

Abstract
Context:
Anterior cruciate ligament (ACL) injury risk reduction programs have become increasingly popular. As ACL injuries continue to reflect high incidence rates, the continued optimization of current risk reduction programs, and the exercises contained within them, is warranted. The exercises must evolve to align with new etiology data, but there is concern that the exercises do not fully reflect the complexity of ACL injury mechanisms. It was outside the scope of this review to address each possible inciting event, rather the effort was directed at the elements more closely associated with the end point of movement during the injury mechanism.
Objective:
To examine if exercises designed to reduce the risk of ACL injury reflect key injury mechanisms: multiplanar movement, single limb stance, trunk and hip dissociative control, and a flight phase.
Data Sources:
A systematic search was performed using PubMed, Medline, EBSCO (CINAHL), SPORTSDiscus, and PEDro databases.
Study Selection:
Eligibility criteria were as follows: (1) randomized controlled trials or prospective cohort studies, (2) male and/or female participants of any age, (3) exercises were targeted interventions to prevent ACL/knee injuries, and (4) individual exercises were listed and adequately detailed and excluded if program was unable to be replicated clinically.
Study Design:
Scoping review.
Level of Evidence:
Level 4.
Data Extraction:
A total of 35 studies were included, and 1019 exercises were extracted for analysis.
Results:
The average Consensus on Exercise Reporting Template score was 11 (range, 0-14). The majority of exercises involved bilateral weightbearing (n = 418 of 1019; 41.0%), followed by single limb (n = 345 of 1019; 33.9%) and nonweightbearing (n = 256 of 1019; 25.1%). Only 20% of exercises incorporated more than 1 plane of movement, and the majority of exercises had sagittal plane dominance. Although 50% of exercises incorporated a flight phase, only half of these also involved single-leg weightbearing. Just 16% of exercises incorporated trunk and hip dissociation, and these were rarely combined with other key exercise elements. Only 13% of exercises challenged more than 2 key elements, and only 1% incorporated all 4 elements (multiplanar movements, single limb stance, trunk and hip dissociation, flight phase) simultaneously.
Conclusion:
Many risk reduction exercises do not reflect the task-specific elements identified within ACL injury mechanisms. Addressing the underrepresentation of key elements (eg, trunk and hip dissociation, multiplanar movements) may optimize risk reduction in future trials.
Keywords: exercise, hip, knee, injury prevention, neuromuscular training
Anterior cruciate ligament (ACL) injuries can be devastating to athletes. In the United States, 120,000 to 200,000 ACL injuries occur every year, 37 with surgical and related costs upward of $1 billion to $3 billion.36,53,63 ACL injury can have both significant short-term (time away from sport) and long-term implications.
They carry a high risk of reinjury, 57 with up to 50% of patients failing to return to their preinjury level of athletic participation.2,3,34,48 ACL injury is also associated with a significant increased risk for posttraumatic knee osteoarthritis, which may present as early as 2 years after initial ACL reconstruction. 57 In an effort to mitigate the effects of ACL injuries, particularly for society at large and for female athletes, ACL injury prevention programs have become increasingly popular. It is important to note, even though there have been tremendous resources placed into the research and development of ACL injury prevention programs, ACL injuries continue at a high rate.1,25,37,53,55,70,74 As ACL injuries continue to reflect high incidence rates, the continued optimization of current injury prevention programs is warranted. 65
In a meta-analysis of meta-analyses, Webster and Hewett 70 found conclusive evidence that injury prevention programs reduce the risk of ACL injury by half in female athletes. However, the risk reduction varies considerably across individual studies and there exist insufficient data to make conclusions on the effectiveness of injury prevention programs in male athletes. 70 This inconsistency may be driven by several factors, but variations in injury prevention programs content seem to be important, with published research comprising wide combinations of strength, balance, flexibility, and jump training elements. Reviews that have tried to identify which training elements are most associated with prophylactic effectiveness, have found greatest effectiveness in programs, specifically from controlled studies, emphasizing strengthening and proximal control training, 62 and some have failed to find strong evidence for an optimal and specific exercise combination.20,34,53
Understanding the global 3-dimensional position of the athlete’s body and the mechanisms that lead to ACL injuries is crucial to effectively design specific preventative exercises.14,21 Video analysis studies 14 provide insight into the situational patterns most associated with ACL injury in sport. An analysis of 107 ACL injuries in men’s soccer emphasizes the large proportion associated with mechanical perturbation to the upper body, single-leg landings, and high horizontal speeds. 14 Studies have also found that multidirectional, reactive phases of play (eg, pressing/defending/tackling) or high-speed jumping and landing events 42 were the most common inciting events. 14 These patterns largely corroborate previous research from male 69 and female 12 soccer players, American football, 35 and the rugby union. 45 There is also consistent evidence that a large proportion of ACL injury events involve large base of support to center of mass distance, 56 excessive or aberrant movements of the trunk, 33 and knee valgus moments, 58 particularly when the lower extremity is fixed on the ground (eg, timing related to landing from a jump).31,42
There is a concern that current ACL prevention exercises lack complexity.26,28,30 Although basic exercise programs are easily replicated in clinical trials, they may not adequately challenge motor learning in the athlete, and may lack context and specificity, when juxtaposed to complex injury mechanisms.9,27,28,30 Adopting a more complex approach to exercise design may invoke a nonlinear interaction between varying risk-factors, better preparing the athlete across multiple constructs simultaneously. 29
Although it is injury risk reduction that is the overarching goal of these programs, 70 the name “injury prevention programs” will be used to reflect the term most often utilized in the literature that was scoped. Our primary objective was to quantify the extent to which injury prevention programs incorporate complex tasks associated with common ACL injury mechanisms based on the presence or absence of multiplanar movements, single limb stance, trunk and hip dissociative control, and a flight phase (phase of gait when both feet are off the ground at the same time).
