

Abstract
Aim:
The present study was to investigate the root canal morphology of mandibular premolars in Malaysian population using cone-beam computed tomography (CBCT) and microcomputed tomography (micro-CT) scanned images.
Materials and Methods:
Sixty selected mandibular premolars were evaluated in vitro and the root canal morphologies of the samples were categorized based on Vertucci's classification. The position of apical foramen, presence, and location of lateral canal, as well as prevalence of apical delta, were also determined.
Results:
Invariably, Type I variety (Vertucci's classification) was the most frequent root canal morphology followed by Type V and Type III after micro-CT imaging. CBCT investigation also revealed Type I as the most numerous; however, the second most common configuration was Type III followed closely by others. There was a moderate agreement in Vertucci's classification of root canal configuration and also prevalence of apical delta (kappa: 0.516 and 0.550, respectively). However, only a fair agreement (kappa: 0.289) was observed between CBCT and micro-CT on the prevalence of lateral canal.
Conclusion:
CBCT should be cautiously used in determining root canal configuration as deficiencies were evident and revealed during micro-CT imaging.
Keywords: Apical delta, cone-beam computed tomography, lateral canal, microcomputed tomography, root canal morphology
INTRODUCTION
A thorough and complete understanding of the root canal morphology is paramount to the success of root canal therapy. The inability to detect, carry out proper mechanochemical preparation, and seal one or more of the root canals is one of the main causes of endodontic treatment failure.[1] Based on the findings in a study by Hoen and Pink,[2] the incidence of missed roots or canals in the teeth that needed retreatment was 42%. In addition, great difficulty can be anticipated when carrying out mandibular premolar root canal treatment due to the wide variability of the root canal configuration.[3] Multiple root canals, lateral canals, apical deltas, and C-shaped canals are commonly found in lower premolar teeth.[4] Root canal configurations in lower premolars may vary significantly with respect to gender[5,6] and also ethnicity.[6,7,8]
Numerous studies have indicated that 11.53% to 46% of mandibular first premolars have more than one root canal.[9] Another common anatomical variation that may contribute significantly to the clinical outcome, treatment strategy, and success rate is the presence of apical delta. Apical delta is the pulp canal morphology, in which the main canal divides into multiple accessory canals at or near the apex,[10] and is almost inaccessible by instrumentation, irrigation, and medicaments.[4] This will therefore cause the retention and multiplication of bacteria.
The most common method of imaging for the evaluation of root canal configuration, diagnosis, and treatment planning is intraoral periapical radiograph/digital images. However, this two-dimensional imaging technique may not produce enough information that can be of sufficient help in achieving accurate diagnosis.[11,12,13,14,15] Cone-beam computed tomography (CBCT) imaging can reveal clear and precise three-dimensional (3D) images without superimposition of anatomical structures. Studies have shown that despite slightly higher exposure to radiation, the benefit of CBCT imaging in the evaluation of root canal anatomy outweighs any associated risk due to X-rays.[16,17]
Several recent studies, however, found that CBCT imaging could fail in the identification of lateral canals[18] and the detection of some varieties of root canal morphology.[15,19] Therefore, other advanced imaging methods need to be explored for extensive understanding of the root canal morphology and any radicular variations in three dimensions.[20] Microcomputed tomography (micro-CT) imaging provided for these deficiencies as it more precise due to its high spatial resolution. Moreover, with the availability of the 3D analysis software, it makes the images the gold standard as they provide optimum image quality for visualizing various structures.
Realizing that a more detailed study of the canal system was important, this study was conducted to evaluate the root canal anatomy classification (based on Vertucci's method)[21] and to detect lateral canals as well as apical deltas using CBCT scanned images and comparing them with more exacting and divulging micro-CT images.
MATERIALS AND METHODS
Tooth selection
Extracted mandibular premolars with fully formed apices from patients of Mongoloid ancestry (ethnic Chinese and Malays) were collected. Teeth that were carious, restored, fractured, showing evidence of root resorption or endodontically treated, were excluded from this study. Consequently, from a sample size of 89 teeth, 60 teeth that fulfilled the criteria were carefully selected. Institutional ethical approval was requested although the study was conducted on in vitro teeth.
Specimen preparation
All teeth were placed in 2.5% sodium hypochlorite for 2 h, after which any remaining extraneous tissues and calculus were removed with ultrasonic scalers.
