

Abstract
Purpose
This study aimed to describe the demographic and clinical characteristics of individuals involved in electric scooter (E-scooter) accidents and the factors associated with these incidents.
Methods
We conducted a prospective observational study of individuals involved in E-scooter accidents admitted to the emergency department of Saint-Pierre Hospital. The highest abbreviated injury score above or equal to two classified the injury as significant. Injuries during working hours were compared to those during off-working hours.
Results
During the study period from June 1, 2019, to June 30, 2020, 170 individuals were admitted to the emergency department following an E-scooter accident. In 73.5% of the accidents, rented E-scooters were involved. Of the patients, 68.2% were male, 6.4% wore helmets, and 30% were under the influence of alcohol. Upper limb and cranial injuries were more frequently severe (abbreviated injury score ≥ 2) than other injuries (p < 0.05). Accidents during off-working hours were significantly related to alcohol consumption (p < 0.001), non-usage of helmets (p < 0.01), head and neck injuries (p < 0.01), and rented E-scooters (p < 0.01). Alcohol consumption was itself associated with the non-usage of helmets (p < 0.05) and major head and neck injuries (p < 0.001).
Conclusion
Given the increasing popularity of E-scooters as an alternative mode of transportation, our study can inform public policy on patterns of injuries associated with E-scooter utilization for future injury prevention policies. Using helmets, avoiding alcohol consumption, and regulating use at night can improve outcomes in E-scooter accidents.
Trial registration: ClinicalTrials.gov Identifier: NCT04778332.
Keywords: Electric scooter injury, Emergency medicine, E-scooters, Micro-mobility, Trauma
Introduction
Electric scooters (E-scooters) are becoming increasingly used worldwide as an alternative to major modes of transportation. A report from Berg insight recently forecasted that by 2024, 4.6 million E-scooters would be in use worldwide, nearly a 600% increase from 2019 [1]. E-scooters were first introduced to the market by several private companies in 2018. In 2020, the combined fleet of the three major E-scooter companies accounted for 3200–4800 active E-scooters in Brussels [2].
Alongside their many benefits, there are significant risks of accidents and traumatic injuries associated with E-scooters, both for the rider and other road users [3]. Several studies have reported an increased rate of E-scooter trauma worldwide [3–14]. In Salt Lake City, USA, a trauma center saw a 625% increase in E-scooter-related trauma after launching an E-scooter share program [6]. An ED in Singapore reported a 230% increase in cases from 2015 to 2016 [11].
Countries worldwide are investigating how to handle this new mode of transportation by creating a legal framework or by outright banning the use of E-scooters on public roads. In 2019, Singapore and France prohibited their use on public sidewalks, and the UK prohibited their use on public roads until further evaluation [15].
Since May 31, 2019, regulations on E-scooters have been incorporated into the Belgian traffic code, giving riders the right to drive on the sidewalk at a walking pace (6 km/h) or on public roads at a higher speed (with a maximum set at 25 km/h) [16]. Very little is known about the risk factors and outcomes of E-scooter accidents. Therefore, we aimed to analyze the demographics and clinical characteristics of individuals involved in these events. Moreover, we sought to find the factors associated with these incidents. Our study is distinctive as it analyzes the characteristics of significant injuries with leisure usage.
Materials and methods
Saint-Pierre University hospital is a tertiary-care hospital that serves the city center of Brussels, the night life center with a large pedestrian zone; 14 other emergency departments are present in the Brussels Region.
Study design and patients
We conducted a prospective observational study, which included individuals > 16 years involved in E-scooter accidents, admitted to the adult ED at the Saint-Pierre Hospital (Brussels) between June 1, 2019, and June 30, 2020.
Data on usage, lesion types, and injury outcomes were collected through a standardized form upon admission to the ED. The data collected included (1) the time and date of the accident; (2) delay of presentation at the hospital since the accident; (3) mechanism of the accident; (4) use of a protective helmet; (5) consumption of alcohol before the accident; (6) mode of arrival at the emergency room (spontaneous or by ambulance); (7) injury assessment and use of imaging; (8) treatments; (9) hospital admission; and (10) temporary work interruption.
Working hours were defined as 7 am until 6 pm, evening as 6 pm until 11 pm, and nighttime as 11 pm until 7 am.
Injury evaluation
A specialist in traumatology scored each patient’s injury on the Abbreviated Injury Scale (AIS) [17], and a second researcher validated his scoring process. AIS classifies each injury by body region on a 6-point scale, with 1 indicating minor injury; 2, moderate injury; 3, serious injury up to 6 indicating a virtually non-survivable injury. A “major injury” was defined as the highest rating of the injuries suffered by the patient on the AIS scale that is ≥ 2.