Methods
A systematic literature search was conducted after consulting the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) statement and the checklist completed. 68 The final protocol was registered with the Open Science Framework on April 8, 2020 (https://osf.io/wvqxp). A scoping review design and methodology was used because of the exploratory nature of the research question. Scoping reviews aim to report concepts and theories related to knowledge gaps on a specific topic and key factors related to a concept.46,68 Because of the nature of scoping reviews, the risk of bias assessment is not applicable and does not influence scoping review outcomes. 68 However, a measure of the quality of the reported injury prevention programs was relevant to this review. The assessment tool utilized was the Consensus on Exercise Reporting Template (CERT).59,60 A score for each included article on the quality of reporting the listed exercise program was recorded.
Search Strategy
A systematic literature search of the PubMed, EBSCO (CINAHL), Medline, Physiotherapy Evidence Database (PEDro), and SPORTDiscus databases was performed from inception to April 8, 2020, to obtain relevant studies for the review. Language was limited to English and study participants were all human. Electronic databases were searched using a combination of generalized keywords related to ACL injury prevention programs in an effort to obtain a broad search of injury prevention programs (anterior cruciate ligament* OR knee injur* AND prevent*). The search results are presented in the PRISMA-ScR flow diagram (Figure 1). A manual search of the reference lists from articles gathered during the primary search as well as from related systematic reviews was also performed.
Figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews flow diagram.
Eligibility Criteria
The inclusion criteria were the following: (1) randomized controlled trials, prospective cohort studies; (2) the authors clearly stated that the exercises in the reported program were targeted interventions to prevent ACL/knee injuries or explicitly part of an ACL injury prevention program; (3) male and/or female participants of any age; and (4) exercises contained in the ACL injury prevention programs must be specifically listed and the program explicitly detailed.
Study Selection
The identification of relevant articles, titles, and abstracts were downloaded into EndNote X8.2 (Thomson Reuters), where duplicates were removed. All relevant articles, titles, and abstracts were captured and independently screened by 5 authors applying the a priori inclusion criteria. If the abstract provided insufficient information to determine eligibility for inclusion, full-text articles were then retrieved. In the case of differing assessments of the retrieved studies between the reviewing authors, the specific study was collaboratively discussed among the assigned author and the principal investigator and a consensus was reached. All criteria were again independently applied by the authors to the full-text articles that passed the initial screening process. If a consensus could not be reached on the decision for final inclusion, another senior author was consulted. If multiple studies included the same ACL injury prevention program, only 1 study was included that detailed all the specific exercises. The authors of any duplicated programs were also acknowledged in the analysis.
Quality Assessment
Consensus on Exercise Reporting Template
The lead author randomly assigned the studies to the coauthors who extracted the intervention data and scored each program using the CERT reporting form with guidance from the Explanation and Elaboration Statement document. 59 The CERT is a 16-item checklist developed and endorsed by an international panel of exercise experts designed to assess the quality/comprehensiveness of reporting of exercise and contains seven categories: materials, provider, delivery, location, dosage, tailoring, and compliance. 60 After data extraction, any differences between reviewers were discussed and a final score was reached via a consensus meeting between the assessing author and the lead author. A third reviewer was consulted when consensus could not be met initially.
Data Extraction, Analysis, and Definitions
All therapeutic exercises were extracted for data analysis from the included studies. The elements of each exercise were chosen to assess commonly reported events occurring during an ACL injury (Appendix 1, available in the online version of this article). In instances where the listed exercise was not clear, it was marked with an asterisk and the senior authors collaborated to determine how the exercise should be analyzed. Two senior reviewers initially analyzed all the exercises, and exercises that needed another senior reviewer facilitated a final decision. A priori definitions were used to categorize each exercise element into the appropriate column, signifying if the element was present or not. It is acknowledged by the authors that many human movements can be argued to be multiplanar in nature, but it was the motive and intent of the prescribing author that was attempted to be captured, allowing the definitions to be as pragmatic and as relatable to a clinical context as possible. The exercise elements were defined as follows.
Plane of Movement
The exercise was analyzed to see how many planes of movement occurred to achieve the primary purpose. The knee joint has been reported to move in all 3 planes, 33 so this analysis sought to score if the exercises challenged the knee in multiple planes. There were 3 subcategories, including sagittal, frontal, and transverse planes. If an exercise was identified as multiplanar, the multiplanar box was checked, and then the 2 or 3 planes were also identified in the analysis. This analysis focused on identifying if the exercise reflected a progression to multi- or triplanar movements, which is reflective of sporting movements. 67 The highest level of complexity in this category would be an exercise that captured a multiplanar movement that included rotation in the transverse plane.
Sagittal plane
The primary intent of the exercise utilized movement that occurred primarily within the sagittal plane. Exercises such as forward and backward running, jumping, or hopping, and forward lunges were considered to occur primarily in the sagittal plane.
Frontal plane
The primary movement of the exercise occurred within the frontal plane. An example would be a side-lying straight leg raise, and more functional type exercises such as a side shuffle or lateral hops and jumps. If a frontal plane movement occurred with a coupled movement into another plane, the additional planes of movement were credited.
Transverse plane
The primary movement of the exercise occurred within the transverse plane. Seated external rotation with a band is an isolated transverse plane exercise. Exercises where the authors reported at least a quarter turn or a 90° rotational change of direction was included as movement on the transverse plane.
