

1. Introduction
Globally, pain impacts billions of people daily [10,37,59]. Given its ubiquity, and its accompanying disability and mortality, there is ample reason to regard pain as a major global health burden and priority [3,29]. Estimating prevalence across countries, and assessing whether and how these estimates vary, is an important step in understanding the global challenge of pain.
Studies around the world that use survey data to estimate pain prevalence suggest there is wide cross-national variation [4,24,25,33,40,41]. A meta-analysis of 25 studies estimating prevalence of chronic widespread pain across countries and cultural groups in Europe, Asia, and the Americas, found estimates ranging between 0% and 24% [50]. This variation may be partly explained by methodological difference across studies and partly by cultural idiosyncrasies [5,15,29]. It may also be explained by ‘compositional’ individual-level factors [6]. For instance, variations in the prevalence of any health condition cross-nationally is frequently a function of several demographic characteristics that are important determinants of health. Studies have consistently shown that women report pain more frequently than men, that pain prevalence increases with age, and that pain prevalence tends to be higher in rural as opposed to urban areas [4,7,25,26,33,40,50,57]. As a result, older populations with a higher proportion of women and rural residents would be expected to have higher pain prevalence.
While research frequently considers these types of individual factors in studies of prevalence, they are unlikely to fully explain cross-national variations and run the risk of underrepresenting the impact of systemic processes on cross-national inequalities, which in turn has implications for the development of appropriate health policies [6]. Research on global health inequalities has identified a number of consequential ‘contextual’ country-level factors [64,70]. In particular, research has implicated macro political and economic factors as determinants of health. These include the impact of national health expenditures, national income, and quality of governance on life expectancy and mortality [39,43,44,49]. Social inequalities are also an important factor when considering health disparities [2]. Studies demonstrate significant relationships between within-country income inequality, as measured by indicators like the Gini coefficient, and a variety of health outcomes [56]. Gender inequality has also been associated with some health outcomes [61] including musculoskeletal pain [11], child mortality [14], mental health and overall self-rated health [45]. While these studies have focused on other health outcomes, we hypothesize that these types of country-level contextual factors would also impact pain, given that there is a close association between chronic pain and other health conditions [9,13,21,22,31,62]. The extent to which country-level factors influence pain prevalence has, however, not been adequately examined.
The current study estimates country-level pain prevalence from a single global survey with a consistent definition of pain and instrumentation protocol. We combine survey data with country-level indicators gathered from global databases to create a multilevel dataset for 52 countries. The study uses these data to: (a) estimate and compare pain prevalence across countries, and (b) explore the degree to which variations in prevalence are explained by country-level contextual factors commonly considered as macro-determinants of health.
2. Methods
2.1. Ethical clearance
The study protocol was approved by the Mount Saint Vincent University Research Ethics Board [2021-014].
2.2. World Health Survey
Data on pain and individual-level demographic characteristics were obtained from the World Health Survey (WHS), implemented between 2002 and 2004 by the World Health Organization. The WHS involved cross-sectional data collection in 70 countries across five continents. Countries participating in the WHS were chosen to provide a range of different national income categories, and to include countries with large adult populations. These data have been commonly used for comparative research on health [35,36,66]. Details of the WHS survey and data are provided elsewhere [68,74].
Each respective Ministry of Health within the 70 countries designed a local sampling strategy based on World Health Organization guidelines, and administered standardized questionnaires. A nationally representative, multistage cluster design was used in all countries except China, Comoros, Cote d'Ivoire, Croatia, India, and Russia, where the WHS was carried out in more geographically limited regions. Designs were based on probability strategies, with sampling frames covering 100% of eligible adults aged 18+ stratified by gender, age, and urban/rural setting [68]. Weights that account for sampling design and non-response and assure that prevalence estimates are representative of total country populations are provided for most countries. These sampling weights are applied as in other publications using these data [72].
Questionnaires went through back- and forward- translations into multiple languages, with end results being checked by linguists. Data collection was completed by trained interviewers, either face-to-face or by telephone. The individual country response rates ranged from 63% to 99% [72]. Ethics boards at each study site reviewed study protocols. Informed consent was obtained from all participants. The WHS was carried out in accordance with the latest version of the Declaration of Helsinki.
Of the 70 initial countries, 18 were excluded from the current analysis. One country did not make data available publicly. Ten countries do not include sampling weights, and since these are required for prevalence estimates, these countries were excluded. Five were excluded because of a high level of missing data (>20%) on the pain item used to estimate prevalence. Norway was excluded because its data did not include information on rural versus urban residence, a variable we use in our modeling of pain prevalence. After preliminary analysis, Comoros (population of <600,000 in 2003) was excluded because it was an outlier with respect to pain prevalence; its prevalence was more than 3.5 standard deviations above the cross-country mean.
For the purpose of these analyses, we considered all respondents aged 25+ from the remaining 52 countries. Starting the sample at this age maximizes the chance that the sample would be comprised of working age adults with completed education. Completed education level is one of the contextual variables in the analysis. Sensitivity analyses that included respondents 18+ yielded comparable results. This provided an initial sample size of 210,763 possible respondents. A small percentage of these respondents had missing data in variables of interest. Respondents with missing data in one variable of interest tended to have missing data across multiple variables. Subjects with any missing information were excluded (N=10,901), resulting in a final sample of N=199,862 for all analyses. The average within-country sample size was 3,844, with numbers ranging from a low of 620 in Luxembourg to a high of 32,028 in Mexico. Thirty-seven countries included at least 2,000 observations. See Supplementary Table 1 for a list of sample sizes by country and region.
2.3. Measuring pain
Pain is assessed by the following WHS question asked of all participants: “Overall in the last 30 days, how much of bodily aches or pains did you have?” with answer options being none, mild, moderate, severe, and extreme. The question did not specify the location of pain in the body or specific length of time for which pain has been present. We dichotomized the variable as none or mild versus moderate, severe, or extreme pain; a threshold meant to capture meaningful levels of pain. Previous research has indicated that compared to mild pain, moderate and severe pain strongly predict mortality [30] and the development of functional limitations at much earlier ages [20]. Thus, we followed the ‘no worse than mild pain’ model of pain, a designation that is indicative of analgesic control and carries significant health and economic benefits to patients [55]. Sensitivity analyses were conducted to calculate pain prevalence resulting from alternate measurement treatments (e.g. no pain vs. any pain) and to assess whether these alternate categorizations of pain resulted in different rank orderings of countries. Spearman's rank correlations indicated a strong, positive monotonic correlation between pain prevalence rankings across different categorizations of pain, indicating a congruence across these.
2.4. Demographic predictors
Models first adjust prevalence for three individual-level demographic variables that come from WHS data. These include interviewer-observed gender (dichotomized as woman=1 or man=0), self-reported age in years (categorized in ten-year increments as 25–34, 35–44, 45–54, 55–64, and 65 or older), and rural/urban setting (rural=1 or urban=0). We avoided over-controlling for individual-level variables as the current study prioritizes the impact of contextual variables on pain.
2.5. Country-level contextual predictors
We combined individual-level information from the WHS with country-level contextual covariates assembled from a series of global data banks, such as World Bank and United Nations Development Programme, to derive a dataset for the analysis. The contextual variables represent domains of socioeconomic, political, cultural, and environmental conditions, selected based on availability of data, and previous literature on contextual factors considered to impact population health [2,71].