Statistical analysis
Statistical Package for the Social Sciences version 24 was used for all statistical analyses. Values are reported as mean ± standard deviation (SD) for continuous normally distributed variables and used medians and 95% confidence interval (CI) for continuous non-Gaussian ones. For discrete variables, we reported numbers and percentages. The Chi-square test and Fisher’s exact test (when necessary) were used to assess the association between discrete variables. A stepwise logistic regression model was constructed to evaluate the independent contribution of covariates to accidents during working and off-working hours. Statistical significance was set at a two-sided 5% level of significance.
Results
Data from 170 patients were collected between June 1, 2019, and June 30, 2020. Patients’ demographics and accident characteristics are summarized in (Table 1). The median age was 29.5 years (95% CI: 24–40) (Fig. 1). In total, 68.2% (116/170) of the patients were male; 42.6% of the patients (72/169) were admitted during working hours (7 am to 6 pm), 27.2% (46/169) during the evening (6 pm–11 pm), and 30.2% (51/169) during nighttime (11 pm–7 am) (Fig. 2).
Table 1.
Description of cohort: patient and accident characteristics associated with e-scooters
| Characteristics | N = 170 | 95% CI | Mean | Median | Std deviation |
|---|---|---|---|---|---|
| Gender (man) | 116 (68.2%) | 60.4–74.6 | |||
| Age* | 32.33 | 29.48 (95% CI: 24.15–40.0) | 11.134 | ||
| Hour of admission* | |||||
| 7am–6 pm | 72 (42.6%) | 35.5–50.3 | |||
| 6 pm–11 pm | 46 (27.2%) | 20.1–34.9 | |||
| 11 pm–7am | 51 (30.2%) | 23.1–37.3 | |||
| Rented | 125 (73.5%) | 66.9–80.5 | |||
| Arrived by ambulance | 68 (40.0%) | 32.5–46.7% | |||
| Helmet usage | 11 (6.4%) | 3.0–10.1 | |||
| Alcohol consumption | 51 (30.0%) | 23.7–37.9 | |||
| Mechanism of the accident** | |||||
| Loss of balance | 142 (84.5%) | 77.5–88.8 | |||
| Two drivers on the e-scooter | 11 (6.5%) | 3.0–11.0 | |||
| Pedestrians hit by the e-scooter | 7 (4.1%) | 1.2–7.7 | |||
| Accident with another vehicle | 9 (5.3%) | 2.4–8.9 | |||
| Scanner in ER | 24 (14.1%) | 8.9–19.5 | |||
| ICU | 1 (< 1%) | ||||
| Temporary incapacity for work | 71 (41.7%, 1193 days in total) | 16.8 | 7.0 (95% CI: 3–21) | 20.08 | |
| Hospitalization | 20 (11.7%) | 7.1–16.5 | |||
*1 patient with missing data
**2 patients with missing data
Fig. 1.
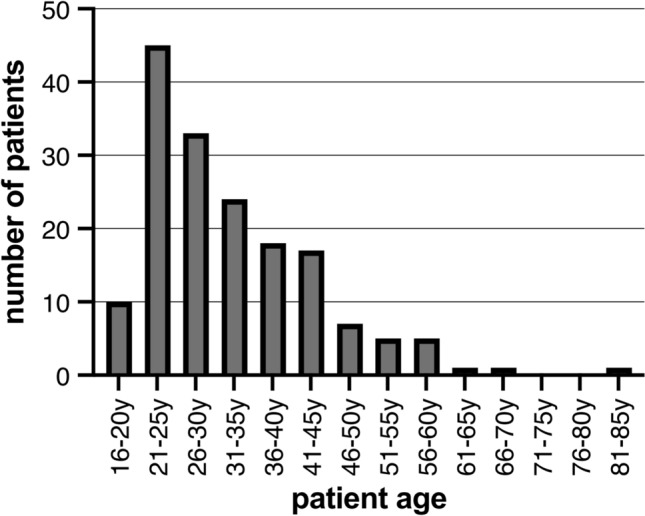
Age distribution
Fig. 2.