Weightbearing Status
The primary movement of the exercise was analyzed to determine how the lower extremities were contacting the ground. The analysis sought to determine if the target lower extremity was in a position of extension with the acetabulum oriented vertically over the femur in a long-axis full weightbearing position. This position rules out exercises such as bridging or quadruped as weightbearing in the context of preventing an ACL injury. The highest level of complexity in this category was single limb stance. When illustrations or written details were not provided, the authors conferred and agreed on how to score the exercise.
Unilateral weightbearing
The primary movement of the exercise had a single lower extremity contacting the ground, where the hip was in a position of extension and the acetabulum positioned over the femur in a long-axis full weightbearing position. The subject performing the exercise must have been in an upright vertical position. A single limb plank, although the hip is in extension, was not considered unilateral weightbearing for this reason.
Bilateral weightbearing
The primary intent of the exercise occurred when both the lower extremities were contacting the ground in the acetabulum over femur orientation of closed chain movement. All variations of lunges were considered to be bilateral weight bearing exercises because both feet were on the ground during the intentional phase of the exercise.
Nonweightbearing
The exercise was carried out while neither lower extremity was in a functional upright acetabulum over femur position with the feet on the ground. The category was analyzed to determine if the weight bearing position is reflective of the specific upright tasks encountered during the injury mechanism. Quadruped exercises, planks, Nordic hamstring curls, and bridging were not considered weightbearing since the method and position of delivery was not reflective of the upright position identified in the injury mechanism.
Trunk and Hip Dissociative Control
The authors of this review acknowledge that most any exercise or movement involves the trunk. This analysis seeks to assess if the trunk is deliberately and purposefully being involved in dissociative movements related to the pelvifemoral complex and lower extremity. The analysis was focused on the identified task, and if the exercise involved the dissociation of trunk. This element was scored as being present if there was a specific task of the trunk and pelvis, so essentially the acetabulum, is moving in a dissociative relationship with the femur. For example, how the trunk moves during single limb balance exercises on an unstable surface or during an exercise where the trunk is being utilized as a lever to dissociate its movement on a stable weightbearing extremity, as in a single limb dead lift, the trunk is purposefully moving in relation to a stable femur. The analysis was designed to identify how the trunk was moving over the femur because exercises aimed at improving trunk control may reduce ACL injury risk.33,61,72,73
Flight Phase
The exercise must include a phase where both lower extremities are simultaneously off the ground during the exercise. This would include any running, jumping, or hopping variations. The purpose was to identify if the exercise included a specific element of the injury mechanism, which would be a deceleratory landing phase. Injuries often occur during the landing phase, after running (which can occur in 30-100 ms), thus incorporating a landing element and focusing on lower limb and trunk alignment may induce neuromuscular adaptations and activation strategies to reduce ACL injury risk.20,64
Results
Exercise Analysis
A total of n = 1019 exercises were extracted from the 35 included studies (Appendix 1, available online). The number of exercises employed within each study varied considerably, with a median of 24 exercises per program (range, 4-104). The majority of exercises involved bilateral weightbearing (n = 418 of 1019; 41.0%), followed by single limb (n = 345 of 1019; 33.9%) and nonweightbearing (n = 256 of 1019; 25.1%) (Figure 2a). Nonweightbearing exercises typically involved variations of pelvic bridges, abdominal crunches, and planks. Most exercises (834 of 1019; 81.8%) involved movements in the sagittal plane, with just 27.3% and 10.6% involving the frontal and transverse planes, respectively (Figure 2b).
Figure 2.
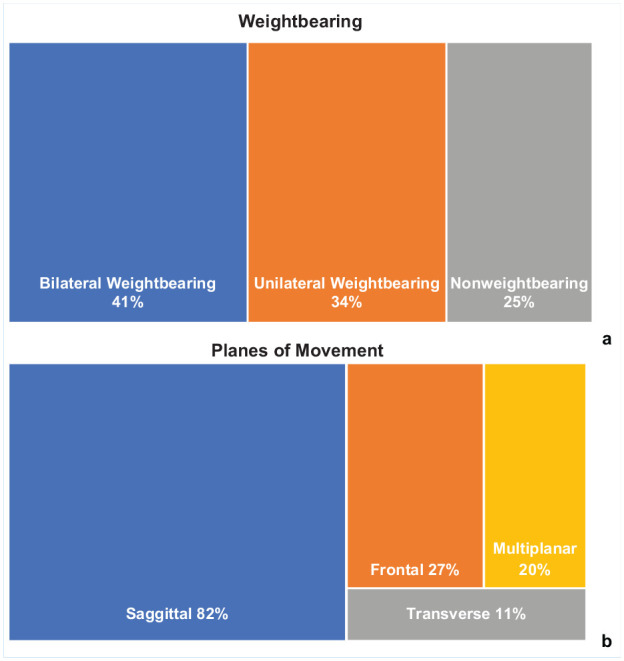
(a) Weightbearing. (b) Planes of movement.
Furthermore, only 1 in 5 exercises (19.5%) incorporated more than 1 plane of movement. The majority of multiplanar exercises (~94%) combined movements in either the sagittal/transverse (n = 86 of 199; 43.2%) such as jumps or lunges with a 90° or 180° turn in position or movements in the sagittal/frontal (n = 101 of 199; 50.7%) such as a squat to a lateral hop or jump or single limb balance on an unstable surface. Just 2 exercises (<0.1%), both versions of the T test, simultaneously challenged movement in all 3 planes. A total of n = 518 of 1019 (50.8%) exercises incorporated a flight phase component, of which, just under half involved a single-leg landing (n = 251). The most underrepresented exercise element was trunk and hip dissociative control, which was present in just 16.1% of all exercises (n = 164 or 1019). In all, 33.7% of exercises (344 of 1019) did not feature any of the core elements: (A) multiplanar movements, (B) single limb stance, (C) trunk and hip dissociative control, and (D) flight phase.
