

Abstract
Internationally recognized best practice care in the early management and rehabilitation of individuals following stroke includes multidisciplinary assessment and treatment by a coordinated team of health care professionals that includes occupational therapists. Occupational therapists assess the impact of changes in motor function, sensation, coordination, visual perception, and cognition on a person's capacity to manage daily life tasks. Intervention improves participation in meaningful roles, tasks, and activities; remediates deficits; minimizes secondary complications; and provides education and support to the patient and caregivers. Occupational therapists' focus on independence and function, individual goal-setting, and their specialist skills in task adaptation and environmental modification underpin the profession's contribution to the multidisciplinary stroke rehabilitation team. The aim of this paper is to provide an overview of occupational therapy practice in stroke patients.
Keywords: Assessment, intervention, occupational therapy, role, stroke
After stroke, occupational therapists work to facilitate and improve motor control and hand function in the stroke-affected upper limb; to maximize the person's ability to undertake his or her own personal self-care tasks and domestic tasks; to help the patient learn strategies to manage the cognitive, perceptual, and behavioral changes associated with stroke; and to prepare the home and work environment for the patient's return.
Internationally recognized best practice care in the early management and rehabilitation of individuals following stroke includes multidisciplinary assessment and treatment by a coordinated team of health care professionals, including occupational therapists.[1] Occupational therapists work collaboratively with the patient to establish the impact of stroke on the performance of daily tasks, including personal cares, domestic tasks, and work and leisure activities, and develop a goal-focused program to develop the required skills for participation in daily life. The aim of this paper is to provide an overview of occupational therapy practice in stroke.
The Clinical Guidelines for Acute Stroke Management[2] and Stroke Rehabilitation and Recovery[3] provides a framework that is based on the best available evidence. There is a growing research evidence base in support of the benefits of occupational therapy management following stroke.
There are 15 occupational therapy education centers in India that are recognized by the All India Occupational Therapists' Association (AIOTA) and the World Federation of Occupational Therapy (WFOT). The International Journal of Occupational Therapy is an official publication of AIOTA.[4]
Occupational Therapy Assessment after Stroke
Assessment is conducted to understand the impact of changes in motor function, sensation, coordination, visual perception, and cognition on the stroke victim's capacity to manage daily life tasks. Assessment is used to identify areas of individual and environmental difficulties and to enable patient-centered goal-setting with the participation of both the patient and the family members. Table 1 lists the core areas of occupational therapy assessment, summarized according to the International Classification of Functioning (ICF) terminology.[5] Occupational therapists endeavor to set rehabilitation goals related to activity and participation that are specific, measurable, attainable, realistic, and relevant to the individual person.
Table 1.
Core areas of occupational therapy assessment.[5]

Activities of Daily Living (ADL)
The initial process of occupational therapy assessment involves interviews with the patient and the carer to establish previously held life roles and the tasks and activities that were completed within these roles. Observational assessment is undertaken of personal self-care tasks, including showering, dressing, toileting, grooming, and eating, and domestic or instrumental tasks, including meal preparation, shopping, cleaning, laundry, and management of finances and medications. Standardized measures may include the Functional Independence Measure (FIM),[6] the Modified Barthel Index (MBI),[7] the Assessment of Motor and Process Skills (AMPS),[8] the Assessment of Living Skills and Resources (ALSAR),[9] and the Reintegration to Normal Living Index.[10] Understanding the level of assistance needed in each of these areas and the priorities of the individuals helps the occupational therapist target rehabilitation interventions appropriately and to measure progress towards individual goals. Observation of activity limitations allows the occupational therapist to identify the impairments that underpin these limitations, including the motor, sensory, cognitive and/or perceptual sequelae of stroke. These will now be described in more detail.
Vision and Visual Perception
Screening of primary visual skills, including visual acuity, visual fields, and visual tracking are undertaken by the occupational therapist before examining for changes in visual perception.[11] Routine occupational therapist assessment for impairments of perception are integral to the rehabilitation of patients following stroke[12] and are prerequisites to the overall goal of optimizing functional independence.[13] Standardized assessment tools used in this area include the Occupational Therapy Adult Perceptual Screening Test (OT-APST),[14] the Rivermead Perceptual Assessment Battery (RPAB),[15] the Behavioral Inattention Test (BIT),[16] and the Ontario Society of Occupational Therapists Perceptual Evaluation (OSOT).[17] Following stroke, occupational therapists routinely screen for visual-perceptual impairments such as agnosia; visuospatial relations problems, eg, figure-ground, body scheme disorders, depth perception, and unilateral neglects, and impairments in constructional skills.[14] Other neurobehavioral changes, including praxis and acalculia, are commonly assessed in conjunction with visual-perceptual screening following both right and left hemisphere stroke. A more detailed summary of the visual-perceptual and motor planning changes that are screened for by occupational therapists is shown in Table 2.
Table 2.