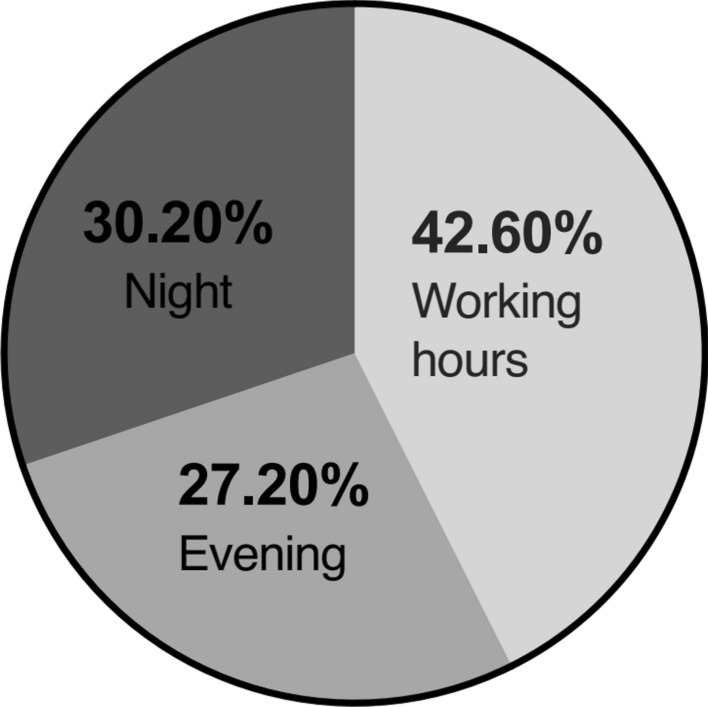
Distributions of admissions based on time periods
In 73.5% of the accidents (125/170), rented E-scooters were implied, and 40.0% (68/170) of the accident victims arrived at the hospital using an ambulance service. Among our study population, only 6.4% (11/170) were equipped with a protective helmet, and 30.0% (51/170) testified they were under the influence of alcohol. In 84.5% (142/168) of the accidents, the driver fell on their own. In 6.5% of the cases (11/168), there was inappropriate use of the E-scooter (i.e., two users on the same scooter), and in 4.1% of the cases (7/168), pedestrians were the victims of the accident. In 5.3% (9/168) of the cases, accidents occurred with another vehicle. In 24 patients (14.1%), a computed tomography scan was necessary to complete the work-up. Twenty patients were admitted to the hospital (11.7%), and one patient (< 1%) had to be monitored in the ICU. Seventy-one patients (41.7%) had temporary incapacity to work, and the median of these periods was 7.0 days (95% CI 3–21) (Table 1).
The limbs were affected in 60.6% of the patients (103/170), with a predominance of the upper limbs in 56.3% (58/103) compared to the lower limbs 51.4% (53/103). Both the upper and lower limbs were affected in 7.7% (8/103) of the patients. The head and neck were involved in 45.9% (78/170) of the patients. Within this population, 25.6% (20/78) had cranial trauma, and 87.2% (68/78) had a maxillofacial injury. Contusions and abrasions were present in 37.1% of the patients (63/170), while 26.5% presented with fractures (45/170). Fractures were more frequent in the upper limbs (44.4%; 20/45), followed by head and neck (31.1%; 14/45), lower limbs (28.9%; 13/45), and thoracic rib fractures (6.7%; 3/45). Multiple fractures were found in 11.1% (5/45) of the patients. Wounds requiring suturing were present in 32.9% of the patients (56/170), of which the majority (82.1%; 46/56 cases) were in the head and neck region. Sprains were present in 9.4% (16/170) of the patients. There were 4.7% of patients with limb dislocation (8/170), seven of which were in the upper limbs, while one had a maxillofacial dislocation. Within the study population, 13.5% (23/170) required surgery, of which 39.1% (9/23) were in the head and neck region, and the other 16 were in the upper and lower limbs (69.6%) (Table 2).
Table 2.
Traumatic injury description
| Characteristics | Number % of the total | Number (%) in the subgroup | Total subgroup |
|---|---|---|---|
| Region of the body | |||
| Limbs | 103/170 (60.6%) | ||
| Upper limb | 34.1% | 58 (56.3%) | 103 |
| Lower limb | 31.2% | 53 (51.4%) | 103 |
| Both limbs | 8 (7.7%) | 103 | |
| Thorax | 9 (5.3%) | ||
| Head and neck | 78/170 (45.9%) | ||
| Cranial trauma | 11.8% | 20 (25.6%) | 78 |
| Maxilofacial trauma | 40.0% | 68 (87.2%) | 78 |
| Contusions and abrasions | 63/170 (37.1%) | ||
| Upper limb | 29 (46.0%) | 63 | |
| Lower limb | 24 (38.1%) | 63 | |
| Thorax | 6 (9.5%) | 63 | |
| Head and neck injuries | 29 (46.0%) | 63 | |
| Fractures | 45/170 (26.5%) | ||
| Upper limb | 20 (44.4%) | 45 | |
| Lower limb | 13 (28.9%) | 45 | |
| Thorax | 3 (6.7%) | 45 | |
| Head and neck | 14 (31.1%) | 45 | |
| Multiple fractures | 5 (11.1%) | 45 | |
| Sutures | 56/170 (32.9%) | ||
| Upper limb | 7 (12.5%) | 56 | |
| Lower limb | 11 (19.6%) | 56 | |
| Head and neck | 46 (82.1%) | 56 | |
| Sprain | 16/170 (9.4%) | ||
| Dislocation | 8/170 (4.7%) | ||
| Upper limb | 7 (87.5%) | ||
| Lower limb | 1 (12.5%) | ||
| Head and neck | 1 (12.5%) | ||
| Surgery | 23/170 (13.5%) | ||
| Upper limb | 8 (34.8%) | 23 | |
| Lower limb | 8 (34.8%) | 23 | |
| Thorax | 0 (0.0%) | 23 | |
| Head and neck | 9 (39.1%) | 23 | |
We found that the non-usage of helmets was associated with an increased risk of cranial trauma (p = 0.036) but not with maxillofacial trauma (p = 0.203) (Table 3a).
