perceived behavioral control. We used this theory to predict Crisis Intervention Team (CIT)-trained and non-CIT officers’ intention to facilitate referral of persons with suspected mental illnesses to mental health services. CIT-trained (n = 251) and non-CIT (n = 335) officers from six law enforcement agencies participated. CIT-trained officers had significantly greater scores on all constructs. Theory constructs fit the data well, and fit did not differ meaningfully between the two groups. Direct and indirect predictors together accounted for 28% and 21%, respectively, of variance in behavioral intention. Attitude was the strongest predictor. Intentions to facilitate mental health referrals may be driven by the same factors among CIT-trained and non-CIT officers, but CIT officers, even at a median of 22 months after training, have significantly higher scores on those factors.
Keywords: Crisis Intervention Team, Law enforcement, Police officers, Theory of Planned Behavior
In response to concerns that police encounters with individuals with mental illnesses or in psychiatric crisis too often result in violence, and are undertaken by police officers with limited specialized training, the Crisis Intervention Team (CIT) model is being implemented in law enforcement agencies across the U.S. as a means of improving officers’ responses. The model facilitates pre-booking jail diversion when appropriate, and emphasizes de-escalation and safe alternatives to the use of force in resolving crisis situations. In addition to revised procedures in both the law enforcement agency and local psychiatric services that enhance collaboration between the two sectors, the CIT model includes a 40-h block of training for select officers who then become specialized first-responders. CIT training improves officers’ knowledge, attitudes, self-efficacy, and skills, while reducing their stigma toward people with mental illnesses (Bahora et al., 2008; Broussard et al., 2011; Compton et al., 2006, 2014a; Hanafi et al., 2008) and potentially lowering their reliance on and perceived effectiveness of physical force (Compton et al., 2011).
Although the existing literature indicates these promising effects of CIT, how CIT influences the attitudes, decisions, and behaviors of individual officers requires further study. To help fill this gap in research, this study examined a model that might hold promise for understanding CIT’s officer-level effects. A number of behavioral models and theories have been developed and studied (e.g., Health Belief Model, Social Cognitive Theory, Transtheoretical Model, Diffusion of Innovations theory) in relation to a range of health-related behaviors. One such theory, the Theory of Planned Behavior, postulates that the most important determinant of a behavior is a person’s behavioral intention. Ajzen (1985) distinguished three factors (or constructs) that determine the strength of a behavioral intention. Attitude toward the behavior refers to the degree to which a person has a favorable or unfavorable evaluation of the planned behavior. Subjective norm represents perceived social pressure to perform or not perform the behavior. Perceived behavioral control refers to the perceived ease or difficulty of performing the behavior. When an individual has a more favorable attitude and subjective norm, and perceives a greater amount of control, the intention to perform the behavior will be stronger (Ajzen, 1985). The Theory of Planned Behavior builds on the straightforward notion that many behaviors can be reliably predicted by a person’s intention to perform those behaviors (Perkins et al., 2007). Diverse factors can interfere with control over intended behavior, including internal factors such as skills and knowledge, and external factors such as time, opportunity, and dependence of the behavior on the cooperation of other people (Ajzen & Madden, 1986). The Theory of Planned Behavior has been applied to many types of behavior, and the perceived behavioral control construct, accounting for the partly non-volitional nature of many behaviors, is an important construct across many behaviors (Godin & Kok, 1996). For the behavior of facilitating mental health referrals for individuals with a suspected serious mental illness, these non-volitional factors may be important. The theory is shown in Fig. 1.