Classifi cation of terminology for visual perceptual impairments and apraxia.[14]

Memory and Cognition
The occupational therapist conducts initial screening, and more detailed assessments if indicated, in the areas of memory, cognition, and executive functioning to determine the impact of changes in these areas on the ability to resume daily function. The occupational therapist uses standardized measures in addition to structured observational techniques, and the results are then used in treatment planning and outcome measurement. These measures may include the Mini Mental State Examination (MMSE),[18] the Cognitive Assessment of Minnesota (CAM),[19] the Rivermead Behavioral Memory Test (RBMT),[20] and the Assessment of Motor and Process Skills (AMPS).[8] Unless identified and addressed, impairments in memory, cognition, and executive skills can impact significantly upon a person's ability to participate in a rehabilitation program and to complete personal, domestic, leisure, and work-related tasks.[21] Difficulty in initiating regular tasks such as preparing breakfast, impaired capacity to plan in advance to attend an appointment or take medication appropriately, reduced attentional capacity to attend to a task such as using the computer, or impulsiveness that poses safety risks for the individual are practical examples of the effects of these impairments.
Sensory, Motor, and Upper Limb Function
Occupational therapists conduct detailed assessment of the motor and sensory changes following stroke, with particular emphasis on upper limb and hand function. Occupational therapy interventions then address changes in motor power, muscle tone, sensory loss, motor planning/praxis, fine motor coordination, and hand function, with the aim of regaining upper limb control and function. Standardized assessment methods may include Manual Muscle Testing,[22] grip and pinch strengths,[23,24] Nine Hole Peg Test,[25] Modified Ashworth Scale (MAS),[26] and Modified Tardieu Scale (MTS).[27] Functional upper limb ability measures are taken throughout the rehabilitation program to assess progress towards individual goals and for further treatment planning. These measurements supplement the measures of impairment by identifying how stroke-related deficits impact on the ability to use the upper limb in activities of daily living. Measures of upper limb ability may include the Action Research Arm Test (ARAT),[28] Wolf Motor Function Test (WMFT),[29] Arm Motor Ability Test (AMAT),[30] Upper Limb-Motor Assessment Scale (UL-MAS),[31] Chedoke Arm and Hand Activity Inventory (CAHAI),[32] Motor Activity Log (MAL),[33] and ABILHAND.[34] Currently, there is no single upper limb assessment method that is universally accepted,[35] and the choice of the method may be influenced by the level and pattern of motor control available to the patient, the clinical setting, the time available to administer the test, the resources available, and the intended use of the results.
Home Assessment
During the rehabilitation phase of stroke, and close to the time of hospital discharge, the occupational therapist will examine the patient's capacity to complete their usual activities, to manage safely in their own home environment, and to access the community. The occupational therapist will evaluate the need for a home assessment, taking into consideration the environmental barriers, specific impairments, risk of falls, and the needs of the patient/carer. The purpose of the assessment is to establish whether it is safe for the stroke patient to return to their pre-stroke environment or if alternate accommodation will be required. A home assessment involves the occupational therapist observing the patient's ability to physically negotiate their environment and perform their usual activities. For instance, the occupational therapist may assess the patient's ability to safely transfer from their bed or toilet. The occupational therapist will also assess a patient's ability to plan, implement, and problem-solve tasks like making a simple meal, safely administering medications, using the telephone to call for assistance, or paying bills.
Illustrative Case Study
A 69-year-old retired male with a middle cerebral artery stroke on CT scan presented with a dense left hemiplegia, severe left-sided neglect, and cognitive changes.
During the initial ADL shower assessment, Mr S required prompting to locate and identify the items needed for showering, cueing and physical assistance to dress, one-person assistance for all transfers, and cueing to sequence the tasks. Mr S achieved a score of 48/135 using the Functional Independence Measure (FIM) (26/91 motor and 22/35 cognitive scores), indicating moderate to full assistance with self-cares.
Initial cognitive screening using the MMSE revealed impairment of basic level cognition (score of 22/30). The CAM identified moderate deficits in the areas of attention, visual and auditory memory and sequencing, mental manipulations relating to money use, foresight/planning, concrete problem-solving, and severe visual neglect. On the ward Mr S needed significant cueing to locate items. His poor problem-solving skills and planning were evident in the incorrect use of switches in the kitchen to turn on/off appliances and inability to recognise an item burning on the stove top,along with inability to problem-solve how to correct this. He was also unsafe attempting to cross the road, and slow and inaccurate in handling money.
Visual perceptual screening using the OT-APST revealed agnosia, unilateral neglect, impairments in constructional skills, and impairment on the functional skills subscale of this assessment. Figure 1 shows the OT-APST items on initial assessment, where Mr S attempted to draw a clock and copy the picture of a house. He lacked insight into the errors of performance that he made on the OT-APST and his speed of information processing was slow.
Figure 1a.
