

Abstract
Employment problems are common among people with substance use disorders (SUDs), and improving vocational functioning is an important aspect of SUD treatment. More detailed understanding of the psychosocial benefits of employment may help refine vocational interventions for people with SUDs. Here, we used ecological momentary assessment to measure possible affective improvements associated with work. Participants (n = 161) with opioid use disorder were randomized to work (job-skills training) in a contingency-management-based Therapeutic Workplace either immediately or after a waitlist delay. Throughout, participants responded via smartphone to randomly scheduled questionnaires. In linear mixed models comparing responses made at work vs. all other locations, being at work was associated with: less stress, less craving for opioids and cocaine, less negative mood, more positive mood, and more flow-like states. Some of these differences were also observed on workdays vs. non-workdays outside of work hours. These results indicate that benefits associated with work may not be restricted to being actually in the workplace; however, randomization did not reveal clear changes coinciding with the onset of work access. Overall, in contrast to work-associated negative moods measured by experience-sampling in the general population, Therapeutic Workplace participants experienced several types of affective improvements associated with work.
Introduction
People with opioid use disorder (OUD) and other substance use disorders (SUDs) often have employment problems (Bauld et al. 2012; Bell & Strang 2020), including high rates of unemployment (~65% or more unemployed largely independent of macroeconomic conditions, reviewed by Magura & Marshall 2020; Magura et al. 2004; Platt 1995; see also Bauld et al. 2012; Henkel 2011; Nagelhout et al. 2017). Unemployment has been associated with greater consumption of both licit and illicit drugs in the general population (Henkel 2011; Huang et al. 2011; Mulia et al. 2014), and for people with OUD, unemployment can trigger relapse/resumption of drug use (Platt 1995). Conversely, engaging with employment activities (broadly including job-searching and/or -training, as well as actual employment) has been associated with improved quality of life for people with OUD (De Maeyer et al. 2011; see also Petry et al. 2014). Having fewer employment problems has also been associated with better adherence to medication for opioid use disorder (MOUD) (reviewed by Brewer et al. 1998; Platt 1995; see also Kidorf et al. 1998, 2004; Proctor et al. 2015). Therefore, improving patients’ vocational functioning is an important aspect of OUD treatment, both for patients themselves and policymakers (Bauld et al. 2012; De Maeyer et al. 2011; Henkel 2011; Magura et al. 2004; Monaghan & Wincup 2013; Platt 1995).
Despite this general emphasis on employment, the psychosocial mechanisms by which people with SUDs may benefit from employment have been relatively unexplored (e.g., Henkel 2011; see also Nagelhout et al. 2017). Clarifying these mechanisms is important for understanding specifically who benefits from employment and how those benefits can be maximized without potentially harming vulnerable populations with broad, vague, or inflexible advocacy of work (cf., Monaghan & Wincup 2013). Several different mechanisms for beneficial effects of employment have been proposed (reviewed by Henkel 2011; Monaghan & Wincup 2013; Nagelhout et al. 2017; Platt 1995): social network changes (e.g., including more people who do not use drugs) or reductions in social exclusion/isolation; improvements in self-esteem; reductions in “free” time in which drugs can be used; and changes in material conditions (i.e., regular income) that could facilitate meeting specific program requirements (e.g., reduced absenteeism from improved transportation) or reduce stress (cf., Panlilio et al. 2019 on stress and treatment dropout). Work may also be an important element of people’s “stake in conventional life,” whereby they feel vested in and hopeful about their everyday roles and obligations (Waldorf et al. 1991): employment can help people with OUD reduce criminal behavior and re-center their sense of identity on normative/adaptive activities (Bell & Strang 2020; Monaghan & Wincup 2013; Platt 1995). Although plausible, it is important to note that, in many cases, those proposed mechanisms reflect (or are only slightly adapted from) prevailing societal beliefs about the value of and benefits from work. Work is seen as the proper, salutary duty of all members of society, and people with SUDs should not be exempted or excluded (e.g., Monaghan & Wincup 2013). Certainly, people with SUDs should not be excluded from potentially beneficial activities; however, it is important to determine directly how the experience of work and benefits from work actually apply to people with SUDs.
The potentially complex effects of work, and potential for differences across populations, are highlighted by studies assessing daily life using ecological momentary assessment (EMA) and related experience-sampling methods. In an EMA study of people with heroin and cocaine dependence during MOUD, Epstein and Preston (2012) found that participants employed in jobs in the community reported better moods when they were at work: more happiness and less stress, boredom, irritation, and craving for heroin and cocaine. In contrast, experience-sampling studies in the general population have found, in various ways, less positive mood and/or more negative mood at work vs. elsewhere or during workdays vs. free days (Brandstätter 1994; Csikszentmihalyi & Graef 1980; Killingsworth & Gilbert 2010; Steptoe et al. 2005). Considering substance use more specifically, EMA data from people attempting to quit smoking cigarettes showed that negative affect was higher during work activities vs. leisure activities, and higher during business interactions vs. social interactions (Shiffman & Waters 2004). Thus, it is possible that the experience of work is different for people in OUD treatment compared to other populations, but more research is needed to understand the effects of being at work per se. As they themselves point out, Epstein and Preston (2012) were able to compare at-work and not-at-work conditions only because some participants happened to be employed outside of the study, and the investigators could not control for participants’ self-selection into workplace environments, schedules, and activities.
Therefore, we used EMA to measure the mood and behavior of people with OUD during standardized experimental employment in a contingency-management-based Therapeutic Workplace (for more detailed reviews, see Silverman et al. 2016, 2018; Wong & Silverman 2007). Generally, in the Therapeutic Workplace, participants are paid a stipend (expressed as an hourly wage rate) for computerized job-skills-training activities. Drug abstinence and workplace attendance/productivity are supported by contingency management that reinforces drug-negative urine samples: drug-positive or missing samples produce temporary suspensions of workplace access or wage-rate reductions that are reversed by subsequent negative urinalysis. For people with SUDs, these interventions improve retention and drug abstinence and can be adapted to promote other health behaviors. Here, we used the Therapeutic Workplace to provide all participants with similar, typical work activities in a common location on a shared schedule during EMA. We also were able to study the effects of access to paid work by restricting access in two ways: (1) participants were randomized at the beginning of the study to start their access immediately or after a waitlist delay, and (2) participants were given experimentally determined “random vacation days.” Based on the previous EMA study of community employment (Epstein & Preston 2012) and a study of unstructured time vs. time spent on obligations (Kowalczyk et al. 2017), we hypothesized that participants would report less stress and craving and more positive moods at work vs. elsewhere, and on days when they had access to the Therapeutic Workplace vs. when they did not.
Methods
Setting and participants
This study was conducted at the Johns Hopkins University Center for Learning and Health (CLH) in Baltimore, MD, USA. EMA data collection was administered by the National Institute on Drug Abuse (NIDA) Intramural Research Program (IRP) in Baltimore, MD, USA. All study procedures were approved by the Johns Hopkins Medicine IRB, and all participants provided prior written informed consent. EMA data were collected between November 2015 and July 2018.
All participants were enrolled in a longer study of the effects of abstinence-contingent wage supplementation on community employment, called here the “Workplace Study” (ClinicalTrials.gov NCT02487745; Holtyn et al. 2020, Toegel et al. 2020). EMA data were collected during the Workplace Study’s first ~3 months, in each participant’s initial abstinence-initiation and job-skills-training period. During this time, participants’ experimental work consisted of computer-based skills-training and educational activities (e.g., mathematics and typing courses) in the CLH Therapeutic Workplace, and urine drug screens were conducted thrice weekly (typically Mondays, Wednesdays, and Fridays). This study concluded when the Workplace Study completed its enrollment.
Baseline participant characteristics (Table 1) were collected with the ASI-Lite (Cacciola et al. 2007). Workplace Study inclusion criteria were: age 18 years or older, residence in or near Baltimore City, current unemployment with self-reported interest in gaining employment, current enrollment in or eligibility for methadone or buprenorphine maintenance treatment, and an opioid-positive urine sample. From November 2015 to June 2016, the inclusion criteria also included a cocaine-positive urine sample and self-report and visible evidence (i.e., track marks) of injection drug use; afterward, these criteria were eliminated to improve recruitment, but many participants still also had histories of cocaine use. Workplace Study exclusion criteria were: physical limitations that prevented typing; current suicidal or homicidal ideation; active hallucinations, delusions, or thought disorder; or current imprisonment. Although it was not required for enrollment, most participants were receiving opioid agonist treatment at baseline (for the n = 161 EMA participants described below: n = 149 methadone, n = 8 buprenorphine, n = 4 no treatment); additional treatment details (e.g., medication dose) were not collected.
Table 1.
Characteristics of participants randomized to the Immediate vs. Delayed Work Groups, including all participants who provided any EMA data (n = 161) and the subsample of EMA Completers (n = 88).