Fig. 1.
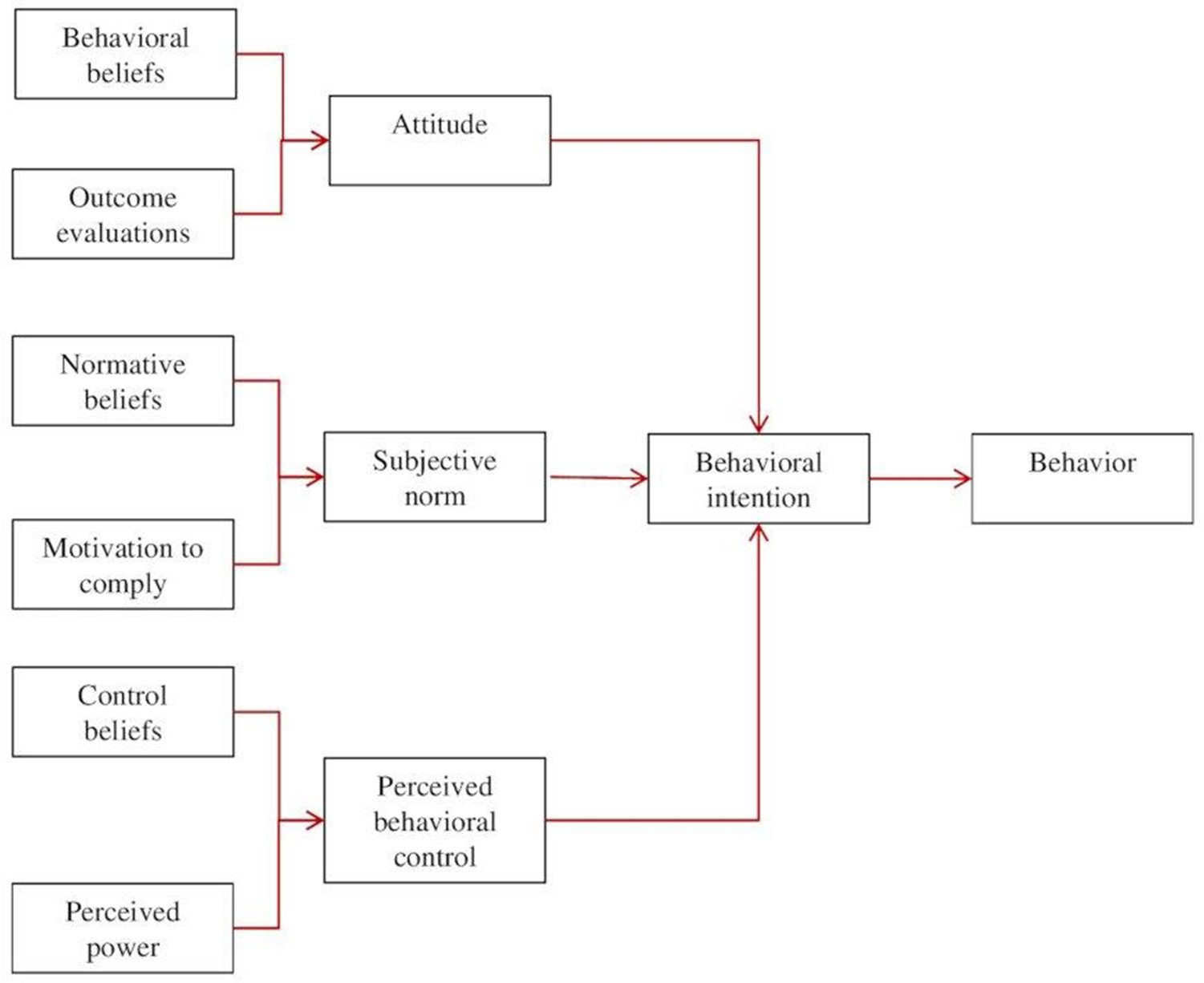
The Theory of Planned Behavior
The three main constructs of the Theory of Planned Behavior (attitude toward the behavior, subjective norm, and perceived behavioral control) all impact behavioral intention, which has high predictive validity in relation to behavior (Committee on Communication for Behavior Change in the 21st Century, 2002). Other constructs, such as personality, environmental, and demographic variables, may influence behavioral intentions, but in the Theory of Planned Behavior, they do so through their influence on the three main constructs (Perkins et al., 2007). Each of these three is determined mathematically by two sub-components. For example, perceived behavioral control is the sum of the products of control beliefs (expectancies) and the evaluation of perceived power.
The Theory of Planned Behavior has been applied to numerous health-related behaviors, such as substance use (Bashirian et al., 2012), automobile safety-related behaviors (Şimşekoğlu & Lajunen, 2008), bicycle helmet-wearing (Ross et al., 2011), cigarette smoking (Topa & Moriano, 2010), exercise/physical activity (Boudreau & Godin, 2007), hand-washing by healthcare professionals (O’Boyle et al., 2001), and uptake of mammography (Steele & Porche, 2005), to name a few. Hundreds of studies support the utility of the main constructs of the Theory of Planned Behavior. Compton and Esterberg (2005) used its constructs to examine treatment delay among family members of young adults experiencing first-episode psychosis and found that perceived behavioral control was inversely correlated with treatment delay. Others have used the Theory of Planned Behavior to study intention to promptly seek medical care (Godin et al., 1993) or to examine clinicians’ behaviors (Perkins et al., 2007). Like most behavior theories, the Theory of Planned Behavior is behavior-specific; in this study, the behavior of interest is officers’ facilitation of mental health referrals for individuals suspected to have a serious mental illness.
The Theory of Planned Behavior is especially suitable for the study of officer-level effects of CIT because it is likely that officers’ facilitation of mental health referrals is influenced by their attitude toward these actions (CIT has been shown to improve officers’ attitudes about serious mental illnesses and treatments), what they perceive to be the attitudes of influential others (e.g., subjective norm pertaining to their peers and supervisors), and their sense of control over the situation (CIT improves self-efficacy for responding to people with suspected serious mental illnesses). Self-efficacy, or confidence in one’s ability to successfully execute the behavior required to produce the outcome (Bandura, 1977; Strecher & Rosenstock, 1997), is closely linked to the theory’s perceived behavioral control construct (Ajzen, 2002). We developed a Theory of Planned Behavior rating scale, assessed differences between CIT-trained and non-CIT officers across all of the theory’s constructs, and used structural equation modeling to evaluate the theory in predicting officers’ intentions in both CIT-trained and non-CIT groups. This work is of relevance to CIT programs—which have been implemented in several thousand police agencies across the U.S. in an effort to improve police-based crisis response to individuals suspected to have a serious mental illness or those in psychiatric crisis—in two key ways. First, differences between CIT-trained and non-CIT officers are documented across all of the measured constructs, which has never been done but represents another officer-level outcome of CIT training. Second, the Theory of Planned Behavior gives a framework for understanding which of the measured constructs are most impactful in determining officers’ intentions of facilitating mental health referrals for those in need of such referrals. As such, the study adds to the literature on which officers refer individuals to mental health services, and why.