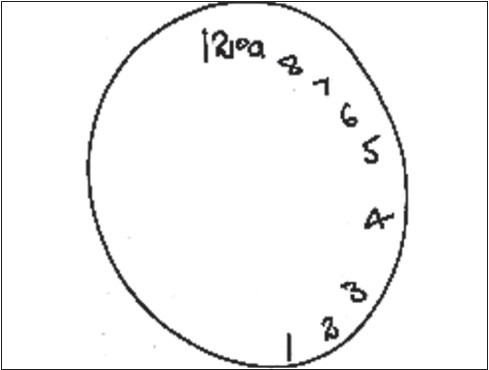
Mr S OT-ASPT clock drawing item on admission
Figure 1b.
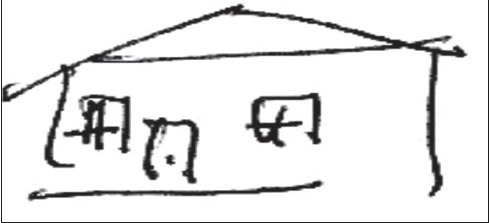
Mr S OT-ASPT house copy item on admission
Upper limb assessment revealed weak active movement in left shoulder elevation and internal rotation, mild increase in tone in finger and elbow flexors, and absent protective and discriminative sensation.
Occupational Therapy Intervention after Stroke
Rehabilitation following stroke should begin as soon as the medical condition is stable. Occupational therapy intervention improves participation in meaningful roles, tasks, and activities. A recent systematic review of randomized trials found that stroke patients who receive occupational therapy focused on personal activities of daily living, as opposed to no occupational therapy, are more likely to be independent in those activities.[36] Treatment, including individually selected and graded tasks and activities, involves retraining motor, sensory, visual, perceptual, and cognitive skills within the context of functional activities; minimizing secondary complications; and providing education and support to the patient and caregivers.[11]
Occupational therapy interventions may include methods aimed at maintaining or improving soft tissue properties of the upper limb. For example, techniques that may be used to reduce spasticity include stretching [37] and static or dynamic splinting,[38] either alone or in combination with the use of medically administered botulinum toxin therapy.[39] Other methods employed to prevent contracture or dependant edema may include education for the patient and family in ways to support and position the stroke-affected upper limb. For patients who have developed contractures, management may include electrical stimulation[40] or casting.[41] The occupational therapist may prescribe a firm support device to reduce the risk of shoulder subluxation or prevent further subluxation.[42,43,44,45] Upper limb positioning, bandaging, compression garments,[38] retrograde massage, and electrical stimulation[46] are some of the techniques that may be employed by the occupational therapist to prevent or reduce the hand edema that may occur after a stroke. Active therapy and graded task selection is used to encourage sensorimotor return; the therapy may include muscle facilitation and strengthening, in conjunction with everyday activities to develop reach, grasp, and object manipulation skills. Specific techniques include functional electrical stimulation,[47] constraint-induced movement therapy,[48] progressive resistive exercise[49] and sensory-related training,[50] and avoidance of movements that reinforce the synergistic movement patterns of the upper limb that limit function. Patients are encouraged to continue activities outside of therapy time and are prescribed a task-specific[51,52,53] rehabilitation program, encouraging as much practice as possible.[54] This is achieved by loaning therapy kits to enable self-directed practice. Examples of practice tasks include: using a keyboard, mobile phone, television remote, or calculator to practice fine motor skills; opening a range of jars and containers of varying sizes and weights and with different types of lids; turning the pages of books, magazines, and newspapers; and managing fastenings of clothing items with different-sized buttons, zippers, Velcro, clips, and laces. The occupational therapist reviews and upgrades the therapy program on a daily basis.
Visual and perceptual impairments are minimized by retraining in specific skills, teaching compensation techniques, substitution of unimpaired skills, or adapting the task or environment.[1] Methods include visual scanning training[55] to assist a person with a hemianopia or neglect to locate items more accurately in their environment. A person with depth perception problems may be encouraged to hold the handrail for additional proprioceptive cues to safely negotiate stairs, as well as to pace themselves and go more slowly down a flight of stairs. A person with praxis[56] or motor planning problems affecting one upper limb may initially practice a range of remediation techniques involving feedback, cueing, and functional repetitive practice to overcome the impairment. If the impairment of the stroke-affected hand is resistant to remediation methods, the occupational therapist may teach the patient to compensate by using the other, unaffected, upper limb for tasks requiring greater precision such as shaving, thus increasing the patient's level of independence.
Cognitive therapy may be used in rehabilitation of attention and concentration impairments.[57] For patients with memory difficulties, external cues may help prompt their memory,[58] for example, using a diary, visual prompts, or an alarm. An external cue, for example a pager,[58] may help patients with impaired executive functioning to initiate tasks.
Occupational therapists will establish how tasks can be adapted or the environment changed to improve the patient's level of independence. For the physical environment, the occupational therapist may prescribe assistive equipment or home modifications to enable task performance with greater ease or safety.[59] For example, installing grab rails near steps, raising the chair height, or prescribing a wheeled mobility tray for transporting meals.
