

Abstract
Background:
Greater neck strength is associated with fewer head and neck injuries. Neck-strengthening programs are commonly burdensome, requiring specialist equipment or significant time commitment, which are barriers to implementation.
Hypothesis:
Completing a neck-strengthening program will increase isometric neck strength in age-group rugby players.
Study Design:
A pilot randomized controlled exercise intervention study.
Level of Evidence:
Level 2.
Methods:
Twenty-eight U18 (under 18) male regional age-group rugby union players were randomized (intervention n =15/control n = 13). An 8-week exercise program was supervised during preseason at the regional training center. Control players continued their “normal practice,” which did not include neck-specific strengthening exercises. The 3-times weekly trainer-led intervention program involved a series of 15-second self-resisted contractions, where players pushed maximally against their own head, in forward, backward, left, and right directions.
Outcome Measure:
Peak isometric neck strength (force N) into neck flexion, extension, and left and right side flexion was measured using a handheld dynamometer.
Results:
Postintervention between-group mean differences (MDs) in isometric neck strength change were adjusted for baseline strength and favored the intervention for total neck strength (effect size [ES] = 1.2, MD ± 95% CI = 155.9 ± 101.9 N, P = 0.004) and for neck strength into extension (ES = 1.0, MD ± 95% CI = 59.9 ± 45.4 N, P = 0.01), left side flexion (ES = 0.7, MD ± 95% CI = 27.5 ± 26.9 N, P = 0.05), and right side flexion (ES = 1.3, MD ± 95% CI = 50.5 ± 34.4 N, P = 0.006).
Conclusion:
This resource-efficient neck-strengthening program has few barriers to implementation and provides a clear benefit in U18 players’ neck strength. While the present study focused on adolescent rugby players, the program may be appropriate across all sports where head and neck injuries are of concern and resources are limited.
Clinical Relevance:
Greater neck strength is associated with fewer head and neck injuries, including concussion. Performing this neck exercise program independently, or as part of a whole-body program like Activate, an interactive guide for players and coaches, could contribute to lower sports-related head and neck injuries.
Keywords: concussion, neck strength, rugby football, injury prevention
Concussion is the most common rugby match-play injury in men’s professional, 9 community,1,28 university, 30 and youth 19 levels of the game. Concussion is also the most common rugby match-play injury in Women’s Premiership 15 31 and collegiate 26 levels of the game. The consequences of concussion have been shown to occur over varying time frames, such as associated increases in subsequent injury risk8,23 and documented links with decrements in later-life cognitive function. 20 Despite the uncertainty surrounding the long-term effects of concussion in former players, reducing the incidence of concussion across rugby is recognized as a priority. 27
Youth rugby (under 18 years [U18]) players have significantly lower neck strength compared with adult rugby players,10,16 which may predispose these players to injury if this discrepancy is not addressed, particularly when transitioning to the adult game. Greater neck strength has been associated with decreased acceleration of the head during rugby contact events 11 and increasing neck strength is speculated as a potential means to help reduce incidence of concussion. 6 In professional, 24 adult, 1 and youth 19 players, lower head and neck injury incidence has been attributed to implementation of neck strength resistance exercises, although players’ neck strength was not always measured in these studies. Maximal loading improved neck strength in professional players 15 and in recreationally active college students, neck resistance exercises resulted in neurological adaptation, specifically reduced cross-sectional muscle recruitment for submaximal contractions, and increased cross-sectional muscle contribution for maximal contractions. 7 These studies demonstrate that neck muscle function can be altered with targeted resistance training, but the time and equipment demands are barriers to their implementation. 25 As the self-resisted neck exercises of the Activate program, 29 an interactive guide for players and coaches, require minimal time and no specialist equipment to complete, barriers to exercise implementation are few; in this context, whether the self-resisted neck exercises can improve neck strength warrants further investigation.
The aim of this research was to investigate the effect of self-resisted neck exercises on neck muscle strength in U18 male regional age-group rugby union players. If neck muscle strength increases postintervention, implementing the resistance program may benefit sporting populations where higher neck muscle strength is desirable.