| Total EMA | Immediate Work Group | Delayed Work Group | p-valuea | Completers | Immediate Work Group | Delayed Work Group | p-valuea | |
|---|---|---|---|---|---|---|---|---|
| n = 161 | n = 78 (48.4%) | n = 83 (51.6%) | n = 88 | n = 46 (52.3%) | n = 42 (47.7%) | |||
| Age (years) | 48.6 (9.5) | 47.9 (11.0) | 49.3 (7.8) | .687 | 47.9 (8.9) | 47.2 (10.3) | 48.6 (7.3) | .802 |
| Male | 55.9% | 59.0% | 53.0% | .547 | 56.8% | 63.0% | 50.0% | .308 |
| Race/ethnicity | .745 | .690 | ||||||
| African American | 62.1% | 59.0% | 75.1% | 56.8% | 52.2% | 61.9% | ||
| White | 34.2% | 37.2% | 31.3% | 40.9% | 45.7% | 35.7% | ||
| Hispanic/Native American | 3.7% | 3.8% | 3.6% | 2.3% | 2.2% | 2.4% | ||
| Married | 13.0% | 14.1% | 12.0% | .879 | 14.8% | 17.4% | 11.9% | .672 |
| Currently on probation/parole | 11.2% | 10.3% | 12.0% | .912 | 11.4% | 10.9% | 11.9% | 1.000 |
| Lifetime incarceration history | ||||||||
| Any | 82.0% | 85.9% | 78.3% | .295 | 85.2% | 87.0% | 83.3% | .859 |
| Monthsb | 69.0 (91.0) | 62.0 (93.0) | 75.5 (88.2) | .138 | 57.0 (74.5) | 57.4 (83.2) | 56.0 (64.3) | .510 |
| High school diploma/GED | 58.4% | 52.6% | 63.9% | .196 | 63.6% | 56.5% | 71.4% | .219 |
| Technical training, any | 33.5% | 34.6% | 32.5% | .910 | 30.7% | 34.8% | 26.2% | .521 |
| Typical employment pattern, past 3 years | .363 | .730 | ||||||
| Full-time | 14.3% | 12.8% | 15.7% | 21.6% | 19.6% | 23.8% | ||
| Part-time | 12.4% | 14.1% | 10.8% | 9.1% | 6.5% | 11.9% | ||
| Retired/Disabled | 29.2% | 34.6% | 24.1% | 29.5% | 32.6% | 26.2% | ||
| Unemployed | 44.1% | 38.5% | 49.4% | 39.8% | 41.3% | 38.1% | ||
| Years at longest-held full-time job | 6.3 (5.6) | 6.2 (6.1) | 6.4 (5.2) | .350 | 6.6 (5.5) | 6.5 (5.9) | 6.8 (5.0) | .390 |
| Skilled worker (Hollingshead index) | 29.8% | 28.2% | 31.3% | .795 | 39.8% | 34.8% | 45.2% | .434 |
| Paid workdays, past month | 5.0% | 5.1% | 4.8% | 1.000 | 5.7% | 4.3% | 7.1% | .666 |
| Past-month income (USD)c | ||||||||
| Employment income | $5.2 (26.2) | $5.6 (27.4) | $4.8 (25.3) | .680 | $5.2 (24.9) | $3.5 (16.2) | $7.1 (31.9) | .871 |
| Non-employment incomed | $536.8 (374.7) | $563.3 (360.8) | $511.9 (387.9) | .282 | $486.9 (338.2) | $482.5 (332.2) | $491.7 (348.5) | .844 |
| Opioid agonist treatmentd | ||||||||
| Past month, any | 97.5% | 98.7% | 96.4% | .621 | 100.0% | 100.0% | 100.0% | – |
| Past month, days | 27.6 (8.0) | 28.9 (5.8) | 26.5 (9.6) | .059 | 28.6 (6.3) | 29.4 (4.4) | 27.9 (7.8) | .266 |
| Opioid use | ||||||||
| Heroin, lifetime | 100.0% | 100.0% | 100.0% | – | 100.0% | 100.0% | 100.0% | – |
| Prescription opioids, lifetime | 25.5% | 28.2% | 22.9% | .554 | 25.0% | 30.4% | 19.0% | .324 |
| Heroin, past 30 days | 67.1% | 65.4% | 68.7% | .782 | 63.6% | 58.7% | 69.0% | .432 |
| Prescription opioids, past 30 days | 14.9% | 11.5% | 18.1% | .346 | 12.5% | 10.9% | 14.3% | .872 |
| Cocaine use | ||||||||
| Lifetime | 86.3% | 84.6% | 88.0% | .699 | 87.5% | 84.8% | 90.5% | .628 |
| Past 30 days | 65.2% | 66.7% | 63.9% | .835 | 63.6% | 60.9% | 66.7% | .732 |
p-values calculated using chi-square, Fisher’s exact test, or 2-tailed Mann-Whitney U test. Continuous data are presented as means and standard deviations. Categorical data are presented as counts and percentages.
Calculated for those who were ever incarcerated.
Employment income consisted of income from paid wages from taxed work as well as “under the table” money. Non-employment income consisted of income from unemployment benefits, welfare (e.g., cash assistance, food stamps), pensions/retirement disbursements, Social Security Insurance Disability benefits, money received from friends or family, and income generated through illicit activities.
Opioid agonist treatment included past-month participation in methadone (95.0%) and buprenorphine (5.0%) programs.
All participants who were enrolled in the Workplace Study were eligible to begin EMA; however, EMA data collection was terminated before completion if a participant: (1) failed more than 12 smartphone “status checks,” (2) did not complete ≥ 82% of random prompts during 2 consecutive weeks, or (3) lost or damaged their smartphone. Smartphone status checks and random prompts are described below. Participants could continue to attend all other Workplace Study activities after their EMA data collection was terminated, or if they voluntarily withdrew from EMA data collection. Participants discharged early from the Workplace Study for any reason also had their EMA data collection terminated.
Of the n = 166 participants enrolled in the Workplace Study, n = 161 participants provided at least 1 EMA response, and n = 88 completed EMA data collection. Analyses were based on these samples of 161 or 88 participants, as described below.
Therapeutic Workplace procedures
Supplementary Figure S1 presents a schematic timeline of participants’ access to paid work in the Therapeutic Workplace, and the absence/presence of wage-resetting contingencies there to reinforce opiate- and cocaine-negative urinalysis.
Access to paid work in the Therapeutic Workplace
Randomization to Immediate vs. Delayed Work Groups
Upon enrollment, participants were randomly assigned (1:1) to the Immediate Work Group (IWG) or Delayed Work Group (DWG) using a computerized urn randomization procedure (Wei & Lachin, 1988). Various staff members operated the randomization program, but the NIDA investigators who collected participants’ EMA data were not involved in randomization. IWG could access paid work in the Therapeutic Workplace for up to 4 hours per day (10:00–12:00 and 13:00–15:00, with a “lunch break” from 12:00–13:00) each day Monday–Friday beginning on the day of their randomization. For DWG, a waitlist delay preventing access was in force for the first 3 weeks after randomization. During the delay, DWG only provided urine samples on the same schedule as IWG and completed EMA data collection tasks (smartphone issue and training, status checks, compliance review meetings). Although DWG were prevented from working, they were paid by the Therapeutic Workplace as though they had engaged in all paid work activities available to IWG (up to $8.00/hour base pay + $2.00/hour performance pay). Both DWG and IWG were also paid for EMA data collection during the delay. At the end of the delay, DWG could access paid work in the Therapeutic Workplace under the same conditions as IWG.
For the first 5 weeks, all participants earned from the Therapeutic Workplace the maximum base pay rate of $8.00/hour. Once abstinence-reinforcement contingencies were introduced at week 6: participants’ base pay was reduced to $1.00/hour (a “wage reset”) if they did not provide a required sample, or they provided an opiate-positive sample (weeks 6—7) or an opiate- or cocaine-positive sample (weeks 8—14). After a reset, participants’ base pay rate returned progressively to $8.00/hour once they provided drug-negative urine (see Toegel et al. 2020 for additional details).
Thus, EMA data were collected across four phases: (1) the final 2 weeks of the “Waitlist” phase, when only IWG could access paid work, and there were no wage-resetting contingencies in place; (2) the 2-week “Induction” phase, when both IWG and DWG could access paid work, and there were no wage-resetting contingencies; (3) the 2-week “Opiate contingency” phase (Opi con), when both IWG and DWG could access paid work, and a wage-resetting contingency for opiate-positive, but not cocaine-positive, urinalysis was in place; and (4) the 7-week “Opiate + cocaine contingency” phase (Opi+coc con), when both IWG and DWG could access paid work, and there were wage-resetting contingencies for both opiate-positive and cocaine-positive urinalysis.
Random vacation days
Throughout the four phases, the Therapeutic Workplace was closed to all participants on quasirandomly selected Tuesdays or Thursdays for “random vacation days.” On average, 1 random vacation day was given every other week (days between random vacation days: 12.6 ± 0.1 [average ± SEM]; range: 4—22). Random vacation days were intended to provide participants with unexpected time off from paid work in addition to their regular weekend time off. To provide minimal advance notice, Therapeutic Workplace staff did not alert participants until the day before that a Tuesday or Thursday would be a random vacation day. Written notice was also placed on the outer door of the CLH on random vacation days to alert participants of the closure. Participants were paid by the Therapeutic Workplace for random vacation days according to the average amount earned on the immediately preceding and following days.
EMA data collection procedures
One week after randomization, all participants were scheduled to be issued a smartphone (Samsung Galaxy Grand Prime or Samsung Galaxy On5 models; Samsung Telecommunications, Suwon, South Korea) and trained to use the Android-OS version of a custom-made app, mPAL (NIDA IRP Biomedical Informatics Section, Baltimore, MD, USA), to provide EMA data. Participants randomized from May 2017–July 2018 also used their study smartphones to access questionnaires on quality of life topics using the Delight Me mobile web app (Delight Me, Inc.; Washington, DC, USA); details of those assessments are reported elsewhere (Bertz et al. 2021).
Other features/functions of the smartphone were not disabled by mPAL, and smartphones were issued with active voice/MMS messaging/cellular data service plans (T-Mobile USA, Bellevue, WA, USA). The mPAL app used the cellular data service to transmit EMA and global positioning system (GPS) location data from participants’ handsets to secure servers at NIDA. Otherwise, we believed that having an active smartphone would help with participant “buy in” to EMA. If their phone status checks and weekly EMA compliance reviews were successful, participants were broadly permitted to use their smartphone as they would have used a commercially obtained device (e.g., change settings, install other apps, use the service plan). To preserve participant privacy, NIDA staff maintained all service plans, and no personal information about study participants was provided to the service provider.
Smartphone status checks
Once issued, participants were instructed to present their smartphones to study staff to be checked each day the Therapeutic Workplace was open and they were permitted to access paid work. Staff verified that each participant had his/her phone, and it was functioning and not damaged. The day’s check was failed if those criteria were not met, or if the participant did not request a check. Staff were also available to troubleshoot device or service issues identified in status checks.
EMA question types
Participants completed up to 4 types of EMA questionnaire: a “random prompt” questionnaire, which participants completed when alerted by their smartphones at randomly determined times during their self-reported typical waking hours, and 3 types of “event contingent” questionnaires, which participants initiated for themselves to report (1) drug use, (2) drug craving, or (3) stress. All present analyses are based on the random prompts; select event-contingent responses from a subset of participants have been used previously to validate the detection of drug use episodes by ambulatory physiological monitoring (Ertin et al. 2021).
Participants were issued 3 random prompts per day. After 15 min without a response, random prompts “expired” and could not be answered. We relied on prompts’ random timing to obtain responses at the Therapeutic Workplace and elsewhere (i.e., at work vs. not at work). Broadly consistent with the relative lengths of the Therapeutic Workplace workday and their waking hours, participants made 13.2% ± 0.9% (mean ± SEM) of their random prompt responses at work.
Supplementary Table S1 lists all random prompt questions and their response options. Stress, opioid craving, cocaine craving, and individual moods were measured with single items (scales: 1 = “No”/“None”/“Not at all” to 5 = “An extreme amount”/”Extremely”) asking about participants’ experience “right now.” The 6 items assessing flow-like states (scales: 1 = “NO!!” to 4 = “YES!!”) referenced participants’ activity at the time the phone alerted and were designed to capture several aspects of psychological flow commonly identified in previous studies: absorption/time distortion, enjoyment, intrinsic/extrinsic motivation, and challenge–skill matching (Bakker 2008; Engeser & Rheinberg 2008; Nakamura & Csikszentmihalyi 2009; Nielsen & Cleal 2010; Rodríguez-Sánchez et al. 2011).
Compliance reviews
EMA data reviews including payment were held with participants once per week, independently of any payments from the Therapeutic Workplace. Participants could earn up to $50.00 per week for providing EMA data: (1) $5.00 for completing all required smartphone status checks; (2) $15.00 for accurately reporting their drug use, as assessed by the congruence of their event-contingent reports and thrice-weekly urinalysis results; and (3) $20.00 for completing ≥ 82% (i.e., 18/21) random prompts scheduled that week.
Data analysis
Participant characteristics were compared using chi-square or Fisher’s exact test for categorical variables and t-tests or Mann-Whitney U for continuous variables. EMA data were analyzed as described below. For all analyses, differences were considered significant when p < .05, two-tailed. Familywise error rates were controlled with the adaptive Holm method (SAS proc MULTTEST) when performing multiple pairwise comparisons. Participant characteristics were analyzed using SPSS Statistics Subscription (IBM, Armonk, NY, USA). EMA data were analyzed using SAS version 9.4 (SAS Institute, Cary, NC, USA) or R version 3.6 (R Core Team 2018).