The occupational therapist liaises with the discharge planner, patient, and caregivers to establish the anticipated frequency, duration, intensity, and type of carer support required for return home.[33] For instance, the patient may need supervision with medications because of memory difficulties, assistance for dressing because of dyspraxia, or help with the laundry because of balance problems. The occupational therapist may train carers to use assistive equipment or modifications safely with the patient.[60] When a patient returns home without the capacity to get out of bed themselves, the occupational therapist trains relatives to safely operate an electric hoist or wheelchair. Continual education of the patient and family, and participation of the family in a treatment program, is essential for the smooth transition to discharge, carry-over of skills learnt to the home environment, and for facilitating psychosocial adjustment.
Case Study Continued
Daily occupational therapy treatment involved improving awareness of the impact of left neglect on daily tasks, systematic visual scanning training, and practical strategies for daily task completion to overcome the impact of neglecting behavior. These included tasks and strategies of graded complexity including dressing, meal preparation, money management and, eventually, crossing the road and shopping. Feedback was provided continually and consistently by occupational therapy and other staff to facilitate increased insight and awareness of deficits and to facilitate anticipatory use of left-sided visual scanning to help achieve 'over learning' of this skill. Perceptual and cognitive retraining was undertaken to achieve a level of safety and independence in the personal care tasks of dressing, showering, toileting, grooming, and eating, as well as in the domestic tasks of meal preparation and shopping.
Daily upper limb movement facilitation and positioning, massage, elevation, and compression were employed to address muscle weakness and edema of the left upper limb. Education was provided for safety in the care of his arm and practical training in one-handed methods of completing daily tasks, including dressing, grooming, and eating.
Occupational Therapy Post-discharge Intervention after Stroke
Outpatient services
When patients return home, referral to outpatient or community occupational therapy is sometimes required.[61] Either hospital or center-based rehabilitation services or therapy provided in the home can be used; the aim is to enable independence in the activities of daily living.[62] Rehabilitation is equally effective if delivered in the hospital as an outpatient, in a day hospital, or in the community, and should be offered to all stroke patients as needed.[61,62,63] Economic evaluations of community rehabilitation are limited to cost description studies.[3] In India, community-based rehabilitation is described as a strategy within general community development for rehabilitation, equalization of opportunities, and social inclusion of people with disability.[64]
Residential care
If a stroke patient is unlikely to benefit from active rehabilitation and requires residential care, the occupational therapist may be involved in training the carer of the facility to manage the patient's functional difficulties and enabling maximum patient participation.[65] For instance, this may involve proper positioning for eating tasks or visual scanning strategies for reading. The occupational therapist may suggest equipment to enable the patient to participate in their cares or return to leisure activities.[66] For instance, custom clothing[67] for easier toileting or modifying the television on-off switch to assist the patient regulate their environment.[68] The occupational therapist may provide advice on pressure-relieving mattresses and cushions for patients managed in bed and seated in wheelchairs, or education regarding positioning for comfort and prevention of deformity.[69]
Return to driving services
For patients who drove before their stroke, the occupational therapist provides information and advice on their post-stroke driving responsibilities.[70] In Australia, it is recommended that the patient should not drive for a minimum of 1 month after stroke or transient ischemic attack (TIA), and perhaps longer if there is significant neurological, perceptual, or cognitive deficit, depending on medical advice.[71] In addition to a medical examination, the patient may be referred to an occupational therapy driver assessor for off-road and on-road driving assessment.[72] Off-road assessment includes an evaluation of skills such as scanning, attention, visual perception, hazard perception, executive function, reaction time, and knowledge of road law. This assessment is also designed to identify patients not suitable for on-road assessment. On-road assessment evaluates driving performance in a dual-control vehicle with a driving instructor.[72] Examples of recommendations from this assessment include the need for specialist equipment or vehicle modifications, need for rehabilitation or retraining, review of license conditions, or need for reassessment. When patients are unable to return to driving, they are commonly provided with information regarding transport subsidies or their local community transport schemes.
Return to work services
For the patient in paid employment before their stroke, assessment regarding return to work commences in the acute setting. The occupational therapist gathers a history of the patient's occupation, i.e., job duties (frequency and duration) and work conditions (hours, environment, etc.). Using the results of assessment of the sensorimotor, cognitive, visual-perceptual, and psychological abilities of the patient, the occupational therapist considers the feasibility of return to work. Often the patient is referred to an occupational therapist specializing in occupational rehabilitation[70] to conduct a workplace assessment and negotiate a graded return to work hours and duties.[68]
Case Study Continued
An occupational therapy home assessment was conducted prior to discharge. Recommendations included the installation of grab rails in the shower and toilet, removal of a shower screen that limited safe access, purchase of a shower stool for seated showering as his balance remained impaired, and purchase of a lounge chair of a suitable height.
Mr S's functional improvements included independence with dressing, showering, toileting, mobilizing with a single stick, and preparing breakfast. His performance on standardized cognitive and perceptual assessments improved; however, he continued to require close supervision for outdoor mobility, kitchen tasks requiring use of electrical appliances, and management of his medications and finances. Safety concerns in the kitchen at time of discharge included the need for cueing to turn off the hot plate of the stove after use, turning off the tap before the sink overflowed if distracted by another task, and shutting cupboards and drawers after use. His wife participated in many occupational therapy sessions to gain an understanding of the type of supervision and assistance her husband would need upon return home.