Method
Study Design and Participants
This pilot parallel group randomized controlled trial was designed in accordance with the CONSORT framework 33 and was conducted between mid-July 2019 and end-September 2019. A convenience sampling method was used as one of the study team was the strength and conditioning coach for the U18 regional age-group, who delivered the program. The players were informed of the risks involved in the research. Written informed consent (players) and assent (parent/legal guardian) was provided before participation. Data collection and intervention implementation were conducted at a regional training center in Wales. Ethical approval was granted from the institution’s ethics board (ref: PGT-1315).
Sample Size
Using published data 15 sample size calculation indicated a minimum sample of 20 players (intervention = 10, control = 10) would be necessary to identify a 15% change in neck strength. All players (n = 34, mean ± SD; age = 16.9 ± 0.6 years, height = 180 ± 8 cm, mass = 87.8 ± 14.0 kg) were contacted for recruitment as a sample of 34 players would allow for a 30% drop out rate, while maintaining sufficient power.
Eligibility
Players were male members of the U18 regional age-group and had to be fit to participate in all training and matches; be free from upper limb, head and neck injury at enrollment and throughout the trial period; must not have completed targeted neck-strengthening exercises within the previous 6 months nor undertake targeted neck-strengthening exercises during the study period beyond those prescribed within the study; and have no current, or any history of undiagnosed neck pain.
Randomization and Blinding
Thirty-four players were stratified according to their playing position (forwards/backs) and randomized to either intervention or control group on a 1:1 basis by a member of the research team using a computer-generated list postenrollment (Figure 1). The tester (the team’s strength and conditioning coach) was not blinded to group allocation because he was also leading the intervention. Control players were not blinded to the intervention groups protocol. Analysis was performed blind by a member of the research group. Six players dropped out of the study: 4 from the control group (injury, n = 1; other reason, n = 3) and 2 from the intervention group (injury, n = 1; other reason = 1).
Figure 1.

Flowchart of participants through the study and timing of maximal voluntary isometric contraction (MVIC) testing blocks.
Training Protocols
Three times per week, for 8 weeks, the team’s strength and conditioning coach attended U18 squad training and led the intervention group protocol. An 8-week trial was considered sufficient stimulus for neuromuscular adaptation within the preseason period and could be completed before any competitive fixtures were scheduled. Training days followed players’ normal training patterns (Monday, Wednesday, Friday) and any injuries sustained within training sessions were reported to the team’s physical therapist. After the normal team warm-up, intervention players performed 1 maximal contraction in each direction (into neck flexion, extension, left side flexion and right side flexion) by pushing against their own head using their hands (Figure 2). Each contraction lasted 15 seconds and was performed with 30 seconds of rest between frontal and sagittal plane movements reflecting the Activate 29 program. Neck exercises, intensity, and volume were maintained throughout the trial period. The total time taken for all exercises was 3 minutes. Intervention players then continued their normal rugby training. Control group players maintained their normal training, which did not involve neck-specific muscle-strengthening exercises (see Appendix, available in the online version of this article).
Figure 2.

Illustration of hand placements for isometric neck strength training protocol. From the left image, contractions are into flexion, right side flexion, left side flexion, and extension.
Familiarization
Two weeks preceding baseline testing, all players were exposed to the neck-testing protocol to reduce likelihood of a learning effect. This involved performing each neck strength testing measure twice per player, limiting performances to 50% perceived effort.
Data Collection
Participants’ height (m) (Leicester Height Measure, Seca) and mass (kg) (SC-240 body composition monitor, Tanita) were recorded to help describe the sample population. Neck strength (peak isometric force [N]) was measured using a handheld dynamometer (HHD; Hoggan Scientific MicroFet 2) in frontal (right and left neck side-flexion) and sagittal planes (neck flexion, extension) and was reassessed after 8 weeks of intervention. A register of attendance was taken at each training session, while intervention players performed neck strength exercises to enable reporting of compliance during the study.
Neck Strength Measurement
Testing took place in the gymnasium of the regional training center. After a 24-hour rest period, where players were requested not to perform any vigorous activity, neck strength testing took place before players’ evening training. Before all testing sessions, each player was reminded of the testing procedures and performed a standardized warm-up, including range of motion exercises of the cervical spine and shoulder joints.
