

Abstract
Sri Lanka was endorsed by the World Health Organization as a country that made immense progress in controlling the COVID-19 pandemic. This chapter focuses on the health-care structure, strategic use of Police, Tri-forces, and other government entities, media support, traditional social practices, the public responsiveness, and even the geographic location of the country that contribute to the overall control of the pandemic and management of the disease plausibly. Despite the nearly successful achievement, the country has faced economic, political, and social challenges during this critical period, through which many lessons are learnt. Sri Lanka has had few H1N1 outbreaks in the recent past. However, till the spread of COVID-19, the current population had not experienced the spread of a highly contagious disease in the country. Therefore, this chapter aims to share the novel experience, strategies used, challenges faced, and ways adapted in confronting COVID-19 as a country.
Keywords: Control, COVID-19, Health care, Management, Pandemic, Quarantine, Sri Lanka
1. Introduction
The pandemic, Coronavirus disease 2019 (COVID-19) caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2 virus) is among the deadliest events happened to the humankind in the recent history. The pandemic has triggered devastating effects on economic and sociopolitical conditions of tens of millions of people. Owing to the novelty of the virus, the development of remedial measures including vaccines posed many challenges. Thus, people had to adhere to many, mostly previously unpracticed precautionary measures including extensive hand washing, wearing masks, and social distancing. The spread of the disease was rapid and exponential in many regions severely affecting the day-to-day lives of people.
Sri Lanka is a tropical island in the Indian Ocean with an estimated population of 21,919,000 (Department of Census and Statistics, Sri Lanka, 2020). Population density is highest in the Western Province of the country, especially concentrated in and around the capital city, Colombo. Large crowds enter Colombo on a daily basis or seek temporary accommodation in Colombo or suburbs as many government and private offices, best hospitals, leading schools, several large state universities, free trade zones, the main seaport, and the prime airport of the country are situated in the Western Province. Sri Lanka being a popular tourist destination, earns a large amount of foreign exchange from the tourism industry; thus, its economy relies heavily on tourism (Ranasinghe & Sugandhika, 2018). The apparel industry also contributes largely to export income catering to the high-end US and European markets. The livelihood of a substantial portion of the population hence depends directly or indirectly on tourism and the apparel industry. Yet another considerable majority depends on agricultural industries, as producers, processors, retailers, or at a different scale in the market chain.
The main economic challenges faced by Sri Lanka as a country in the past few decades were the civil war, the tsunami, and the most recent Easter Sunday attack in 2019. COVID-19 pandemic hit Sri Lanka at a time the country was grappling to recover from the loss of the Easter Sunday attack in April 2019. The health sector of Sri Lanka is at a reasonably plausible level for a middle-income country. Sri Lanka ranked 73rd among 195 countries for personal health-care access and quality, being fairly ahead of other South Asian countries (Barber et al., 2017). Therefore, the state health sector was vigilant and ready to take up the health challenge of COVID-19. The Tri-forces, the Police, and government administrative workers are other main forces that strengthen and support the health-care sector in Sri Lanka throughout this mission. The cooperation and the commitment of the private sector and the public also play a pivotal role in succeeding the COVID-19 battle.
The very first COVID-19 case from a Sri Lankan citizen was reported on March 11, 2020 (Ediriweera et al., 2020), and the second after 2 weeks. Since then, the number of cases increased very slowly, not more than 10 patients on most days up to mid-April 2020. Besides the three to four spikes reported due to clusters from quarantine centers, a Navy base, and a rehabilitation center, the numbers remained in a range of 0–30 up to early October 2020 (Epidemiology Unit, 2020a). This period was considered the first COVID-19 wave in the country. The second COVID-19 wave hit the country harder than the first, just when the society was adopting the “New normal” life. The disease pattern and the trend were dissimilar to the first wave, where the daily numbers became 10–20 times higher by December 2020 (Epidemiology Unit, 2020b), supposedly due to different strategies adopted by the Government keeping in line with new global knowledge about the pandemic. Despite the recent increase in positive cases, the death rate of Sri Lanka is at 0.48% which is considerably lower than the global rate: 2.14% (Sri Lanka Health Promotion Bureau Website Dashboard, 2021). Several factors such as the robust health-care structure, strategic use of Police, Tri-Forces and other government entities, media support, traditional social practices, the public responsiveness, and the geographic location of the country have contributed largely for the control of the pandemic and management of the disease in the country.