Cognitive reassessment on discharge revealed an MMSE score of 27/30 (which is within the normal range for his level of education), and Montreal Cognitive Assessment (MoCA) score of 25/30 (normal = 26 and above), revealing ongoing impairment, particularly in the areas of executive functioning. The OT-APST on discharge continued to show evidence of agnosia and neglect and impairment of constructional skills and functional skills, although gains were made in each of these areas since admission. Figure 2 demonstrates changes in his visual perceptual abilities at the time of discharge and also the presence of ongoing visual neglect. His discharge FIM score of 94/135 (68/91 motor, 26/35 cognitive) also revealed improvement since admission in his level of functioning, but reflects an ongoing need for supervision and assistance from his wife in daily living tasks. Mr S was not able to return to driving due to the impact of his perceptual and cognitive impairments on safety and judgment and therefore disability parking and transport subsidies were organized.
Figure 2a.
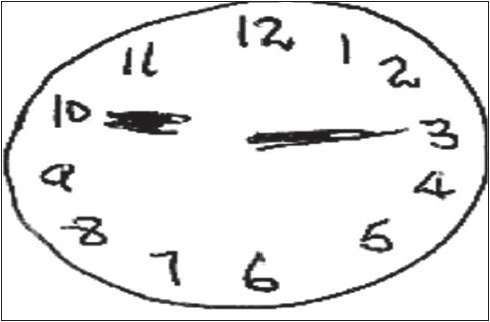
Mr S OT-ASPT clock drawing items on discharge
Figure 2b.

Mr S OT-ASPT house copy items on discharge
Mr S did not regain functional use of his left upper limb and continued to use the one-handed dressing and daily living techniques. Community-based occupational therapy and physiotherapy was organized for follow-up care.
Summary
The occupational therapist's focus on independence and function, individual goal-setting, and specialist skills in task adaptation and environmental modification underpin the profession's contribution to the multidisciplinary stroke rehabilitation team. Assessment of important roles and stroke deficits such as sensorimotor, musculoskeletal changes (biomechanical), cognition, perception, and psychosocial adjustment assist with planning restorative and compensatory intervention plans and measuring the patient outcomes. Occupational therapists' treatment contributes to both the quality of life for survivors of stroke and their families and to timely evaluation of clinical outcomes for the multidisciplinary rehabilitation team.
Acknowledgments
The authors would like to thank Dr Stephen Read and Dr Robert Henderson from the Neurology Department, Royal Brisbane and Women.s Hospital.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.Gresham GE, et al. Clinical practice guidelines. Rockville: U.S Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1995. Post-stroke rehabilitation: Assessment, referral, and patient management. [PubMed] [Google Scholar]
- 2.National Stroke Foundation, Clinical guidelines for acute stroke management. Australia: National Health and Medical Research Council; 2007. [Google Scholar]
- 3.National Stroke Foundation, Clinical guidelines for stroke rehabilitation and recovery. Australia: National Health and Medical Research Council; 2005. [Google Scholar]
- 4.Kenkre IR, Srivastava AK. Occupational therapy in India: The academic profile. WFOT Bull. 2003;48:9–12. [Google Scholar]
- 5.World Health Organisation. International classification of functioning introduction. last cited on 2001 Jul 25. Available from: http://www3.who.int/icf/icftemplate .
- 6.Granger CV. Buffalo: State University of New York; 1993. Guide for the uniform data set for medical rehabilitation (Adult FIM) [Google Scholar]
- 7.Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J Clin Epidemiol. 1989;42:703–9. doi: 10.1016/0895-4356(89)90065-6. [DOI] [PubMed] [Google Scholar]
- 8.Fisher AG. Assessment of motor and process skills. 2nd ed. Fort Collins: Three Star Press; 1997. [Google Scholar]
- 9.Williams JH, Drinka TJ, Greenberg JR, Farrell-Holtan J, Euhardy R, Schram M. Development and testing of the Assessment of Living Skills and Resources (ALSAR) in elderly community-dwelling veterans. Gerontologist. 1991;31:84–91. doi: 10.1093/geront/31.1.84. [DOI] [PubMed] [Google Scholar]
- 10.Wood-Dauphinee S, Williams JI. Reintegration to normal living as a proxy to quality of life. J Chronic Dis. 1987;40:491–9. doi: 10.1016/0021-9681(87)90005-1. [DOI] [PubMed] [Google Scholar]
- 11.Woodson AM. Stroke, in Occupational therapy for physical dysfunction. In: Radomski MV, Trombly CA, editors. Philadelphia: Lippincott Williams and Wilkins; 2008. pp. 1001–41. [Google Scholar]