Participants sat on a 40-cm box in an upright position adjacent to a squat rack (Power Rack, Performance Power Rack, Perform Better Limited). A trunk fixation belt (Fixation Belt, Physique Management Company Ltd) was placed around the upper torso of the participant and an upright of the squat rack. The dynamometer was placed in line with the participant’s forehead behind the upright of the squat rack and held in position by the rater. A second fixation belt (head belt) was placed around the participant’s head (level with their eyebrows anteriorly, and occiput posteriorly), the upright of the squat rack and the dynamometer such that when the player contracted their neck muscles, the belt pulled the dynamometer into the upright of the rack. This method was devised to overcome the reliability of measures being affected by tester strength. 36 During neck flexion strength measurement, players sat facing away from the squat rack with their back against the upright of the squat rack. During extension strength measurement, players sat facing toward the squat rack. For left and right side flexion strength measurements, players sat with their right or left shoulder touching the front of the squat rack, respectively (Figure 3).
Figure 3.

Example of player and equipment positioning during maximal voluntary isometric contraction testing during neck left side flexion.
After a “ready, steady, start” instruction from the tester, players performed 3 maximal isometric contractions in each of the 4 directions: flexion, extension, right and left side flexion each separated by a 1-minute rest period. Ordering of measurements was randomized to reduce risk of systematic bias. Participants were instructed to gradually build up to a maximal contraction within 5 seconds. Players’ head position was monitored by the rater who encouraged a neutral head position was maintained during testing. All scores were recorded, and the highest score was used for analysis.
Analysis
Descriptive characteristics and neck strength were reported as mean and standard deviation. Overall compliance was measured as the number of compliant player-sessions/total potential compliant player-sessions. Because of the nature of attendance at regional training, players were assumed to have “completed exercises as directed”; thus, if they were in the intervention group and they attended training, then the neck exercises were performed. Differences in neck strength at 8 weeks (into flexion, extension, left side flexion, right side flexion, total [the sum of force in all directions]) compared with baseline were calculated for each player and expressed as a percentage relative to the player’s baseline strength. Between-group mean difference (MD, %) in neck strength change and 95% CI were calculated. Between-group neck strength change (N) was assessed using general linear model (one-way analysis of covariance [ANCOVA]), where the group (intervention/control) × “neck strength change” interaction was adjusted for baseline neck strength (covariate). Levene’s test was conducted and assumptions were met. Bonferroni post hoc test was used to explore differences between groups and was reported as adjusted MD and 95% CI. Effect size (ES) was estimated using Cohen d and quantified using standard ES analyses 5 (negligible ≤0.2, small >0.2-0.5, medium/moderate >0.5-0.8, large >0.8-1.2, and very large >1.2). A priori P < 0.05 was accepted for all analysis, and exact P values are stated.
Results
Twenty-eight players completed the study (intervention [n = 15, mean ± SD; height = 179 ± 7 cm; mass = 87.8 ± 14.0 kg; neck circumference = 38.2 ± 2.7 cm]; control [n = 13, mean ± SD; height = 181 ± 5 cm; mass = 87.9 ± 14.9 kg; neck circumference = 37.5 ± 2.2 cm]). Mean compliance across groups was 88% (intervention = 94% [253 of 270 player-sessions attended], control = 81% [189 of 234 player-sessions attended]). Baseline and posttrial neck strength is displayed in Table 1.
Table 1.
Peak voluntary isometric contraction force outputs (in N) for the cervical spine in 4 contraction directions (flexion, extension, left side flexion, and right side flexion) for the intervention and control groups at baseline and posttrial a
| Control (n = 13) | Intervention (n = 15) | |||
|---|---|---|---|---|
| Baseline, Mean ± SD, N | Posttrial, Mean ± SD, N | Baseline, Mean ± SD, N | Posttrial, Mean ± SD, N | |
| Flexion | 190.2 ± 35.0 | 222.2 ± 49.6 | 183.4 ± 36.0 | 225.8 ± 35.2 |
| Extension | 271.3 ± 73.2 | 307.2 ± 57.5 | 270.8 ± 72.9 | 376.3 ± 69.0 |
| Left side flexion | 184.9 ± 41.5 | 256.7 ± 40.1 | 192.1 ± 68.1 | 290.1 ± 60.8 |
| Right side flexion | 199.5 ± 60.8 | 240.5 ± 57.0 | 185.3 ± 59.0 | 291.8 ± 53.3 |
| Total | 845.9 ± 164.5 | 1026.5 ± 155.8 | 831.6 ± 204.5 | 1184 ± 189.4 |
Data are presented as group mean ± SD.