When available, these measures are taken for the year 2003, the midpoint of the WHS data collection. In a small number of instances, for a few of the country-level variables, information for the year 2003 was not available. In these cases, the measure came from the closest year for which data were available. Additional sensitivity analyses tested for the impact of including data from different years by modeling a variable that measured the difference between the year 2003 and the year in which data was observed. No bias was identified.
The following are the country-level contextual variables:
1) The Gini Index (Gini): a measure of economic inequality that ranges from 0 (no inequality) to 100 (totally unequal) [54].
2) Gross National Income (GNI): measured in current U.S. dollars per capita.
3) Average years of education completed by those age 25+ (Education).
4) Total labour force participation rate (TLFP): expressed as a percentage of the population.
5) Life expectancy at birth (LE), which serves as a proxy for the overall population health.
6) Health expenditure (HE%GDP): annual health expenditure expressed as a percentage of GDP.
7) Population density (Pop Density): number of residents per square kilometre.
6) The Gender Inequality Index (GII): ranges from 0 to 1, with higher scores indicating more inequalities between genders and greater disadvantages for women [27]. The index is derived from a series of dimensions that include educational attainment, economic and political participation, and reproductive health issues.
7) Quality of Government index (QoG). constructed using a principal-component factor analysis, with promax rotation, of six worldwide governance indicators (WGI) provided by the World Bank. These indicators are commonly used as proxies for governance quality [42,44]. The factor analysis resulted in one factor containing all six governance indicators (alpha=0.948). High internal consistency and correlation between the predicted factor and a summed score of the six items (r=0.999, p=0.000) indicated that a summed, factor-based score was an appropriate and parsimonious choice. All governance indicators have values of −2.5 to 2.5; these are summed with a higher score indicating better governance.
To allow for comparability across these country-level contextual variables, all were standardized to have a mean of 0 and standard deviation of 1 in multivariate regression equations.
Finally, to account for potential regional heterogeneity in pain reporting across world regions, the 52 countries were categorized into one of six world regions according to the World Health Organization regional groupings [73]: the Americas, Africa, Europe, Eastern Mediterranean, Western Pacific, and South-East Asia. These were entered into models as dummy variables with Western Pacific, the region that was found to have the overall lowest levels of pain prevalence, as the comparison category. Since the WHO regional groupings differ from other standard ways of grouping countries, supplemental analyses tested other reasonable combinations and the overall pattern of findings did not differ from those reported herein.
Supplementary Tables 2, 3, and 4 provide details on country-level variables, unstandardized raw data by country, and results of the factor analysis used to create the Quality of Government variable, respectively.
2.6. Statistical analysis
We first calculate a standardized pain prevalence for each country, with the standardization being based on the global age and sex distribution for the year 2003 obtained from the United Nations Population Database [67]. This allows for a comparison of prevalence and an assessment of variation after accounting for cross-national age and sex differences.
Next, we examined associations between each separate individual- and country-level variable and pain by pooling data from all countries and calculating zero-order correlations. Using these pooled data, we then modeled the variation in the prevalence across countries by fitting nested multilevel random intercept logistic regression models predicting the odds that an individual living in a particular country reports pain. Because odds can be used to calculate predicted probabilities of reporting pain, and these probabilities translate into prevalence rates, higher odds are interpreted directly as higher prevalence. Multilevel models fit two types of equations. The first is the individual-level equation that estimates fixed effects, which capture the influence of covariates on the odds that an individual in any country reports pain. The covariates are both at the individual- and country-level. The second is the country-level equation to assess the random effect of country, which quantifies the variance in the odds of reporting pain that is a function of the unmeasured country-specific heterogeneity that remains after controlling for fixed effect covariates. This random effect accounts for the idiosyncratic likelihood of reporting pain that is unique to each country.
We tested a series of nested models, each of which adds different variables to a base model. The base model (Model 1) is an individual-level only model that adjusts for age, sex, and urban/rural residence. The magnitude of the random effect is expected to change as country-level variables are added, indicating the degree to which contextual covariates account for the variation in pain prevalence. Because a high correlation between a number of the contextual country-level variables is likely, we assessed the potential for, and developed models to avoid, collinearity. To do this, bivariate correlations were first examined across predictors. These are shown Table 1. As can be seen, there are some very high correlations. For instance, higher average education is negatively and very strongly correlated with the Gender Inequality Index, meaning that these two variables will share a degree of variance that may be too large to adequately assess the independent impact of either variable when both are included in the same model. Thus, we tested variance inflation factors (VIF) to obtain a statistical basis for determining variables to be included in the same models [65]. There is little consensus on a cut-off that is most appropriate; however, most conventions dictate that a VIF greater than 10 indicates a danger of collinearity [17,53,69]. The VIF results are provided in Supplementary Table 5. Based on the VIF findings, the final presentation comprises several models, all of which have VIF values below the cut-off of 10. As noted, Model 1 is the base that includes only the individual-level variables: age, sex, and rural/urban setting. Model 2 adds a set of country-level contextual variables that do not pose shared variance problems. In Models 3 to 5, other contextual variables are added to Model 2 that individually do not pose issues, but would if entered together. In this way, the analysis examines the largest set of predictor variables possible while avoiding collinearity.
Table 1.
Weighted Pearson correlation matrix for country-level variables.
| Gini | GNI | Education | TLFP | QoG | HE%GDP | LE | GII | Pop Density | |
|---|---|---|---|---|---|---|---|---|---|
| Gini1 | |||||||||
| GNI2 | −0.12 | ||||||||
| Education3 | 0.14 | 0.49 | |||||||
| TLFP4 | 0.13 | −0.14 | −0.20 | ||||||
| QoG5 | 0.23 | 0.78 | 0.51 | −0.21 | |||||
| HE%GDP6 | 0.37 | 0.57 | 0.50 | 0.09 | 0.70 | ||||
| LE7 | 0.03 | 0.58 | 0.48 | −0.34 | 0.58 | 0.34 | |||
| GII8 | −0.01 | −0.72 | −0.74 | −0.08 | −0.71 | −0.62 | −0.69 | ||
| Pop Density9 | −0.36 | −0.23 | −0.29 | −0.16 | −0.35 | −0.53 | −0.01 | 0.39 | |
| Country Region | |||||||||
| Europe | −0.30 | 0.54 | 0.65 | −0.29 | 0.43 | 0.45 | 0.40 | −0.66 | −0.27 |
| Africa | 0.15 | −0.17 | −0.25 | 0.42 | −0.09 | 0.07 | −0.75 | 0.29 | −0.23 |
| Americas | 0.70 | 0.06 | 0.08 | 0.10 | 0.24 | 0.44 | 0.35 | −0.10 | −0.29 |
| SE Asia | −0.29 | −0.27 | −0.32 | −0.01 | −0.32 | −0.45 | −0.12 | 0.44 | 0.72 |
| W Pacific | 0.09 | −0.11 | 0.12 | 0.25 | −0.03 | −0.17 | 0.18 | −0.23 | 0.02 |
| E Medi | −0.26 | −0.11 | −0.30 | −0.40 | −0.26 | −0.37 | −0.09 | 0.24 | −0.06 |
Note. All correlations are significant at p<0.001.