Table 3.
Risk factors and outcomes by personal and trip characteristics
| (a) Helmet usage | Use of helmet N = 11 (6.5%) | No helmet N = 159 (93.5%) | |
|---|---|---|---|
| Head and neck injuries | 2 (18.2%) | 76 (47.8%) | Fisher’s exact test p = 0.067 |
| Cranial trauma | 0 (0.0%) | 20 (12.6%) | Fisher’s exact test p = 0.036 |
| Maxillofacial trauma | 2 (18.2%) | 66 (41.5%) | Fisher’s exact test p = 0.203 |
| (b) Age groups | Age < 25 years N = 43 (25.6%) | Age ≥ 25 years N = 125 (74.4%) | |
|---|---|---|---|
| Off-working hours | 31 (72.1%) | 65 (52.0%) | p = 0.022 |
| AIS ≥ 2 | 9 (20.9%) | 50 (40.0%) | p = 0.024 |
| Alcohol consumption | 17 (39.5%) | 34 (27.2%) | p = 0.130 |
| (c) Major injuries | AIS ≥ 2 N = 60 (35.3%) | AIS < 2 N = 110 (64.7%) | p Value |
|---|---|---|---|
| Patients and driving conditions | |||
| Helmet | 4 (6.7%) | 7 (6.4%) | p = 1.000 fisher’s exact test |
| Alcohol | 21 (35.0%) | 30 (27.3%) | p = 0.293 |
| Rented | 47 (78.3%) | 78 (70.9%) | p = 0.294 |
| Gender | |||
| Male N = 116 | 43 (37.1%) | 73 (62.9%) | p = 0.478 |
| Woman N = 54 | 17 (31.5%) | 37 (68.5%) | |
| Ambulance | 33 (55.0%) | 35 (31.8%) | p = 0,003** |
| Upper limbs | 28 (46.7%) | 30 (27.3%) | p = 0.011* |
| Lower limbs | 16 (26.7%) | 37 (33.6%) | p = 0.348 |
| Head and neck injuries | 26 (43.3%) | 52 (47.3%) | p = 0.622 |
| Cranial trauma | 11 (18.3%) | 9 (8.2%) | p < 0.05* |
| Maxilla-facial trauma | 22 (36.7%) | 46 (41.8%) | p = 0.512 |
| (d) Alcohol consumption | Alcohol consumption N = 51 (30.0%) | No alcohol consumption N = 119 (70.0%) | p Value |
|---|---|---|---|
| Helmet | 0 (0.0%) | 11 (9.2%) | p = 0.025 Fisher’s exact test |
| Head and neck injuries | 39 (76.5%) | 39 (32.8) | p < 0.001*** |
| Significant head and neck injuries AIS ≥ 2 | 13 (25.5%) | 10 (8.4%) | p < 0.001*** |
| Rented | 44 (86.3%) | 81 (68.1%) | p = 0.014** |
| (e) Working hours | Working hours N = 73 (43.2%) | Off-working hours 97 (57.1%) | p Value |
|---|---|---|---|
| Helmet | 10 (13.7%) | 1 (1.0%) | p < 0,01** Fisher’s exact test |
| Alcohol | 9 (12.3%) | 42 (43.3%) | p < 0.001*** |
| Gender | |||
| Male N = 116 | 50 (43.1%) | 66 (56.9%) | p = 0.950 |
| Woman N = 54 | 23 (42.6%) | 31 (57.4%) | |
| Head and neck injuries | 25 (34.2%) | 53 (54.6%) | p = 0.008* |
| Head and neck injuries AIS ≥ 2 | 6 (8.2%) | 17 (17.5%) | p = 0.079 |
| AIS score ≥ 2 | 25 (34.2%) | 35 (36.1%) | p = 0,804 |
| Rented | 46 (63.0%) | 79 (81.4%) | p = 0.007** |
Patients under 25 years of age (Table 3b) were more frequently involved in accidents during off-working hours (p = 0.022). Patients above 25 years were associated with severe injuries (p = 0.024). Alcohol consumption did not significantly differ between the age groups (p = 0.130).