The Venn diagram (Figure 3) categorizes 675 exercises, with 41.6% (281 of 675) challenging a single element, represented by sections A, B, C, and D. The overlapping sections represent the various combinations of exercise elements. Overall, 58.3% of exercises (394 of 675) involved more than 1 element, but there is a general trend that as more elements are combined, the values in the Venn decrease. Overall, 38.5% (260 of 675) of exercises combined 2 elements, 16.4% (111/675) combined 3 elements, and just 3.4% (23/675) combined all 4 exercise elements. The most common combinations were BD (flight phase and single limb stance) and ABD (multiplanar movements, single limb stance, and flight phase). Exercises involving trunk and hip dissociation were underrepresented.
Figure 3.
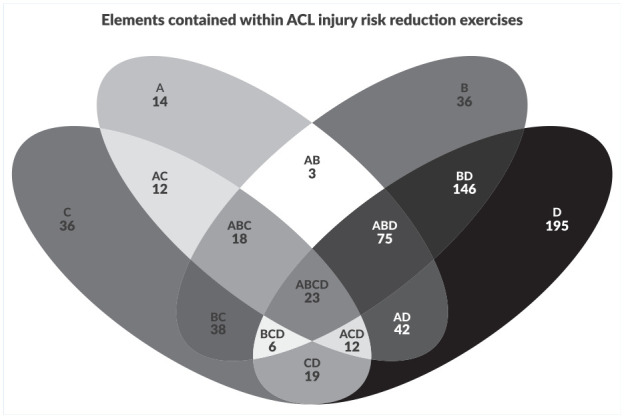
Venn diagram of exercise elements.
Quality Assessment
Consensus on Exercise Reporting Template
The CERT reporting form results (Appendix 2, available online) ranged from 0 to 14 (19 total possible points) with an average score of 11.0. Most shortcomings concerned items 7a, 9, 10, 11, 14a, and 15 (Figure 4). For calculation of the completeness of the exercise descriptions, a single score was calculated for CERT for each study. Items 1, 3, and 14a scored the highest; exercise equipment described, exercises performed individually or in a group and generic or individually tailored, each scoring affirmative in 35 of the 35 studies. None of the studies completed all items in the checklist, for a score of 19, the highest score for an individual CERT was 14, with 3 articles achieving the highest score.19,23,25
Figure 4.

Consensus on Exercise Reporting Template (CERT) scoring summary.
Discussion
This scoping review analyzes exercises contained within ACL injury risk reduction programs. Previous reviews in this field have categorized exercise-based training components using macroelements based on proximal control exercises, strength training, plyometrics, balance exercises, agility training, and flexibility.4,34,53,55,62,66 This may be the first review to quantify the extent to which individual exercises comprise task-specific elements (multiplanar movements, single limb stance, trunk and hip dissociative control, and a flight phase) closely associated with ACL injury mechanism. We analyzed an aggregate of 1019 exercises extracted from 35 studies. Overall, we found that few programs exposed athletes to the task-specific injury mechanism elements identified specifically contained within this review. It was also noted that representation diminished as multiple elements were combined into a singular exercise. Incorporating multiple elements, which may increase the complexity of the exercises, has the potential to improve motor learning strategies needed to control various interactions between multiple risk factors.
The large majority of exercises in the ACL injury prevention program literature have sagittal plane dominance (81.8%). Common examples were straight line running, squats, forward/reverse lunges, and forward/backward jumping/hopping. We acknowledge that straight ahead running was potentially used as a “warm-up” strategy versus an exercise for risk reduction. That said, if running/sprinting was listed as a clear part of the injury prevention program, it was analyzed as it was reported. It could not be assumed that running exercises were only utilized as non-risk-reducing activities. Adopting a shallow knee flexion angle on landing or side cutting is a key risk factor associated with ACL injuries, 14 and sagittal plane exercises may help to optimize landing mechanics, allowing athletes to better absorb ground-reaction forces.6,40,50 However, we would suggest that sagittal plane movements are overrepresented in the current literature. ACL injuries typically involve a multiplanar event, yet only 19.5% exercises challenged athletes in more than 1 movement plane. The majority of multiplanar movements (~94%), utilized the sagittal/frontal plane or sagittal/transverse plane. The fewest multiplanar exercises utilized the coupling of the frontal and transverse planes. A primary mechanism of the ACL injury is a valgus collapse about the frontal plane coupled with a rotational component,5,14,39,41,43,44 yet this multiplanar combination was only included in 1% (n = 10 of 1019) of the exercises analyzed. These exercises were primarily running sideways with a carioca or crossover type of movement or stationary exercises such as a lateral lunge with a rotational twist. These exercises met the definition of a multiplanar movement, but we would suggest that they are not fully representative of a high-speed deceleratory landing observed during sports. 14 Furthermore, these exercises were often in isolation and were rarely combined with the other exercise elements recognized as being present during an ACL injury (flight, single-leg stance, or trunk and hip control) 18 This seems to represent a reductionist approach common to many areas of musculoskeletal rehabilitation, whereby simplistic frameworks are applied to complex injury pathologies.7,8,10,15,16,29
It is well documented that a large proportion of ACL injuries occur in unilateral weightbearing, that is, some authors report as high as 70% of ACL injuries.38,45,49,69 This is not yet fully reflected in current injury prevention program literature, with 25% of exercises undertaken in nonweightbearing and 41% in bilateral weightbearing. Furthermore, many of these exercises focused on developing strength in various muscle groups, such as the quadriceps, hamstrings, hip abductors, and core musculature. Although strengthening exercises remain important, isolated strengthening does not fully address many of the aberrant biomechanical patterns associated with injury.5,54,71 Replicating the specificity of a task may improve neuromotor planning.27,28 As single-leg landings with a rotary component are a commonly reported mechanism of a noncontact ACL injury,45,49,69 it was surprising that there were so few exercises with these elements simultaneously represented.