Methods
Setting, Sample, and General Procedures
Data collection for the current study was embedded within a larger project comparing CIT-trained and non-CIT officers in terms of: (1) six key constructs pertinent to the goals of CIT training (knowledge about mental illnesses, attitudes about serious mental illnesses and treatments, self-efficacy for de-escalating crisis situations and making referrals to mental health services, stigma, de-escalation skills, and referral decisions) (Compton et al., 2014a), and (2) levels of force used and disposition decisions made during encounters with individuals suspected of having a mental illness (Compton et al., 2014b). The current report pertains to additional data that were collected in order to assess the utility of constructs of the Theory of Planned Behavior in predicting officers’ behavioral intention with regard to facilitating mental health referrals.
Police officers were recruited from a mix of six rural and metropolitan police departments across the state of Georgia, all of which had CIT programs. Several recruitment methods were employed. Department-approved emails were sent to all personnel stating the need for both CIT and non-CIT trained officers, 21 or older, to voluntarily participate in the study. Additionally, announcements, followed by registration for the research project, were made during roll call meetings. Lastly, flyers were posted in police facilities and officers identified as CIT-trained were individually contacted and invited to participate. From April through October 2010, 586 police officers—251 CIT-trained officers (at a median of 22 months since their training) and 335 non-CIT officers—were recruited. As detailed in another report (Compton et al., 2017), among the 251 CIT-trained officers, 171 reported having volunteered/self-selected for the training and 80 reported having been assigned to it. Each police department had its own CIT program and determined which, when, and how many officers received CIT training.
Survey measures were administered in 34 proctored groups that included 6–29 officers. Prior to survey administration, a study team member explained the process and answered any questions. Participants provided written informed consent. All study procedures were approved by the university’s institutional review board. Officers who participated while off duty received a compensation of $200 upon completion of study measures, which took approximately three hours (Compton et al., 2014a, 2014b) and included the Theory of Planned Behavior rating scale described below.
The authors certify that they accept responsibility for the conduct of the study, analysis, and interpretation of the data, that they all contributed to the manuscript and decisions regarding it, that they are all authors as defined by the International Committee of Medical Journal Editors, that they have seen and approved the final manuscript, and that neither the article nor any essential part of it will be published or submitted elsewhere before appearing in Community Mental Health Journal. Emory University’s Institutional Review Board approved the study.
Measures
The assessment for the parent project included demographic characteristics and a number of constructs pertaining to knowledge about mental illnesses, attitudes toward mental illnesses and their treatments, stigma, and self-efficacy for responding to persons in psychiatric crisis (Compton et al., 2014a). A Theory of Planned Behavior measurement instrument is typically created by operationalizing the theory’s variables in terms of the population and behavior being studied, using open-ended elicitation interviews to provide the specific content and context. The instrument in this case was developed specifically for this study by conducting these with police officers, community advisory board (CAB) members, and a retired law enforcement official. Specifically, we had an hour-long, focus group-style discussion with a group of approximately 20 officers going through CIT training, we interviewed eight individuals composing the CAB (six law enforcement supervisory staff from the six participating agencies, along with two consumer/family member advocates), and we interviewed a retired state law enforcement officer serving as a consultant on the project. The elicitation interview instrument included open-ended questions about: (a) the actions performed during encounters with individuals who have a suspected mental illness (behavior), (b) positive/negative perceptions or outcomes of actions performed during encounters with individuals who have a suspected mental illness (attitude), (c) persons, groups, or establishments that influence professional actions when dealing with persons suspected to have a mental illness (subjective norm), and (c) factors and resources that regulate, facilitate, or impede actions performed during encounters with individuals who have a suspected mental illness (perceived behavioral control). The interview guide included probes and follow-up questions to gather qualitative data about respondents’ insights into interacting with persons with suspected mental illnesses. The content of interviews was analyzed using qualitative thematic analysis methods, and categorized to define the theory’s constructs and create items for the survey instrument.
As is usual in applying the Theory of Planned Behavior, constructs were measured using both “direct” and “indirect” measures, scored with Likert-scaled items. As such, “direct measures” refer to those that measure the theory’s major constructs—summed scores obtained from items worded to directly measure the constructs of attitude, subjective norm, and perceived behavioral control, respectively. On the other hand, “indirect measures” are those that measure the minor constructs that comprise the major constructs; these constructs are calculated as follows: (a) the indirect attitude score was obtained by summing the products of behavioral beliefs and outcome evaluations, (b) the indirect subjective norm score by summing the products of normative beliefs and motivation to comply, and (c) the indirect perceived behavioral control score by summing the products of control beliefs and perceived power. The definitions of the constructs, and examples of items used to measure them, are given in Table 1.
