

Abstract
Introduction:
There is limited understanding of how burn injuries at different ages are associated with normal growth and development as well as the burn recovery process. This study provides new useful insights by comparing social participation outcomes among burn survivors injured in childhood compared with injuries sustained in middle age, and older adulthood.
Methods:
Items from the development of the LIBRE profile were administered to 601 adult burn survivors with ≥5% TBSA burned or burns to critical areas (hands, feet, face, or genitals). Each item was answered on a 5-point Likert scale with higher scores denoting better outcomes. Mean scores for the 6 LIBRE profile scales (sexual relationships, family and friends, social interactions, social activities, work and employment, and romantic relationships) were compared between those burned as children (<18years) and those burned as adults (≥18years). Regression analyses were used to assess differences between groups with adjustment for demographic and clinical characteristics.
Results:
Of the 597 burn survivors having complete data on age at injury, 165 (27.6%) sustained burn injuries as a child. Those burned as children were more frequently female than those burned as adults (57% vs 47%) and were also more frequently white non-Hispanic (89% vs 77%). Marital status and education level were similar in the two groups. Those who were burned as children had slightly higher scores on the social activities, work and employment and romantic relationships scales. However, these differences did not persist in adjusted regression analyses.
Conclusions:
Burn survivors who sustained injuries as a child fared at least as well as those burned as adults in a broad range of long-term social participation outcomes. The impact on long-term social participation outcomes of burn survivors was not significantly different between individuals with burns sustained during important developmental stages at young ages and those injured later in life.
Keywords: Burn injury, Psychosocial outcomes, Pediatrics, Developmental stages, Resilience
1. Introduction
An estimated 2 million individuals each year experience a burn injury in the U.S., with a 96.8% survival rate and 480,000 requiring medical treatment [1,2]. With improvements in survival rates over the past generation, there is an increasing clinical and research focus on social participation among burn survivors [3]. Social participation includes involvement in social, domestic and occupational domains, which are prominent areas of focus during rehabilitation for various injuries and impairments [4]. The crux of rehabilitation is community reintegration, social participation and quality of life. Burn survivors experience long term sequelae of their injuries that may include pain, itch, scarring, chronic wounds, contractures, bone complications, neuropathies, metabolic abnormalities, post-traumatic stress, depression, body image impairments, and sleep disorders [5]. In light of these multiple issues, individuals with burns experience social, physical, and emotional challenges related to their burn injuries that impact reintegration into the community.
Age at burn injury has a significant impact on morbidity and mortality outcomes [6]. The physical and psychological outcomes of young adults burned as children compared to young adults who had not experienced burn injuries have been studied, though to a limited extent and with inconsistent results. Studies show that young adults who experienced burns during childhood were functioning physically and psychologically within the normal range compared to aged-matched non-burned controls [7]. In contrast, other studies have shown that children who experience burn injuries had positive psychosocial outcomes as adults [8,9], but rated their overall quality of life lower than the general population [10]. A study shows that children burned at very young ages have similar mortality rates to those burned later in childhood [11]. Research to date has been limited by small sample sizes, varying burn sizes, single center study designs, and variation in the time since injury.
In light of normal aging and development, children experience additional challenges to psychosocial adjustment and recovery after burn injuries compared to adults [12]. The current literature supports both resilience and vulnerability in children when faced with traumatic injuries. There are several factors that influence a child’s adjustment after trauma and their level of resilience. The developmental stage a child is in when he or she sustains a burn injury may have an impact on psychosocial adjustment [13]. Children are often resilient when faced with challenges; however, sustaining a burn during critical stages of psychosocial development may hinder their adjustment and reintegration [14]. Studies within the pediatric resilience literature have described various factors that influence resilience, including positive self-perceptions, positive self-efficacy, faith and self-meaning, good cognitive abilities, close relationship with caregiving adults, structure/monitoring and expectations within the home and organized home environment. Studies have also looked at community factors that support resilience in children who have experienced trauma, including public health support services, health care availability, public safety and effective schools [15]. Despite the known factors contributing to resilience in children, not all children are fortunate enough to have this support and are at high risk for poor recovery [16–19]. Specifically, within the burn literature, factors associated with resilience in children after burn injuries include younger age and less severe intrusive and avoidance symptoms in caregivers [14]. Studies have also revealed that time elapsed since injury was related to resilience and improved quality of life [14,20]. It is not entirely clear how children will fare in the face of trauma.
Social participation in burn survivors has been less studied and there are currently no studies directly comparing social participation outcomes between burn survivors injured as children and those injured as adults [21,22]. The life impact burn recovery evaluation (LIBRE Profile) is a questionnaire developed to comprehensively assess the social impacts of burns [23–25]. The assessment focuses on capturing how burn survivors are reintegrating into the community. The purpose of the present study was to compare social participation of individuals burned as children with those burned as adults, by administering items from the large item pool used to calibrate the LIBRE profile and thus providing greater granularity at the item level. Identifying differences between these populations in terms of social participation and psychosocial aspects of recovery may facilitate how the interdisciplinary burn team focuses treatment plans.