Data reduction before analysis
The 12 individual mood items were reduced using non-metric multidimensional scaling (NMDS; Hout et al. 2013; Rabinowitz 1975) using R package MASS (Sammon NMDS procedure; Venables & Ripley, 2002), producing an arrangement in two dimensions that we interpreted as valence (positive/negative) and activation (high/low) consistent with a circumplex model of emotion (Remington et al. 2000; Russell 1980): (1) high-activation positive mood (items Lively, Cheerful, Happy, Pleased); (2) low-activation positive mood (items Relaxed, Contented); (3) high-activation negative mood (items Afraid, Annoyed or angry, Sad, Bored or lonely); (4) low-activation negative mood (items Exhausted, Uneasy). For each random prompt response, (1) ratings of the individual moods within each category were averaged, and (2) responses to the 6 items assessing flow-like states were summed (total flow-like score range: 4–24).
Analysis 1: Differences in stress, craving, and mood “not at work” vs. “at work”
The first set of analyses was based on those of Epstein & Preston (2012) to examine participants’ stress, craving, mood, and flow-like states when they were not at work vs. at work. For each random prompt, participants (n = 161 who provided any EMA data) were classified as “at work” when they indicated their location was “Work (research program or other workplace)” and “not at work” when they indicated any other location (Supplementary Table S1). We included the “On a job search/interview/training” response among the “not at work” locations, as the search/interview aspects of this response differentiate it from actually being at work.
A mixed linear model (SAS proc. MIXED) was constructed for each endpoint (stress, opioid craving, cocaine craving, high-activation positive mood, low-activation positive mood, high-activation negative mood, low-activation negative mood, flow-like states) including location (not at work, at work), vocational skill1 (Hollingshead index from the ASI Lite; skilled = 1–5, semi/unskilled = 6–7), and the location X skill interaction. Control terms for Therapeutic Workplace phase (Waitlist, Induction, Opi con, Opi+coc con); group (IWG, DWG); sex (male, female); race/ethnicity (white, non-white); and age (years) were included. In these models, and those in Analyses 2 and 3 described below, predictors were treated as fixed, and a fixed intercept was used because models with a random intercept did not converge. An autoregressive error structure was used in all models, and denominator degrees of freedom were determined by the between-within method. Pairwise comparisons were performed post hoc within groups between locations or within location between groups using t-tests. For t-tests and for F-tests with dfnumerator = 1, we calculated effect size as reffect by the method of Rosnow and colleagues (2000) (for more on the issues around calculating effect sizes in multilevel models, see Lorah, 2018; Rights & Cole, 2018).
Analysis 2: Stress, craving, and mood during unexpected vs. expected time off from paid work
The second set of analyses assessed the associates of time off from paid work and differences when that time off was unexpected/unpredictable (random vacation days) vs. expected/predictable (weekends, when the Therapeutic Workplace was always closed). For each participant-day, the Therapeutic Workplace’s operating status was coded as (1) a Workday, when the Therapeutic Workplace was open under its normal operating schedule (10,260 participant-days); (2) a Vacation day (1,031 participant-days); or (3) a Weekend day (Saturday/Sunday; 4,088 participant-days). Days were excluded when the Therapeutic Workplace was closed for university holidays or weather/other emergency closures (785 participant-days). Participants’ EMA data were then used to check that they were following the Therapeutic Workplace’s operating schedule: days were excluded if a participant (1) did not report being at work on a Workday at least once (2,415 participant-days) or (2) reported being at work on a Vacation day (88 participant-days) or Weekend day (109 participant-days). These analyses also included all n = 161 participants who provided any EMA data.
Comparison of responses among day types was made using linear mixed models (R package lme4; Bates et al., 2015). Similarly to Analysis 1, a model was constructed for each endpoint including day type (Workday, Vacation, Weekend); vocational skill; and the day type X skill interaction. Control terms for Therapeutic Workplace phase, group, sex, race/ethnicity, and age were included. Separate models were created for responses made during the Therapeutic Workplace workday itself (10:00–15:00), when the time off from paid work was actually occurring/not occurring, and for responses made in the hours leading up to the Therapeutic Workplace workday (16:00–09:00), which were coded with the subsequent day’s day type to examine differences once participants knew that the following day would or would not have time off from paid work. Pairwise comparisons were performed post hoc among day types using t-ratios (R package emmeans; Lenth 2021).
After these endpoint-by-endpoint analyses of stress, craving, and mood, we explored relationships between pairs of EMA items and between each EMA item and day type using NMDS (Sammon NMDS procedure; R package MASS), which provides a concise graphic depiction of the relationships among all of these variables (see the Supplementary Methods and Results for additional details).
Analysis 3: Effects of randomization to work immediately vs. waitlist delay
The third set of analyses assessed effects of access to paid work by comparing IWG vs. DWG over time as each was or was not permitted to work. To ensure that participants contacted all 4 phases of the Therapeutic Workplace intervention, these analyses were conducted with the n = 88 EMA completers. A linear mixed model (SAS proc. MIXED) was constructed for each endpoint including group, Therapeutic Workplace phase, and the group X phase interaction. Control terms for sex, race/ethnicity, skill, and age were also included. Pairwise comparisons were performed post hoc within groups among phases or within phases between groups using t-tests. In these analyses, we observed group differences in stress and craving that persisted across phases. Therefore, we also examined participants’ urinalysis data to explore possible inadvertent group differences in drug use (Supplementary Methods and Results).
Results
For brevity, statistically nonsignificant results are not reported numerically.
Compliance with EMA data collection
A CONSORT diagram of participant flow through the Workplace Study is provided by Holtyn and colleagues (2020). 161/166 participants enrolled in the Workplace Study provided at least 1 EMA response; the other 5 were never issued a smartphone because they were discharged from the Workplace Study before the training session (n = 3) or did not attend and were lost to contact (n = 2). 88 participants completed EMA data collection; reasons for non-completion were: damaged or lost smartphone (n = 24), ceased attending the Therapeutic Workplace/lost to contact (n = 21), noncompliant with random prompting (n = 17), withdrew voluntarily from EMA (n = 9), discharged from the Workplace Study for non-EMA reasons (n = 2). Rates of non-completion were similar for IWG (n = 32, 43.8%) vs. DWG (n = 41, 56.2%).
Compliance with random prompting among the n = 161 EMA participants was good. Participants completed an average (standard deviation) of 153.9 (82.5) random prompt questionnaires, for a total response rate of 24,776/29,723 questionnaires scheduled (83.4%).
Participant characteristics
Table 1 presents the characteristics of participants in the full EMA sample and in the subset of completers, with IWG and DWG presented separately in each. There were no significant differences between IWG and DWG in the full sample or the completers. There were no significant differences between EMA completers and non-completers collapsing IWG and DWG, except in typical employment history, χ2(3) = 9.82, p = .020, and vocational skill, χ2(1) = 8.18, p = .004. Non-completers were less likely to report full-time employment (5.5% vs. 21.6%), but not part-time employment (16.4% vs. 9.1%), and to be skilled workers (17.8% vs. 39.8%).
Analysis 1: Differences in stress, craving, and mood “not at work” vs. “at work”
Figure 1 presents the stress, craving, and mood of participants, separated by vocational skill, when sampled “not at work” or “at work.” All endpoints had a significant main effect of location. When at work, participants reported: less stress, F(1,151) = 8.05, p = .0052, reffect = .22; less opioid craving, F(1,151) = 14.54, p = .0002, reffect = .29; less cocaine craving, F(1,151) = 42.53, p < .0001, reffect = .46; more high-activation positive mood, F(1,151) = 116.05, p < .0001, reffect = .65; more low-activation positive mood, F(1,151) = 12.38, p = .0006, reffect = .27; less high-activation negative mood, F(1,151) = 12.48, p = .0005, reffect = .27; less low-activation negative mood, F(1,151) = 45.88, p < .0001, reffect = .48; and more flow-like states, F(1,151) = 210.97, p < .0001, reffect = .76. As detailed below, there were also significant effects of vocational skill, as a main effect of skill and/or location X skill interaction, depending on the endpoint.
Figure 1:
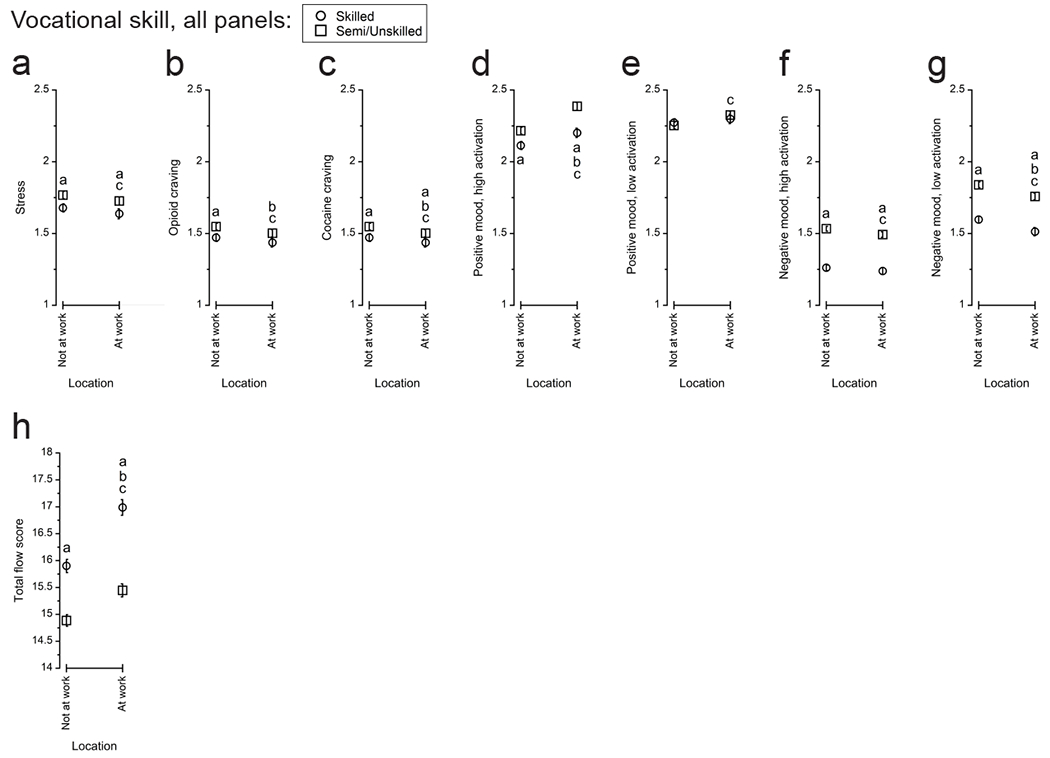
Affective differences when participants reported being “not at work” vs. “at work” by their EMA random prompting. a) stress, b) opioid craving, c) cocaine craving, d) high-activation positive mood, e) low-activation positive mood, f) high-activation negative mood, g) low-activation negative mood, h) flow-like states (total flow score). Within each panel, letters indicate statistically significant (p < .05) differences: a, difference by vocational skill within location; b, difference between locations for skilled workers; c, difference between locations for semi/unskilled workers.