AIS ≥ 2 injuries (Table 3c) more frequently involved upper limb injuries (p = 0.011). We did not identify a significant association of AIS ≥ 2 injuries with helmet use, alcohol intoxication, utilization of rented E-scooters, gender, lower limb, or head and neck injury.
We observed an association between alcohol consumption and the non-usage of helmets (p = 0.025), presence of head and neck injuries (p < 0.001), significant head and neck injuries (p < 0.001), and utilization of rented E-scooters (p = 0.014) (Table 3d).
Helmet use was more frequently observed in accidents occurring during working hours (p < 0.01). Accidents during off-working hours occurred more frequently in association with alcohol consumption (p < 0.001), head and neck injuries (p = 0.008), and use of rented E-scooters (p = 0.007). There was no association between the severity of the injury and the time of the accident (p = 0.804) (Table 3e).
The multivariate forward stepwise logistic regression model for determining factors discriminating between accidents during working and off-working hours identified “usage of helmets” (Odds Ratio [OR], 0.100) and “alcohol consumption” (OR, 4.67) as independent variables associated with accidents during working hours (Table 4). Rented E-scooters, gender, and age were also considered, but were not retained in the analysis.
Table 4.
Risk factors for the occurrence of accidents during off-working hours (forward stepwise)
| Odds ratio | 95% CI | p | |
|---|---|---|---|
| Helmet | 0.10 | 0.12–0.809 | p = 0.031 |
| Alcohol | 4.67 | 2.07–10.54 | p < 0.001 |
Discussion
We found an association between age and time of accident occurrence and the increased frequency of younger drivers involved in accidents at night (72.1% versus 52.0% for older drivers). However, major injuries were associated with older patients (40.0% versus 20.9% for younger drivers). In a study by Cicchino et al., there was a trend, suggesting that severe lesions were more frequent in older drivers [13].
The gender distribution is comparable with other studies, with about two-thirds (69.4%) of the individuals being male [3, 4, 6, 7, 9, 10, 13, 14]. Rented E-scooters were more frequently involved in accidents than privately owned scooters. This could suggest the potential role of lack of driver experience in the occurrence of accidents. Accidents were more frequently observed after working hours. We observed an increased burden to the ED in terms of scanner usage (14.1%). This increase was in line with the observations from a recent retrospective study documenting [10] 477 radiological examinations of 192 victims of E-scooter accidents.
In our study, 73.5% of the accidents were associated with occasional users (rented E-scooters), and 57.4% occurred after work hours, in line with previous regional data [2]; The same data observed that occasional users used the E-scooters mainly for leisure instead of regular users who used the E-scooters for work and daily commute.
The majority of the accidents occurred without antagonists (83.5%). Our figures are higher than reported in other studies [11, 13]. In Brussels, there are many streets with cobblestones, which can explain the high number of accidents observed in our study where riders fell. Moreover, the absence of a dedicated pathway and quality of the road/sidewalk could increase accident risk. In our study, 6.5% of accidents occurred with more than one person on the E-scooter. Accidents with other motor vehicles or pedestrians were low, which is consistent with those reported in other studies [3, 10, 11]. Our hospital serves the center of Brussels, which is a pedestrian zone; we believe that this contributed to the low number of accidents with motor vehicles seen in our study.
We found that most fractures involved the upper limbs followed by the head and neck, lower limb, and then the ribs. The numbers seem to differ between the studies; upper limb and lower limb fractures are typically very close in percentage, and sometimes, accidents involving the lower limbs are more frequent [13]. The high rates of head and neck injuries combined with upper extremity injuries could suggest that drivers tried to break their fall before landing [14].
The proportion of patients wearing a helmet was low in our study, as in the majority of the studies. Trivedi et al. also reported 100 head injuries (40.2%), with only 4.4% of 249 patients wearing a helmet (6). In this study, the lack of helmet usage was observed in 94.3% of the riders. Although the use of protective headgear is strongly encouraged in Brussels, it is currently not mandated by law [15], and it was reported that only 16% of E-scooters users wear helmets regularly [10]. As reported in other studies, head injuries seem frequent, seen in 40% of the patients [1, 12, 16]. Helmet usage was associated with “working hours,” and head and neck trauma was associated with “off-working hours.” Therefore, we propose that the use of helmets is associated with lowering head trauma incidents and severity.
The severity analysis was aimed at understanding the characteristics of significant lesions. Upper limb injuries were associated with AIS ≥ 2 (p = 0.011). This is in accordance with a study done in Tel Aviv, which found that the spontaneous act of falling on an outstretched hand as protection from head injury led to radial head, distal radial, and scaphoid fractures as the most common fractures of the upper extremities [14].