2. Materials and methods
2.1. Study population
A total of 601 burn survivors were administered the LIBRE-192, which is comprised of 192 items used for field testing and calibration of the LIBRE profile [23]. The development of the 126-item LIBRE profile derived from the LIBRE-192 has been previously described [26]. The study population included 601 individuals >18years old with >5% TBSA burned or burns to critical areas (hands, feet, face, or genitals). Burn size was self reported. For patients that did not know their own TBSA, study staff used a systematic procedure to determine estimated burn size with the palmar method and rule of nine’s [27,28]. This systematic procedure included assigning a median value for burn size in participants who reported a TBSA range. All participants were assigned a TBSA quintile. Participants were recruited from burn conferences, clinical settings, direct mailings, the Internet, social media and peer support groups from October 2014 to December 2015. Not all participants were hospitalized. The battery was administered to each participant either by phone or via the Internet with a link to the survey website after obtaining informed consent. The survey was developed from a conceptual framework stemming from the World Health Organization (WHO) international classification of functioning, disability and health. Exploratory and confirmatory factor analysis were used to identify and validate six scales underlying the LIBRE profile: sexual relationships, family and friends, social interactions, social activities, work and employment, and romantic relationships [23,24,20]. Each item was answered on a 5-point Likert scale with higher scores denoting better outcomes. Connor Davidson’s Resilience scale while not specifically included in this study does overlap in terms of the internal-external locus of control nature of selected items expressed by some of the content in the LIBRE profile. The study was approved by the Boston University Medical Campus Institutional Review Board (Protocol H-32928) and all subjects provided informed consent (oral for phone participants, written for self-administered participants) prior to participating in any research study activities.
2.2. Statistical analysis
Scale scores were standardized to a mean of 50 and standard deviation of 10 based upon the entire burn sample of 601 participants used for the calibration phase of the LIBRE profile [24]. Mean scale scores for each of the six scales were compared between those burned as children (<18years) and those burned as adults (≥18years). A Generalized Additive Model (GAM) was used to test for a nonlinear relationship between independent variables (age at injury/time since burn, standardized continuous variables) and dependent variable (the scale scores). The model was adjusted by gender, marital status, TBSA burned, and work situation. In order to account for the non-linear relationship, GAM is the extension of the generalized linear model, which includes the non-parametric smooth function for the independent variables. Further, analysis of deviance (Chi-square test) was used to examine whether or not to include the smooth function to improve the model fit. If the Chi-square test was not statistically significant (P>0.05), a linear model (ordinary least squares regression analysis) was used to assess differences in scale scores between those who were burned at <18years of age versus those burned at 18years or greater, with adjustments for demographic and clinical characteristics. Adjusted models include gender, marital status, work status, TBSA burned, and time since burn injury. If the Chi-square test was statistically significant (p<0.05), a nonlinear (curvilinear) model was selected. The relationship between age at burn and scale score was plotted for participants at time since burn of 0.5 standard deviations below the mean of the sample, the mean of the sample, and 0.5 standard deviations above the mean of the sample. 0.5 standard deviations is considered a moderate effect size [27]. As a secondary exploratory analysis, the percentage of participants reporting low scores (1 or 2 on the Likert scale ranging from 1 to 5), in the work and employment and romantic relationships domains were assessed to further delineate differences in these domains. We chose these two domains because we found that adults burned as children did better and their scores were statistically different from those of adults burned later in life in our initial exploratory analysis.
3. Results
3.1. Study population characteristics
Of the 601 participants, four were missing data for age of injury and were excluded from further analyses. Of the participants included in the analysis, 317, 595, and 418 completed the work and employment, romantic relationships, and sexual relationships domains, respectively. Of the co-variates, there was <2% data missing with the exception of TBSA burned in which 6.5% were missing data. Complete demographic and clinical characteristics of the study population are shown in Tables 1 and 2. The final study sample of 597 individuals had a mean age at injury (± standard deviation) of 7.8±5.8years in the <18years group and 37.6±14.3 in the group ≥18years of age. Those burned as children responded to items from the development of the LIBRE profile with an average of 30.9±17.6years after their injury, while those burned as adults completed the survey an average of 9.4±10.8years after injury. Demographic data for time since burn injury was grouped into less than 3years after injury, 3–10years after injury, and greater than 10years after injury. There was no minimum time since injury. There was no statistically significant difference between the adult and pediatric populations for time since burn injury. About one-third of women in the study had been burned as children, compared to about one-fifth of men. More than three-fourths of participants in both groups reported white ethnicity. Those burned as children had slightly larger burns on average [mean TBSA burned (standard deviation) =46.6% (SD 25.1) vs 38.1% (SD 22.6)]. A significantly larger portion of individuals burned as children were working at the time of the study interview compared to those who were burned as adults (64.2% vs 49.3%). There were no statistically significant differences in race/ethnicity, education level, marital status, or burns to critical areas between the individuals burned as children and those burned as adults.
Table 1 –
Age at burn injury, age at study interview and time since burn injury for participants sustaining burn injuries as children vs as adults.
| Age at burn injury | Mean (std. dev.) |
||
|---|---|---|---|
| Age at burn injury | Age at study interview | Time since burn injury | |
| <18years | 7.8 (5.8) | 38.6 (16.0) | 30.9 (17.6) |
| ≥18years | 37.6 (14.3) | 46.9 (15.3) | 9.4 (10.8) |
| p-value | <0.01 | <0.01 | <0.01 |
Table 2 –
Demographic and clinical characteristics of study participants.