Gini Index,
Gross National Income in current U.S. dollars, per capita,
Average years of education (25+ years old),
Total Labour Force Participation,
Quality of Government Index,
Health Expenditure (%GDP),
Life Expectancy from birth,
Gender Inequality Index,
Population density (per sq. km).
In a final procedure, results of the multilevel analysis were used to calculate an adjusted pain prevalence for each of the 52 countries in the data. The country-level prevalence rates that adjust for the effects of the individual- and country-level variables included in particular models were computed by summing the resulting fixed and random effects from logistic regression models with random effects (i.e. intercepts) by country [25] such that:
We calculated the coefficient of variation (CV) to assess the disparity in prevalence estimates across countries for each model’s predicted country-level prevalence rates. Thus, the coefficient of variation, which is the ratio of the standard deviation in prevalence to mean prevalence, allows us to assess how much variation in prevalence is explained by the contextual factors included in each model.
Data manipulations and descriptive analyses were performed using Stata 16.1 [63], while multilevel effects models were estimated using SPSS 26 software [38].
3. Results
Table 2 presents unweighted descriptive statistics for study variables. For the individual-level variables, we report statistics for samples pooled across countries within regions, and the total sample pooled across all countries. Sample sizes are also shown. The overall unweighted prevalence of reported pain for the total combined sample is 28%. Regionally, the lowest unweighted prevalence is for the sample that combines observations from across the five Western Pacific countries at 21%, and the highest prevalence is for the 18 European countries at 34%.
Table 2.
Unweighted descriptive statistics showing proportions and means for study variables by world region.
| Europe | Africa | Americas | SE Asia | E Mediterranean | W Pacific | Total | |
|---|---|---|---|---|---|---|---|
| Countries (N) | 18 | 14 | 6 | 5 | 4 | 5 | 52 |
| Participants (N) | 39,036 | 42,608 | 50,363 | 29,857 | 13,694 | 24,304 | 199,862 |
| Individual-Level (proportions) | |||||||
| With pain | 0.34 | 0.28 | 0.26 | 0.30 | 0.31 | 0.21 | 0.28 |
| Age | |||||||
| 25-34 | 0.20 | 0.36 | 0.30 | 0.30 | 0.30 | 0.30 | 0.29 |
| 35-44 | 0.23 | 0.26 | 0.26 | 0.28 | 0.31 | 0.30 | 0.27 |
| 45-54 | 0.19 | 0.16 | 0.18 | 0.20 | 0.18 | 0.19 | 0.18 |
| 55-64 | 0.15 | 0.10 | 0.12 | 0.11 | 0.10 | 0.11 | 0.12 |
| 65+ | 0.23 | 0.10 | 0.14 | 0.11 | 0.11 | 0.10 | 0.14 |
| Woman | 0.60 | 0.55 | 0.56 | 0.54 | 0.51 | 0.54 | 0.56 |
| Rural | 0.37 | 0.64 | 0.28 | 0.77 | 0.46 | 0.54 | 0.49 |
| Country-Level (means) | |||||||
| Gini1 | 35.57 | 43.00 | 51.21 | 38.26 | 36.29 | 42.29 | 42.37 |
| GNI(/1000)2 | 8.82 | 0.95 | 5.60 | 0.47 | 3.72 | 1.61 | 3.86 |
| Education3 | 9.13 | 4.68 | 7.04 | 4.96 | 4.68 | 6.91 | 6.46 |
| TLFP4 | 56.13 | 68.60 | 61.02 | 66.03 | 51.11 | 68.32 | 62.64 |
| QoG5 | 1.36 | −2.52 | −0.44 | −4.25 | −2.22 | −2.57 | −1.48 |
| HE%GDP6 | 6.23 | 5.53 | 5.99 | 3.45 | 3.95 | 3.72 | 5.15 |
| LE7 | 72.38 | 53.22 | 74.03 | 65.71 | 69.37 | 69.54 | 67.16 |
| GII8 | 0.32 | 0.61 | 0.45 | 0.58 | 0.50 | 0.39 | 0.47 |
| Pop Density9 | 66.21 | 91.93 | 55.33 | 364.83 | 111.22 | 169.38 | 129.19 |
Note. Countries organized into six world regions according to World Health Organization regional groupings.
Gini Index,
Gross National Income in current U.S. dollars, per capita (/1000),
Average years of education (25+ years old),
Total Labour Force Participation,
Quality of Government Index,
Health Expenditure (%GDP),
Life Expectancy from birth,
Gender Inequality Index,
Population density (per sq. km).
For the country-level contextual variables, we report means for countries grouped within regions and the total for all 52 countries prior to standardization. There is variation in country-level variables across regions. Generally, the 18 countries in Europe have the least income and gender inequality as measured by the Gini and the GII, and the highest gross national income (per capita GNI), average years of education, quality of government (QoG), health expenditure as a proportion of GDP, and life expectancy. The highest income inequality is found across countries in the Americas, while African countries display the highest gender inequalities. Gross National Income, Quality of Government, and health expenditures are lowest, and population density is highest, in the South-East Asian countries.
The prevalence of pain in each country, standardized by age and sex, is displayed as the proportion reporting pain, with 95% confidence intervals, in Figure 1. The figure clearly shows a wide range in prevalence. China has the lowest proportion with pain at 0.099 (95% CI: 0.090 - 0.108) and Morocco has the highest proportion at 0.503 (95% CI: 0.487 – 0.519). However, aside from some countries on the higher and lower end, most report a prevalence within a somewhat narrower range. The average for the combined sample across the 52 countries is 0.275 with a cross-country standard deviation of 0.084. Thirty-eight countries fall within one standardized unit from the cross-country mean with a prevalence between 0.191 and 0.359. Eight countries fall under a prevalence of 0.191 and six countries have a prevalence over 0.359. Supplementary Table 6 provides details for both unstandardized (crude) and standardized point prevalence estimates.
Figure 1.
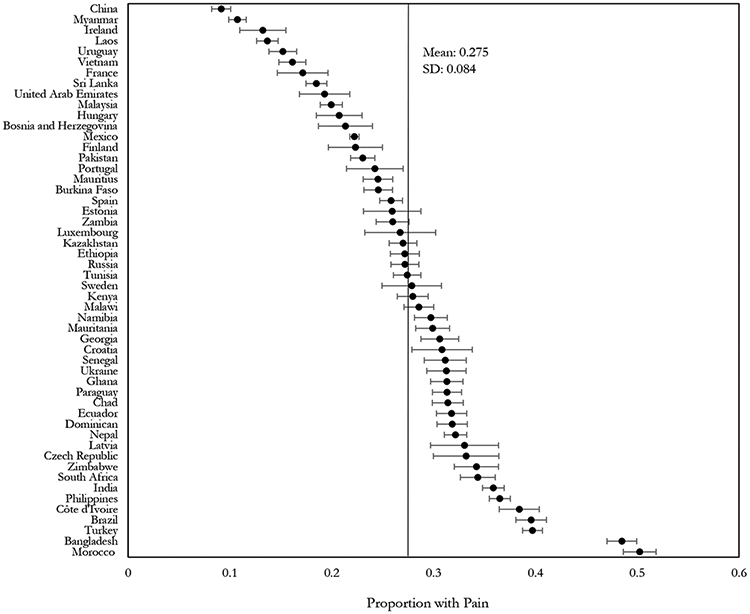
Age and sex standardized point estimates (with 95% CI) of prevalence of pain in 52 countries, 2002-2004 World Health Survey. Vertical line represents the cross-country prevalence.