Table 1.
Definitions of Theory of Planned Behavior constructs, and examples of items used to measure each
| Measure | Construct | Example |
|---|---|---|
|
| ||
| Direct | Attitude | Attitude toward performing the behavior: The police officer’s evaluation (unfavorable or favorable) of referring individuals with a suspected mental illness to mental health services (e.g., “I think that referring subjects who appear to have a mental illness to mental health services is: [useless – useful]”) |
| Subjective norm | Belief regarding whether most people approve or disapprove of the behavior: The police officer’s perceived social pressure to refer individuals with a suspected mental illness to mental health services (e.g., “Most people who are important to me would approve of me referring a subject who appears to have a mental illness to mental health services” [extremely unlikely – extremely likely]) | |
| Perceived behavioral control | Overall perception of the officer’s control over performing the behavior: The police officer’s perceived ease or difficulty of referring individuals with a suspected mental illness to mental health services (e.g., “I am confident that I can refer a subject who appears to have a mental illness to mental health services, if needed” [strongly disagree – strongly agree]) | |
| Indirect | Attitude | Attitude = Behavioral beliefs × Outcome evaluations Behavioral beliefs: Beliefs about the likelihood that referring individuals with a suspected mental illness to mental health services will result in certain outcomes (e.g., “Referring subjects who appear to have a mental illness to mental health services helps avoid incarceration of these individuals” [extremely unlikely – extremely likely]) Outcome evaluations: Good/bad value of the outcome (e.g., “Incarceration of subjects who appear to have a mental illness is: [undesirable – desirable]”) |
| Subjective norm | Subjective norm = Normative beliefs × Motivation to comply Normative beliefs: Beliefs about referents’ approval or disapproval of referral to mental health services. The referents included supervisors, coworkers, family members, friends/ neighbors, mental health professionals, on-site partner, subjects with a mental illness, and the general public. (e.g., “My supervisor would approve of me referring a subject who appears to have a mental illness to mental health services” [extremely unlikely – extremely likely]) Motivation to comply: Motivation to do what each referent thinks (e.g., “When dealing with subjects who appear to have a mental illness, I usually do what my supervisor thinks I should do” [strongly disagree – strongly agree]) |
|
| Perceived behavioral control | Perceived behavioral control = Control beliefs × Perceived power Control beliefs: Beliefs about likelihood of occurrence of factors that may facilitate or impede mental health services referral (e.g., “Subjects who appear to have a mental illness may not recognize that they have a mental illness and/or substance use problem” [extremely unlikely – extremely likely]) Perceived power: Perceived effect about each of these factors in making mental health services referral difficult or easy (e.g., “When a subject who appears to have a mental illness does not recognize that he/she has a mental illness, this makes it [difficult – easy] for me to refer them to mental health services”) |
|
| Behavioral intention | The police officer’s perceived/reported likelihood of referring individuals with a suspected mental illness to mental health services (e.g. “When I encounter subjects who appear to have a mental illness, I take them to emergency receiving facilities” [extremely unlikely – extremely likely]) | |
Data Analyses
We first examined the psychometric properties (Cronbach’s alpha internal consistency reliability) of the scales developed. We then compared CIT-trained and non-CIT officers on all Theory of Planned Behavior constructs. Finally, we examined fit of the Theory of Planned Behavior (all constructs through behavioral intention) using structural equation modeling and also the fit of this model in CIT-trained and non-CIT officers separately. Analyses were conducted using IBM SPSS Statistics and LISREL.
Results
The six predictor variables were direct and indirect assessments of attitude, subjective norm, and perceived behavioral control. The indirect measure of attitude had a lower than preferred alpha of 0.43 (Table 2). Regarding CIT-trained versus non-CIT differences, means for all seven variables (predictors and behavioral intention) were higher for the CIT-trained group (Table 2). The measures of effect size (Cohen’s d) reveal that behavioral intention, attitude, and subjective norm all differed with a small but significant effect. For example, regarding the direct measure of attitude, the effect size of d = 0.32 indicates that the mean of the CIT-trained group is at about the 62nd percentile of the non-CIT group (and that there is non-overlap of approximately 21% in the two groups’ distributions). Similarly, regarding the indirect measure of subjective norm, the effect size of d = 0.20 indicates that the mean of the CIT-trained group is at about the 58th percentile of the non-CIT group (and that there is non-overlap of approximately 15% in the two distributions). On the other hand, both the direct and indirect measures of perceived behavioral control differed with a medium effect (d = 0.54 and d = 0.59, respectively), indicating that the means of the CIT-trained group are at about the 70th–73rd percentile of the non-CIT group, and that there is non-overlap of approximately 35–38% in the two distributions.
Table 2.