| Variable | All participants | Age at burn injury |
||
|---|---|---|---|---|
| <18years | ≥18years | |||
| All participants, N (%) | 597 (100) | 165 (27.6) | 432 (72.4) | |
| Age at time of survey, N (%)* | ≤30 | 155 (26) | 72 (43.6) | 83 (19.2) |
| 31–50 | 206 (34.5) | 50 (30.3) | 156 (36.1) | |
| 51–65 | 180 (30.2) | 34 (20.6) | 146 (33.8) | |
| >65 | 55 (9.2) | 9 (5.5) | 46 (10.6) | |
| Gender, N (%)* | Female | 327 (54.8) | 108 (65.5) | 219 (50.7) |
| Male | 269 (45.1) | 57 (34.4) | 212 (49.1) | |
| Race/ethnicity, N (%) | White non-Hispanic | 465 (77.9) | 138 (83.6) | 327 (75.7) |
| Black or African-American | 55 (9.2) | 11 (6.7) | 44 (10.2) | |
| Hispanic/Latino | 40 (6.7) | 6 (3.6) | 34 (7.9) | |
| Othera | 32 (5.4) | 7 (4.2) | 25 (5.8) | |
| Education level, N (%) | High school or less | 246 (41.2) | 68 (41.2) | 178 (41.2) |
| Marital status, N (%) | Married/live with significant other | 270 (45.2) | 76 (46.1) | 194 (44.9) |
| Current work status, N (%)* | Working | 319 (53.4) | 106 (64.2) | 213 (49.3) |
| Not working | 191 (32) | 36 (21.8) | 155 (35.9) | |
| Otherb | 83 (13.9) | 21 (12.7) | 62 (14.4) | |
| TBSA burned, N (%)* | 0–20 | 142 (23.8) | 33 (20.0) | 109 (25.2) |
| 21–40 | 184 (30.8) | 41 (24.8) | 143 (33.1) | |
| 41–60 | 115 (19.3) | 26 (15.8) | 89 (20.6) | |
| 61–80 | 85 (14.2) | 40 (24.2) | 45 (10.4) | |
| 81–100 | 32 (5.4) | 11 (6.7) | 21 (4.9) | |
| Burns to critical areas, N (%) | 484 (81.1) | 128 (77.6) | 356 (82.4) | |
| Time since burn injury, N (%)* | <3years | 156 (26.1) | 2 (1.2) | 154 (35.6) |
| 3–10years | 165 (27.6) | 22 (13.3) | 143 (33.1) | |
| >10years | 276 (46.2) | 141 (85.5) | 135 (31.3) | |
Characteristics differing significantly between the groups (p<0.01) are denoted with an asterisk (*).
Includes Asian (N=8), American Indian or Alaskan Native (4), Native Hawaiian or Pacific Islander (2), Multiracial (15), and other reported race/ethnicity (3).
Includes homemaker/caregiver, volunteer, retired, and unknown.
3.2. Scale scores
Using GAM, the analysis of deviance test indicates that for social activity and work employment scales, the model fit would significantly improve if we included the smooth function for age at burn (social activity scale: Chi-square (df), p=39.8 (15.6), 0.0007; work and employment scale: Chi-square (df), p=23.1 (10.8), 0.02; romantic relationships scale: Chi-square (df), p=26.8(14.4), 0.02; for all the other scales, the smooth function did not improve the model fit (p>0.05). But since the sample size in work and employment scale was small (N=320) and the 95% confidence band of the smooth function of the age variable includes 0 for most of the age ranges, we decided to use the linear model for the work and employment scale. For the romantic relationships scale, because the sample size was small (N=378), and p values of the squared and cubed age variables in curvilinear model were greater than 0.05, we decided to use the linear model as well. Based on the GAM results, using a smoothing model (analysis of deviance approach), a linear model was selected for five scales (Social Interaction, Work and employment, Romantic Relationships, Sexual relationships, and Family and friends) and a nonlinear (curvilinear) model was selected for one scale (Social activities) (Appendix Fig. A1) [29]. In the linear analysis, when comparing mean scale scores between the two groups, individuals burned as children reported similar or higher scores compared to those burned as adults, with statistically significant differences for two of the scales, work and employment and romantic relationships (Table 3). Adjusted linear regression analyses showed that those burned as children fared slightly better than those burned as adults on two scales: work and employment (B=2.62, p=0.04) and romantic relationships (B=2.51, p=0.05) (Table 4). Burns to critical areas in the multivariate regression models were not adjusted for, because it did not differ significantly by the initial analysis of dichotomized age at burn injury. Burns to individual critical areas (hands, feet, face, genitals) also did not differ significantly by dichotomized age at burn injury. In separate sensitivity analyses for the regression models with adjustment for burns to critical areas, results were not changed from the principal findings. In the curvilinear analysis (Social Activities scale), the relationship between age at burn and the social activity score was plotted for participants in the reference groups indicated at 7.3years since burn (0.5 standard deviation below the mean of the sample), 15.4years since burn (the mean of the sample), and 23.4years since burn (0.5 standard deviation above the mean of the sample) (Appendix Fig. A1). For the Social activities scale, at 7.3years since the burn injury, individuals burned from ages 20 to 65 had scores significantly below the mean while the scores of both children and older adults were not significantly different from the mean. At 15.4years since burn, ages 30–55 had scores significantly below the mean, while the scores of both children and older adults were not significantly different from the mean. At 23.4years since burn, participants across all ages had scores that did not significantly differ from the mean. It appears that among those closer to the time of injury, individuals burned in middle age fared worse than those burned either in childhood or old age, but later on individuals burned at any age fared about the same. For demographic groups other than the one we presented in the figure, the plot would be the same shape but shifted up or down in the y-axis. The results for a different gender or TBSA burned would display similar patterns for the relationship among age at burn injury and time since burn but the mean score would be different. For example, if we display the figure for females instead of males, the curves will stay the same shape but shift down the y axis (Social Activities score) by 1.58 points.
Table 3 –
Mean scale scores for participants sustaining burn injuries as children vs as adults.
Scale scores were standardized to a mean of 50 and standard deviation of 10 based upon the entire burn sample of 601 participants used for the calibration phase of the LIBRE Profile. The scale used for each LIBRE item is the Likert scale ranging from 1 to 5.
| Age at burn injury | Sexual relationships | Family & friends | Social interactions | Social activities | Work & employment | Romantic relationships |
|---|---|---|---|---|---|---|
| <18years | 50.8 (12.2) | 52.1 (10.65) | 47.8 (9.59) | 55.6 (9.83) | 52.2 (8.63) | 50.3 (10.86) |
| ≥18years | 48.9 (10.9) | 50.4 (10.33) | 47.1 (10.03) | 51 (10.29) | 48.0 (9.53) | 47.2 (12.02) |
| p-value | 0.14 | 0.07 | 0.48 | <0.01 | <0.01 | <0.01 |
Values presented are mean (standard deviation).