One-way ANCOVA identified significant differences in the magnitude of neck strength change between arms for total neck strength (F25, 2 = 8.794, P = 0.001, Figure 4), as well as neck strength into right side flexion (F25, 2 = 9.765, P = 0.001), left side flexion (F25, 2 = 5.302, P = 0.01), and extension (F25, 2 = 10.547, P < 0.001). The magnitude of neck strength change into flexion was not significant (F25, 2 = 2.328, P = 0.12) between arms.
Figure 4.
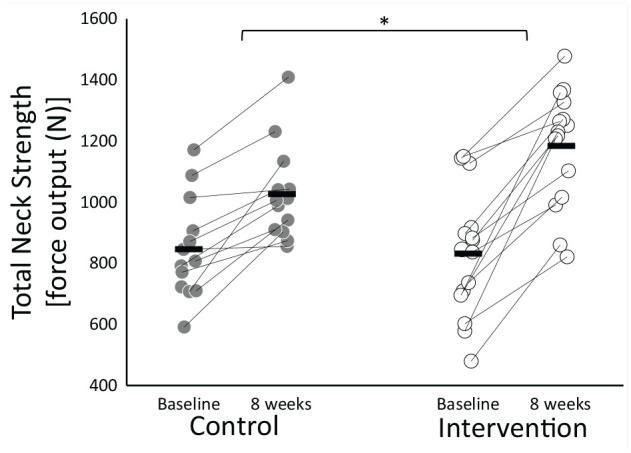
Total neck force (N) for the intervention and control groups at baseline and 8 weeks. Dots represent individual data points. Horizontal bars represent group mean values. Brackets with asterisk indicate significant difference between within-group peak strength change.
Post hoc analysis indicated a large effect (ES = 1.2, P = 0.004) in favor of the intervention for increase in total neck strength (MD = 155.9 N, 95% CI = 54.0-257.8 N) compared with control, a very large effect (ES = 1.3, P = 0.006) in favor of the intervention for increase in right side flexion neck strength (MD = 50.4 N, 95% CI = 16.0-84.7 N) compared with control, a moderate effect (ES = 0.7, P = 0.05) in favor of the intervention for increase in left side flexion neck strength (MD = 27.5 N, 95% CI = 0.6-54.4 N) compared with control, and a large effect (ES = 1.0, P = 0.01) in favor of the intervention for increase in extension neck strength (MD = 59.9 N, 95% CI = 14.5-105.3 N). The effect of the intervention on neck strength into flexion was small (ES = 0.3, MD = 8.8 N, 95% CI = −20.2 to 37.7 N) compared with control (Figure 5).
Figure 5.
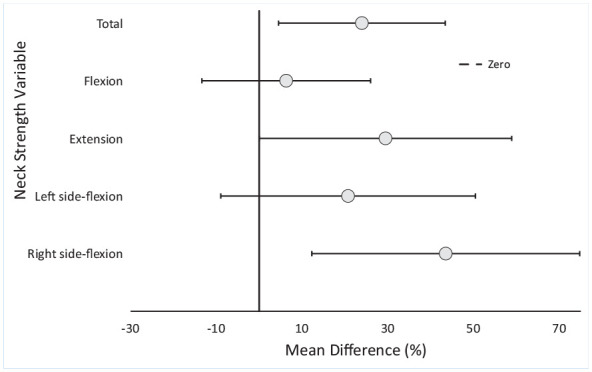
Mean difference (95% CI) between the intervention and control groups at 8 weeks. Vertical dashed line represents no effect compared with the control group.