The first column of results in Table 3 shows the zero-order correlations with 95% confidence intervals and p-values that indicate whether there is an association between each individual covariate and the probability of reporting pain for the total sample. Without controls, all of the variables, with the exception of Quality of Government and life expectancy, appear to have an association with reported pain.
Table 3.
Zero-order correlations and multilevel logistic models showing associations between individual- and country-level variables and pain.
| Zero-Order Correlation |
Model 1 OR (95% CI) |
Model 2 OR (95% CI) |
Model 3 OR (95% CI) |
Model 4 OR (95% CI) |
Model 5 OR (95% CI) |
|
|---|---|---|---|---|---|---|
| Intercept | 0.126 (0.109-0.145) 0.000 |
0.068 (0.042-0.110) 0.000 |
0.088 (0.058-0.134) 0.000 |
0.069 (0.042-0.112) 0.000 |
0.076 (0.048–0.121) 0.000 |
|
| Age | ||||||
| 25-34 | −0.140 (−0.144-0.135) 0.000 |
- | - | - | - | - |
| 35-44 | −0.059 (−0.063-−0.055) 0.000 |
1.362 (1.282-1.448) 0.000 |
1.362 (1.282-1.448) 0.000 |
1.362 (1.282-1.448) 0.000 |
1.362 (1.282-1.448) 0.000 |
1.362 (1.282-1.448) 0.000 |
| 45-54 | 0.020 (0.015-0.024) 0.000 |
1.910 (1.812-2.013) 0.000 |
1.910 (1.812-2.013) 0.000 |
1.910 (1.812-2.013) 0.000 |
1.910 (1.812-2.013) 0.000 |
1.910 (1.812-2.013) 0.000 |
| 55-64 | 0.076 (0.072-0.081) 0.000 |
2.762 (2.493-3.061) 0.000 |
2.762 (2.493-3.061) 0.000 |
2.762 (2.493-3.061) 0.000 |
2.762 (2.493-3.061) 0.000 |
2.762 (2.493-3.061) 0.000 |
| 65+ | 0.178 (0.174-0.183) 0.000 |
4.850 (4.115-5.716) 0.000 |
4.850 (4.115-5.716) 0.000 |
4.850 (4.115-5.716) 0.000 |
4.850 (4.115-5.716) 0.000 |
4.850 (4.115-5.716) 0.000 |
| Woman | 0.145 (0.141-0.150) 0.000 |
1.973 (1.746-2.228) 0.000 |
1.973 (1.746-2.228) 0.000 |
1.973 (1.746-2.228) 0.000 |
1.973 (1.746-2.228) 0.000 |
1.973 (1.746-2.228) 0.000 |
| Rural | 0.018 (0.013-0.022) 0.000 |
1.199(1.053-1.365) 0.000 |
1.199(1.053-1.365) 0.000 |
1.199(1.053-1.365) 0.000 |
1.199(1.053-1.365) 0.000 |
1.199(1.053-1.365) 0.000 |
| GII1 | 0.049 (0.045-0.053) 0.000 |
1.307 (1.073-1.437) 0.001 |
||||
| QoG2 | −0.001(−0.006-−0.003) 0.534 |
0.918 (0.796-1.059) 0.242 |
||||
| LE3 | 0.003 (−0.001-−0.008) 0.134 |
0.785 (0.620-0.995) 0.045 |
||||
| Gini4 | 0.031 (0.026-0.035) 0.000 |
1.242 (1.073-1.437) 0.004 |
1.225 (1.073-1.398) 0.003 |
1.255 (1.094-1.439) 0.001 |
1.212 (1.042-1.410) 0.013 |
|
| GNI5 | −0.041(−0.045-−0.037) 0.000 |
0.935 (0.873-1.001) 0.054 |
0.977 (0.909-1.051) 0.534 |
0.977 (0.889-1.073) 0.622 |
0.979 (0.915-1.048) 0.544 |
|
| Education6 | 0.005 (0.001-0.010) 0.022 |
0.944(0.827-1.077) 0.391 |
0.977 (0.858-1.113) 0.725 |
0.943 (0.834-1.066) 0.347 |
0.946 (0.841-1.065) 0.357 |
|
| TLFP7 | −0.047(−0.052-−0.043) 0.000 |
0.989 (0.890-1.099) 0.838 |
0.954 (0.865-1.052) 0.345 |
0.961 (0.847-1.089) 0.532 |
0.927 (0.804-1.068) 0.294 |
|
| HE%GDP8 | 0.012 (0.008-0.017) 0.000 |
0.966 (0.861-1.084) 0.555 |
1.025 (0.916-1.146) 0.668 |
0.976 (0.879-1.084) 0.654 |
0.959 (0.862-1.066) 0.437 |
|
| Pop Density9 | 0.089 (0.085-0.094) 0.000 |
1.264 (1.049-1.523) 0.014 |
1.288 (1.136-1.461) 0.000 |
1.276 (1.076-1.513) 0.005 |
1.304 (1.123-1.515) 0.001 |
|
| Region | ||||||
| Europe | 0.020 (0.016-0.025) 0.000 |
3.194 (1.831-5.572) 0.000 |
3.090 (1.461-5.061) 0.000 |
3.254 (1.897-5.582) 0.000 |
2.990 (1.766-5.062) 0.000 |
|
| E Medi | −0.051 (−0.055-−0.047) 0.000 |
2.656 (1.334-5.285) 0.005 |
1.855 (0.953-3.611) 0.069 |
2.521 (1.236-5.140) 0.011 |
2.318 (1.141-4.710) 0.020 |
|
| Americas | 0.019 (0.014-0.023) 0.000 |
1.816 (1.026-3.214) 0.041 |
1.401 (0.851-2.304) 0.185 |
1.779(1.010-3.134) 0.046 |
1.966 (1.150-3.359) 0.013 |
|
| Africa | −0.026 (−0.031-−0.022) 0.000 |
2.054 (1.210-3.487) 0.008 |
1.303 (0.799-2.124) 0.289 |
2.044 (1.220-3.423) 0.007 |
1.345 (0.730-2.479) 0.342 |
|
| SE Asia | 0.057 (0.053-0.061) 0.000 |
1.289 (0.608-2.734) 0.508 |
0.889 (0.471-1.677) 0.716 |
1.227 (0.573-2.629) 0.599 |
1.078 (0.522-2.229) 0.839 |
|
| W Pacific | −0.046 (−0.050-−0.042) 0.000 |
- | - | - | - | |
| N | 199861 | 199861 | 199861 | 199861 | 199861 | |
| Random Intercept | 0.256 | 0.188 | 0.161 | 0.188 | 0.179 | |
| 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | ||
| AIC | 1575838859.653 | 1575838917.394 | 1575838916.776 | 1575838921.395 | 1575838917.504 | |
Note. Table presents odds ratios with 95% confidence intervals in parentheses and p-values in italics.
Gender Inequality Index,
Quality of Government Index,
Life Expectancy from birth,
Gini Index,
Gross National Income in current U.S. dollars, per capita,
Average years of education (25+ years old),
Total Labour Force Participation,
Health Expenditure (%GDP),
Population density (per sq. km).