2. The health-care structure of Sri Lanka
Sri Lanka's health-care system comprises allopathic, traditional, Ayurveda, Yunani, Siddha, homeopathy, and acupuncture practices (Ministry of Health and Indigenous Medical Services, 2020a). Allopathic or Western medical service is largely available via public and private sector service providers. Public allopathic care is provided by a robust network spanning across the country. Most importantly the public health-care sector is commonly accessible for the entire population free of charge. Private allopathic services provided at a cost are concentrated in metropolitan areas, enhanced by modern equipment and facilities (Perera & Perera, 2017). They attract the more modernized and economically sound fraction of the public. Nevertheless, the majority of the population seeks inpatient care primarily in the public sector. Twenty four million patients have been implicated to benefit through routine health clinics conducted at these facilities in 2014 (Perera & Perera, 2017). Moreover, the public sector offers Ayurvedic care free of charge to the public through regional Ayurveda hospitals/centers although the network is as not as much expanded as of the Western health-care structure. The private sector is also involved in providing Ayurveda, traditional Sri Lankan, and other conventional medical care. Most importantly, the private health-care institutions in Sri Lanka are regulated by the Private Health Regulatory Council (PHRC) while the conventional medical services are also regulated under different authorities to a great extent.
2.1. The state health sector
The state health sector caters to the nation in two main aspects; a) providing curative care services ranging from nonspecialized primary care to specialized care delivered through hospitals of different grades, and b) providing community health services focusing on promotive and preventive health. The curative care institutions are of three levels: tertiary care institutions (National Hospital of Sri Lanka, Teaching Hospitals, and Provincial General Hospitals), secondary care institutions (District General Hospitals and Base Hospitals (Type A, B)), and primary care institutions (Divisional Hospitals (Type A, B, C)) and primary medical care units (Ministry of Health and Indigenous Medical Services, 2020a). The management of the National Hospital and 21 teaching hospitals is driven by the Ministry of Health while the provincial councils are given the authority to manage other hospitals.
An excellent set of community health services are offered to the public through the Medical Officer of Health (MOH) offices, which are divisional health units, formed to reach almost all families throughout the country (Perera & Perera, 2017). Their prime focus is on maternal and child health, followed by communicable and noncommunicable diseases. As of 2018, 353 MOH offices have been functioning across the country (Ministry of Health and Indigenous Medical Services, 2020a). These units are managed by a medical doctor and supported by public health field staff, mainly consisting of Public Health Inspectors (PHIs) and Public Health Midwives (PHMs). The central authority of all public health services, however, lies on the Ministry of Health, and it is responsible for the provision of trained human resources, drug supply, and major infrastructure developments for all hospitals in the country. The effectiveness of this well-structured health-care system is clearly evident by its credible health indicators (Ministry of Health and Indigenous Medical Services, 2020a).
2.2. Excellence in disease management and surveillance
Before the emergence of COVID-19, Dengue was the most challenging public health concern in Sri Lanka (Tissera et al., 2020). Due to the high receptivity and the vulnerability to the disease, and the major Dengue outbreak in year 2004, Sri Lanka has established a dedicated unit for Dengue control: the National Dengue Control Unit, and a Presidential task force on dengue control headed by the President. Despite the lapses in vector control, disease management is well under control having skilled practitioners in the state hospitals and elaborate disease management guidelines set up by the authorities. Sustaining the Malaria-free status since 2012 further explains the strong and continuous disease surveillance system in Sri Lanka. However, Sri Lanka had not experienced any pandemic in the recent past.
2.3. Initial responses to COVID-19 disease management
The first COVID-19 patient, a foreign national, was reported from Sri Lanka in late January 2020 at the departure terminal of the main international airport of the country. The patient was treated at the National Institute of Infectious Diseases (Infectious Diseases Hospital – IDH) in Colombo and discharged mid-February after full recovery. Sri Lanka's preparedness for COVID-19 prevention and cure was well displayed through the prompt detection and successful management of this first patient. The first Sri Lankan patient was reported in early March, more than a month apart from the first patient diagnosis, followed by a slow daily rise in the numbers, establishing the first COVID-19 wave in the country. Based on the global disease trends and patterns, the health authorities paid much attention to strengthen the hospital emergency preparedness and response plans of all health-care institutions. The needs were addressed by the Government using a three-tier approach as shown in Fig. 10.1 (Ministry of Health and Indigenous Medical Services, 2020b).