Discussion
This is the first randomized controlled trial to evaluate the efficacy of self-resisted neck strength exercises on isometric neck strength in adolescent male rugby players. At 8 weeks, the intervention group total neck strength demonstrated a significant 24% increase over that of the control group. As lower neck strength has been associated with higher risk of injury, 6 this time-efficient neck-strengthening program, which requires no equipment to complete, may provide an important clinical benefit for players.
Previous studies have investigated the effect of different neck-strengthening programs with varying results. Strengthening programs that involved 50% to 70% maximal voluntary contraction during exercises for 5 to 6 weeks resulted in no clinically meaningful changes in total neck strength in male rugby players 2 under 19 years old or professional rugby players. 24 A 5-week program involving maximal resistance to an external load applied by a strength and conditioning coach resulted in a clinically significant ~19% increase in total neck strength compared with baseline in professional rugby players. 15 Exercises performed by amateur rugby players at 80% to 100% of maximal effort for 6 weeks, resulted in 12% to 24% mean increase in neck strength compared with control. 18 The present study prescribed exercises at 100% of “self-resistance” (the equivalent of 10/10 rated perceived exertion) and resulted in a 24% increase in total neck strength compared with controls at 8 weeks in adolescent male rugby players. As the weekly exercise prescriptions (2-3 times weekly) and study durations (5-8 weeks) were relatively similar across studies, it appears that near maximal to maximal loads may be required to induce meaningful changes in neck strength when considering isometric or isotonic neck exercises.
Posttrial, both intervention and control groups demonstrated improvements in neck strength from baseline, despite the control group not performing targeted neck specific strength exercises. In Premier rugby players, a significant ~10% increase was measured for total strength compared with noncontact control players over a 20-week season, 32 suggesting neck strength increases with exposure to contact training/match-play. As such, improvement in control group neck strength was anticipated. Across this study’s trial period, players likely received sufficient stimulus for strength adaptation from their normal training (a combination of strength and conditioning [3 × 1-hour weekly], and rugby-specific activities [3 × 1-hour weekly]). Muscles including the upper trapezius, erector spinae, and sternocleidomastoid stabilize the neck during scrummaging, 3 and limit shoulder depression and excessive neck movement during the tackle. As such these muscles receive stimulus within “normal training.” However, the 24% increase in total neck strength of the intervention group above that of the control group demonstrates program efficacy. This is a very encouraging result and supports implementation of these neck-strengthening exercises within elite age-group training environments.
Intervention group player-level compliance was high (94%), which is reflective of a regional training environment, where players are likely keen to maximize their training exposure. Club-level compliance was 100% (3 of 3 sessions per week), though this is because of a researcher being the strength and conditioning coach for the club. For comparison, club- and school-level mean compliance to the Activate program was 66% (2 of 3 sessions per week).1,19 To be effective as an injury prevention measure in the real world, 12 players must comply with the injury-prevention program. 22 Two neck-strengthening programs required equipment such as weights machines2,24 or head harnesses18,24 and required ~8 15 to 20 minutes 2 per player to perform, and 1 required trained personnel such as strength and conditioning coaches to apply resistance. 15 Time, personnel, and equipment are common barriers to compliance, particularly within nonprofessional settings. 25 Our exercise program, reflecting neck exercises recommended in Activate,1,19,29 was completed by all players simultaneously with no equipment requirement and required just 3 minutes for the whole squad to complete. With limited resources available to adolescent players, we believe this exercise program has potential to be an effective means for improving neck strength.
Before implementing a training program, particularly where injury prevention is concerned, the return on investment of implementation should be considered. 13 In cluster randomized controlled trial settings, Activate resulted in lower injury rates, including concussion, in rugby players.1,19 A proposed mechanism for the lower concussion rate was increased neck strength after players’ exposure to isometric neck-strengthening exercises.1,19 The present study employed neck strength exercises of Activate1,19,29 and demonstrated significant large increases in total neck strength in the intervention group compared with the control group. This study offers evidence that 1 potential mechanism for injury and concussion reduction when using the Activate program was an increase in neck strength. As whole-body approaches to injury prevention (such as FIFA 11+) have been suggested to provide a positive return on investment for clubs compared with individual exercises (such as the Nordic hamstring exercise), 13 implementation of the full Activate program in adolescent rugby settings is recommended.