Comparisons of CIT-trained (n = 251) and non-CIT officers (n = 335) on Theory of Planned Behavior construct scores
| Variable | CIT-Trained |
Non-CIT |
Independent samples t tests |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| α | M | SD | α | M | SD | t | df | p | d | |
|
| ||||||||||
| Behavioral intention (facilitating referral) | .69 | 1.63 | 4.16 | .74 | .86 | 4.55 | 2.09 | 579 | .04 | .18 |
| Direct Predictors | ||||||||||
| Attitude toward facilitating referral | .78 | 22.47 | 5.04 | .78 | 20.80 | 5.53 | 3.75 | 581 | < .001 | .32 |
| Officers’ subjective norm | N/A | 2.30 | .75 | N/A | 2.05 | .96 | 3.27 | 584 | .001 | .29 |
| Perceived behavioral control | .67 | 17.90 | 2.86 | .68 | 16.16 | 3.60 | 6.42 | 582 | < .001 | .54 |
| Indirect Predictors | ||||||||||
| Attitude toward facilitating referral | .43 | 6.56 | 14.30 | .58 | 3.09 | 15.3 | 2.78 | 577 | .006 | .23 |
| Officers’ subjective norm | .85 | 80.15 | 39.01 | .85 | 72.22 | 4.67 | 2.36 | 577 | .02 | .20 |
| Perceived behavioral control | .72 | 14.61 | 19.62 | .69 | 3.65 | 17.65 | 6.98 | 565 | < .001 | .59 |
The next analyses used structural equation modeling to investigate possible group differences in associations between the three direct predictor variables and outcome (behavioral intention) and the three indirect predictor variables and outcome. We defined two straightforward path models, one with the three direct and one with the three indirect variables predicting behavioral intention. Model 1 constrained the path coefficients to be the same for CIT-trained and non-CIT groups. For both direct and indirect predictors, this model fit the data well: χ2 = 2.69 and 6.77, p = 0.61 and 0.15. As expected, Model 2, which estimated the path coefficients for the two groups separately, fit the data somewhat but not significantly better: χ2 = 2.43 and 0.58, p = 0.12 and 0.45. In both cases, Δχ2 = 0.26 and 6.19, which, with 3 degrees of freedom, is not significant.
Thus, although means for the variables differed between the groups, their associations with behavioral intention did not differ. The direct variables together accounted for 28%, and the indirect variables 21%, of the variance in behavioral intention (p < 0.001 for both). Path coefficients and their significance are shown in Table 3. For both direct and indirect measures, attitude had the strongest association with behavioral intention, followed by subjective norm, followed by perceived behavioral control.
Table 3.
Associations between direct and indirect Theory of Planned Behavior constructs and behavioral intention, path coefficients, and significance
| Variable | Direct |
Indirect |
||
|---|---|---|---|---|
| β | p | β | p | |
|
| ||||
| Attitude | .46 | < .001 | .31 | < .001 |
| Subjective norm | .13 | .001 | .21 | < .001 |
| Perceived behavioral control | .09 | .017 | .08 | .048 |
Discussion
In this first application of a widely studied behavioral sciences model to CIT, we observed several interesting findings. First, all of the direct and indirect measures of the three predictor constructs (in addition to the behavioral intention outcome variable) differed significantly between the two groups, indicating that CIT-trained officers had a more positive attitude toward facilitating mental health referral, greater subjective norm for doing so, and higher perceptions of control for making referrals (with the latter, perceived behavioral control, showing the greatest difference between groups). Second, the Theory of Planned Behavior fit our data well, and the fit did not differ meaningfully between the two groups of officers. Third, in predicting behavioral intention, attitude had the strongest effect, followed by subjective norm, followed by perceived behavioral control.
Although accumulating research shows that CIT training has beneficial impacts with regard to officers’ knowledge, attitudes, stigma, self-efficacy, de-escalation skills, and referral decisions (Watson et al., 2017), we expand that evidence by showing that—even at a median of 22 months after their training—CIT-trained officers also have significantly higher scores on all of the Theory of Planned Behavior constructs. They differed most prominently on perceptions of behavioral control in the process of facilitating a referral. It could be that CIT training not only changes officers’ attitude and subjective norm, but it also provides officers with a sense of control and self-efficacy over the referral process. Recalling that perceived behavioral control is the officer’s overall perception of control over performing the behavior, and self-efficacy is defined as how confident one feels in engaging in a task, the two concepts are intimately related (Ajzen, 2002). Past CIT research (e.g., Bahora et al., 2008; Compton et al., 2014a, 2014b; Hanafi et al., 2008) shows that CIT training increases self-efficacy, which aligns with the current findings. It could be, for example, that the enhanced organizational linkages of the CIT model increase an officer’s familiarity with, and confidence in, referring a person to treatment. Repeatedly engaging in the practice of referral could then increase confidence in their ability to do so. Such an association between functional attitudes, intentions to refer, and organizational linkages has been demonstrated in the case of community corrections personnel who work closely with treatment providers and must decide whether to refer their clients to treatment for substance use disorder (Friedmann et al., 2015). Future research should explore this possible effect with the CIT model as well: it could be that the model’s collaborative nature enhances self-efficacy.