Cone-beam computed tomography scan acquisition
The teeth were mounted in upright position and stabilized using beading wax. The wax block was then placed in a paper cup, stabilized on the CBCT machine's chin rest, and the teeth scanned. The CBCT EzDent-Vatech Imaging Systems (Korea) was set at parameters of 85 kV and 4.5 mA, with the smallest voxel size of 0.125 mm and a field-of-view 5 cm × 5 cm throughout the whole imaging procedure [Figure 1].
Figure 1.

Placement of the samples on beading wax for Placement of the samples on beading wax for cone-beam computed tomography imaging on the machine's chinrest imaging on the machine's chinrest
Microcomputed tomography investigation
The teeth were placed in horizontal position in the specimen chamber of the micro-CT scanner and stabilized using paper adhesive tape [Figure 2]. Scans were acquired with a Skyscan 1076 (Bruker Corporation, Billerica, Massachusetts, USA), with the following specifications: electrical circuit's power of 70 kV, pixel size of 9, aluminum filter 0.5 mm, utilization of 3 frames, and a rotation degree of 0.7°. This system allows to reach a spatial resolution of 15 um corresponding to near 3 × 10− 6 cubic mm voxel size. The data were then reconstructed for image interpretation and analysis using CTvox software (Bruker Corporation, Billerica, Massachusetts, USA). All data gathered were analyzed using SPSS version 25 (SPSS Inc., Chicago, USA) software program.
Figure 2.
A close-up view of the placement of the specimen in the micro-computed tomography machine for scanning
RESULTS
The mean length of the selected premolars was measured to be 19.9 mm with a standard deviation of 2.08 mm. 43 out of 60 teeth (71.67%) showed distal curvature of the root canal system. Single root canals were noticed in CBCT scans of 49 teeth (81.67%), whereas micro-CT images showed 37 teeth (61.67%). A more complicated root canal system (i.e., more than one root canal) was observed in 11 teeth (18.33%) and 23 teeth (38.33%) by CBCT and micro-CT imaging, respectively.
Besides root canal configuration, other important characteristics of root canal morphology such as position of apical foramen, prevalence, and position of lateral canal, as well as the prevalence of apical delta, were also determined and recorded [Table 1]. Based on the micro-CT evaluation, fifty-five percent of the apical foramina (33 out of 60 teeth) were found to be located in the center of root apices. The rest were located on the lateral aspect of the root apices. Lateral canals were detected in 35% (21 out of 60 teeth) of the samples. Lateral canals were located in the coronal (4%), middle (44%), and apical thirds (52%) of the roots. Some teeth were found to possess more than one lateral canal. Apical deltas were found in 5 (8.33%) of the samples.
Table 1.
Number of teeth with apical foramina, lateral canal, and apical delta and their positions
| Position of apical foramen | |
| Centre | 33 (55) |
| Lateral | 27 (45) |
| Teeth with lateral canal | 21 (35) |
| Location of lateral canal | |
| Coronal | 1 (4) |
| Middle | 11 (44) |
| Apical | 13 (52) |
| Teeth with apical delta | 5 (8.33) |
Root canal configuration
The results indicated that Vertucci's Type I canal configuration represented the highest percentage 49 (81.7%) and 37 (61.67%) when analyzed with CBCT and micro-CT, respectively. With regard to numbers, micro-CT images revealed Type I (37 teeth), followed by Type V (10 teeth) and III (7 teeth) [Table 2]. Types VI and VII configurations were seen in 2 teeth each, while one tooth each showed Types II and IV canal systems. No tooth was detected as having Type VIII configuration. As indicated earlier, 49 teeth were reported as having Type I root canal configuration in CBCT images. Out of these, four teeth were actually Type III and eight teeth were Type V when verified with micro-CT.
Table 2.