Strengths and Limitations
Strengths of the study include the use of a representative sample from regional age-group rugby. Neck strength research involving U18 players has previously been limited to front-row players only.10,16 Another strength of this study is the results are valid across elite age-group environments as “real-world” methodology was employed. For instance, the effects of the intervention occurred despite less than 100% adherence, reflecting that in real life, players miss training and thus do not receive the ideal training load as was intended. Furthermore, no player reported any adverse event associated with the program to the team’s physical therapist during the trial.
A major limitation of this study is that the method of measuring neck strength is not well established and has not been published in the peer-reviewed literature. However, isometric neck muscle testing is well validated,4,14,17,21,34,35 and this study’s technique overcomes limitations of previous HHD methods relating to tester strength, 36 the potential for eccentric strength capture as per a “break contraction” method,10,15 and maintaining a standardized head position compared with self-testing. 34 Reviewing the force output measured during this study, the players strength was similar to that of U18 school rugby players (mean ± 95% CI = 333.4 ± 79.4 N), which was a similar population. 17 Another limitation is that the exercises were self-administered by players, and the actual load applied by players was not evaluated and could have been inconsistent. Because of the strength and conditioning coach delivering the intervention and performing neck strength testing, they could not be blinded and thus could have influenced players’ efforts. Finally, the number of players, tested was small and this should be viewed as a pilot study.
There is growing evidence that performing neck-strengthening exercises as part of a warm-up,1,19 or within strength and conditioning sessions 24 has been associated with fewer head and neck injuries, including concussion in rugby. Higher neck strength has also been associated with reduced concussion in high school athletes. 6 The present study demonstrates that a 3-minute neck strength program taken from Activate offers an efficacious means for adolescent rugby players to improve their neck strength. In the absence of evidence suggesting the program could cause harm, there is compelling evidence that neck strengthening should be included within players’ training, ideally 3 times weekly and, as it has been shown to reduce incidence of injuries in rugby, as part of the Activate program. The minimal time burden and no need for equipment mean neck strengthening has few barriers to implementation and provides a clear beneficial improvement in players neck strength. While the present study focused on adolescent rugby players, this approach to neck strengthening may be appropriate across all sports where head and neck injuries occur.
Key Points
Findings
Implementing self-resisted neck strength exercises 3 times per week increased age-group rugby players’ neck strength compared with players’ normal practice.
Implications
Greater neck strength has been associated with lower risk of head and neck injury, including concussion in athletes. This approach to neck strengthening may be appropriate across all sports where head and neck injury are of concern.
Caution
Inferences made regarding associations between higher neck strength and lower concussion risk have not been established in clinical trials and should be interpreted with caution.
Supplemental Material
Supplemental material, sj-docx-1-sph-10.1177_19417381211044736 for Eight Weeks of Self-Resisted Neck Strength Training Improves Neck Strength in Age-Grade Rugby Union Players: A Pilot Randomized Controlled Trial by Matthew J. Attwood, Lewis-Jon W. Hudd, Simon P. Roberts, Gareth Irwin and Keith A. Stokes in Sports Health: A Multidisciplinary Approach
Acknowledgments
The authors would like to sincerely thank all staff and the players that supported or otherwise participated in this study from Dragons Rugby Football Club.
Footnotes
The following authors declared potential conflicts of interest: M.J.A., S.P.R., and K.A.S. report grants from Rugby Football Union, outside the submitted work. G.I. reports grants from World Rugby, outside the submitted work.