Stress
For stress (Figure 1a), the location X skill interaction was not significant, but there was a significant main effect of skill, F(1,114) = 6.71, p = .0108, reffect = .23. By pairwise comparison, skilled workers reported less stress than semi/unskilled workers both not at work, t(151) = 2.73, p = .0071, reffect = .22, and at work, t(151) = 2.15, p = .0333, reffect = .17. Semi/unskilled workers reported less stress at work than not at work, t(151) = 2.41, p = .0172, reffect = .19.
Craving
For opioid craving (Figure 1b), the location X skill was not significant, but there was a significant main effect of skill, F(1,114) = 4.84, p = .0299, reffect = .20. Compared to semi/unskilled workers, skilled workers reported less opioid craving when not at work, t(151) = 2.46, p = .0152, reffect = .20. Both skilled workers, t(151) = 2.02, p = .0451, reffect = .16, and semi/unskilled workers, t(151) = 3.69, p = .0003, reffect = .29, reported less opioid craving at work vs. not at work.
For cocaine craving (Figure 1c), both the main effect of skill, F(1,114) = 23.40, p < .0001, reffect = .41, and the location X skill interaction, F(1,151) = 10.26, p = .0017, reffect = .25 were significant. Compared to semi/unskilled workers, skilled workers reported less cocaine craving both not at work, t(151) = 6.10, p < .0001, reffect = .44, and at work, t(151) = 3.32, p = .0011, reffect = .26. Both skilled workers, t(151) = 2.06, p = .0411, reffect = .17, and semi/unskilled workers, t(151) = 8.21, p < .0001, reffect = .56, reported less cocaine craving at work than not at work, with the significant interaction indicating a larger difference between locations for the semi/unskilled workers.
Positive mood
For high-activation positive mood (Figure 1d), both the main effect of skill, F(1,114) = 18.54, p < .0001, reffect = .37, and the location X skill interaction, F(1,151) = 11.66, p = .0008, reffect = .26, were significant. Compared to semi/unskilled workers, skilled workers reported less high-activation positive mood both not at work, t(151) = 3.19, p = .0034, reffect = .25, and at work, t(151) = 4.80, p < .0001, reffect = .36. Both skilled workers, t(151) = 4.57, p < .0001, reffect = .35, and semi/unskilled workers, t(151) = 11.97, p < .0001, reffect = .70, reported more high-activation positive mood at work than not at work, with the significant interaction indicating a larger difference for semi/unskilled workers.
For low-activation positive mood (Figure 1e), neither the main effect of skill nor the location X skill interaction was significant. Semi/unskilled workers reported more low-activation positive mood at work than not at work, t(151) = 4.43, p < .0001, reffect = .34, the only significant pairwise difference.
Negative mood
For high-activation negative mood (Figure 1f), the location X skill interaction was not significant, but there was a significant main effect of skill, F(1,114) = 131.51, p < .0001, reffect = .73. Compared to semi/unskilled workers, skilled workers reported less high-activation negative mood both not at work, t(151) = 12.38, p < .0001, reffect = .71, and at work, t(151) = 9.40, p < .0001, reffect = .61. By pairwise comparison, semi/unskilled workers reported less high-activation negative mood at work than not at work, t(151) = 3.84, p = .0002, reffect = .30.
For low-activation negative mood, (Figure 1g), the location X skill interaction was not significant, but there was a significant main effect of skill, F(1,114) = 74.97, p < .0001, reffect = .62. Compared to semi/unskilled workers, skilled workers reported less low-activation negative mood both not at work, t(151) = 9.09, p < .0001, reffect = .59, and at work, t(151) = 7.16, p < .0001, reffect = .50. Both skilled workers, t(151) = 4.27, p < .0001, reffect = .50, and semi/unskilled workers, t(151) = 5.63, p < .0001, reffect = .42, reported less low-activation negative mood at work than not at work.
Flow-like states
For flow-like states (Figure 1h), both the main effect of skill, F(1,113) = 75.36, p < .0001, reffect = .63, and the location X skill interaction, F(1,151) = 21.62, p < .0001, reffect = .35, were significant. Compared to semi/unskilled workers, skilled workers reported more flow-like states both not at work, t(151) = 7.18, p < .0001, reffect = .50, and at work, t(151) = 8.93, p < .0001, reffect = .59. Both skilled workers, t(151) = 11.94, p < .0001, reffect = .70, and semi/unskilled workers, t(151) = 8.29, p < .0001, reffect = .56, reported more flow-like states at work than not at work, with the significant interaction indicating a larger difference for skilled workers.
Analysis 2: Stress, craving, and mood during unexpected vs. expected time off from paid work
Figure 2a–h presents the stress, craving, and mood of participants, separated by vocational skill, when sampled on regularly scheduled Therapeutic Workplace workdays and days with time off from the Therapeutic Workplace that was either unexpected (random vacation days) or expected (weekend days). These different day types were divided into the hours of the Therapeutic Workplace workday itself (10:00–15:00, right pane of each panel in Figure 2a–h) and before the hours of the Therapeutic Workplace workday (16:00–09:00, left pane of each panel in Figure 2a–h), i.e., to examine possible anticipatory differences that could emerge once participants knew the following day’s type. Figure 2i presents a scattergram depicting the similarities among random prompt items and the day types in two dimensions (for more details see Supplementary Methods and Results).
Figure 2:
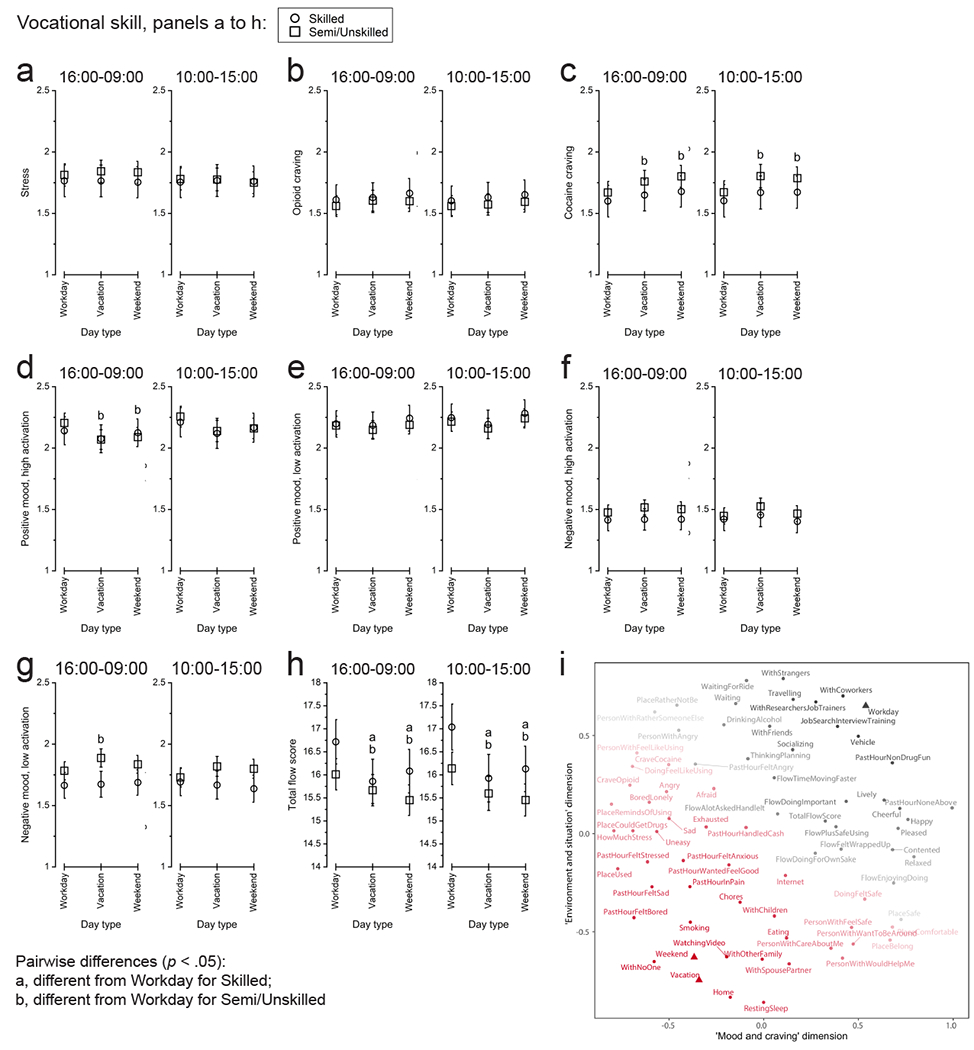
Affective differences on regularly scheduled Therapeutic Workplace workdays (Workday), random vacation days (Vacation) to provide unexpected time off from paid work, and weekends (Weekend) to provide expected time off from paid work: a) stress, b) opioid craving, c) cocaine craving, d) high-activation positive mood, e) low-activation positive mood, f) high-activation negative mood, g) low-activation negative mood, h) flow-like states (total flow score), i) arrangement of EMA random prompt items in two dimensions by non-metric multidimensional scaling. For panels a-h, 16:00-09:00 (left pane within the panel for each endpoint) refers to the evening before to the morning of the indicated day type; 10:00-15:00 (right pane within the panel for each endpoint) refers to the day of the indicated day type. These intervals correspond, respectively, to the time between the end of one Therapeutic Workplace work shift and the beginning of the next Therapeutic Workplace work shift, and to the time of the Therapeutic Workplace work shift itself. Within each panel, letters indicate statistically significant (p < .05) differences: a, difference from Workday for skilled workers; b, difference from Workday for semi/unskilled workers. For panel i, the color and shading of each item represents its correlational distance from Workdays (gray) or Weekend days (red). The axis labels (x-axis as “Mood and craving” and y-axis as “Environment and situation”) are based on our inspection of the overall arrangement of the items.
Stress, craving, and mood during the Therapeutic Workplace workday (10:00–15:00) among day types
During the hours of the Therapeutic Workplace workday itself, neither the main effect of skill nor the location X skill interaction was significant for any endpoint.
The main effect of day type and all pairwise comparisons among types were not significant for stress (Figure 2a), opioid craving (Figure 2b), or low-activation positive mood (Figure 2e). There were significant main effects of day type for the remaining endpoints: cocaine craving (Figure 2c), F(2,142) = 7.27, p = .0010; high-activation positive mood (Figure 2d), F(2,141) = 5.02, p = .0078; high-activation negative mood (Figure 2f), F(2,141) = 3.55, p = .0312; low-activation negative mood (Figure 2g), F(2,141) = 3.36, p = .0374; and flow-like states (Figure 2h), F(2,141) = 8.90, p = .0002. There were significant pairwise differences for cocaine craving and flow-like states. Semi/unskilled workers reported less cocaine craving on workdays than on random vacation days, t(142) = 3.18, p = .0126, reffect = .26, or on weekends, t(142) = 3.36, p = .0070, reffect = .27. Both skilled workers and semi/unskilled workers reported more flow-like states on workdays than on random vacation days or on weekend days: workdays vs. random vacation days for skilled workers, t(141) = 4.20, p < .0001, reffect = .33; workdays vs. random vacation days for semi/unskilled workers, t(141) = 2.68, p = .0162, reffect = .22; workdays vs. weekends for skilled workers, t(141) = 4.10, p = .0002, reffect = .33; workdays vs. weekends for semi/unskilled workers, t(141) = 4.13, p = .0002, reffect = .33.