Distribution of root canal systems found in mandibular premolars according to Vertucci’s classification
| Vertucci’s classification | CBCT, n (%) | Micro-CT, n (%) |
|---|---|---|
| I (1) | 49 (81.67) | 37 (61.67) |
| II (2-1) | 1 (1.67) | 1 (1.67) |
| III (1-2-1) | 3 (0.05) | 7 (11.67) |
| IV (2) | 2 (3.33) | 1 (1.67) |
| V (1-2) | 2 (3.33) | 10 (16.67) |
| VI (2-1-2) | 2 (3.33) | 2 (3.33) |
| VII (1-2-1-2) | 1 (1.67) | 2 (3.33) |
| VIII (3) | 0 | 0 |
CT: Computed tomography, CBCT: Cone-beam CT
Out of the seven Type III cases confirmed by the micro-CT technique, only three teeth were described as Type III by CBCT technique, and the remaining four teeth were recorded as Type I [Table 2]. As for Type IV, out of two cases reported with CBCT technique, only one tooth was confirmed with micro-CT as being correct; the other tooth was eventually confirmed as Type V using micro-CT [Figure 3]. For Type V canal configuration, out of ten cases confirmed with the micro-CT technique, only one was revealed as Type V with CBCT; the remaining nine teeth were recorded as Type I (eight teeth) and Type IV (one tooth). Out of the two cases of Type VII confirmed with micro-CT, only one case was correctly identified with CBCT; the other tooth was reported as Type V. Nevertheless, almost three quarter of the sample, that is, 46 teeth (76.67%), were classified to be similar by both techniques.
Figure 3.
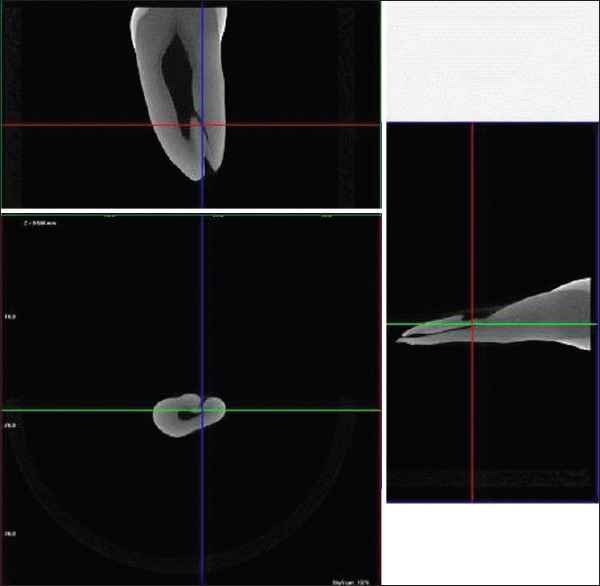
Micro-computed tomography image showing Vertucci Type V root canal configuration
Lateral canal
Table 3 shows that 44 teeth (73.33%) were in agreement when imaged using both techniques (Kappa = 0.289). This means the findings from both techniques (CBCT and micro-CT) shared similar results. 5 teeth showed the presence of lateral canals and 39 teeth did not reveal any lateral canals. However, on closer analysis of the table shows micro-CT detected another 16 teeth with lateral canals.
Table 3.
Cross-tabulation between cone-beam computed tomography and micro-computed tomography in detecting lateral canals
| Lateral canal CBCT | Micro-CT | Total | |
|---|---|---|---|
|
| |||
| Yes | No | ||
| Yes | 5 | 0 | 5 |
| No | 16 | 39 | 55 |
| Total | 21 | 39 | 60 |
CT: Computed tomography, CBCT: Cone-beam CT, Yes: Lateral canal detected, No: Lateral canal not detected
Apical delta
Of all teeth studied, apical deltas were found in 5 out of 60 teeth (8.33%) [Table 4]. However, 57 teeth (95%) shared similar findings when both CBCT and micro-CT techniques were used (Kappa = 0.550) [Table 4].
Table 4.
Cross-tabulation between cone-beam computed tomography and micro-computed tomography in detecting apical deltas
| Apical delta CBCT | Micro-CT | Total | |
|---|---|---|---|
|
| |||
| SF | AD | ||
| SF | 55 | 3 | 58 |
| AD | 0 | 2 | 2 |
| Total | 55 | 5 | 60 |
SF: Single foramen, AD: Apical delta, CT: Computed tomography, CBCT: Cone-beam CT
DISCUSSION
CBCT offers a practical, reliable, and accurate modality to three-dimensionally assess the root canal morphology of in vivo teeth. Higher cost and relatively higher radiation dose may hinder its routine usage for all endodontic patients. However, CBCT should be considered as first-hand supplement when the routine two-dimensional intraoral periapical (IOPA) radiographs/digital images appear inconclusive. Micro-CT is a relatively new technology, which has recently gained popularity in laboratory endodontic research. Small voxel size of micro-CT creates excellent images based on the multislice of X-ray. It can be used to evaluate the internal morphology of tooth, obturation of the canal, and also to calculate the filling area.[22]
Preoperative understanding of the root canal configuration is paramount to the success of endodontic therapy. The knowledge also helps reducing procedural accidents during root canal treatment. A study to assess the root canal morphology of permanent teeth in a Malaysian subpopulation was undertaken by Pan et al. in 2019.[23] Two hundred and eight CBCT images were evaluated retrospectively. The researchers evaluated the extra root or canal prevalence and configuration according to the Vertucci's method of classification. Their findings showed that 18.7% of mandibular first premolars and 0.5% of second premolars contained 2 canals. This was similar to the CBCT finding in this study but definitely did not correspond the results employing micro-CT.