References
- 1. Attwood MJ, Roberts SP, Trewartha G, England M, Stokes K. Efficacy of a movement control injury prevention programme in adult men’s community rugby union: a cluster randomised controlled trial. Br J Sports Med. 2018;52:368-374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Barrett MD, McLoughlin TF, Gallagher KR, et al. Effectiveness of a tailored neck training program on neck strength, movement, and fatigue in under-19 male rugby players: a randomized controlled pilot study. Open Access J Sports Med. 2015;6:137-147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Cazzola D, Stone B, Holsgrove T, Trewartha G, Preatoni E. Spinal muscle activity during different rugby scrum engagement procedures. In: Colloud F, Domalain M, Monnet T, eds. Proceedings of the 33rd International Conference on Biomechanics in Sports, Poitiers, France. 2016:559. [Google Scholar]
- 4. Chiu TT, Sing KL. Evaluation of cervical range of motion and isometric neck muscle strength: reliability and validity. Clin Rehabil. 2002;16:851-858. [DOI] [PubMed] [Google Scholar]
- 5. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Lawrence Erlbaum; 1988. [Google Scholar]
- 6. Collins CL, Fletcher EN, Fields SK, et al. Neck strength: a protective factor reducing risk for concussion in high school sports. J Prim Prev. 2014;35:309-319. [DOI] [PubMed] [Google Scholar]
- 7. Conley MS, Stone MH, Nimmons M, Dudley G. Resistance training and human cervical muscle recruitment plasticity. J Appl Physiol (1985). 1997;83:2105-2111. [DOI] [PubMed] [Google Scholar]
- 8. Cross M, Kemp S, Smith A, Trewartha G, Stokes K. Professional Rugby Union players have a 60% greater risk of time loss injury after concussion: a 2-season prospective study of clinical outcomes. Br J Sports Med. 2015;50:926-931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Cross M, Trewartha G, Kemp S, et al. Concussion in rugby union: improved reporting, a more conservative approach or an increased risk? Br J Sports Med. 2017;51:309. [Google Scholar]
- 10. Davies M, Moore IS, Moran P, Mathema P, Ranson CA. Cervical range of motion, cervical and shoulder strength in senior versus age-grade Rugby Union International front-row forwards. Phys Ther Sport. 2016;19:36-42. [DOI] [PubMed] [Google Scholar]
- 11. Dempsey AR, Fairchild TJ, Appleby BB. The relationship between neck strength and head accelerations in a rugby tackle. In: Colloud F, Domalain M, Monnet T, eds. Proceedings of the 33rd International Conference on Biomechanics in Sports, Poitiers, France. 2016:551-554. [Google Scholar]
- 12. Finch C. A new framework for research leading to sports injury prevention. J Sci Med Sport. 2006;9:3-9. [DOI] [PubMed] [Google Scholar]
- 13. Fuller CW. Assessing the return on investment of injury prevention procedures in professional football. Sports Medicine. 2019:49;621-629. [DOI] [PubMed] [Google Scholar]
- 14. Garcés GL, Medina D, Milutinovic L, Garavote P, Guerado E. Normative data- base of isometric cervical strength in a healthy population. Med Sci Sports Exerc. 2002;33:464-470. [DOI] [PubMed] [Google Scholar]
- 15. Geary K, Green BS, Delahunt E. Effects of neck strength training on isometric neck strength in rugby union players. Clin J Sport Med. 2014;24:502-508. [DOI] [PubMed] [Google Scholar]
- 16. Hamilton DF, Gatherer D, Robson J, et al. Comparative cervical profiles of adult and under-18 front row rugby players: implications for playing policy. BMJ Open. 2014;4:e004975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Hamilton DF, Simpson HR, Gatherer D. Repeatability and inter-tester reliability of a new tool to assess isometric neck strength in adolescents. In: Proceedings of Physiotherapy Research Society, Middlesbrough. Physiotherapy Research Society; 2010. [Google Scholar]
- 18. Hamlin M, Deuchress R, Elliot C, Raj T, Promkeaw D, Phonthee S. Effect of a 6-week exercise intervention for improved neck muscle strength in amateur male rugby union players. J Sport Exerc Sci. 2020;4:33-40. [Google Scholar]