Stress, craving, and mood before the Therapeutic Workplace workday (16:00–09:00) among day types
During the hours before the Therapeutic Workplace workday, neither the main effect of skill nor the location X skill interaction was significant for any endpoint. The pattern of endpoints without vs. with significant effects of day type was similar to the hours of the Therapeutic Workplace workday. The main effect of day type and all pairwise comparisons among days were not significant for stress, opioid craving, low-activation positive mood, or high-activation negative mood. There were significant main effects of day type for cocaine craving (Figure 2c), F(2,143) = 12.88, p < .0001; high-activation positive mood (Figure 2d), F(2,143) = 12.56, p < .0001; low-activation negative mood (Figure 2g), F(2,143) = 6.73, p = .0016; and flow-like states (Figure 2h), F(2,143) = 10.43, p < .0001. By pairwise comparison, semi/unskilled workers reported less cocaine craving on workdays than random vacation days, t(143) = 3.04, p = .0056, reffect = .25, or on weekends, t(143) = 5.07, p < .0001, reffect = .39. Semi/unskilled workers reported more high-activation positive mood on workdays than on random vacation days, t(143) = 4.53, p < .0001, reffect = .35, or on weekends, t(143) = 4.37, p < .0001, reffect = .34. Semi/unskilled workers also reported less low-activation negative mood on workdays than random vacation days, t(143) = 3.67, p = .0015, reffect = 0.29. Finally, both skilled workers and semi/unskilled workers reported more flow-like states on workdays than on random vacation days or on weekend days or on vacation days: workdays vs. random vacation days for skilled workers, t(143) = 4.54, p < .0001, reffect = .35; workdays vs. random vacation days for semi/unskilled workers, t(143) = 2.46, p = .0294, reffect = .20; workdays vs. weekends for skilled workers, t(143) = 3.85, p = .0004, reffect = .31; workdays vs. weekends for semi/unskilled workers, t(143) = 4.56, p < .0001, reffect = .36.
Analysis 3: Effects of randomization to work immediately vs. waitlist delay
Figure 3 presents the stress, craving, and mood of participants, separated by IWG vs. DWG, over the course of the Therapeutic Workplace phases determined by the groups’ access to paid work and wage-resetting contingencies to reinforce abstinence from opiates and/or cocaine.
Figure 3:
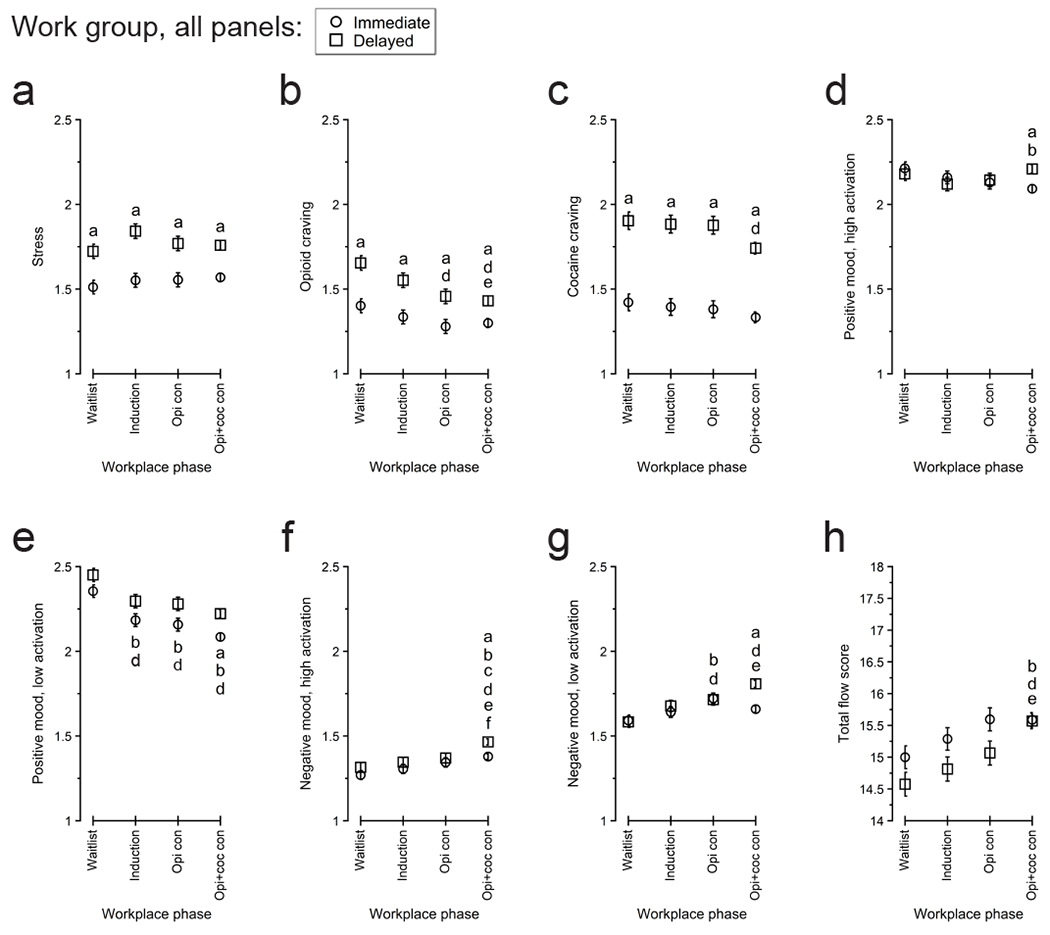
Participants’ EMA-reported affect between groups and across the Therapeutic Workplace phases defined by participants’ access to paid work and the presence of wage-resetting urinalysis contingencies: a) stress, b) opioid craving, c) cocaine craving, d) high-activation positive mood, e) low-activation positive mood, f) high-activation negative mood, g) low-activation negative mood, h) flow-like states (total flow score). Within each panel, letters indicate statistically significant (p < .05) differences: a, difference between groups within phase; b, difference from Waitlist for IWG; c, difference from Induction for IWG; d, difference from Waitlist for DWG; e, difference from Induction for DWG; f, difference from Opi con for DWG. Opi con, opiate contingency; Opi+coc con, opiate and cocaine contingencies.
Stress
Stress (Figure 3a) differed between groups, main effect of group, F(1,50) = 47.79, p < .0001, reffect = .69, but not across phases, with the main effect of phase, group X phase interaction, and all pairwise comparisons nonsignificant. During each phase, IWG reported less stress than DWG: Waitlist, t(258) = 3.60, p = .0044, reffect = .22; Induction, t(258) = 4.90, p < .0001, reffect = .29; Opi con, t(258) = 3.59, p = .0044, reffect = .22; Opi+coc con, t(258) = 5.04, p < .0001, reffect = .30.
Craving
Opioid craving (Figure 3b) differed between groups, main effect of group, F(1,50) = 32.62, p < .0001, reffect = .62, and across phases, main effect of phase, F(3,258) = 9.41, p < .0001, without a significant group X phase interaction. During each phase, IWG reported less opioid craving than DWG: Waitlist, t(258) = 4.26, p < .0001, reffect = .26; Induction, t(258) = 3.66, p = .0006, reffect = .22; Opi con, t(258) = 2.97, p = .0064, reffect = .18; Opi+coc con, t(258) = 3.35, p =.0018, reffect = .20. By pairwise comparison, DWG reported less opioid craving when opiate-abstinence was reinforced than when it was not: Waitlist vs. Opi con, t(258) = 3.51 , p = .0010, reffect = .21; Waitlist vs. Opi+coc con, t(258) = 4.85, p < .0001, reffect = .29; Induction vs. Opi+coc con, t(258) = 2.63, p = .0182, reffect = .16.
Cocaine craving (Figure 3c) also differed between groups, main effect of group, F(1,50) = 128.20, p < .0001, reffect = .85, and across phases, main effect of phase, F(3,258) = 4.86, p = .0026, without a significant group X phase interaction. In each phase, IWG reported less cocaine craving than DWG: Waitlist, t(258) = 6.70, p < .0001, reffect = .38; Induction, t(258) = 6.81, p < .0001, reffect = .39; Opi con, t(258) = 6.85, p < .0001, reffect = .39; Opi+coc con, t(258) = 8.60, p < .0001, reffect = .47. By pairwise comparison, DWG reported less cocaine craving during Opi+coc con vs. Waitlist, t(258) = 2.90, p = .0451, reffect = .18.
Positive mood
For high-activation positive mood (Figure 3d), the difference between groups depended on the Therapeutic Workplace phase, group X phase interaction, F(3,258) = 3.63, p = .0135, with the main effects of group and phase nonsignificant. By pairwise comparison, IWG reported less high-activation positive mood during Opi+coc con than Waitlist, t(258) = 2.90, p = .0160, reffect = .18. IWG also reported less high-activation positive mood than DWG during Opi+coc con, t(258) = 3.33, p = .0040, reffect = .20.
Low-activation positive mood (Figure 3e) differed between groups, main effect of group, F(1,50) = 15.08, p = .0003, reffect = .48, and across phases, main effect of phase, F(3,258) = 24.21, p < .0001, without a significant group X phase interaction. Generally, low-activation positive mood decreased over time. IWG reported less low-activation positive mood during all subsequent phases vs. Waitlist: Induction, t(258) = 3.44, p = .0021, reffect = .21; Opi con, t(258) = 3.87, p = .0003, reffect = .23; Opi+coc con, t(258) = 6.57, p < .0001, reffect = .38. DWG also reported less low-activation positive mood during all subsequent phases vs. Waitlist: Induction, t(258) = 3.02, p = .0084, reffect = .18; Opi con, t(258) = 3.30, p = .0033, reffect = .20; Opi+coc con, t(258) = 5.46, p < .0001, reffect = .32. Between groups, IWG reported less low-activation positive mood than DWG during Opi+coc con, t(258) = 3.97, p = .0003, reffect = .24.
Negative mood
High-activation negative mood (Figure 3f) differed between groups, main effect of group, F(1,50) = 5.22, p = .0266, reffect = .31, and across phases, main effect of phase, F(3,258) = 16.00, p < .0001, without a significant group X phase interaction. High-activation negative mood generally was higher when the opiate- and cocaine-abstinence reinforcement contingencies were present. IWG reported more high-activation negative mood during Opi+coc con than during Waitlist, t(258) = 3.71, p = .0006, reffect = .23, and Induction, t(258) = 2.47, p = .0284, reffect = .17. DWG reported more high-activation negative mood during Opi+coc con than during each of the preceding phases: Waitlist, t(258) = 5.02, p < .0001, reffect = .30; Induction, t(258) = 3.96, p = .0002, reffect = .24; Opi con, t(258) = 3.18, p = .0034, reffect = .19. Between groups, IWG reported less high-activation negative mood than DWG during Opi+coc con, t(258) = 3.49, p = .0012, reffect = .21.