Similarly, John et al. carried out a CBCT study to evaluate the configuration of the root canal system in 400 lower first premolars in an Indian subpopulation.[24] A 3D reconstruction technique utilizing semiautomated threshold-based segmentation was carried out on the CBCT imaging of the samples. The configuration of the mandibular first premolar root canal system was studied and classified according to the Vertucci's method. 78.75% (315 teeth) of the samples showed Type I root canal configuration. 1.25% (5 teeth) were seen to have Type II, while Type III was detected in 3 teeth (0.75%). Types IV, V, and VIII root canal configurations were seen in 64 teeth (16%), 11 teeth (2.75%), and 2 teeth (0.5%), respectively. Interestingly, the study drew a conclusion that Type I configuration made up most of the samples (78.75%), which corresponded with the findings of the present study. Type IV was the second highest, followed by Types V, II, III, and VIII in the declining order.
An investigation to study the root canal anatomy of lower premolars using tooth clearing and CBCT techniques was carried out by Khademi et al. in 2017.[25] The study involved an in vitro evaluation of 182 lower first and second premolars. The root canal configuration of the teeth was determined according to the Vertucci's method of classification. Further investigations were carried out to determine prevalence of lateral canals and C-shaped canals. After Type I, the next most frequent morphologies in both first and second premolars were Type V and Type IV. C-shaped root canal morphology was seen in 6.6% and 4.4% of the first premolars using CBCT and clearing techniques, respectively. However, no C-shaped canal was detected in second premolars. Interestingly, CBCT showed a higher accuracy in determining C-shaped root canal morphology than the clearing technique. However, no C-shaped canals were noticed in the present study.
In another study which was carried out in Iran, Hajihassani et al. in 2017 utilized 145 CBCT images to evaluate the lower premolar root canal configurations.[26] It was reported that 95.97% of first premolars and all second premolars had a single root. 62.6% Type I, 0.8% Type II, 10.9% Type III, 0.8% Type IV, 20.3% Type V, 4.2% Type VI, and 0.8% Type VII were detected in the lower first premolars. 78% Type I, 3% Type II, 11% Type III, 7% Type V, and 1% Type VI configurations were seen in the mandibular second premolars. In general, the variations in this study concur with the present study despite being studied in a different population.
In the study by Dou et al.[27] in the Chinese population, 178 teeth were evaluated using micro-CT.[25] Types I, V, and III canals based on Vertucci's method were noted in 114 teeth (64.04%), 39 teeth (21.91%), and 19 teeth (10.67%), respectively. This sequence of top three most frequent root canal configurations is in agreement with the present study. Other canal types (i.e., II, IV, and VIII) were observed in 2 teeth (1.12%), 1 tooth (0.56%), and 2 teeth (1.12%), respectively. Lateral canals were detected in 71 teeth (39.89%), which is comparable to 35% recorded in the present study. 10.11% (18 teeth) of the samples were found to have apical deltas; this is also quite close to the 8.33% (5 teeth) prevalence seen in the present study.
In another investigation, the performance of IOPA radiography and CBCT imaging to determine the root canal morphology and detect apical delta was studied against micro-CT scanned images.[11] In the results, apical deltas were detected in 33.3% of root canals using the micro-CT. When comparisons were made, both IOPA and CBCT imaging tend to underestimate the presence of apical deltas rendering it an unreliable imaging method, a finding similar to the present study. Interestingly, Gao et al.[28] found that the apical delta branches were not straight, and the cross-sections of the branches were not circular either.
Clinical implications of this study indicate that the CBCT imaging technique is a moderately reliable tool to assess the configuration of the root canal system and the presence of apical deltas in patients. In addition, Vertucci's type I configuration is the most commonly found root canal system in lower premolar teeth. Types V and III are second and third most common, respectively. Lateral canals are frequently seen in lower premolars (35%) as revealed by micro-CT; hence, its presence can be expected in about one-third of lower premolar teeth during root canal treatment. Apical deltas are rare (8.33%), and its presence can be expected in <10% of lower premolars during root canal therapy.