The remaining columns in Table 3 present the odds ratios of reporting pain for five multilevel logistic regression models with 95% confidence intervals and p-values. Model 1 shows associations between pain and individual-level covariates. Women (OR=1.973), older persons (OR=4.850), and rural residents (OR=1.199) have higher odds of reporting pain. The magnitude of these associations is consistent across all our models.
Models 2-5 present associations that include both individual- and country-level covariates. Model 2 shows that living in a country with a higher level of income inequality (i.e., higher Gini Index) predicts higher odds of reporting pain (OR=1.242; 95% CI: 1.073-1.437). This effect remains stable across models 3-5. Because contextual covariates are standardized, odds are interpreted as the expected change in pain prevalence given a standard deviation change in the predictor. A one standard deviation change in GNI is associated with 21-26% higher odds of pain. Population density (Pop Density) is also associated with a 26% higher odds of reporting pain (OR=1.264; 95% CI: 1.049-1.523) in model 2, and this effect persists in every following model (26-30% higher odds). The Gender Inequality Index (GII) in Model 3 is associated with pain (OR=1.307; 95% CI: 1.073-1.437), indicating that pain prevalence is 31% higher for each standard unit of gender inequality. We subsequently tested an interaction between gender (woman=1) and the Gender Inequality Index. The result (OR=1.085; 95% CI: 0.999-1.177) indicates that the disadvantage that women have in experiencing pain may be even greater in countries with more gender inequality. However, both men and women are disadvantaged by country-level gender inequality such that both are more likely to report pain in countries with high gender inequality compared to countries with low gender inequality. A standard unit increase in life expectancy (LE) is associated with 21% lower odds of pain in Model 5 (OR=0.785; 95% CI: 0.620-0.995). Covariates not associated with the odds of reporting pain in multilevel models include Quality of Government (QoG), average level of education (Education), Total Labor Force Participation (TLFP) and health expenditures as a proportion of GDP (HE%GDP). Gross National Income (GNI) is associated with slightly lower odds of reporting pain in Model 2 (OR=0.935; 95% CI: 0.873-1.001), but this is a small effect, and does not carry over in other models.
Region is associated with the odds of reporting pain. The main finding here is that, adjusting for other factors, living in a European country predicts higher odds of reporting pain relative to living in the Western Pacific region, which has the lowest odds. This finding remains stable across models 2-5. Otherwise, living in an Eastern Mediterranean country is associated with higher odds in pain compared to the Western Pacific, although the strength of effect is less consistent across models compared to living in Europe. Living in Africa and the Americas is associated with the odds of reporting pain in some of the models and not others, with greater odds of pain in comparison to the Western Pacific.
The random effect in model 1 is 0.256 and indicates substantial variance in the odds of reporting pain between countries. The random effect is reduced when country-level variables are added to models. For instance, the random intercept reduces by about 27% between models 1 and 2, after country-level variables are added to the model in addition to individual-level variables. The random intercept is at its lowest point in Model 3, having reduced by 37% from model 1. This occurs when adjusting for the Gender Inequality Index, suggesting that this model accounts for more cross-country variance than others. However, a large portion of the heterogeneity in pain prevalence remains unexplained by covariates across the models.
To illustrate the unexplained variation further, we present in Figure 2 the range and variance in pain across countries in the age-/sex-standardized prevalence and the predicted prevalence based on each of the multilevel models. Each dot in the figure is the prevalence of pain in one country given the specific type of estimate. The countries with the highest and lowest predicted values are listed with their predicted prevalence, shown as the proportion reporting pain, in order to assess the range. The Figure illustrates graphically the wide range in prevalence in age- and sex-standardized estimates. Notably, adjustment for age, gender, and rural/urban setting in Model 1 produces no reduction in the large variation of prevalence across countries. In fact, based on the Coefficient of Variation (CV) and the range, the variation increases, likely due to how controlling for age, gender, and rural setting interacts with the unique population distributions in each country to shift pain prevalence further from the grand mean. However, when additionally adjusted for country-level factors, the estimated variance in prevalence decreases, as can be seen in a narrowing of the range and a decrease in CV. Consistent with the random effect in the multilevel model, the smallest variation is seen in model 3. This model included individual-level factors, the Gini index, Gross National Income, average education, Total Labor Force Participation, health expenditures, population density, and the Gender Inequality Index. There is a definite tightening in the predicted values for this model. Nonetheless, a substantial amount of variation remains. The adjusted rates in Model 3 vary from a predicted low of 0.152 in Ireland to a predicted high of 0.432 in Morocco. The CV drops to .252 for this model, which represents a 25% reduction in the CV in comparison to Model 1.
Figure 2.
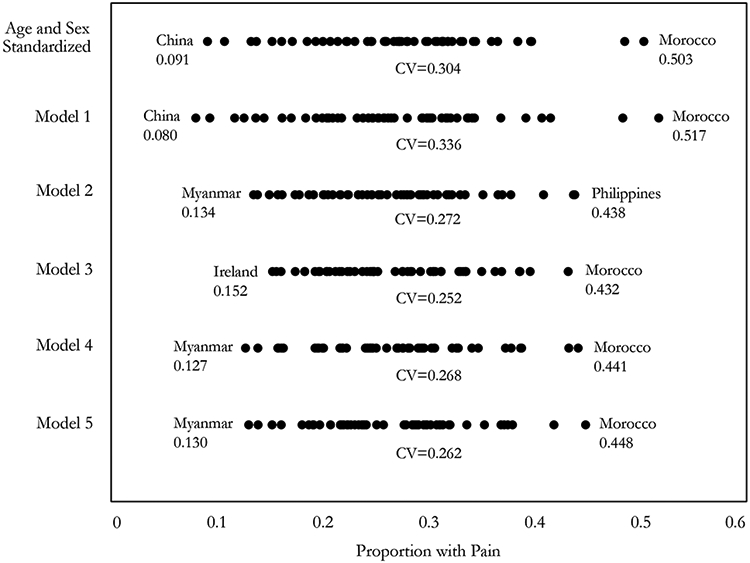
Estimated prevalence of pain by country. Unstandardized refers to raw estimates from WHS samples. Standardized estimates are standardized by global population in 2003. Model 1 is adjusted for individual factors: age, gender, and rural setting. Model 2 is adjusted for individual factors plus several country-level factors: Gini, GNI, education, TLFP, health expenditure, and population density. Model 3 adds GII to variables in Model 2. Model 4 adds QoG to variables in Model 2. Model 5 adds LE to variables in Model 2.
We conducted sensitivity analyses in which we dichotomized the pain outcome as no pain versus any pain. The pain prevalence estimated for this definition is shown in Supplementary Figure 1. The average prevalence for the combined sample across 52 countries doubles to 0.532, with a standard deviation of 0.077. However, the wide range in pain prevalence across countries remains, ranging from 0.237 to 0.784, in Ireland and Bangladesh respectively. The ranking of pain across countries is also largely the same (rs=0.81). Likewise, with the no vs. any pain categorization as outcome, the inclusion of country-level variables in multilevel models results in a reduction in the CV of up to 20% compared to model 1, even though there is an overall lower level of variation between countries. This confirms that the country-level variables are largely insensitive to the categorization of pain.