Despite the fact that perceived behavioral control differed more than subjective norm and attitude, interestingly, attitude toward facilitating mental health referral had the strongest effect in predicting officers’ behavioral intention. Thus, while improving one’s self-efficacy is important, changes in attitude are critical given that one’s motivation or intention to refer is driven by one’s attitude. Attitudes are complex and shaped by cognitive, affective, and behavioral factors (Maio & Haddock, 2010). CIT research has shown the program’s success in changing attitudes toward various facets of interacting with persons experiencing a mental health crisis, such as improved safety and skills available to the officer (Bahora et al., 2008; Bonfine et al., 2014; Compton et al., 2014a, 2014b).
The literature on applications of the Theory of Planned Behavior to policing is very limited; only four studies were found, and only one studied how it can be used to assess the intentions of police officers in making enforcement-related decisions in the field. The first (Hyland et al., 2012) examined officers’ intentions to participate in a psychological counseling program. The authors found the theory to be an effective predictive model, accounting for 92.6% of variance in behavioral intention, with self-efficacy (the internal control facet of perceived behavioral control) showing the strongest association with intention. The second study (Keller & Miller, 2015) used the Theory of Planned Behavior to look at the intention of members of the public to report crimes to police, for which support was found, with social norm being the most influential factor. The third study used a sample of 296 South Korean police officers to assess what determined their intention to report misconduct or corruption (Park & Blenkinsopp, 2008). In a fourth study (Ishoy, 2016) officers’ personal attitudes about discretionary enforcement behaviors were found to impact their decisions, though the effects of attitudes varied across different contexts of enforcement. Regarding subjective norms, officers were primarily concerned with their supervisors’ expectations. Officers’ enforcement decisions were also impacted by perceived limits on their discretion, which were conditioned by the perceived seriousness of the offense. Building on the limited number of Theory of Planned Behavior studies in the policing literature, our findings indicate that the theory might enhance our understanding of how officers with and without CIT training formulate their intentions to facilitate referrals to mental health services or engage in de-escalation rather than use force.
Given the complexity and diverse intersecting contexts that bear upon police encounters—and the fact that the Theory of Planned Behavior only addresses the internal factors that influence an eventual decision—officers’ behaviors are undoubtedly multiply determined. A deeper understanding of officers’ behaviors must include the context both immediately around the officer and subject, and more broadly in terms of such things as shifting policing policy as well as political and social shifts that impact police decision-making. Although internal factors contribute to behavior (including those factors tapped by the Theory of Planned Behavior), diverse contextual issues cannot be ignored. On the other hand, given the multitude of converging internal and external factors that drive behaviors like facilitating referral of persons suspected to have mental illnesses to psychiatric services, or the decision to de-escalate a situation rather than use force, the fact that these three internal factors (attitudes, subjective norms, and perceived behavioral control) appear to predict behavioral intention (and that CIT-trained officers have higher scores on all three of these variables) could indicate that a program like CIT can have a meaningful impact on behaviors despite complex contextual factors. CIT programs’ impact on officers will be maximized when the training component addresses those cognitive and attitudinal variables most likely to impact behavioral intentions and behaviors, and attitudes appear to be very important.
Several limitations must be acknowledged. First, and most importantly, while the Theory of Planned Behavior was designed to measure actual behaviors, our study measured behavioral intention (whether or not the officer intended to facilitate a referral for “subjects who appear to have a mental illness”). A person can have every intention of engaging in an action without actually executing it, but the effectiveness of the CIT model rests squarely upon the actions police officers ultimately take. Future work should address the constructs of the Theory of Planned Behavior while also measuring officers’ intentions, as well as their actual behaviors in terms of facilitating referrals to mental health services. Second, that we were able to measure intentions among CIT-trained officers, but not outcomes, left us unable to account for the possibility that a social desirability bias affected the answers these officers provided: it is clear that an officer’s training and participation in the CIT model comes with an expectation that they have reduced stigma toward people with mental illnesses, and that they will be more likely to facilitate referrals. This expectation may have affected their responses. Third, although the Cronbach’s alpha internal consistency reliability coefficient for the direct measure of attitudes was acceptable (0.78), it was low for the indirect measure among both CIT-trained (0.43) and non-CIT officers (0.58). As such, the analysis involving direct measures may be more reliable.
Conclusion
The Theory of Planned Behavior has been extensively studied in various arenas to determine one’s intention to engage in a health-related behavior, but only one study has used it to determine how police officers formulate their behavioral intentions about the discretionary decisions they will make in the field. The present study is the first attempt to apply the theory to a specific practice in policing; in this case, the response of police officers trained in the CIT model to persons suspected to have a mental illness or those in the midst of a psychiatric crisis. Findings demonstrate the utility of this model in understanding factors that can shape an officer’s behavioral intentions, and help explain officers’ possible decisions when encountering individuals who have a suspected mental illness. Such findings may inform future training and research. Although CIT training appears to have a prominent impact on improving officers’ self-efficacy or perceived behavioral control, those aspects of the training that change attitudes are also very relevant in driving officers’ decisions. In terms of research, the Theory of Planned Behavior appears to be useful in understanding officers’ referral decisions, and future work should examine its utility regarding other aspects of officers’ decision-making (e.g., calling for assistance from a mobile crisis team, referring to substance abuse treatment services) as well as others’ decisions around facilitating mental health referrals (e.g., family members, concerned coworkers). Our study lays the groundwork for applying the Theory of Planned Behavior to a range of discretionary police behaviors that are of intense concern in light of sustained calls for police reform. These include police responses to not only individuals in mental health crises, but persons who use drugs, those experiencing homelessness, and instances in which police make decisions about the use of force. Each would benefit from interventions that cultivate behavioral intentions to improve health outcomes rather than diminish them. Such encounters require police officers to make decisions that could be shaped by stigma or other negative attitudes, and they can be of significant consequence. We would benefit from a more robust understanding of what factors drive the behavioral intentions of individual police officers, as well as insights into how to effectively shape them.