Figure 10.1.
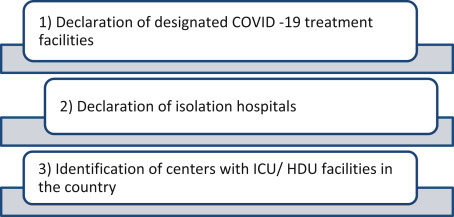
The three-tier approach used by the Ministry of Health of Sri Lanka to immediately address the need of strengthening the hospital emergency preparedness and response plan of all state health-care institutions of the country.
Initially only three hospitals—the IDH, Colombo East Base Hospital, and the Welikanda Base hospital in the North Central Province of Sri Lanka—were designated as COVID-19 treatment facilities. IDH was immediately designated to treat COVID-19 positive individuals and its infrastructure was rapidly developed. By mid-March the Welikanda Base hospital was converted to a fully equipped COVID-19 treatment center. Personnel from the Tri-forces were deployed in rapid construction activities where facilities were uplifted. By April 2020 just as the total number of COVID-19 patients was reaching 700, the authorities designated the Defence University (Kotelawala Defence University) hospital as a treatment center and 30 other hospitals as isolation centers to house suspected patients. They included tertiary as well as secondary care institutions covering most districts in the island. This was an important measure to ensure local preparedness to respond to a large number of suspected and confirmed cases as was reported in China and Europe during that period.
Hospitals with isolation centers, however, continue to provide the usual diverse health-care services, other than routine clinics, to the general public. Patients at risk, i.e., those with noncommunicable diseases, elderly patients, and pregnant women, are discouraged to attend the clinics. As many of these patients depend on freely issued medication, they are given options to get their prescribed medicine delivered to their residence or to be issued to a relative visiting the clinic. This arrangement was possible as the hospitals have well-maintained clinic registers with patient information. COVID-19 surveillance was expanded using existing respiratory disease surveillance systems and hospital-based surveillance. Heads of all the state health-care institutions were strongly advised by the health authorities not to deprive any patient of their usual standard of care due to their COVID-19 status. Such directions are vital to ensure the general well-being of the majority while caring for the directly affected, as the general public highly depends on state hospitals for any medical emergency and inpatient care.
The central health-care authority further advised and guided all the tertiary and secondary care hospitals including those with isolation centers to make arrangements to immediately scale up their COVID-19 preparedness as and when necessitated, based on the crisis status. The preparedness plan of the said hospitals included the establishment of a COVID-19 operational cell, outpatient and emergency department care, establishment of a designated COVID-19 suspected section/ward, provision of critical care for non-COVID and COVID suspected patients, safe transferring of patients to a COVID-19 designated/isolation hospital, ensuring safety of health-care staff, and managing COVID-19 cured patients (Ministry of Health and Indigenous Medical Services, 2020b). The COVID-19 operational cell is established with the expectation to ensure effective and collective decision-making at the hospital level at a critical time, and it consisted of the Head of the Institution, relevant consultants, and persons in-charge of other staff. The authorities had identified that ensuring the safety of staff is crucial in effectively managing the pandemic. Thus, supply of personal protective equipment (PPE), provision of required infrastructure and transport, continuous education and awareness programs, provision of psychological support, and ensuring surge capacity by deploying an adequate number of staff from other units of the hospital if needed were considered as essential steps to be taken at all hospitals to ascertain safety and well-being of the staff.
The Ministry of Health in no time published the guidelines for clinical management of COVID-19 (Ministry of Health and Indigenous Medical Services, 2020b). These guidelines, compiled by a group of expert medical practitioners in the country, highlight the importance of early case detection, prompt isolation of ill people, appropriate and timely management of patients, comprehensive contact tracing, and immediate quarantine of all possible contacts to minimize widespread community transmission to mitigate a major outbreak and associated mortality. The guidelines have even provided insight to develop the capacity of the health sector to be prepared to successfully handle any outbreak. Uniform and systematic management of all COVID-19 patients is ensured by the guideline, which is strictly followed at all state hospitals, where COVID-19 patients are managed. The private sector was not permitted to manage COVID-19 patients initially.