4. Discussion
We examined prevalence of moderate to extreme pain among adults aged 25+ across 52 countries using data from the 2002 - 2004 World Health Survey (WHS). The cross-country average reporting pain over the 30 days preceding the interview was 27.5%, and ranged from a minimum of 9.9% in China to a maximum of 50.3% in Morocco. Though not directly comparable, this pain prevalence is not radically different from that in Jackson et al. [40], who reported pooled prevalence of unspecified persistent pain to be 34% across studies and lower- and middle- income countries. Also consistent with previous literature, we found substantial variation in pain prevalence across countries [4,24,26,33,40,50,60]. This variation exists despite the information on pain coming from a single data source - the World Health Survey - that used a standardized measure across countries.
Like previous research, this study found that the odds of experiencing pain is higher for women, older persons, and those living in rural settings [8,19,26,28,40,50,60]. These individual-level characteristics –age, sex, and rural/urban residence—did not explain the cross-country variation in pain prevalence. Also comparable to the findings of similar research, the observed cross-national variation could not be completely explained with the inclusion of higher-level variables. For instance, research based on the Cultural and Psychosocial Influences on Disability (CUPID) study found marked variation in musculoskeletal pain across 18 countries, and though reduced, between-country variance was not completely accounted for by the inclusion of group-level variables [18,19]. This indicates a complex interaction between individual- and country-level factors, as well as other factors, in explaining variation in pain, and highlights a need to better understand why people in some countries appear to be more prone to pain. However, five contextual country-level factors were associated with pain: region, population density, life expectancy, gender inequality, and income inequality. Moreover, they explained some of the cross-country variation in pain levels. Residents of European countries were most likely to report pain, while those living in countries in the Western Pacific region were least likely. These regional variations may partly reflect the distinctive subjective nature of pain reporting on surveys.
With respect to population density, the environment in which people live, shaped by factors such as urbanization, is a major factor influencing public health [47]. The World Health Organization, for instance, has highlighted the negative impact of high population density on mental and physical health [75]. Inadequate housing, congested public transport, poor hygiene, high pollution levels, a lack of safe spaces for active living, and greater perceived stress may all increase the likelihood of experiencing physical and mental health conditions. Thus, though living in a rural area may contribute to more adverse health outcomes due to the reduced availability and accessibility of health care [58], the quality of the built environment in urban areas also matters, having possible implications for health conditions such as pain. Given the lack of research on population density and pain prevalence, these results must be interpreted cautiously, although it seems likely that population density may be reflecting one or more of the detrimental conditions associated with rapid urbanization.
Life expectancy is a key metric for assessing population health. However, life expectancy may also be a proxy representing other determinants that support a longer life expectancy beyond the country-level variables included in this study. Hauck, Martin, and Smith [32] suggested that life expectancy may be robustly associated with a variety of possible social determinants, including gender equality, agricultural production, political stability, access to clean water and sanitation, good governance, primary school enrolment, private health expenditure, overseas development assistance, control of armed conflict, and HIV prevalence. Thus, beyond the determinants that were already included in this analysis, it is possible that life expectancy may be representing one or more of these, and should be researched further.
Importantly, this study found two different forms of social inequality, income and gender, to be independently and strongly associated with the probability of reporting pain. Research attests that income inequality affects population health and wellbeing [56], and that individual income is related to health as a marker of individual social status [1,51]. Moreover, not only may income inequality have a direct impact on health outcomes across countries [56], but greater inequality also likely worsens other outcomes that impact health, such as social mobility and mental health conditions, all of which contribute to a cycle of inequality, and therefore worse health outcomes, through fewer resources [16,52,56].
It has also long been known that pervasive gender inequality and restrictive gender norms result in a range of negative health outcomes for the total population, not only for women and girls [61]. Subsequent testing of the interaction between gender and the Gender Inequality Index in the current data indicated that greater gender inequality increases the probability of pain among both women and men, although the association is stronger for women. This is a promising area of future research to explore, as gender inequalities and gender discrimination can contribute to poor health outcomes through complex pathways including how the gender system interacts with other axes of power and privilege across the gender spectrum to shape an individual's social position throughout life [61].
Some theories have attempted to explain the impact of inequality on health as solely the result of indirect forces, including the availability of “neo-materials”, such as societal investment in education, occupation, and health services [48]. However, this study has suggested that income inequality and gender inequality have negative impacts on health outcomes such as pain even when accounting for possible effects of social inputs, such as GNI, education, health expenditure, and labour force participation. It is possible that psychosocial factors, such as social capital and trust [56], or consequences of feeling socially inferior, lacking control, and feeling unsafe [12] may mediate the relationship, contributing to a physiological chain of events that translate into heightened risk of mental and physical health conditions over time. While these effects are felt most among the marginalized groups, they may also extend to other strata of the population due to generally higher levels of stress and distrust. Our findings about gender and income inequalities are of particular concern at time of writing given gender inequalities that are being exacerbated by a global pandemic lockdown [46], and income inequalities that are on the rise globally [23,34]. Thus, social inequalities remain a critical area for future research and health policy, including in, but not restricted to the realm of pain.
Strengths of our study include a large sample size and substantial number of countries representing a variety of country regions and income levels. Moreover, due to rigorous sampling and survey protocol in the WHS, the survey was conducted using standardized measures among representative samples.
Our study also had limitations. Though the WHS survey provides a unique opportunity as a standardized source of international health data when there are few comparable data sources available for examining global variations in pain prevalence [33], it is an older dataset, which may limit its current generalizability. In addition, due to the way pain was assessed in the WHS survey, only accounting for pain experienced in the previous 30 days, it may be difficult to conclude that these results point to prevalence of chronic pain (which is often assessed with respect to a longer time frame), making it challenging to compare to other studies. Likewise, due to a lack of data, we could only assess the general intensity of pain, and not the frequency of pain experienced within the month. Finally, the WHS was cross-sectional and causal relationships cannot be assumed. However, even with these challenges, this study has contributed unique insight into the potential impacts of contextual factors on pain around the world, and presents a starting point for further research.
In conclusion, prevalence of pain varied substantially across countries (9.9 – 50.3%). A portion of this variation was explained by contextual country-level social and economic factors. Importantly, these factors included two indicators of social inequality, income inequality and gender inequality. However, residual variation in pain prevalence across countries remains even in our most robust model. Given the consistency of measurement across the surveys, the remaining variation in pain across countries points to a complex interaction between known and unknown personal, local, economic and political impacts on pain prevalence, as well as inherent differences in language, interpretations of health, and other difficult-to-assess cultural idiosyncrasies. The frequency with which individuals around the world report moderate to severe pain, and the association of pain reporting with social, economic, and political determinants, provides further justification for regarding pain as a global public health priority. It also suggests that global attention and resources be shifted to the macrosocial determinants that shape patterns of pain and differentially impact quality of life on a larger scale. Future research should delve further into the complex association between inequality and pain in order to obtain a more complete picture of the possible explanatory power of social and political determinants of pain around the world.
Supplementary Material
Acknowledgements
Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number R01AG065351 (PI: HGP). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Financial support was also provided by the Social Sciences and Humanities Research Council of Canada through the Canada Research Chairs Program to ZZ.
Footnotes
Conflict of interest statement
The authors have no conflicts of interest to declare.
