

Abstract
Studies documenting self-reported experiences of discrimination over the life course have been limited. Such information could be important for informing longitudinal epidemiologic studies of discrimination and health. We characterized trends in self-reports of racial, socioeconomic status, and gender discrimination over time measured using the Experiences of Discrimination Scale, with a focus on whether individuals’ reports of lifetime discrimination were consistent over time. Overall experiences of discrimination and the number of settings in which discrimination was reported in 1992, 2000, and 2010 were examined among 2,774 African-American and White adults in the Coronary Artery Risk Development in Young Adults (CARDIA) Study. Reports of “ever” experiencing discrimination decreased for all forms of discrimination across the 3 study visits. Approximately one-third (30%–41%) of the sample inconsistently reported ever experiencing any discrimination over time, which contributed to the observed decreases. Depending on the form of discrimination, inconsistent reporting patterns over time were more common among African-American, younger, less educated, and lower-income individuals and women—groups who are often most exposed to and severely impacted by the health effects of discrimination. Our findings highlight the possible underestimation of the lifetime burden of discrimination when utilizing the Experiences of Discrimination Scale to capture self-reports of discrimination over time.
Keywords: classism, gender discrimination, life course, racial discrimination, racism, sexism, socioeconomic status discrimination
Abbreviations:
- CARDIA
Coronary Artery Risk Development in Young Adults
- CI
confidence interval
- EOD
Experiences of Discrimination
- PR
prevalence ratio
- SD
standard deviation
- SES
socioeconomic status
Editor’s note: An invited commentary on this article appears on page 379, and the authors’ response appears on page 384.
Research on self-reports of discrimination and health has proliferated over the last 2 decades, with the documentation of associations between discrimination and many indicators of health (1), including but not limited to inflammation (2), hypertension (3), coronary artery calcium level (4), sleep quality (5–7), asthma (8), diabetes (9), and obesity (10, 11). However, much of this research has focused on reports of discrimination at a single point in time. It has been posited that constant or pervasive exposure to discriminatory stress across the life course may lead to the “wear and tear” or “weathering” of a range of physiological systems, thereby giving rise to adverse health conditions later in life (3, 12, 13). In keeping with this, studies have found (4, 10, 14, 15) that chronic or pervasive exposure to discrimination over time may be more deleterious for health than discrimination experienced at a single time point. Yet, the descriptive examination of individual-level self-reported experiences of discrimination over the life course, or at the least across extended periods of life, has been limited. Two studies examining trends in reports of general discrimination among middle-aged adults over periods of 4 and 9 years, respectively, documented overall stable reporting over time (10, 16). In another study among working US women, Gee et al. (17) observed relatively stable or increasing reports of racial and gender discrimination across 4 study visits from 1972 to 1989. Other studies documenting trends in the reporting of discrimination within individuals were only conducted among youth/adolescents or over short periods of time (i.e., <2 years) (18–23).
One major barrier to conducting research using longitudinal self-reports of discrimination is the lack of clarity around whether scales traditionally used to measure experiences of discrimination, such as the Experiences of Discrimination (EOD) Scale (24), reliably capture experiences over time. Specifically, for the EOD Scale, individuals are queried on whether they have “ever” experienced discrimination in at least 1 of 7 settings at study visits. The expectation would be that if someone reported “ever” experiencing discrimination in an earlier visit, they would also report “ever” experiencing discrimination in later visits. Thus, for such lifetime measures, the reporting of discrimination should theoretically remain stable or increase over time among individuals as they age. However, this expectation is in direct contrast to empirical evidence from several large cohort studies (the Midlife in the United States (MIDUS) Study, the Jackson Heart Study, and the National Latino and Asian American Study) (25–27) that show lower reporting of discriminatory experiences among older individuals. Further, external to a specific scale’s ability to reliably measure discrimination over time, previous research on the recall of stressful life events (28, 29) suggests that an individual’s tendency to recall stressful experiences (e.g., discrimination) may decrease as time passes. Thus, it is not known whether commonly used measures of discrimination may be more suitable as measures of cross-sectional or more recent experiences of discrimination rather than as reliable measures of experiences of discrimination across time (i.e., over consecutive years or longer periods of time).
The Coronary Artery Risk Development in Young Adults (CARDIA) Study (30) is a rich data source that offers a unique opportunity to examine self-reports of discrimination over time in a socioeconomically diverse cohort of African-American and White adults. In the current study, we describe the pattern of reporting racial, socioeconomic status (SES), and gender discrimination at study visits in 1992, 2000, and 2010 using the EOD Scale. Additionally, because it is unclear whether individuals consistently report lifetime experiences of discrimination over time using the EOD Scale, we examined whether individuals recalled or inconsistently reported discrimination over time and whether inconsistent reporting varied by type of discrimination and/or demographic factors.