Disease diagnosis was limited to PCR tests during the first wave. Majority of the tests were done by the Medical Research Institute (MRI). With the rise in patient numbers during the first wave, the PCR testing facilities were established in state hospital laboratories and other government institutions, viz. universities in parallel to upgrading hospital facilities, as the authorities foresaw the need of bulk testing. In order to prevent over burdening of the laboratories, the treatment and isolation hospitals were assigned with specific laboratories for diagnostic testing.
2.4. COVID-19 community health services
The MOHs providing community health services are effectively utilized in engaging the public in quarantine and self-isolation activities where necessary. The close contacts of COVID-19 positive persons are quarantined at home or specially designated quarantine centers for 14 days irrespective of their initial PCR results. When people are home quarantined, the PHIs of the relevant MOH area is made responsible to ensure, the people under quarantine are made aware of the need to quarantine, and their basic needs such as food and other medical needs are fulfilled. The PHIs are the ideal resource persons that could be deployed to ensure the quarantine process is proper and adequate because they are the field health officers who are familiar with the neighborhood and the general requirements of the people in the area. The first wave of the pandemic halted the services of field clinics for pregnant women and the child immunization program, which are otherwise successfully handled by the PHMs in the country. However, their well-established communication network with the public has enabled them to continuously support and guide women in pregnancy-related matters and childcare. The Family Health Bureau functioning under the Ministry of Health released specific guidelines to ensure uninterrupted field maternal and child health-care services for lockdown areas and quarantined families. Safety of both the health-care workers as well as the community is given attention while guidance on field care and hospital care is provided in the instructions to field workers (Adikari et al., 2020). The need of continuous therapeutic communication was also highlighted to assure that necessary mental and emotional support is extended to the community as domestic violence is inevitable at a time when people are struggling to make a living while surviving a pandemic.
3. The public responsiveness
COVID-19 pandemic has created anxiety and uncertainty, worsening the economic crisis globally, in a similar or worse manner than other pandemics have. However, it is the worst and possibly the first pandemic that the current population is experiencing during their lifetime. In that light, the current Sri Lankan population has not even experienced an epidemic that is slightly in par with the COVID-19 pandemic. The worst epidemic faced by Sri Lankans in the recent past was the Dengue epidemic in 2017. A few H1N1 outbreaks in the recent past raised the alertness of the health sector, but the risk was not sensed significantly by the general public. Thus, similarly to the majority of the world's population, the COVID-19 pandemic is a novel experience to Sri Lankans.
Although the authorities imposed restrictions on overseas visitors in a gradual manner at the emergence of the first wave, i.e., over more than 6 weeks from the first patient being reported, a public holiday was declared abruptly overnight with a slight rise of the number of patients. The holiday was extended for several days and curfew was imposed on the entire country which lasted for 52 days. This unexpected sudden lockdown immensely affected the lives of general public. The fundamental challenge for the urban population was to secure their food and medical needs. The government authorities worked out to allow essential services to function under special permission and extremely high restrictions. Mobile vending was encouraged and well guided. The postal service workers were deployed to deliver medicine to patients being followed up at state hospital clinics. The public was very much enthusiastic to grow their own vegetables and cooking their own meals during the curfew period. Gardening and cooking became good hobbies for many people who used to work strenuously at offices. Many people made use of such opportunities to rebond with families which they had missed due to their hectic lifestyles. On the contrary, another portion of the society who depends largely on daily wages lost their livelihood due to the lockdown. Challenges faced by them are discussed in a later section in this chapter.
The Sri Lanka COVID-19 Healthcare and Social Security Fund was introduced by the President. The general public, government servants, and private entrepreneurs contributed generously in different scales to the fund. In addition, they assured direct donations of medical equipment, food, and other necessities to other needy entities. Many garment factories ran out of their regular orders. However, they started producing face masks and other PPE in large scales to meet the increasing demand in the country.