References
- [1].Adler NE, Epel ES, Castellazzo G, Ickovics JR. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychol 2000;19:586. [DOI] [PubMed] [Google Scholar]
- [2].Amate-Fortes I, Guarnido-Rueda A, Molina-Morales A. World Analysis of the Determinants of the Inequality in Health. Is the Measurement of Inequality Important? Rev Za Soc Polit 2020;27:83–98. [Google Scholar]
- [3].Andrews JS, Cenzer IS, Yelin E, Covinsky KE. Pain as a risk factor for disability or death. J Am Geriatr Soc 2013;61:583–589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Andrews P, Steultjens M, Riskowski J. Chronic widespread pain prevalence in the general population: a systematic review. Eur J Pain 2018;22:5–18. [DOI] [PubMed] [Google Scholar]
- [5].Angel RJ, Cleary P. The effects of social structure and culture on reported health. Soc Sci Q 1984;65:814. [Google Scholar]
- [6].Bambra C, Smith KE, Pearce J. Scaling up: the politics of health and place. Soc Sci Med 2019;232:36–42. [DOI] [PubMed] [Google Scholar]
- [7].Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth 2013;111:52–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Bergman S, Herrström PER, Högström K, Petersson IF, Svensson B, Jacobsson LT. Chronic musculoskeletal pain, prevalence rates, and sociodemographic associations in a Swedish population study. J Rheumatol 2001;28:1369–1377. [PubMed] [Google Scholar]
- [9].Blyth FM, March LM, Brnabic AJ, Jorm LR, Williamson M, Cousins MJ. Chronic pain in Australia: a prevalence study. Pain 2001;89:127–134. [DOI] [PubMed] [Google Scholar]
- [10].Blyth FM, Schneider CH. Global burden of pain and global pain policy—creating a purposeful body of evidence. Pain 2018;159:S43–S48. [DOI] [PubMed] [Google Scholar]
- [11].Bohlin A, Ahlgren C, Hammarstrom A, Gustafsson PE. Perceived gender inequality in the couple relationship and musculoskeletal pain in middle-aged women and men. Scand J Public Health 2013;41:825–831. [DOI] [PubMed] [Google Scholar]
- [12].Bonathan C, Hearn L, Williams AC de C. Socioeconomic status and the course and consequences of chronic pain. Pain Manag 2013;3:159–162. [DOI] [PubMed] [Google Scholar]
- [13].Brattberg G, Thorslund M, Wikman A. The prevalence of pain in a general population. The results of a postal survey in a county of Sweden. Pain 1989;37:215–222. [DOI] [PubMed] [Google Scholar]
- [14].Brinda EM, Rajkumar AP, Enemark U. Association between gender inequality index and child mortality rates: a cross-national study of 138 countries. BMC Public Health 2015;15:1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Brønnum-Hansen H Ranking health between countries in international comparisons. Scand J Public Health 2014;42:242–244. [DOI] [PubMed] [Google Scholar]
- [16].Chapple S, Richardson D. Doing better for children. OECD, 2009. Available: https://www.oecd.org/els/family/doingbetterforchildren.htm. [Google Scholar]
- [17].Chatterjee S, Price B. Regression analysis by example. 2nd ed. New York, NY: Wiley, n.d. [Google Scholar]
- [18].Coggon D, Ntani G, Palmer KT, Felli VE, Harari F, Quintana LA, Felknor SA, Rojas M, Cattrell A, Vargas-Prada S. Drivers of international variation in prevalence of disabling low back pain: findings from the cultural and psychosocial influences on disability study. Eur J Pain 2019;23:35–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Coggon D, Ntani G, Palmer KT, Felli VE, Harari R, Barrero LH, Felknor SA, Gimeno D, Cattrell A, Serra C. Disabling musculoskeletal pain in working populations: is it the job, the person, or the culture? Pain® 2013;154:856–863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Covinsky KE, Lindquist K, Dunlop DD, Yelin E. Pain, functional limitations, and aging. J Am Geriatr Soc 2009;57:1556–1561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Croft P, Rigby AS, Boswell R, Schollum J, Silman A. The prevalence of chronic widespread pain in the general population. J Rheumatol 1993;20:710–713. [PubMed] [Google Scholar]
- [22].Crook J, Rideout E, Browne G. The prevalence of pain complaints in a general population. Pain 1984;18:299–314. [DOI] [PubMed] [Google Scholar]
- [23].Diffenbaugh NS, Burke M. Global warming has increased global economic inequality. Proc Natl Acad Sci 2019;116:9808–9813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Elzahaf RA, Tashani OA, Unsworth BA, Johnson MI. The prevalence of chronic pain with an analysis of countries with a Human Development Index less than 0.9: a systematic review without meta-analysis. Curr Med Res Opin 2012;28:1221–1229. [DOI] [PubMed] [Google Scholar]
- [25].Farioli A, Mattioli S, Quaglieri A, Curti S, Violante FS, Coggon D. Musculoskeletal pain in Europe: role of personal, occupational and social risk factors. Scand J Work Environ Health 2014;40:36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley III JL. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain 2009;10:447–485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Gaye A, Klugman J, Kovacevic M, Twigg S, Zambrano E. Measuring key disparities in human development: The gender inequality index. Hum Dev Res Pap 2010;46:1–37. [Google Scholar]
- [28].Gibson SJ, Helme RD. Age-related differences in pain perception and report. Clin Geriatr Med 2001;17:433–456. [DOI] [PubMed] [Google Scholar]
- [29].Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health 2011;11:1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Grol-Prokopczyk H Sociodemographic disparities in chronic pain, based on 12-year longitudinal data. Pain 2017;158:313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Gureje O, Von Korff M, Simon GE, Gater R. Persistent pain and well-being: a World Health Organization study in primary care. Jama 1998;280:147–151. [DOI] [PubMed] [Google Scholar]
- [32].Hauck K, Martin S, Smith PC. Priorities for action on the social determinants of health: Empirical evidence on the strongest associations with life expectancy in 54 low-income countries, 1990–2012. Soc Sci Med 2016;167:88–98. [DOI] [PubMed] [Google Scholar]
- [33].Henschke N, Kamper SJ, Maher CG. The epidemiology and economic consequences of pain. Mayo Clinic Proceedings. Elsevier, 2015, Vol. 90. pp. 139–147. [DOI] [PubMed] [Google Scholar]
- [34].Hickel J Is global inequality getting better or worse? A critique of the World Bank’s convergence narrative. Third World Q 2017;38:2208–2222. [Google Scholar]
- [35].Hosseinpoor AR, Parker LA, d’Espaignet ET, Chatterji S. Socioeconomic inequality in smoking in low-income and middle-income countries: results from the World Health Survey. PloS One 2012;7:e42843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Hosseinpoor AR, Stewart Williams JA, Gautam J, Posarac A, Officer A, Verdes E, Kostanjsek N, Chatterji S. Socioeconomic inequality in disability among adults: a multicountry study using the World Health Survey. Am J Public Health 2013;103:1278–1286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Hoy D, Brooks P, Blyth F, Buchbinder R. The epidemiology of low back pain. Best Pract Res Clin Rheumatol 2010;24:769–781. [DOI] [PubMed] [Google Scholar]
- [38].IBM Corp. SPSS. IBM Corp, 2019. Available: https://www.ibm.com/analytics/spss-statistics-software. [Google Scholar]