METHODS
Study participants
The CARDIA Study is a longitudinal cohort study of cardiovascular disease risk among 5,115 African-American and White adults (52% African-American, 55% female) aged 18–30 years at baseline (1985–1986) from 4 US urban areas (Birmingham, Alabama; Chicago, Illinois; Minneapolis, Minnesota; and Oakland, California (30). Of the 5,115 adults enrolled at baseline, 2,774 (52.4%) were included in the analytical sample, as they had data on reports of discrimination for all 3 types of discrimination examined, including racial, SES, and gender discrimination, at visits 7 (1992–1993), 15 (2000–2001), and 25 (2010–2011). Compared with people who were included in the study at the 1992 visit but did not have data on discrimination at all 3 visits (n = 1,311), the analytical sample was older (mean age = 32.2 years vs. 31.6 years), had a higher proportion of White persons (57.5% vs. 39.4%) and women (56.5% vs. 52.1%), and was on average more educated (≥16 years of education: 45.8% vs. 29.1%) and had higher incomes (≥$50,000/year: 22.2% vs. 15.3%). The CARDIA Study was approved by institutional review boards at each study center, and participants provided written informed consent.
Reports of discrimination
Self-reports of discrimination were measured using the EOD Scale, which was created by Krieger et al. (24). The EOD Scale has been widely used among both African-American and White persons and has been validated against other discrimination scales and examined for test-retest reliability 2–4 weeks after initial assessment (24). In CARDIA, the EOD Scale was self-administered; it was provided to participants after a self-administered recreational drug-use questionnaire at the 1992 visit and after the self-administered Center for Epidemiological Studies Depression Scale at the 2000 and 2010 visits. Participants were asked at the 1992, 2000, and 2010 visits if they had ever “been prevented from doing something” or “been hassled or made to feel inferior” in 7 different settings: at school; getting a job; at work; getting housing; getting medical care; from the police or in the courts (1992 visit only)/at home (2000 and 2010 visits); and on the street or in a public setting. Participants were queried about experiences of discrimination 3 separate times at each visit, each time with a different attribution: “socioeconomic position or social class,” “race or color,” and “gender.” A dichotomous “ever/never” variable was created to characterize any self-reports of discrimination at each visit for each form of discrimination (10).
We focused on the reporting patterns for each form of discrimination across the 3 visits to determine whether and the extent to which individuals inconsistently reported ever experiencing discrimination across time. Inconsistent reporting of discrimination—in the context of a lifetime measure of discrimination—was classified in 4 categories: “never, ever, never;” “ever, never, never;” “ever, ever, never;” and “ever, never, ever.” For example, inconsistent reporting using the EOD Scale could have occurred if participants initially reported “ever” experiencing discrimination in any setting in 1992 (visit 7) but then reported “never” experiencing discrimination in any setting in 2000 (visit 15) and/or 2010 (visit 25). Similarly, it could have occurred if participants initially reported “ever” experiencing discrimination in any setting at the 2000 visit but then reported “never” experiencing discrimination in any setting at the 2010 visit.
Sociodemographic factors
Sociodemographic factors included in the analyses were: self-reported race (non-Hispanic African American or non-Hispanic White) and sex (female or male), with data collected at baseline (1985–1986), and age (in 3 categories: 24–29 years, 30–34 years, and 35–40 years, which corresponded to the birth cohorts 1968–1963, 1962–1958, and 1957–1952), education (in 2 categories: <16 or ≥16 years of education), and annual income (in 2 categories reflecting yearly pretax family income from all sources: <$50,000 or ≥$50,000), with data collected at visit 7 (1992).
Statistical methods
Descriptive statistics (frequencies or mean values) for self-reports of each form of discrimination at the 3 study visits were calculated overall and by setting. We also calculated descriptive statistics for the unique reporting patterns for each form of discrimination across the 3 visits to determine whether and the extent to which individuals inconsistently reported ever experiencing discrimination across time. Following the examination of inconsistent reporting patterns over time for each form of discrimination, log binomial regression was used to determine the demographic factors (i.e., race, age, education, income, and/or sex) associated with inconsistent reporting over time. We conducted additional exploratory descriptive analyses to examine differences in the reported number of settings in which discrimination was ever experienced among people who inconsistently reported discrimination over time compared with people who did not.
To evaluate linear and nonlinear trends in the reporting of discrimination across the 3 visits, we utilized generalized estimating equations models with the reporting of discrimination as the outcome and included study site, age group, linear and quadratic terms for time (i.e., 3 time points for visits in 1992, 2000, and 2010), and a term for interaction between linear time and age. Generalized estimating equations models were employed to account for the repeated measures of individuals’ reports of discrimination across study waves, with an assumption of autoregressive correlation through time within each individual. The log binomial distribution was specified in the models, given the dichotomous outcome (i.e., reporting of discrimination “ever” vs. “never”). A quadratic term for time was included in models to allow for possible nonlinear patterns in the reporting of discrimination over time (i.e., the reporting of discrimination in 1992 and 2010 but not in 2000). Age was included to evaluate any variation in the reporting of discrimination across age groups (25–27), which also corresponded with certain birth cohorts, allowing for the possibility that the reporting of discrimination may be shaped by life stage, as well as the historical context in which individuals were born and aged independent of secular trends (17). All analyses were conducted in SAS, version 9.4 (SAS Institute, Inc., Cary, North Carolina).