Table 4 –
Adjusted linear regression analyses of associations between age at injury and scale scores.
| Domain | Crude results |
Adjusted results |
||||
|---|---|---|---|---|---|---|
| B | 95% CI | p-value | B | 95% CI | p-value | |
| Sexual relationships | 1.83 | −0.59, 4.25 | 0.14 | 1.58 | −1.24, 4.40 | 0.27 |
| Family & friends | 1.75 | −0.12, 3.63 | 0.07 | 0.67 | −1.49, 2.82 | 0.54 |
| Social interactions | 0.65 | −1.13, 2.43 | 0.48 | −0.58 | −2.57, 1.41 | 0.57 |
| Work & employment | 4.26 | 2.09, 6.43 | <0.01 | 2.62 | 0.14, 5.09 | 0.04 |
| Romanic relationships | 3.09 | 0.98, 5.19 | <0.01 | 2.51 | 0.04, 4.99 | 0.05 |
Regression coefficients refer to difference in scale scores (standard deviation=10) between participants aged <18 at burn injury and those aged ≥18years at burn injury. Adjusted models include gender, marital status, work status, TBSA burned and time since burn injury.
When looking at individual response items in the secondary analysis, the percentage of participants reporting low scores (1–2 out of 5) was higher in the group burned as adults for these two scales (Table 5). Those burned as adults were more likely to report being limited in what they can provide for their family and limited in their abilities at work than their counterparts who were burned as children.
Table 5 –
Percentage of participants reporting low score (1 or 2 on the scale 1–5), by age at burn injury, items in work & employment scale, romantic relationships scale.
| Item work & employment scale | <18 at burn injury | ≥18 at burn injury | Difference |
|---|---|---|---|
| Q43 At my job, I can do everything for work that I want | 1.9 | 17.5 | 15.5 |
| Q426 I get tired too quickly at my job | 5.8 | 16.9 | 11.1 |
| Q416 I have enough energy to complete my work | 3.8 | 13.3 | 9.5 |
| Q44 I am satisfied with how much I can do at my job | 1.9 | 10.9 | 9.0 |
| Q417 Compared to others, I am limited in the amount of work I can do | 11.5 | 19.1 | 7.6 |
| Q45 I am satisfied with my work | 5.7 | 11.8 | 6.1 |
| Q427 I get unwanted attention from my coworkers | 13.7 | 19.6 | 5.9 |
| Q423 I am afraid of losing my job because of my burns | 3.9 | 8.5 | 4.6 |
| Q420 My emotions make it difficult for me to go to work | 10.5 | 14.8 | 4.4 |
| Q415 Because of my burns, I am unable to finish many work tasks | 1.0 | 4.8 | 3.8 |
| Q418 Compared to others, I miss work more often due to health problems related to my burns | 8.7 | 12.6 | 3.8 |
| Q46 I can keep up with my work responsibilities | 2.9 | 6.2 | 3.3 |
| Q419 I am afraid to go to my job | 1.0 | 3.9 | 2.9 |
| Q421 My burns have stopped me from learning new things on the job | 4.8 | 7.7 | 2.9 |
| Q49 I feel that I am disappointing other people at my job | 6.8 | 8.8 | 2.0 |
| Q412 I work well with coworkers | 1.0 | 1.5 | 0.5 |
| Q422 I cannot find a better job because of my burns | 7.7 | 7.7 | 0.0 |
| Q48 Because of how my burns make me look, I find it difficult to complete my work | 2.9 | 2.4 | −0.5 |
| Q410 My boss feels I can do my work | 3.9 | 2.1 | −1.8 |
| Item romantic relationships scale | <18 at burn injury | ≥18 at burn injury | Difference |
|
| |||
| Q725 My relationship with my partner got stronger since my burn injury | 0.0 | 11.8 | 11.8 |
| Q712 My relationship with my partner has gotten worse since my burn | 0.0 | 11.7 | 11.7 |
| Q729 I think that my partner is uncomfortable seeing my burns | 4.1 | 11.6 | 7.6 |
| Q79 I am comfortable talking openly with my partner | 3.0 | 10.1 | 7.1 |
| Q733 My partner does not want sex when I do | 10.3 | 17.2 | 6.9 |
| Q720 My partner makes me feel needed | 2.0 | 8.7 | 6.7 |
| Q74 I am comfortable discussing significant problems with my partner | 5.0 | 11.6 | 6.6 |
| Q713 My partner gets on my nerves all of the time | 4.0 | 10.5 | 6.5 |
| Q721 Things between my partner and me are going well | 3.0 | 8.7 | 5.7 |
| Q76 I trust my partner with my deepest thoughts and feelings | 5.0 | 10.5 | 5.5 |
| Q711 I am worried that my partner will leave me | 11.1 | 16.3 | 5.2 |
| Q719 My partner is very loving to me | 2.0 | 7.2 | 5.2 |
| Q726 I feel that my partner accepts how I look | 0.0 | 4.4 | 4.4 |
| Q1018 I enjoy going out with friends | 2.5 | 6.3 | 3.8 |
| Q107 I talk openly with friends | 4.9 | 7.7 | 2.8 |
| Q714 I have a partner who meets many of my emotional needs | 6.1 | 8.7 | 2.6 |
| Q731 I find it difficult to tell my partner that I love him or her | 7.0 | 9.6 | 2.6 |
| Q722 It is easy to tell my partner that I care about him or her | 2.0 | 4.3 | 2.3 |
| Q78 I feel comfortable sharing fears about my burns with my partner | 7.4 | 9.8 | 2.3 |
| Q710 I find it difficult listening to my partner’s personal problems | 8.1 | 10.2 | 2.1 |
| Q72 How often do you and your partner do things together? | 1.0 | 2.9 | 1.9 |
| Q819 There is no one that I hug, hold, or kiss | 3.6 | 4.9 | 1.3 |
| Q718 My partner is fun to be with | 1.0 | 2.2 | 1.2 |
| Q716 My partner makes me happy | 3.0 | 3.6 | 0.6 |
| Q724 I shy away from being close to my partner | 11.1 | 11.6 | 0.5 |
| Q71 My partner is gentle with me | 2.0 | 1.9 | −0.1 |
| Q717 My partner is a good companion | 2.0 | 1.1 | −0.9 |
| Q77 I am afraid to share with my partner what I dislike about myself | 29.0 | 28.0 | −1.0 |
4. Discussion
This is the first study directly comparing social participation between burn survivors injured as children and those injured as adults. While there have been previous studies examining mental and physical health sequelae in pediatric burn survivors, no prior studies specifically compared social participation between individuals burned as children and those burned as adult [26]. Compared with individuals burned as adults, those injured in childhood did as well or better reintegrating into the community at long term follow up. In addition, for social activities, individuals burned as children as well as those burned as older adults scored no different than the mean at 7.3years and 15.4 after the burn injury, while those burned in midlife scored below the mean at these time points. For all ages, they scored no different than the mean at 23.4years since burn. Though the study is limited by its cross sectional nature, it may indicate that individuals burned as children or older adults “bounce back” more quickly in social activities than those burned in midlife.