Low-activation negative mood (Figure 3g) differed among phases, main effect of phase, F(3,258) = 12.86, p < .0001, differently for the groups, group X phase interaction, F(3,258) = 5.81, p = .0007. The main effect of group was not significant. Low-activation negative mood was also generally higher when abstinence-reinforcement contingencies were present than when they were absent. IWG reported more low-activation negative mood during Opi con than during Waitlist, t(258) = 3.03, p = .0189, reffect = .19. DWG reported more low-activation negative mood during Opi con, t(258) = 3.01, p = .0203, reffect = .18, and Opi+coc con, t(258) = 6.39, p < .0001, reffect = .37, than during Waitlist. DWG also reported more low-activation negative mood during Opi+coc con than Induction, t(258) = 3.68, p = .0021, reffect = .22. Between groups, IWG reported less low-activation negative mood than DWG during Opi+coc con, t(258) = 5.19, p < .0001, reffect = 0.31.
Flow-like states
Flow-like states (Figure 3h) differed between groups, main effect of group, F(1,50) = 6.24, p = .0158, reffect = .33, and across phases, main effect of phase, F(3,258) = 12.30, p < .0001, without a significant group X phase interaction. Flow-like states increased for both groups over the course of the study. IWG reported more flow-like states during Opi+coc con than Waitlist, t(258) = 2.99, p = .0155, reffect = .18. DWG reported more flow-like states during Opi+coc con than Waitlist, t(258) = 4.95, p < .0001, reffect = .29, and Induction, t(258) = 3.74, p = .0010, reffect = .23. No pairwise difference between groups was significant.
Discussion
We used EMA to measure the stress, craving, and mood of participants with OUD during a randomized trial of a contingency-management-based Therapeutic Workplace. Expanding on previous research with participants employed in the community apart from the study itself (Epstein & Preston 2012; Shiffman & Waters 2004), we used the Therapeutic Workplace to (1) standardize participants’ job site and activities and (2) control participants’ access to work with a waitlist delay and random vacation days. Under these conditions, we were able to detect specific affective improvements associated with work. Surprisingly, however, the waitlist delay did not produce the expected effects.
Participants’ better mood (less negative mood, more positive mood) at work vs. not at work is consistent with Epstein and Preston’s (2012) finding differences in people with OUD that contrast with the general population. In previous experience-sampling studies, participants from the general population have reported work as an undesired location/activity (Csikszentmihalyi & Graef 1980) where they experience either the same or less happiness compared to other locations/activities (Killingsworth & Gilbert 2010; Steptoe et al. 2005; see also Brandstätter 1994). This is still a potentially important contrast, but influences of unemployment history, both proximal and distal, on emotional responses to work may also be relevant. Because they had to be initially unemployed for this study, participants’ ratings of the Therapeutic Workplace may reflect effects of re-employment. Generally, in studies with retrospective self-report, re-employment after unemployment is associated with improvements in mood or in mental health more broadly (e.g., Ginexi et al. 2000; Kessler et al. 1989; Zhou et al. 2019), but responses can depend on job quality (Monfort et al. 2015; Wanberg 1995) and the reasons for unemployment (Waters 2007). Even without a study inclusion criterion of unemployment (e.g., Epstein and Preston 2012), the responses of people with SUDs to work may be shaped by unemployment histories that tend to be more severe than the general population (as reviewed in the Introduction). More experience-sampling work is needed to understand the influences of unemployment history specifically on differences between work and elsewhere in daily life (cf. Kirchler 1985).
Stress, craving, and mood improvements at work vs. not at work
Whereas the significant main effect of location indicated improvements at work for all endpoints in Analysis 1, the interactions with skill are also noteworthy because they show that, at least for certain endpoints (cocaine craving, high-activation positive mood), workers with lower vocational skill may actually experience greater benefits from being at work. It is important to demonstrate that the benefits of work are not necessarily restricted to more skilled or higher status workers, who may be expected to have access to “better” jobs; conversely, skilled workers also still reported benefits from the comparatively basic tasks in the Therapeutic Workplace training programs. Thus, including vocational skill in our analyses demonstrates the findings’ generality in key ways (see also Silverman et al. 2018 on the use of different kinds of employment interventions in workers with different skill levels).
In addition to replicating the findings of Epstein and Preston (2012) on stress, craving, and mood, we were also able to measure increases in flow-like states at work in this study. Flow is generally considered a positive or desirable psychological state (Nakamura & Csikszentmihalyi 2009; but see also Abuhamdeh 2020). Therefore, it is reasonable to consider flow as an additional potential benefit from work in this population. Whereas earlier studies related flow to “peak” or “optimal” performance, i.e., highly skilled individuals such as virtuoso musicians or elite athletes executing complex routines (e.g., Jackson et al. 2001; Marin & Bhattacharya 2013; cf., Abuhamdeh 2020), our results illustrate the potential importance of also characterizing flow-like states in non-expert or novice populations acquiring new skills (or re-acquiring skills not recently or frequently used) (Gold & Ciorciari 2019; Wang & Chen 2011; cf., Rau et al. 2006). Flow may still reflect a peak or optimal performance for the level of performance an individual can currently obtain (i.e., a local vs. global maximum), but there is growing recognition that flow-like states may help people acquire skills, not only use them in an advanced state. Even so, several aspects of our findings are also consistent with models of flow that emphasize challenge–skill matching (Abuhamdeh 2020; Engeser & Rheinberg 2008): the location X skill interaction indicating a larger increase in flow-like states at work for skilled workers, and the increase in flow-like states reported over the course of the study as participants gained more experience working in the Therapeutic Workplace. Additional studies are needed to understand fully the function of flow-like states in SUDs and their treatment. It has been suggested that aspects of flow, or a “dark flow” counterpart to the positive psychological experience, could contribute to behavioral addictions such as gambling or (potentially) video gaming (Chou & Ting, 2003; Dixon et al. 2018; Hull et al. 2013; Partington et al. 2009; Rau et al. 2006; but see Wan & Chiou 2006). However, it has not always been clear that these risks are specific to flow vs. other emotional/cognitive experiences, and there may also be potential beneficial effects from commonalities between flow and mindfulness (cf., Meggs & Chen, 2021; Reid, 2011).
Effects of restricting access to the Therapeutic Workplace: workdays vs. free days and immediate vs. delayed work
Some of the differences observed in moments not at work vs. at work were also observed when participants were restricted from working in the Therapeutic Workplace on weekends and random vacation days. These results show that some of the positive effects of work are not necessarily restricted to moments actually in a workplace. In particular, we observed differences in the hours before regular workdays in addition to the hours of the workdays themselves, indicating more clearly that the benefits of work extend beyond work itself: less cocaine craving, more high-activation positive mood, less low-activation negative mood, and more flow-like states.
We did not find a significant difference in any endpoint between random vacation days and weekends. Unstructured time, and/or its associated boredom, have previously been identified as a relapse risk for people with OUD (e.g., Bradley et al. 1989, Epstein et al. 2009; Kowalczyk et al. 2017; McKay et al. 2006, Notley et al. 2015). To the extent that participants themselves recognize this risk and employ strategies to counter it (e.g., planning activities ahead of time to avoid boredom), we anticipated that unexpected free time (random vacation days) would be worse than expected free time (weekends). It is possible that participants simply did not experience unexpected free time more negatively, as indicated by the lack of differences in their EMA reports themselves, or they did not engage in planning/coping strategies even when the free time was predictable. Although we coded participants’ time outside the Therapeutic Workplace workday to examine possible anticipatory effects once participants knew the next day’s type, participants may also have been influenced by residual effects from work- vs. free-time earlier in the day/on the previous day.
Considering the difference between IWG and DWG, we were surprised to find no significant differences related specifically to the beginning of DWG’s access to the paid work (i.e., differences between IWG and DWG during the Waitlist phase but not subsequently, or differences only within DWG from the Waitlist phase to the Induction phase). Instead, we found differences that either persisted across all study phases or occurred later in the study after both groups could work. There were not significant differences between the groups in the baseline parameters we measured, and their drug use during the study did not persistently differ (Supplementary Methods and Results). There may still have been inadvertent group differences in parameters not measured in this study. Nonetheless, it is noteworthy that the group differences predominantly indicated that DWG participants were having worse experiences, with higher levels of stress, opioid craving, and cocaine craving. Similar group differences were also observed in the subset of participants that completed quality of life measures in addition to EMA (Bertz et al. 2021): DWG had consistently lower quality of life in several areas that was not clearly associated with the onset of Therapeutic Workplace access. We speculated that some of those differences were related to exposure to the waitlist itself: waiting for treatment could have given DWG different expectations about themselves or the study (reviewed by Bertz et al. 2021). This is potentially an important issue for studies using waitlists; however, other control conditions may also produce their own unintended effects. For clinical practice, the clear implication is to begin participants working in the Therapeutic Workplace as soon as possible.
For interpreting both of the above analyses, it is possible that some participants may have worked jobs outside the Therapeutic Workplace at some point during the course of the study. This was not explicitly prevented (e.g., as a study exclusion criterion), but we believe it is unlikely to have been widespread. In monthly assessments conducted for the Workplace Study, very few participants reported any outside employment (Holtyn et al. 2020), and in the EMA data themselves, few days were excluded from Analysis 2 due to participants reporting work on Therapeutic Workplace non-work days.
Finally, participants reported mood differences that coincided with the introduction of the urinalysis contingencies. Increased negative mood/decreased positive mood may have been associated in several ways with the abstinence requirement, either as participants successfully became abstinent (cf., De Leon et al. 2020 on EMA-reported negative mood and alcohol abstinence), or as they did not and experienced wage resets. In assessing possible negative effects of wage resets, Holtyn and Silverman (2016) found that resets produced only transient effects on Therapeutic Workplace engagement (attendance and hours worked) immediately after they occurred, with no overall reductions in engagement. Nonetheless, future work should focus on how enhanced support could be given to participants experiencing worse moods at these points.
Limitations
Participants in this study had to express an interest in ultimately obtaining employment in the community, and it is unclear how our results would apply to those working in the Therapeutic Workplace without that interest. Our sample also consists of workers in one city in the United States. There may be differences in workers’ affective experiences (e.g., stress, satisfaction) in urban and rural areas (e.g., Ehly & Reimers 1986; Gellis et al. 2004), and workers in other countries may also have different experiences. As discussed above, DWG participants may have inadvertently been affected by exposure to the waitlist per se. This possibility should be considered in light of the rarity of the opportunity to determine experimentally participants’ ability to work.
Conclusion
This study provides additional insight into how people with SUDs respond emotionally to work. Although participants in this study engaged in contingency-management-based experimental work and did not have “real” jobs, there is a stronger case to be made that people with OUD experience emotional improvements at work when considering these results alongside those of Epstein and Preston (2012) on community employment. As a “respite from drug using companions” (Epstein & Preston 2012, p. 189), work could provide predictability, physical safety, comfort, and a lack of exposure to drug-associated stimuli, but there are also possible sources of stress and negative mood in workplaces (e.g., conflicts with coworkers or bosses, exposure to risk of physical injury). Our exploratory NMDS of the random prompt questionnaire (Figure 2i, Supplemental Methods and Results) supports the idea that the Therapeutic Workplace was comparatively free of associations with drug use and negative social and physical features; however, it will be important in future work to clarify further which social and physical aspects of workplaces are most impactful for which workers, and the extent to which those properties are unique to workplaces vs. other settings. Although the group effect may be a positive one, EMA and related intensive longitudinal methods may also help identify cases (in individual workers or individual workplaces) where people are not experiencing such benefits. Ultimately, while recognizing the benefits of work, it is important not to advocate for overly broad or overly strict advocacy of work programs for people with SUDs, and we would expect only adverse consequences if those with persistent employment problems are stigmatized.