Funding
Research reported in this publication was supported by National Institute of Mental Health grant R01 MH082813 (“Modeling Officer-Level Effects of Crisis Intervention Team (CIT) Training”) to the first author. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or National Institute of Mental Health.
Footnotes
Conflict of interest The authors declare that they have no conflict of interest.
Consent to participate Informed consent was obtained from all individual participants included in the study.
References
- Ajzen I (1985). From intentions to actions: A theory of planned behavior. In: Action control: From cognition to behavior (Kuhl J, Beckmann J, Editors). SSSP Springer Series in Social Psychology. Springer [Google Scholar]
- Ajzen I (2002). Perceived behavioral control, self-efficacy, locus of control, and the Theory of Planned Behavior. Journal of Applied Social Psychology, 32(4), 665–683. 10.1111/j.1559-1816.2002.tb00236.x [DOI] [Google Scholar]
- Ajzen I, & Madden T (1986). Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. Journal of Experimental Social Psychology, 22, 453–474. [Google Scholar]
- Bahora M, Hanafi S, Chien VH, & Compton MT (2008). Preliminary evidence of effects of crisis intervention team training on self-efficacy and social distance. Administration and Policy in Mental Health and Mental Health Services Research, 35(3), 159–167. 10.1007/s10488-007-0153-8 [DOI] [PubMed] [Google Scholar]
- Bandura A (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215. 10.1037/0033-295X.84.2.191 [DOI] [PubMed] [Google Scholar]
- Bashirian S, Hidarnia A, Allahverdipour H, & Hajizadeh E (2012). Application of the Theory of Planned Behavior to predict drug abuse related behaviors among adolescents. Journal of Research in Health Sciences, 12(1), 54–60. [PubMed] [Google Scholar]
- Bonfine N, Ritter C, & Munetz MR (2014). Police officer perceptions of the impact of Crisis Intervention Team (CIT) programs. International Journal of Law and Psychiatry, 37(4), 341–350. 10.1016/j.ijlp.2014.02.004 [DOI] [PubMed] [Google Scholar]
- Boudreau F, & Godin G (2007). Using the Theory of Planned Behaviour to predict exercise intention in obese adults. Canadian Journal of Nursing Research, 39(2), 112–125. http://www.ncbi.nlm.nih.gov/pubmed/17679588 [PubMed] [Google Scholar]
- Broussard B, Krishan S, Hankerson-Dyson D, Husbands L, Stewart-Hutto T, & Compton MT (2011). Development and initial reliability and validity of four self-report measures used in research on interactions between police officers and individuals with mental illnesses. Psychiatry Research, 189(3), 458–462. 10.1016/j.psychres.2011.06.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Committee on Communication for Behavior Change in the 21st Century. (2002). Speaking of Health: Assessing Health Communication Strategies for Diverse Populations. National Academies Press. [PubMed] [Google Scholar]
- Compton MT, Bakeman R, Broussard B, D’Orio B, & Watson AC (2017). Police officers’ volunteering for (rather than being assigned to) Crisis Intervention Team (CIT) training: Evidence for a beneficial self-selection effect. Behavioral Sciences and the Law, 35, 470–479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compton MT, Bakeman R, Broussard B, Hankerson-Dyson D, Husbands L, Krishan S, Stewart-Hutto T, D’Orio BM, Oliva JR, Thompson NJ, & Watson AC (2014a). The police-based Crisis Intervention Team (CIT) model: I. Effects on officers’ knowledge, attitudes, and skills. Psychiatric Services, 65(4), 517–522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compton MT, Bakeman R, Broussard B, Hankerson-Dyson D, Husbands L, Krishan S, Stewart-Hutto T, D’Orio BM, Oliva JR, Thompson NJ, & Watson AC (2014b). The police-based Crisis Intervention Team (CIT) model: II. Effects on level of force and resolution, referral, and arrest. Psychiatric Services, 65(4):523–529. [DOI] [PubMed] [Google Scholar]
- Compton MT, Demir Neubert BN, Broussard B, Mcgriff JA, Morgan R, & Oliva JR (2011). Use of force preferences and perceived effectiveness of actions among Crisis Intervention Team (CIT) police officers and non-CIT officers in an escalating psychiatric crisis involving a subject with schizophrenia. Schizophrenia Bulletin, 37, 737–745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compton MT, & Esterberg ML (2005). Treatment delay in first-episode nonaffective psychosis: A pilot study with African American family members and the theory of planned behavior. Comprehensive Psychiatry, 46(4), 291–295. 10.1016/j.comppsych.2004.10.006 [DOI] [PubMed] [Google Scholar]