4. Traditional social practices
Sri Lanka is a multiethnic country with different cultures, practices, and beliefs. The current generation is often criticized by the older generation for ignoring the rich traditional cultures and practices and embracing more of western practices. The COVID-19 pandemic has now granted an opportunity for Sri Lankans to apply such cultural practices in the day-to-day lives. The traditional way of greeting in Sri Lanka is to join the palms together and to wish “Ayubowan” (“may you live longer!”). At a time when hand shaking is discouraged globally to avoid physical contact with outsiders, Sri Lankans found it intriguing to readopt their own way of greeting which does not involve physical contact. More fascinatingly the greeting gives out an energetic vibe when people wish good health and long life at a time they need it the most.
Quarantining became a new term for the general public. But the concept is not. Sri Lankans get self-isolated for 14–21 days when they contract contagious diseases such as chicken pox, measles, and mumps. Although curative allopathic medicine for such diseases is available currently, patient isolation and warning of visitors by hanging Neem leaves at the entrance to the house are still practiced by many. The health promotion workers used this traditional practice to make the public aware and understand the requirement of home quarantining.
One other strong advice given to the general public is that, before entering the house after being outside they should remove all clothing and footwear and shower outside if possible. The older generations in Sri Lanka have long been practicing such manners, or at least are familiar with such practices. Hence people are not reluctant to adhere to similar advice by the health authorities. Sri Lankans frequently consume ginger, coriander, and many other spices. There is belief that such spices can boost immunity, and thus play a protective role against the Coronavirus. Therefore, with the onset of the pandemic, the use of such home remedies has increased. Steam inhaling, another practice of traditional household to ease the sinuses, and upper respiratory tract infections, has lately become a common practice among many.
Having a Buddhist majority, Buddhist temples started enchanting the Ratana sutta (Jewel discourse) with belief that it protects a person or society from evil influences and pestilences. Similarly, there have been many religious rituals carried out by others including the Christian churches and Hindu temples. Such religious practices close to the people's heart may help to uplift the spiritual well-being of the public.
5. The geographic location of the country
There is evidence that countries closer to the equator have lower COVID-19 fatality rates than those that are away from the equator (Whittemore, 2020). Having exposed to optimum levels of sunlight prevents vitamin D deficiency, a reason associated with COVID-19 deaths (Whittemore, 2020). Moreover, sunlight can be used as a disinfectant of the SARS-CoV-2 virus as it is known to be inactivated in 30 min at 56°C (Eslami & Jalili, 2020; Whittemore, 2020). Being closer to the equator, Sri Lanka has a hot climate year around and can be considered a blessing in mitigating the effects of the virus.
Sri Lanka encompasses a limited number of ports to enter the country. The main international airport is the Bandaranayake International Airport among four other airports with less international functioning. There are seven seaports in the country, the Colombo port being the largest and busiest. As one of the very first precautionary actions against COVID-19 spread, the airports started monitoring the temperature of the passengers. It is undoubtedly an important step as the first COVID-19 patient was identified at the departure terminal when under surveillance (Sri Lanka Tourism Development Authority, 2020). From the first week of March 2020, passengers arriving from high-risk countries were sent for 14 days essential quarantine at centers specifically set up by the Sri Lanka Army to control the entry of COVID-19 patients to the country. The government decided to totally suspend all passenger flight and ship arrivals into Sri Lanka from third week of March 2020, with the gradual increase of patients reported in the country (Sri Lanka Tourism Development Authority, 2020). Being an island placed Sri Lanka in an advantageous position in controlling and surveillance of patients entering the country.