Supplementary Material
Highlights.
People with opioid use disorder (OUD) often need help with employment problems.
We “employed” people with OUD in a contingency-management-based study workplace.
We collected randomly timed ratings of stress, craving, and mood via smartphone.
Stress, craving, and mood were better at work and, for some endpoints, on workdays.
These results highlight some particular benefits of employment for people with OUD.
Acknowledgments:
We thank Andrew Rodewald, Calvin Jackson, Jacqueline Hampton, and all CLH staff members for their work on the Therapeutic Workplace intervention; Gabriela Gonzalez for her assistance with EMA data collection; and Rayfield Yarbrough for his assistance managing participants’ phone service accounts.
Role of the funding source:
This research was supported by the Intramural Research Program of the NIH, NIDA and by NIDA grant R01DA037314. NIDA had no involvement in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of interest: none
We are using the terms semi-skilled and unskilled because these are the labels of the Hollingshead categories used by the ASI. We do not mean to minimize the capacity of workers or imply any negative value judgments about the occupations classified in these ways.
References
- Abuhamdeh S (2020). Investigating the “flow” experience: Key conceptual and operational issues. Frontiers in Psychology, 11, 158. doi: 10.3389/fpsyg.2020.00158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bakker AB (2008). The work-related flow inventory: Construction and initial validation of the WOLF. Journal of Vocational Behavior, 72(3), 400–414. doi: 10.1016/j.jvb.2007.11.007 [DOI] [Google Scholar]
- Bates D, Maechler M, Bolker B, & Walker S (2015). Fitting linear mixed-effects models using lme4. Journal of Statistical Software, 67(1), 1–48. doi: 10.18637/jss.v067.i01 [DOI] [Google Scholar]
- Bauld L, McKell J, Carroll C, Hay G, & Smith K (2012). Benefits and employment: How problem drug users experience welfare and routes into work. Journal of Social Policy, 41(4), 751–768. doi: 10.1017/S004727941200030X [DOI] [Google Scholar]
- Bell J, & Strang J (2020). Medication treatment of opioid use disorder. Biological Psychiatry, 87(1), 82–88. doi: 10.1016/j.biopsych.2019.06.020 [DOI] [PubMed] [Google Scholar]
- Bertz JW, Smith KE, Panlilio LV, Stull SW, Reamer D, Murville M-L, Sullivan M, Holtyn AF, Toegel F, Epstein DH, Phillips KA, & Preston KL (2021). Quality of life during a randomized trial of a therapeutic-workplace intervention for opioid use disorder: Web-based mobile assessments reveal effects of drug abstinence and access to paid work. Drug and Alcohol Dependence Reports, 1, 100011. 10.1016/j.dadr.2021.100011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bradley BP, Phillips G, Green L, & Gossop M (1989). Circumstances surrounding the initial lapse to opiate use following detoxification. British Journal of Psychiatry, 154, 354–359. doi: 10.1192/bjp.154.3.354 [DOI] [PubMed] [Google Scholar]
- Brandstätter H (1994). Well-being and motivational person–environment fit: A time-sampling study of emotions. European Journal of Personality, 8, 75–93. doi: 10.1002/per.2410080202 [DOI] [Google Scholar]
- Brewer DD, Catalano RF, Haggerty K, Gainey RR, & Fleming CB (1998). A meta-analysis of predictors of continued drug use during and after treatment for opiate addiction. Addiction, 93(1), 73–92. doi: 10.1046/j.1360-0443.1998.931738.x [DOI] [PubMed] [Google Scholar]
- Cacciola JS, Alterman AI, McLellan AT, Lin YT, & Lynch KG (2007). Initial evidence for the reliability and validity of a “Lite” version of the Addiction Severity Index. Drug and Alcohol Dependence, 87(2-3), 297–302. doi: 10.1016/j.drugalcdep.2006.09.002 [DOI] [PubMed] [Google Scholar]
- Chou TJ, & Ting CC (2003). The role of flow experience in cyber-game addiction. CyberPsychology & Behavior, 6(6), 663–675. doi: 10.1089/109493103322725469 [DOI] [PubMed] [Google Scholar]
- Csikszentmihalyi M, & Graef R (1980). The experience of freedom in daily life. American Journal of Community Psychology, 8(4), 401–414. doi: 10.1007/BF00912853 [DOI] [Google Scholar]
- De Leon AN, Dvorak RD, Kramer MP, Peterson R, Pinto DA, Leary AV, & Magri TD (2020). Daily patterns of emotional functioning on drinking and nondrinking days. Alcoholism, Clinical and Experimental Research, 44(12), 2598–2610. doi: 10.1111/acer.14480 [DOI] [PubMed] [Google Scholar]
- De Maeyer J, Vanderplasschen W, Camfield L, Vanheule S, Sabbe B, & Broekaert E (2011). A good quality of life under the influence of methadone: a qualitative study among opiate-dependent individuals. International Journal of Nursing Studies, 48(10), 1244–1257. doi: 10.1016/j.ijnurstu.2011.03.009 [DOI] [PubMed] [Google Scholar]
- Dixon MJ, Stange M, Larche CJ, Graydon C, Fugelsang JA, & Harrigan KA (2018). Dark flow, depression and multiline slot machine play. Journal of Gambling Studies, 34(1), 73–84. doi: 10.1007/sl0899-017-9695-l [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ehly S, & Reimers TM (1986). Perceptions of job satisfaction, job stability, and quality of professional life among rural and urban school psychologists. Psychology in the Schools, 23(2), 164–170. doi: 10.1002/1520-6807(198604)23:2<164::AID-PITS2310230209>3.0.CO;2-Z [DOI] [Google Scholar]
- Engeser S, & Rheinberg F (2008). Flow, performance and moderators of challenge-skill balance. Motivation and Emotion, 32(3), 158–172. doi: 10.1007/sll031-008-9102-4 [DOI] [Google Scholar]
- Epstein DH, & Preston KL (2012). TGI Monday?: drug-dependent outpatients report lower stress and more happiness at work than elsewhere. The American Journal on Addictions, 21(3), 189–198. doi: 10.1111/j.1521-0391.2012.00230.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epstein DH, Willner-Reid J, Vahabzadeh M, Mezghanni M, Lin JL, & Preston KL (2009). Real-time electronic diary reports of cue exposure and mood in the hours before cocaine and heroin craving and use. Archives of General Psychiatry, 66(1), 88–94. doi: 10.1001/archgenpsychiatry.2008.509 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ertin E, Sugavanam N, Holtyn AF, Preston KL, Bertz JW, Marsch LA, McLeman B, Shmueli-Blumberg D, Collins J, King JS, McCormack J, & Ghitza UE (2021). An examination of the feasibility of detecting cocaine use using smartwatches. Frontiers in Psychiatry, 12, 674691. doi: 10.3389/fpsyt.2021.674691 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gellis ZD, Kim J, & Hwang SC (2004). New York State case manager survey: Urban and rural differences in job activities, job stress, and job satisfaction. The Journal of Behavioral Health Services & Research, 31(4), 430–440. doi: 10.1007/BF02287694 [DOI] [PubMed] [Google Scholar]
- Ginexi EM, Howe GW, & Caplan RD (2000). Depression and control beliefs in relation to reemployment: What are the directions of effect? Journal of Occupational Health Psychology, 5(3), 323–336. doi: 10.1037/1076-8998.5.3.323 [DOI] [PubMed] [Google Scholar]
- Gold J, & Ciorciari J (2019). A transcranial stimulation intervention to support flow state induction. Frontiers in Human Neuroscience, 13, 274. doi: 10.3389/fnhum.2019.00274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henkel D (2011). Unemployment and substance use: A review of the literature (1990-2010). Current Drug Abuse Reviews, 4(1), 4–27. 10.2174/1874473711104010004 [DOI] [PubMed] [Google Scholar]
- Holtyn AF, Toegel F, Subramaniam S, Jarvis BP, Leoutsakos JM, Fingerhood M, & Silverman K (2020). Abstinence-contingent wage supplements to promote drug abstinence and employment: a randomised controlled trial. Journal of Epidemiology and Community Health, 74(5), 445–452. doi: 10.1136/jech-2020-213761 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holtyn AF, & Silverman K (2016). Effects of pay resets following drug use on attendance and hours worked in a therapeutic workplace. Journal of Applied Behavior Analysis, 49(2), 377–382. doi: 10.1002/jaba.298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hout MC, Papesh MH, & Goldinger SD (2013). Multidimensional scaling. Wiley Interdisciplinary Reviews. Cognitive Science, 4(1), 93–103. doi: 10.1002/wcs.1203 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang DY, Evans E, Hara M, Weiss RE, & Hser YI (2011). Employment trajectories: Exploring gender differences and impacts of drug use. Journal of Vocational Behavior, 79(1), 277–289. doi: 10.1016/j.jvb.2010.12.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hull DC, Williams GA, & Griffiths MD (2013). Video game characteristics, happiness and flow as predictors of addiction among video game players: A pilot study. Journal of Behavioral Addictions, 2(3), 145–152. doi: 10.1556/JBA.2.2013.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson SA, Thomas PR, Marsh HW, and Smethurst CJ (2001). Relationships between flow, self-concept, psychological skills, and performance. Journal of Applied Sport Psychology, 13(2), 129–153. doi: 10.1080/104132001753149865 [DOI] [Google Scholar]
- Kessler RC, Turner JB, & House JS (1989). Unemployment, reemployment, and emotional functioning in a community sample. American Sociological Review, 54(4), 648–657. doi: 10.2307/2095885 [DOI] [Google Scholar]
- Kidorf M, Hollander JR, King VL, & Brooner RK (1998). Increasing employment of opioid dependent outpatients: An intensive behavioral intervention. Drug and Alcohol Dependence, 50(1), 73–80. doi: 10.1016/s0376-8716(98)00005-2 [DOI] [PubMed] [Google Scholar]
- Kidorf M, Neufeld K, & Brooner RK (2004). Combining stepped-care approaches with behavioral reinforcement to motivate employment in opioid-dependent outpatients. Substance use & Misuse, 39(13-14), 2215–2238. doi: 10.1081/ja-200034591 [DOI] [PubMed] [Google Scholar]
- Killingsworth MA, & Gilbert DT (2010). A wandering mind is an unhappy mind. Science, 330(6006), 932. doi: 10.1126/science.1192439 [DOI] [PubMed] [Google Scholar]
- Kirchler E (1985). Job loss and mood. Journal of Economic Psychology, 6(1), 9–25. doi: 10.1016/0167-4870(85)90003-0 [DOI] [Google Scholar]
- Kowalczyk WJ, Bertz JW, Moran LM, Phillips KA, Ghitza UE, Epstein DH, & Preston KL (2017). Clonidine increases the likelihood that abstinence can withstand unstructured time in buprenorphine-maintained outpatients. Journal of Addiction Medicine, 11(6), 454–460. doi: 10.1097/ADM.0000000000000345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lenth RV (2021). emmeans: Estimated Marginal Means, aka Least-Squares Means. https://CRAN.R-project.org/package=emmeans. Accessed 11/21/2021.