RESULTS
The sample included 1,179 African-American and 1,595 White adults and was 56.5% female. At visit 7 (1992), the average age of the analytical sample was 32.2 years (standard deviation (SD), 3.6); range, 24–40), and 45.8% of the sample had 16 or more years of education. As Figure 1A shows, the percentage of individuals reporting any racial, SES, or gender discrimination decreased across the 3 study visits. In 1992, 2000, and 2010, 50%, 45%, and 35% of participants reported ever experiencing any racial discrimination, respectively; 36%, 32%, and 24% reported ever experiencing any SES discrimination; and 58%, 52%, and 35% reported ever experiencing any gender discrimination. Similar declines were also observed in the average number of settings in which each form of discrimination was reported across visits (Figure 1B). Overall, on average, in 1992, 2000, and 2010, participants reported 1.4 (SD, 1.9), 1.2 (SD, 1.7), and 0.9 (SD, 1.6) racial discrimination settings; 0.9 (SD, 1.6), 0.8 (SD, 1.5), and 0.6 (SD, 1.3) SES discrimination settings; and 1.4 (SD, 1.6), 1.3 (SD, 1.7), and 0.9 (SD, 1.5) gender discrimination settings. As Figure 2 shows, the predicted probability of reporting any racial, SES, or gender discrimination decreased across the 3 visits for all age groups. At each visit, people in the youngest age group and the latest birth cohort (i.e., persons aged 24–29 years in 1992 and born 1968–1963) were more likely to report racial discrimination than their older counterparts (i.e., people who were aged 30–34 and 35–40 years in 1992 and were born in 1962–1958 and 1957–1952, respectively; Figure 2A).
Figure 1.
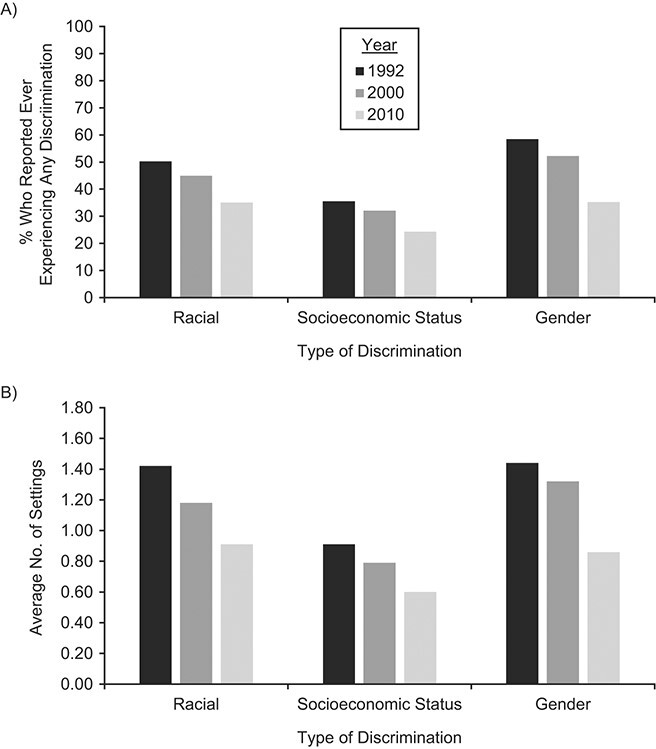
Percentage of individuals reporting “ever” experiencing discrimination (A) and average number of settings in which discrimination was reported (B) in 1992, 2000, and 2010 (n = 2,774), Coronary Artery Risk Development in Young Adults Study. Participants were queried with regard to 6 possible settings in 1992 (visit 7) for gender discrimination, while participants were queried about 7 settings for all other visits for each form of discrimination.
Figure 2.
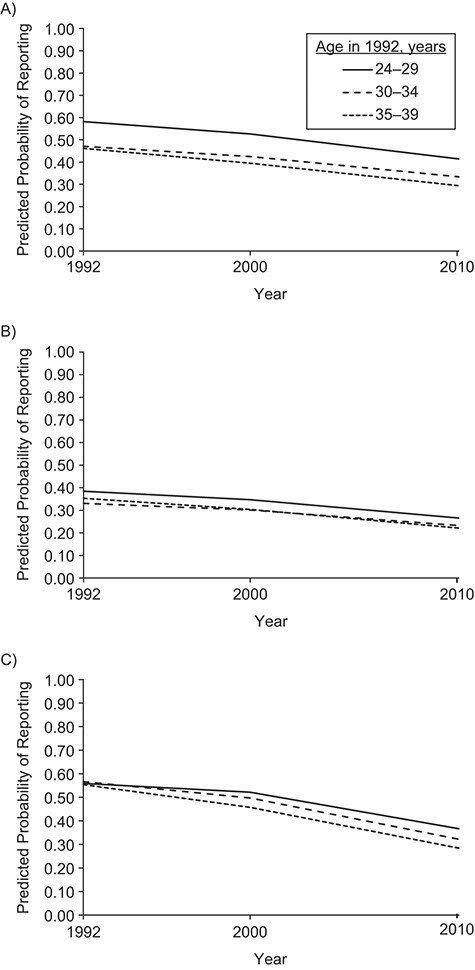
Predicted probability of reporting “ever” experiencing discrimination due to race (A), socioeconomic status (B), and gender (C) across time (1992, 2000, and 2010), by age group (n = 2,774), Coronary Artery Risk Development in Young Adults Study. Predicted probabilities were produced by means of generalized estimating equations models that included time (year), time squared, study site, age group, and a term for interaction between time and age group. Differences in the reporting of racial discrimination across study visits were observed for persons aged 24–29 years versus persons aged 30–34 and 35–40 years (2-sided P < 0.05).