Only 16.1% (164 of 1019) of exercises in ACL injury prevention programs incorporated trunk and hip dissociative control. This was also surprising as excessive or aberrant trunk movement is present in 34% to 83% of ACL injuries. 14 Aberrant trunk position alters muscle performance leading to, stiffer landings, 32 increased knee abduction moments, dynamic valgus, and ultimately excessive loading of the ACL. 31 In the current review, most trunk and hip dissociation exercises were limited to catching and throwing or single-leg dead lifts. Future injury prevention programs should consider hip focused progressions training to reduce the mediolateral landing posture, aligning foot contact with trunk position, 58 whereby allowing athletes to learn to control trunk perturbations, ipsilateral lean, and counter-trunk rotation movements.14,17
Optimal injury reduction methods require a task-specific approach, whereby exercises are progressed via specificity and optimal loading principles. 11 This means that injury prevention programs should eventually expose athletes to nonlinear and task-specific challenges that are representative of the forces and loads that may occur within open-systems, such as an injury event. 52 A multidimensional exercise approach will utilize principles of dynamic systems and motor learning principles to engage the athlete in movements that complex, yet safe and achievable. 11 The exercises should progress the athlete toward movements that will be encountered during sport, while ensuring a high quality of task performance with a criteria-based approach.11,18 This review clearly identifies that the current literature lacks many important exercise progressions and does not fully reflect the elements found within ACL injury mechanisms. The progression from uniplanar to multiplanar movements, and from bilateral to unilateral stance were underrepresented. The collective integration of all key exercise elements was rare, and we found just <1% of exercises incorporating flight phase, single-leg rotary loading, while simultaneously challenging the trunk, pelvis, and hip control beyond the sagittal plane.13,19,23-25,47,50
Last, when reporting and developing exercise-based interventions, the CERT is an available tool. 59 Programs designed to reduce the numbers of ACL injuries have inherent limitations that have been highlighted by utilizing the CERT scoring method. Programs to prevent ACL injuries are typically generically implemented to large groups, lacking individualization, without progression decisions being reported. Improved reporting of programs is critical to move forward in the quality and completeness of ACL injury prevention programs. A key shortcoming of the existing injury prevention program literature, however, is that few articles have published programs that are considered thoroughly reported according to the CERT scoring guidelines. This contributes to the known implementation challenges of intervention, individuality, adaptation, and fidelity. 22 Since many of the injury prevention programs reported here were published before the development of the CERT, there should be an improvement with the reporting of exercise programs moving forward.
Limitations
The authors of this review acknowledge the multidimensional nature of an ACL injury, and the complex interactions between both modifiable and non-modifiable risk factors as well as considering other infinite combinations of complex variables such as feedback, dosage, sport, age, and sex.26,51 This review only focuses on a specific portion of the exercise prescription and methods which is based on core elements associated with ACL injury. As the current literature is based primarily on more basic, preliminary exercises, we acknowledge the challenges associated with implementing task-specific exercises. For example, these exercises may require increased supervision to ensure appropriate performance, potentially making it less desirable for coaches and clinicians to implement, consequently, affecting fidelity. It is also a consideration that exercises reflective of injury mechanisms should be added as optimizing adjunctive exercises and should not be the sole focus of the program, which will avoid the program becoming so targeted they fail to provide a large enough “blanket effect” to reach a wide variety of sports.
Conclusion
Current injury prevention programs have reported reductions in injury, but the exact mechanism under which they reduce risk is unclear. Perhaps, optimal risk reduction in this field may require exercise progressions which culminate in movements that more closely resemble the mechanism of an ACL injury. This should ultimately include exercises that simultaneously integrate multiplanar movements, dissociative control between the trunk and hip, during single-leg landings. While it is pragmatic that more functionally task-specific exercises would be associated with greater risk reduction, high-quality prospective trials are warranted, before potential adoption and implementation.