6. The role of military and police on COVID-19 management in Sri Lanka
As a country, Sri Lanka took strong measures to manage and mitigate the crisis at the initial stages of the pandemic and continue with the same. The government deployed the Tri-forces—Army, Navy, and the Air force—as well as the Police in different activities related to the management of the pandemic. Among the key activities are facilitating quarantine/isolation services, services at the COVID-19 intermediate care centers for nonsymptomatic patients, and community behavior control. Society believes that the proactive contribution of health professionals and the military personnel in battling against COVID-19 is the major reason for keeping the pandemic under control. When compared to some countries with a similar socioeconomic setting, Sri Lanka so far has successfully managed the pandemic while minimizing deaths. According to the report on combating COVID-19 Sri Lankan approach by the State Intelligence Service, the first line of the operations of preventing the spread of COVID-19 is through the military, police, and Intelligence sector of the country (State Intelligence Service, 2020). The major task of this line of operations was to sustain the magnitude of the pandemic into a manageable scale for the medical and health-care sectors. There are three major components of this process, i.e., detection, isolation, and tracing (Fig. 10.2 ). The Ministry of Defense has taken the lead in coordinating between all these agencies in this first line of operations in Sri Lanka. In addition, the forces are at the forefront of border management to control the entry of infected persons from overseas.
Figure 10.2.

Major components of the operations undertaken by the military, police, and intelligence sector of Sri Lanka to prevent the spread of COVID-19.
Roping the military in community behavior control could restrict the public freedom; nevertheless, the military has been one of the key supporters of crisis assistance and thus of humanitarian aid (Jayasena & Chinthaka, 2020). In this regard, as the first line of operations, members of the military built a national resilience against the pandemic situation.
7. The role of media on COVID-19 management in Sri Lanka
Dissemination of accurate, reliable, and useful information to the public is crucial for any disaster management effort. Mass media acts as a powerful force in shaping people's attitudes and ideas. Publishing the right information regarding the pandemic situation in the country to the local and international community is critical to keep them well-informed. In this regard, there are different types of sources of information in operation. Presidential Media Division acts as the official source of information for all the initiatives, actions, and progress regarding the process of combating the COVID-19 pandemic by providing the right information to the public through its website and social media. During this crisis period, traditional media including television (TV) channels, radio channels, and newspapers, in addition to social media forums, contribute significantly to the dissemination of correct information to the community (Hettiarachchi et al., 2020). Positive health practices are well promoted by the mass media via different advertisements to increase public awareness and control the spread of the disease in the country. For instance, for groups with inadequate literacy rates such as younger children (e.g., preschool level) and adults who are less conversant with reading, pictorial or video messages are the best source of information, especially on disease preventive measures such as wearing masks and washing hands. Experts from different fields have extensively used state and private media (both TV and radio channels), social media platforms to share the correct information with the general public through discussions and programs. Many TV commercials appeared with creative messages that encompass essential information to reduce exposure, social distancing, hand washing, face protection etiquette, etc.
However, since the recent past, there is an increasing concern about the misinformation spread especially by social media. There have been reports on unethical behavior of local media who had reported recognizable personal information, publishing the ethnicity of the COVID-19 patients which leads to stigmatization in the society (Ayub, 2020). On the other hand, the spread of fake news via social media platforms has significantly risen which mislead the community perception regarding COVID-19 spread, its causes, and prevention (Limaye et al., 2020). Many social media groups target providing “hot news” without verifying the sources and reliability.
7.1. Official COVID-19 information websites in Sri Lanka at a glance
As the COVID-19 outbreak is considered a health emergency in Sri Lanka, the government websites, especially the website of the Ministry of Health, are the official sources of information. The Ministry of Health website provides essential information on summary statistics including active cases and number recovered as well as deaths by each district. In addition, details on hospital admissions and tests carried out (PCR) are included. A Presidential Taskforce hotline is available on the Ministry of Health website for any emergency information (Ministry of Health, Sri Lanka, home page). Other important information including notices, guidelines, letters, and circulars are displayed on the website and these are updated frequently to provide the latest information (Figure 10.3, Figure 10.4 ).
Figure 10.3.

Guidelines on general preventive measures for work settings.
Information source: https://hpb.health.gov.lk/media/pdf/operational-guidelines.pdf.
Figure 10.4.

Preventive measures for special settings. The specific settings identified are displayed.
Information source: https://hpb.health.gov.lk/media/pdf/operational-guidelines.pdf.
8. Risk communication plan
In any disaster, risk communication plays a crucial role in the management and reducing impacts. The risk communication framework and risk communication plan for COVID-19 in Sri Lanka were developed by the Health Promotion Bureau of the Ministry of Health in January 2020. Accordingly, the risk communication plan consists of four phases (Health Promotion Bureau, 2020) (Table 10.1 ).
Table 10.1.