Facial injuries are complicated and frequently involve multiple regions of the head. Isolated cranial traumas were associated with AIS ≥ 2 (p < 0.05); this could point to a dangerous mechanism of the accident where the loss of balance is combined with speed. There was no association between significant injuries (AIS ≥ 2) and the other risk factors (helmet usage, alcohol consumption, working hours, gender, and rental status). These findings are consistent with a recent study on severity conducted by Cicchino et al. [13], which found that E-scooters were a risk factor for severe injuries (AIS ≥ 2) and that the severity of injuries incurred by the riders may reflect higher travel speeds.
Our study showed that most accidents occurred after working hours. Similarly, in a study done in Germany by Störmann et al., peak E-scooter-related ED presentations were observed on weekends or during the late evening and night hours [4]. Accidents involving rented E-scooters were associated with higher rates of alcohol consumption which could be explained by the increased usage of E-scooters for leisure[2]. AIS ≥ 2 injuries were associated with higher rates of accidents after working hours in patients > 25 years, pointing to the leisure motive behind using a rented E-scooter. We suggest that after-work alcohol consumption combined with a lack of experience in maneuvering the vehicle might be the cause of most severe injuries.
The non-usage of helmets and alcohol consumption were found to be the independent variables discriminating between accidents occurring at night and during the day.
We observed that the injury pattern differed according to the accident’s timing. Individuals driving during the evening and nighttime sustained more maxillofacial and cranial injuries. These types of lesions are sometimes complicated and need to be addressed by a maxillofacial specialist. Moreover, although rarely a life-threatening issue, facial injuries can have significant functional or cosmetic consequences. In our study, higher consumption of alcohol after work hours and probable low visibility due to darkness could explain the change in the accident mechanism. We postulate that with alcohol consumption, there is an alteration in the capacity to protect the head [18].
To get more insight into E-scooter injuries, we analyzed alcohol consumption. In our survey, 30% of the patients testified they were under the influence of alcohol. Current literature demonstrates a high rate of intoxicated patients, ranging from 17.8% to 36.6% in different studies [3, 6–8, 13, 19]. Our figures are high compared to the current literature, and we attribute this to our hospital's location in the center of Brussels, near the nightlife district. Another interesting detail was that 12% of the accidents during working hours took place under the influence of alcohol. We observed a clear association between alcohol intoxication and failure to wear a helmet as none of the intoxicated patients were wearing helmets in our study. Significant head and neck injuries were also associated with alcohol consumption. These traumas are considered dangerous and severe. We hypothesize that alcohol consumption alters the spontaneous reflex of falling on an outstretched hand as protection from head injury. From these findings, we suggest an explanation to the increase in significant head and neck injuries while under the influence of alcohol. In our study, older patients sustained more severe injuries. We hypothesize that alcohol consumption shifts the older population toward riskier behaviors exposing them to more severe injuries. On the other hand, younger patients have better postural stability and shorter reaction times than older patients, which could mitigate the severity of an accidental fall [20].
The consumption of alcohol was associated with rented E-scooters; this points to the occasional risk riders expose themselves compared to owners and regular users. A recent retrospective study published in February 2021 in New Zealand compared E-scooters to other forms of transport. E-scooter drivers presented a significant difference in blood ethanol levels, mechanism of injury (isolated falls), time of injury (between 5 pm and 8 am), and protective gear use [19].
Despite pictograms that suggest the use of helmets and one driver usage, users do not receive clear explanations for the safe usage of E-scooters. Law enforcement is minimal and does not differentiate between other modes of micro-transportation (bicycles, small mopeds, etc.). A study performed by McGuinness et al. [19] demonstrated concerningly high E-scooter-related hospitalization rates and suggests that E-scooters are currently not as safe as cycles.
In particular, our study concerns the number of accidents per month (Fig. 3). After March 2020, we saw a decrease in accidents connected to the COVID-19 pandemic, which began on March 13, 2020. During this period, two of the major companies announced that they would temporarily pull their electric sharing bikes and scooters from the streets in light of the coronavirus pandemic [21].
Fig. 3.
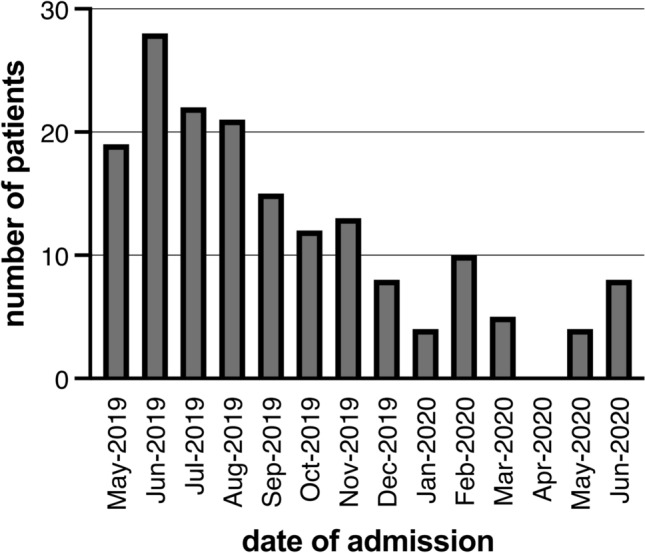
Distribution of accidents by month
Our study employed a prospective study design. Data collection was limited to what was gathered from the patients at the time of the accident.