- Lorah J (2018). Effect size measures for multilevel models: Definition, interpretation, and TIMSS example. Large-scale Assessments in Education, 6, 8. doi: 10.1186/s40536-018-0061-2. [DOI] [Google Scholar]
- Magura S, & Marshall T (2020). The effectiveness of interventions intended to improve employment outcomes for persons with substance use disorder: An updated systematic review. Substance Use & Misuse, 55(13), 2230–2236. doi: 10.1080/10826084.2020.1797810 [DOI] [PubMed] [Google Scholar]
- Magura S, Staines GL, Blankertz L, & Madison EM (2004). The effectiveness of vocational services for substance users in treatment. Substance Use & Misuse, 39(13-14), 2165–2213. doi: 10.1081/ja-200034589 [DOI] [PubMed] [Google Scholar]
- Marin MM, & Bhattacharya J (2013). Getting into the musical zone: trait emotional intelligence and amount of practice predict flow in pianists. Frontiers in Psychology, 4, 853. doi: 10.3389/fpsyg.2013.00853 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKay JR, Franklin TR, Patapis N, & Lynch KG (2006). Conceptual, methodological, and analytical issues in the study of relapse. Clinical Psychology Review, 26(2), 109–127. doi: 10.1016/j.cpr.2005.11.002 [DOI] [PubMed] [Google Scholar]
- Meggs J, & Chen M (2021). The effect of a brief-mindfulness intervention on psychophysiological exertion and flow-state among sedentary adults. Perceptual and Motor Skills, 128(3), 1078–1090. doi: 10.1177/0031512520984422 [DOI] [PubMed] [Google Scholar]
- Monaghan M, & Wincup E (2013). Work and the journey to recovery: Exploring the implications of welfare reform for methadone maintenance clients. The International Journal on Drug Policy, 24(6), e81–e86. doi: 10.1016/j.drugpo.2013.08.006 [DOI] [PubMed] [Google Scholar]
- Monfort SS, Howe GW, Nettles CD, & Weihs KL (2015). A longitudinal examination of re-employment quality on internalizing symptoms and job-search intentions. Journal of Occupational Health Psychology, 20(1), 50–61. doi: 10.1037/a0037753 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulia N, Zemore SE, Murphy R, Liu H, & Catalano R (2014). Economic loss and alcohol consumption and problems during the 2008 to 2009 U.S. recession. Alcoholism, Clinical and Experimental Research, 38(4), 1026–1034. doi: 10.1111/acer.12301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nagelhout GE, Hummel K, de Goeij M, de Vries H, Kaner E, & Lemmens P (2017). How economic recessions and unemployment affect illegal drug use: A systematic realist literature review. International Journal on Drug Policy, 44, 69–83. doi: 10.1016/j.drugpo.2017.03.013 [DOI] [PubMed] [Google Scholar]
- Nakamura J, & Csikszentmihalyi M (2009). Flow theory and research. In Lopez SJ & Snyder CR (Eds.), Oxford Handbook of Positive Psychology (pp. 195–206). Oxford University Press: New York. [Google Scholar]
- Nielsen K, & Cleal B (2010). Predicting flow at work: investigating the activities and job characteristics that predict flow states at work. Journal of Occupational Health Psychology, 15(2), 180–190. doi: 10.1037/a0018893 [DOI] [PubMed] [Google Scholar]
- Notley C, Blyth A, Maskrey V, Pinto H, & Holland R (2015). Exploring the concepts of abstinence and recovery through the experiences of long-term opiate substitution clients. Substance Abuse, 36(2), 232–239. doi: 10.1080/08897077.2014.941085 [DOI] [PubMed] [Google Scholar]
- Panlilio LV, Stull SW, Kowalczyk WJ, Phillips KA, Schroeder JR, Bertz JW, Vahabzadeh M, Lin JL, Mezghanni M, Nunes EV, Epstein DH, & Preston KL (2019). Stress, craving and mood as predictors of early dropout from opioid agonist therapy. Drug and Alcohol Dependence, 202, 200–208. doi: 10.1016/j.drugalcdep.2019.05.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Partington S, Partington E, & Olivier S (2009). The dark side of flow: A qualitative study of dependence in big wave surfing. The Sport Psychologist, 23(2), 170–185. doi: 10.1123/tsp.23.2.170 [DOI] [Google Scholar]
- Petry NM, Andrade LF, Rash CJ, & Cherniack MG (2014). Engaging in job related activities is associated with reductions in employment problems and improvements in quality of life in substance abusing patients. Psychology of Addictive Behaviors, 28(1), 268–275. 10.1037/a0032264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Platt JJ (1995). Vocational rehabilitation of drug abusers. Psychological Bulletin, 117(3), 416–433. doi: 10.1037/0033-2909.117.3.416 [DOI] [PubMed] [Google Scholar]
- Proctor SL, Copeland AL, Kopak AM, Hoffmann NG, Herschman PL, & Polukhina N (2015). Predictors of patient retention in methadone maintenance treatment. Psychology of Addictive Behaviors, 29(4), 906–917. doi: 10.1037/adb0000090 [DOI] [PubMed] [Google Scholar]
- R Core Team. (2018). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. [Google Scholar]
- Rabinowitz GB (1975) An introduction to nonmetric multidimensional scaling. American Journal of Political Science, 19(2), 343–390. [Google Scholar]
- Rau PL, Peng SY, & Yang CC (2006). Time distortion for expert and novice online game players. CyberPsychology & Behavior, 9(4), 396–403. doi: 10.1089/cpb.2006.9.396 [DOI] [PubMed] [Google Scholar]
- Reid D (2011). Mindfulness and flow in occupational engagement: presence in doing. Canadian journal of occupational therapy. Revue canadienne d’ergotherapie, 78(1), 50–56. doi: 10.2182/cjot.2011.78.1.7 [DOI] [PubMed] [Google Scholar]
- Remington NA, Fabrigar LR, & Visser PS (2000). Reexamining the circumplex model of affect. Journal of Personality and Social Psychology, 79(2), 286–300. doi: 10.1037/0022-3514.79.2.286 [DOI] [PubMed] [Google Scholar]
- Rights JD, & Cole DA (2018). Effect size measures for multilevel models in clinical child and adolescent research: New R-squared methods and recommendations. Journal of Clinical Child and Adolescent Psychology, 47(6), 863–873. doi: 10.1080/15374416.2018.1528550. [DOI] [PubMed] [Google Scholar]
- Rodríguez-Sánchez AM, Schaufeli W, Salanova M, Cifre E, and Sonnenschein M (2011). Enjoyment and absorption: An electronic diary study on daily flow patterns. Work and Stress, 25(1), 75–92. doi: 10.1080/02678373.2011.565619 [DOI] [Google Scholar]
- Rosnow RL, Robert R, & Rubin DB (2000). Contrasts and correlations in effect-size estimation. Psychological Science, 11(6), 446–453. doi: 10.1111/1467-9280.00287. [DOI] [PubMed] [Google Scholar]
- Russell JA. (1980). A circumplex model of affect. Journal of Personality and Social Psychology, 39(6), 1161–1178. doi: 10.1037/h0077714 [DOI] [Google Scholar]
- Shiffman S, & Waters AJ (2004). Negative affect and smoking lapses: a prospective analysis Journal of Consulting and Clinical Psychology, 72(2), 192–201. doi: 10.1037/0022-006X.72.2.192 [DOI] [PubMed] [Google Scholar]
- Silverman K, Holtyn AF, & Morrison R (2016). The therapeutic utility of employment in treating drug addiction: Science to application. Translational Issues in Psychological Science, 2(2), 203–212. doi: 10.1037/tps0000061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silverman K, Holtyn AF, & Subramaniam S (2018). Behavior analysts in the war on poverty: Developing an operant antipoverty program. Experimental and Clinical Psychopharmacology, 26(6), 515–524. doi: 10.1037/pha0000230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steptoe A, Wardle J, & Marmot M (2005). Positive affect and health-related neuroendocrine, cardiovascular, and inflammatory processes. Proceedings of the National Academy of Sciences of the United States of America, 102(18), 6508–6512. doi: 10.1073/pnas.0409174102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toegel F, Holtyn AF, Subramaniam S, & Silverman K (2020). Effects of time-based administration of abstinence reinforcement targeting opiate and cocaine use. Journal of Applied Behavior Analysis, 52(3), 1726–1741. doi: 10.1002/jaba.702 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Venables WN & Ripley BD (2002). Modern Applied Statistics with S, Fourth edition. Springer, New York. ISBN 0-387-95457-0, https://www.stats.ox.ac.uk/pub/MASS4/. [Google Scholar]
- Waldorf D, Reinarman C, & Murphy S (1991). Cocaine Changes: The Experience of Using and Quitting. Temple University Press, Philadelphia, PA. [Google Scholar]
- Wan CS, & Chiou WB (2006). Psychological motives and online games addiction: a test of flow theory and humanistic needs theory for Taiwanese adolescents. Cyber Psychology & Behavior, 9(3), 317–324. doi: 10.1089/cpb.2006.9.317 [DOI] [PubMed] [Google Scholar]
- Wanberg CR (1995). A longitudinal study of the effects of unemployment and the quality of re-employment. Journal of Vocational Behavior, 46(1), 40–54. doi: 10.1006/jvbe.1995.1003 [DOI] [Google Scholar]
- Wang L-C, & Chen M-P (2011). Effects of type of learning approach on novices’ motivation, flow, and performance in game-based learning. In: Chang M, Hwang W-Y, Chen M-P, & Müller W (Eds.) Edutainment Technologies. Educational Games and Virtual Reality Augmented Reality Applications. 6th International Conference on E-learning and Games, Edutainment 2011, Taipei, Taiwan, September 7-9, 2011. Proceedings. Berlin: Springer. p. 238. [Google Scholar]
- Waters L (2007). Experiential differences between voluntary and involuntary job redundancy on depression, job-search activity, affective employee outcomes and re-employment quality. Journal of Occupational and Organizational Psychology, 80(2), 279–299. doi: 10.1348/096317906X104004 [DOI] [Google Scholar]
- Wei L, & Lachin JM (1988). Properties of the urn randomization in clinical trials. Controlled Clinical Trials, 9(4), 345–364. doi: 10.1016/0197-2456(88)90048-7 [DOI] [PubMed] [Google Scholar]
- Wong CJ, & Silverman K (2007). Establishing and maintaining job skills and professional behaviors in chronically unemployed drug abusers. Substance Use & Misuse, 42(7), 1127–1140. doi: 10.1080/10826080701407952erences [DOI] [PubMed] [Google Scholar]
- Zhou Y, Zou M, Woods SA, & Wu C-H (2019). The restorative effect of work after unemployment: An intraindividual analysis of subjective well-being recovery through reemployment. Journal of Applied Psychology, 104(9), 1195–1206. doi: 10.1037/apl0000393 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.