Four phases of the COVID-19 risk communication plan in Sri Lanka.
| Phase 1: preparedness phase | Phase 2: initial response phase | Phase 3: crisis phase | Phase 4: outbreak phase |
|---|---|---|---|
| Adherence of preparedness plan with no case reporting | Adherence of initial response plan with sporadic cases reporting |
|
Risk communication at the stage of community transmission |
Information source: Health Promotion Bureau. (2020). COVID-19 risk communication and community engagement (RCCE). Sri Lanka: Health Promotion Bureau.
However, the control strategies implemented in the country have been reported to be effective with at least 50% contact rate reduction or with at least 40% isolation of the contact history of infected population (Erandi et al., 2020).
9. Challenges faced
COVID-19 pandemic is not only affecting physical and mental health but also disrupting lives and livelihoods. Many pressing concerns and challenges are being increasingly appearing in the “new normal” status of the pandemic. New problems have emerged in economic development at both local and national levels and beyond as “business as usual” scenarios have changed. In times of uncertainty and with a plethora of regulations to manage the pandemic many vulnerable groups including poor and marginalized communities, part-time and temporary workers, low-income households, fishery and agricultural workers, and self-employed individuals are severely affected (Deyshappriya, 2020). Hospitality, apparel, and other export-oriented industries on which a considerable portion of the country's economy rely on are facing the greatest challenges. The exceptional and sudden increased costs of health care and safety management have taken the country's focus away from some essential developmental activities.
The interruption caused to the social structure is formidable. As Sri Lanka is a country with a social fabric of interconnected societal segments of family members, relatives, and friends, social isolation, quarantine, and lockdowns have affected psychosocial health. Among the most vulnerable groups are the poor, women, children, sick, and elderly. Restrictions on social gatherings that include religious rituals, cultural events, functions, sports, and leisure activities have hit the society badly. The virtual work environment has resulted in individuals being restricted to their homes and weakened social cohesion and discontent.
10. Conclusion
COVID-19 is still spreading globally at an alarming rate. While some countries that were fortunate to fully or nearly fully vaccinate their populations fight to restore health and normal life, some countries are still far from coming out of the COVID-19 disaster. Even though with unprecedented challenges, Sri Lanka's struggle to control the emergency situation which is basically managed by the health authorities and supported by other agencies has been successful to date. Specifically, the three-tier approach adopted has generated fruitful results. Public responsiveness to successful containment of the disease is increasingly evident. The media and the armed forces extend help in managing the pandemic situation. Yet, the pandemic has necessitated the need for a broader and integrated attempt to understand and act on many pressing socioeconomic concerns and as issues that are growing day by day.
Acknowledgment
We profoundly thank Dr. Sachini Amarasekara of the Department of Zoology and Environment Science, University of Colombo, Sri Lanka, for the English Language check.
References
- Adikari P.S., Pathirathna K.G.R.V., Kumarawansa W.K.W.S., Koggalage P.D. Role of MOH as a grassroots public health manager in preparedness and response for COVID-19 pandemic in Sri Lanka. AIMS Public Health. 2020;7(3):606. doi: 10.3934/publichealth.2020048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ayub M.S.M. Daily Mirror; May 1, 2020. Coronavirus and invasion of privacy.http://www.dailymirror.lk/opinion/Coronavirus-and-invasion-of-privacy/172-187540 Retrieved from. [Google Scholar]