In the absence of selection bias, observational studies have the advantage of reflecting real-world practice and are less stringent in their inclusion criteria than randomized clinical trials. Although these studies cannot conclude with certainty that there is a causal link between an event and an exposure, they provide an estimate of their association [22].
Limitations
Only patients > 16 years old were included. Our emergency and trauma center also contains a pediatric trauma ward, but patients < 16 were not included in this study. A study in Israel found that 33% of the total casualties were reported in children aged 0–14 years. In comparison, pedestrians < 16 years hit by E-scooters accounted for 42% (the casualties from the electric bike and motorized scooter road accidents, Siman Tov et al. [18]. A future study should also include the pediatric population.
There are two hospitals in the center of Brussels and 12 in other regions of Brussels. In Belgium, road accidents wherein a patient needs referrals by ambulance generally are transported to the ED nearby. Self-referrals patients’ numbers are unknown (ED and general practitioners). Although Saint-Pierre is the main hospital where trauma injury patients are referred to in central Brussels, some other centers could be included in future study.
The pandemic represents a possible bias in our study as it was associated with a swift change in the pattern of use of E-scooters with shared E-scooters being withdrawn from the market and a rapid surge of privately owned ones. Although a significant number of trials (mainly due to difficulties in recruiting) during the pandemic were stopped, the decision to continue the study was taken in light of the increase of usage of all micromobility vehicles and sustained recruitment. We suppose that the actual numbers of patients under the influence of alcohol were higher than testified. We did not include blood tests in the collection of data which could have yielded higher numbers. A study by Cermonte and Cherpitel estimated the risk of injury after acute alcohol consumption. They compared two methods of collection of data—self-reported drinking prior to the event and blood alcohol concentration. Higher risks of accidents were found when blood alcohol concentration was used as a measure of consumption [23].
Conclusion
Strategies to improve the safety of E-scooters are recommended, and we suggest the inclusion of alcohol restrictions, since the head and major upper limb injuries have been associated with its consumption. Mandatory helmet usage, limited periods of use in rented E-scooters, and education on proper use should be considered. Users should be aware of the risks associated with alcohol consumption and nighttime use. Our study can inform public policy for future prevention of severe injuries.
Acknowledgements
The authors wish to thank Antoine PLUMACKER for contributing to the statistical analysis.
Authors’ contribution
All authors contributed to the study's conception and design. Material preparation, data collection, and analysis were performed by Eyal Gan-El, Maarten Ulrix (assistant research), and Pierre Youatou Towo. Eyal Gan-El wrote the first draft of the manuscript, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Ethics approval
The study was approved by the local Ethics committee of the Saint-Pierre Hospital (Brussels) and has been registered in ClinicalTrials.gov (NCT04778332).
Informed consent
Informed consent was obtained from all individual participants included in the study.
References
- 1.Martin S. The Bike and Scootersharing Telematics Market 2nd Edition. 2020. In: Berg Insight AB (ed.) Berg Insight AB?, Viktoriagatan 3, SE-411 25 Gothenburg, Sweden. https://media.berginsight.com/2021/02/07193526/bi-micromobilitytelematics2-ps.pdf
- 2.SPRB – Bruxelles Mobilité. Enquête sur l’usage des trottinettes électriques à Bruxelles. 2019.