The various unique reporting patterns of each form of discrimination across the 3 study visits can be found in Table 1. Twenty-six percent, 12%, and 25% of participants consistently reported ever experiencing any racial, SES, and gender discrimination, respectively, across the 3 visits, while 38%, 48%, and 27% consistently reported never experiencing any racial, SES, and gender discrimination, respectively, across the 3 visits. The categories in Table 1 (“never, ever, never;” “ever, never, never;” “ever, ever, never;” and “ever, never, ever”) represent reporting patterns of individuals who inconsistently reported “ever” experiencing any discrimination at some point across the 3 visits. Overall, 30%, 31%, and 41% of individuals were included in these categories for racial, SES, and gender discrimination, respectively, as they had reported “ever” experiencing any discrimination at a given visit but then reported “never” experiencing any discrimination at a later visit. Patterns of reporting of racial discrimination by race, SES discrimination by education, and gender discrimination by sex are presented in Web Table 1.
Table 1.
Reporting Patterns of “Ever” Experiencing Discrimination in the CARDIA Study Across the Years 1992, 2000, and 2010 (n = 2,774)a
| Discrimination Reporting Pattern in 1992, 2000, and 2010 | Racial Discrimination | SES Discrimination | Gender Discrimination | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| Never, never, never | 1,054 | 38.0 | 1,325 | 47.8 | 759 | 27.4 |
| Never, never, ever | 87 | 3.1 | 135 | 4.9 | 71 | 2.6 |
| Never, ever, ever | 91 | 3.3 | 113 | 4.1 | 114 | 4.1 |
| Never, ever, neverb | 149 | 5.4 | 216 | 7.8 | 210 | 7.6 |
| Ever, never, neverb | 312 | 11.3 | 335 | 12.1 | 389 | 14.0 |
| Ever, never, everb | 75 | 2.7 | 91 | 3.3 | 106 | 3.8 |
| Ever, ever, neverb | 285 | 10.3 | 223 | 8.0 | 440 | 15.9 |
| Ever, ever, ever | 721 | 26.0 | 336 | 12.1 | 685 | 24.7 |
| Total inconsistent reportingc | 821 | 29.7 | 865 | 31.2 | 1,145 | 41.3 |
Abbreviations: CARDIA, Coronary Artery Risk Development in Young Adults; SES, socioeconomic status.
a Percentages sum to 100.1 because of rounding.
b These 4 categories denote inconsistent reporting patterns across the 3 study visits and are represented in the “total inconsistent reporting” category.
c Results for the 4 categories with inconsistent reporting patterns across the 3 study visits.
Inconsistent reporting of ever experiencing discrimination in a given setting was also observed across 1992, 2000, and 2010 (Web Table 2). The proportion of individuals reporting ever experiencing discrimination in a specific setting decreased for nearly all settings from 1992 to 2010, with the steepest declines occurring primarily from 2000 to 2010. Notably, among people who consistently reported ever experiencing any discrimination across time, there were some who reported ever experiencing discrimination in one setting at a given visit (i.e., in 1992) and then, at a later visit (i.e., in 2000), did not report ever experiencing discrimination in that same setting but instead reported ever experiencing discrimination in a different setting. For example, among people who consistently reported SES discrimination across the 3 visits (n = 1,909), of those reporting ever experiencing SES discrimination while at work in 1992 (n = 193), only 64.8% also reported ever experiencing SES discrimination while at work in 2000 (data not shown).
Results from regression models examining demographic factors associated with the inconsistent reporting of ever experiencing any discrimination across visits can be found in Table 2. Compared with people who consistently reported racial discrimination over time, people who inconsistently reported racial discrimination were more likely to be African-American (prevalence ratio (PR) = 1.23, 95% confidence interval (CI): 1.10, 1.38), to have less than 16 years of education (PR = 1.33, 95% CI: 1.18, 1.50), and to be younger. Compared with people who consistently reported SES discrimination over time, people who inconsistently reported SES discrimination were more likely to be African-American (PR = 1.63, 95% CI: 1.46, 1.82), to have less than 16 years of education (PR = 1.42, 95% CI: 1.26, 1.59), to earn less than $50,000 annually (PR = 1.23, 95% CI: 1.06, 1.43), and to be younger in age. Women were more likely to inconsistently report gender discrimination over time compared with men (PR = 1.18, 95% CI: 1.08, 1.29), and people with less than 16 years of education were more likely to inconsistently report gender discrimination than people with 16 or more years of education (PR = 1.13, 95% CI: 1.03, 1.23). Demographic groups more likely to inconsistently report discrimination across time were often also more likely to report ever experiencing discrimination at a given visit (Web Table 3).
Table 2.