Resilience (return to the same ability as prior injury), posttraumatic growth (achieving higher ability than that prior to injury) and response shift (adjusting perspective such that expectations correspond to ability following injury) are possible mediators of social recovery following burns or other injuries and conditions [30–33]. Resilience was defined in an early important article in 1998 by Holaday and McPherson as a process rather than an outcome under which a burn survivor can adapt to adversity and face challenges on a daily basis not being able to achieve a life they had prior to the burn [34]. Resilience is a continuing process that becomes part of the burn survivor’s life. In addition, the key elements that influence resilience conceptually include: (1) social support systems such as family, community and a key friend; (2) cognitive skills such as intelligence, coping style and self-efficacy, and (3) psychological resources that protect the individual from stress such as “internal locus of control” where the perception of the burn survivor is that external events do not control you. Other elements include, empathy and curiosity and the desire to seek new experiences. In a recent article based upon a comprehensive literature review by Martin et al. in 2016 post traumatic growth was described as a separate construct from resilience where the two may not always be in parallel with each other [35]. The area is a complex one and should be understood in terms of the dynamics of the individual.
Future research can explore whether the mechanisms for social recovery are different for those burned at different ages. For example, previous studies have shown mixed results as to whether and how resilience and post-traumatic growth vary by age at burn [36–38]. Individuals burned as children did particularly well in social participation regarding work and employment and romantic relationships. Interestingly, those burned as adults reported lower scores on most of the individual questionnaire items within the work and employment and romantic relationships scales. In addition, fewer of those burned as adults were working at the time of the study. We postulate that our findings suggest a resilience factor in children that might relate to the process of social participation following a burn injury. Another possible explanation is that individuals burned early in life are directed to more accommodating or accessible activities and careers, while those burned later in life may not be able to make such adjustments.
Advances in burn care have led to improved survival rates and to a research focus on quality of life in the burn population [39]. An important component of quality of life is social participation, which is influenced by resilience. Three prior studies assessing resilience in childhood cancer survivors determined that resilience is fostered by relationships with parents, psychospiritual growth and coping with uncertainties of the illness [40–42]. In a systematic review of resilience in the physically ill, several psychological factors were identified as predictive of resilience, including self-efficacy, self-esteem, internal locus of control, optimism and mastery. Social support was also found to correlate with resilience [43]. We postulate that resilience of children may also be influenced by insurance coverage, psychosocial family-centered care and nonprofit institutions supporting their recovery. Being aware and identifying areas of social participation where individuals with burn injuries struggle will help clinicians to identify appropriate psychosocial interventions. Patient-reported outcome measures can be used at the individual level to screen for areas of difficulty and guide discussion during clinical visits, as demonstrated by previous research using the Young Adult Burn Outcomes Questionnaire [44]. Psychological factors predictive of resilience can be used to guide these interventions, targeted at specific areas of reintegration and even individual response items. Data showing resilience in children faced with various types of physical trauma or illnesses can help to reassure parents regarding their child’s recovery from a burn injury. Parents and caregivers may facilitate resilience in traumatized children by providing adequate caregiver support [14].
In contrast to the above mentioned literature, some studies assessing mental health and lifetime physical health disorders in individuals burned as children reported worse outcomes in this population compared to the general U.S. population. One study compared adults burned as children to the general U.S. population and found an increased rate of axis I mental disorders in the burn population [45]. Another study found an elevated suicide rate in a population of childhood burn survivors [46]. It is recognized in the burn literature that individuals are at increased risk of mental and physical disorders. One study conducted by Stone et al. [47] found increased rates of substance abuse, anxiety and major depressive disorders in individuals burned as children compared to matched controls. Based on the current literature, it is unknown how age at injury affects social outcomes in the burn population, but Quezada et al. [14] suggests younger age at injury is a positive predictor of resilience. By specifically comparing community integration outcomes among individuals burned as children vs as adults, our study begins to address this gap in the literature. Future studies similar to this may provide novel information to clinicians and parents of childhood burn survivors.