- Compton MT, Esterberg ML, McGee R, Kotwicki RJ, & Oliva JR (2006). Crisis Intervention Team training: Changes in knowledge, attitudes, and stigma related to schizophrenia. Psychiatric Services, 57(8), 1199–1202. 10.1176/ps.2006.57.8.1199 [DOI] [PubMed] [Google Scholar]
- Friedmann PD, Wilson D, Knudsen HK, Ducharme LJ, Welsh WN, Frisman L, Knight K, Lin HJ, James A, Albizu-Garcia CE, & Vocci FJ (2015). Effect of an organizational linkage intervention on staff perceptions of medication-assisted treatment and referral intentions in community corrections. Journal of Substance Abuse Treatment, 50, 50–58. 10.1016/j.jsat.2014.10.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Godin G, Fortin C, Mahnès BR, Nadeau D, Duval B, et al. (1993). University students’ intention to seek medical care promptly if symptoms of sexually transmitted diseases were suspected. Sexually Transmitted Diseases, 20, 100–104. [DOI] [PubMed] [Google Scholar]
- Godin G, & Kok G (1996). The Theory of Planned Behavior: A review of its applications to health-related behaviors. American Journal of Health Promotion, 11(2), 87–98. 10.4278/0890-1171-11.2.87 [DOI] [PubMed] [Google Scholar]
- Hanafi S, Bahora M, Demir BN, & Compton MT (2008). Incorporating Crisis Intervention Team (CIT) knowledge and skills into the daily work of police officers: A focus group study. Community Mental Health Journal, 44(6), 427–432. 10.1007/s10597-008-9145-8 [DOI] [PubMed] [Google Scholar]
- Hyland P, Boduszek D, Shevlin M, & Adamson G (2012). Investigating the latent structure of the Theory of Planned Behavior and its effectiveness in explaining intentions to participate in counseling among a sample of police officers. Journal of Police and Criminal Psychology, 27(2), 129–140. 10.1007/s11896-012-9103-9 [DOI] [Google Scholar]
- Ishoy GA (2016). The Theory of Planned Behavior and policing: How attitudes about behavior, subjective norms, and perceived behavioral control affect the discretionary enforcement decisions of police officers. Criminal Justice Studies, 29(4), 345–362. 10.1080/1478601X.2016.1225362 [DOI] [Google Scholar]
- Keller PH, & Miller MK (2015). Using the Theory of Planned Behavior to predict crime reporting intent. Applied Psychology in Criminal Justice, 11, 193–206. [Google Scholar]
- Maio GR, & Haddock G (2010). The Psychology of Attitudes and Attitude Change. SAGE Publications Ltd. 10.4135/9781446214299 [DOI] [Google Scholar]
- O’Boyle CA, Henly SJ, & Larson E (2001). Understanding adherence to hand hygiene recommendations: The Theory of Planned Behavior. American Journal of Infection Control, 29(6), 352–360. 10.1067/mic.2001.18405 [DOI] [PubMed] [Google Scholar]
- Park H, & Blenkinsopp J (2008). Whistleblowing as planned behaviour—A survey of South Korean police officers. Journal of Business Ethics, 85, 545–556. [Google Scholar]
- Perkins MB, Jensen PS, Jaccard J, Gollwitzer P, Oettingen G, Pappadopulos E, & Hoagwood KE (2007). Applying theory-driven approaches to understanding and modifying clinicians’ behavior: What do we know? Psychiatric Services, 58(3), 342–348. 10.1176/ps.2007.58.3.342 [DOI] [PubMed] [Google Scholar]
- Ross LT, Ross TP, Farber S, Davidson C, Trevino M, & Hawkins A (2011). The Theory of Planned Behavior and helmet use among college students. American Journal of Health Behavior, 35(5), 581–590. 10.5993/AJHB.35.5.7 [DOI] [PubMed] [Google Scholar]
- Şimşekoğlu Ö, & Lajunen T (2008). Social psychology of seat belt use: A comparison of Theory of Planned Behavior and Health Belief Model. Transportation Research Part F: Traffic Psychology and Behaviour, 11(3), 181–191. 10.1016/j.trf.2007.10.001 [DOI] [Google Scholar]
- Steele SK, & Porche DJ (2005). Testing the Theory of Planned Behavior to predict mammography intention. Nursing Research, 54(5), 332–338. [DOI] [PubMed] [Google Scholar]
- Strecher VJ, Rosenstock IM (1997). Health Behavior and Health Education: Theory, Research, and Practice (Glanz K, Marcus LF, Rimer BK, Second Edition). Jossey-Bass Publishers. [Google Scholar]
- Topa G, & Moriano JA (2010). Theory of Planned Behavior and smoking: Meta-analysis and SEM model. Substance Abuse and Rehabilitation, 1, 23–33. 10.2147/sar.s15168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson AC, Compton MT, & Draine JN (2017). The Crisis Intervention Team (CIT) model: An evidenced-based policing practice? Behavioral Sciences and the Law, 35, 431–441. [DOI] [PubMed] [Google Scholar]