Demographic Factors Associated With Inconsistent Reporting Patterns of “Ever” Experiencing Discrimination in the CARDIA Study Across the Years 1992, 2000, and 2010 (n = 2,774)
| Inconsistent Reporting (Yes vs. No) | |||||||
|---|---|---|---|---|---|---|---|
| Demographic Factor | Referent Group | Racial Discrimination | SES Discrimination | Gender Discrimination | |||
| PR a | 95% CI | PR a | 95% CI | PR a | 95% CI | ||
| Age in 1992, years | 24–29 | ||||||
| 30–34 | 0.85 | 0.74, 0.97 | 0.79 | 0.69, 0.90 | 0.95 | 0.85, 1.07 | |
| 35–40 | 0.89 | 0.77, 1.03 | 0.83 | 0.72, 0.95 | 0.98 | 0.87, 1.10 | |
| Female sex | Male | 0.97 | 0.86, 1.08 | 0.97 | 0.87, 1.08 | 1.18 | 1.08, 1.29 |
| African-American race | White | 1.23 | 1.10, 1.38 | 1.63 | 1.46, 1.82 | 1.11 | 1.02, 1.22 |
| Education duration <16 years | ≥16 | 1.33 | 1.18, 1.50 | 1.42 | 1.26, 1.59 | 1.13 | 1.03, 1.23 |
| Annual income <$50,000 | ≥$50,000 | 1.12 | 0.96, 1.31 | 1.23 | 1.06, 1.43 | 0.98 | 0.88, 1.10 |
Abbreviations: CARDIA, Coronary Artery Risk Development in Young Adults; CI, confidence interval; PR, prevalence ratio; SES, socioeconomic status.
a Models adjusted for study site and additionally included age, education, income, race, or sex.
In exploratory analyses among people who reported ever experiencing any discrimination in 1992, people who inconsistently reported ever experiencing any discrimination at a later visit on average reported a lower number of settings in which they had ever experienced discrimination in 1992 (racial discrimination settings: mean = 2.1 (SD, 1.4); SES discrimination settings: mean = 2.2 (SD, 1.5); gender discrimination settings: mean = 2.1 (SD, 1.2)) in comparison with people who did not inconsistently report ever experiencing any discrimination at a later visit (racial discrimination settings: mean = 3.5 (SD, 1.8); SES discrimination settings: mean = 3.2 (SD, 1.8); gender discrimination settings: mean = 2.9 (SD, 1.5)) (t tests: 2-sided P < 0.001; data not shown).
DISCUSSION
In this study documenting trends and patterns in self-reports of racial, SES, and gender discrimination using the EOD Scale among African-American and White adults across time, reports of ever experiencing discrimination consistently decreased across 3 visits from 1992 to 2010. Given the expectation that lifetime reports of discrimination should theoretically remain stable or increase over time among individuals as they age and given the wording of the EOD Scale, such that individuals were queried on “ever” experiencing discrimination, it is not clear why reports of discrimination declined over time. Moreover, given the potential increase in the relevance of some forms of discrimination over time (i.e., SES discrimination—due to growing divides along lines of income and wealth in the United States (31)), the declines in reports of discrimination are counter to expected secular trends. Nonetheless, one contributor to the declines is the inconsistent reporting of discrimination over time, as 30%–41% of our sample reported “ever” experiencing any discrimination at a given visit but then reported “never” experiencing any discrimination at a later visit.
The EOD Scale is a commonly used measure of discrimination in studies of discrimination and health, and the observed inconsistent reporting of “ever” experiencing any discrimination across time suggests that for some individuals this measure might be an indicator of cross-sectional or more recent experiences of discrimination rather than an indicator of lifetime, or accumulated, experiences of discrimination over time. Currently it is unclear whether this lack of stability in reporting is unique to the EOD Scale, or a function of how individuals experience discrimination across the life course. At least one other scale, the Everyday Discrimination Scale, has observed stable reporting of discrimination over time (16); however, that scale measures day-to-day interpersonal discrimination, with a focus on routine and relatively minor experiences of unfair treatment (32). In contrast, the EOD Scale focuses on major experiences, requires individuals to identify an attribute, and asks respondents to recall “ever” experiencing discrimination. It is currently unknown which, if any, of these factors might lead to inconsistencies in reporting over time. Future research in this area is warranted.
There were also inconsistencies over time in the reporting of settings where discrimination occurred, which may have implications for studies that have used the number of settings across visits to categorize participants into varying levels of exposure to discrimination (33). Nonetheless, the approach used by some researchers (34), which considers individuals who ever reported discrimination at an earlier visit as having ever experienced discrimination at later visits, regardless of the response given by those individuals at later visits, may inadvertently circumvent inconsistent reporting problems over time. However, while theoretically appropriate, this approach may prevent the consideration of potential differences in the pervasiveness of discrimination across the life course by ignoring patterns of reporting (consistent vs. inconsistent) over time. Patterns of inconsistent reporting—which represent an example of exposure misclassification—may be important to consider when examining the health effects associated with chronic discrimination.
While it is possible that individuals who inconsistently reported discrimination over time completed the EOD Scale without considering all experiences of discrimination they had “ever” been exposed to and thus focused on more recent experiences, it is also possible that experiences of discrimination may mean something different or may be less severe or less pervasive for this group, leading to differential recall. In line with this, we observed that people who were inconsistent reporters in 2000 and/or 2010 on average reported a lower number of settings in which they had experienced racial, SES, and gender discrimination in 1992 as compared with people who were consistent reporters. However, we were not able to examine a rating of severity of the experiences reported. Thus, research investigating possible differential recall of experiences of discrimination related to the severity or pervasiveness of the experience(s) is necessary.