- [39].Jaba E, Balan CB, Robu I-B. The relationship between life expectancy at birth and health expenditures estimated by a cross-country and time-series analysis. Procedia Econ Finance 2014;15:108–114. [Google Scholar]
- [40].Jackson T, Thomas S, Stabile V, Shotwell M, Han X, McQueen K. A systematic review and meta-analysis of the global burden of chronic pain without clear etiology in low-and middle-income countries: trends in heterogeneous data and a proposal for new assessment methods. Anesth Analg 2016;123:739–748. [DOI] [PubMed] [Google Scholar]
- [41].Johnson MI, Elzahaf RA, Tashani OA. The prevalence of chronic pain in developing countries. Pain Manag 2013;3:83–86. [DOI] [PubMed] [Google Scholar]
- [42].Kaufmann D, Kraay A, Mastruzzi M. The Worldwide Governance Indicators: Methodology and Analytical Issues. Hague J Rule Law 2011;3:220–246. [Google Scholar]
- [43].Kim JI, Kim G. Relationship between the remaining years of healthy life expectancy in older age and national income level, educational attainment, and improved water quality. Int J Aging Hum Dev 2016;83:402–417. [DOI] [PubMed] [Google Scholar]
- [44].Kim S, Wang J. Does quality of government matter in public health?: comparing the role of quality and quantity of government at the National Level. Sustainability 2019;11:3229. [Google Scholar]
- [45].King TL, Kavanagh A, Scovelle AJ, Milner A. Associations between gender equality and health: a systematic review. Health Promot Int 2020;35:27–41. [DOI] [PubMed] [Google Scholar]
- [46].Landivar LC, Ruppanner L, Scarborough WJ, Collins C. Early Signs Indicate That COVID-19 Is Exacerbating Gender Inequality in the Labor Force. Socius 2020;6:2378023120947997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Leung KM, Yeung KW, You J, Choi K, Zhang X, Smith R, Zhou G-J, Yung MM, Arias-Barreiro C, An Y-J. Toward sustainable environmental quality: priority research questions for Asia. Environ Toxicol Chem 2020;39:1485–1505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].Lynch JW, Smith GD, Kaplan GA, House JS. Income inequality and mortality: importance to health of individual income, psychosocial environment, or material conditions. BMJ 2000;320:1200–1204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [49].Mackenbach JP, Looman CW. Life expectancy and national income in Europe, 1900-2008: an update of Preston’s analysis. Int J Epidemiol 2013;42:1100–1110. [DOI] [PubMed] [Google Scholar]
- [50].Mansfield KE, Sim J, Jordan JL, Jordan KP. A systematic review and meta-analysis of the prevalence of chronic widespread pain in the general population. Pain 2016;157:55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [51].Marmot M Status syndrome. Significance 2004;1:150–154. [Google Scholar]
- [52].Messias E, Eaton W, Grooms A. Income Inequality and Depression Prevalence Across the United States: An Ecological Study. Psychiatr Serv 2011;62:710–712. [DOI] [PubMed] [Google Scholar]
- [53].Midi H, Bagheri A. Robust multicollinearity diagnostic measure in collinear data set. Proceedings of the 4th international conference on applied mathematics, simulation, modeling. World Scientific and Engineering Academy and Society, 2010. pp. 138–142. [Google Scholar]
- [54].Milanovic B Global income inequality in numbers: In history and now. Glob Policy 2013;4:198–208. [Google Scholar]
- [55].Moore R, Straube S, Aldington D. Pain measures and cut-offs–‘no worse than mild pain’as a simple, universal outcome. Anaesthesia 2013;68:400–412. [DOI] [PubMed] [Google Scholar]
- [56].Pickett KE, Wilkinson RG. Income inequality and health: a causal review. Soc Sci Med 2015;128:316–326. [DOI] [PubMed] [Google Scholar]
- [57].Pieretti S, Di Giannuario A, Di Giovannandrea R, Marzoli F, Piccaro G, Minosi P, Aloisi AM. Gender differences in pain and its relief. Ann Ist Super Sanita 2016;52:184–189. [DOI] [PubMed] [Google Scholar]
- [58].Probst J, Eberth JM, Crouch E. Structural Urbanism Contributes To Poorer Health Outcomes For Rural America. Health Aff (Millwood) 2019;38:1976–1984. [DOI] [PubMed] [Google Scholar]
- [59].Rice AS, Smith BH, Blyth FM. Pain and the global burden of disease. Pain 2016;157:791–796. [DOI] [PubMed] [Google Scholar]
- [60].Robinson ME, Riley JL III, Myers CD, Papas RK, Wise EA, Waxenberg LB, Fillingim RB. Gender role expectations of pain: relationship to sex differences in pain. J Pain 2001;2:251–257. [DOI] [PubMed] [Google Scholar]
- [61].Sen G, Östlin P. Gender inequity in health: why it exists and how we can change it. Glob Public Health 2008;3:1–12. [DOI] [PubMed] [Google Scholar]
- [62].Smith BH, Elliott AM, Chambers WA, Smith WC, Hannaford PC, Penny K. The impact of chronic pain in the community. Fam Pract 2001;18:292–299. [DOI] [PubMed] [Google Scholar]
- [63].StataCorp LLC. Stata. College Station, TX, 2021. Available: https://www.stata.com/. [Google Scholar]
- [64].Swift R The relationship between health and GDP in OECD countries in the very long run. Health Econ 2011;20:306–322. [DOI] [PubMed] [Google Scholar]
- [65].Thompson CG, Kim RS, Aloe AM, Becker BJ. Extracting the variance inflation factor and other multicollinearity diagnostics from typical regression results. Basic Appl Soc Psychol 2017;39:81–90. [Google Scholar]
- [66].To T, Stanojevic S, Moores G, Gershon AS, Bateman ED, Cruz AA, Boulet L-P. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health 2012;12:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2019 custom data acquired via website. 2019. Available: https://population.un.org/wpp/. Accessed 3 Mar 2021. [Google Scholar]
- [68].Üstün T, Chatterji S, Mechbal A, Murray C. WHS Collaborating Groups: The World Health Surveys. In: Murray C, Evans D, editors. Health systems performance assessment: debates, methods and empiricism. World Health Organization, 2003. pp. 797–808. [Google Scholar]
- [69].Vittinghoff E, Glidden DV, Shiboski SC, McCulloch CE. Regression methods in biostatistics: linear, logistic, survival, and repeated measures models. Springer Science & Business Media, 2011. [Google Scholar]
- [70].Wagstaff A, Van Doorslaer E. Income inequality and health: what does the literature tell us? Annu Rev Public Health 2000;21:543–567. [DOI] [PubMed] [Google Scholar]
- [71].Wilkinson RG, Marmot M eds. Social determinants of health: The solid facts. 2nd ed. Copenhagen: World Health Organization, 2003. [Google Scholar]
- [72].World Health Organization. Chapter 3 - General health care. World report on disability 2011. World Health Organization, 2011. Available: https://www.ncbi.nlm.nih.gov/books/NBK304072/. [Google Scholar]
- [73].World Health Organization. Definition of regional groupings. World Health Organ; 2021. Available: http://www.who.int/healthinfo/global_burden_disease/definition_regions/en/. Accessed 16 Mar 2021. [Google Scholar]
- [74].World Health Organization. World Health Survey (WHS). 2021b. Available: https://apps.who.int/healthinfo/systems/surveydata/index.php/catalog/whs/about. Accessed 19 May 2021. [Google Scholar]
- [75].World Health Organization, South East Asia. Population density – A growing concern. 2020. Available: http://origin.searo.who.int/. Accessed 23 Mar 2021. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.