Another consideration of child resilience and social participation outcomes is the developmental stage in which the burn injury was sustained. Erik Erikson, a developmental psychologist and psychoanalyst, described eight stages of psychosocial development in life and their role in the development of various personality traits [48]. One would anticipate that burn injuries sustained during the adolescent stage, when an individual is formulating a sense of self and place in the community, could be particularly detrimental to personal identity and social participation. To date, few studies have assessed the psychosocial impact of burn injury in relation to developmental stages. One recent study found an association between higher resilience and younger age of burn injury [14]. Developmental stage may impact the understanding of the burn injury, which can contribute to emotional response and adjustment. Future work can begin to address how developmental stage relates to recovery in those with burn injuries with some focus on social activities.
4.1. Strengths and limitations
While our study has several strengths, including a large overall sample size and level of participation, several limitations merit attention. One limitation of this study is its cross-sectional design, which does not capture the variability in social participation after burn injury over time had this been a cohort study. Cause and effect relationships also are not possible given this design. Another possible limitation is sample selection bias. Burn survivors included in the convenience sample may have higher levels of social participation than the general burn survivor population; for example, those recruited through advocacy groups and clinics may have more established social support. Recall bias may also be present, given all participants completed the survey as an adult. In addition, we did not stratify individuals burned as children into specific age groups at time of injury to determine if specific psychosocial developmental stages influence their social participation, due to limited sample sizes. Another limitation of this study was the inability to assess the impact of trauma and support variables provided to children during their recovery process. It is possible they are doing well secondary to integrating their burn injuries into their sense of self and/or due to psychological support and teaching of coping techniques. The level of support received in the acute recovery period was also not measured on the survey. In addition, this study did not measure the opportunities for interventions over time to the individuals burned as children. We suspect interventions would influence this group positively and improve their social participation scores, leading them to be on par with the adult group. In spite of these limitations, this is the first study to compare social participation of individuals burned as children with those burned as adults.
We realize our study does not address children with burn injuries compared to children without burn injury. The LIBRE profile items were specifically designed for the burn population and are not applicable to controls without burn injury. This is a unique tool with particular questions for the burn population.
5. Conclusions
In our study, we found individuals burned as children as a whole to perform at least as well as those burned as adults on the LIBRE profile scales. These results are encouraging for health care providers and families of individuals burned as children, but also highlight areas that could be targeted for intervention to further improve social participation. Future work, comparing different developmental stages at time of injury may reveal stages of development where children are particularly vulnerable. These results are encouraging and highlight the resilience of children in the face of hardships and significant trauma.
Acknowledgment
The authors would like to acknowledge the contributions of the LIBRE Advisory Board to this study.
Funding source
The contents of this manuscript were developed under grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR), [grant numbers 90DP0055,90DP0035, and 90DPBU0001]. NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this manuscript do not necessarily represent the policy of NIDILRR, ACL, HHS, and you should not assume endorsement by the Federal Government. The funder had no involvement in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Declaration of interests
Drs. Kazis and Ryan report fees from Avita Medical outside the submitted work. Dr. Ryan reports a grant paid to the institution from Shriners Hospitals for Children outside the submitted work. No other interests to declare. All authors have approved the final article.
Appendix A. Curvilinear analysis of social activities scale
Fig. A1 –
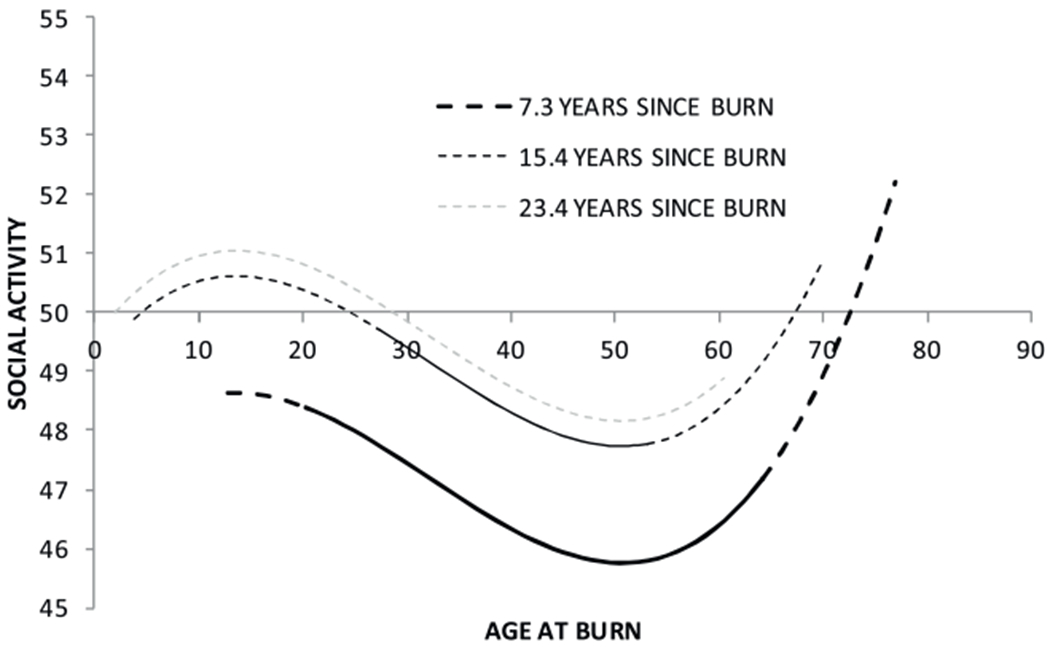
The relationship between the social activities score and the age at burn for the subjects at 7.3, 15.4, and 23.4years time since burn (The figure displays the relationship for these reference groups: gender male, marital status single, TBSA burned > 80%, work status other (includes homemaker/caregiver, volunteer, retired, and unknown.) The solid curves are the age range where the social activity scores are statistically significantly different from the mean of the scores in the sample (50), the dash curves are the age range where the social activities scores are not statistically significantly different from the mean of the sample.