Supplemental Material
Supplemental material, sj-docx-2-sph-10.1177_19417381211037966 for Do ACL Injury Risk Reduction Exercises Reflect Common Injury Mechanisms? A Scoping Review of Injury Prevention Programs by Steven L. Dischiavi, Alexis A Wright, Rachel A. Heller, Claire E. Love, Adam J. Salzman, Christian A. Harris and Chris M. Bleakley in Sports Health: A Multidisciplinary Approach
Supplemental material, sj-pdf-1-sph-10.1177_19417381211037966 for Do ACL Injury Risk Reduction Exercises Reflect Common Injury Mechanisms? A Scoping Review of Injury Prevention Programs by Steven L. Dischiavi, Alexis A Wright, Rachel A. Heller, Claire E. Love, Adam J. Salzman, Christian A. Harris and Chris M. Bleakley in Sports Health: A Multidisciplinary Approach
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
ORCID iD: Steven L Dischiavi  https://orcid.org/0000-0002-1133-2508
https://orcid.org/0000-0002-1133-2508
References
- 1. Agel J, Rockwood T, Klossner D. Collegiate ACL injury rates across 15 sports: National Collegiate Athletic Association Injury Surveillance System data update (2004-2005 through 2012-2013). Clin J Sport Med. 2016;26:518-523. [DOI] [PubMed] [Google Scholar]
- 2. Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48:1543-1552. [DOI] [PubMed] [Google Scholar]
- 3. Ardern CL, Taylor NF, Feller JA, Webster KE. Return-to-sport outcomes at 2 to 7 years after anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2012;40:41-48. [DOI] [PubMed] [Google Scholar]
- 4. Arundale AJH, Bizzini M, Giordano A, et al. Exercise-based knee and anterior cruciate ligament injury prevention. J Orthop Sports Phys Ther. 2018;48:A1-A42. [DOI] [PubMed] [Google Scholar]
- 5. Arundale AJH, Silvers-Granelli HJ, Marmon A, Zarzycki R, Dix C, Snyder-Mackler L. Changes in biomechanical knee injury risk factors across two collegiate soccer seasons using the 11+ prevention program. Scand J Med Sci Sports. 2018;28:2592-2603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bahr R. ACL injuries—problem solved? Br J Sports Med. 2009;43:313-314. [DOI] [PubMed] [Google Scholar]
- 7. Bekker S. Shuffle methodological deck chairs or abandon theoretical ship? The complexity turn in injury prevention. Inj Prev. 2019;25:80-82. [DOI] [PubMed] [Google Scholar]
- 8. Bekker S, Clark AM. Bringing complexity to sports injury prevention research: from simplification to explanation. Br J Sports Med. 2016;50:1489-1490. [DOI] [PubMed] [Google Scholar]
- 9. Benjaminse A, Otten B, Gokeler A, Diercks RL, Lemmink K. Motor learning strategies in basketball players and its implications for ACL injury prevention: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2017;25:2365-2376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguirre A, Ocarino JM, Fonseca ST. Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition-narrative review and new concept. Br J Sports Med. 2016;50:1309-1314. [DOI] [PubMed] [Google Scholar]
- 11. Blanchard S, Glasgow P. A theoretical model for exercise progressions as part of a complex rehabilitation programme design. Br J Sports Med. 2019;53:139-140. [DOI] [PubMed] [Google Scholar]
- 12. Brophy RH, Stepan JG, Silvers HJ, Mandelbaum BR. Defending puts the anterior cruciate ligament at risk during soccer: a gender-based analysis. Sports Health. 2015;7:244-249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Chena M, Rodriguez ML, Bores AJ, Ramos-Campo DJ. Effects of a multifactorial injuries prevention program in young Spanish football players. J Sports Med Phys Fitness. 2019;59:1353-1362. [DOI] [PubMed] [Google Scholar]
- 14. Della Villa F, Buckthorpe M, Grassi A, et al. Systematic video analysis of ACL injuries in professional male football (soccer): injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br J Sports Med. 2020;54:1423-1432. [DOI] [PubMed] [Google Scholar]
- 15. Dischiavi SL, Wright AA, Hegedus EJ, Bleakley CM. Biotensegrity and myofascial chains: a global approach to an integrated kinetic chain. Med Hypotheses. 2018;110:90-96. [DOI] [PubMed] [Google Scholar]
- 16. Dischiavi SL, Wright AA, Hegedus EJ, Bleakley CM. Rethinking dynamic knee valgus and its relation to knee injury: normal movement requiring control, not avoidance. J Orthop Sports Phys Ther. 2019;49:216-218. [DOI] [PubMed] [Google Scholar]
- 17. Dischiavi SL, Wright AA, Hegedus EJ, Ford KR, Bleakley C. Does ‘proximal control’ need a new definition or a paradigm shift in exercise prescription? A clinical commentary. Br J Sports Med. 2019;53:141-142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Dischiavi SL, Wright AA, Hegedus EJ, Thornton EP, Bleakley CM. Framework for optimizing ACL rehabilitation utilizing a global systems approach. Int J Sports Phys Ther. 2020;15:478-485. [PMC free article] [PubMed] [Google Scholar]
- 19. DiStefano LJ, Blackburn JT, Marshall SW, Guskiewicz KM, Garrett WE, Padua DA. Effects of an age-specific anterior cruciate ligament injury prevention program on lower extremity biomechanics in children. Am J Sports Med. 2011;39:949-957. [DOI] [PubMed] [Google Scholar]
- 20. Donnelly CJ, Elliott BC, Ackland TR, et al. An anterior cruciate ligament injury prevention framework: incorporating the recent evidence. Res Sports Med. 2012;20:239-262. [DOI] [PubMed] [Google Scholar]
- 21. Finch C. A new framework for research leading to sports injury prevention. J Sci Med Sport. 2006;9:3-9. [DOI] [PubMed] [Google Scholar]
- 22. Finch CF. Implementation and dissemination research: the time has come! Br J Sports Med. 2011;45:763-764. [DOI] [PubMed] [Google Scholar]
- 23. Finch CF, Doyle TL, Dempsey AR, et al. What do community football players think about different exercise-training programmes? Implications for the delivery of lower limb injury prevention programmes. Br J Sports Med. 2014;48:702-707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Foss KDB, Thomas S, Khoury JC, Myer GD, Hewett TE. A school-based neuromuscular training program and sport-related injury incidence: a prospective randomized controlled clinical trial. J Athl Train. 2018;53:20-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Fox AS, Bonacci J, McLean SG, Saunders N. Exploring individual adaptations to an anterior cruciate ligament injury prevention programme. Knee. 2018;25:83-98. [DOI] [PubMed] [Google Scholar]