- 3.Beck S, Barker L, Chan A, Stanbridge S. Emergency department impact following the introduction of an electric scooter sharing service. Emerg Med Australas. 2020;32:409–415. doi: 10.1111/1742-6723.13419. [DOI] [PubMed] [Google Scholar]
- 4.Störmann P, Klug A, Nau C, Verboket RD, Leiblein M, Müller D, Schweigkofler U, Hoffmann R, Marzi I, Lustenberger T. Characteristics and injury patterns in electric-scooter related accidents-a prospective two-center report from Germany. J Clin Med. 2020;9:1569. doi: 10.3390/jcm9051569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Trivedi B, Kesterke MJ, Bhattacharjee R, Weber W, Mynar K, Reddy LV. Craniofacial injuries seen with the introduction of bicycle-share electric scooters in an urban setting. J Oral Maxillofac Surg. 2019;77:2292–2297. doi: 10.1016/j.joms.2019.07.014. [DOI] [PubMed] [Google Scholar]
- 6.Badeau A, Carman C, Newman M, Steenblik J, Carlson M, Madsen T. Emergency department visits for electric scooter-related injuries after introduction of an urban rental program. Am J Emerg Med. 2019;37:1531–1533. doi: 10.1016/j.ajem.2019.05.003. [DOI] [PubMed] [Google Scholar]
- 7.Shichman I, Shaked O, Factor S, Elbaz E, Khoury A. Epidemiology of fractures sustained during electric scooter accidents: a retrospective review of 563 cases. J Bone Joint Surg Am. 2021;103:1125–1131. doi: 10.2106/JBJS.20.01746. [DOI] [PubMed] [Google Scholar]
- 8.Mitchell G, Tsao H, Randell T, Marks J, Mackay P. Impact of electric scooters to a tertiary emergency department: 8-week review after implementation of a scooter share scheme. Emerg Med Australas. 2019;31:930–934. doi: 10.1111/1742-6723.13356. [DOI] [PubMed] [Google Scholar]
- 9.Trivedi TK, Liu C, Antonio ALM, Wheaton N, Kreger V, Yap A, Schriger D, Elmore JG. Injuries associated with standing electric scooter use. JAMA Netw Open. 2019 doi: 10.1001/jamanetworkopen.2018.7381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mukhtar M, Ashraf A, Frank MS, Steenburg SD. Injury incidence and patterns associated with electric scooter accidents in a major metropolitan city. Clin Imaging. 2021;74:163–168. doi: 10.1016/j.clinimag.2021.02.005. [DOI] [PubMed] [Google Scholar]
- 11.Liew YK, Wee CPJ, Pek JH. New peril on our roads: a retrospective study of electric scooter-related injuries. Singapore Med J. 2020;61:92–95. doi: 10.11622/smedj.2019083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bekhit MNZ, Le Fevre J, Bergin CJ. Regional healthcare costs and burden of injury associated with electric scooters. Injury. 2020;51:271–277. doi: 10.1016/j.injury.2019.10.026. [DOI] [PubMed] [Google Scholar]
- 13.Cicchino JB, Kulie PE, McCarthy ML. Severity of e-scooter rider injuries associated with trip characteristics. J Safety Res. 2021;76:256–261. doi: 10.1016/j.jsr.2020.12.016. [DOI] [PubMed] [Google Scholar]
- 14.English KC, Allen JR, Rix K, Zane DF, Ziebell CM, Brown CVR, Brown LH. The characteristics of dockless electric rental scooter-related injuries in a large U.S. city. Traffic Inj Prev. 2020;21:476–481. doi: 10.1080/15389588.2020.1804059. [DOI] [PubMed] [Google Scholar]
- 15.CNN, J. B. E-scooters suddenly appeared everywhere, but now they’re riding into serious trouble. CNNhttps://www.cnn.com/travel/article/electric-scooter-bans-world/index.html.
- 16.Koninklijk besluit houdende algemeen reglement op de politie van het wegverkeer en van het gebruik van de openbare weg. 1975.
- 17.Mireille Chicron HG. Description et gravité des lésions traumatiques selon les classifications AIS 1998 et IIS 1994. 2003.
- 18.Siman-Tov M, Radomislensky I, Peleg K, Israel Trauma Group The casualties from electric bike and motorized scooter road accidents. Traffic Inj Prev. 2017;18:318–323. doi: 10.1080/15389588.2016. [DOI] [PubMed] [Google Scholar]
- 19.McGuinness MJ, Tiong Y, Bhagvan S. Shared electric scooter injuries admitted to Auckland City Hospital: a comparative review one year after their introduction. N Z Med J. 2021;134:21–29. [PubMed] [Google Scholar]
- 20.Talbot LA, Musiol RJ, Witham EK, Metter EJ. Falls in young, middle-aged and older community dwelling adults: perceived cause, environmental factors and injury. BMC Public Health. 2005;5:86. doi: 10.1186/1471-2458-5-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chini M, Hope A. Coronavirus: Uber and Lime pull sharing vehicles from streets. The brussels time 2020, Brussels, Belgium. https://www.brusselstimes.com/brussels/101717/coronavirus-uber-and-lime-pull-sharing-vehicles-from-streets
- 22.Claustre C, El Khoury C, Fraticelli L. Clés de compréhension du score de propension à l’usage du clinicien. Ann Fr Med Urgence. 2021;11:25–32. doi: 10.3166/afmu-2020-0235. [DOI] [Google Scholar]
- 23.Cremonte M, Cherpitel CJ. Alcohol intake and risk of injury. Medicina (B Aires) 2014;74:287–292. [PMC free article] [PubMed] [Google Scholar]