- 12.Cermak SA, Lin KC. Assessment in occupational therapy and physical therapy. Assessmnet of perceptual dysfunction in the adult. In: Van Deusen J, Brunt D, editors. Philadelphia: W.B. Saunders Company; 1997. pp. 302–33. [Google Scholar]
- 13.Berspang B, Asplund K, Eriksson S, Fugl-Meyer AR. Motor and perceptual impairments in acute stroke patients: Effects on self-care ability. Stroke. 1987;18:1081–6. doi: 10.1161/01.str.18.6.1081. [DOI] [PubMed] [Google Scholar]
- 14.Cooke D, McKenna K, Fleming J. Development of a standardised occupational therapy screening tool for visual perception in adults. Scand J Occup Ther. 2005;12:59–71. doi: 10.1080/11038120410020683-1. [DOI] [PubMed] [Google Scholar]
- 15.Whiting S, et al. RPAB - Rivermead Perceptual Assessment Battery. Windsor, UK: Nfer-Nelson; 1985. [DOI] [PubMed] [Google Scholar]
- 16.Wilson B, Cockburn J, Halligan P. Behavioural Inattention Test Manual. Bury St Edmunds, UK: Thames Valley Test Company; 1987. [Google Scholar]
- 17.Boys MP, Fisher P, Holzberg C, Reid DW. The OSOT perceptual evaluation: A research perspective. Am J Occup Ther. 1988;42:92–8. doi: 10.5014/ajot.42.2.92. [DOI] [PubMed] [Google Scholar]
- 18.Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: A practical method for grading cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–98. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- 19.Rustad RA, et al. Cognitive Assessment of Minnesota. Texas, USA: Harcourt Assessment; 1993. [Google Scholar]
- 20.Wilson B, Cockburn J, Baddeley A, Hiorns R. The development and validation of a test battery for detecting and monitoring everyday memory problems. J Clin Exp Neuropsychol. 1989;11:855–70. doi: 10.1080/01688638908400940. [DOI] [PubMed] [Google Scholar]
- 21.Unsworth CA. Cognitive and perceptual dysfunction. Philadelphia FA: Davis Company; 1999. [Google Scholar]
- 22.Kendall FP, McCreary EK. Muscles: Testing and function. 2nd ed. Baltimore: Williams and Wilkins; 1983. [Google Scholar]
- 23.Hammer A, Lindmark B. Test-retest reliability of grip force in patients with stroke. J Rehabil Med. 2003;35:189–94. doi: 10.1080/16501970306132. [DOI] [PubMed] [Google Scholar]
- 24.Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, Rogers S. Grip and pinch strength: normative data for adults. Arch Phys Med Rehabil. 1985;66:69–74. [PubMed] [Google Scholar]
- 25.Croarkin E, Danoff J, Barnes C. Evidence-based rating of upper-extremity motor function tests used for people following a stroke. Phys Ther. 2004;84:62–74. [PubMed] [Google Scholar]
- 26.Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987;67:206. doi: 10.1093/ptj/67.2.206. [DOI] [PubMed] [Google Scholar]
- 27.Boyd R, Graham H. Objective measurement of clinical findings in the use of botulinum toxin for the management of children with cerebral palsy. Eur J Neurol. 1999;6:523. [Google Scholar]
- 28.Lyle RC. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int J Rehabil Res. 1981;4:483–92. doi: 10.1097/00004356-198112000-00001. [DOI] [PubMed] [Google Scholar]
- 29.Wolf SL, Catlin PA, Ellis M, Archer AL, Morgan B, Piacentino A. Assessing Wolf Motor Function Test as an outcome measure for research in patients after stroke. Stroke. 2001;32:1635–9. doi: 10.1161/01.str.32.7.1635. [DOI] [PubMed] [Google Scholar]
- 30.Kopp B, Kunkel A, Flor H, Platz T, Rose U, Mauritz KH, et al. The arm motor ability test: Reliability, validity, and sensitivity to change of an instrument for assessing disabilities in activities of daily living. Arch Phys Med Rehabil. 1997;78:615–20. doi: 10.1016/s0003-9993(97)90427-5. [DOI] [PubMed] [Google Scholar]
- 31.Lannin NA. Reliability, validity and factor structure of the upper limb subscale of the Motor Assessment Scale (UL-MAS) in adults following stroke. Disabil Rehabil. 2004;26:109–15. doi: 10.1080/0963828032000157970. [DOI] [PubMed] [Google Scholar]
- 32.Barreca S, Stratford PW, Lambert CL, Masters LM, Streiner DL. Test-retest reliability, validity, and sensitivity of the Chedoke arm and hand activity inventory: A new measure of upper-limb function for survivors of stroke. Arch Phys Med Rehabil. 2005;56:1616–22. doi: 10.1016/j.apmr.2005.03.017. [DOI] [PubMed] [Google Scholar]
- 33.Dai YT. Effectiveness of a pilot project of discharge planning in Taiwan. Res Nursing Health. 2003;26:53–63. doi: 10.1002/nur.10067. [DOI] [PubMed] [Google Scholar]