Notably, African-American, younger, lower-income/less educated individuals, and women were more likely to inconsistently report ever experiencing discrimination across visits. This may partially be due to the fact that groups disadvantaged by race, age, SES, and/or gender are less likely to report “never” at all time points (e.g., reports of “never, never, never” experiencing discrimination are most likely among individuals who do not encounter discriminatory treatment) (34–37). Nonetheless, one potential consequence of this disparity in inconsistent reporting over time is the disproportionate underestimation of the lifetime burden of discrimination for these groups. This could be important, given that these groups are often among the populations that are most severely impacted by the health effects of discrimination (1, 5, 37, 38). In this respect, underestimation of the lifetime burden of discrimination may have actually biased prior studies of discrimination and health toward the null, particularly among those groups most burdened (39, 40), suggesting that the true population-level effects of discrimination on health may be greater than previously estimated for African-American persons, women, and lower-SES individuals (41). Additional research is needed to examine valid and reliable ways to measure lifetime experiences of discrimination over time across different populations.
Findings from the broader literature on stressful life events may be of particular relevance, as research suggests that during the first 12 months after the occurrence of a stressful life event, there is a rapid fall-off in reporting (42, 43). However, the rate of fall-off varies by the type of event. For example, highly impactful events, such as the death of a spouse, a marriage, or a birth, have essentially no fall-off, while other, less impactful events have higher rates of fall-off. For experiences of discrimination, which are conceptualized as a form of psychosocial stress, personality factors, changes in the climate of public opinion (e.g., as a result of the “Me Too” or “Black Lives Matter” movement), the memory reconstruction of the experience, and the level of trauma related to the experience might all affect the ability to accurately recall an event (28, 29). Additionally, the understanding and reinterpretation of the question asking about experiences of discrimination may also affect individuals’ ability to recall experiences (28). For example, time may change perceptions or interpretations of past events, such that an experience that was considered discriminatory at age 25 might be viewed differently at age 43. Given this, future scales of self-reported discrimination should query individuals about experiences over a shorter time frame and possibly avoid questions about experiences respondents have “ever” had.
There are additional considerations that longitudinal studies of discrimination and health might consider when conceptualizing cumulative or lifetime measurements of self-reported discrimination measured with current methodology and scales. One is the role of aging in reporting lifetime discrimination, as we observed that older individuals were less likely to report racial discrimination than their younger counterparts and reports of all forms of discrimination declined as individuals aged over time. Given that all of our participants were below age 60 years at the time of administration of the EOD Scale in 2010, this was not likely to be due to a deterioration in episodic memory or to cognitive decline more broadly. Rather, this decrease may be related to the “socioemotional selectivity” (44) that occurs with aging, where older adults “self-select out of undesirable social situations” (45, p. 179). For example, a 50-year-old African-American man or woman may choose to avoid individuals and/or settings (e.g., workplaces, stores, etc.) where they might have encountered discriminatory treatment in their 20s or 30s, which would then lead to lower exposure to (and reports of) racial discrimination in their 50s than in earlier years. Thus, as individuals age, the composition of social networks and the perception of limited time may all influence exposure to discrimination (44). This is consistent with prior research that has found lower reports of discrimination among older adults than among younger adults (25–27). Additionally, while it was not possible to fully evaluate birth cohorts in this study, the role of birth cohort (e.g., pre– vs. post–Civil Rights-era United States) in the reporting of discrimination across the life course warrants exploration in future studies (46, 47).
The method and order of administration of the EOD Scale may also be a consideration for reporting patterns over time. While the EOD Scale was self-administered in the CARDIA Study, avoiding potential interviewer-related influences on reporting, the order in which the EOD Scale was provided to participants differed in 2000 and 2010 compared with 1992. At the 2000 and 2010 visits, a self-administered depression symptomology scale was answered by participants prior to the EOD Scale. While it is not clear how the change in the order and type of scale preceding the EOD Scale might have affected reporting patterns over time, this could be an important consideration.
There were limitations to this study. First, we only examined trends in reports of discrimination across 3 study visits, albeit an 18-year period was covered altogether. Second, we were not able to fully examine the roles of secular trends, birth cohorts, and age in reporting patterns as has been done in previous work (17), given the limited range of birth years (1952–1968) in CARDIA and the limited ability to select cutpoints that would overlap with changes in influential time periods (e.g., before vs. after the Civil Rights Acts of 1964 and 1968) relevant for all 3 forms of discrimination. Lastly, the CARDIA Study includes African-American and White adults from 4 US metropolitan areas (48); thus, these findings may not be generalizable to other geographic areas or demographic groups.
In this study examining trends in self-reports of discrimination across time in the CARDIA Study using the EOD Scale, reports of ever experiencing any racial, SES, or gender discrimination decreased across 3 study visits in 1992, 2000, and 2010. These findings contrast with a theoretical expectation that lifetime reports of discrimination ought to remain stable or increase over the life course. However, inconsistent reporting of ever experiencing discrimination over time contributed to these declines and suggests possible underestimation of the lifetime burden of discrimination when utilizing the EOD Scale. Findings from this study highlight methodological considerations for the measurement of self-reported lifetime experiences of discrimination over time using the EOD Scale. Research improving the measurement of lifetime discrimination, particularly among populations disproportionately impacted by the health effects of discrimination (1, 35–38), is warranted.
Supplementary Material
ACKNOWLEDGMENTS
Author affiliations: Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta, Georgia, United States (Miriam E. Van Dyke, Michael R. Kramer, Viola Vaccarino, Tené T. Lewis); Department of Preventive Medicine, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, United States (Kiarri N. Kershaw); and Department of Behavioral, Social, and Health Education Sciences, Rollins School of Public Health, Emory University, Atlanta, Georgia, United States (Natalie D. Crawford).