- 19. Hislop MD, Stokes KA, Williams S, et al. Reducing musculoskeletal injury and concussion risk in schoolboy rugby players with a pre-activity movement control exercise programme: a cluster randomised controlled trial. Br J Sports Med. 2017;51:1140-1146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Hume PA, Theadom A, Lewis GN, et al. A comparison of cognitive function in former Rugby Union players compared with former non-contact-sport players and the impact of concussion history. Sports Med. 2016;417:1209-1220. [DOI] [PubMed] [Google Scholar]
- 21. Jordan A, Mehlsen J, Bülow PM, Ostergaard K, Danneskiold-Samsøe B. Maximal isometric strength of the cervical musculature in 100 healthy volunteers. Spine (Phila Pa 1976). 1999;24:1343-1348. [DOI] [PubMed] [Google Scholar]
- 22. McKay CD, Verhagen E. ‘Compliance’ versus ‘adherence’ in sport injury prevention: why definition matters. Br J Sports Med. 2016;50:382-383. [DOI] [PubMed] [Google Scholar]
- 23. Moore IS, Mount S, Mathema P, Ranson C. Application of the subsequent injury categorisation model for longitudinal injury surveillance in elite rugby and cricket: intersport comparisons and inter-rater reliability of coding. Br J Sports Med. 2018;52:1137-1142. [DOI] [PubMed] [Google Scholar]
- 24. Naish R, Burnett A, Burrows S, Andrews W, Appleby B. Can a specific neck strengthening program decrease cervical spine injuries in a men’s professional Rugby Union team? A retrospective analysis. J Sports Sci Med. 2013;12:542-550. [PMC free article] [PubMed] [Google Scholar]
- 25. O’Brien J, Finch CF. The implementation of musculoskeletal injury-prevention exercise programmes in team ball sports: a systematic review employing the RE-AIM framework. Sports Med. 2014;44:1305-1318. [DOI] [PubMed] [Google Scholar]
- 26. Peck KY, Johnston DA, Owens BD, Cameron KL. The incidence of injury among male and female intercollegiate rugby players. Sports Health. 2013;5:327-333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Raftery M, Tucker R, Falvey ÉC. Getting tough on concussion: how welfare-driven law change may improve player safety—a Rugby Union experience. Br J Sports Med. 2021;55:527-529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Roberts SP, Trewartha G, England M, Goodison W, Stokes KA. Concussions and head injuries in English Community Rugby Union match play. Am J Sports Med. 2016;45:480-487. [DOI] [PubMed] [Google Scholar]
- 29. Rugby Football Union. Activate adult—injury prevention exercise programme [2017]. Accessed April 28, 2019. https://www.englandrugby.com/dxdam/b1/b10a5208-cc25-413b-9475-c1902a4f54cd/Activate%20Adult-v7.pdf
- 30. Rugby Football Union. BUCS Super Rugby Injury Surveillance Project Season Report 2017-2018. Accessed June 18, 2020. https://www.englandrugby.com/dxdam/b5/b57fb79a-3a0e-4ba8-8719-4bd540e9ea1e/BUCS%20ISP%20Annual%20Report%202017-18.pdf
- 31. Rugby Football Union. Women’s Rugby Injury Surveillance Project Season Report 2017/18 Accessed June 29, 2020. https://www.englandrugby.com//dxdam/b8/b84c93db-c91d-4c5a-a45c-30fad4bfeb81/WRISP%2017-18.pdf. Accessed June 29, 2020.
- 32. Salmon DM, Sullivan SJ, Handcock P, Rehrer NJ, Niven B. Neck strength and self-reported neck dysfunction: what is the impact of a season of Rugby Union? J Sports Med Phys Fitness. 2018;58:1078-1089. [DOI] [PubMed] [Google Scholar]
- 33. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Versteegh T, Beaudet D, Greenbaum M, Hellyer L, Tritton A, Walton D. Evaluating the reliability of a novel neck-strength assessment protocol for healthy adults using self-generated resistance with a hand-held dynamometer. Physiother Can. 2015;67:58-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Wadsworth CT, Nielsen DH, Corcoran DS, Phillips CE. Interrater reliability of hand-held dynamometry: effects of rater gender, body weight, and grip strength. J Orthop Sports Phys Ther. 1992;16:74-81. [DOI] [PubMed] [Google Scholar]
- 36. Wikholm JB, Bohannon RW. Hand-held dynamometer measurements: tester strength makes a difference. J Orthop Sports Phys Ther. 1991;13:191-198. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-1-sph-10.1177_19417381211044736 for Eight Weeks of Self-Resisted Neck Strength Training Improves Neck Strength in Age-Grade Rugby Union Players: A Pilot Randomized Controlled Trial by Matthew J. Attwood, Lewis-Jon W. Hudd, Simon P. Roberts, Gareth Irwin and Keith A. Stokes in Sports Health: A Multidisciplinary Approach