- 34.Gustafsson S, Sunnerhagen KA, Dahlin-Ivanoff S. Occupational Therapists' and patients' perceptions of ABILHAND, a new assessment tool for measuring manual ability. Scand J Occup Ther. 2004;11:107–17. [Google Scholar]
- 35.Morris DM, Uswatte G, Crago JE, Cook EW, 3 rd, Taub E. The reliability of the Wolf Motor Function Test for assessing upper extremity function after stroke. Arch Phys Med Rehabil. 2001;82:750–5. doi: 10.1053/apmr.2001.23183. [DOI] [PubMed] [Google Scholar]
- 36.Legg L, Drummond A, Leonardi-Bee J, Gladman JR, Corr S, Donkervoort M, et al. Occupational therapy for patients with problems in personal activities of daily living after stroke: Systematic review of randomised trials. BMJ. 2007;335:922–30. doi: 10.1136/bmj.39343.466863.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nuyens GE, De Weerdt WJ, Spaepen AJ, Jr, Kiekens C, Feys HM. Reduction of spastic hypertonia during repeated passive knee movements in stroke patients. Arch Phys Med Rehabil. 2002;83:930–5. doi: 10.1053/apmr.2002.33233. [DOI] [PubMed] [Google Scholar]
- 38.Gracies JM, Marosszeky JE, Renton R, Sandanam J, Gandevia SC, Burke D. Short-term effects of dynamic lycra splints on upper limb in hemiplegic patients. Arch Phys Med Rehabil. 2000;81:1547–55. doi: 10.1053/apmr.2000.16346. [DOI] [PubMed] [Google Scholar]
- 39.Van Kuijk AA, Geurts AC, Bevaart BJ, van Limbeek J. Treatment of upper extremity spasticity in stroke patients by focal neuronal or neuromuscular blockade: A systematic review of the literature. J Rehabil Med. 2002;34:51–61. doi: 10.1080/165019702753557836. [DOI] [PubMed] [Google Scholar]
- 40.Pandyan AD, Granat MH, Stott DJ. Effects of electrical stimulation on flexion contractures in the hemiplegic wrist. Clin Rehabil. 1997;11:123–30. doi: 10.1177/026921559701100205. [DOI] [PubMed] [Google Scholar]
- 41.Mortenson PA, Eng JJ. The use of casts in the management of joint mobility and hypertonia following brain injury in adults: A systematic review. Phys Ther. 2003;83:648–58. [PubMed] [Google Scholar]
- 42.Brooke MM, de Lateur BJ, Diana-Rigby GC, Questad KA. Shoulder subluxation in hemiplegia: Effects of three different supports. Arch Phys Med Rehabil. 1991;72:582–6. [PubMed] [Google Scholar]
- 43.Moodie N, Brisbin J, Morgan A. Subluxation of the glenohumeral joint in hemiplegia: Evaluation of supportive devices. Physiother Can. 1986;38:151–7. [Google Scholar]
- 44.Williams R, Tafts L, Minuk T. Evaluation of two support methods for the subluxed shoulder of hemiplegic patients. Phys Ther. 1988;68:1209–14. [PubMed] [Google Scholar]
- 45.Zorowitz RD, Idank D, Ikai T, Hughes MB, Johnston MV. Shoulder subluxation after stroke: A comparison of four supports. Arch Phys Med Rehabil. 1995;76:763–71. doi: 10.1016/s0003-9993(95)80532-x. [DOI] [PubMed] [Google Scholar]
- 46.Faghri PD. The effects of neuromuscular stimulation-induced muscle contraction versus elevation on hand edema in CVA patients. J Hand Ther. 1997;10:29–34. doi: 10.1016/s0894-1130(97)80008-7. [DOI] [PubMed] [Google Scholar]
- 47.Glanz M, Klawansky S, Stason W, Berkey C, Chalmers TC. Functional electrical stimulation in poststroke rehabilitation: A meta-analysis of the randomized controlled trials. Arch Phys Med Rehabil. 1996;77:549–53. doi: 10.1016/s0003-9993(96)90293-2. [DOI] [PubMed] [Google Scholar]
- 48.Van Peppen RP, Kwakkel G, Wood-Dauphinee S, Hendriks HJ, Van der Wees PJ, Dekker J. The impact of physical therapy on functional outcomes after stroke: What's the evidence? Clin Rehabil. 2004;18:833–62. doi: 10.1191/0269215504cr843oa. [DOI] [PubMed] [Google Scholar]
- 49.Morris SL, Dodd KJ, Morris ME. Outcomes of progressive resistance strength training following stroke: A systematic review. Clin Rehabil. 2004;18:27–39. doi: 10.1191/0269215504cr699oa. [DOI] [PubMed] [Google Scholar]
- 50.Carey J, Matyas T. 3rd annual perception for action. Melbourne: Cleveland Digital Printing; 2000. Somatosensory discrimination after stroke: Stimulus speciþ c versus generalisation training. [Google Scholar]
- 51.Duncan P, Studenski S, Richards L, Gollub S, Lai SM, Reker D, et al. Randomized clinical trail of therapeutic exercise in subacute stroke. Stroke. 2003;34:2173–80. doi: 10.1161/01.STR.0000083699.95351.F2. [DOI] [PubMed] [Google Scholar]