The Coronary Artery Risk Development in Young Adults (CARDIA) Study is conducted and supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham (contracts HHSN268201800005I and HHSN268201800007I), Northwestern University (contract HHSN268201800003I), the University of Minnesota (contract HHSN268201800006I), and the Kaiser Foundation Research Institute (contract HHSN268201800004I). M.E.V.D. was supported by a Howard Hughes Medical Institute Gilliam Fellowship for Advanced Study. M.E.V.D. received additional funding from the National Institutes of Health (grant 1 T32 HL130025-01A1).
This article was reviewed for scientific content by the CARDIA investigators.
Conflict of interest: none declared.
REFERENCES
- 1. Williams DR, Lawrence JA, Davis BA. Racism and health: evidence and needed research. Annu Rev Public Health. 2019;40:105–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Cuevas AG, Ong AD, Carvalho K, et al. Discrimination and systemic inflammation: a critical review and synthesis. Brain Behav Immun. 2020;89:465–479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Forde AT, Sims M, Muntner P, et al. Discrimination and hypertension risk among African Americans in the Jackson Heart Study. Hypertension. 2020;76(3):715–723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Lewis TT, Everson-Rose SA, Powell LH, et al. Chronic exposure to everyday discrimination and coronary artery calcification in African-American women: the SWAN Heart Study. Psychosom Med. 2006;68(3):362–368. [DOI] [PubMed] [Google Scholar]
- 5. Lee S, Chang AM, Buxton OM, et al. Various types of perceived job discrimination and sleep health among working women: findings from the Sister Study. Am J Epidemiol. 2020;189(10):1143–1153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Gaston SA, Feinstein L, Slopen N, et al. Everyday and major experiences of racial/ethnic discrimination and sleep health in a multiethnic population of U.S. women: findings from the Sister Study. Sleep Med. 2020;71:97–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Slopen N, Lewis TT, Williams DR. Discrimination and sleep: a systematic review. Sleep Med. 2016;18:88–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Coogan PF, Yu J, O’Connor GT, et al. Experiences of racism and the incidence of adult-onset asthma in the Black Women’s Health Study. Chest. 2014;145(3):480–485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Whitaker KM, Everson-Rose SA, Pankow JS, et al. Experiences of discrimination and incident type 2 diabetes mellitus: the Multi-Ethnic Study of Atherosclerosis (MESA). Am J Epidemiol. 2017;186(4):445–455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hunte HE. Association between perceived interpersonal everyday discrimination and waist circumference over a 9-year period in the Midlife Development in the United States cohort study. Am J Epidemiol. 2011;173(11):1232–1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Lewis TT, Kravitz HM, Janssen I, et al. Self-reported experiences of discrimination and visceral fat in middle-aged African-American and Caucasian women. Am J Epidemiol. 2011;173(11):1223–1231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Goosby BJ, Cheadle JE, Mitchell C. Stress-related biosocial mechanisms of discrimination and African American health inequities. Annu Rev Sociol. 2018;44:319–340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Daniels KP, Valdez Z, Chae DH, et al. Direct and vicarious racial discrimination at three life stages and preterm labor: results from the African American Women’s Heart & Health Study. Matern Child Health J. 2020;24(11):1387–1395. [DOI] [PubMed] [Google Scholar]
- 14. Bécares L, Zhang N. Perceived interpersonal discrimination and older women’s mental health: accumulation across domains, attributions, and time. Am J Epidemiol. 2018;187(5):924–932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Slopen N, Williams DR. Discrimination, other psychosocial stressors, and self-reported sleep duration and difficulties. Sleep. 2014;37(1):147–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Lewis TT, Troxel WM, Kravitz HM, et al. Chronic exposure to everyday discrimination and sleep in a multiethnic sample of middle-aged women. Health Psychol. 2013;32(7):810–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Gee GC, Pavalko EK, Long JS. Age, cohort and perceived age discrimination: using the life course to assess self-reported age discrimination. Soc Forces. 2007;86(1):265–290. [Google Scholar]
- 18. Rosenthal L, Earnshaw VA, Lewis TT, et al. Changes in experiences with discrimination across pregnancy and postpartum: age differences and consequences for mental health. Am J Public Health. 2015;105(4):686–693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Stein GL, Supple AJ, Huq N, et al. A longitudinal examination of perceived discrimination and depressive symptoms in ethnic minority youth: the roles of attributional style, positive ethnic/racial affect, and emotional reactivity. Dev Psychol. 2016;52(2):259–271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Brody GH, Chen YF, Murry VM, et al. Perceived discrimination and the adjustment of African American youths: a five-year longitudinal analysis with contextual moderation effects. Child Dev. 2006;77(5):1170–1189. [DOI] [PubMed] [Google Scholar]
- 21. Greene ML, Way N, Pahl K. Trajectories of perceived adult and peer discrimination among black, Latino, and Asian American adolescents: patterns and psychological correlates. Dev Psychol. 2006;42(2):218–236. [DOI] [PubMed] [Google Scholar]