- 26. Gokeler A, Benjaminse A, Hewett TE, et al. Feedback techniques to target functional deficits following anterior cruciate ligament reconstruction: implications for motor control and reduction of second injury risk. Sports Med. 2013;43:1065-1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Gokeler A, Neuhaus D, Benjaminse A, Grooms DR, Baumeister J. Principles of motor learning to support neuroplasticity after ACL injury: implications for optimizing performance and reducing risk of second ACL injury. Sports Med. 2019;49:853-865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Gokeler A, Seil R, Kerkhoffs G, Verhagen E. A novel approach to enhance ACL injury prevention programs. J Exp Orthop. 2018;5:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Gokeler A, Verhagen E, Hirschmann MT. Let us rethink research for ACL injuries: a call for a more complex scientific approach. Knee Surg Sports Traumatol Arthrosc. 2018;26:1303-1304. [DOI] [PubMed] [Google Scholar]
- 30. Grooms DR, Onate JA. Neuroscience application to noncontact anterior cruciate ligament injury prevention. Sports Health. 2016;8:149-152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Hewett TE, Myer GD. The mechanistic connection between the trunk, hip, knee, and anterior cruciate ligament injury. Exerc Sport Sci Rev. 2011;39:161-166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492-501. [DOI] [PubMed] [Google Scholar]
- 33. Hewett TE, Myer GD, Ford KR, Paterno MV, Quatman CE. Mechanisms, prediction, and prevention of ACL injuries: cut risk with three sharpened and validated tools. J Orthop Res. 2016;34:1843-1855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Huang YL, Jung J, Mulligan CMS, Oh J, Norcross MF. A majority of anterior cruciate ligament injuries can be prevented by injury prevention programs: a systematic review of randomized controlled trials and cluster-randomized controlled trials with meta-analysis. Am J Sports Med. 2020;48:1505-1515. [DOI] [PubMed] [Google Scholar]
- 35. Johnston JT, Mandelbaum BR, Schub D, et al. Video analysis of anterior cruciate ligament tears in professional American football athletes. Am J Sports Med. 2018;46:862-868. [DOI] [PubMed] [Google Scholar]
- 36. Joseph AM, Collins CL, Henke NM, Yard EE, Fields SK, Comstock RD. A multisport epidemiologic comparison of anterior cruciate ligament injuries in high school athletics. J Athl Train. 2013;48:810-817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Kaeding CC, Leger-St-Jean B, Magnussen RA. Epidemiology and diagnosis of anterior cruciate ligament injuries. Clin Sports Med. 2017;36:1-8. [DOI] [PubMed] [Google Scholar]
- 38. Kajiwara M, Kanamori A, Kadone H, et al. Knee biomechanics changes under dual task during single-leg drop landing. J Exp Orthop. 2019;6:5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Koga H, Nakamae A, Shima Y, Bahr R, Krosshaug T. Hip and ankle kinematics in noncontact anterior cruciate ligament injury situations: video analysis using model-based image matching. Am J Sports Med. 2018;46:333-340. [DOI] [PubMed] [Google Scholar]
- 40. Koga H, Nakamae A, Shima Y, et al. Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med. 2010;38:2218-2225. [DOI] [PubMed] [Google Scholar]
- 41. Kristianslund E, Faul O, Bahr R, Myklebust G, Krosshaug T. Sidestep cutting technique and knee abduction loading: implications for ACL prevention exercises. Br J Sports Med. 2014;48:779-783. [DOI] [PubMed] [Google Scholar]
- 42. Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35:359-367. [DOI] [PubMed] [Google Scholar]
- 43. McLean SG, Huang X, Su A, Van Den Bogert AJ. Sagittal plane biomechanics cannot injure the ACL during sidestep cutting. Clin Biomech (Bristol, Avon). 2004;19:828-838. [DOI] [PubMed] [Google Scholar]
- 44. McLean SG, Huang X, van den Bogert AJ. Association between lower extremity posture at contact and peak knee valgus moment during sidestepping: implications for ACL injury. Clin Biomech (Bristol, Avon). 2005;20:863-870. [DOI] [PubMed] [Google Scholar]
- 45. Montgomery C, Blackburn J, Withers D, Tierney G, Moran C, Simms C. Mechanisms of ACL injury in professional rugby union: a systematic video analysis of 36 cases. Br J Sports Med. 2018;52:994-1001. [DOI] [PubMed] [Google Scholar]
- 46. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18:143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Myer GD, Ford KR, McLean SG, Hewett TE. The effects of plyometric versus dynamic stabilization and balance training on lower extremity biomechanics.Am J Sports Med. 2006;34:445-455. [DOI] [PubMed] [Google Scholar]
- 48. Myklebust G, Bahr R. Return to play guidelines after anterior cruciate ligament surgery. Br J Sports Med. 2005;39:127-131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32:1002-1012. [DOI] [PubMed] [Google Scholar]