In summary, the findings in the present study indicate that CBCT imaging is in moderate agreement with micro-CT in identifying root canal configuration based on Vertucci's classification and (kappa = 0.550) and in detecting apical deltas (kappa = 0.516). However, it is only in fair agreement with micro-CT in detecting lateral canals (kappa = 0.289). However, it is evident that the detection of lateral canals and apical deltas from CBCT images is much fewer than noticed with micro-CT images. Moreover, their detection will reduce further if scanned in vivo teeth are studied, unlike with extracted teeth in the present study.
It is recommended that in future studies, investigations should be undertaken on a bigger sample size with more advanced CBCT (smaller voxel sizes) and micro-CT imaging systems. Considerations should also be given to the ethnicity, gender, and quadrant of the origin of the sample (both in vitro and in vivo teeth).
CONCLUSION
Micro-CT is an excellent tool to study the internal morphology of human teeth due to its high resolution of the in situ specimen. Its high capability to capture anatomical details such as lateral canals and apical deltas makes micro-CT the gold standard for root canal morphology. However, this can only be performed with in vitro teeth in a laboratory-related environment. Our comparison study demonstrates that CBCT is still an accepted imaging modality. However, caution must be expressed here as there is a possibility of mistaking the type of root canals, likelihood of missing the lateral canals and apical deltas in a limited number of patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The research was supported by MAHSA University Research Grant.
REFERENCES
- 1.Cantatore G, Berutti E, Castellucci A. Missed anatomy: Frequency and clinical impact. Endod Top. 2006;15:3–31. [Google Scholar]
- 2.Hoen MM, Pink FE. Contemporary endodontic retreatments: An analysis based on clinical treatment findings. J Endod. 2002;28:834–6. doi: 10.1097/00004770-200212000-00010. [DOI] [PubMed] [Google Scholar]
- 3.Slowey RR. Root canal anatomy. Road map to successful endodontics. Dent Clin North Am. 1979;23:555–73. [PubMed] [Google Scholar]
- 4.De Moor RJ, Calberson FL. Root canal treatment in a mandibular second premolar with three root canals. J Endod. 2005;31:310–3. doi: 10.1097/01.don.0000140578.36109.c0. [DOI] [PubMed] [Google Scholar]
- 5.Serman NJ, Hasselgren G. The radiographic incidence of multiple roots and canals in human mandibular premolars. Int Endod J. 1992;25:234–7. doi: 10.1111/j.1365-2591.1992.tb01155.x. [DOI] [PubMed] [Google Scholar]
- 6.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30:391–8. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 7.Trope M, Elfenbein L, Tronstad L. Mandibular premolars with more than one root canal in different race groups. J Endod. 1986;12:343–5. doi: 10.1016/S0099-2399(86)80035-8. [DOI] [PubMed] [Google Scholar]
- 8.Walker RT. Root form and canal anatomy of mandibular second molars in a southern Chinese population. J Endod. 1988;14:325–9. doi: 10.1016/S0099-2399(88)80192-4. [DOI] [PubMed] [Google Scholar]
- 9.Scarfe WC. Imaging of maxillofacial trauma: Evolutions and emerging revolutions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100:S75–96. doi: 10.1016/j.tripleo.2005.05.057. [DOI] [PubMed] [Google Scholar]
- 10.AAE Special Committee to Revise the Glossary. 10th ed. Chicago: American Association of Endodontists; 2020. Glossary of Endodontic Terms. [Google Scholar]
- 11.Bueno MR, Estrela C, De Figueiredo JA, Azevedo BC. Map-reading strategy to diagnose root perforations near metallic intracanal posts by using cone beam computed tomography. J Endod. 2011;37:85–90. doi: 10.1016/j.joen.2010.08.006. [DOI] [PubMed] [Google Scholar]
- 12.Durack C, Patel S. Cone beam computed tomography in endodontics. Braz Dent J. 2012;23:179–91. doi: 10.1590/s0103-64402012000300001. [DOI] [PubMed] [Google Scholar]