- Barber R.M., Fullman N., Sorensen R.J., Bollyky T., McKee M., Nolte E., Davey G. Healthcare access and quality index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990–2015: A novel analysis from the global burden of disease study 2015. The Lancet. 2017;390(10091):231–266. doi: 10.1016/S0140-6736(17)30818-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Department of census and statistics, Sri Lanka. 2020. http://www.statistics.gov.lk/Resource/en/Population/Vital_Statistics/Mid-year_population_by_district.pdf Retrieved from. [Google Scholar]
- Deyshappriya N.P. May 10, 2020. Economic impacts of COVID-19 macro and microeconomics evidences from Sri Lanka. [Google Scholar]
- Ediriweera D.S., de Silva N.R., Malavige G.N., de Silva H.J. An epidemiological model to aid decision-making for COVID-19 control in Sri Lanka. PLoS One. 2020;15(8):e0238340. doi: 10.1371/journal.pone.0238340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epidemiology Unit . 2020. COVID-19 daily report on 5 October 2020.https://www.epid.gov.lk/web/images/pdf/corona_virus_report/sitrep-sl-en-05-10_10.pdf Retrieved from. [Google Scholar]
- Epidemiology Unit . 2020. COVID-19 daily report on 31 December 2020.https://www.epid.gov.lk/web/images/pdf/corona_virus_report/sitrep-sl-en-31-12_10.pdf Retrieved from. [Google Scholar]
- Erandi K.K.W.H., Mahasinghe A.C., Perera S.S.N., Jayasinghe S. Effectiveness of the strategies implemented in Sri Lanka for controlling the COVID-19 outbreak. Journal of Applied Mathematics. 2020;2020 doi: 10.1155/2020/2954519. [DOI] [Google Scholar]
- Eslami H., Jalili M. The role of environmental factors to transmission of SARS-CoV-2 (COVID-19) AMB Express. 2020;10(1):1–8. doi: 10.1186/s13568-020-01028-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Health Promotion Bureau . Health Promotion Bureau; Sri Lanka: 2020. COVID-19 Risk Communication and Community Engagement (RCCE) [DOI] [PubMed] [Google Scholar]
- Hettiarachchi D., Noordeen N., Gamakaranage C., Somarathne E.R.B.D., Jayasinghe S. Ethical responses to the COVID-19 pandemic—lessons from Sri Lanka. Asian Bioethics Review. 2020:1–9. doi: 10.1007/s41649-020-00153-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jayasena H., Chinthaka W. COVID-19 and developing countries: Lessons learnt from the Sri Lankan experience. Journal of the Royal Society of Medicine. 2020;113(11):464–465. doi: 10.1177/0141076820947367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Limaye R.J., Sauer M., Ali J., Bernstein J., Wahl B., Barnhill A., Labrique A. Building trust while influencing online COVID-19 content in the social media world. The Lancet Digital Health. 2020;2(6):e277–e278. doi: 10.1016/S2589-7500(20)30084-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ministry of Health, Sri Lanka home page. Retrieved from http://www.health.gov.lk/moh_final/english/. (Accessed 8 January 2021).
- Ministry of Health and Indigenous Medical Services . Ministry of Health and Indigenous Medical Services; Sri Lanka: 2020. Annual health statistics 2018, medical statistics unit. [Google Scholar]
- Ministry of Health and Indigenous Medical Services . Epidemiology unit, Ministry of Health and Indigenous Medical Services; Sri Lanka: 2020. Provisional clinical practice guidelines on COVID-19 suspected and confirmed patients. [Google Scholar]
- Perera A., Perera H.S.R. World Health Organization; Geneva: 2017. Primary health care systems (PRIMASYS): case study from Sri Lanka. [Google Scholar]
- Ranasinghe R., Sugandhika M.G.P. The contribution of tourism income for the economic growth of Sri Lanka. Journal of Management and Tourism Research. 2018;1:67–84. [Google Scholar]
- Sri Lanka Health Promotion Bureau Website Dashboard. Retrieved from https://hpb.health.gov.lk/covid19-dashboard/. (Accessed 13 January 2021).
- Sri Lanka tourism development authority. 2020. https://srilanka.travel/covid19/ Retrieved from. [Google Scholar]
- State Intelligence Service . 2020. Combating COVID – 19 Sri Lankan approach.https://www.president.gov.lk/.Documents/Concept-Paper-COVID-19-Ver-6-11-May-20-E.pdf [Google Scholar]
- Tissera H.A., Jayamanne B., Raut R., Janaki S., Tozan Y., Samaraweera P.C.…Fernando S.D. Severe dengue epidemic, Sri Lanka, 2017. Emerging Infectious Diseases. 2020;26(4):682–691. doi: 10.3201/eid2604.190435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whittemore P.B. COVID-19 fatalities, latitude, sunlight, and vitamin D. American Journal of Infection Control. 2020;48(9):1042–1044. doi: 10.1016/j.ajic.2020.06.193. [DOI] [PMC free article] [PubMed] [Google Scholar]