- 50. Olsen OE, Myklebust G, Engebretsen L, Holme I, Bahr R. Exercises to prevent lower limb injuries in youth sports: cluster randomised controlled trial. BMJ. 2005;330:449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Otte FW, Davids K, Millar SK, Klatt S. When and how to provide feedback and instructions to athletes? How sport psychology and pedagogy insights can improve coaching interventions to enhance self-regulation in training. Front Psychol. 2020;11:1444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Otte FW, Millar SK, Klatt S. Skill training periodization in “specialist” sports coaching—an introduction of the “PoST” framework for skill development. Front Sports Act Living. 2019;1:61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Padua DA, DiStefano LJ, Hewett TE, et al. National Athletic Trainers’ Association position statement: prevention of anterior cruciate ligament injury. J Athl Train. 2018;53:5-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Palmer K, Hebron C, Williams JM. A randomised trial into the effect of an isolated hip abductor strengthening programme and a functional motor control programme on knee kinematics and hip muscle strength. BMC Musculoskelet Disord. 2015;16:105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Petushek EJ, Sugimoto D, Stoolmiller M, Smith G, Myer GD. Evidence-based best-practice guidelines for preventing anterior cruciate ligament injuries in young female athletes: a systematic review and meta-analysis. Am J Sports Med. 2019;47:1744-1753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Sheehan FT, Sipprell WH, 3rd, Boden BP. Dynamic sagittal plane trunk control during anterior cruciate ligament injury. Am J Sports Med. 2012;40:1068-1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Shultz SJ, Schmitz RJ, Cameron KL, et al. Anterior Cruciate Ligament Research Retreat VIII summary statement: an update on injury risk identification and prevention across the anterior cruciate ligament injury continuum, March 14-16, 2019, Greensboro, NC. J Athl Train. 2019;54:970-984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Sigurðsson HB, Karlsson J, Snyder-Mackler L, Briem K. Kinematics observed during ACL injury are associated with large early peak knee abduction moments during a change of direction task in healthy adolescents. J Orthop Res. Published online December 6, 2020. doi: 10.1002/jor.24942 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Slade SC, Dionne CE, Underwood M, Buchbinder R. Consensus on Exercise Reporting Template (CERT): explanation and elaboration statement. Br J Sports Med. 2016;50:1428-1437. [DOI] [PubMed] [Google Scholar]
- 60. Slade SC, Dionne CE, Underwood M, et al. Consensus on Exercise Reporting Template (CERT): modified Delphi study. Phys Ther. 2016;96:1514-1524. [DOI] [PubMed] [Google Scholar]
- 61. Sugimoto D, Myer GD, Barber Foss KD, Pepin MJ, Micheli LJ, Hewett TE. Critical components of neuromuscular training to reduce ACL injury risk in female athletes: meta-regression analysis. Br J Sports Med. 2016;50:1259-1266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Sugimoto D, Myer GD, Foss KD, Hewett TE. Specific exercise effects of preventive neuromuscular training intervention on anterior cruciate ligament injury risk reduction in young females: meta-analysis and subgroup analysis.Br J Sports Med. 2015;49:282-289. [DOI] [PubMed] [Google Scholar]
- 63. Sugimoto D, Myer GD, McKeon JM, Hewett TE. Evaluation of the effectiveness of neuromuscular training to reduce anterior cruciate ligament injury in female athletes: a critical review of relative risk reduction and numbers-needed-to-treat analyses. Br J Sports Med. 2012;46:979-988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Tamura A, Akasaka K, Otsudo T, Shiozawa J, Toda Y, Yamada K. Dynamic knee valgus alignment influences impact attenuation in the lower extremity during the deceleration phase of a single-leg landing. PLoS One. 2017;12:e0179810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Taylor JB, Ford KR, Schmitz RJ, Ross SE, Ackerman TA, Shultz SJ. A 6-week warm-up injury prevention programme results in minimal biomechanical changes during jump landings: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2018;26:2942-2951. [DOI] [PubMed] [Google Scholar]
- 66. Taylor JB, Waxman JP, Richter SJ, Shultz SJ. Evaluation of the effectiveness of anterior cruciate ligament injury prevention programme training components: a systematic review and meta-analysis. Br J Sports Med. 2015;49:79-87. [DOI] [PubMed] [Google Scholar]
- 67. Taylor JB, Wright AA, Dischiavi SL, Townsend MA, Marmon AR. Activity demands during multi-directional team sports: a systematic review. Sports Med. 2017;47:2533-2551. [DOI] [PubMed] [Google Scholar]
- 68. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467-473. [DOI] [PubMed] [Google Scholar]
- 69. Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: a systematic video analysis of 39 cases. Br J Sports Med. 2015;49:1452-1460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Webster KE, Hewett TE. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. J Orthop Res. 2018;36:2696-2708. [DOI] [PubMed] [Google Scholar]
- 71. Willy RW, Davis IS. The effects of a hip strengthening program on running and squatting kinematics in females at risk for patellofemoral pain syndrome—2010 Combined Sections Meeting (CSM), San Diego, California, February 17-20, 2010. J Orthop Sports Phys Ther. 2010;40:A50. [Google Scholar]
- 72. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in neuromuscular control of the trunk predict knee injury risk: a prospective biomechanical-epidemiologic study. Am J Sports Med. 2007;35:1123-1130. [DOI] [PubMed] [Google Scholar]
- 73. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. The effects of core proprioception on knee injury: a prospective biomechanical-epidemiological study. Am J Sports Med. 2007;35:368-373. [DOI] [PubMed] [Google Scholar]
- 74. Zbrojkiewicz D, Vertullo C, Grayson JE. Increasing rates of anterior cruciate ligament reconstruction in young Australians, 2000-2015. Med J Aust. 2018;208:354-358. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-2-sph-10.1177_19417381211037966 for Do ACL Injury Risk Reduction Exercises Reflect Common Injury Mechanisms? A Scoping Review of Injury Prevention Programs by Steven L. Dischiavi, Alexis A Wright, Rachel A. Heller, Claire E. Love, Adam J. Salzman, Christian A. Harris and Chris M. Bleakley in Sports Health: A Multidisciplinary Approach
Supplemental material, sj-pdf-1-sph-10.1177_19417381211037966 for Do ACL Injury Risk Reduction Exercises Reflect Common Injury Mechanisms? A Scoping Review of Injury Prevention Programs by Steven L. Dischiavi, Alexis A Wright, Rachel A. Heller, Claire E. Love, Adam J. Salzman, Christian A. Harris and Chris M. Bleakley in Sports Health: A Multidisciplinary Approach