- 52.Winstein CJ, Rose DK, Tan SM, Lewthwaite R, Chui HC, Azen SP. A randomized controlled comparison of upper-extremity rehabilitation strategies in acute stroke: A pilot study of immediate and long-term outcomes. Arch Phys Med Rehabil. 2004;85:620–8. doi: 10.1016/j.apmr.2003.06.027. [DOI] [PubMed] [Google Scholar]
- 53.Nelson DL, Konosky K, Fleharty K, Webb R, Newer K, Hazboun VP, et al. The effects of an occupationally embedded exercise on bilaterally assisted supination in persons with hemiplegia. Am J Occup Ther. 1996;50:639–46. doi: 10.5014/ajot.50.8.639. [DOI] [PubMed] [Google Scholar]
- 54.Kwakkel G, van Peppen R, Wagenaar RC, Wood Dauphinee S, Richards C, Ashburn A, et al. Effects of augmented exercise therapy time after stroke: A meta-analysis. Stroke. 2004;35:2529–39. doi: 10.1161/01.STR.0000143153.76460.7d. [DOI] [PubMed] [Google Scholar]
- 55.Bowen A, Lincoln NB, Dewey M. Cognitive rehabilitation for spatial neglect following stroke. Cochrane Database Syst Rev. 2002;2:CD003586. doi: 10.1002/14651858.CD003586. [DOI] [PubMed] [Google Scholar]
- 56.Donkervoort M. Efficacy of strategy training in left hemisphere stroke patients with apraxia: A randomised clinical trial. Neuropsychol Rehabil. 2001;11:549. [Google Scholar]
- 57.Lincoln NB, Majid MJ, Weyman N. Cognitive rehabilitation for attention deficits following stroke. Cochrane Database Syst Rev. 2000;4:CD002842. doi: 10.1002/14651858.CD002842. [DOI] [PubMed] [Google Scholar]
- 58.Wilson BA, Emslie HC, Quirk K, Evans JJ. Reducing everyday memory and planning problems by means of a paging system: A randomised controlled control crossover study. J Neurol Neurosurg Psychiatry. 2001;70:477–82. doi: 10.1136/jnnp.70.4.477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Corr S, Bayer A. Occupational therapy for stroke patients after hospital discharge: A randomized controlled trial. Clin Rehabil. 1995;9:291–6. [Google Scholar]
- 60.Kalra L, Evans A, Perez I, Melbourn A, Patel A, Knapp M, et al. Training carers of stroke patients: Randomised controlled trial. Br Med J. 2004;328:1099. doi: 10.1136/bmj.328.7448.1099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Forster A, Young J, Langhorne P. Medical day hospital care for elderly versus alternative forms of care. Cochrane Database Syst Rev. 2000;2:CD001730. doi: 10.1002/14651858.CD001730. [DOI] [PubMed] [Google Scholar]
- 62.Trialists OS. Therapy-based rehabilitation services for stroke patients at home. 2002 doi: 10.1002/14651858.CD002925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Britton M, Andersson A. Home rehabilitation after stroke: Reviewing the scientific evidence on effects and costs. Int J Technol Assess Health Care. 2000;16:842–8. doi: 10.1017/s0266462300102119. [DOI] [PubMed] [Google Scholar]
- 64.Mishra S. Occupational therapy in community based rehabilitation. Indian J Occup Ther. 2003;35:13–6. [Google Scholar]
- 65.Winkler D, Farnworth L, Sloan S. People under 60 living in aged acre facilities in Victoria. Aust Health Rev. 2006;30:100–8. [PubMed] [Google Scholar]
- 66.Walker MF, Leonardi-Bee J, Bath P, Langhorne P, Dewey M, Corr S, et al. Individual patient data analysis of randomized controlled trials of community occupational therapy for stroke patients. Stroke. 2004;35:2226–32. doi: 10.1161/01.STR.0000137766.17092.fb. [DOI] [PubMed] [Google Scholar]
- 67.Huck J, Bonhotal B. Fastener systems on apparel for hemiuplegic stroke victims. Appl Ergon. 1997;28:277–82. doi: 10.1016/s0003-6870(96)00072-5. [DOI] [PubMed] [Google Scholar]
- 68.Trombly CA, Radomski MV. Occupational therapy for physical dysfunction. 5th ed. Baltimore: Lippincott Williams and Wilkins; 2002. [Google Scholar]
- 69.Carr E, Kenney F. Positioning of the stroke patient: A review of the literature. Int J Nursing Studies. 1992;29:355–69. doi: 10.1016/0020-7489(92)90014-8. [DOI] [PubMed] [Google Scholar]
- 70.Royal College of Physicians, National clinical guidelines for stroke. 2nd ed. Royal College of Physicians; 2004. [Google Scholar]
- 71.Ausroads, Assessing þ tness to drive: For commercial and private vehicle drivers. Sydney: Ausroads; 2003. [Google Scholar]
- 72.Unsworth CA. Review of tests contributing to the occupational therapy off road driver assessment. Aust Occup Ther J. 2005;52:57–74. [Google Scholar]