- 13.Junqueira RB, Verner FS, Campos CN, Devito KL, do Carmo AM. Detection of vertical root fractures in the presence of intracanal metallic post: A comparison between periapical radiography and cone-beam computed tomography. J Endod. 2013;39:1620–4. doi: 10.1016/j.joen.2013.08.031. [DOI] [PubMed] [Google Scholar]
- 14.Patel S, Durack C, Abella F, Shemesh H, Roig M, Lemberg K. Cone beam computed tomography in endodontics – A review. Int Endod J. 2015;48:3–15. doi: 10.1111/iej.12270. [DOI] [PubMed] [Google Scholar]
- 15.Espir CG, Nascimento CA, Guerreiro-Tanomaru JM, Bonetti-Filho I, Tanomaru-Filho M. Radiographic and micro-computed tomography classification of root canal morphology and dentin thickness of mandibular incisors. J Conserv Dent. 2018;21:57–62. doi: 10.4103/JCD.JCD_230_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sousa TO, Haiter-Neto F, Nascimento EH, Peroni LV, Freitas DQ, Hassan B. Diagnostic accuracy of periapical radiography and cone-beam computed tomography in identifying root canal configuration of human premolars. J Endod. 2017;43:1176–9. doi: 10.1016/j.joen.2017.02.021. [DOI] [PubMed] [Google Scholar]
- 17.Venskutonis T, Plotino G, Juodzbalys G, Mickevičienė L. The importance of cone-beam computed tomography in the management of endodontic problems: A review of the literature. J Endod. 2014;40:1895–901. doi: 10.1016/j.joen.2014.05.009. [DOI] [PubMed] [Google Scholar]
- 18.Sousa TO, Hassan B, Mirmohammadi H, Shemesh H, Haiter-Neto F. Feasibility of cone-beam computed tomography in detecting lateral canals before and after root canal treatment: An ex vivo study. J Endod. 2017;43:1014–7. doi: 10.1016/j.joen.2017.01.025. [DOI] [PubMed] [Google Scholar]
- 19.Natanasabapathy V, Rajesh PS, Ashritha MC, Mishra A, Namasivayam A, Kandaswamy D, et al. Root canal isthmi and interorifice distance in human permanent teeth of an Indian subpopulation using cone-beam computed tomography: A retrospective cross-sectional study. J Conserv Dent. 2020;23:563–70. doi: 10.4103/JCD.JCD_576_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kottoor J, Albuquerque D, Velmurugan N, Kuruvilla J. Root anatomy and root canal configuration of human permanent mandibular premolars: A systematic review. Anat Res Int. 2013;2013:254250. doi: 10.1155/2013/254250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 22.Nascimento EH, Abrahão Elias MR, Vasconcelos VH, Haiter-Neto F, Mendonça EF, Sousa TO. Ex vivo detection of apical delta in premolars: A comparative study using periapical radiography, cone-beam computed tomography, and micro-computed tomography. J Endod. 2019;45:549–53. doi: 10.1016/j.joen.2019.02.022. [DOI] [PubMed] [Google Scholar]
- 23.Pan JY, Parolia A, Chuah SR, Bhatia S, Mutalik S, Pau A. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC Oral Health. 2019;19:14. doi: 10.1186/s12903-019-0710-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.John D, Jayasree S, Ramesh Kumar M, Abdul Rahman TV, Gokulraj R. A cone-beam computed tomography study of the root canal morphology of mandibular first premolars in an Indian subpopulation. IOSR J Dent Med Sci. 2017;16:51–6. [Google Scholar]
- 25.Khademi A, Mehdizadeh M, Sanei M, Sadeqnejad H, Khazaei S. Comparative evaluation of root canal morphology of mandibular premolars using clearing and cone beam computed tomography. Dent Res J (Isfahan) 2017;14:321–5. doi: 10.4103/1735-3327.215964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hajihassani N, Roohi N, Madadi K, Bakhshi M, Tofangchiha M. Evaluation of root canal morphology of mandibular first and second premolars using cone beam computed tomography in a defined group of dental patients in Iran. Scientifica (Cairo) 2017;2017:1504341. doi: 10.1155/2017/1504341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Dou L, Li D, Xu T, Tang Y, Yang D. Root anatomy and canal morphology of mandibular first premolars in a Chinese population. Sci Rep. 2017;7:750. doi: 10.1038/s41598-017-00871-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gao X, Tay FR, Gutmann JL, Fan W, Xu T, Fan B. Micro-CT evaluation of apical delta morphologies in human teeth. Sci Rep. 2016;6:36501. doi: 10.1038/srep36501. [DOI] [PMC free article] [PubMed] [Google Scholar]