- 22. Brody GH, Yu T, Miller GE, et al. Discrimination, racial identity, and cytokine levels among African-American adolescents. J Adolesc Health. 2015;56(5):496–501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Simons RL, Lei MK, Beach SRH, et al. Discrimination, segregation, and chronic inflammation: testing the weathering explanation for the poor health of black Americans. Dev Psychol. 2018;54(10):1993–2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Krieger N, Smith K, Naishadham D, et al. Experiences of discrimination: validity and reliability of a self-report measure for population health research on racism and health. Soc Sci Med. 2005;61(7):1576–1596. [DOI] [PubMed] [Google Scholar]
- 25. Kessler RC, Mickelson KD, Williams DR. The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. J Health Soc Behav. 1999;40(3):208–230. [PubMed] [Google Scholar]
- 26. Sims M, Wyatt SB, Gutierrez ML, et al. Development and psychometric testing of a multidimensional instrument of perceived discrimination among African Americans in the Jackson Heart Study. Ethn Dis. 2009;19(1):56–64. [PMC free article] [PubMed] [Google Scholar]
- 27. Pérez DJ, Fortuna L, Alegria M. Prevalence and correlates of everyday discrimination among U.S. Latinos. J Community Psychol. 2008;36(4):421–433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Dohrenwend BP. Inventorying stressful life events as risk factors for psychopathology: toward resolution of the problem of intracategory variability. Psychol Bull. 2006;132(3):477–495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Reuben A, Moffitt TE, Caspi A, et al. Lest we forget: comparing retrospective and prospective assessments of adverse childhood experiences in the prediction of adult health. J Child Psychol Psychiatry. 2016;57(10):1103–1112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.University of Alabama at Birmingham. CARDIA. Scientific Resources Section. https://www.cardia.dopm.uab.edu/study-information. Accessed April 15, 2021.
- 31. Congressional Budget Office . Trends in the Distribution of Household Income Between 1979 and 2007. (Publication no. 4031). Washington, DC: Congressional Budget Office; 2011. https://www.cbo.gov/publication/42729. Accessed April 15, 2021. [Google Scholar]
- 32. Williams DR, Yan Y, Jackson JS, et al. Racial differences in physical and mental health: socio-economic status, stress and discrimination. J Health Psychol. 1997;2(3):335–351. [DOI] [PubMed] [Google Scholar]
- 33. Borrell LN, Kiefe CI, Diez-Roux AV, et al. Racial discrimination, racial/ethnic segregation, and health behaviors in the CARDIA Study. Ethn Health. 2013;18(3):227–243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Bey GS, Jesdale B, Forrester S, et al. Intersectional effects of racial and gender discrimination on cardiovascular health vary among black and white women and men in the CARDIA Study. SSM Popul Health. 2019;8:100446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Ren XS, Amick BC, Williams DR. Racial/ethnic disparities in health: the interplay between discrimination and socioeconomic status. Ethn Dis. 1999;9(2):151–165. [PubMed] [Google Scholar]
- 36. van Dyke M, Vaccarino V, Dunbar SB, et al. Socioeconomic status discrimination and C-reactive protein in African-American and white adults. Psychoneuroendocrinology. 2017;82:9–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Fuller-Rowell TE, Curtis DS, Chae DH, et al. Longitudinal health consequences of socioeconomic disadvantage: examining perceived discrimination as a mediator. Health Psychol. 2018;37(5):491–500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. van Dyke M, Vaccarino V, Quyyumi AA, et al. Socioeconomic status discrimination is associated with poor sleep in African-Americans, but not whites. Soc Sci Med. 2016;153:141–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Krieger N, Sidney S. Racial discrimination and blood pressure: the CARDIA study of young black and white adults. Am J Public Health. 1996;86(10):1370–1378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Allen AM, Thomas MD, Michaels EK, et al. Racial discrimination, educational attainment, and biological dysregulation among midlife African American women. Psychoneuroendocrinology. 2019;99:225–235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Paradies Y, Ben J, Denson N, et al. Racism as a determinant of health: a systematic review and meta-analysis. PLoS One. 2015;10(9):e0138511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Funch DP, Marshall JR. Measuring life stress: factors affecting fall-off in the reporting of life events. J Health Soc Behav. 1984;25(4):453–464. [PubMed] [Google Scholar]
- 43. Kessler RC, Wethington E. The reliability of life event reports in a community survey. Psychol Med. 1991;21(3):723–738. [DOI] [PubMed] [Google Scholar]
- 44. Carstensen LL, Isaacowitz DM, Charles ST. Taking time seriously. A theory of socioemotional selectivity. Am Psychol. 1999;54(3):165–181. [DOI] [PubMed] [Google Scholar]
- 45. Lewis TT, Van Dyke M. Discrimination and the health of African Americans: the potential importance of intersectionalities. Curr Dir Psychol Sci. 2018;27(3):176–182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Gee GC, Walsemann KM, Brondolo E. A life course perspective on how racism may be related to health inequities. Am J Public Health. 2012;102(5):967–974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Krieger N. Measures of racism, sexism, heterosexism, and gender binarism for health equity research: from structural injustice to embodied harm—an ecosocial analysis. Annu Rev Public Health. 2020;41:37–62. [DOI] [PubMed] [Google Scholar]
- 48. Kershaw KN, Robinson WR, Gordon-Larsen P, et al. Association of changes in neighborhood-level racial residential segregation with changes in blood pressure among black adults: the CARDIA Study. JAMA Intern Med. 2017;177(7):996–1002. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.