REFERENCES
- [1].American Burn Association. Burn incidence and treatment in the US: 2016 fact sheet. 2016. https://ameriburn.org/who-we-are/media/burn-incidence-fact-sheet/. [Accessed 16 January 2017].
- [2].Brigham PA, McLoughlin E. Burn incidence and medical care use in the United States: estimates, trends, and data sources. J Burn Care Rehabil 1996;17(2):95–107. [DOI] [PubMed] [Google Scholar]
- [3].National burn repository 2017 report. 2017. http://ameriburn.org/wp-content/uploads/2018/04/2017_aba_nbr_annual_report_summary.pdf. [Accessed 1 October 2018].
- [4].Hirsh AT, Braden AL, Craggs JG, Jensen MP. Psychometric properties of the community integration questionnaire in a heterogeneous sample of adults with physical disability. Arch Phys Med Rehabil 2011;92(10):1602–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Schneider J, Spires M. Burn rehabilitation. DeLisa’s physical medicine and rehabilitation: principles and practice, two volume set. Philadelphia, PA: Lippincott Willaims & Wilkins; 2010. p. 1125–50. [Google Scholar]
- [6].Wolf SE, Rose JK, Desai MH, Mileski JP, Barrow RE, Herndon DN. Mortality determinants in massive pediatric burns: an analysis of 103 children with > or=80% TBSA burns (> or= 70% full-thickness). Ann Surg 1997;225(5):554–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Baker CP, Russell WJ, Meyer W, Blakeney P. Physical and psychologic rehabilitation outcomes for young adults burned as children. Arch Phys Med Rehabil 2007;88(12):S57–64. [DOI] [PubMed] [Google Scholar]
- [8].Blakeney P, Meyer W, Moore P, Murphy L, Broemeling L, Robson M, et al. Psychosocial sequelae of pediatric burns involving 80% or greater total body surface area. J Burn Care Rehabil 1993;14(6):684–9. [DOI] [PubMed] [Google Scholar]
- [9].Sheridan RL, Hinson MI, Liang MH, Nackel AF, Schoenfeld DA, Ryan CM, et al. Long-term outcome of children surviving massive burns. JAMA 2000;283(1):69–73. [DOI] [PubMed] [Google Scholar]
- [10].Rosenberg M, Blakeney P, Robert R, Thomas C, Holzer C, Meyer W. Quality of life of young adults who survived pediatric burns. J Burn Care Res 2006;27(6):773–8. [DOI] [PubMed] [Google Scholar]
- [11].Sheridan RL, Weber JM, Schnitzer JJ, Schulz JT, Ryan CM, Tompkins RG. Young age is not a predictor of mortality in burns. Pediatr Crit Care Med 2001;2(3):223–4. [DOI] [PubMed] [Google Scholar]
- [12].Kazak AE, Kassam-Adams N, Schneider S, Zelikovsky N, Alderfer MA, Rourke M. An integrative model of pediatric medical traumatic stress. J Pediatr Psychol 2006;31(4):343–55. [DOI] [PubMed] [Google Scholar]
- [13].Svetina M Resilience in the context of Erikson’s theory of human development. Curr Psychol 2014;33(3):393–404. [Google Scholar]
- [14].Quezada L, González MT, Mecott GA. Explanatory model of resilience in pediatric burn survivors. J Burn Care Res 2016;37(4):216–25. [DOI] [PubMed] [Google Scholar]
- [15].Masten AS, Cutuli J, Herbers J, Reed M. Resilience in development – Oxford handbooks. New York: Oxford University Press; 2002. [Google Scholar]
- [16].Byrne C, Love B, Browne G, Brown B, Roberts J, Streiner D. The social competence of children following burn injury: a study of resilience. J Burn Care Rehabil 1986;7(3):247–52. [DOI] [PubMed] [Google Scholar]
- [17].Holaday M, McPhearson RW. Resilience and severe burns. J Couns Dev 1997;75(5):346–56. [Google Scholar]
- [18].Lau U, Van Niekerk A. Restorying the self: an exploration of young burn survivors’ narratives of resilience. Qual Health Res 2011;21(9):1165–81. [DOI] [PubMed] [Google Scholar]
- [19].Powers SE. Risk versus resilience: an exploratory study of factors influencing the development of posttraumatic stress symptoms in pediatric burn patients. 2011. https://ir.uiowa.edu/etd/2759.
- [20].van Baar ME, Polinder S, Essink-Bot ML, van Loey NE, Oen IM, Dokter J, et al. Quality of life after burns in childhood (5-15 years): children experience substantial problems. Burns 2011;37(6):930–8. [DOI] [PubMed] [Google Scholar]
- [21].Pochon JP, Bayer B, Irniger N, Lusser R, Pfenninger I, Sauer I. Early rehabilitation and psychosocial problems of burns in childhood. Z Kinderchir 1983;38:12–5. [DOI] [PubMed] [Google Scholar]
- [22].Gerrard P, Kazis LE, Ryan CM, Shie L, Holavanahalli R, Lee A, et al. Validation of the Community Integration Questionnaire in the adult burn injury population. Qual Life Res 2015;24(11):2651–5. [DOI] [PubMed] [Google Scholar]
- [23].Marino M, Soley-Bori M, Jette AM, Slavin MD, Ryan CM, Schneider JC, et al. Development of a conceptual framework to measure the social impact of burns. J Burn Care Res 2016;37(6):e569–78. [DOI] [PubMed] [Google Scholar]
- [24].Kazis LE, Marino M, Ni P, Soley-Bori M, Amaya F, Dore E, et al. Development of the life impact burn recovery evaluation (LIBRE) profile: assessing burn survivors’ social participation. Qual Life Res 2017;26(10):2851–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Marino M, Soley-Bori M, Jette AM, Slavin MD, Ryan CM, Schneider JC, et al. Measuring the social impact of burns on survivors. J Burn Care Res 2017;38(1):e377–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Marino ME, Dore EC, Ni P, Ryan CM, Schneider JC, Acton A, et al. Developing item response theory-based short forms to measure the social impact of burn injuries. Arch Phys Med Rehabil 2018;99(3):521–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Perry RJ, Moore CA, Morgan BD, Plummer DL. Determining the approximate area of a burn: an inconsistency investigated and reevaluated. BMJ 1996;312(7042):1338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Knayst GA, Crickelair GF, Cosman B. The rule of nines: its history and accuracy. Plast Reconstr Surg 1968;41(6):360–3. [PubMed] [Google Scholar]
- [29].Cohen J Statistical power analysis for the behavioral sciences. New York: Academic Press; 1977. [Google Scholar]
- [30].He F, Cao R, Feng Z, Guan H, Peng J. The impacts of dispositional optimism and psychological resilience on the subjective well-being of burn patients: a structural equation modelling analysis. PLoS One 2013;8(12):e82939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Attoe C, Pounds-Cornish E. Psychosocial adjustment following burns: an integrative literature review. Burns 2015;41(7):1375–84. [DOI] [PubMed] [Google Scholar]
- [32].Rose AJ, Sacks NC, Deshpande AP, Griffin SY, Cabral HJ, Kazis LE. Single-change items did not measure change in quality of life. J Clin Epidemiol 2008;61(6):603–8. [DOI] [PubMed] [Google Scholar]
- [33].Rapkin BD, Schwartz CE. Toward a theoretical model of quality-of-life appraisal: implications of findings from studies of response shift. Health Qual Life Outcomes 2004;2:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Holaday M, McPhearson RW. Resilience and severe burns. J Couns Dev 1997;75:346–56. [Google Scholar]
- [35].Martin LM, Byrnes M, McGarry S, Rea S, Wood F. Posttraumatic growth after burn in adults: an integrative literature review. Burns 2016;43(3):459–70. [DOI] [PubMed] [Google Scholar]
- [36].Rosenbach C, Renneberg B. Positive change after severe burn injuries. J Burn Care Res 2008;29(4):638–43. [DOI] [PubMed] [Google Scholar]
- [37].Yang Z, Wang J, Zhang B, Zeng Y, Ma H. Factors influencing resilience in patients with burns during rehabilitation period. Int J Nurs Sci 2014;1(1):97–101. [Google Scholar]
- [38].Kornhaber R, Bridgman H, McLean L, Vandervord J. The role of resilience in the recovery of the burn-injured patient: an integrative review. Chronic Wound Care Manage Res 2016 2016: 3 Pages 41–50 https://www.dovepress.com/the-role-of-resilience-in-the-recovery-of-the-burn-injured-patient-an-peer-reviewed-article-CWCMR. [Accessed 15 May 2018]. [Google Scholar]
- [39].Van Loey NEE, Van Son MJM. Psychopathology and psychological problems in patients with burn scars: epidemiology and management. Am J Clin Dermatol 2003;4(4):245–72. [DOI] [PubMed] [Google Scholar]
- [40].Orbuch TL, Parry C, Chesler M, Fritz J, Repetto P. Parent-Child relationships and quality of life: resilience among childhood cancer survivors. Fam Relat 2005;54(2):171–83. [Google Scholar]
- [41].Parry C, Chesler MA. Thematic evidence of psychosocial thriving in childhood cancer survivors. Qual Health Res 2005;15(8):1055–73. [DOI] [PubMed] [Google Scholar]
- [42].Parry C Embracing uncertainty: an exploration of the experiences of childhood cancer survivors. Qual Health Res 2003;13(2):227–46. [DOI] [PubMed] [Google Scholar]
- [43].Stewart DE, Yuen T. A systematic review of resilience in the physically ill. Psychosomatics 2011;52(3):199–209. [DOI] [PubMed] [Google Scholar]
- [44].Ryan CM, Lee AF, Kazis LE, Shapiro GD, Schneider JC, Goverman J, et al. Is real-time feedback of burn-specific patient-reported outcome measures in clinical settings practical and useful? A pilot study implementing the young adult burn outcome questionnaire. J Burn Care Res 2016;37(1):64–74. [DOI] [PubMed] [Google Scholar]
- [45].Meyer WJ, Blakeney P, Thomas CR, Russell W, Robert RS, Holzer CE. Prevalence of major psychiatric illness in young adults who were burned as children. Psychosom Med 2007;69(4):377–82. [DOI] [PubMed] [Google Scholar]
- [46].Goodhew F, Van Hoof M, Sparnon A, Roberts R, Baur J, Saccone EJ, et al. Psychiatric outcomes amongst adult survivors of childhood burns. Burns 2014;40(6):1079–88. [DOI] [PubMed] [Google Scholar]
- [47].Stone J, Gawaziuk JP, Khan S, Chateau D, Bolton JM, Sareen J, et al. Outcomes in Adult Survivors of Childhood Burn Injuries as Compared with Matched Controls. J Burn Care Res 2016;37(2):e166–73. [DOI] [PubMed] [Google Scholar]
- [48].Kivnick HQ, Wells CK. Untapped richness in Erik H. Erikson’s rootstock. Gerontologist 2014;54(1):40–50. [DOI] [PubMed] [Google Scholar]